 M. Asunción González-González1
M. Asunción González-González1 M. Aránzazu Pedrosa-Naudín1
M. Aránzazu Pedrosa-Naudín1 Diego Fernández-Lázaro2Isabel Díaz Planelles3
Diego Fernández-Lázaro2Isabel Díaz Planelles3 F. Javier Álvarez4,5,6
F. Javier Álvarez4,5,6 Eduardo Gutiérrez-Abejón1,3,4,5,7*
Eduardo Gutiérrez-Abejón1,3,4,5,7*- 1Pharmacy Directorate, Castilla y León Health Council, Valladolid, Spain
- 2Area of Histology and Neurobiology Research Group, Faculty of Medicine, University of Valladolid, Valladolid, Spain
- 3Facultad de Empresa y Comunicación, Universidad Internacional de la Rioja (UNIR), Logroño, Spain
- 4Laboratory of Pharmacoepidemiological Research in Primary Care, Health Research Institute of Valladolid (IBioVALL), Valladolid, Spain
- 5Area of Pharmacology, Department of Cell Biology, Genetics, Histology and Pharmacology, Faculty of Medicine, University of Valladolid, Valladolid, Spain
- 6CEIm of the Valladolid Health Areas, Valladolid, Spain
- 7Atención Primaria, Área de Salud de Valladolid Este, Valladolid, Spain
This retrospective study aimed to compare the clinical and economic outcomes of single-inhaler triple therapy (SITT) versus multiple-inhaler triple therapy (MITT) in a large cohort of COPD patients. Metrics on adherence, prevalence, and incidence of exacerbations in COPD patients treated with SITT or MITT were analyzed using pharmacy claims data integrated with the Spanish public health database. At the 12-month follow-up, patients in the SITT cohort were significantly more adherent (75.22% vs 70.1%; OR = 1.33), more persistent (64.32% vs 52.4%; HR = 1.56) and had a lower incidence of moderate exacerbations (53.53% vs 64.07%; OR = 0.65) than patients in the MITT cohort. The main predictors associated with lack of persistence were being a naïve patient (HR = 0.55) and moderate exacerbations (HR = 0.85). Furthermore, medication costs were lower for SITT (EUR 909.31 vs EUR 1025.31), demonstrating its cost-effectiveness. Our results suggest that SITT not only may improve adherence and persistence but also contributes to a relevant reduction in the risk of moderate exacerbations. Additionally, SITT offers a more cost-effective alternative for patients with moderate to severe COPD with documented exacerbations, making it a valuable strategy in real-world clinical practice.
1 Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive inflammatory disease characterized by severe respiratory symptoms that can cause irreversible airflow limitation (Torpy et al., 2012). COPD has a global prevalence of 10.3% (Adeloye et al., 2022) and is a leading cause of morbidity and mortality, particularly in patients with exacerbations (Global Initiative for Chronic Obstructive and Lung Disease, 2024). In fact, COPD is expected to become the fourth leading cause of death worldwide by 2030 (Mathers and Loncar, 2006).
Treatment for COPD includes inhaled medications such as long-acting β2-agonists (LABA), long-acting muscarinic antagonists (LAMA), and inhaled corticosteroids (ICS). Medications are selected based on symptoms and risk of exacerbations. For patients with moderate to severe disease who continue to experience exacerbations or poor symptom control on dual therapy, triple therapy (LABA/LAMA/ICS) is recommended (Global Initiative for Chronic Obstructive and Lung Disease, 2024). For these patients, triple therapy has been shown to provide clinical benefits over dual therapy, including improved lung function, lower hospitalization rates (Frith et al., 2015), and reduced mortality (Lipson et al., 2020; Rabe et al., 2020).
In patients with COPD, medication adherence is lower than in other chronic diseases, such as diabetes, depression, or hypertension (Rolnick et al., 2013). According to the literature, the rate of non-adherence to inhaled medications ranges from 22% to 93% (Bhattarai et al., 2020). Adherence to treatment is negatively impacted by the use of different inhalation devices, errors in inhalation technique, and complex dosing regimens (Honkoop et al., 2022). In this sense, non-adherence to inhaled medications for COPD has been associated with a worsening of symptoms, an increased risk of exacerbations, a reduced quality of life, increased hospitalization rates, and higher mortality (Świątoniowska et al., 2020). Additionally, non-adherence to inhaled therapy in patients with COPD is associated with poorer economic outcomes (Cushen et al., 2018).
Triple therapy can be administered as single-inhaler triple therapy (SITT) or multiple-inhaler triple therapy (MITT). In this sense, SITT offers a simplified inhalation regimen (Meynell and Capstick, 2018), improving adherence (Mannino et al., 2022; Lin et al., 2023; Bogart et al., 2024) and persistence (Alcázar-Navarrete et al., 2022; Mannino et al., 2022; Deslee et al., 2023; Lin et al., 2023) while also reducing exacerbations and healthcare resource utilization (Alcázar-Navarrete et al., 2022; Bogart et al., 2024).
This study compared the use of SITT versus MITT in a large cohort of COPD patients. It evaluated treatment adherence and persistence, exacerbation prevention, and analyzed cost-effectiveness, providing new insights into the potential advantages of SITT in a real-world setting.
2 Materials and methods
2.1 Study design and data source
This observational and retrospective cohort study was conducted in Castilla y León, Spain, with a population of 2,327,420 inhabitants (Spanish National Statistics Institute INE, 2024). The study was designed according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) (Von Elm et al., 2008) and the Reporting of Studies Conducted using Observational Routinely collected health Data for Pharmacoepidemiology (RECORD-PE) (Langan et al., 2018) recommendations.
Claims data were obtained from the Pharmaceutical Information System of Castilla y León (CONCYLIA) (Castile and Leon Health Council, 2024). This data source contains primary care prescribing and dispensing data for all patients covered by the Spanish National Health Service, approximately 97% of the population.
Patient data in CONCYLIA are anonymized, so informed consent was not required. This study was approved by the Ethics Committee of the Valladolid Health Areas on October 9, 2024 (reference number PI-24-561-APE).
2.2 Study population
Patients with a diagnosis of COPD according to the International Classification of Diseases-10 (ICD-10) (World Health Organization, 2016), ≥40 years of age, and with at least two prescription refills of SITT or MITT between January 1, 2021, and December 31, 2023, were selected. The index date was defined as the date of SITT or MITT initiation. For MITT, the date considered was the first day with an overlapping supply of all MITT components. Supplementary Table S1 shows the SITTs and MITTs available in Spain.
Patients with less than 12 months of follow-up, inconsistent medication records (date of dispensing not available), or who died during the study period were excluded.
Naive patients were defined as those who had not received inhaled medication (ATC subgroups R03A and R03B) 12 months before study entry.
2.3 Study variables and definitions
Sociodemographic, clinical and economic data were obtained from CONCYLIA. Sociodemographic data included sex, age, institutionalization, healthcare area and socioeconomic level. Clinical data included type of inhaled medication (dose and dosing regimen), concomitant medication (polypharmacy), multiple prescribers and multiple pharmacies (≥3/year), comorbidities, adherence, persistence at 3, 6 and 12 months, mean persistence (in days), persistence rate and moderate exacerbations (frequency and rate). Economic data included medication costs per patient/year and incremental cost-effectiveness ratio (ICER).
A moderate exacerbation is characterized by administering oral corticosteroids and respiratory antibiotics (ATC subgroups J01AA and J01CA) for COPD diagnosis. A recurrence of the same exacerbation was considered if the interval between exacerbations was less than 4 weeks. Severe exacerbations could not be collected as CONCYLIA does not include data on hospital admissions.
Adherence was measured using the Medication Possession Rate (MPR), calculated as the number of days’ supply during a specified follow-up period (365 days) divided by the number of days from the first dispensing to the end of the follow-up period (Andrade et al., 2006). Adherence was classified according to MPR as follows: none (<20), poor (20-49), moderate (50-79) and adherent (≥80) (Krivoy et al., 2016; Pedrosa-Naudín et al., 2022). The percentage of adherent patients was calculated for each type of therapy.
Persistence was defined as the period between the index date and treatment discontinuation. A gap of >60 days between prescription refills for any component of MITT or SITT was considered a discontinuation. The percentage of persistent patients at 3, 6 and 12 months was calculated. The persistence rate for each patient was calculated as the persistent days divided by the follow-up period (365 days). Drug switching (different ATC codes) within the same type of triple therapy (any component of MITT or SITT) was considered as discontinuation. A dose escalation was considered a continuation of treatment. Sensitivity analyses were performed by modifying the allowed gap between prescription refills from 60 to 90 days.
Medication costs were calculated using the prices listed in the official medicines formulary of the Spanish National Health System (Spanish Ministry of Health, 2025). The mean cost per patient/year was calculated for MITT and SITT. The persistence rate was used to measure the effectiveness of ICER calculation (Romagnoli et al., 2020). All costs were reported in euros using 2023 values. The exchange rates of EUR1 = US$1.105 and EUR1 = £0.8683 were based on the European Central Bank rate on December 29, 2023.
2.4 Statistical analysis
Results are presented as means with their standard deviations (SD) or as percentages with their 95% confidence intervals (95% CI), as appropriate. The Kolmogorov-Smirnov test determined the sample’s normality. Student’s t-test for continuous variables and chi-squared test for categorical variables were used to assess differences between groups.
Binary logistic regression was used to analyze the factors influencing adherence. Treatment persistence and duration were analyzed using Kaplan-Meier survival analysis and the log-rank test to compare both groups. The absence of an event (treatment discontinuation) resulted in data censoring. Cox proportional hazards regression was used to assess persistence at 12 months. Univariate and multivariate analyses were performed. All study variables were included in the univariate analysis. Variables with p ≤ 0.05 in the univariate analysis were excluded from the multivariate analysis.
SPSS version 24.0 (SPSS Inc, Chicago, IL) was used for statistical analysis. Statistical significance was determined at p ≤ 0.05.
3 Results
The study population included 7,099 patients in the SITT cohort and 12692 in the MITT cohort. In the MITT cohort, 90% of patients received a LABA/ICS plus LAMA combination (Figure 1). The mean age was 74.71 ± 11.98 years; 63% were male, and 9.5% were naïve patients (Supplementary Table S2).
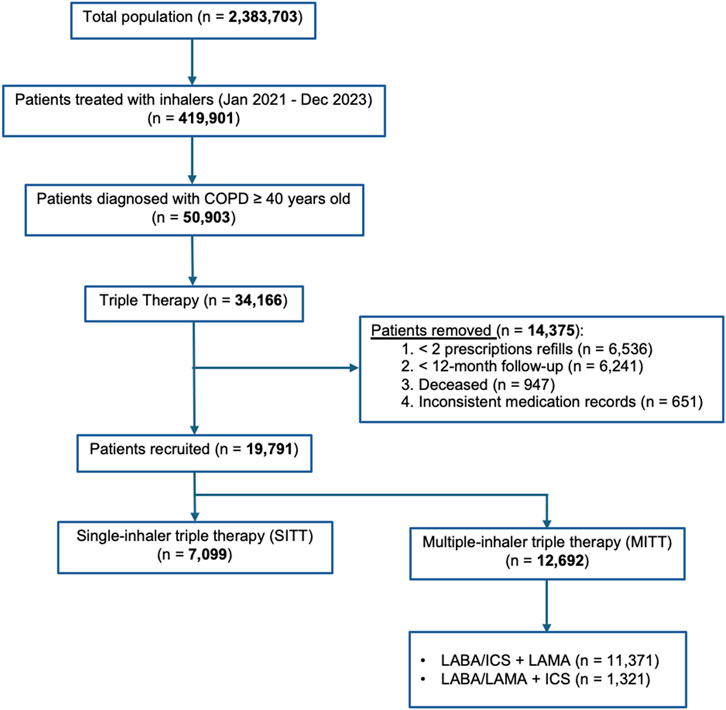
Figure 1. Flowchart of the study population (MITT, multiple-inhaler triple therapy; SITT, single-inhaler triple therapy; LABA, long-acting β2-agonists; LAMA, long-acting muscarinic antagonists; ICS, inhaled corticosteroids).
The incidence of moderate exacerbations was lower in the SITT cohort (53.53%) than in the MITT cohort (64.07%). A decreased risk was also observed in the SITT group (OR = 0.65; p = 0.001) (Table 1). Patients in the SITT cohort required less dose escalation than those in the MITT cohort (6.55% vs 11.84%; p = 0.001) (Supplementary Table S2).
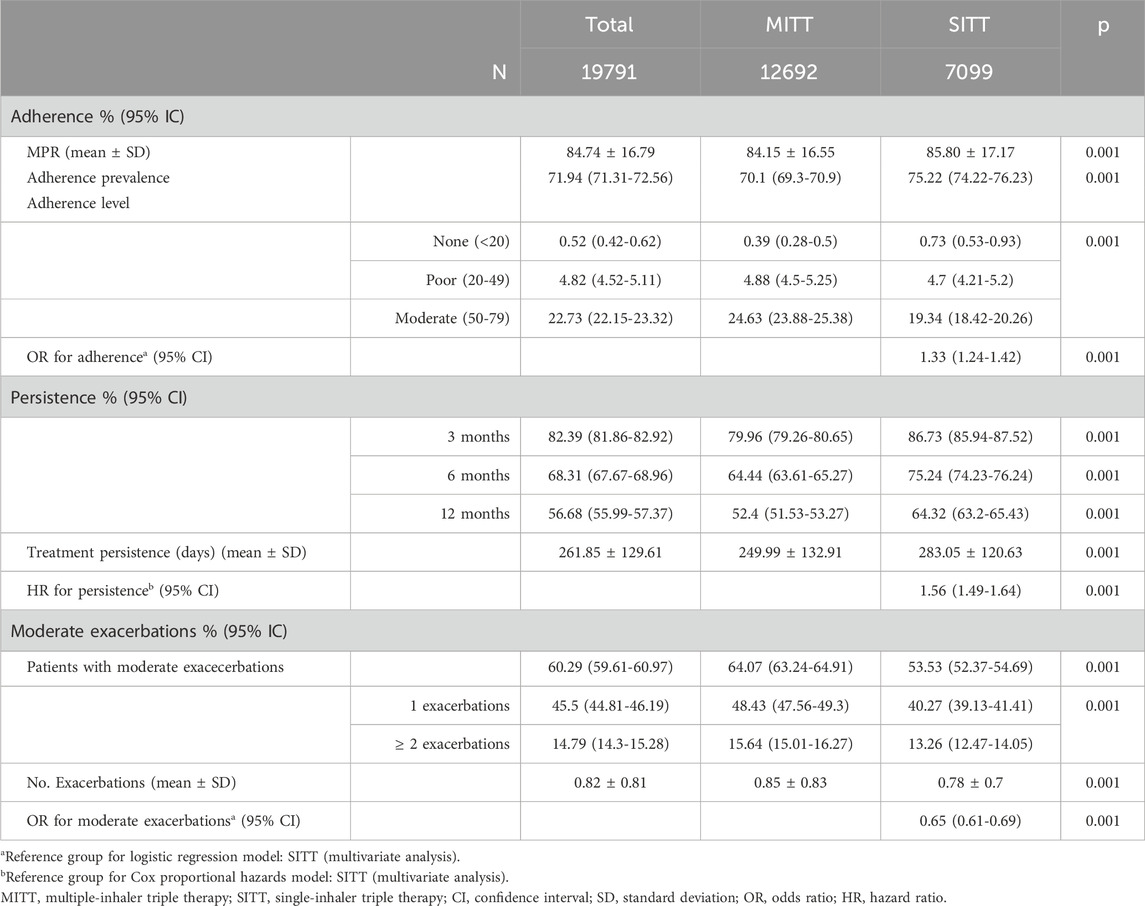
Table 1. Adherence, persistence and moderate exacerbations during 12-month follow-up.
The proportion of adherent patients was higher in the SITT cohort than in the MITT cohort (75.22% vs 70.1%; p = 0.001). Patients in the SITT cohort were more likely to be adherent than those in the MITT cohort (OR = 1.33; p = 0.001) (Table 1).
Patients in the SITT group were more persistent than those in the MITT group at 3 (86.73% vs 79.96%; p = 0.001), 6 (75.24% vs 64.44%; p = 0.001), and 12 months (64.32% vs 52.4%: p = 0.001). Furthermore, mean treatment persistence was higher in the SITT cohort than in the MITT cohort (283.05 ± 120.63 vs 249.99 ± 132.91; p = 0.001) (Table 1; Figure 2).
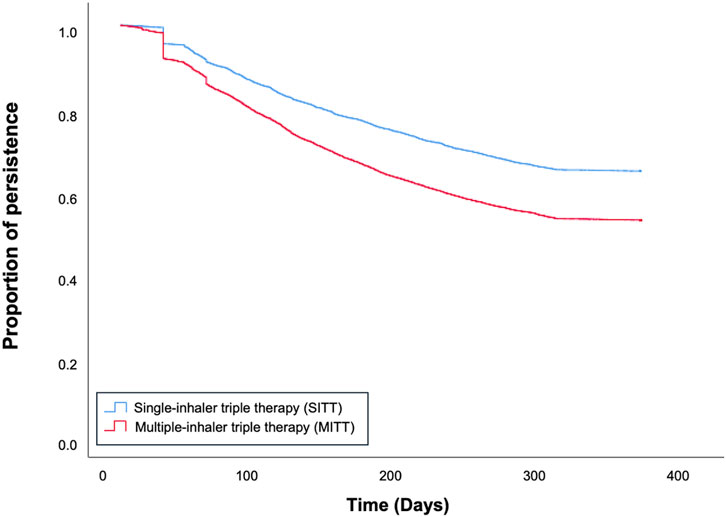
Figure 2. Kaplan-Meier curve for treatment persistence in patients with COPD on single-inhaler triple therapy (SITT) and multiple-inhaler triple therapy (MITT) in Spain.
At the 12-month follow-up, persistence was favored in the SITT cohort (HR = 1.56; p = 0.001) (Table 1). Modifying the gap between prescription refills from 60 to 90 days had comparable results (Supplementary Table S3).
Being a naïve patient was associated with a lack of persistence (HR = 0.55; p = 0.001). Only 46.63% and 30.65% of naïve patients in the SITT and MITT cohorts were persistent, with mean treatment persistence decreasing to 237.12 ± 131.77 and 188.74 ± 132.45 days, respectively. Moderate exacerbations were strongly associated with a lack of persistence (HR = 0.85; p = 0.001). Other associated factors were female sex, institutionalization, multiple prescribers, polypharmacy, and diagnoses of asthma and depression (Table 2; Supplementary Figure S1).

Table 2. Predictors of persistence in patients with COPD on triple inhaled therapy in Spain.
Persistence rates were 0.78 ± 0.33 for the SITT cohort and 0.68 ± 0.36 for the MITT cohort. The mean costs of SITT and MITT were EUR 909.31 ± 13.86 and EUR 1,025.31 ± 96.05 per patient per year, respectively. The ICER of SITT versus MITT ranged from EUR −1,160 to EUR −1,450 per persistence rate, depending on the gap between prescription refills (60 or 90 days).
4 Discussion
Our findings show that patients in the SITT cohort were more adherent than those in the MITT cohort (75% vs 70%). Furthermore, patients in the SITT group showed greater persistence, with a rate more than 10% higher after 12 months of treatment. The main predisposing factors for lack of persistence were identified as being a naive patient, having multiple prescribers, being female, and experiencing moderate exacerbations. Additionally, moderate exacerbations occurred 10% more frequently among patients in the MITT cohort.
Our patients’ baseline characteristics are like those in other European (Alcázar-Navarrete et al., 2022; Deslee et al., 2023), American (Mannino et al., 2022; Bogart et al., 2024), and Chinese (Lin et al., 2023) studies. The presence of almost 10% of naïve patients is relevant and similar to another European study (Deslee et al., 2023). However, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) report (Global Initiative for Chronic Obstructive and Lung Disease, 2024) recommends, albeit with reservations, triple therapy for naïve patients with a blood eosinophil count ≥300 cells/μl. As in other observational studies (Alcázar-Navarrete et al., 2022; Mannino et al., 2022; Deslee et al., 2023), patients with a concomitant diagnosis of asthma were not excluded, in contrast to other more restrictive studies (Lin et al., 2023).
Previous studies show higher adherence in the SITT group than in the MITT group (Mannino et al., 2022; Lin et al., 2023; Bogart et al., 2024), except for a French study (Deslee et al., 2023), although its results are not significant. For the SITT cohort, results ranged from 26% (Bogart et al., 2024) to 76.8% (Mannino et al., 2022) of adherent patients, and for the MITT cohort, from 13.1% (Bogart et al., 2024) to 65.5% (Lin et al., 2023). Our results are like the maximum adherence values, although the comparison should be made cautiously because the other studies used the proportion of days covered (PDC) (Mannino et al., 2022; Lin et al., 2023; Bogart et al., 2024) as a measure of adherence instead of MPR. As in other studies (Alcázar-Navarrete et al., 2022; Mannino et al., 2022; Deslee et al., 2023; Lin et al., 2023; Bogart et al., 2024), higher persistence was observed in the SITT cohort than in the MITT cohort. Our findings were like those of other studies that defined discontinuation with a gap between prescription refills of 60 days (Deslee et al., 2023; Lin et al., 2023; Bogart et al., 2024) and higher than those that used a gap of 30 days (Mannino et al., 2022).
The incidence and risk of moderate exacerbations were lower in the SITT cohort than in the MITT cohort, consistent with other published results (Alcázar-Navarrete et al., 2022; Lin et al., 2023). In addition, our results showed a direct relationship between moderate exacerbations and lack of persistence. On the other hand, this result may have been influenced by the higher proportion of patients with concomitant asthma in the MITT group than in the SITT group.
Additionally, the MITT cohort required almost twice dose escalation as the SITT cohort. A greater need for dose escalation, lower persistence, and a higher incidence of moderate exacerbations may suggest that the MITT cohort has lower treatment efficacy than the SITT cohort.
Being a naïve patient was associated with a 45% decrease in persistence, reducing the mean treatment persistence by 50 days in both cohorts. Other predictors of decreased persistence were a diagnosis of asthma (8%) and depression (9%). Another study looking at the same predictors (Deslee et al., 2023) found only depression to be significant.
As in other studies (Alcázar-Navarrete et al., 2022; Bogart et al., 2024), medication costs were lower in the SITT cohort than in the MITT cohort. The cost-effectiveness analysis results showed that SIIT was the dominant option. Similar results were found in a systematic review evaluating the cost-effectiveness of single versus multiple inhalers in asthma and COPD (Zhang et al., 2020). However, our region has more patients with MITT than with SITT. This may be because SITTs have been on the market for a shorter time than MITTs, and changes in prescribing habits occur gradually.
The limitations of our study are similar to those of other observational studies (Alcázar-Navarrete et al., 2022; Mannino et al., 2022; Deslee et al., 2023; Lin et al., 2023; Bogart et al., 2024). As in other studies published by our group (Pedrosa-Naudín et al., 2022; Gutiérrez-Abejón et al., 2023; 2024; Martín-Fernández et al., 2025), we assumed that dispensing approximates consumption. As in previous studies (Martín-Fernández et al., 2025), we excluded patients who had fewer than two prescription refills. This may be a confounding factor because not filling more prescriptions could be related to the perception that the treatment is ineffective. In this case, the number of patients excluded from each cohort was similar: 3,172 from the MITT group and 3,364 from the SITT group. Moderate exacerbations were extrapolated from pharmacy claims without physician confirmation. Due to a lack of access to hospital admission data, severe exacerbations could not be assessed. Finally, only drug-related costs were included in the cost-effectiveness analysis.
In conclusion, the SITT cohort showed a 33% increase in adherence, a 56% improvement in persistence, and a 35% reduction in the risk of moderate exacerbations compared to the MITT cohort. In addition, moderate exacerbations were associated with a 15% reduction in the likelihood of persistence. Lastly, this study confirms that SITT is the most cost-effective treatment for patients with moderate to severe COPD and a history of exacerbations. These findings support the SITT initiation, especially for naïve patients, offering a practical and effective strategy for optimizing COPD management.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: Restrictions apply to the availability of these data. Data were obtained from regional health authorities (Gerencia Regional de Salud (GRS)) and may be requested fromY29uY2llcnRvZmNvQHNhbHVkY2FzdGlsbGF5bGVvbi5lcw==. Requests to access these datasets should be directed toY29uY2llcnRvZmNvQHNhbHVkY2FzdGlsbGF5bGVvbi5lcw==.
Ethics statement
The studies involving humans were approved by the Valladolid Health Area Ethics Committee on October 9, 2024 (reference number PI-24-561-APE). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because in accordance with the national legislation and institutional requirements.
Author contributions
MG-G: Methodology, Conceptualization, Investigation, Writing – review and editing. MP-N: Writing – review and editing, Validation, Formal Analysis, Conceptualization, Investigation, Software. DF-L: Writing – review and editing, Formal Analysis, Methodology, Investigation. IP: Methodology, Writing – review and editing, Investigation. FÁ: Conceptualization, Writing – review and editing, Supervision, Writing – original draft, Validation, Visualization, Methodology. EG-A: Funding acquisition, Writing – review and editing, Methodology, Software, Formal Analysis, Project administration, Data curation, Writing – original draft, Resources, Conceptualization.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by Gerencia Regional de Salud de Castilla y León, Spain, grant number GRS 2778/C/23. AstraZeneca funded the medical writing adaptation services and article processing costs associated with this publication. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the funders and collaborating institutions.
Acknowledgments
The authors thank the Pharmacy Directorate (Gerencia Regional de Salud de Castilla y León) for access to the Concylia database.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2025.1642470/full#supplementary-material
References
Adeloye, D., Song, P., Zhu, Y., Campbell, H., Sheikh, A., Rudan, I., et al. (2022). Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir. Med. 10, 447–458. doi:10.1016/S2213-2600(21)00511-7
Alcázar-Navarrete, B., Jamart, L., Sánchez-Covisa, J., Juárez, M., Graefenhain, R., and Sicras-Mainar, A. (2022). Clinical characteristics, treatment persistence, and outcomes among patients with COPD treated with Single- or multiple-inhaler triple therapy: a retrospective analysis in Spain. Chest 162, 1017–1029. doi:10.1016/j.chest.2022.06.033
Andrade, S. E., Kahler, K. H., Frech, F., and Chan, K. A. (2006). Methods for evaluation of medication adherence and persistence using automated databases. Pharmacoepidemiol Drug Saf. 15, 565–574. doi:10.1002/pds.1230
Bhattarai, B., Walpola, R., Mey, A., Anoopkumar-Dukie, S., and Khan, S. (2020). Barriers and strategies for improving medication adherence among people living with COPD: a systematic review. Respir. Care 65, 1738–1750. doi:10.4187/respcare.07355
Bogart, M., Bengtson, L. G. S., Johnson, M. G., Bunner, S. H., Gronroos, N. N., and DiRocco, K. K. (2024). Outcomes following initiation of triple therapy with fluticasone furoate/umeclidinium/vilanterol versus multiple-inhaler triple therapy among medicare advantage with part D beneficiaries and those commercially enrolled for health care insurance in the United States. Int. J. Chron. Obstruct Pulmon Dis. 19, 97–110. doi:10.2147/COPD.S424497
Castile and Leon Health Council (2024). CONCYLIA, the pharmacy information System of Castile and Leon. Available online at: https://www.saludcastillayleon.es/portalmedicamento/es/indicadores-informes/concylia (Accessed November 29, 2023).
Cushen, B., Sulaiman, I., Greene, G., MacHale, E., Mokoka, M., Reilly, R. B., et al. (2018). The clinical impact of different adherence behaviors in patients with severe chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 197, 1630–1633. doi:10.1164/rccm.201712-2469LE
Deslee, G., Fabry-Vendrand, C., Poccardi, N., Thabut, G., Eteve Pitsaer, C., Coriat, A., et al. (2023). Use and persistence of single and multiple inhaler triple therapy prescribed for patients with COPD in France: a retrospective study on THIN database (OPTI study). BMJ Open Respir. Res. 10, e001585. doi:10.1136/bmjresp-2022-001585
Frith, P. A., Thompson, P. J., Ratnavadivel, R., Chang, C. L., Bremner, P., Day, P., et al. (2015). Glycopyrronium once-daily significantly improves lung function and health status when combined with salmeterol/fluticasone in patients with COPD: the GLISTEN study, a randomised controlled trial. Thorax 70, 519–527. doi:10.1136/thoraxjnl-2014-206670
Global Initiative for Chronic Obstructive and Lung Disease (2024). Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease. Glob. Initiative Chronic Obstr. Lung Dis. - GOLD. Available online at: https://goldcopd.org/2024-gold-report/(Accessed October 23, 2024).
Gutiérrez-Abejón, E., Pedrosa-Naudín, M. A., Fernández-Lázaro, D., and Alvarez, F. J. (2023). Medication economic burden of antidepressant non-adherence in Spain. Front. Pharmacol. 14, 1266034. doi:10.3389/fphar.2023.1266034
Gutiérrez-Abejón, E., Pedrosa-Naudín, M. A., Fernández-Lázaro, D., Díaz Planelles, I., and Álvarez, F. J. (2024). Non-adherence to antidementia medications and associated factors: a study of Spanish population-based registry data. Front. Pharmacol. 15, 1425442. doi:10.3389/fphar.2024.1425442
Honkoop, P., Usmani, O., and Bonini, M. (2022). The current and future role of technology in respiratory care. Pulm. Ther. 8, 167–179. doi:10.1007/s41030-022-00191-y
Krivoy, A., Balicer, R. D., Feldman, B., Hoshen, M., Zalsman, G., Weizman, A., et al. (2016). Adherence to antidepressants is associated with lower mortality: a 4-year population-based cohort study. J. Clin. Psychiatry 77, e566–e572. doi:10.4088/JCP.14m09531
Langan, S. M., Schmidt, S. A., Wing, K., Ehrenstein, V., Nicholls, S. G., Filion, K. B., et al. (2018). The reporting of studies conducted using observational routinely collected health data statement for pharmacoepidemiology (RECORD-PE). BMJ 363, k3532. doi:10.1136/bmj.k3532
Lin, L., Liu, C., Cheng, W., Song, Q., Zeng, Y., Li, X., et al. (2023). Comparison of treatment persistence, adherence, and risk of exacerbation in patients with COPD treated with single-inhaler versus multiple-inhaler triple therapy: a prospective observational study in China. Front. Pharmacol. 14, 1147985. doi:10.3389/fphar.2023.1147985
Lipson, D. A., Crim, C., Criner, G. J., Day, N. C., Dransfield, M. T., Halpin, D. M. G., et al. (2020). Reduction in all-cause mortality with fluticasone furoate/umeclidinium/vilanterol in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 201, 1508–1516. doi:10.1164/rccm.201911-2207OC
Mannino, D., Bogart, M., Wu, B., Germain, G., Laliberté, F., MacKnight, S. D., et al. (2022). Adherence and persistence to once-daily single-inhaler versus multiple-inhaler triple therapy among patients with chronic obstructive pulmonary disease in the USA: a real-world study. Respir. Med. 197, 106807. doi:10.1016/j.rmed.2022.106807
Martín-Fernández, M., González-González, M. A., Pedrosa-Naudín, M. A., Fernández-Lázaro, D., Álvarez, F. J., and Gutiérrez-Abejón, E. (2025). Newly started versus previously treated Statin patients: a retrospective cohort study comparing adherence and persistence with reference to cardiovascular prevention. Pharm. (Basel) 18, 634. doi:10.3390/ph18050634
Mathers, C. D., and Loncar, D. (2006). Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 3, e442. doi:10.1371/journal.pmed.0030442
Meynell, H., and Capstick, T. (2018). Role of dual and triple fixed-dose combination inhalers in the treatment of chronic obstructive pulmonary disease. Clin. Pharm. 10. doi:10.1211/PJ.2018.20205647
Pedrosa-Naudín, M. A., Gutiérrez-Abejón, E., Herrera-Gómez, F., Fernández-Lázaro, D., and Álvarez, F. J. (2022). Non-adherence to antidepressant treatment and related factors in a region of Spain: a population-based registry study. Pharmaceutics 14, 2696. doi:10.3390/pharmaceutics14122696
Rabe, K. F., Martinez, F. J., Ferguson, G. T., Wang, C., Singh, D., Wedzicha, J. A., et al. (2020). Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N. Engl. J. Med. 383, 35–48. doi:10.1056/NEJMoa1916046
Rolnick, S. J., Pawloski, P. A., Hedblom, B. D., Asche, S. E., and Bruzek, R. J. (2013). Patient characteristics associated with medication adherence. Clin. Med. Res. 11, 54–65. doi:10.3121/cmr.2013.1113
Romagnoli, A., Santoleri, F., and Costantini, A. (2020). Adherence and persistence analysis after three years in real-life of inhalation therapies used in the treatment of COPD. Curr. Med. Res. Opin. 36, 2055–2061. doi:10.1080/03007995.2020.1841617
Spanish Ministry of Health (2025). Information on products included in the Spanish national health System’s pharmaceutical benefits. Available online at: https://www.sanidad.gob.es/en/profesionales/nomenclator.do (Accessed June 5, 2025).
Spanish National Statistics Institute (INE) (2024). Demographics and population. Available online at: https://www.ine.es/jaxiT3/Datos.htm?t=2915 (Accessed April 8, 2024).
Świątoniowska, N., Chabowski, M., Polański, J., Mazur, G., and Jankowska-Polańska, B. (2020). Adherence to therapy in chronic obstructive pulmonary disease: a systematic review. Adv. Exp. Med. Biol. 1271, 37–47. doi:10.1007/5584_2019_477
Torpy, J. M., Goodman, D. M., Burke, A. E., and Livingston, E. H. (2012). JAMA patient page. Chronic obstructive pulmonary disease. JAMA 308, 1281. doi:10.1001/jama.2012.12362
von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gøtzsche, P. C., Vandenbroucke, J. P., et al. (2008). The strengthening the reporting of observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J. Clin. Epidemiol. 61, 344–349. doi:10.1016/j.jclinepi.2007.11.008
World Health Organization (2016). International statistical classification of diseases and related health problems, ICD-10 volume 2. Available online at: https://www.who.int/publications/m/item/international-statistical-classification-of-diseases-and-related-health-problems---volume-2 (Accessed December 28, 2023).
Keywords: chronic obstructive pulmonary disease, multiple-inhaler triple therapy, single-inhaler triple therapy, adherence, persistence, exacerbations
Citation: González-González MA, Pedrosa-Naudín MA, Fernández-Lázaro D, Planelles ID, Álvarez FJ and Gutiérrez-Abejón E (2025) Single-versus multiple-inhaler triple therapy in patients with COPD in Spain: a retrospective cohort study comparing adherence, persistence, risk of exacerbations and economic outcomes. Front. Pharmacol. 16:1642470. doi: 10.3389/fphar.2025.1642470
Received: 06 June 2025; Accepted: 01 September 2025;
Published: 19 September 2025.
Edited by:
Roberto Giovanni Carbone, University of Genoa, ItalyReviewed by:
Ranjit Sivanandham, The MetroHealth System, United StatesSara Shahid, Lahore University of Biological and Applied Sciences, Pakistan
Copyright © 2025 González-González, Pedrosa-Naudín, Fernández-Lázaro, Planelles, Álvarez and Gutiérrez-Abejón. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eduardo Gutiérrez-Abejón, ZWd1dGllcnJlemFAc2FsdWRjYXN0aWxsYXlsZW9uLmVz