 Gilberto Sousa Alves1,2*
Gilberto Sousa Alves1,2* Maria Eduarda Casali3André Barciela Veras4
Maria Eduarda Casali3André Barciela Veras4 Carolina Gomes Carrilho3Eriko Bruno Costa1Valeska Marinho Rodrigues2,5
Carolina Gomes Carrilho3Eriko Bruno Costa1Valeska Marinho Rodrigues2,5 Marcia Cristina Nascimento Dourado2,5
Marcia Cristina Nascimento Dourado2,5- 1Translational Psychiatry Research Group, Federal University of Maranhão, São Luís, Brazil
- 2Post Graduation in Psychiatry and Mental Health (PROPSAM), Institute of Psychiatry, UFRJ, Rio de Janeiro, Brazil
- 3Dom Bosco Catholic University (UCDB), Campo Grande, Brazil
- 4Medical School, State University of Mato Grosso do Sul (UEMS), Dourados, Brazil
- 5Center for Alzheimer’s Disease, Institute of Psychiatry, Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, Brazil
Background: Impacts of social isolation measures imposed by COVID-19 Pandemic on mental health and quality of life of older adults living with dementia and their caregivers remain unexplored. Studies have shown that psychoeducational and psychosocial interventions can manage behavioral and psychological symptoms in dementia (BPSD) and reduce the emotional burden on family members when applied in home-setting scenarios.
Method: a comprehensive systematic review of useful interventions for easing the BPSD burden in patients with dementia (PwD) and their caregivers in the context of COVID-19 quarantine was performed from January 2010 to March 2020.
Results: From a total of 187 articles retrieved from electronic databases (MEDLINE, LILACS, Cochrane and SCOPUS), 43 studies were eligible for this review. Most of the psychosocial and psychoeducational interventions described were person-centered strategies based on the cognitive-behavioral approach or informational tools to enhance care providers’ knowledge of dementia. Most studies achieved successful results in handling BPSD and mood-anxiety symptoms of care providers, contributing to an overall improvement in dyad life quality.
Conclusion: Evidence from the last few years suggest that low-cost techniques, tailored to the dyad well-being, with increasing use of technology through friendly online platforms and application robots, can be an alternative to conventional assistance during COVID-19 Pandemic. Nevertheless, the world’s current experience regarding the duration of the COVID-19 Pandemic and its effects on the cognition, behavior, and life quality of PwD will demand research on preventive and protective factors of dementia and the pursue of efficient interventions in different scenarios.
Introduction
Dementia is a progressive syndrome and the associated functional decline inevitably leads to increasing dependence on others in different activities of daily living (1, 2). Patients with dementia (PwD) represent a heterogeneous group regarding diagnosis, stages of the disease, and level of functional decline. Behavioral and psychological symptoms in dementia (BPSD) are present at some point in almost 90% of PwD (3, 4), which is related to increased morbidity and mortality, caregiver burden, early institutionalization, and reduced survival (5, 6). One recent estimation of the global costs of dementia in Brazil cited values of US$1,012.35 (7). Although the economic and social impact remains to be further understood, the elevated healthcare costs resulting from the use of higher doses of psychoactive medications and falls, treatment dropouts, and wandering have all been thoroughly described in the literature (8).
A large number of PwD, mostly in moderate and advanced stages, require constant supervision (9). Since they are at the forefront of care, caregivers—family members and professionals, have a strategic role in the PwD quality of life and survival. A model of coping with stress is embedded in multiple stress-based problems, such as lack of social interactions, financial difficulties, frustration, anxiety, reduction of leisure activities, and concerns about the future (10, 11). Therefore, caregivers need professional assistance to cope with dementia, as they are a group particularly vulnerable to emotional burden, depression, and physical exhaustion. (10, 12).
Also, the COVID-19 Pandemic, which started in September of 2019 in Wuhan, the capital city of Hubei Province (China), had a crucial psychosocial impact on the mental health of older adults with pre-diagnosed dementia, especially after social isolation measures such as lock-down, and is still an unexplored topic. Despite dementia’s heterogeneity and psychoeducation measures, which are defined as a set of information provided by healthcare professionals that help in understanding the biological and social phenomena involved in the illness process and contribute to delivering higher-quality care in a home setting (13).
Measures directed to the dyad—caregiver and PwD—at home can be of a psychoeducational or psychosocial nature. Psychosocial interventions, defined as a set of techniques developed to use cognitive and behavioral mechanisms to promote the caregiver and PwD psychological well-being, can be associated with psychoeducation. Evidence shows that both measures, when aimed at understanding dementia and managing behavioral changes in a home setting and social isolation, can benefit PwD therapeutically, minimizing complications and reducing the emotional burden on family members during the isolation period, when social contact with specialized services is limited.
Furthermore, evidence has shown that PwD wish to participate in interventions that enhance their well-being, confidence, health, social participation, and human rights. This point highlights a need for improvements in psychosocial research to capture these outcomes (14). The present article aims to discuss psychoeducation measures and brief psychosocial interventions designed in a home setting, based on an integrative literature review, to manage behavioral changes in individuals with dementia and social isolation, which may be useful for the COVID-19 pandemic and post-pandemic assistance.
Methods
An integrative literature review was conducted to gather and summarize the evidence available from original articles for the issue investigated. This integrative review study included six stages: 1 – formulation of the central research question (theme identification); Step 2 – definition of inclusion and exclusion criteria and literature search; Step 3 – categorization of primary studies (description of data to be extracted from the selected studies); Step 4 – assessment of the studies included; Step 5 – interpretation of results; 6 – knowledge synthesis of the results obtained from the studies assessed (15–17).
The central research question was formulated using the PVO method, where P is the study population (adults over 60 years of age with a diagnosis of dementia); V is the variable (psychoeducation measures), and O is the outcome (BPSD management).
Our review’s guiding question was: “Which psychoeducational and psychosocial measures are used for easing the BPSD burden in both PwD and their caregivers in the home setting?” The inclusion criteria were English language articles in the electronic databases (Medical Literature Analysis and Retrieval System Online (MEDLINE), Latin American and Caribbean Health Sciences Literature (LILACS), Cochrane, and SCOPUS); cross-sectional or prospective design; outpatient or population-based samples of adults over 60 years of age with irreversible and progressive dementia (e.g., Alzheimer’s disease, vascular dementia; Parkinson’s dementia); and non-pharmacological treatment through psychoeducation and psychosocial measures. The exclusion criteria were guidelines, systematic reviews, institutional protocols, psychoeducation measurements in other psychiatric or neurological conditions, and psychosocial intervention in hospitalized patients. The publications were individually searched and selected by two investigators during March and April 2020 and included papers from January 2010–April 2020.
The Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines (18) were used as a basis for the search and selection of studies (Supplement Material). A search strategy was created to conduct searches in the following databases: MEDLINE via PubMed from the US National Library of Medicine, LILACS, Cochrane, and SCOPUS with no time restriction. To expand our search, we chose to use a natural controlled language. The following descriptors (bold), synonyms, natural language, and Boolean operators were used to cross-check the databases: MEDLINE (Medical Subject Headings [MeSH]: search strategy – (aged or elderly or old or elder) and (non-pharmacological treatment or psychosocial treatment or ”) and (“Alzheimer disease” or Alzheimer’s) and (“dementia” or “cognitive dysfunction”).
Two investigators independently conducted the literature search and data extraction to minimize selection bias (misinterpretation of results and study design), and any discrepancies were resolved by consensus. We also performed a qualitative rating (see Supplement Material) of all selected studies through the Newcastle-Ottawa-Scale score (http://www.ohri.ca/programs/clinical_epidemiology/nosgen.pdf).
Results
The study selection process, according to the PRISMA guidelines, is illustrated in Supplement Material flow chart. A total of 187 articles were retrieved and read, and from these, only 43 studies were considered eligible for our review. The selected studies are described in Tables 1, 2. The sample sizes ranged from 6 to 555 participants. They were conducted in 16 countries, with the most substantial proportion nested in Europe (n = 23, 53.49%) and United States (n = 10, 23.26%). In contrast, the same ratio (n = 9, 20.93%) was found in Eastern Asia or Oceania, and only one was in Africa (2.32%). No studies were found for Latin America.
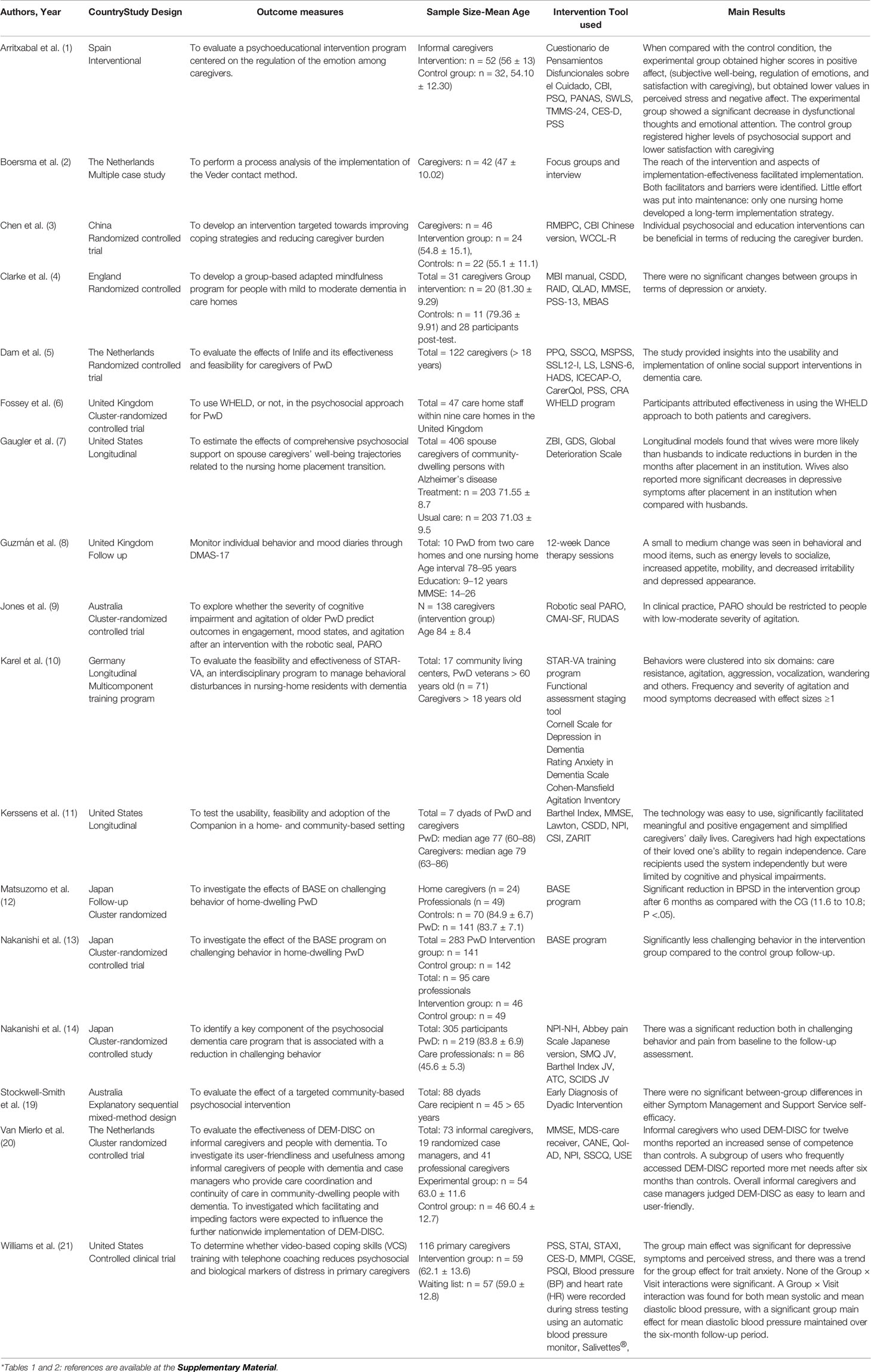
Table 1 Characteristics of Intervention studies with patients with dementia and caregivers*.
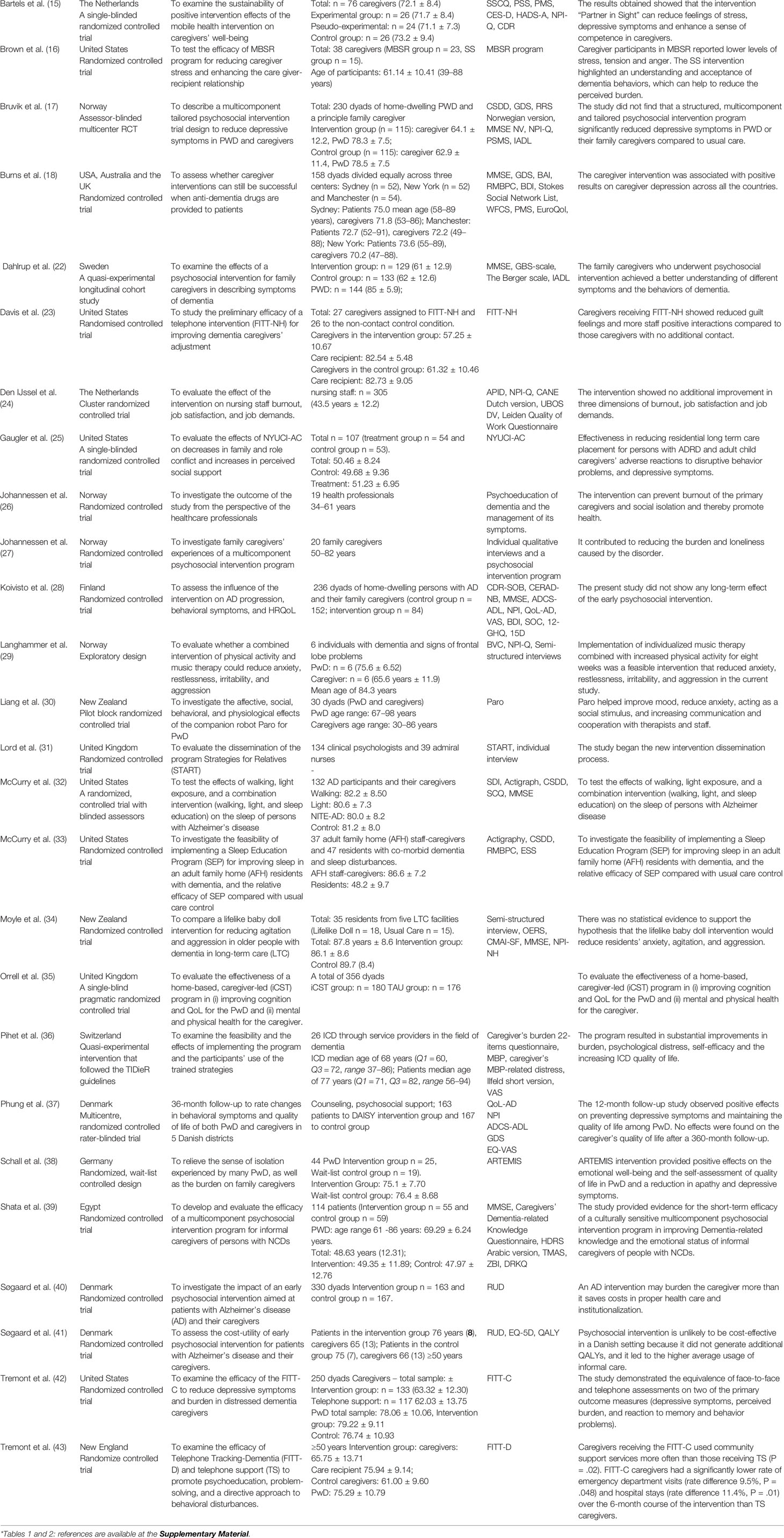
Table 2 Characteristics of Intervention studies with patients with dementia and caregivers*.
Almost all studies (n = 42, 97.67%) employed psychosocial and-or psychoeducational strategies addressing the dyad, and only one used cognitive-behavioral intervention (2.33%) for the caregiver solely (Table 1). The majority of investigations (n = 33, 76.74%) were based on randomized controlled trials, as following: 1 interventional study design (2.22%), 1 multiple case (2.22%), 6 longitudinal studies (13.95%), 1 explanatory sequential mixed-method design (2.22%), 1 exploratory design (2.22%), 2 quasi-experimental interventions (4.44%), and 1 controlled clinical trial alternately assigned (2.22%). A few studies used more than one design method.
The studies included in our review evaluated participants with distinct levels of dementia, being most of them (n = 34, 79.07%) focused on mild-moderate dementia. In comparison, 8 (18.60%) other studies investigated mild Alzheimer’s disease, and only 1 (2.32%) moderate-severe dementia. Cognitive and functional scores were provided only by a few studies (n = 10, 23.26%). Most caregivers were familiar or informal caregivers (n = 30, 69.76%), albeit professional care providers could be found in the remaining studies (n = 13, 30.23%). For most of the compelled studies, the primary outcome result was evaluating and reducing behavioral disturbances in PwD, such as agitation, restlessness, anxiety (n = 17, 39.53%), including specific interventions for decreasing sleep disturbances (n = 2, 4.65%). Concerning caregivers, the most important outcome was the reduction of burden and stress (n = 21, 48.84%), including the attenuation of depression or other mood symptoms (n = 4, 9.30%). Also, studies aimed at evaluating caregiver wellbeing, quality of life and satisfaction of with caregiving (n = 6, 13.95%); some outcome measures comprised the enhancement of knowledge on dementia through psychoeducation and the development of a sense of competence in dealing with BPSD (n = 9, 20.93%) and reducing guilty and adverse reactions toward PwD (n = 2, 4.65%). Finally, other studies had primary goals evaluating online psychosocial support, including robot-guided psychosocial intervention (n = 3, 6.98%).
The primary interventions are summarized in the following topics.
An Overview of the Psychosocial and Psychoeducational Interventions
Most of the studies of psychosocial and psychoeducational interventions for the field of dementia use an umbrella of techniques, most of them based on cognitive-behavioral therapy (CBT) (19) or a combination of psychotherapy and essential information on dementia (20). Caregivers were generally encouraged to share feelings about dementia such as guilt, loneliness, worry and sadness (20). The majority of studies carried out interventions for dyad (15). Caregivers may learn from CBT to develop self-monitoring of depressive or anxiety symptoms or help PwD do so (4). One study, for instance, employed CBT in PwD at moderate stages (16). The Coping with Caregiver model – CCM (5) articulates cognition and behavior with negative affective states and teaches cognitive-behavioral mood management skills. In one investigation consisting of a 14 h training program with CCM, the intervention group exhibited significantly less depressive symptoms and experienced lower caregiver burden than the control group at the end of study (5). The Residential Care Transition Module (RCTM) consists of a six-session, 4-month psychosocial intervention designed to help families manage their emotional and psychological distress following residential care placement of a cognitively impaired relative (17). Cognitive Stimulation Therapy (CST) is a psychosocial group intervention recommended by the UK NICE guidelines that have shown to improve cognition and quality of life (18). There is some evidence showing the efficacy of CST in apathy and depression-dysphoria (21). Multisensory stimulation (MS) comprises a set of sensory stimuli (visual, auditory, tactile) and controlled environment, following a schedule of reinforcement and has been studied in AD, Huntington’s disease (15). Mindfulness-based intervention (MBI) is based on paying attention in a particular way, i.e., at the present moment and non-judgmentally to enhance emotional regulation (22, 23). This meditation method focuses mainly on breath or body and open monitoring of the whole cognitive-affective field (22). One single-blind intervention conducted by Churcher Clarke and colleagues included a 10-session MBI with mild and moderate dementia and found a medium effect size improvement in overall quality of life, but no significant changes in depression or anxiety symptoms (22).
Main Goals of Interventions
Overall, most psychoeducational and psychosocial interventions aimed to enhance care providers’ knowledge about the required skills of caregiving and, ultimately, to reduce dementia sufferers’ illness deterioration and institutionalization (24, 25). Most studies employed personalized and person-centered strategies (26, 27) designed to fulfill the needs, characteristics and preferences of both PwD and their caregivers (28). As an example, the Person-centered care (PCC), widely recognized concept in dementia research and care and the Dementia Care Mapping (DCM), a method for implementing PCC (29).
Some strategies seek to promote the general well-being and life quality of the dyad (17, 20), such as the case of the Dealing Well with Dementia project, which used the “Dignity Therapy” (30), the Family Intervention (FITT-C) (31) or the Northern Manhattan Caregiver Intervention Project, which addressed the relief of stress symptoms in Hispanic spouses of PwD in NYC (32). In Denmark, a large multicentric study (DAISY) evaluated the effectiveness of a program for outpatients with Alzheimer’s disease in 12 months (33, 34). The therapy was based on measures of education, counseling and support for family members (33). Raeanne and colleagues (35) evaluated the efficacy of the Pleasant Events Program (PEP), a 6-week Behavioral Activation intervention designed to reduce CVD risk and depressive symptoms in caregivers. According to the authors, the group receiving PEP intervention had significant reductions in depressive symptoms (p = .039) and negative affect (p = .021) from pre- to post-treatment (35).
Other examples included multiple activities, such as the Pleasant Events Program, in which a protocol comprised physical exercise, occupational therapy and support intervention for the dyad, have also been employed (28). The caregivers were encouraged to learn from cognitive stimulation through specific protocols, by dealing with their stress and anxiety feelings and the daily routine; this was the case of the individual Cognitive Stimulation Therapy (iCST) (36).
The promotion of well-being through dancing was also a therapeutic tool in some studies (37), improving social activity and psychical health. The Project DANCIN (Dance Therapy Intervention) measured in two daily sessions (in a total of 24 sessions) PwD with mild and moderate stages and caregivers who want to include this activity in their daily routine (38). Participants exhibited a set of BPSD assessed by the Dementia Mood Assessment Scale (DMAS-17) (39), including insomnia, agitation, angry outbursts, daytime drowsiness, continually fidgeting and staring at the floor and perseverative questioning (38). PwD and also those showing sensory or auditory deficits could benefit from the dancing sessions (38). Additionally, the absence of dance experience was not a limitation to overall engagement in the PwD group.
The reduction of psychological distress among familiar care providers was pursued by the START Project (Strategies for Relatives Intervention) by developing healthy coping strategies (40). Family member’s engagement was reinforced through partnership interventions, as a critical element to reduce behavioral disturbances and enhance well-being in another study (41).
The specific training of staff members showed useful outside metropolitan areas, where memory clinics are not available. One example is the Clinical Antipsychotic Trials of Intervention Effectiveness—CATIE-AD study (n = 421 AD outpatients), which implemented psychoeducation training for GP and non-specialists to the early identification of behavior disturbances, clarifying its main behavior dimensions. A total of 4 distinct clusters have been identified: a) agitation and irritability, b) apathy and eating problems, c) psychosis (delusions and hallucinations, and d) emotion and disinhibition (depression, euphoria and disinhibition) (42).
In other studies, self-monitoring skills were assessed both by the staff and the family member (43). In agitation management, a study aimed at satisfying basic needs proved effective in reducing verbal agitation (44). Improving the patient’s food intake and nutritional status is also essential to reduce agitation and improve this group’s quality of life (45).
Adopting Tailored Activities
One aspect regarded as crucial to warranty the effectiveness of psychosocial interventions is the provision of tailored activities, particularly for home-dwelling PwD (9, 46). As the caregiver group usually varies from adolescents (including “adult children”), adults, spouses to professional care providers, individualized dyadic interventions shall be designed in any dyadic compositions to reduce the caregiver social strain (47) and improve PwD functional ability (47). One of the strategies credited as successful is the promotion of multiagency discussions, which enable the evaluation and provision of unmet needs (19). Dyadic interventions may also be addressed to the primary health care system (48), and GPs may receive training in psychosocial counseling (49). Another innovative intervention allowed personalized interventions to integrate home and residential care services in Japan (19). Noteworthy, the level of PwD engagement shall consider not only the degree of cognitive decline but the preservation of sensory stimuli (e.g., sight, smell, and touch), since potential sensory dysfunctions may be associated with apathy and isolation (23, 50).
Optimal care also involves adapting the expectations of both professionals and the dyad. In one interesting study conducted by Popham and colleagues (13), the main obstacles to optimal care through the Sheffield Care Environment Assessment Matrix (SCEAM) questionnaire (51). The main themes for the dyad were the lack of social interaction activities, more freedom for PwD to go outside, more freedom to choose what activities they could do according to the program, while health and safety, most of the times involving spatial restriction for the patient to wander, were the strong concern for health professionals (13). The support tool Inlife was launched in the Netherlands, developed explicitly for caregivers and PwD to lower the threshold for asking and support (52) in an ongoing 16-week RCT. Primary outcomes comprised the caregiver’s sense of competence and secondary, while secondary outcomes consist of evaluating mood symptoms (anxiety and depression), social network, and feelings of loneliness.
Albeit most studies showed successful results in stimulating PwD, negative results were also reported. One follow-up investigation of 3 years revealed no benefit on the well-being and delay of cognitive decline in mild and very-mild DA (53). The absence of regular weekly phone support and a lack of homogeneity in patient recruitment, including culturally heterogeneous groups, are significant limitations (53).
Intervention Programs Targeting Home-Dwelling PwD and Caregivers
Evidence has suggested that caregivers living outside metropolitan areas (e.g., in rural areas) are more prone to develop emotional burden and instability in the dyad (54), mostly due to the scarcity of specialized facilities, including a memory outpatient service and the absence or lack of psychosocial counseling. Conversely, similarly to their counterparts in major cities, these subjects may benefit mainly from home-based psychosocial intervention targeting the caregiver’s depressive symptoms and burden (55) and short and long term complications associated with BPSD (56). Thus, both low cost and more comprehensive strategies should be favored, especially in times of pandemics. Some experiences have successfully engaged GPs in a psychosocial counseling initiative (41). The adaptation of the protocol “Living Well with Dementia” stimulated the search for psychosocial support among users of the United Kingdom’s primary healthcare system (21). One cluster-randomized trial conducted by Nakanishi and colleagues (19) in a local home setting implemented through a 6-month follow the BASE program, a palliative care approach lead by care managers and professional caregivers, which resulted in a significant reduction of challenging BPSD of PwD. The project Staff Training in Assisted Living Residences (STAR-VA) assessed the frequency and intensity of BPSD in veterans PwD in nursing home care (52). In Germany, the Project Future Workshop Dementia (Zukunftswerkstatt Demenz) has followed Family members and PwD in rural areas (57).
Home-based approaches, including a complete set of activities, such as cognitive and physical training combined, may exhibit better results in randomized controlled trials (RCTs) with community-dwelling PwD. The NYU Caregiver Intervention (NYUCI) was designed to provide caregiver support for adult children and prevent residential care placement through 2 years. The term “adult children” is applied to the child or teenager relatives, most of them sons or daughters or grandchildren compelled to assume caregiving duties, including personal hygiene, economy, and safety (58). NYUCI intervention included family counseling, support group referral and ad hoc consultation, or a contact control group. Participants of NYUCI were found to be less prone to admit their parents to a residential care setting (p < 0.05) and also delayed their parent’s time to admission significantly longer (228.36 days) than those of the control group (17).
Interventions Based on Phone Calls and Internet Apps
Internet psychosocial interventions hold considerable promise for meeting the educational and support needs of informal dementia caregivers at reduced costs (52, 59). A number of them have been delivered to support caregivers (60). The types of intervention vary widely, as does the quality of the methods used (46). Person-centered care approaches designed to home settings have been performed using observational tools and practice development cycles, such as the Dementia Care Mapping™ (DCM™) (61). Besides, touch screen technologies, such as the Companion, have offered an exciting opportunity to deliver the psychosocial intervention and monitor BPSD and caregiver distress and represent a promising field of development for the caregiver network (62). The Dementia Digital Interactive Social Chart (DEM-DISC) is an e-advice ICT tool to support customized disease management in dementia. This study aimed to improve and evaluate DEM-DISC, its user-friendliness and usefulness, and investigate future implementation (63). A total of 73 informal caregivers of PwD, supported by 19 randomized case managers. This study demonstrates that using DEM-DISC positively affected the sense of competence and experienced (met) needs of informal caregivers (63). Care providers could also manifest their opinion about the user-friendliness and usefulness of DEM-DISC through telephone interviews.
The “Ability Program” conducted by Realdon and colleagues in RCT lasted six weeks and comprised cognitive, physical activities, and a set of devices measuring and monitoring remotely vital and psychical health parameters (64). Another relevant follow-up intervention was promoted by the FITT-C study, using telephone-based interventions with trained therapists to manage the caregiver´s depression and burden. Those who received the FITT-C along six months tended to seek less medical attention in the urgency and had fewer hospital stays than the control group (65).
Discussion
Our review provided a concise perspective of the last ten years of research on psychoeducational and psychosocial interventions directed to PwD and caregivers. Most studies achieved successful results in handling BPSD and mood-anxiety symptoms of the care provider, leading to an increase in skills related to caring and contributing to an overall improvement of the dyad quality of life. Telephone-based interventions have also shown effectiveness in reducing presential medical consultation and hospitalization. Similarly, studies adapting to friend-technology devices, including robots and remote-monitoring apps, exhibited promising results for promoting knowledge and facilitating decision-making among care providers. The world currently experiences uncertainty on the COVID-19 pandemic duration, and its effects in the cognition, behavior, and quality of life of PwD are yet to be understood. The current review sheds light on this theme, highlighting the potential use of low-cost and high-impact strategies actionable at the home-dwelling during the quarantine and the post-pandemic period.
The existing approaches tend to favor elements of the dyadrelationship differently. Such aspects involve, in summary, caregivers’ awareness of what behavioral changes are. These approaches can range from simple monitoring to psychotherapy. Conversely, taking care of restlessness, apathy and other behavioral symptoms is also critical. If applied for the current pandemics, measures to monitor sleep, daily walks, and light exposure can counteract the prolonged quarantine period. Another critical aspect is promoting the caregiver’s well-being, by reducing depressive symptoms and burden related to the isolation and permanent contact with PwD. Feelings of being overwhelmed, frustration, and loss of family contact may benefit from regular support and assistance, as demonstrated by telephone-derived interventions (31, 65).
One exciting field of research, for instance, will be the home-based adaptation through technological devices of classic intervention tools, including visual arts (66), museum visitations (61), or artistic, educational workshops (67, 68). The overall adherence and engagement by caregivers to e-devices have shown to be enjoyable and positive (60, 63, 69). Furthermore, technology devices also offer an opportunity for disease management to health assistants (63). In the future, user-friendly ICT solutions may be used to promote self-management by informal caregivers and assist caregivers in finding appropriate care services tailored to their specific situation and needs. Albeit the benefits of computer-based assistive technology have been evidenced, barriers and impediments still threaten the extensive use of these tools, including the inability of partners and care providers to recognize its added value, the lack of potential financial investors and the lack of government support for the development and enhancement of such instruments (63). Possibly, the undetermined duration of pandemics will demand the need for modifying the current protocols and research programs through the emphasis of support group intervention (70) and optimal staff training (13). Future studies will also require personalized protocols to overcome regional challenges, such as the low access of material resources, diversity of school background and the profile of BPSD among PwD.
A multiplicity of factors in primary care may serve as obstacles to optimal primary dementia care, as pointed by previous studies (71), including challenges related to a) the complex biomedical, psychosocial, and ethical nature of the condition; b) the gaps in knowledge, skills, attitudes, and resources of PWD/caregivers and their primary caregivers, thus affecting the active engagement of the latter; and c) the broader systemic and structural barriers negatively affecting the context of dementia care. As previously outlined, from the methods reported in this systematic review, a significant part requires long-term training (i.e., 4–12 weeks) and could not be accessible to a vast parcel of elderlies outside metropolitan areas or modest resource centers (72). Thus, one of the significant challenges is the home-setting adaptation of well-established double-blind, placebo-controlled protocols. In this scenario, both PwD and care providers should be encouraged to influence the organization and living environment of care homes whenever possible (13). Also, some evidence has highlighted the role of ethnicity and cultural background (e.g., Hispanic and Afro-Americans) and the importance of religious coping (73) in the context of psychosocial intervention and recommend the inclusion of ethnic and cultural variables in a more comprehensive program (74, 75). Gender differences, particularly in symptom profile, living condition, and coping style and response, seem to affect the outcome of psychosocial intervention, as highlighted by the literature (76). Another relevant aspect is the educational attainment of PwD (77); interestingly, prior evidence has suggested more significant benefits of cognitive intervention among higher educated patients (77). The importance of continuous follow-up, support, and professional reinforcement, mostly offering help based on the family’s needs, has been outlined in previous studies with no benefit of psychosocial interventional (35, 78).
The present work has some limitations that deserve further comment. First, the broad scope of the theme, encompassing studies with multiple methods and outcomes. Second, the difficulty in transposing the current evidence to the real scenario of the COVID-19 pandemics, particularly in different continents and socio-cultural and economic realities. Although there is a vast multiplicity of psychosocial health programs for the old age with dementia and behavioral disturbances, we expect to bring a sum of the well-succeeded initiatives and, through that, global insights directed to best practices of caring for this population. We believe that future programs targeting behavioral disturbances and caregiver mental health issues in dementia shall consider general principles such as those briefly commented in our review.
Concluding Remarks
Before the COVID-19 epidemy, many studies have invested in evidence-based models targeting the provision of personalized interventions to implement community-based customized dementia care. Conversely, the experience of dealing with social isolation during the pandemic period will demand research on preventive and protective factors of dementia and the pursue of efficient intervention from every perspective, notably the domestic setting. The summary of the evidence from the last ten years suggests that low-cost techniques, tailored to the dyad, with increasing use of technology through friendly online platforms and application robots, can counteract the team’s physical absence during the COVID-19 Pandemic. Such techniques should be directed to mood, sleep, and physical exercise, exploring playful music and dance activities. The potential benefits of different programs are substantial: Improve mood in dementia, reduce lack of mobility, decrease social isolation and integrate the outcomes with more general medical support, helping avoid complications and early recognition of delirium and other physical problems. Also, the caregiver’s self-monitoring, the further understanding of the PwD symptoms, the development of a sense of competence, well-being, and the treatment of mood changes in caregivers are crucial endpoints. Other aspects still to explore are related to adapting the protocols to distant areas or where the pandemics have increased. The integration of support networks with expertise centers is also essential. Lastly, it is also essential to acknowledge the importance of real-world studies, even when limited by resources and strict bias control. Therefore, the existing studies may provide useful information on the effect size of specific interventions, the optimal number of sessions, participants enrolled in staff supervision in different scenarios. The future investigation, supporting the implementation of evidence-based psychosocial interventions, will help optimizing training programs for caregivers in post-pandemic times.
Author Contributions
GA: method design, systematic review of literature and results compilation (including creation of figures and tables), writing of the manuscript (abstract, introduction, methods, results, discussion and conclusions), selection and organization of bibliographic references. MD: method design, systematic review of literature and results compilation (including creation of figures and tables), writing of the manuscript (abstract, introduction, methods, results, discussion and conclusions), selection and organization of bibliographic references. VR: discussion of the theory and method, critical review and text editing. MC: discussion of the theory, critical review and text editing. AV: discussion of the theory and method, writing of the manuscript, critical review and text editing. CC: discussion of theory, writing of the manuscript and critical review. EB: discussion of the theory and method, writing of the manuscript, critical review and text editing.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors thank Letice Valente for editorial assistance.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2020.577871/full#supplementary-material
References
1. Goeman D, Renehan E, Koch S. What is the effectiveness of the support worker role for people with dementia and their carers? A systematic review. BMC Health Serv Res (2016) 1916:285. doi: 10.1186/s12913-016-1531-2
2. American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: Author.
3. Cummings JL, Schneider L, Tariot PN, Kershaw PR, Yuan W. Reduction of behavioral disturbances and caregiver distress by galantamine in patients with Alzheimer’s disease. Am J Psychiatry (2004) 161(3):532–8. doi: 10.1176/appi.ajp.161.3.532
4. Koder D. The use of cognitive behaviour therapy in the management of BPSD in dementia (Innovative practice). Demen (London) (2018) 17(2):227–33. doi: 10.1177/1471301216636261
5. Santos RL, de Sousa MFB, Simões-Neto JP, Nogueira ML, Belfort TT, Torres B, et al. Caregivers’ quality of life in mild and moderate dementia. Arquivos Neuro-Psiquiatria (2014) 72(12):931–7. doi: 10.1590/0004-282X20140155
6. Assal F, Cummings JL. Neuropsychiatric symptoms in the dementias. Curr Opin Neurol (2002) 15(4):445–50. doi: 10.1097/00019052-200208000-00007
7. Ferretti C, Sarti FM, Nitrini R, Ferreira FF, Brucki SMD. An assessment of direct and indirect costs of dementia in Brazil. Larson BA, editor. PloS One (2018) 13(3):e0193209. doi: 10.1371/journal.pone.0193209
8. Søgaard R, Sørensen J, Waldorff FB, Eckermann A, Buss DV, Waldemar G. Cost analysis of early psychosocial intervention in Alzheimer’s disease. Dement Geriatr Cognit Disord (2014) 37(3–4):141–53. doi: 10.1159/000355368
9. Gitlin LN, Piersol CV, Hodgson N, Marx K, Roth DL, Johnston D, et al. Reducing neuropsychiatric symptoms in persons with dementia and associated burden in family caregivers using tailored activities: Design and methods of a randomized clinical trial. Contemp Clin Trials (2016) 49:92–102. doi: 10.1016/j.cct.2016.06.006
10. Folkman S, Lazarus RS, Gruen RJ, DeLongis A. Appraisal, coping, health status, and psychological symptoms. J Pers Soc Psychol (1986) 50(3):571–9. doi: 10.1037/0022-3514.50.3.571
11. Snyder CM, Fauth E, Wanzek J, Piercy KW, Norton MC, Corcoran C, et al. Dementia caregivers’ coping strategies and their relationship to health and well-being: the Cache County Study. Aging Ment Health (2015) 19(5):390–9. doi: 10.1080/13607863.2014.939610
12. Kneebone II, Martin PR. Coping and caregivers of people with dementia. Br J Health Psychol (2003) 8(Pt 1):1–17. doi: 10.1348/135910703762879174
13. Popham C, Orrell M. What matters for people with dementia in care homes? Aging Ment Health (2012) 16(2):181–8. doi: 10.1080/13607863.2011.628972
14. Øksnebjerg L, Diaz-Ponce A, Gove D, Moniz-Cook E, Mountain G, Chattat R, et al. Towards capturing meaningful outcomes for people with dementia in psychosocial intervention research: A pan-European consultation. Health Expect (2018) 21(6):1056–65. doi: 10.1111/hex.12799
15. Krishnamoorthy A, Craufurd D. Treatment of Apathy in Huntington’s Disease and Other Movement Disorders. Curr Treat Options Neurol (2011) 13(5):508–19. doi: 10.1007/s11940-011-0140-y
16. Forstmeier S, Maercker A, Savaskan E, Roth T. Cognitive behavioural treatment for mild Alzheimer’s patients and their caregivers (CBTAC): study protocol for a randomized controlled trial. Trials (2015) 16:526. doi: 10.1186/s13063-015-1043-0
17. Gaugler JE, Reese M, Sauld J. A Pilot Evaluation of Psychosocial Support for Family Caregivers of Relatives with Dementia in Long-Term Care: The Residential Care Transition Module. Res Gerontol Nurs (2015) 8(4):161–72. doi: 10.3928/19404921-20150304-01
18. Streater A, Spector A, Aguirre E, Hoe J, Hoare Z, Woods R, et al. Maintenance Cognitive Stimulation Therapy (CST) in practice: study protocol for a randomized controlled trial. Trials (2012) 13(1):91. doi: 10.1186/1745-6215-13-91
19. Cristina Nascimento Dourado M, Laks J. Psychological Interventions for Neuropsychiatric Disturbances in Mild and Moderate Alzheimer’s Disease: Current Evidences and Future Directions. Curr Alzheimer Res (2016) 13(10):1100–11. doi: 10.2174/1567205013666160728143123
20. Marshall A, Spreadbury J, Cheston R, Coleman P, Ballinger C, Mullee M, et al. A pilot randomised controlled trial to compare changes in quality of life for participants with early diagnosis dementia who attend a “Living Well with Dementia” group compared to waiting-list control. Aging Ment Health (2015) 19(6):526–35. doi: 10.1080/13607863.2014.954527
21. Niu Y-X, Tan J-P, Guan J-Q, Zhang Z-Q, Wang L-N. Cognitive stimulation therapy in the treatment of neuropsychiatric symptoms in Alzheimer’s disease: a randomized controlled trial. Clin Rehabil (2010) Dec24(12):1102–11. doi: 10.1177/0269215510376004
22. Churcher Clarke A, Chan JMY, Stott J, Royan L, Spector A. An adapted mindfulness intervention for people with dementia in care homes: feasibility pilot study. Int J Geriatr Psychiatry (2017) 32(12):e123–31. doi: 10.1002/gps.4669
23. Kabat-Zinn J. Mindfulness-Based Interventions in Context: Past, Present, and Future. Clin Psychol: Sci Pract (2003) 10(2):144–56. doi: 10.1093/clipsy.bpg016
24. Chien WT, Lee IYM. Randomized controlled trial of a dementia care programme for families of home-resided older people with dementia. J Adv Nurs (2011) 67(4):774–87. doi: 10.1111/j.1365-2648.2010.05537.x
25. Karel MJ, Teri L, McConnell E, Visnic S, Karlin BE. Effectiveness of Expanded Implementation of STAR-VA for Managing Dementia-Related Behaviors Among Veterans. Gerontologist (2016) 56(1):126–34. doi: 10.1093/geront/gnv068
26. Hendriks IH, van Vliet D, Gerritsen DL, Dröes R-M. Nature and dementia: development of a person-centered approach. Int Psychogeriatr (2016) 28(9):1455–70. doi: 10.1017/S1041610216000612
27. Van Haitsma KS, Curyto K, Abbott KM, Towsley GL, Spector A, Kleban M. A randomized controlled trial for an individualized positive psychosocial intervention for the affective and behavioral symptoms of dementia in nursing home residents. J Gerontol B Psychol Sci Soc Sci (2015) 70(1):35–45. doi: 10.1093/geronb/gbt102
28. Van’t Leven N, de Lange J, Prick A-E, Pot AM. How do activating interventions fit the personal needs, characteristics and preferences of people with dementia living in the community and their informal caregivers? Demen (London) (2019) 18(1):157–77. doi: 10.1177/1471301216662378
29. Dichter MN, Quasdorf T, Schwab CGG, Trutschel D, Haastert B, Riesner C, et al. Dementia care mapping: effects on residents’ quality of life and challenging behavior in German nursing homes. A quasi-experimental trial. Int Psychogeriatr (2015) 27(11):1875–92. doi: 10.1017/S1041610215000927
30. Johnston B, Lawton S, McCaw C, Law E, Murray J, Gibb J, et al. Living well with dementia: enhancing dignity and quality of life, using a novel intervention, Dignity Therapy. Int J Older People Nurs (2016) 11(2):107–20. doi: 10.1111/opn.12103
31. Tremont G, Davis J, Papandonatos GD, Grover C, Ott BR, Fortinsky RH, et al. A telephone intervention for dementia caregivers: background, design, and baseline characteristics. Contemp Clin Trials (2013) 36(2):338–47. doi: 10.1016/j.cct.2013.07.011
32. Luchsinger J, Mittelman M, Mejia M, Silver S, Lucero RJ, Ramirez M, et al. The Northern Manhattan Caregiver Intervention Project: a randomised trial testing the effectiveness of a dementia caregiver intervention in Hispanics in New York City. BMJ Open (2012) 2(5). doi: 10.1136/bmjopen-2012-001941
33. Waldorff FB, Buss DV, Eckermann A, Rasmussen MLH, Keiding N, Rishøj S, et al. Efficacy of psychosocial intervention in patients with mild Alzheimer’s disease: the multicentre, rater blinded, randomised Danish Alzheimer Intervention Study (DAISY). BMJ (2012) 345:e4693. doi: 10.1136/bmj.e4693
34. Phung KTT, Waldorff FB, Buss DV, Eckermann A, Keiding N, Rishøj S, et al. A three-year follow-up on the efficacy of psychosocial interventions for patients with mild dementia and their caregivers: the multicentre, rater-blinded, randomised Danish Alzheimer Intervention Study (DAISY). BMJ Open (2013) 3(11):e003584. doi: 10.1136/bmjopen-2013-003584
35. Moore RC, Chattillion EA, Ceglowski J, Ho J, von Känel R, Mills PJ, et al. A randomized clinical trial of Behavioral Activation (BA) therapy for improving psychological and physical health in dementia caregivers: results of the Pleasant Events Program (PEP). Behav Res Ther (2013) 51(10):623–32. doi: 10.1016/j.brat.2013.07.005
36. Yates LA, Orrell M, Spector A, Orgeta V. Service users’ involvement in the development of individual Cognitive Stimulation Therapy (iCST) for dementia: a qualitative study. BMC Geriatr (2015) 15:4. doi: 10.1186/s12877-015-0004-5
37. Tang H-YJ, Vezeau T. The use of music intervention in healthcare research: a narrative review of the literature. J Nurs Res (2010) 18(3):174–90. doi: 10.1097/JNR.0b013e3181efe1b1
38. Guzmán A, Robinson L, Rochester L, James IA, Hughes JC. A process evaluation of a Psychomotor Dance Therapy Intervention (DANCIN) for behavior change in dementia: attitudes and beliefs of participating residents and staff. Int Psychogeriatr (2017) 29(2):313–22. doi: 10.1017/S104161021600171X
39. Sunderland T, Alterman IS, Yount D, Hill JL, Tariot PN, Newhouse PA, et al. A new scale for the assessment of depressed mood in demented patients. Am J Psychiatry (1988) 145(8):955–9. doi: 10.1176/ajp.145.8.955
40. Li R, Cooper C, Barber J, Rapaport P, Griffin M, Livingston G. Coping strategies as mediators of the effect of the START (strategies for RelaTives) intervention on psychological morbidity for family carers of people with dementia in a randomised controlled trial. J Affect Disord (2014) Oct168:298–305. doi: 10.1016/j.jad.2014.07.008
41. Bramble M, Moyle W, Shum D. A quasi-experimental design trial exploring the effect of a partnership intervention on family and staff well-being in long-term dementia care. Aging Ment Health (2011) 15(8):995–1007. doi: 10.1080/13607863.2011.583625
42. Nagata T, Nakajima S, Shinagawa S, Plitman E, Graff-Guerrero A, Mimura M, et al. Psychosocial or clinico-demographic factors related to neuropsychiatric symptoms in patients with Alzheimer’s disease needing interventional treatment: analysis of the CATIE-AD study: Risk factors for neuropsychiatric symptoms of dementia (48 letters). Int J Geriatr Psychiatry (2017) 32(12):1264–71. doi: 10.1002/gps.4607
43. Quinn C, Toms G, Anderson D, Clare L. A Review of Self-Management Interventions for People With Dementia and Mild Cognitive Impairment. J Appl Gerontol (2016) 35(11):1154–88. doi: 10.1177/0733464814566852
44. Bédard A, Landreville P, Voyer P, Verreault R, Vézina J. Reducing verbal agitation in people with dementia: evaluation of an intervention based on the satisfaction of basic needs. Aging Ment Health (2011) Sep15(7):855–65. doi: 10.1080/13607863.2011.569480
45. Keller HH. Improving food intake in persons living with dementia. Ann N Y Acad Sci (2016) 1367(1):3–11. doi: 10.1111/nyas.12997
46. Nakanishi M, Endo K, Hirooka K, Granvik E, Minthon L, Nägga K, et al. Psychosocial behaviour management programme for home-dwelling people with dementia: A cluster-randomized controlled trial. Int J Geriatr Psychiatry (2018) 33(3):495–503. doi: 10.1002/gps.4784
47. Dawson N, Menne H. Can Interpreting Nonsignificant Findings Inform the Lessons Learned From an Intervention? Am J Lifestyle Med (2017) 11(4):354–60. doi: 10.1177/1559827615614571
48. Van’t Leven N, Prick A-EJC, Groenewoud JG, Roelofs PDDM, de Lange J, Pot AM. Dyadic interventions for community-dwelling people with dementia and their family caregivers: a systematic review. Int Psychogeriatr (2013) 25(10):1581–603. doi: 10.1017/S1041610213000860
49. Geschke K, Scheurich A, Schermuly I, Laux N, Böttcher A, Fellgiebel A. [Effectivity of early psychosocial counselling for family caregivers in general practioner based dementia care]. Dtsch Med Wochenschr (2012) 137(43):2201–6. doi: 10.1055/s-0032-1305320
50. Behrman S, Chouliaras L, Ebmeier KP. Considering the senses in the diagnosis and management of dementia. Maturitas (2014) 77(4):305–10. doi: 10.1016/j.maturitas.2014.01.003
51. Parker C, Barnes S, Mckee K, Morgan K, Torrington J, Tregenza P. Quality of life and building design in residential and nursing homes for older people. Ageing Soc (2004) 24(6):941–62. doi: 10.1017/S0144686X04002387
52. Dam AEH, de Vugt ME, van Boxtel MPJ, Verhey FRJ. Effectiveness of an online social support intervention for caregivers of people with dementia: the study protocol of a randomised controlled trial. Trials (2017) 2918(1):395. doi: 10.1186/s13063-017-2097-y
53. Koivisto AM, Hallikainen I, Välimäki T, Hongisto K, Hiltunen A, Karppi P, et al. Early psychosocial intervention does not delay institutionalization in persons with mild Alzheimer disease and has impact on neither disease progression nor caregivers’ well-being: ALSOVA 3-year follow-up. Int J Geriatr Psychiatry (2016) 31(3):273–83. doi: 10.1002/gps.4321
54. Brijoux T, Kricheldorff C H, Ll M, Bonfico S. Supporting Families Living With Dementia in Rural Areas. Dtsch Arztebl Int (2016) 113(41):681–7. doi: 10.3238/arztebl.2016.0681
55. Prick A-E, de Lange J, Scherder E, Pot AM. Home-based exercise and support programme for people with dementia and their caregivers: study protocol of a randomised controlled trial. BMC Public Health (2011) 11:894. doi: 10.1186/1471-2458-11-894
56. Schoenmakers B, Buntinx F, DeLepeleire J. Supporting the dementia family caregiver: the effect of home care intervention on general well-being. Aging Ment Health (2010) 14(1):44–56. doi: 10.1080/13607860902845533
57. Kricheldorff C, Brijoux T. [Family companions. New facets in accompanying relatives caring for people with dementia]. Z Gerontol Geriatr (2016) 49(3):201–8. doi: 10.1007/s00391-016-1038-9
58. Kjällman-Alm A, Norbergh K-G, Hellzen O. What it means to be an adult child of a person with dementia. Int J Qual Stud Health Well-being (2013) 8(1):21676. doi: 10.3402/qhw.v8i0.21676
59. Boots LMM, de Vugt ME, van Knippenberg RJM, Kempen GIJM, Verhey FRJ. A systematic review of Internet-based supportive interventions for caregivers of patients with dementia. Int J Geriatr Psychiatry (2014) 29(4):331–44. doi: 10.1002/gps.4016
60. McKechnie V, Barker C, Stott J. Effectiveness of computer-mediated interventions for informal carers of people with dementia-a systematic review. Int Psychogeriatr (2014) 26(10):1619–37. doi: 10.1017/S1041610214001045
61. Surr CA, Walwyn REA, Lilley-Kelly A, Cicero R, Meads D, Ballard C, et al. Evaluating the effectiveness and cost-effectiveness of Dementia Care MappingTM to enable person-centred care for people with dementia and their carers (DCM-EPIC) in care homes: study protocol for a randomised controlled trial. Trials (2016) 17(1):300. doi: 10.1186/s13063-016-1416-z
62. Kerssens C, Kumar R, Adams AE, Knott CC, Matalenas L, Sanford JA, et al. Personalized technology to support older adults with and without cognitive impairment living at home. Am J Alzheimers Dis Other Demen (2015) 30(1):85–97. doi: 10.1177/1533317514568338
63. Van Mierlo LD, Meiland FJM, Van de Ven PM, Van Hout HPJ, Dröes R-M. Evaluation of DEM-DISC, customized e-advice on health and social support services for informal carers and case managers of people with dementia; a cluster randomized trial. Int Psychogeriatr (2015) 27(8):1365–78. doi: 10.1017/S1041610215000423
64. Realdon O, Rossetto F, Nalin M, Baroni I, Cabinio M, Fioravanti R, et al. Technology-enhanced multi-domain at home continuum of care program with respect to usual care for people with cognitive impairment: the Ability-TelerehABILITation study protocol for a randomized controlled trial. BMC Psychiatry (2016) 16(1):425. doi: 10.1186/s12888-016-1132-y
65. Tremont G, Davis JD, Ott BR, Galioto R, Crook C, Papandonatos GD, et al. Randomized Trial of the Family Intervention: Telephone Tracking-Caregiver for Dementia Caregivers: Use of Community and Healthcare Resources. J Am Geriatr Soc (2017) 65(5):924–30. doi: 10.1111/jgs.14684
66. Windle G, Gregory S, Newman A, Goulding A, O’Brien D, Parkinson C. Understanding the impact of visual arts interventions for people living with dementia: a realist review protocol. Syst Rev (2014) 3:91. doi: 10.1186/2046-4053-3-91
67. Ullán AM, Belver MH, Badía M, Moreno C, Garrido E, Gómez-Isla J, et al. Contributions of an artistic educational program for older people with early dementia: an exploratory qualitative study. Demen (London) (2013) 12(4):425–46. doi: 10.1177/1471301211430650
68. Johnson J, Culverwell A, Hulbert S, Robertson M, Camic PM. Museum activities in dementia care: Using visual analog scales to measure subjective wellbeing. Demen (London) (2017) 16(5):591–610. doi: 10.1177/1471301215611763
69. Liang A, Piroth I, Robinson H, MacDonald B, Fisher M, Nater UM, et al. A Pilot Randomized Trial of a Companion Robot for People With Dementia Living in the Community. J Am Med Dir Assoc (2017) 18(10):871–8. doi: 10.1016/j.jamda.2017.05.019
70. Leung P, Orrell M, Orgeta V. Social support group interventions in people with dementia and mild cognitive impairment: a systematic review of the literature. Int J Geriatr Psychiatry (2015) 30(1):1–9. doi: 10.1002/gps.4166
71. Aminzadeh F, Molnar FJ, Dalziel WB, Ayotte D. A review of barriers and enablers to diagnosis and management of persons with dementia in primary care. Can Geriatr J (2012) 15(3):85–94. doi: 10.5770/cgj.15.42
72. Bier N, Grenier S, Brodeur C, Gauthier S, Gilbert B, Hudon C, et al. Measuring the impact of cognitive and psychosocial interventions in persons with mild cognitive impairment with a randomized single-blind controlled trial: rationale and design of the MEMO+ study. Int Psychogeriatr (2015) 27(3):511–25. doi: 10.1017/S1041610214001902
73. Kennedy E, Allen B, Hope A, James IA. Christian worship leaders’ attitudes and observations of people with dementia. Demen (London) (2014) 13(5):586–97. doi: 10.1177/1471301213479786
74. Lee CC, Czaja SJ, Schulz R. The moderating influence of demographic characteristics, social support, and religious coping on the effectiveness of a multicomponent psychosocial caregiver intervention in three racial ethnic groups. J Gerontol B Psychol Sci Soc Sci (2010) 65B(2):185–94. doi: 10.1093/geronb/gbp131
75. Napoles AM, Chadiha L, Eversley R, Moreno-John G. Reviews: developing culturally sensitive dementia caregiver interventions: are we there yet? Am J Alzheimers Dis Other Demen (2010) 25(5):389–406. doi: 10.1177/1533317510370957
76. Baron S, Ulstein I, Werheid K. Psychosocial interventions in Alzheimer’s disease and amnestic mild cognitive impairment: evidence for gender bias in clinical trials. Aging Ment Health (2015) 19(4):290–305. doi: 10.1080/13607863.2014.938601
77. Contador I, Fernández-Calvo B, Ramos F, Olazarán J. Influence of Educational Attainment on Cognition-Based Intervention Programs for Persons with Mild Alzheimer’s Disease. J Int Neuropsychol Soc (2016) 22(5):577–82. doi: 10.1017/S135561771600014X
78. Brodaty H, Mittelman M, Gibson L, Seeher K, Burns A. The effects of counseling spouse caregivers of people with Alzheimer disease taking donepezil and of country of residence on rates of admission to nursing homes and mortality. Am J Geriatr Psychiatry (2009) 17(9):734–43. doi: 10.1097/JGP.0b013e3181a65187
Glossary

Keywords: dementia, psychoeducation, psychosocial intervention, caregiver, COVID-19
Citation: Alves GS, Casali ME, Veras AB, Carrilho CG, Bruno Costa E, Rodrigues VM and Dourado MCN (2020) A Systematic Review of Home-Setting Psychoeducation Interventions for Behavioral Changes in Dementia: Some Lessons for the COVID-19 Pandemic and Post-Pandemic Assistance. Front. Psychiatry 11:577871. doi: 10.3389/fpsyt.2020.577871
Received: 30 June 2020; Accepted: 07 September 2020;
Published: 29 September 2020.
Edited by:
Gianfranco Spalletta, Santa Lucia Foundation (IRCCS), ItalyReviewed by:
Maria Donata Orfei, IMT School for Advanced Studies Lucca, ItalyDeana Davalos, Colorado State University, United States
Copyright © 2020 Alves, Casali, Veras, Carrilho, Bruno Costa, Rodrigues and Dourado. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gilberto Sousa Alves, Z3NhbHZlczEyM0Bob3RtYWlsLmNvbQ==