 Hannah Burton
Hannah Burton Yan Zhi Tan2
Yan Zhi Tan2 Catarina Neves
Catarina Neves Raquel Aguiar-Ibáñez
Raquel Aguiar-Ibáñez- 1MSD (UK) Ltd., London, United Kingdom
- 2Lumanity, Utrecht, Netherlands
- 3Lumanity, London, United Kingdom
- 4Merck Canada Inc., Kirkland, QC, Canada
Background: Anti-PD-1 agents are recommended in adjuvant or perioperative settings in some early-stage cancers. The health and productivity benefits of anti-PD-1 use on a population level, however, are unknown.
Methods: A decision model was developed to quantify the health and productivity outcomes of adding anti-PD-1 agents to traditional management strategies in the adjuvant or perioperative setting for melanoma stage IIB/IIC/III, triple negative breast cancer, and renal cell carcinoma in the United Kingdom. The model consisted of four separate Markov models and compared outcomes in two scenarios: one where anti-PD-1 agents are restricted to advanced/metastatic disease, against one where anti-PD-1 agents are used as adjuvant or perioperative therapy for early-stage cancers. Population and incidence inputs were obtained from nation-specific sources, while efficacy and quality of life data were informed by the individual trials. Productivity outcomes were estimated using a human capital approach.
Results: Between 2023 and 2032, 57,075 (60.4%) of 94,426 patients with early-stage cancers eligible for adjuvant or perioperative treatment are estimated to receive anti-PD-1 agents. This was associated with an increase in total life years (8,878, 2.4%), quality-adjusted life-years (9,029, 3.1%), and event-/disease-/recurrence-free life years (25,149, 9.0%), and a reduction in progression events or recurrences (6,839, 16.8%), active metastatic treatments (4,845, 14.0%), and deaths (3,013, 16.2%). The clinical benefits also resulted in a gain in productive years (20,717, 17.6%).
Conclusion: The use of anti-PD-1 agents in adjuvant or perioperative settings can lead to substantial health and productivity gains. Effective planning and investment are needed for timely access to these agents for patients.
1 Introduction
Cancer is a prevalent disease globally with severe health and economic implications. Like similar trends observed worldwide, the incidence of cancer in the UK has risen steadily over the past decades (Shelton et al., 2024; Bray et al., 2024); nearly half of the UK’s population is estimated to be diagnosed with cancer in their lifetime (Cancer Research UK, 2024; Aggarwal et al., 2024), and this incidence is set to rise further (Aggarwal et al., 2024).
Patients living with cancer face considerable health challenges and implications, especially in advanced disease. Despite improving survival rates due to increased implementation of cancer prevention and detection strategies, and advent of more effective cancer therapies (Shelton et al., 2024), cancer patients continue to experience impairments in daily activities, including patients with early-stage cancers (van Leeuwen et al., 2018; Roberts et al., 2024). Additionally, treatment and management of cancer is costly and resource intensive (Landeiro et al., 2024). This also leads to productivity losses for both patients and caregivers due to absences from work or requirements for informal care (Aguiar-Ibáñez et al., 2024). The wider economic impact of cancer on society is therefore extremely large, and was estimated at £18.9 billion in 2018 in England alone (Landeiro et al., 2024).
There has been a concerted effort to address this public health challenge in the United Kingdom. This has culminated in detailed strategies and long-term plans put forward by each of the four devolved nations (Scottish Government, 2023; Wales Cancer Network, 2023; Department of Health, 2022; Department of Health and Social Care, 2024). All nations emphasized the importance of earlier cancer diagnosis where prognosis is better, and disease burden lower, compared with cancers diagnosed at a late-stage. Wide-ranging measures, such as encouraging cancer screening uptake and coverage, optimizing diagnostic and referral pathways, and capacity building, were further identified to achieve this objective (Scottish Government, 2023; Wales Cancer Network, 2023; Department of Health, 2022; Department of Health and Social Care, 2024).
However, for health outcomes to be improved, earlier cancer diagnosis must be accompanied by timely receipt of effective treatments. While surgery remains one of the primary treatment modalities for many early-stage cancers, patients may still experience high risk of disease recurrence (Loibl et al., 2024; Michielin et al., 2019; Powles et al., 2024). Adjuvant or perioperative therapies that are given for a short period either after and/or before surgery have been shown to further reduce risk of recurrences and improve long-term outcomes. One example of such therapies includes the anti-PD-1 agents. These agents function by modulating immune checkpoints, thereby enhancing the immune system’s capacity to recognize and target malignant cells (LaFleur et al., 2018). Initially approved for advanced stage cancers, more recently anti-PD-1 agents have been shown to significantly improve event-free (EF), disease-free (DF) and recurrence-free (RF) survival when given as adjuvant or perioperative therapy for approximately 1 year in several early-stage cancers (Choueiri et al., 2024; Eggermont et al., 2021; Luke et al., 2022; Schmid et al., 2024; Wakelee et al., 2023). Furthermore, improvements in overall survival were also observed (Choueiri et al., 2024; Schmid et al., 2024; Wakelee et al., 2023).
However, these outcomes were reported in individual indications, and the potential health and productivity benefits of anti-PD-1 agents use across multiple early-stage cancer indications on a population level remain unknown. We therefore conducted this study to estimate the impact of wide-scale adoption of anti-PD-1 agents at a population level when used as adjuvant or perioperative treatment for some early-stage cancers in the United Kingdom.
2 Methods
2.1 Model overview
A decision model was developed to quantify the health and productivity outcomes of adding anti-PD-1 agents to traditional management strategies in the adjuvant or perioperative setting for three early-stage cancers over a 10-year period in the UK from 2023 to 2032. This time horizon was selected to balance capturing the potential long-term benefits of anti-PD-1 agents with the greater uncertainty in outcomes when extrapolating further into the future and unknown future changes in the external environment. The model examined and compared the outcomes in two scenarios – one where anti-PD-1 agents are not used as adjuvant or perioperative therapy for early-stage cancers (Scenario 1), against one where anti-PD-1 agents are used as adjuvant or perioperative therapy for early-stage cancers (Scenario 2) (Figure 1). Three licensed indications (melanoma stage IIB/IIC/III, triple negative breast cancer [TNBC] and renal cell carcinoma [RCC]) where anti-PD-1 agents had been approved by the Medicines & Healthcare products Regulatory Agency (MHRA) and recommended, based on clinical and cost-effectiveness, by the National Institute for Health and Care Excellence (NICE) and the Scottish Medicines Consortium (SMC) for routine use throughout the UK were selected (National Institute for Health and Care Excellence, 2022a; National Institute for Health and Care Excellence, 2022b; National Institute for Health and Care Excellence, 2022c; National Institute for Health and Care Excellence, 2022d; Scottish Medicines Consortium, 2023a; Scottish Medicines Consortium, 2023b; Scottish Medicines Consortium, 2019; Scottish Medicines Consortium, 2022a). To ensure methodological robustness, the decision model comprised of four separate Markov models (melanoma stage IIB/C, melanoma stage III, TNBC, and RCC) that had been submitted to, and accepted by, health technology assessment (HTA) bodies (National Institute for Health and Care Excellence, 2022a; National Institute for Health and Care Excellence, 2022b; National Institute for Health and Care Excellence, 2022c; National Institute for Health and Care Excellence, 2022d; Scottish Medicines Consortium, 2023a; Scottish Medicines Consortium, 2023b; Scottish Medicines Consortium, 2019; Scottish Medicines Consortium, 2022a). All outcomes were discounted at 3.5% following prevailing NICE guidance (National Institute for Health and Care Excellence, 2022e).
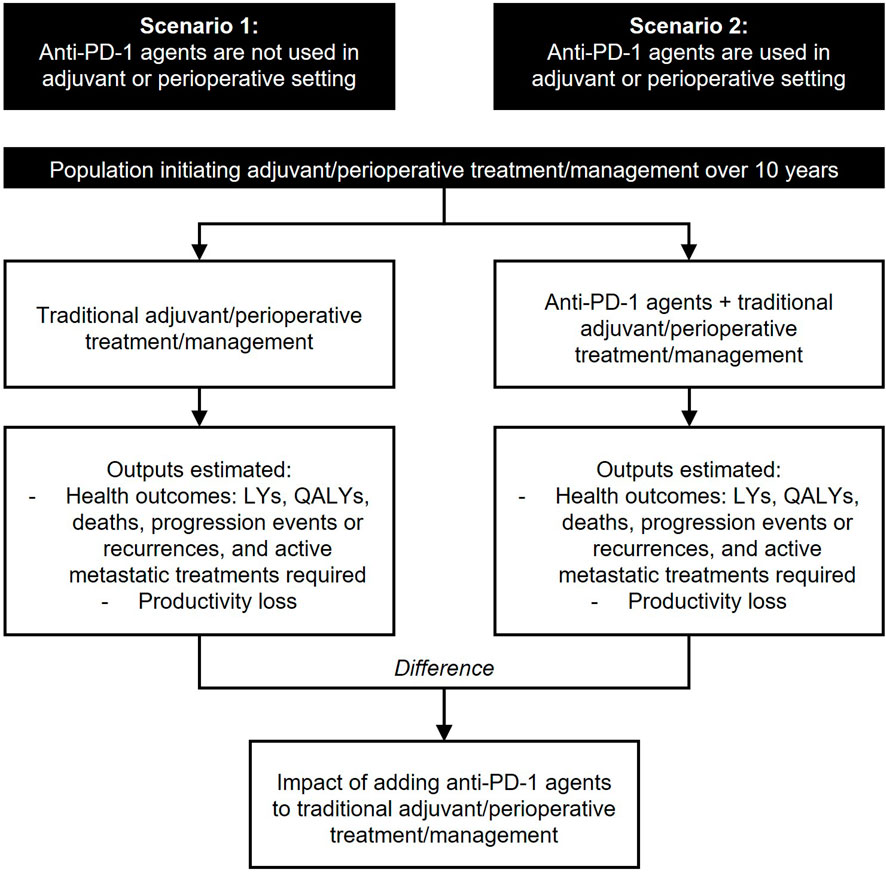
Figure 1. Analysis overview. Key: LY, life-year, QALY, quality-adjusted life-year.
Analyses were conducted separately for each devolved UK nation (i.e., England, Scotland, Wales, and Northern Ireland) and then aggregated to obtain results for the entire United Kingdom. All models shared the same structure with four mutually exclusive health states. New incident cohorts entered the model in the EF/DF/RF state on a weekly basis, initiated treatment with an anti-PD-1 agent or conventional strategies in the adjuvant or perioperative setting (as per the relevant license), and were subjected to a risk of three competing events: locoregional recurrence (LR), distant metastases (DM), or death, the absorbing state (Supplementary Figure S1). To enable granular calculation of health state occupancy and outcomes, a 1-week cycle length was used.
2.2 Model inputs
2.2.1 Population
All starting patient characteristics in the model were consistent with the population from relevant trials at baseline. Eligible population size for each indication was derived by multiplying the general population size with indication- and nation-specific incidence and eligibility rates (Supplementary Figure S2; Supplementary Table S1). General population size was retrieved from the Office for National Statistics (ONS) for all nations (Office for National Statistics, 2024a). The estimated annual growth rate for each nation was also derived from ONS and assumed to be equal across the 10-year horizon (Office for National Statistics, 2024b). Incidence rates for each of the three tumour types were derived from country specific databases (National Disease Registration Service, 2024; Northern Ireland Cancer Registry, 2024a; Northern Ireland Cancer Registry, 2024b; Northern Ireland Cancer Registry, 2024c; Public Health Scotland, 2021; Public Health Scotland, 2024a; Public Health Scotl and, 2024; Public Health Scotland, 2024b; Public Health Wales, 2024); 2022 rates were used where possible as these were the most recent data available, although values for Wales were for 2021 as 2022 data were not available at the time of the analysis.
2.2.2 Treatment mix
Treatment mix in the adjuvant or perioperative setting in Scenarios 1 and 2 was informed by published resource impact templates (RITs) that reflected NHS England predictions of treatment practices and uptake of anti-PD-1 agents at the time of the NICE technology appraisal guidance (Table 1) (National Institute for Health and Care Excellence, 2021a; National Institute for Health and Care Excellence, 2022f; National Institute for Health and Care Excellence, 2022g; National Institute for He alth and Care Excellence, 2022). The same mix was assumed across the model time horizon.
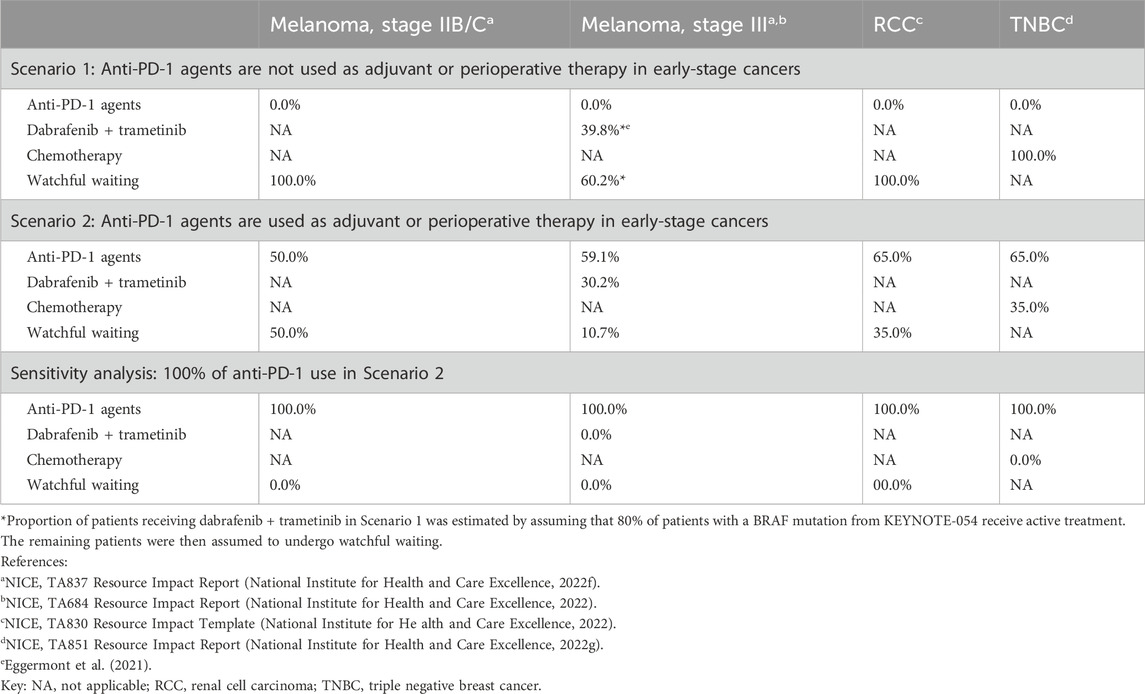
Table 1. Treatment mix in the adjuvant or perioperative setting, by indication.
Upon entry into the DM state (from EF/DF/RF or LR states), patients were assumed to initiate first-line metastatic treatment contingent on: (a) previous treatments used in the adjuvant or perioperative setting; and (b) whether re-treatment with anti-PD-1 agents was allowed. The choice of possible therapies was based on treatment options approved by NICE and the SMC, and the proportion of patients receiving each therapy was informed by market research and expert clinical opinion. Re-treatment with anti-PD-1 agents in the metastatic setting was permitted for patients who entered the DM state at least 6 months after completing adjuvant or perioperative therapy.
2.2.3 Efficacy
Transition probabilities from the EF/DF/RF states were derived from parametric modelling fitted to patient-level data from the respective trials of pembrolizumab (Eggermont et al., 2021; Long et al., 2022; Powles et al., 2022; Schmid et al., 2022). Extrapolations of trial data were aligned with those used in the corresponding HTA cost-effectiveness models, where the parametric distributions were selected based on a combination of statistical fit, visual fit to observed trial data, and clinical plausibility (National Institute for Health and Care Excellence, 2022a; National Institute for Health and Care Excellence, 2022b; National Institute for Health and Care Excellence, 2022c; National Institute for Health and Care Excellence, 2022d; Scottish Medicines Consortium, 2023a; Scottish Medicines Consortium, 2023b; Scottish Medicines Consortium, 2019; Scottish Medicines Consortium, 2022a). Long-term survival estimates were validated against relevant external sources of data where available. Transitions from the LR state were estimated from the relevant trials, or real-world evidence if trial data were insufficient.
For dabrafenib + trametinib in melanoma stage III, transitions from the RF state were estimated by applying a hazard ratio against the RFS curve of pembrolizumab, while transitions from the LR state were assumed to be similar to that of pembrolizumab. For simplicity, efficacy of other anti-PD-1 agents (applicable only for melanoma stage III) was assumed to be equivalent to that of pembrolizumab (Franken et al., 2019). The efficacy of individual first-line subsequent treatments was used to derive transitions from the DM state to death. All transitions to death were adjusted for background mortality.
2.2.4 Utilities
Utility values were assigned to each health state to represent the differences in health-related quality of life (HRQoL) between different recurrence statuses. All health-state utility values (HSUVs) were mapped to EQ-5D-3L using the UK value set based on the EQ-5D-5L questionnaire responses collected in the pivotal trials (van Hout et al., 2012; Dolan, 1997), or other published sources where necessary, and adjusted for age and sex (Ara and Brazier, 2010). Adverse event (AE) disutilities associated with Grade 3+ adverse events that occurred in ≥5% of patients in either arm of the respective clinical trials were applied once at treatment initiation to capture the impact of treatment tolerability on HRQoL.
2.2.5 Productivity losses
Acknowledging that there may be wider societal benefits associated with improving health outcomes, patients’ and caregivers’ productivity was examined in the model using a human capital approach. Standard working hours per week were assumed to be 36.6 for all nations, based on UK labour estimates (Office for National Statistics, 2024c). Inputs relating to the impact of early stage cancer on patients’ and caregivers’ presenteeism and absenteeism within these standard working hours were obtained from a survey on the human and economic burden of early-stage cancer and applied across all indications (Supplementary Table S2) (Aguiar-Ibáñez et al., 2024).
2.3 Outcomes
The modelled outcomes for Scenarios 1 and 2 included total and event-/disease-/recurrence-free life years and quality-adjusted life-years (QALYs), progression events or recurrences, number of active metastatic treatments, deaths, and productivity losses. The impact of adding anti-PD-1 agents to the early-stage setting was estimated by taking the difference between the outcomes of the two scenarios. For each outcome, model results for the four individual indications were then summed to derive the total impact and appropriately reflect the incidence of each cancer.
To examine the potential benefits of broader adoption of anti-PD-1 agents beyond current estimates, a sensitivity analysis was conducted by assuming all patients will be treated with anti-PD-1 agents (i.e. 100% uptake). While a small proportion of patients may be contraindicated to immuno-oncology (IO) therapy, this analysis will represent the most optimistic impact should there be full uptake of anti-PD-1 agents.
3 Results
Between 2023 and 2032, 57,075 (60.4%) of 94,426 patients with early-stage cancers eligible for adjuvant or perioperative treatment are estimated to receive adjuvant or perioperative anti-PD-1 agents for the treatment of melanoma stage IIB/C and III, RCC, and TNBC across all four devolved nations (Supplementary Table S3). Using anti-PD-1 agents in early-stage cancer was estimated to result in overall health gains with increases in total life years (8,878, 2.4%), QALYs (9,029, 3.1%), and event-/disease-/recurrence-free life years (25,149, 9.0%) (Table 2). The use of anti-PD-1 agents was also associated with reductions in progression events or recurrences (6,839, 16.8%), active metastatic treatments (4,845, 14.0%), and deaths (3,013, 16.2%). The gains in total life years, event-/disease-/recurrence-free life years and QALYs were also expected to accumulate steadily over the 10-year horizon, reflecting long-term clinical benefit resulting from reductions in progression events or recurrences, and increasing number of patients treated over the years (Figure 2). Benefits of treatment were seen across the four cancer types (Supplementary Table S4).
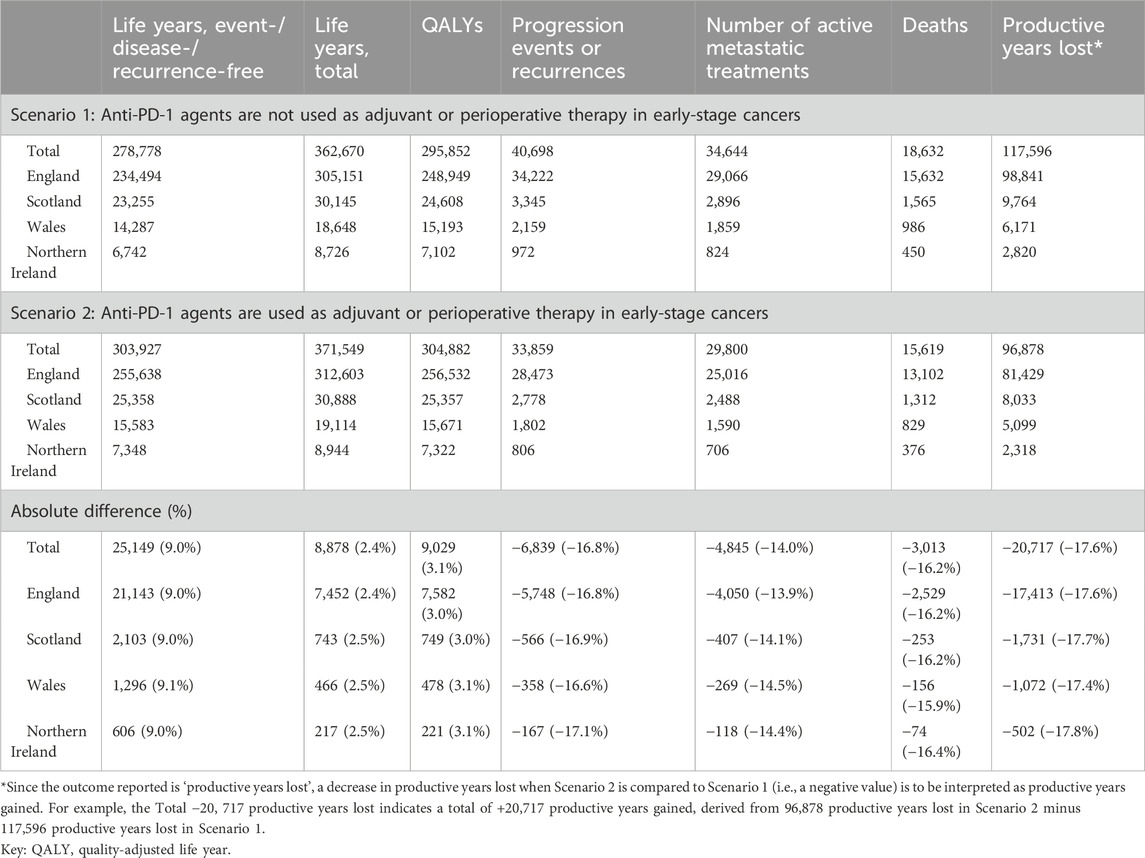
Table 2. Estimated outcomes, by nation.
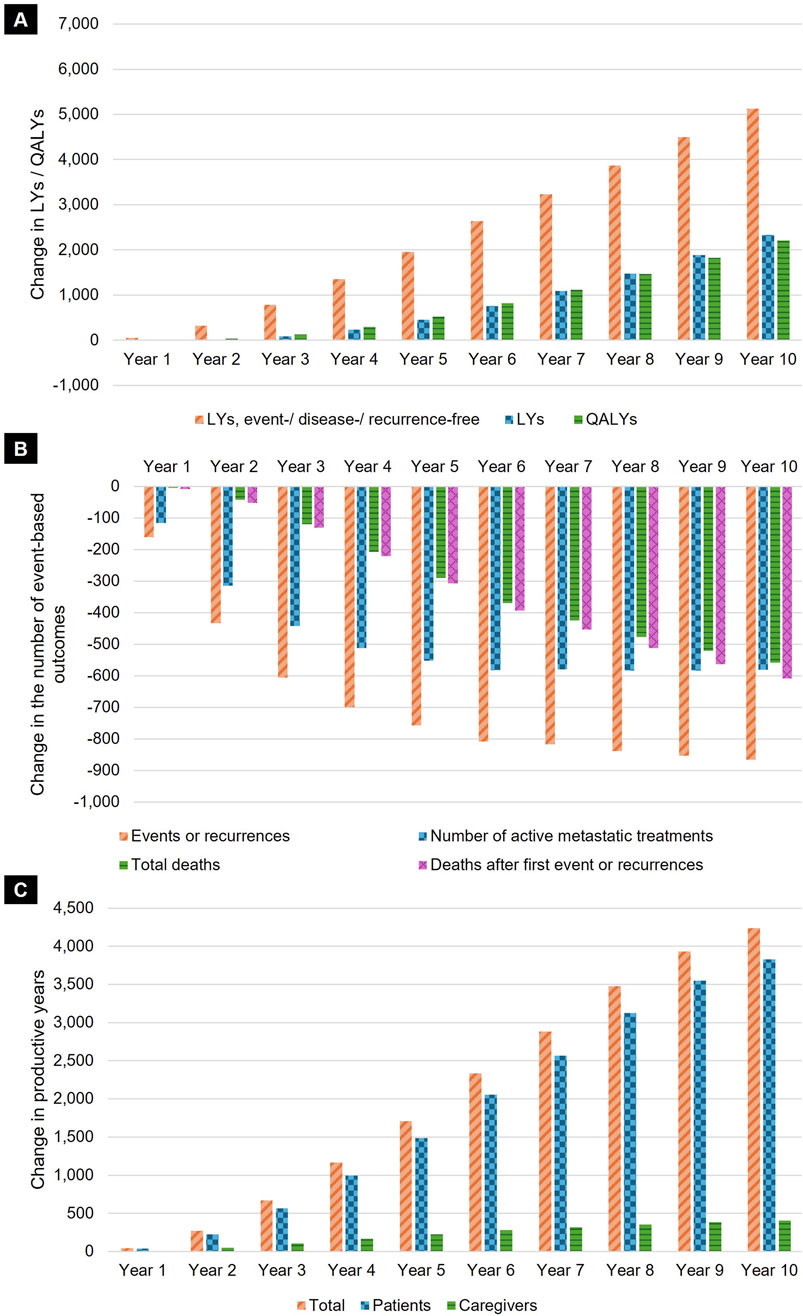
Figure 2. Annual impact of using anti-PD-1 agents in early-stage cancer. Results presented reflect the annual impact of the modelled uptake of anti-PD-1 agents (i.e., Scenario 2 vs. Scenario 1) on the total estimated (A) LYs, event-/disease-/recurrence-free LYs, and QALYs; (B) event-based outcomes (progression events or recurrences, deaths, deaths after first event or recurrence, and number of active metastatic treatments after progression or recurrence); and (C) productive years gained (increase in productive working time for patients and their caregivers, as a result of improved health outcomes). Key: LY, life-year; QALY, quality-adjusted life-year.
As a result of the reductions in progression events, recurrences and death, use of anti-PD-1 agents was also associated with overall productivity gains due to lower presenteeism and absenteeism for both patients and caregivers (Figure 2). This is estimated to result in a gain of 20,717 productive years (17.6%) across the entire 10-year horizon.
Increasing anti-PD-1 agent uptake in the adjuvant or perioperative setting to all eligible patients resulted in further health and productivity gains (Supplementary Table S5). Assuming 100% uptake of anti-PD-1 agents can lead to further gains of 58.6%, 60.7%, and 60.6% in life years, event-/disease-/recurrence-free life years, and QALYs, respectively, compared with the primary analysis. Additionally, there were greater reductions in progression events or recurrences, number of active metastatic treatments, and deaths (60.3%, 71.0%, and 62.6% respectively), corresponding to larger productivity gains (12,598 productive years, 60.8%).
4 Discussion
Previous studies have demonstrated the clinical efficacy and cost-effectiveness of anti-PD-1 agents as treatments for early-stage cancers. Building on this, our study demonstrates that substantial health and productivity gains can be realized on a population level with adjuvant or perioperative anti-PD-1 use across multiple early-stage cancers throughout the United Kingdom. These benefits are considerable even with modest predictions regarding the extent of anti-PD-1 uptake in each indication and are estimated to be even greater with higher levels of uptake. Furthermore, the potential reduction in cancer progression events or recurrences and number of active metastatic treatments is pronounced across all nations. While differences in magnitude were observed across individual cancer types, primarily reflecting variations in relative efficacy, place in therapy, and disease incidence, the overall health and societal benefits associated with the introduction of anti-PD-1 agents were consistently demonstrated. In addition to direct impact on a patient’s life expectancy and quality of life, these reductions may avert potential costs and resource use associated with later lines of treatment for metastatic disease as well as terminal care, both of which are often costly and require extensive healthcare resource use (Ray et al., 2013). This study estimated productivity gains of 17.6%, suggesting that adjuvant or perioperative anti-PD-1 agent use in early cancers may lead to notable societal benefits.
Our findings underscore the importance of advancing access for new treatment options, such as anti-PD-1 agents, in early-stage cancers. The health and productivity benefits that increased uptake of such agents may confer are synergistic to the intended outcomes of enhanced screening, detection, and diagnosis outlined by all four devolved nations in their cancer strategies. Specifically, all nations have committed to increasing the share of early-stage cancer diagnosis. Under the NHS Long Term Plan, NHS England has committed to increase the proportion of cancers diagnosed at stages I and II in England from half to three-quarters of cases by 2028 (National Health Services, 2019). This is anticipated to result in 55,000 more people being expected to survive their cancer for at least 5 years annually. Similarly, the Scottish government plans to reduce the proportion of late-stage cancer diagnoses from 42% to 24% by 2033 (Scottish Government, 2023). While no specific targets have been set by Northern Ireland and Wales, plans to enhance early-stage cancer diagnosis were regarded as important measures to tackle growing health inequalities in both nations (Wales Cancer Network, 2023; Department of Health, 2022).
However, the benefits of early diagnosis can only be achieved when coupled with timely initiation of effective treatments. Cancers that are diagnosed early are more likely to undergo surgical treatment with a curative intent (Cancer Research UK, 2024). Despite this, the chance of recurrence following surgery may still be high in aggressive cancers such as TNBC and melanoma (Romano et al., 2010; Costa and Gradishar, 2017). Current clinical evidence supports the addition of adjuvant or perioperative treatments, such as anti-PD-1 agents, to reduce the risk of relapse and mortality after surgical resection compared to traditional adjuvant or perioperative options such as chemotherapy or watchful waiting (Choueiri et al., 2024; Eggermont et al., 2021; Luke et al., 2022; Schmid et al., 2024). Economic analyses have frequently demonstrated that these new treatments are also cost-effective, and have resulted in recommendations by NICE and the SMC for nationwide routine commissioning (National Institute for Health and Care Excellence, 2022a; National Institute for Health and Care Excellence, 2022b; National Institute for Health and Care Excellence, 2022c; National Institute for Health and Care Excellence, 2022d; Scottish Medicines Consortium, 2023a; Scottish Medicines Consortium, 2023b; Scottish Medicines Consortium, 2019; Scottish Medicines Consortium, 2022a; National Institute for Health and Care Excellence, 2021b; Scottish Medicines Consortium, 2018). Facilitating and expanding consistent access to these agents will therefore be needed to translate the advantages of early diagnosis into more substantial health gains, and to ensure equitable access across the United Kingdom.
Despite the importance of prompt initiation of cancer treatment, waiting times to start treatment are currently long and disparate across all four devolved nations. The proportion of patients meeting the 62-day standard, a measure where patients begin treatment within 62 days of an urgent referral, ranged from 38% in Northern Ireland to 72% in Scotland in the fourth quarter of 2022, well below the targets for each nation (Scottish Government, 2023; Wales Cancer Network, 2023; Department of Health, 2022; Office for National Statistics, 2025). An international benchmarking study further highlights that UK cancer patients face longer waits and lower treatment uptake than those in comparable countries (McPhail et al., 2024). Treatment for cancer is often time-sensitive, and delays in initiating treatment may reduce patients’ capacity to benefit. In some instances, patients may even miss the opportunity to receive treatment if the disease progresses. Effective treatment options, and the corresponding prognosis, may also be limited for advanced disease, and treatment delays have been associated with poorer outcomes across many cancers (Hanna et al., 2020). This may result in poorer health outcomes on a population level that may lead to wider societal impact.
Understanding potential reasons for delays in diagnosis and subsequently starting cancer treatment may provide better insights into how earlier diagnosis and access to effective treatments can be improved. First, ongoing capacity and workforce challenges in healthcare systems across all four nations have been cited as key reasons for delayed access to cancer services, including consultations and drug administrations (Wales Cancer Network, 2023; Department of Health, 2022; Department of Health and Social Care, 2024). Access to general practitioners and emergency departments has also been impaired, resulting in delayed or missed diagnoses and, by extension, treatment initiation (Department of Health and Social Care, 2024). Despite concerns that increased adoption of immunotherapies may exacerbate the already strained healthcare system (Scottish Government, 2023; Wales Cancer Network, 2023), encouraging its use in early-stage cancer represents a partial shift in capacity allocation rather than isolated increased demand for healthcare resources. Investing in optimal care for patients with early-stage cancers, which includes the use of adjuvant and perioperative treatments such as anti-PD-1 agents, may contribute to alleviation of capacity requirements in the advanced setting in the longer-term. Results may be even more pronounced with larger and wider adoption of these therapies, as demonstrated in this study.
Secondly, delivery of systemic anti-cancer therapy (SACT), including anti-PD-1 agents, has traditionally been confined to hospitals which may deter some patients from initiating treatment due to cost or inconvenience (Scottish Government, 2023; Department of Health, 2022). Channelling newly diagnosed patients into an already constrained system may lead to further delay in initiation of cancer care. Novel methods of treatment delivery could be explored to ease hospital footfall; suggestions to shift some SACT delivery to homes and community settings may increase accessibility and appeal (Franken et al., 2020), particularly for those who are initiating cancer treatment.
Finally, the role of geographic and socioeconomic factors should also be considered. Ensuring equitable access is a stated priority in each nation’s cancer plan (Scottish Government, 2023; Department of Health, 2022; National Health Services, 2019; Welsh Government, 2025). However, people living in more rural or more deprived areas of the UK are less likely to have their cancer diagnosed at an early stage and are more likely to have longer waits to begin cancer treatment (Cancer Research UK, 2025; Dobson et al., 2022). Whilst the reasons for these disparities are multifaceted and complex, targeted interventions within these areas to improve symptom awareness, health literacy and screening attendance, to remove or reduce practical barriers to accessing care, and to ensure healthcare providers are adequately resourced would support earlier diagnoses and shorter intervals to initiation of effective treatments overall.
4.1 Strengths and limitations
This study is the first to examine the impact of the widespread adoption of anti-PD-1 agents for multiple early-stage cancers in the UK, using models accepted by HTA agencies. Outcomes in this model were accrued from the point of adjuvant and perioperative treatment initiation with new incident cohorts entering the model on a weekly basis until the end of the study time horizon; this provides a dynamic and more accurate representation of overall benefits compared to typical models where outcomes are modelled from a single treatment initiation timepoint. In addition, incidence and population projections specific to each of the four UK nations were used wherever possible to increase significance of the results. Further, subsequent treatments were comprehensively modelled, which enhanced the relevance of the outcomes to real-world clinical practice. Whilst this study focused on the impact in the UK, the overall conclusions are also applicable to other countries and healthcare systems.
Our study had some limitations. First, the 10-year study horizon may not be sufficient to confirm the long-term trajectory of current findings, but is intended to balance capturing potential benefits with future uncertainty and is also aligned with the time frame considered in the government’s 10-Year Health Plan for England (Department of Health and Social Care, 2025). Second, productivity inputs were proxied from a survey of US patients given the lack of relevant UK-specific values (Aguiar-Ibáñez et al., 2024), although overall conclusions relating to societal benefits observed in this analysis would not be expected to change. Third, uptake of anti-PD-1 agents was assumed to be constant across the time horizon. Thus any changes to the uptake due to newly approved agents in the future could not be accounted for. Similarly, constant incidence rates were applied; if cancer incidence rates continue to rise over time, the benefits of anti-PD-1 agents estimated here may be slightly underestimated. Fourth, while the model used the latest trial data-cuts available at the time of the HTA appraisals, more mature data can be used to validate current results in the future. Further, in the absence of real-world evidence, this analysis is based on clinical trial data; trial populations tend to be fitter than real-world populations, therefore it is plausible that the benefits of anti-PD-1 agents in the real-world differ slightly to those estimated in this study. Lastly, while this study focused on three specific indications driven by availability of patient-level data, other anti-PD-1 agents have also been approved by NICE and the SMC for routine use in further tumour types (Scottish Medicines Consortium, 2018; National Institute for Health and Care Excellence, 2021c; National Institute for Health and Care Excellence, 2022h; National Institute for Health and Care Excellence, 2023; Scottish Medicines Consortium, 2022b; Scottish Medicines Consortium, 2023c), and the number of recommended early-stage indications is set to grow as the evidence base evolves. Therefore, the full extent of the health and societal impact of anti-PD-1 agents reported in this study is likely to be underestimated and the results of this study are likely to be conservative.
5 Conclusion
Access to anti-PD-1 agents as adjuvant or perioperative therapy for early-stage cancers is estimated to deliver substantial health benefits at a UK population level over a 10-year time horizon. These benefits are expected to rise in the longer-term, following trends observed from this study, and will increase further if uptake exceeds predictions. Adopting anti-PD-1 agents in the treatment of early-stage cancers may also lead to substantial productivity gains. However, these gains may not be fully realized if ongoing access challenges, particularly capacity constraints within the health system, are not addressed. It is therefore imperative to effectively plan and invest in the necessary resources and implementation strategies to ensure consistent access and timely initiation of appropriate treatment for patients with early-stage cancer across the whole of the United Kingdom.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
HB: Conceptualization, Writing – review and editing, Writing – original draft, Methodology. YT: Writing – review and editing, Writing – original draft, Methodology. SG: Methodology, Writing – review and editing. CN: Methodology, Writing – review and editing, Conceptualization. NM: Conceptualization, Writing – review and editing, Supervision. RA-I: Supervision, Writing – review and editing, Methodology, Conceptualization.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article.
Conflict of interest
HB and NM are employees of MSD (UK) Ltd., and may own stock and/or hold stock options in Merck & Co., Inc, Rahway, NJ, USA. RAI is an employee of Merck Canada Inc., and may own stock and/or hold stock options in Merck & Co., Inc, Rahway, NJ, USA. YZT, SG and CN are employees of Lumanity which received consultancy fees for the study from Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc, Rahway, NJ, USA.
The authors declare that this study received funding from Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. The funder was involved in the study design, collection, analysis, interpretation of data, the writing of this article and the decision to submit it for publication.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2025.1613120/full#supplementary-material
References
Aggarwal, A., Choudhury, A., Fearnhead, N., Kearns, P., Kirby, A., Lawler, M., et al. (2024). The future of cancer care in the Uk; time for a radical and sustainable national cancer plan. Lancet Oncol. 25 (1), e6–e17. doi:10.1016/S1470-2045(23)00511-9
Aguiar-Ibáñez, R., McQuarrie, K., Jayade, S., Penton, H., DiGiovanni, L., Raina, R., et al. (2024). Impact of recurrence on employment, finances, and productivity for early-stage cancer patients and caregivers: us survey. Future Oncol., 1–17. doi:10.1080/14796694.2024.2436342
Ara, R., and Brazier, J. E. (2010). Populating an economic model with health state utility values: moving toward better practice. Value Health 13 (5), 509–518. doi:10.1111/j.1524-4733.2010.00700.x
Bray, F., Laversanne, M., Sung, H., Ferlay, J., Siegel, R. L., Soerjomataram, I., et al. (2024). Global cancer statistics 2022: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 74 (3), 229–263. doi:10.3322/caac.21834
Cancer Research UK (2024). Cancer in the Uk, overview 2024. Available online at: https://www.cancerresearchuk.org/sites/default/files/cancer_in_the_uk_overview_2024.pdf.
Choueiri, T. K., Tomczak, P., Park, S. H., Venugopal, B., Ferguson, T., Symeonides, S. N., et al. (2024). Overall survival with adjuvant pembrolizumab in renal-cell carcinoma. N. Engl. J. Med. 390 (15), 1359–1371. doi:10.1056/NEJMoa2312695
Costa, R. L. B., and Gradishar, W. J. (2017). Triple-negative breast cancer: current practice and future directions. J. Oncol. Pract. 13 (5), 301–303. doi:10.1200/JOP.2017.023333
Department of Health (2022). A cancer strategy for northern Ireland 2022-2032. Available online at: https://www.health-ni.gov.uk/sites/default/files/publications/health/doh-cancer-strategy-march-2022.pdf.
Department of Health and Social Care (2024). Independent investigation of the national health service in England. Available online at: https://assets.publishing.service.gov.uk/media/66f42ae630536cb92748271f/Lord-Darzi-Independent-Investigation-of-the-National-Health-Service-in-England-Updated-25-September.pdf.
Department of Health and Social Care (2025). 10 year health plan for England: fit for the future. Available online at: https://www.gov.uk/government/publications/10-year-health-plan-for-england-fit-for-the-future.
Dobson, C., Deane, J., Macdonald, S., Murchie, P., Ellwood, C., Angell, L., et al. (2022). Barriers to early presentation amongst rural residents experiencing symptoms of colorectal cancer: a qualitative interview study. Cancers (Basel) 15 (1), 274. doi:10.3390/cancers15010274
Dolan, P. (1997). Modeling valuations for euroqol health states. Med. Care 35 (11), 1095–1108. doi:10.1097/00005650-199711000-00002
Eggermont, A. M. M., Blank, C. U., Mandalà, M., Long, G. V., Atkinson, V. G., Dalle, S., et al. (2021). Adjuvant pembrolizumab versus placebo in resected stage iii melanoma (eortc 1325-Mg/Keynote-054): distant metastasis-free survival results from a double-blind, randomised, controlled, phase 3 trial. Lancet Oncol. 22 (5), 643–654. doi:10.1016/s1470-2045(21)00065-6
Franken, M. G., Leeneman, B., Gheorghe, M., Uyl-de Groot, C. A., Haanen, J., and van Baal, P. H. M. (2019). A systematic literature review and network meta-analysis of effectiveness and safety outcomes in advanced melanoma. Eur. J. Cancer 123, 58–71. doi:10.1016/j.ejca.2019.08.032
Franken, M., Kanters, T., Coenen, J., de Jong, P., Jager, A., and Groot, C. U. (2020). Hospital-based or home-based administration of oncology drugs? A micro-costing study comparing healthcare and societal costs of hospital-based and home-based subcutaneous administration of trastuzumab. Breast 52, 71–77. doi:10.1016/j.breast.2020.05.001
Hanna, T. P., King, W. D., Thibodeau, S., Jalink, M., Paulin, G. A., Harvey-Jones, E., et al. (2020). Mortality due to cancer treatment delay: systematic review and meta-analysis. BMJ 371, m4087. doi:10.1136/bmj.m4087
LaFleur, M. W., Muroyama, Y., Drake, C. G., and Sharpe, A. H. (2018). Inhibitors of the Pd-1 pathway in tumor therapy. J. Immunol. 200 (2), 375–383. doi:10.4049/jimmunol.1701044
Landeiro, F., Harris, C., Groves, D., O’Neill, S., Jandu, K. S., Tacconi, E. M. C., et al. (2024). The economic burden of cancer, coronary heart disease, dementia, and stroke in England in 2018, with projection to 2050: an evaluation of two cohort studies. Lancet Healthy Longev. 5 (8), e514–e523. doi:10.1016/S2666-7568(24)00108-9
Loibl, S., André, F., Bachelot, T., Barrios, C. H., Bergh, J., Burstein, H. J., et al. (2024). Early breast cancer: esmo clinical practice guideline for diagnosis, treatment and Follow-Up. Ann. Oncol. 35 (2), 159–182. doi:10.1016/j.annonc.2023.11.016
Long, G. V., Luke, J. J., Khattak, M. A., de la Cruz Merino, L., Del Vecchio, M., Rutkowski, P., et al. (2022). Pembrolizumab versus placebo as adjuvant therapy in resected stage iib or Iic Melanoma (Keynote-716): distant metastasis-free survival results of a multicentre, Double-Blind, randomised, phase 3 trial. Lancet Oncol. 23 (11), 1378–1388. doi:10.1016/s1470-2045(22)00559-9
Luke, J. J., Rutkowski, P., Queirolo, P., Del Vecchio, M., Mackiewicz, J., Chiarion-Sileni, V., et al. (2022). Pembrolizumab versus placebo as adjuvant therapy in completely resected stage iib or Iic Melanoma (Keynote-716): a randomised, double-blind, phase 3 trial. Lancet 399 (10336), 1718–1729. doi:10.1016/s0140-6736(22)00562-1
McPhail, S., Barclay, M. E., Johnson, S. A., Swann, R., Alvi, R., Barisic, A., et al. (2024). Use of chemotherapy in patients with oesophageal, stomach, Colon, rectal, liver, pancreatic, lung, and ovarian cancer: an international cancer benchmarking partnership (Icbp) population-based study. Lancet Oncol. 25 (3), 338–351. doi:10.1016/s1470-2045(24)00031-7
Michielin, O., van Akkooi, A. C. J., Ascierto, P. A., Dummer, R., and Keilholz, U.ESMO Guidelines Committee. Electronic address:Y2xpbmljYWxndWlkZWxpbmVzQGVzbW8ub3Jn(2019). Cutaneous Melanoma: Esmo Clinical Practice Guidelines for diagnosis, treatment and Follow-Up. Ann. Oncol. 30 (12), 1884–1901. doi:10.1093/annonc/mdz411
National Disease Registration Service (2024). Cancer Incidence and Mortality, 2022. Available online at: https://nhsd-ndrs.shinyapps.io/incidence_and_mortality/.
National Health Services (2019). The nhs long term plan. Available online at: https://www.longtermplan.nhs.uk/wp-content/uploads/2019/08/nhs-long-term-plan-version-1.2.pdf.
National Institute for Health and Care Excellence (2022). Resource impact report: pembrolizumab for adjuvant treatment of renal cell carcinoma (Ta830). Available online at: https://www.nice.org.uk/guidance/ta830/resources/resource-impact-report-pdf-11253520477.
National Institute for Health and Care Excellence (2021a). Resource impact report: nivolumab for adjuvant treatment of completely resected melanoma with lymph node involvement or metastatic disease (Ta684). Available online at: https://www.nice.org.uk/guidance/ta684/resources/resource-impact-report-pdf-9024957757.
National Institute for Health and Care Excellence (2021b). Nivolumab for adjuvant treatment of completely resected melanoma with lymph node involvement or metastatic disease. Available online at: https://www.nice.org.uk/guidance/ta684/documents/committee-papers-5.
National Institute for Health and Care Excellence (2021c). Nivolumab for adjuvant treatment of resected oesophageal or gastro-oesophageal junction cancer. Available online at: https://www.nice.org.uk/guidance/ta746/documents/committee-papers.
National Institute for Health and Care Excellence (2022). Resource impact statement: pembrolizumab for adjuvant treatment of completely resected stage 3 melanoma (Ta766). Available online at: https://www.nice.org.uk/guidance/ta766/resources/resource-impact-statement-pdf-14195345122501.
National Institute for Health and Care Excellence (2022a). Pembrolizumab for neoadjuvant and adjuvant treatment of triple-negative early or locally advanced breast cancer. Available online at: https://www.nice.org.uk/guidance/ta851/history.
National Institute for Health and Care Excellence (2022b). Pembrolizumab for adjuvant treatment of resected stage 2b or 2c melanoma. Available online at: https://www.nice.org.uk/guidance/ta837.
National Institute for Health and Care Excellence (2022c). Pembrolizumab for adjuvant treatment of completely resected stage 3 melanoma. Available online at: https://www.nice.org.uk/guidance/ta766.
National Institute for Health and Care Excellence (2022d). Pembrolizumab for adjuvant treatment of renal cell carcinoma. Available online at: https://www.nice.org.uk/guidance/ta830.
National Institute for Health and Care Excellence (2022e). Nice health technology evaluations: the manual. Available online at: https://www.nice.org.uk/process/pmg36/chapter/economic-evaluation-2.
National Institute for Health and Care Excellence (2022f). Resource impact report: pembrolizumab for adjuvant treatment of resected stage 2b or 2c melanoma (Ta837). Available online at: https://www.nice.org.uk/guidance/ta837/resources/resource-impact-report-pdf-11256975613.
National Institute for Health and Care Excellence (2022g). Resource impact report: pembrolizumab for neoadjuvant and adjuvant treatment of triple-negative early or locally advanced breast cancer (Ta851). Available online at: https://www.nice.org.uk/guidance/ta851/resources/resource-impact-report-pdf-11315579437.
National Institute for Health and Care Excellence (2022h). Nivolumab for adjuvant treatment of invasive urothelial cancer at high risk of recurrence. Available online at: https://www.nice.org.uk/guidance/ta817/documents/committee-papers.
National Institute for Health and Care Excellence (2023). Nivolumab with chemotherapy for neoadjuvant treatment of resectable non-small-cell lung cancer. Available online at: https://www.nice.org.uk/guidance/ta876/documents/committee-papers.
Northern Ireland Cancer Registry (2024a). Malignant melanoma, 2022. Available online at: https://www.qub.ac.uk/research-centres/nicr/CancerInformation/official-statistics/BySite/MalignantMelanoma/.
Northern Ireland Cancer Registry (2024b). Kidney cancer, 2022. Available online at: https://www.qub.ac.uk/research-centres/nicr/CancerInformation/official-statistics/BySite/Kidneycancer/.
Northern Ireland Cancer Registry (2024c). Breast cancer and insitu tumours, 2022. Available online at: https://www.qub.ac.uk/research-centres/nicr/CancerInformation/official-statistics/BySite/Breastcancerandinsitutumours/.
Office for National Statistics (2024a). Estimates of the population for the UK, England, Wales, Scotland, and Northern Ireland. Available online at: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/datasets/populationestimatesforukenglandandwalesscotlandandnorthernireland.
Office for National Statistics (2024b). Population estimates time series dataset. Available online at: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/datasets/populationestimatestimeseriesdataset.
Office for National Statistics (2024c). Hour01 Sa: actual weekly hours worked (seasonally adjusted). Available online at: https://www.ons.gov.uk/employmentandlabourmarket/peopleinwork/earningsandworkinghours/datasets/actualweeklyhoursworkedseasonallyadjustedhour01sa/current.
Office for National Statistics (2025). Waiting times for cancer treatment across the UK. Available online at: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthcaresystem/articles/waitingtimesforcancertreatmentacrosstheuk/2024-08-23#comparability-of-cancer-waiting-times-statistics.
Powles, T., Tomczak, P., Park, S. H., Venugopal, B., Ferguson, T., Symeonides, S. N., et al. (2022). Pembrolizumab versus placebo as post-nephrectomy adjuvant therapy for clear cell renal cell carcinoma (Keynote-564): 30-month Follow-up analysis of a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 23 (9), 1133–1144. doi:10.1016/s1470-2045(22)00487-9
Powles, T., Albiges, L., Bex, A., Comperat, E., Grünwald, V., Kanesvaran, R., et al. (2024). Renal cell carcinoma: esmo clinical practice guideline for diagnosis, treatment and Follow-Up. Ann. Oncol. 35 (8), 692–706. doi:10.1016/j.annonc.2024.05.537
Public Health Scotland (2024). Cancer incidence in Scotland - urinary tract, 2022. Available online at: https://publichealthscotland.scot/publications/cancer-incidence-in-scotland/cancer-incidence-in-scotland-to-december-2022/data-files/#Urinary%20tract.
Public Health Scotland (2021). Cancer incidence in Scotland. Available online at: https://publichealthscotland.scot/publications/cancer-incidence-in-scotland/cancer-incidence-in-scotland-to-december-2021/data-files/#Skin.
Public Health Scotland (2024a). Cancer incidence in Scotland - skin, 2022. Available online at: https://publichealthscotland.scot/publications/cancer-incidence-in-scotland/cancer-incidence-in-scotland-to-december-2022/data-files/#Skin.
Public Health Scotland (2024b). Cancer incidence in Scotland - breast, 2022. Available online at: https://publichealthscotland.scot/publications/cancer-incidence-in-scotland/cancer-incidence-in-scotland-to-december-2022/data-files/#Breast.
Public Health Wales (2024). Welsh cancer intelligence and surveillance unit (wcisu), 2021. Available online at: https://phw.nhs.wales/services-and-teams/welsh-cancer-intelligence-and-surveillance-unit-wcisu/.
Ray, S., Bonthapally, V., Meyer, N. M., Miller, J. D., Bonafede, M. M., and Curkendall, S. M. (2013). Direct medical costs associated with different lines of therapy for colorectal cancer patients. Colorectal Cancer 2 (2), 121–134. doi:10.2217/crc.13.15
Roberts, A., Aguiar-Ibáñez, R., Trennery, C., Kendal, H., Shah, H., Rees, H., et al. (2024). “Understanding the experience of patients with early-stage cancers: a targeted qualitative literature review,” in ISPOR Europe 2024.
Romano, E., Scordo, M., Dusza, S. W., Coit, D. G., and Chapman, P. B. (2010). Site and timing of first relapse in stage III melanoma patients: implications for follow-up guidelines. J. Clin. Oncol. 28 (18), 3042–3047. doi:10.1200/jco.2009.26.2063
Schmid, P., Cortes, J., Dent, R., Pusztai, L., McArthur, H., Kümmel, S., et al. (2022). Event-free survival with pembrolizumab in early triple-negative breast cancer. N. Engl. J. Med. 386 (6), 556–567. doi:10.1056/NEJMoa2112651
Schmid, P., Cortes, J., Dent, R., McArthur, H., Pusztai, L., Kümmel, S., et al. (2024). Overall survival with pembrolizumab in early-stage triple-negative breast cancer. N. Engl. J. Med. 391, 1981–1991. doi:10.1056/NEJMoa2409932
Scottish Government (2023). Cancer strategy 2023 to 2033. Available online at: https://www.gov.scot/publications/cancer-strategy-scotland-2023-2033/.
Scottish Medicines Consortium (2018). Smc2112 - nivolumab as monotherapy for the adjuvant treatment of adults with melanoma with involvement of lymph nodes or metastatic disease who have undergone complete resection. Available online at: https://scottishmedicines.org.uk/medicines-advice/nivolumab-opdivo-full-submission-smc2112/.
Scottish Medicines Consortium (2019). Smc2144 - pembrolizumab (keytruda) as monotherapy for the adjuvant treatment of adults with stage iii melanoma and lymph node involvement who have undergone complete resection. Available online at: https://scottishmedicines.org.uk/medicines-advice/pembrolizumab-keytruda-full-submission-smc2144/.
Scottish Medicines Consortium (2022a). “Smc2479 - pembrolizumab monotherapy is indicated for the adjuvant treatment of adults with renal cell carcinoma at increased risk of recurrence following nephrectomy,” in Or following nephrectomy and resection of metastatic lesions. Available online at: https://scottishmedicines.org.uk/medicines-advice/pembrolizumab-keytruda-rcc-full-smc2479/.
Scottish Medicines Consortium (2022b). Smc2429: nivolumab as monotherapy for the adjuvant treatment of adult patients with completely resected oesophageal or gastro-oesophageal junction cancer who have residual pathologic disease following prior neoadjuvant chemoradiotherapy. Available online at: https://scottishmedicines.org.uk/media/6857/nivolumab-opdivo-final-april-2022-for-website.pdf.
Scottish Medicines Consortium (2023a). Smc2538 - Pembrolizumab (keytruda) in combination with chemotherapy as neoadjuvant treatment, and then continued as monotherapy as adjuvant treatment after surgery for the treatment of adults with locally advanced, or early stage triple negative breast cancer at high risk of recurrence. Available online at: https://scottishmedicines.org.uk/medicines-advice/pembrolizumab-keytruda-na-m-tnbc-full-smc2538/.
Scottish Medicines Consortium (2023b). Smc2526 - Pembrolizumab (keytruda) as monotherapy for the adjuvant treatment of adults and adolescents aged 12 years and older with stage 2b or 2c melanoma and who have undergone complete resection. Available online at: https://scottishmedicines.org.uk/medicines-advice/pembrolizumab-keytruda-full-smc2526/.
Scottish Medicines Consortium (2023c). Smc2503 - Nivolumab as monotherapy for the adjuvant treatment of adults with muscle invasive urothelial carcinoma (miuc) with tumour cell Pd-L1 expression ≥1%, who are at high risk of recurrence after undergoing radical resection of miuc. Available online at: https://scottishmedicines.org.uk/media/7404/nivolumab-opdivo-final-jan-2023-for-website.pdf.
Shelton, J., Zotow, E., Smith, L., Johnson, S. A., Thomson, C. S., Ahmad, A., et al. (2024). 25 year trends in cancer incidence and mortality among adults aged 35-69 years in the Uk, 1993-2018: retrospective secondary analysis. BMJ 384, e076962. doi:10.1136/bmj-2023-076962
van Hout, B., Janssen, M. F., Feng, Y. S., Kohlmann, T., Busschbach, J., Golicki, D., et al. (2012). Interim scoring for the Eq-5d-5l: mapping the Eq-5d-5l to Eq-5d-3l value sets. Value Health 15 (5), 708–715. doi:10.1016/j.jval.2012.02.008
van Leeuwen, M., Husson, O., Alberti, P., Arraras, J. I., Chinot, O. L., Costantini, A., et al. (2018). Understanding the quality of life (qol) issues in survivors of cancer: towards the development of an eortc qol cancer survivorship questionnaire. Health Qual. Life Outcomes 16 (1), 114. doi:10.1186/s12955-018-0920-0
Wakelee, H., Liberman, M., Kato, T., Tsuboi, M., Lee, S. H., Gao, S., et al. (2023). Perioperative pembrolizumab for early-stage non-small-cell lung cancer. N. Engl. J. Med. 389 (6), 491–503. doi:10.1056/NEJMoa2302983
Wales Cancer Network (2023). A cancer improvement plan for nhs Wales 2023-2026. Available online at: https://executive.nhs.wales/functions/networks-and-planning/cancer/cancer-improvement-plan-docs/full-plan/.
Welsh Government (2025). A healthier Wales: long term plan for health and social care. Available online at: https://www.gov.wales/healthier-wales-long-term-plan-health-and-social-care.
Keywords: immunotherapy, immuno-oncology therapy, anti-PD-1, oncology, early-stage cancer, resource planning, productivity
Citation: Burton H, Tan YZ, Greenall S, Neves C, Macdonald N and Aguiar-Ibáñez R (2025) Impact on health outcomes and productive work of adding anti-PD-1 agents to treat early-stage cancers in the United Kingdom: a modelling study. Front. Pharmacol. 16:1613120. doi: 10.3389/fphar.2025.1613120
Received: 23 April 2025; Accepted: 29 September 2025;
Published: 30 October 2025.
Edited by:
Alessandra Cuomo, University of Naples Federico II, ItalyReviewed by:
Thi Thu Phuong Tran, University of Science and Technology of Hanoi (USTH), VietnamFei Song, Affiliated Hospital of Nantong University, China
Copyright © 2025 Burton, Tan, Greenall, Neves, Macdonald and Aguiar-Ibáñez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hannah Burton, aGFubmFoLmJ1cnRvbkBtc2QuY29t