 Aasiya Bano1
Aasiya Bano1 Piril Hepsomali2Fazle Rabbani3Umer Farooq4
Piril Hepsomali2Fazle Rabbani3Umer Farooq4 Ayesha Kanwal3Aisha Saleem4Ali Akbar Bugti5Aftab Alam Khan4Zainab Khalid4Mahroo Bugti6Shah Mureed7
Ayesha Kanwal3Aisha Saleem4Ali Akbar Bugti5Aftab Alam Khan4Zainab Khalid4Mahroo Bugti6Shah Mureed7 Saeed Khan8Ikram Din Ujjan9Sümeyye Şahin10
Saeed Khan8Ikram Din Ujjan9Sümeyye Şahin10 Mehtap Kara11
Mehtap Kara11 Amjad Khan12,13*
Amjad Khan12,13*- 1PEOC, Department of Health, Quetta, Balochistan, Pakistan
- 2School of Psychology, University of Roehampton, London, United Kingdom
- 3Department of Psychiatry, Lady Reading Hospital, Peshawar, Pakistan
- 4Ayub Medical College and Teaching Hospital, Abbottabad, Pakistan
- 5Department of General Surgery, Bolan Medical Complex Hospital (BMCH), Quetta, Pakistan
- 6Department of Gynaecology and Obstetrics, BMCH, Quetta, Pakistan
- 7Department of Paediatrics, BMCH, Quetta, Pakistan
- 8Department of Pathology, Dow University of Health Sciences, Karachi, Pakistan
- 9Department of Pathology, Liaquat University of Medical and Health Sciences (LUMHS), Jamshoro, Pakistan
- 10Department of Food Engineering, Ordu University, Ordu, Türkiye
- 11Department of Pharmaceutical Toxicology, Faculty of Pharmacy, Istanbul University, Istanbul, Türkiye
- 12Nuffield Division of Clinical Laboratory Sciences, Radcliffe Department of Medicine, University of Oxford, Oxford, United Kingdom
- 13Department of Biochemistry, LUMHS, Jamshoro, Pakistan
Background: Emotional distress conditions such as depression, anxiety, stress, and poor sleep are widespread health problems that have a significant impact on people’s lives. Conventional drugs are commonly prescribed to treat emotional distress and poor sleep conditions; however, these medications have several limitations and have shown multiple side effects. Over recent years botanicals-based pharmacological agents have gained increasing research and clinical interest in the management of emotional distress and sleep disorder. Of note, Melissa officinalis L. (MO) leaf extract has demonstrated considerable neuropharmacological properties both in animal and human studies and has emerged as a promising natural “calming agent.” However, research in this area is limited, and more studies are needed to validate its efficacy in amelioration of emotional distress and poor sleep conditions.
Objectives: We aimed to assess the pharmacological effects of subchronic supplementation of an innovative standardised phospholipid carrier-based MO aqueous extract on emotional distress and poor sleep conditions.
Design: A 3-week prospective, randomised, placebo-controlled, parallel-group, double-blinded clinical trial was conducted in 100 healthy adults complaining of a moderate degree of depression, anxiety, or stress, with scores of ≥14, ≥10, and ≥19, respectively, in the self-report Depression, Anxiety, and Stress Scale (DASS-42) or poor sleep, as indicated by the score of >5 in the Pittsburgh Sleep Quality Index (PSQI) scale. In addition, the impact of emotional distress and/or poor sleep on participants’ mental wellbeing, emotional feelings, and quality of life was also assessed using the self-reported Warwick–Edinburgh Mental Wellbeing Scale (WEMWBS), Positive and Negative Affect Schedule (PANAS) scale, and quality of life (WHO-QoL-BREF) scale, respectively.
Results: Oral supplementation of 200 mg of phospholipid-based MO aqueous extract (Relissa™) tablets twice a day (i.e., 400 mg/day) for 3 weeks led to significant improvements in the depressive mood, anxiety, stress, positive and negative affect (emotional feelings), overall mental wellbeing, and quality-of-life scores (all p values <0.001). Supplementation of MO extract was well tolerated, and no treatment-emergent effects or serious adverse events were reported.
Conclusion: According to the results of this study, the phospholipid carrier-based MO aqueous extract possesses considerable neuropharmacological properties, and its supplementation may provide a promising therapeutic option for the management of moderate emotional distress and/or poor sleep conditions.
Clinical Trial Registration: clinicaltrials.gov, identifier NCT05602688.
1 Introduction
Emotional distress conditions, such as depression, stress, anxiety, and insomnia (sleep disorder), are the most prevalent mental health conditions affecting a considerable amount of people worldwide (the prevalence of sleep problems ranges from 5.0% to 50.0% (Morin and Jarrin, 2022), while depressive and anxiety disorders affect more than 280 million and 300 million people, respectively (World Health Organization, 2022), causing significant disruption to everyday life, affecting performance in occupational and educational settings, and placing considerable burden (trillions of dollars) on healthcare systems (Hafner et al., 2017; Hillman et al., 2018). It is also important to note that the COVID-19 pandemic has been found to trigger a 25% increase in the prevalence of anxiety and depression worldwide (Kupcova et al., 2023). Conventional drug treatment for depressive conditions involves the use of tricyclic antidepressants (TCAs), monoamine oxidase inhibitors (MAOIs), selective serotonin reuptake inhibitors (SSRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs), norepinephrine–dopamine reuptake inhibitors (NDRIs), and serotonin antagonists and reuptake inhibitors (SARIs) (Arroll et al., 2016), while for anxiety disorders, the drug therapies include SSRIs, SNRIs, pregabalin, TCAs, buspirone, benzodiazepines (BZDs), and MAOIs (Bandelow et al., 2022). However, published data suggest that 30%–60% of people do not comply with these synthetic antidepressant or anxiolytic medications due to adverse events or a signatory delay in effectiveness (Demyttenaere, 2001). According to various studies, most of the conventional drugs used for emotional distress are associated with multiple side effects, such as cognitive dysfunction, excessive sedation, sexual dysfunction, respiratory depression, withdrawal syndrome, seizures, and suicide, caused by prolonged drug use or high drug resistance (de Niet et al., 2009; Seldenrijk et al., 2015; Seldenrijk et al., 2017). Conversely, these were reduced in 45% of the reported studies where dietary supplements were used as adjuvant for the same indications (Yeung et al., 2018). Over the past decades, exploration in botanical psychopharmacology has received considerable attention due to its efficacy, excellent safety, and tolerability. With growing scientific evidence, physicians and patients have developed an interest in the use of botanical-based pharmacological therapies (the use of some of them is supported by the European Medicines Agency herbal monograph (European Medicines Agency, 2023)) for the management of emotional distress and poor sleep conditions (Head and Kelly, 2009; Kavan et al., 2009; Liu et al., 2015; Kenda et al., 2022).
Of note, amongst the several reported botanicals for psychopharmacology, the leaf extract of Melissa officinalis L. (MO), commonly known as lemon balm mint, has emerged as a promising natural “calming agent” (Sharifi-Rad et al., 2021) for emotional distress and related conditions. The main chemical constituents responsible for the MO pharmacological effects are reportedly diverse antioxidant polyphenols (with rosmarinic acid (RA) as the major compound (>5%) and flavonoids, e.g., luteolin-3′-O-glucuronide) and terpenes (with citronellal, neral, and geranial as the most abundant constituents), among others (Uritu et al., 2018). Melissa officinalis L. extract is one of the most popular and widely used dietary supplements in central and southern Europe, the Mediterranean region, the United States, and South and West Asia. Historically, the therapeutic use of MO dates back over 2000 years through the Greeks and the Romans and is mentioned in the Historia Plantarum (approximately 300 B.C.) as “honey leaf”. For centuries, MO has been used in traditional Chinese medicine (TCM), traditional Persian medicine (TPM), Ayurvedic medicine, Arabic medicine, and medieval European medicine for treating diverse health conditions, such as insomnia, migraines, neuroses, and hysteria, among others (Shakeri et al., 2016). In the modern pharmacological studies, various human clinical trials (Kennedy et al., 2002; Akhondzadeh et al., 2003; Kennedy et al., 2003; Kennedy et al., 2004; Kennedy et al., 2006; Cases et al., 2011; Alijaniha et al., 2015; Ranjbar et al., 2018a; Ranjbar et al., 2018b; Haybar et al., 2018; Heydari et al., 2018; Soltanpour et al., 2019; Araj-Khodaei et al., 2020; Noguchi-Shinohara et al., 2020; Shirazi et al., 2021), animal models (Coleta et al., 2001; Guginski et al., 2009; Ibarra et al., 2010; Yoo et al., 2011; Taiwo et al., 2012; Feliú-Hemmelmann et al., 2013; Lin et al., 2015; Ghazizadeh et al., 2020; Talebi et al., 2022), and in vitro studies (Kennedy et al., 2003; Awad et al., 2007; Awad et al., 2009; López et al., 2009; Sahin et al., 2016) have investigated the neurotherapeutic effects of MO extract, with most studies reporting its antidepressant, anti-stress, anxiolytic, anti-insomnia, and anti-oxidative stress (neuroprotective) properties. According to reported evidence, the neuropharmacological effects of MO extract are due to its various biological properties, i.e., its GABAergic properties (upregulation of γ-amino butyric acid (GABA) through GABA-transaminase (GABA-T) inhibition (Awad et al., 2007; Awad et al., 2009; Yoo et al., 2011), GABAA receptor affinity (Salah and Jäger, 2005; Abuhamdah et al., 2008; Sahin et al., 2016)), modulation of the serotonergic pathway (Dimpfel and Suter, 2008; Lin et al., 2015), and inhibition of acetylcholine esterase (AChE) (Perry et al., 1996; Ferreira et al., 2006; Dastmalchi et al., 2009) and monoamine oxidase (MAO) enzymes (Ulbricht et al., 2005; López et al., 2009; Taiwo et al., 2012; Shakeri et al., 2016). Some other studies have suggested that the neuropharmacological mechanism of MO extract may be due to its direct nicotinic and muscarinic cholinergic receptor binding properties (Perry et al., 1996; Wake et al., 2000; Kennedy et al., 2003) and its ability to decrease corticosterone levels (Yoo et al., 2011; Feliú-Hemmelmann et al., 2013). Melissa officinalis L extract also possesses strong antioxidant properties and helps in the protection of neuronal cells against oxidative stress damage (López et al., 2009; Miraj et al., 2017).
However, therapeutic evidence for MO’s neuropharmacological effects is still limited, and the determination of its optimal clinical dosage and duration remains unknown (Świąder et al., 2019). Further studies are needed to validate the efficacy of MO extract supplementation in conditions of depression, mood, anxiety, stress, and related conditions and to demonstrate its mechanism of action, safety, and tolerability. Moreover, many phytochemicals have limited bioavailability and bioactivity after ingestion due to their limited solubility, stability, and absorption characteristics. Hence, efforts should also be focused on developing efficient carrier systems to achieve improved MO bioavailability for physiological functions. In the present prospective, randomised, double-blinded, placebo-controlled clinical trial, for the first time, we investigated the possible neuropharmacological effects of an innovative phospholipid carrier-based (Phytosome™) MO aqueous extract (Relissa™) in individuals with a moderate degree of emotional distress and/or poor sleep conditions. It is anticipated that the phospholipid carrier will aid in achieving the maximum bioavailability of the extract chemical constituents for pharmacological MO effects.
2 Methods
2.1 Study participants
Participants were enrolled at Ayub Teaching Hospital, Abbottabad, Pakistan (PK); Lady Reading Hospital, Peshawar, Pakistan; and Bolan Medical Complex Hospital, Quetta, Pakistan, either at the hospital walk-in outpatients’ clinics or through community-based primary healthcare clinics from 3 January 2023 to 28 February 2023. The inclusion criteria were as follows: healthy adults, age: 18–65 years, of either gender, and with a moderate degree of depression, anxiety, or stress, i.e., with scores of ≥14, ≥10, and ≥19, respectively, in the self-report Depression, Anxiety, and Stress Scale (DASS-42) or poor sleep quality, i.e., score >5 in the Pittsburgh Sleep Quality Index (PSQI) scale. The exclusion criteria were as follows: current use of prescribed conventional medication or supplements for neuropsychiatric or severe sleep disorders; known history of neuropsychiatric or severe sleep disorders; history of any allergic reactions/hypersensitivity to MO extract or its constituent compounds; pregnant or lactating women, current use or history of illicit substance misuse; hypertension (systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90) or other cardiovascular diseases; body mass index (BMI) <18.5 and >29.9 kg/m2; hyperthyroidism, diabetes mellitus (DM), or cancer; use of blood thinner medications such as Coumadin (warfarin) or Plavix (clopidogrel), glaucoma medications like Travatan (travoprost), and chemotherapy drugs like tamoxifen and Camptosar (irinotecan); or any other condition or factor that in the opinion of the treating consultant contraindicates the use of MO extract for the participant.
The study was approved by the Institutional Ethics Review Committee of Ayub Teaching Hospital, Abbottabad, Pakistan (PK) (Ref. No. RC-/EA-01/194); Lady Reading Hospital, Peshawar, PK (Ref. No. 684/LRH/MTI); and Bolan Medical Complex Hospital, Quetta, PK (Ref. No. 5501). The study was carried out in accordance with the guidelines of the Declaration of Helsinki and Good Clinical Practice standards, and all participants provided informed written consent. The study was registered at clinicaltrials.gov, identifier NCT05602688.
2.2 Study design and treatment
This was a prospective, multi-centre, double-blinded, placebo-controlled, randomised clinical trial consisting of two arms: the MO phospholipid extract supplement and the placebo. By using G*Power, the sample size was estimated to be 50 subjects per group based on the results of the previous study, with a confidence interval of 0.95, a test power of 80%, and 25% sample attrition (Soltanpour et al., 2019). The anxiety score was utilised as a primary measure with an effect size of 0.97. The participants received the MO phospholipid extract supplement orally as a 200 mg tablet of Relissa™ (manufacturer: Indena S.p.A., Milan, Italy), taken at home twice a day after meals for 3 weeks. Relissa™ is an MO leaf aqueous extract that has been standardised to 17%–23% hydroxycinnamic acid derivatives; it is analysed for its rosmarinic acid content and formulated with the phospholipid (sunflower) (Phytosome™) carrier for improved bioavailability. Placebo tablets were indistinguishable in appearance from Relissa™ tablets and were used in the same way as Relissa™.
2.3 Clinical measures
Participants were screened for enrolment in the study using either the DASS-42 or PSQI questionnaire (provided in hard copies to the participants by a member of the clinical team) according to the required scores in the inclusion criteria. After enrolment, participants also completed the PSQI (if enrolled by DASS-42 scoring criteria), DASS-42 (if enrolled by PSQI criteria), Warwick–Edinburgh Mental Wellbeing Scale (WEMWBS), Positive and Negative Affect Schedule (PANAS), and WHO-QoL (quality of life)-BREF questionnaires to provide the status of their emotional distress in the form of mental wellbeing, emotional feelings, and quality of life.
The DASS-42 is a 42-item self-report instrument widely used in the clinical diagnosis and outcome monitoring of three related negative emotional states of depression (D), anxiety (A), and stress (S)/tension (Lovibond and Peter F. L., 1995; Wagar and Amir, 2020). The DASS-42 tool assesses the degree of depression, anxiety, and stress in the form of a total score for each of these conditions, with a higher score denoting a more severe emotional state (Table 1 and Supplementary Figure S1).
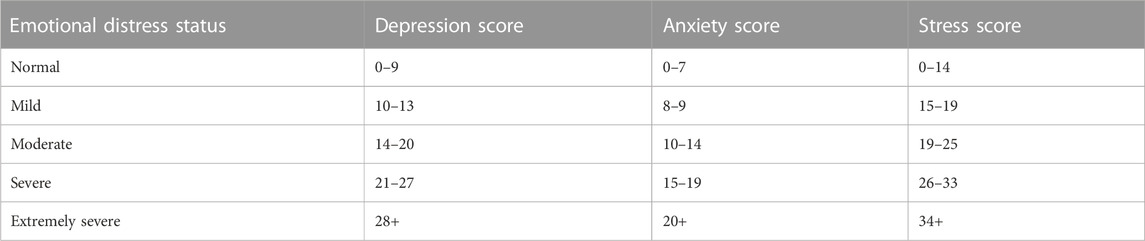
TABLE 1. Interpreting the DASS score (Lovibond and Peter F. L., 1995).
The self-report PSQI (Buysse et al., 1989; Hashmi et al., 2014) scale is an effective tool used in the clinical evaluation of sleep disturbances. It measures the quality and patterns of sleep across seven domains: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, and use of sleep medication. The component scores are summed to produce a global score (range 0–21). Higher scores indicate worse sleep quality. A score of >5 is considered as significant sleep disturbance (Supplementary Figure S2).
The WEMWBS is a 14-item scale of positively worded statements covering feelings and functioning aspects of mental wellbeing (Tennant et al., 2007; Waqas et al., 2015). The score of WEMWBS is calculated by summing the scores of 14 individual items. The total score ranges from 14 to 70, with higher scores indicating greater positive mental wellbeing (Supplementary Figure S3).
The PANAS (short version) is a widely used tool that measures the affective state using 10 different words that describe feelings and emotions (Watson et al., 1988; Kercher, 1992; Akhter, 2017). The affective state is measured on two scales: one scale measures the positive affective state, and the other measures the negative affective state. Positive affectivity refers to positive emotions and expressions such as joy, cheerfulness, or even contentment, while negative affectivity refers to negative emotions and expressions such as anger, fear, or sadness. The score of each affective state is calculated by summing the scores of individual five items, and ranges from 5 to 25, with a higher positive affectivity score indicating being proactive and enthusiastic, while a higher negative affectivity score shows being disengaged (emotionally detached) (Supplementary Figure S4).
The self-report WHO-QoL-BREF is a 26-item scale designed to measure the impact of disease and impairment on daily activities and behaviour, perceived health, disability, and functional capacity (WHO, 2004; Saqib Lodhi et al., 2017). The scale measures the impact on overall quality of life and general health across four domains: physical health, psychological health, social relationships, and environment. Each domain score is calculated by summing up the component item scores, ranging from 2 to 10 for overall QoL and general health, from 7 to 35 for physical health, from 6 to 30 for psychological health, from 3 to 15 for social relationships, and from 8 to 40 for environment, where higher scores represent a better quality of life.
The participants made two visits in total to the clinic: a screening/baseline visit (V1) and a 3-week follow-up (end of study) visit (V2). An improvement in the DASS-42 questionnaire comprising depression, anxiety, and stress scores or the PSQI questionnaire comprising sleep quality scores was the primary endpoint of this study, while an improvement in the WEMWBS, PANAS, and WHO-QoL-BREF scores was the secondary endpoint of this study.
2.4 Statistical analysis
Data were analysed using the Statistical Package for Social Sciences (SPSS; v28.0.1.1), applying standard statistical thresholds (p <0.05), which were tested for normality using the Kolmogorov–Smirnov test. Pearson’s correlations were used to assess the associations between the primary outcomes of interest. Independent samples t-test, Mann–Whitney U-test, or chi-squared tests were performed to detect the differences between demographic and anthropometric data at baseline. The scores on each questionnaire were entered into separate 2 × 2 repeated measures of ANOVA’s, with the group (supplementation and placebo) as the between-subject factor and time (baseline and follow-up) as the within-subject factor. When assumptions of sphericity were violated, Greenhouse–Geisser corrections were applied.
3 Results
3.1 Participants’ baseline characteristics and treatment allocation
Figure 1 shows the flow diagram of the Consolidated Standards of Reporting Trials (CONSORT). In total, 150 participants were initially screened to participate in the study, of which 104 subjects fulfilled the study inclusion/exclusion criteria and were randomly assigned to receive either the MO extract supplement or the placebo using the random number sequence function in Excel at a 1:1 allocation ratio. Randomisation was performed by an independent member of the clinical team who had no role in the study. Out of those randomised participants, 100 participants (supplement group n = 52 and placebo group n = 48) completed the study and were included in the final analysis. At baseline, participants’ levels of emotional distress and sleep disorder were significantly correlated with each other, i.e., depression–anxiety: r (100) = 0.650, p <0.001; depression–stress: r (100) = 0.758, p <0.001; anxiety–stress: r (100) = 0.639, p <0.001; PSQI–depression: r (100) = 0.202, p = 0.044; PSQI–anxiety: r (100) = 0.316, p = 0.001; and PSQI–stress: r (100) = 0.175, p = 0.081. The demographic characteristics of the participants at baseline are shown in Table 2. Participants’ mean age was 31 ± 9.18 years (ranging 18–60 years), and they were mostly women, (study population were mostly women, i.e., 64.0%). At baseline, both groups were reasonably balanced and did not differ significantly in age, body mass index, marital status, or residence, except for sex, with more men in the supplement group vs. the placebo group (24 vs. 12, p = 0.028).
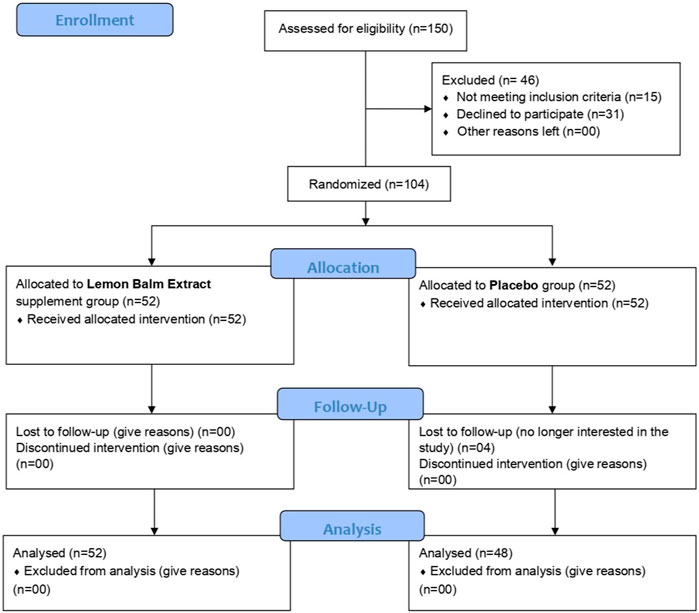
FIGURE 1. Study CONSORT flow diagram.
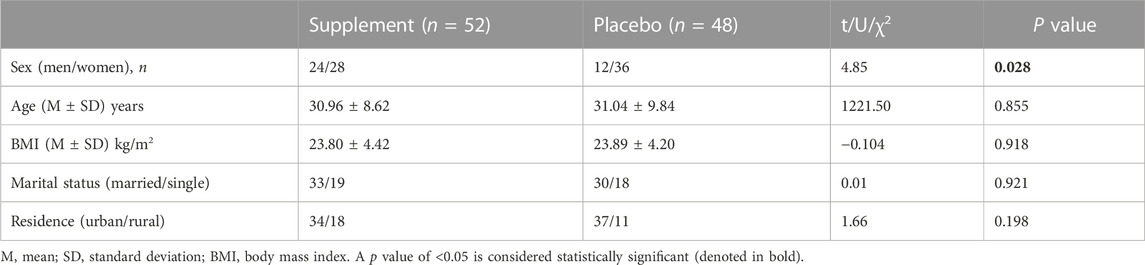
TABLE 2. Demographic characteristics of the study subjects.
3.2 Supplementation effects on mental health and wellbeing and affective state
The results are shown in Table 3 and Figure 2. At baseline, no significant differences were observed between the supplement and placebo groups on the DASS-42 Depression (Figure 2A), Anxiety (Figure 2B), and Stress (Figure 2C) scores. At 3-week follow-up, significant group × time interactions were observed in the DASS-42 Depression [F(1, 98) = 57.809, p <0.001, η2 = 0.371], Anxiety [F(1, 98) = 58.157, p <0.001, η2 = 0.372], and Stress [F(1, 98) = 52.868, p <0.001, η2 = 0.350] scores, such that the supplement group showed significant improvements (decrease in the score) in the measures of emotional distress between baseline and follow-up compared to the placebo group. Additionally, there was a statistically significant difference between the two groups (supplement vs. placebo) in the follow-up score in all the measures of emotional distress (all p values <0.001). The main effects of time and group are presented in the Supplementary Table S1.
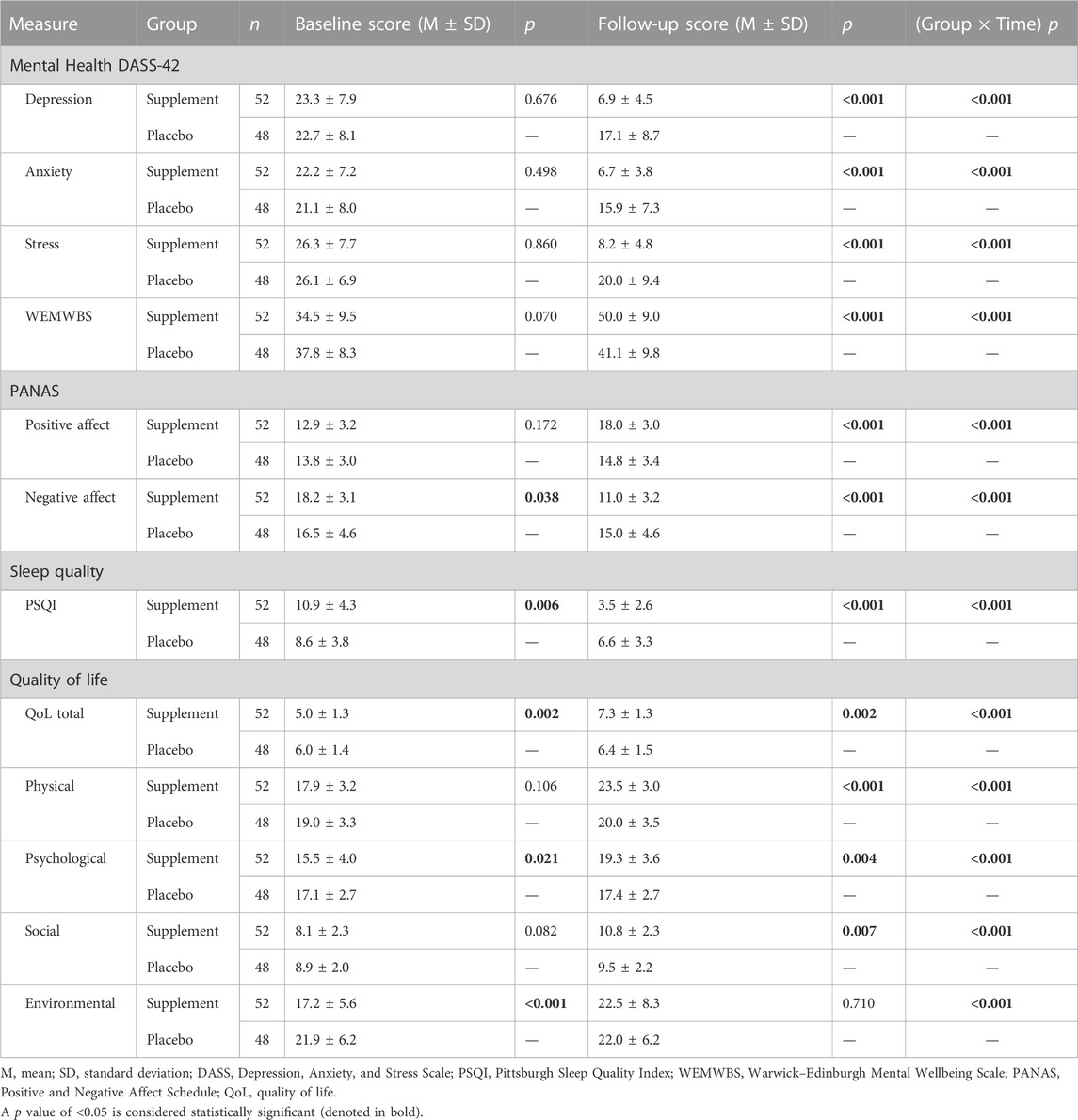
TABLE 3. DASS-42, WEMWBS, PANAS, PSQI, and WHO-QoL-BREF questionnaire scores at baseline and follow-up and differences between groups at baseline, follow-up, and group × time interactions.
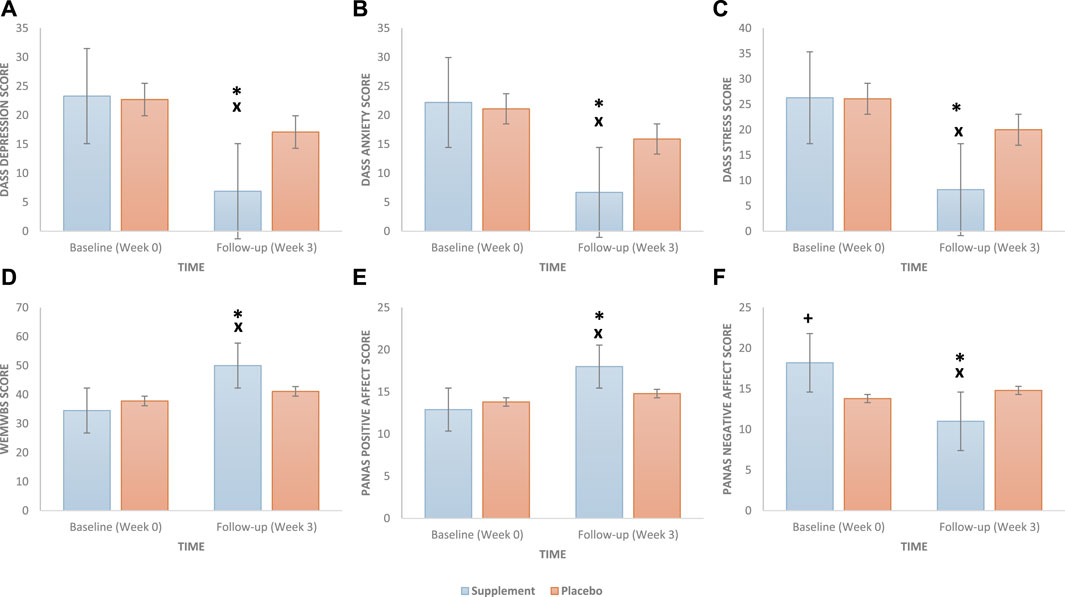
FIGURE 2. Effect of a daily oral 400 mg phospholipid carrier-based Melissa officinalis L. aqueous extract supplementation vs. placebo on study participants’ emotional distress condition scores: (A) depression, (B) anxiety, (C) stress, (D) mental wellbeing, (E) positive affect, and (F) negative affect (bars represent the standard error). DASS, Depression, Anxiety, and Stress Scale; WEMWBS, Warwick–Edinburgh Mental Wellbeing Scale; PANAS, Positive and Negative Affect Schedule. A p value of <0.05 is considered statistically significant. +, significant group differences at baseline; x, significant group differences at follow-up; *, significant group × time interaction.
At baseline, there were no significant differences between the supplement and placebo groups on the WEMWBS (Figure 2D) and PANAS positive affect (Figure 2E) scores; however, the supplemented group (vs. placebo) reported higher PANAS negative affect (Figure 2F) scores (p = 0.038). At the 3-week follow-up, significant group × time interactions were observed for the WEMWBS score [F(1, 98) = 53.617, p <0.001, η2 = 0.354] and PANAS positive [F(1, 98) = 35.605, p <0.001, η2 = 0.266] and negative [F(1, 98) = 71.322, p <0.001, η2 = 0.421] affect scores, such that the supplement group showed significant improvements in the measures of mental wellbeing (increase in the score) and affective state (increase in the score of positive affect and decrease in the score of negative affect) between baseline and follow-up compared to the placebo group. Additionally, there was a statistically significant difference between the two groups (supplement vs. placebo) at the follow-up WEMWBS and PANAS positive and negative affect scores (all p values <0.001). The main effects of time and group are presented in the Supplementary Table S1.
3.3 Supplementation effects on sleep quality and quality of life
The results are shown in Table 3 and Figure 3. There was a significant difference in the baseline PSQI score (p = 0.006) between the two groups, with the supplement group reporting higher PSQI scores (i.e., poor sleep) compared to the placebo group (Figure 3A). At the 3-week follow-up, a significant group × time interaction was found [F(1, 98) = 47.402, p <0.001, η2 = 0.326], such that the supplement group showed significant improvements (decrease in the score) in sleep quality between baseline and follow-up compared to the placebo group. Additionally, there was a statistically significant difference between the two groups’ (supplement vs. placebo) sleep quality scores at the follow-up (p <0.001). The main effects of time and group are presented in the Supplementary Table S1.
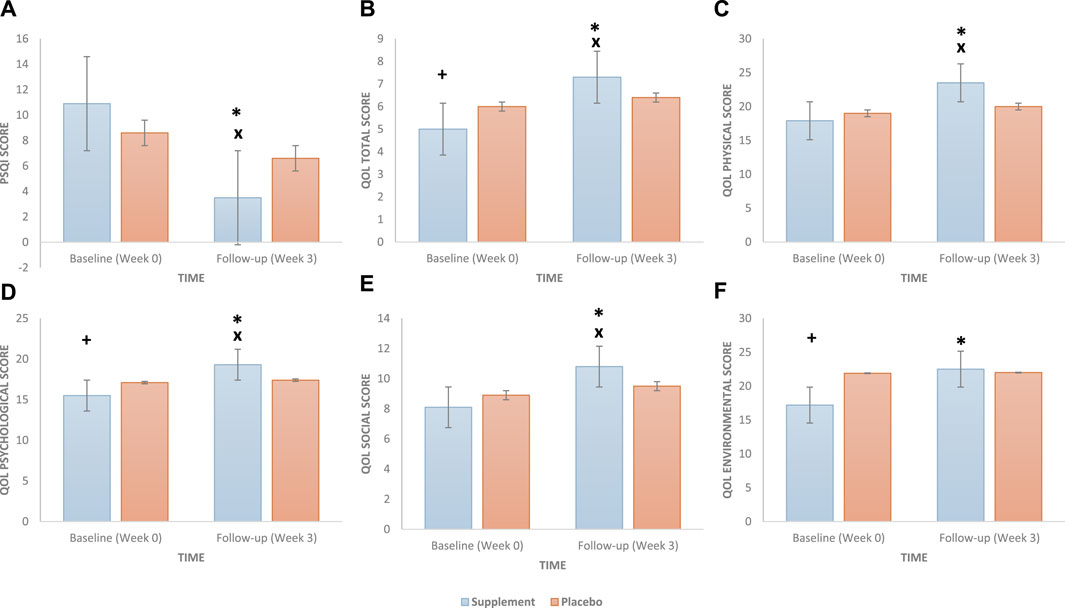
FIGURE 3. Effect of a daily oral 400 mg phospholipid carrier-based Melissa officinalis L. aqueous extract supplementation vs. placebo on study participants: (A) sleep quality (PSQI), (B) quality-of-life total, (C) quality-of-life physical, (D) quality-of-life psychological, (E) quality-of-life social, and (F) quality-of-life environmental scores (bars represent the standard error). PSQI, Pittsburgh Sleep Quality Index. A p value of <0.05 is considered statistically significant. +, significant group differences at baseline; x, significant group differences at follow-up; *, significant group × time interaction.
Moreover, there were no significant differences between the supplement and placebo groups at baseline for the physical (Figure 3C) and social (Figure 3E) QoL subscales; however, the supplement group (vs. placebo) reported worse total (p = 0.002) (Figure 3B), psychological (p = 0.021) (Figure 3D), and environmental (p <0.001) (Figure 3F) QoL scores. At the 3-week follow-up, significant group × time interactions were observed for total QoL [F(1, 98) = 42.391, p <0.001, η2 = 0.302], physical [F(1, 98) = 59.673, p <0.001, η2 = 0.378], psychological [F(1, 98) = 36.524, p <0.001, η2 = 0.272], social [F(1, 98) = 35.055, p <0.001, η2 = 0.263], and environmental [F(1, 98) = 42.204, p <0.001, η2 = 0.301] subscales, such that the supplement group showed significant improvements (increase in score) in all quality-of-life measures between baseline and follow-up compared to the placebo group. Additionally, at follow-up, there was a statistically significant difference between the two groups (supplement vs. placebo) in all QoL measures (all p values <0.001) except for the environmental subscale (p = 0.710). The main effects of time and group are presented in the Supplementary Table S1.
3.4 Compliance, safety, and tolerability of the supplement
Participants’ compliance with the supplement/placebo intake was checked through a weekly phone call. At the completion of the 3-week study period, none of the participants returned any leftover supplement/placebo. Hence, verbal affirmation was taken as a measure of compliance, and most of the participants (>95%) reported adherence to the study protocol. Except a few cases of mild stomach upset, which were equally distributed among the groups (four in the supplement group and five in the placebo group), no specific treatment-emergent effects or serious adverse events were reported by any of the study participants.
4 Discussion
In the present study, we investigated the impact of a 3-week-long supplementation of an innovative phospholipid carrier-based formulation of a standardised MO extract (daily 400 mg dosage) on emotional distress and related conditions. Findings revealed that the consumption of MO extract improved depression, anxiety, and stress scores and sleep quality in individuals with a moderate degree of depression, stress, anxiety, or sleep complaints. Additionally, we found that the extract improved overall mental wellbeing, affective state, and quality of life.
One of the notable outcomes of this study is the significant reduction in depression, anxiety, and stress levels in participants who received MO phospholipid extract supplementation. It is noteworthy that these improvements were observed only after 3 weeks of supplementation, suggesting a relatively rapid onset of therapeutic effects of the extract. These findings are broadly in line with the previous research showing the contemporary role of MO extract as a “calming agent” and a mild sedative following acute and chronic supplementation (Kennedy et al., 2002; Kennedy et al., 2003; Kennedy et al., 2004; Cases et al., 2011; Alijaniha et al., 2015; Soltanpour et al., 2019). It is important to note that, unlike our study utilising well-known and clinically validated scales to measure depression, stress, and anxiety in healthy individuals, previous research has measured calmness/anxiety by utilising visual analogue scales in unhealthy individuals (e.g., individuals undergoing coronary artery bypass surgery); hence, our results, in fact, extend the previous findings and show a potential therapeutic impact of the MO extract on subclinical conditions (such as elevated depression, anxiety, and stress levels) in healthy individuals.
Additionally, participants who consumed MO extract experienced a significant increase in overall mental wellbeing and positive affective state and a significant decrease in negative affective state, as evidenced by improvements in the WEMWBS and PANAS scores, respectively. This outcome suggests that in addition to its calming effect, MO phospholipid extract also fosters positive psychological wellbeing and affective state, as well as mitigates negative emotional states. Given that the supplement and placebo groups differed in baseline negative affect scores, the effect of MO supplementation on alleviating negative emotional feelings should be interpreted with caution. Nevertheless, this improvement in emotional states aligns with the observed reductions in the symptoms of depression, anxiety, and stress and underscores the comprehensive impact of MO supplementation on mental health.
In the realm of sleep quality, consistent with the previous research, participants who consumed the MO phospholipid extract demonstrated a significant improvement in the total PSQI score (Cases et al., 2011; Haybar et al., 2018; Heydari et al., 2018; Soltanpour et al., 2019), highlighting its potential as a holistic approach to sleep management. Given that the MO extract positively affected mental health and wellbeing, it could also indirectly affect the quality of sleep by reducing mental health symptomatology. However, similar to negative affect, participants in the supplement and placebo groups differed in sleep quality at the baseline, hence, the results should be interpreted with caution.
Another important aspect of this study is that the MO supplement elicited a positive impact on various domains of QoL, e.g., physical and social aspects. Although there were differences between the supplement and placebo groups in terms of baseline scores of the total QoL, psychological, and environmental subscales, which may have driven the observed effects, the treatment group exhibited improvements in all quality-of-life measures at 3 weeks follow-up. These improvements suggest that MO supplementation has the potential to enhance overall life satisfaction and functioning and further add to the evidence base.
It is important to highlight that none of the participants who received the supplement (daily dosage 400 mg) reported any serious side effects, such as those associated with conventional antidepressants and anxiolytic drugs, at least during the 3-week study period, demonstrating the excellent safety and tolerability of the phospholipid carrier-based formulation of MO extract supplementation. These results are consistent with the previously reported studies with other MO formulations (Ballard et al., 2002; Akhondzadeh et al., 2003; Burns et al., 2011; Cases et al., 2011; Alijaniha et al., 2015; Noguchi-Shinohara et al., 2015; Soltanpour et al., 2019; Araj-Khodaei et al., 2020). In general, MO extract supplementation is considered a safe alternative therapy for the management of emotional distress and related conditions. Noguchi-Shinohara et al. (2020) analysed that in patients with mild dementia due to Alzheimer’s disease (AD), a daily dose of 500 mg of MO extract supplementation for 24 weeks failed to produce any adverse events. Asadi et al. (2019) observed that in patients with type 2 diabetes, a daily dose of 700 mg of MO extract supplementation for 3 months was safe and tolerable. However, it has been repeatedly pointed out that MO should be used with caution in patients with thyroid dysfunction as it mediates thyroid hormone inhibition (Ulbricht et al., 2005). Overall, no common serious side effects have so far been reported for MO extract supplementation (Rafieian-Kopaei et al., 2013) in otherwise healthy adults or when used in nutritional amounts. As a matter of fact, in 2013, the European Medicines Agency approved MO leaf extract prepared as a herbal infusion, dry extract, or fluid extract as a non-prescription medicine for alleviating mild symptoms of mental stress and fostering sleep, and for relieving mild digestive disorders, which included bloating and flatulence (HMPC Community herbal monograph on Melissa officinalis L. folium, 2007). The European Scientific Cooperative on Phytotherapy (ESCOP) also recommends the use of the MO extract for tenseness, restlessness, and irritability (Escop European Scientific Cooperative on Phytotherapy, 2003). In the US, the MO extract has received FDA GRAS (Generally Recognised as Safe) status for use as a food ingredient (US Food and Drug Administration, 2016).
Due to the demonstrated neuropharmacological therapeutic effects of the oral MO extract, as observed in the present study, it is currently one of the most popular over-the-counter supplements for the management of low mood conditions, particularly in individuals who are refractory to conventional antidepressant/anxiolytic drugs. Among the reported clinical trials, the MO extract supplement dosage of 300 to 1,600 mg has shown benefits in the management of depression, anxiety, stress, and poor sleep. In terms of duration, studies have shown that a period between 10 days and 8 weeks is required to improve depressive symptoms. Some clinical trials have shown that the shortest duration of MO oral supplementation that led to improvement in anxiety disorders was 5–7 days (Soltanpour et al., 2019; Saeidi et al., 2020). In the presence of available evidence on scientific rationale, clinical efficacy, and safety, we propose that phospholipid carrier-based MO extract supplementation may serve as a promising short-term natural intervention for individuals seeking relief from symptoms of depression, anxiety, and stress while simultaneously enhancing their overall mental wellbeing.
With regards to possible mechanisms of action, the beneficial effects of MO supplementation on low mood and/or anxiety are believed to be largely driven by the natural GABAergic properties of the supplement. γ-Amino butyric acid is the principal inhibitory neurotransmitter in the central nervous system (Brambilla et al., 2003; Granger et al., 2005) that has been implicated in a range of behaviours, including, but not limited to, low mood, anxiety, stress regulation, memory enhancement, and circadian rhythm (Hepsomali et al., 2020). Brain cells low GABA levels and/or impaired GABA functioning are known to be associated with the aetiology and maintenance of acute and chronic stress (Jie et al., 2018), anxiety, depressive disorders (Nemeroff, 2003), and insomnia (Gottesmann, 2002). Melissa officinalis L. inhibits GABA-T (Awad et al., 2007; Awad et al., 2009; Yoo et al., 2011), resulting in an increase in brain GABA levels and a subsequent increase in GABA transmission. Amongst the bioactive chemical constituents of the MO extract, rosmarinic acid (a hydroxycinnamic acid ester polyphenol) is the major ingredient and an important biomarker used for the standardisation of MO extract (Arceusz et al., 2015; Noguchi-Shinohara et al., 2015; Shakeri et al., 2016). Rosmarinic acid has the ability to cross the blood–brain barrier (Falé et al., 2011). Therefore, the psychopharmacological effects of the MO extract are predominantly attributed to RA (Awad et al., 2007; Awad et al., 2009; Jin et al., 2013; Sahin et al., 2016; Ghazizadeh et al., 2020), possibly acting in a synergistic or additive way with other biochemical mechanisms (Savelev et al., 2003), such as GABA-T inhibition by ursolic and oleanolic acid contents present in the MO extract (Awad et al., 2009; Ibarra et al., 2010). The Melissa officinalis L. extract has also shown an affinity for GABAA receptors (Salah and Jäger, 2005; Abuhamdah et al., 2008; Sahin et al., 2016), leading to an enhancement in GABAergic signalling. GABA receptors are targets for many pharmacological treatments for insomnia, such as benzodiazepines. GABAA receptor modulation is one of the four key mechanisms of action of the approved pharmacological therapies for insomnia (Avidan and Neubauer, 2017).
The phospholipid carrier-based (Phytosome™) MO extract (Relissa™) used in the present study is an innovative food-grade formulation developed to achieve increased bioavailability and therapeutic effects of the extract. The Phytosome™ carrier is a solid botanical dispersion recently reported to improve the effectiveness and target reach of a wide range of natural compounds, such as quercetin (Riva et al., 2019b), berberine (Rondanelli et al., 2021), curcumin (Pivari et al., 2022), boswellic acids (Riva et al., 2019a), and other botanical extracts, without safety concerns. We can hypothesise that the possible “calming effect” observed in the present study after 3-week supplementation of the phospholipid carrier-based MO extract could also be due to this new formulation used; however, more studies are needed to better clarify the role of the Phytosome™ carrier.
However, it is essential to acknowledge some limitations of this study, such as evaluation of only one dose of MO extract, lack of compliance measurements, and the absence of evaluation of therapeutic effect in the form of objective biomarkers such as cortisol, C-reactive protein (CRP), adrenocorticotropic hormone (ACTH), dehydroepiandrosterone (DHEA), and corticosterone levels etc, which should be considered in future studies. In the current study, although the men/women ratio was somewhat balanced in the supplement group, there were more female participants in the placebo group. Given that the NIH Policy (Arnegard et al., 2020) recommends considering sex as a biological variable, future studies should consider this crucial factor in the recruitment and analysis stages. Although this study primarily focused on short-term effects (3 weeks of supplementation) on mental health and related conditions, it is essential to acknowledge the potential for sustained benefits over extended periods. Future research should explore the long-term impact of MO phospholipid extract supplementation on mental health, wellbeing, and sleep quality to ascertain its utility as a continuous intervention. While this study has demonstrated the positive effects of MO supplementation, the underlying mechanisms remain a subject for further investigation. Understanding how MO’s bioactive compounds interact with neuronal pathways and physiological processes could shed light on its therapeutic actions and guide the development of more targeted interventions. Additionally, research studies should explore optimal dosage regimens and potential interactions with other interventions or medications. The results observed in the present study underscore the potential breadth and depth of MO phospholipid extract supplementation’s effects on mental health and related conditions. They hint at the possibility of enduring benefits, gender-specific responses, and opportunities for elucidating the mechanisms that drive these improvements. As such, they emphasise the need for future research to explore these facets in greater detail and promote a more comprehensive understanding of MO’s extract therapeutic potential.
5 Conclusion
In conclusion, this rigorous, randomised, prospective, multi-centre, double-blinded, placebo-controlled clinical study has provided compelling evidence of the beneficial effects of MO phospholipid extract supplementation on mental health, wellbeing, and sleep quality. The findings of this study have several important implications and open avenues for future research and clinical applications.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
Ethics statement
The study was approved by the Institutional Ethics Review Committee of Ayub Teaching Hospital, Abbottabad (Ref. No. RC-/EA-01/194); Lady Reading Hospital, Peshawar (Ref. No. 684/LRH/MTI/); and Bolan Medical Complex Hospital, Quetta, Pakistan (Ref. no. 5501). The studies were conducted in accordance with local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
Conceptualisation and methodology: AKh and PH; investigation and data curation: AB, AKa, AS, AB, FR, UF, AK, ZK, MB, and SM; resources: AKh; supervision and project administration: AKh, UF, AK, AA, and FR; formal analysis: PH; writing—original draft preparation: AKh and PH; writing—review and editing: SK, IU, UF, SH, and MK. All authors contributed to the article and approved the submitted version.
Acknowledgments
We would like to thank the participants of this study. We are also grateful to Prof. Martino Recchia and Paola Misiano for their valuable editorial support and Mauro A. M. Carai for statistical analysis. We also thank Indena S.p.A, Milan, Italy, for providing the standardized Melissa officinalis L. phospholipids formulated extract (Relissa™) and placebo tablets for the clinical trial.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1250560/full#supplementary-material
References
Abuhamdah, S., Huang, L., Elliott, M. S., Howes, M. J., Ballard, C., Holmes, C., et al. (2008). Pharmacological profile of an essential oil derived from Melissa officinalis with anti-agitation properties: focus on ligand-gated channels. J. Pharm. Pharmacol. 60 (3), 377–384. doi:10.1211/jpp.60.3.0014
Akhondzadeh, S., Noroozian, M., Mohammadi, M., Ohadinia, S., Jamshidi, A. H., and Khani, M. (2003). Melissa officinalis extract in the treatment of patients with mild to moderate alzheimer's disease: A double blind, randomised, placebo controlled trial. J. Neurol. Neurosurg. Psychiatry 74 (7), 863–866. doi:10.1136/jnnp.74.7.863
Akhter, N. (2017). Urdu translation and validation of shorter version of Positive Affect and Negative Affect Schedule (PANAS) on Pakistani bank employees. J. Pak Med. Assoc. 67 (10), 1517–1523.
Alijaniha, F., Naseri, M., Afsharypuor, S., Fallahi, F., Noorbala, A., Mosaddegh, M., et al. (2015). Heart palpitation relief with Melissa officinalis leaf extract: double blind, randomized, placebo controlled trial of efficacy and safety. J. Ethnopharmacol. 164, 378–384. doi:10.1016/j.jep.2015.02.007
Araj-Khodaei, M., Noorbala, A. A., Yarani, R., Emadi, F., Emaratkar, E., Faghihzadeh, S., et al. (2020). A double-blind, randomized pilot study for comparison of Melissa officinalis L. and Lavandula angustifolia Mill. with Fluoxetine for the treatment of depression. BMC Complement. Med. Ther. 20 (1), 207. doi:10.1186/s12906-020-03003-5
Arceusz, A., Wesolowski, M., and Ulewicz-Magulska, B. (2015). Flavonoids and phenolic acids in methanolic extracts, infusions and tinctures from commercial samples of lemon balm. Nat. Prod. Commun. 10 (6), 1934578X1501000–981. doi:10.1177/1934578x1501000645
Arnegard, M. E., Whitten, L. A., Hunter, C., and Clayton, J. A. (2020). Sex as a biological variable: A 5-year progress report and call to action. J. Womens Health (Larchmt) 29 (6), 858–864. doi:10.1089/jwh.2019.8247
Arroll, B., Chin, W.-y., Martis, W., Goodyear-Smith, F., Mount, V., Kingsford, D., et al. (2016). Antidepressants for treatment of depression in primary care: A systematic review and meta-analysis. J. Prim. health care 8 (4), 325–334. doi:10.1071/HC16008
Asadi, A., Shidfar, F., Safari, M., Hosseini, A. F., Fallah Huseini, H., Heidari, I., et al. (2019). Efficacy of Melissa officinalis L. (lemon balm) extract on glycemic control and cardiovascular risk factors in individuals with type 2 diabetes: A randomized, double-blind, clinical trial. Phytotherapy Res. 33 (3), 651–659. doi:10.1002/ptr.6254
Avidan, A. Y., and Neubauer, D. N. (2017). Chronic insomnia disorder. Contin. (Minneap Minn) 23 (4), 1064–1092. doi:10.1212/01.CON.0000522244.13784.bf
Awad, R., Levac, D., Cybulska, P., Merali, Z., Trudeau, V., and Arnason, J. (2007). Effects of traditionally used anxiolytic botanicals on enzymes of the γ-aminobutyric acid (GABA) system. Can. J. physiology Pharmacol. 85 (9), 933–942. doi:10.1139/Y07-083
Awad, R., Muhammad, A., Durst, T., Trudeau, V. L., and Arnason, J. T. (2009). Bioassay-guided fractionation of lemon balm (Melissa officinalis L.) using an in vitro measure of GABA transaminase activity. Phytotherapy Res. Int. J. Devoted Pharmacol. Toxicol. Eval. Nat. Prod. Deriv. 23 (8), 1075–1081. doi:10.1002/ptr.2712
Ballard, C. G., O'Brien, J. T., Reichelt, K., and Perry, E. K. (2002). Aromatherapy as a safe and effective treatment for the management of agitation in severe dementia: the results of a double-blind, placebo-controlled trial with Melissa. J. Clin. Psychiatry 63 (7), 553–558. doi:10.4088/jcp.v63n0703
Bandelow, B., Michaelis, S., and Wedekind, D. (2022). Treatment of anxiety disorders. Dialogues Clin. Neurosci. 19, 93–107. doi:10.31887/DCNS.2017.19.2/bbandelow
Brambilla, P., Perez, J., Barale, F., Schettini, G., and Soares, J. C. (2003). GABAergic dysfunction in mood disorders. Mol. Psychiatry 8 (8), 721–737. doi:10.1038/sj.mp.4001362
Burns, A., Perry, E., Holmes, C., Francis, P., Morris, J., Howes, M. J., et al. (2011). A double-blind placebo-controlled randomized trial of Melissa officinalis oil and donepezil for the treatment of agitation in Alzheimer's disease. Dement. Geriatr. Cogn. Disord. 31 (2), 158–164. doi:10.1159/000324438
Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S. R., and Kupfer, D. J. (1989). The Pittsburgh Sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 28 (2), 193–213. doi:10.1016/0165-1781(89)90047-4
Cases, J., Ibarra, A., Feuillère, N., Roller, M., and Sukkar, S. G. (2011). Pilot trial of Melissa officinalis L. leaf extract in the treatment of volunteers suffering from mild-to-moderate anxiety disorders and sleep disturbances. Med. J. Nutr. Metab. 4 (3), 211–218. doi:10.1007/s12349-010-0045-4
Coleta, M., Campos, M. G., Cotrim, M. D., and Proença da Cunha, A. (2001). Comparative evaluation of Melissa officinalis L., Tilia europaea L., Passiflora edulis Sims. and Hypericum perforatum L. in the elevated plus maze anxiety test. Pharmacopsychiatry 34 (1), S20–S21. doi:10.1055/s-2001-15460
Dastmalchi, K., Ollilainen, V., Lackman, P., Gennäs, G. B. A., Dorman, H. J. D., Järvinen, P. P., et al. (2009). Acetylcholinesterase inhibitory guided fractionation of Melissa officinalis L. Bioorg. Med. Chem. 17 (2), 867–871. doi:10.1016/j.bmc.2008.11.034
de Niet, G. J., Tiemens, B. G., Kloos, M. W., and Hutschemaekers, G. J. (2009). Review of systematic reviews about the efficacy of non-pharmacological interventions to improve sleep quality in insomnia. JBI Evid. Implement. 7 (4), 233–242. doi:10.1111/j.1744-1609.2009.00142.x
Demyttenaere, K. (2001). Compliance and acceptance in antidepressant treatment. Int. J. Psychiatry Clin. Pract. 5 (1), 29–35. doi:10.1080/13651500152048423
Dimpfel, W., and Suter, A. (2008). Sleep improving effects of a single dose administration of a valerian/hops fluid extract. A double blind, randomized, placebo-controlled sleep-EEG study in a parallel design using the electrohypnogram. Z. für Phytother. 29 (S 1), P06.
Escop European Scientific Cooperative on Phytotherapy (2003). ESCOP monographs: The scientific foundation for herbal medicinal products. United Kingdom: ESCOP.
European Medicines Agency (2023). Available at: .https://www.ema.europa.eu/en/medicines/field_ema_web_categories%253Aname_field/Herbal/field_ema_herb_outcome/european-union-herbal-monograph-254 (Accessed August 21, 2023).
Falé, P. L. V., Madeira, P. J. A., Florêncio, M. H., Ascensão, L., and Serralheiro, M. L. M. (2011). Function of Plectranthus barbatus herbal tea as neuronal acetylcholinesterase inhibitor. Food and Funct. 2 (2), 130–136. doi:10.1039/C0FO00070A
Feliú-Hemmelmann, K., Monsalve, F., and Rivera, C. (2013). Melissa officinalis and Passiflora caerulea infusion as physiological stress decreaser. Int. J. Clin. Exp. Med. 6 (6), 444–451.
Ferreira, A., Proença, C., Serralheiro, M., and Araujo, M. (2006). The in vitro screening for acetylcholinesterase inhibition and antioxidant activity of medicinal plants from Portugal. J. Ethnopharmacol. 108 (1), 31–37. doi:10.1016/j.jep.2006.04.010
Ghazizadeh, J., Hamedeyazdan, S., Torbati, M., Farajdokht, F., Fakhari, A., Mahmoudi, J., et al. (2020). Melissa officinalis L. hydro-alcoholic extract inhibits anxiety and depression through prevention of central oxidative stress and apoptosis. Exp. Physiol. 105 (4), 707–720. doi:10.1113/ep088254
Gottesmann, C. (2002). GABA mechanisms and sleep. Neuroscience 111 (2), 231–239. doi:10.1016/s0306-4522(02)00034-9
Granger, R. E., Campbell, E. L., and Johnston, G. A. R. (2005). (+)- and (-)-borneol: efficacious positive modulators of GABA action at human recombinant alpha1beta2gamma2L GABA(A) receptors. Biochem. Pharmacol. 69 (7), 1101–1111. doi:10.1016/j.bcp.2005.01.002
Guginski, G., Luiz, A. P., Silva, M. D., Massaro, M., Martins, D. F., Chaves, J., et al. (2009). Mechanisms involved in the antinociception caused by ethanolic extract obtained from the leaves of Melissa officinalis (lemon balm) in mice. Pharmacol. Biochem. Behav. 93 (1), 10–16. doi:10.1016/j.pbb.2009.03.014
Hepsomali, P., Groeger, J. A., Nishihira, J., and Scholey, A. (2020). Effects of oral gamma-aminobutyric acid (GABA) administration on stress and sleep in humans: A systematic review. Front. Neurosci. 14, 923. doi:10.3389/fnins.2020.00923
Hafner, M., Stepanek, M., Taylor, J., Troxel, W. M., and van Stolk, C. (2017). Why sleep matters-the economic costs of insufficient sleep: A cross-country comparative analysis. Rand Health Q. 6 (4), 11.
Hashmi, A. M., Khawaja, I. S., Butt, Z., Umair, M., Naqvi, S. H., and Jawad Ul, H. (2014). The Pittsburgh Sleep quality index: validation of the Urdu translation. J. Coll. Physicians Surg. Pak 24 (2), 123–126.
Haybar, H., Javid, A. Z., Haghighizadeh, M. H., Valizadeh, E., Mohaghegh, S. M., and Mohammadzadeh, A. (2018). The effects of Melissa officinalis supplementation on depression, anxiety, stress, and sleep disorder in patients with chronic stable angina. Clin. Nutr. ESPEN 26, 47–52. doi:10.1016/j.clnesp.2018.04.015
Head, K. A., and Kelly, G. S. (2009). Nutrients and botanicals for treatment of stress: adrenal fatigue, neurotransmitter imbalance, anxiety, and restless sleep. Altern. Med. Rev. 14 (2), 114–140.
Heydari, N., Dehghani, M., Emamghoreishi, M., and Akbarzadeh, M. (2018). Effect of Melissa officinalis capsule on the mental health of female adolescents with premenstrual syndrome: A clinical trial study. Int. J. Adolesc. Med. Health 31 (3). doi:10.1515/ijamh-2017-0015
Hillman, D., Mitchell, S., Streatfeild, J., Burns, C., Bruck, D., and Pezzullo, L. (2018). The economic cost of inadequate sleep. Sleep 41 (8). doi:10.1093/sleep/zsy083
HMPC Community herbal monograph on Melissa officinalis L. folium (2007). Final initial assessment discussion in working party on community monographs and community list (MLWP). Available at: http://www.teinture-mere.fr/files/boutique/produits/doc/186603-3-melissa-officinalis.pdf (Accessed May 10, 2023).
Ibarra, A., Feuillere, N., Roller, M., Lesburgere, E., and Beracochea, D. (2010). Effects of chronic administration of Melissa officinalis L. extract on anxiety-like reactivity and on circadian and exploratory activities in mice. Phytomedicine 17 (6), 397–403. doi:10.1016/j.phymed.2010.01.012
Jie, F., Yin, G., Yang, W., Yang, M., Gao, S., Lv, J., et al. (2018). Stress in regulation of GABA amygdala system and relevance to neuropsychiatric diseases. Front. Neurosci. 12, 562. doi:10.3389/fnins.2018.00562
Jin, X., Liu, P., Yang, F., Zhang, Y. H., and Miao, D. (2013). Rosmarinic acid ameliorates depressive-like behaviors in a rat model of CUS and Up-regulates BDNF levels in the hippocampus and hippocampal-derived astrocytes. Neurochem. Res. 38 (9), 1828–1837. doi:10.1007/s11064-013-1088-y
Kavan, M. G., Elsasser, G., and Barone, E. J. (2009). Generalized anxiety disorder: practical assessment and management. Am. Fam. Physician 79 (9), 785–791.
Kenda, M., Kočevar Glavač, N., Nagy, M., and Sollner Dolenc, M. (2022). Medicinal plants used for anxiety, depression, or stress treatment: an update. Molecules 27 (18), 6021. doi:10.3390/molecules27186021
Kennedy, D. O., Little, W., Haskell, C. F., and Scholey, A. B. (2006). Anxiolytic effects of a combination of Melissa officinalis and Valeriana officinalis during laboratory induced stress. Phytother. Res. 20 (2), 96–102. doi:10.1002/ptr.1787
Kennedy, D. O., Little, W., and Scholey, A. B. (2004). Attenuation of laboratory-induced stress in humans after acute administration of Melissa officinalis (Lemon Balm). Psychosom. Med. 66 (4), 607–613. doi:10.1097/01.psy.0000132877.72833.71
Kennedy, D. O., Scholey, A. B., Tildesley, N. T., Perry, E. K., and Wesnes, K. A. (2002). Modulation of mood and cognitive performance following acute administration of Melissa officinalis (lemon balm). Pharmacol. Biochem. Behav. 72 (4), 953–964. doi:10.1016/s0091-3057(02)00777-3
Kennedy, D. O., Wake, G., Savelev, S., Tildesley, N. T., Perry, E. K., Wesnes, K. A., et al. (2003). Modulation of mood and cognitive performance following acute administration of single doses of Melissa officinalis (Lemon balm) with human CNS nicotinic and muscarinic receptor-binding properties. Neuropsychopharmacology 28 (10), 1871–1881. doi:10.1038/sj.npp.1300230
Kercher, K. (1992). Assessing subjective well-being in the old-old: the PANAS as a measure of orthogonal dimensions of positive and negative affect. Res. Aging 14, 131–168. doi:10.1177/0164027592142001
Kupcova, I., Danisovic, L., Klein, M., and Harsanyi, S. (2023). Effects of the COVID-19 pandemic on mental health, anxiety, and depression. BMC Psychol. 11 (1), 108. doi:10.1186/s40359-023-01130-5
Lin, S. H., Chou, M. L., Chen, W. C., Lai, Y. S., Lu, K. H., Hao, C. W., et al. (2015). A medicinal herb, Melissa officinalis L. ameliorates depressive-like behavior of rats in the forced swimming test via regulating the serotonergic neurotransmitter. J. Ethnopharmacol. 175, 266–272. doi:10.1016/j.jep.2015.09.018
Liu, L., Liu, C., Wang, Y., Wang, P., Li, Y., and Li, B. (2015). Herbal medicine for anxiety, depression and insomnia. Curr. Neuropharmacol. 13 (4), 481–493. doi:10.2174/1570159x1304150831122734
López, V., Martín, S., Gómez-Serranillos, M. P., Carretero, M. E., Jäger, A. K., and Calvo, M. I. (2009). Neuroprotective and neurological properties of Melissa officinalis. Neurochem. Res. 34 (11), 1955–1961. doi:10.1007/s11064-009-9981-0
Lovibond, S. H., and Peter, F. L. (1995). Manual for the depression anxiety stress scales. Sydney, N.S.W: Psychology Foundation of Australia.
Miraj, S., Rafieian, K., and Kiani, S. (2017). Melissa officinalis L: A review study with an antioxidant prospective. J. Evid. Based Complement. Altern. Med. 22 (3), 385–394. doi:10.1177/2156587216663433
Morin, C. M., and Jarrin, D. C. (2022). Epidemiology of insomnia: prevalence, course, risk factors, and public health burden. Sleep. Med. Clin. 17 (2), 173–191. doi:10.1016/j.jsmc.2022.03.003
Nemeroff, C. B. (2003). The role of GABA in the pathophysiology and treatment of anxiety disorders. Psychopharmacol. Bull. 37 (4), 133–146.
Noguchi-Shinohara, M., Ono, K., Hamaguchi, T., Iwasa, K., Nagai, T., Kobayashi, S., et al. (2015). Pharmacokinetics, safety and tolerability of Melissa officinalis extract which contained rosmarinic acid in healthy individuals: A randomized controlled trial. PLOS ONE 10 (5), e0126422. doi:10.1371/journal.pone.0126422
Noguchi-Shinohara, M., Ono, K., Hamaguchi, T., Nagai, T., Kobayashi, S., Komatsu, J., et al. (2020). Safety and efficacy of Melissa officinalis extract containing rosmarinic acid in the prevention of Alzheimer’s disease progression. Sci. Rep. 10 (1), 18627. doi:10.1038/s41598-020-73729-2
Perry, N., Court, G., Bidet, N., Court, J., and Perry, E. (1996). European herbs with cholinergic activities: potential in dementia therapy. Int. J. geriatric psychiatry 11 (12), 1063–1069. doi:10.1002/(sici)1099-1166(199612)11:12<1063:aid-gps532>3.0.co;2-1
Pivari, F., Mingione, A., Piazzini, G., Ceccarani, C., Ottaviano, E., Brasacchio, C., et al. (2022). Curcumin supplementation (Meriva(®)) modulates inflammation, lipid peroxidation and gut microbiota composition in chronic kidney disease. Nutrients 14 (1), 231. doi:10.3390/nu14010231
Rafieian-Kopaei, M., Baradaran, A., and Rafieian, M. (2013). Plants antioxidants: from laboratory to clinic. J. Nephropathol. 2 (2), 152–153. doi:10.12860/jnp.2013.26
Ranjbar, M., Firoozabadi, A., Salehi, A., Ghorbanifar, Z., Zarshenas, M. M., Sadeghniiat-Haghighi, K., et al. (2018a). Effects of Herbal combination (Melissa officinalis L. and Nepeta menthoides Boiss. and Buhse) on insomnia severity, anxiety and depression in insomniacs: randomized placebo controlled trial. Integr. Med. Res. 7 (4), 328–332. doi:10.1016/j.imr.2018.08.001
Ranjbar, M., Salehi, A., Rezaeizadeh, H., Zarshenas, M. M., Sadeghniiat-Haghighi, K., Mirabzadeh, M., et al. (2018b). Efficacy of a combination of Melissa officinalis L. and nepeta menthoides boiss. and buhse on insomnia: A triple-blind, randomized placebo-controlled clinical trial. J. Altern. Complement. Med. 24, 1197–1203. doi:10.1089/acm.2017.0153
Riva, A., Giacomelli, L., Togni, S., Franceschi, F., Eggenhoffner, R., Zuccarini, M. C., et al. (2019a). Oral administration of a lecithin-based delivery form of boswellic acids (Casperome®) for the prevention of symptoms of irritable bowel syndrome: A randomized clinical study. Minerva Gastroenterol. Dietol. 65 (1), 30–35. doi:10.23736/s1121-421x.18.02530-8
Riva, A., Ronchi, M., Petrangolini, G., Bosisio, S., and Allegrini, P. (2019b). Improved oral absorption of quercetin from quercetin Phytosome™, a new delivery system based on food grade lecithin. Eur. J. Drug Metab. Pharmacokinet. 44 (2), 169–177. doi:10.1007/s13318-018-0517-3
Rondanelli, M., Riva, A., Petrangolini, G., Allegrini, P., Giacosa, A., Fazia, T., et al. (2021). Berberine phospholipid is an effective insulin sensitizer and improves metabolic and hormonal disorders in women with polycystic ovary syndrome: A one-group pretest-post-test explanatory study. Nutrients 13 (10), 3665. doi:10.3390/nu13103665
Saeidi, J., Khansari, Z., and Tozandejani, H. (2020). The effectiveness of Melissa officinalis and lavandula angustifolia in anxiety of oil company employees. J. Sabzevar Univ. Med. Sci. 26 (6), 687–694.
Sahin, S., Eulenburg, V., Kreis, W., Villmann, C., and Pischetsrieder, M. (2016). Three-step test system for the identification of novel GABAA receptor modulating food plants. Plant Foods Hum. Nutr. 71 (4), 355–360. doi:10.1007/s11130-016-0566-1
Salah, S. M., and Jäger, A. K. (2005). Screening of traditionally used Lebanese herbs for neurological activities. J. Ethnopharmacol. 97 (1), 145–149. doi:10.1016/j.jep.2004.10.023
Saqib Lodhi, F., Raza, O., Montazeri, A., Nedjat, S., Yaseri, M., and Holakouie-Naieni, K. (2017). Psychometric properties of the Urdu version of the World Health Organization's quality of life questionnaire (WHOQOL-BREF). Med. J. Islam Repub. Iran. 31, 129. doi:10.14196/mjiri.31.129
Savelev, S., Okello, E., Perry, N., Wilkins, R., and Perry, E. (2003). Synergistic and antagonistic interactions of anticholinesterase terpenoids in Salvia lavandulaefolia essential oil. Pharmacol. Biochem. Behav. 75 (3), 661–668. doi:10.1016/s0091-3057(03)00125-4
Seldenrijk, A., Vis, R., Henstra, M., Ho Pian, K., van Grootheest, D., Salomons, T., et al. (2017). Systematic review of the side effects of benzodiazepines. Ned. Tijdschr. Geneeskd. 161, D1052.
Seldenrijk, A., Vogelzangs, N., Batelaan, N. M., Wieman, I., van Schaik, D. J. F., and Penninx, B. J. W. H. (2015). Depression, anxiety and 6-year risk of cardiovascular disease. J. Psychosomatic Res. 78 (2), 123–129. doi:10.1016/j.jpsychores.2014.10.007
Shakeri, A., Sahebkar, A., and Javadi, B. (2016). Melissa officinalis L. - a review of its traditional uses, phytochemistry and pharmacology. J. Ethnopharmacol. 188, 204–228. doi:10.1016/j.jep.2016.05.010
Sharifi-Rad, J., Quispe, C., Herrera-Bravo, J., Akram, M., Abbaass, W., Semwal, P., et al. (2021). Phytochemical constituents, biological activities, and health-promoting effects of the Melissa officinalis. Oxidative Med. Cell. Longev. 2021, 1–20. doi:10.1155/2021/6584693
Shirazi, M., Jalalian, M. N., Abed, M., and Ghaemi, M. (2021). The effectiveness of Melissa officinalis L. versus citalopram on quality of life of menopausal women with sleep disorder: A randomized double-blind clinical trial. Rev. Bras. Ginecol. Obstet. 43 (2), 126–130. doi:10.1055/s-0040-1721857
Soltanpour, A., Alijaniha, F., Naseri, M., Kazemnejad, A., and Heidari, M. R. (2019). Effects of Melissa officinalis on anxiety and sleep quality in patients undergoing coronary artery bypass surgery: A double-blind randomized placebo controlled trial. Eur. J. Integr. Med. 28, 27–32. doi:10.1016/j.eujim.2019.01.010
Świąder, K., Startek, K., and Wijaya, C. H. (2019). The therapeutic properties of Lemon balm (Melissa officinalis L.): reviewing novel findings and medical indications. J. Appl. Bot. Food Qual. 92, 327–335. doi:10.5073/JABFQ.2019.092.044
Taiwo, A. E., Leite, F. B., Lucena, G. M., Barros, M., Silveira, D., Silva, M. V., et al. (2012). Anxiolytic and antidepressant-like effects of Melissa officinalis (lemon balm) extract in rats: influence of administration and gender. Indian J. Pharmacol. 44 (2), 189–192. doi:10.4103/0253-7613.93846
Talebi, S., Rahmati, B., Jorjani, M., Emadi, F., Ghaffari, F., and Naseri, M. (2022). Synergistic effects of Nepeta menthoides and Melissa officinalis aqueous extracts on reserpine-induced depressive-like behaviors in mice. Phytother. Res. 36 (6), 2481–2494. doi:10.1002/ptr.7457
Tennant, R., Hiller, L., Fishwick, R., Platt, S., Joseph, S., Weich, S., et al. (2007). The Warwick-edinburgh mental well-being scale (WEMWBS): development and UK validation. Health Qual. Life Outcomes 5, 63. doi:10.1186/1477-7525-5-63
Ulbricht, C., Brendler, T., Gruenwald, J., Kligler, B., Keifer, D., Abrams, T. R., et al. (2005). Lemon balm (Melissa officinalis L.): an evidence-based systematic review by the natural standard research collaboration. J. Herb. Pharmacother. 5 (4), 71–114. doi:10.1080/j157v05n04_08
Uritu, C. M., Mihai, C. T., Stanciu, G.-D., Dodi, G., Alexa-Stratulat, T., Luca, A., et al. (2018). Medicinal plants of the family lamiaceae in pain therapy: A review. Pain Res. Manag. 2018, 7801543. doi:10.1155/2018/7801543
US Food and Drug Administration (2016). “§ 182.20 Essential oils, oleoresins (solvent-free), and natural extractives (including distillates),” in Code of federal regulations (21 CFR) (Washington, DC: US Government Printing Office).
Wake, G., Court, J., Pickering, A., Lewis, R., Wilkins, R., and Perry, E. (2000). CNS acetylcholine receptor activity in European medicinal plants traditionally used to improve failing memory. J. Ethnopharmacol. 69 (2), 105–114. doi:10.1016/s0378-8741(99)00113-0
Waqar, H., and Amir, G. (2020). Translation, adaptation and validation of depression, anxiety and stress scale in Urdu. Insights Depress. Anxiety 4, 001–004. doi:10.29328/journal.ida.1001011
Waqas, A., Ahmad, W., Haddad, M., Taggart, F. M., Muhammad, Z., Bukhari, M. H., et al. (2015). Measuring the well-being of health care professionals in the Punjab: A psychometric evaluation of the Warwick-edinburgh mental well-being scale in a Pakistani population. PeerJ 3, e1264. doi:10.7717/peerj.1264
Watson, D., Clark, L. A., and Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: the PANAS scales. J. Pers. Soc. Psychol. 54 (6), 1063–1070. doi:10.1037//0022-3514.54.6.1063
WHO (2004). The World Health Organization quality of life (WHOQOL) - BREF, 2012 revision. https://apps.who.int/iris/handle/10665/77773 (Accessed April 22, 2023).
World Health Organization (2022). Mental disorders. Available at: https://www.who.int/news-room/fact-sheets/detail/mental-disorders (Accessed August 21, 2023).
Yeung, K. S., Hernandez, M., Mao, J. J., Haviland, I., and Gubili, J. (2018). Herbal medicine for depression and anxiety: A systematic review with assessment of potential psycho-oncologic relevance. Phytother. Res. 32 (5), 865–891. doi:10.1002/ptr.6033
Keywords: Melissa officinalis L., lemon balm, depression, anxiety, stress, insomnia, γ-amino butyric acid transaminase, Phytosome™, Relissa™
Citation: Bano A, Hepsomali P, Rabbani F, Farooq U, Kanwal A, Saleem A, Bugti AA, Khan AA, Khalid Z, Bugti M, Mureed S, Khan S, Ujjan ID, Şahin S, Kara M and Khan A (2023) The possible “calming effect” of subchronic supplementation of a standardised phospholipid carrier-based Melissa officinalis L. extract in healthy adults with emotional distress and poor sleep conditions: results from a prospective, randomised, double-blinded, placebo-controlled clinical trial. Front. Pharmacol. 14:1250560. doi: 10.3389/fphar.2023.1250560
Received: 30 June 2023; Accepted: 21 September 2023;
Published: 19 October 2023.
Edited by:
Pinarosa Avato, University of Bari Aldo Moro, ItalyReviewed by:
Emma Wightman, Northumbria University, United KingdomJonathan Cueto-Escobedo, Universidad Veracruzana, Mexico
Copyright © 2023 Bano, Hepsomali, Rabbani, Farooq, Kanwal, Saleem, Bugti, Khan, Khalid, Bugti, Mureed, Khan, Ujjan, Şahin, Kara and Khan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amjad Khan, QW1qYWQua2hhbkByZG0ub3guYWMudWs=, YW1qYWRraGFuQGx1bWhzLmVkdS5waw==