 Mizuki Takegata1,2*
Mizuki Takegata1,2* Asami Matsunaga2,3,4
Asami Matsunaga2,3,4 Yukiko Ohashi5
Yukiko Ohashi5 Michiko Toizumi1
Michiko Toizumi1 Lay Myint Yoshida1
Lay Myint Yoshida1 Toshinori Kitamura2,3,6,7
Toshinori Kitamura2,3,6,7- 1Department of Pediatric Infectious Diseases, Institute of Tropical Medicine, Nagasaki University, Nagasaki, Japan
- 2Kitamura Institute of Mental Health Tokyo, Tokyo, Japan
- 3Kitamura KOKORO Clinic Mental Health, Tokyo, Japan
- 4Department of Community Mental Health and Law, National Institute of Mental Health, National Center of Neurology and Psychiatry, Kodaira, Japan
- 5Faculty of Nursing, Josai International University, Togane, Japan
- 6T. and F. Kitamura Foundation for Studies and Skill Advancement in Mental Health, Tokyo, Japan
- 7Department of Psychiatry, Graduate School of Medicine, Nagoya University, Nagoya, Japan
Background: Temperament involves individual variations in behavioural tendencies of emotional responses and reactions to stimuli after birth. Because ‘foetal programming' is a strong hypothesis in developing temperament, prenatal and intrapartum factors may be significant determinants of infant temperament. This systematic literature review aims to elucidate the evidence of prenatal and intrapartum predictors, including genetic, biological, environmental, socio-demographic, psychological, and obstetric factors of parents and their child.
Methods: Relevant articles were searched using MEDLINE, PubMed, and SCOPUS. The inclusion criteria were (a) original research article, (b) written in English, (c) assessed the temperament of infants 12 months old or younger as an outcome variable, and (d) investigated prenatal and intrapartum factorial variables of infant temperament. Following the PRISMA guideline, the articles found in the three databases were screened and selected according to the inclusion and exclusion criteria before the final review.
Results: Finally, 35 articles were reviewed. This systematic review identified a variety of prenatal and intrapartum factors that were significantly associated with infant temperament: (1) genetic and biological factors: certain genotypes, maternal cortisol and ACTH, and CRHs, (2) environmental factors: substance use such as tobacco, alcohol, and illegal drugs, (3) socio-demographic factor: lower-income, (4) psychological factors: depression or anxiety, eating disorders, personality types of mothers, and domestic violence, and (5) obstetric factors: foetal growth (birth weight), hypertension in mothers, nausea (emesis), and preterm birth.
Conclusion: The findings support gene-environment interaction and biological mechanisms for developing infant temperament, suggesting the importance of ensuring a safe and comfortable environment for pregnant mothers, unborn infants, and families during pregnancy and delivery.
Introduction
In psychiatry, temperament involves individual variations in behavioural tendencies of emotional responses and reactions to stimuli after birth (1). Different concepts and classifications for temperament have been developed. For example, the temperament is conceptualised as ‘the stylistic component of behaviour' (2) showing nine behavioural styles (e.g., activity and regularity). These styles were further categorised into three types of children in terms of how they fit into the family and school: easy, difficult, and slow-to-warm-up (2). Following Chess and Thomas's theory, Buss and Plomin (3) defined temperament as ‘a set of inherited personality traits that appear early in life' (3). Rothbart defined temperament as ‘relatively stable, primarily biologically based individual differences in reactivity and self-regulation' (4). These researchers indicated that temperament developed before higher cognitive and social aspects of personality, and labelled three major dimensions of temperament: surgency/extraversion, negative affect, and effortful control (5). Hence, temperament is considered to be biologically based, exists from early infancy, and plays a core role in forming an individual's personality (1). Some researcher suggested that, although temperament was originally viewed as relatively stable across an individual's life course, the expression of temperament may be modifiable following the interaction with external environments (1).
Chess and Thomas (2) first proposed the difficult temperament of a child. The difficult temperament refers to a child who tends to react negatively to new situations, is fussy, irritable, and may show other negative reactions (2). Their research placed ~40% of American children in the easy child group, 10% were categorised as difficult, and 15% as slow to warm up (2). Several studies have reported that difficult temperament predisposes the child to emotional difficulties, hyperactivity/inattention, and behaviour problems in later childhood and adolescence (6–8). Although the mechanism is not clear, temperament may act as a mediator or moderator contributing to behaviour problems later in life. For example, when a child comes across a stranger, a difficult temperament child would react negatively, such as crying or throwing a tantrum, whereas others may show positive reactions, such as smiling and laughing. Hence, subjective experiences vary among children depending on their reactivity and self-regulation patterns (9).
Although it is generally believed that temperament is formed from biological reactions before birth, as stated above, its mechanism is a mystery. First, ‘foetal programming' is a strong hypothesis of neuropsychological and behavioural development (10). Genetic factors are thought to play an independent role (11) or interact with environmental factors (12–15). Additionally, the programming is influenced by the neurobiological stress-response system of the child, including immune, cardiovascular, and the hypothalamic-pituitary-adrenal axis (HPA) systems exposed to external stressors (16–18). Second, ‘biological embedding' is another hypothesised mechanism. Biological embedding refers to ‘the process by which early life experiences alter biological processes to affect adult health outcomes' (19) and starts in early pregnancy in response to environmental stressors, bringing structural and functional changes at both molecular and physiological levels (12, 20, 21). Hence, prenatal environmental factors should be emphasised to understand the development of a child's temperament (22, 24).
To the best of our knowledge, four relevant systematic reviews have been conducted on the relationship between prenatal mental disorders in mothers and infant temperament. Two reviews, published in 2011 (22) and 2017 (23), found that prenatal depression and anxiety in the mother was associated with the difficult temperament of her child. However, another review published in 2017 (24) concluded that the association was equivocal due to the limited number of articles. Furthermore, another review found that prenatal alcohol consumption by the mother predicted lower positive affect, affiliation/regulation, and orienting capacity of the infant (25). Besides these reviews, one study determined that increased DNA methylation gestational age relative to clinical gestational age was associated with low-socioeconomic status and birth weight independent of gestational age, sex, and ancestry (26), indicating that prenatal stress due to low socioeconomic status may influence foetal programming. In addition, attention is increasingly being paid to the effect of nutritional supplements, such as omega-3 (n = 3) docosahexanoic acid (DHA), on cognitive and neurological development (27, 28). Therefore, considering foetal programming and biological embedding as the possible mechanisms, prenatal factors of temperament may include not only the psychological distress of mothers but also genetic, biological, and socio-demographic aspects such as economic status, maternal nutrition, and pregnancy and delivery complications.
This systematic literature review elucidates the evidence of prenatal and intrapartum predictors, including genetic, biological, socio-demographic, psychological, and obstetric factors of parents and their infant.
Methods
Appendix 1 shows the search strategy for this literature review. Relevant articles were searched by using MEDLINE, PubMed, and SCOPUS. The search terms were as follows: ‘perinatal OR antenatal OR pregnancy,' ‘mental stress OR psychological stress OR depress* OR anxiety OR posttraumatic stress,*' ‘factor OR predictor OR determinant,' ‘infant,' and ‘temperament.' Inclusion criteria were (a) original research article, (b) written in English, (c) assessed temperament of infants who were 12 months old or younger as an outcome variable, and (d) investigated prenatal and intrapartum factorial variables of infant temperament. We limited our search to infancy because it is believed that the expression of temperament is relatively stable in infancy (1). A cross-sectional article that assessed dysphoric moods perceived by parents along with infant temperament during the postpartum period was excluded because emotionally impaired mothers are reportedly more likely to report their child as having behavioural problems (29). Following the PRISMA flow diagram, relevant articles were screened on the three databases. Titles and their abstract of records, after removing duplicates, were reviewed using ENDNOTE software by M.T. (1st author). Full-text articles of relevant records were carefully reviewed by M.T. (1st author) and A.M. (2nd author) according to the inclusion and exclusion criteria and the quality of each article was assessed. After a discussion, 35 articles were selected for the review.
Results
Figure 1 shows a flow chart of the search strategy. Of the 545 papers found on the databases as of 11 March 2020, title screening yielded 82 (15.0%) original articles. Next, 57 articles (10.4%) were selected through title and abstract screening. Finally, after a discussion between the authors, 35 papers (6.4%) were included in the final review.
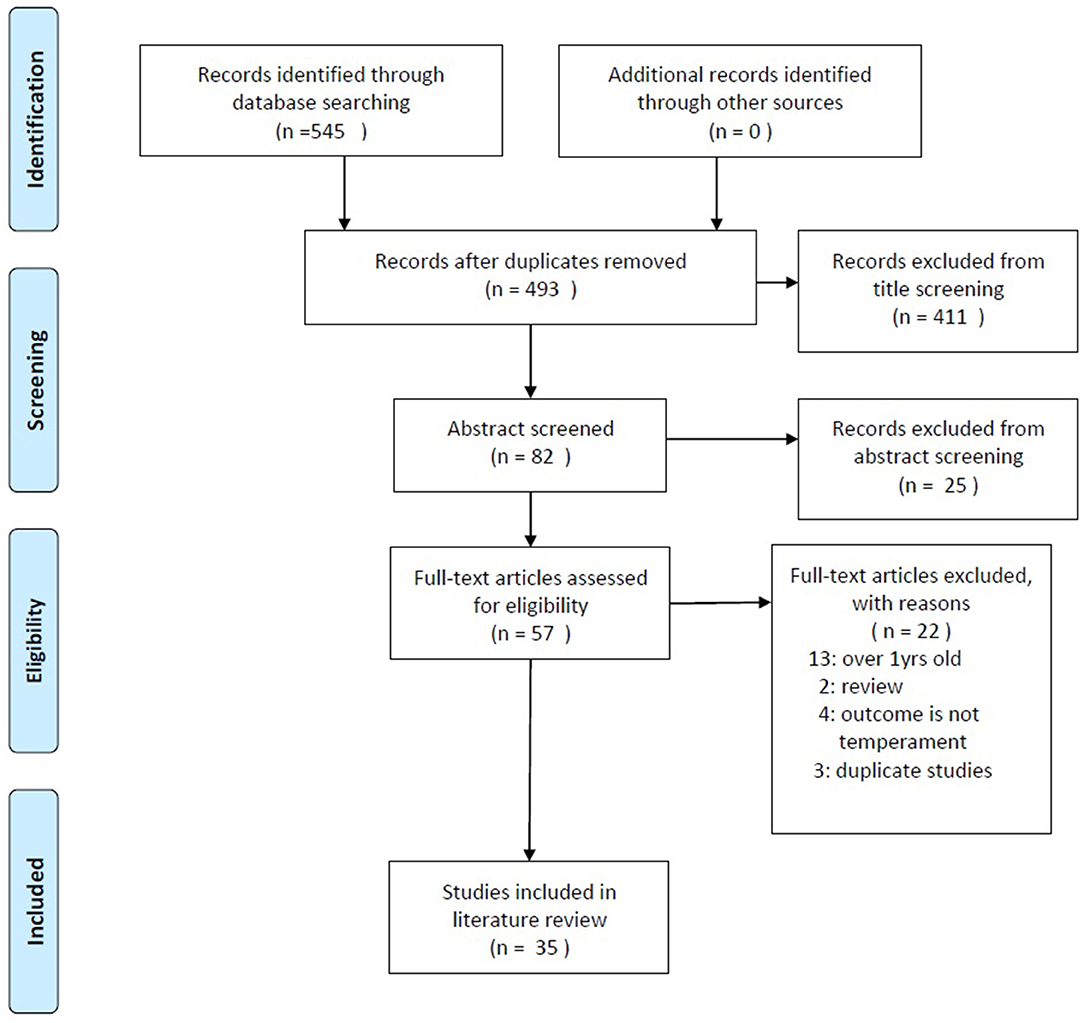
Figure 1. Flow diagram of search strategy.
Nineteen papers (3.4%) were excluded because they did not meet the inclusion criteria: (a) 13 studies observed the temperament of infants older than 12 months of age, (b) two studies were identified as literature reviews, (c) four studies assessed infants' neuro-motor development but not temperament, and (d) two articles referred to the same study as one of the included articles and one did not assess predictors of a child's temperament. Appendix 2 and Appendix 3 summarise the final list of articles and quality assessment, respectively.
Research Trends
Table 1 shows the characteristics of the studies finally reviewed, including region, year published, study design, assessment point of infant temperament, and methods of assessing infant temperament. Most of the studies were conducted in Europe (n = 15) or North America (n = 17), whereas only a few were conducted in Oceania (n = 2) and Asia (n = 1). It was also evident that the number of articles published in this field had increased dramatically after 2006, although this research theme has been emphasised since 1978 (30). Regarding the study design, only a few studies conducted a cohort design (n = 10) or assessed infant temperament during the neonatal period (n = 2). Regarding the methodologies of assessing infant temperament, all the studies used parent-administrative questionnaires; however, two studies adopted the observational assessment of child behaviour by clinical specialist (n = 3). The most frequently used questionnaire was the Infant Behaviour Questionnaire (IBQ), its revised version (31) or a very short version (32) (n =13), followed by the Infant Characteristic Questionnaire (ICQ) (33) (n = 6), the Carey Infant Temperament Questionnaire (CITQ) (n = 4) (34), and the Thomas and Chess Temperament Questionnaire (TTQ) (n = 2) (35), among others. As for the observation of infant behaviour, Kagan's temperament scores were used to observe infants' reactivity in a strange situation (36), as well as ad-hoc methods.
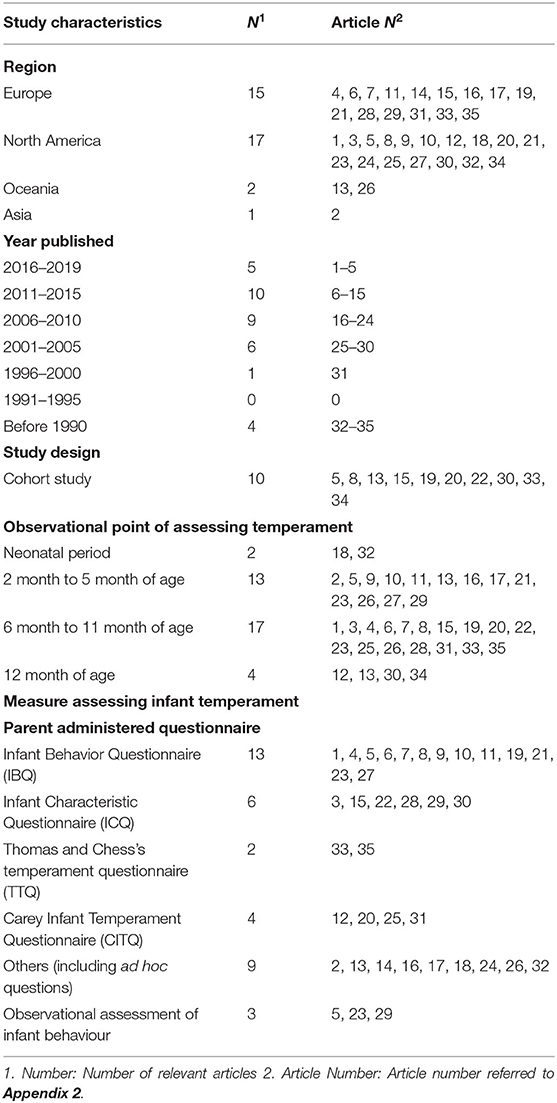
Table 1. Study characteristics of included.
Prenatal and Intrapartum Factors for Infant Temperament
Table 2 summarises the results of prenatal and intrapartum factors for infant temperament.
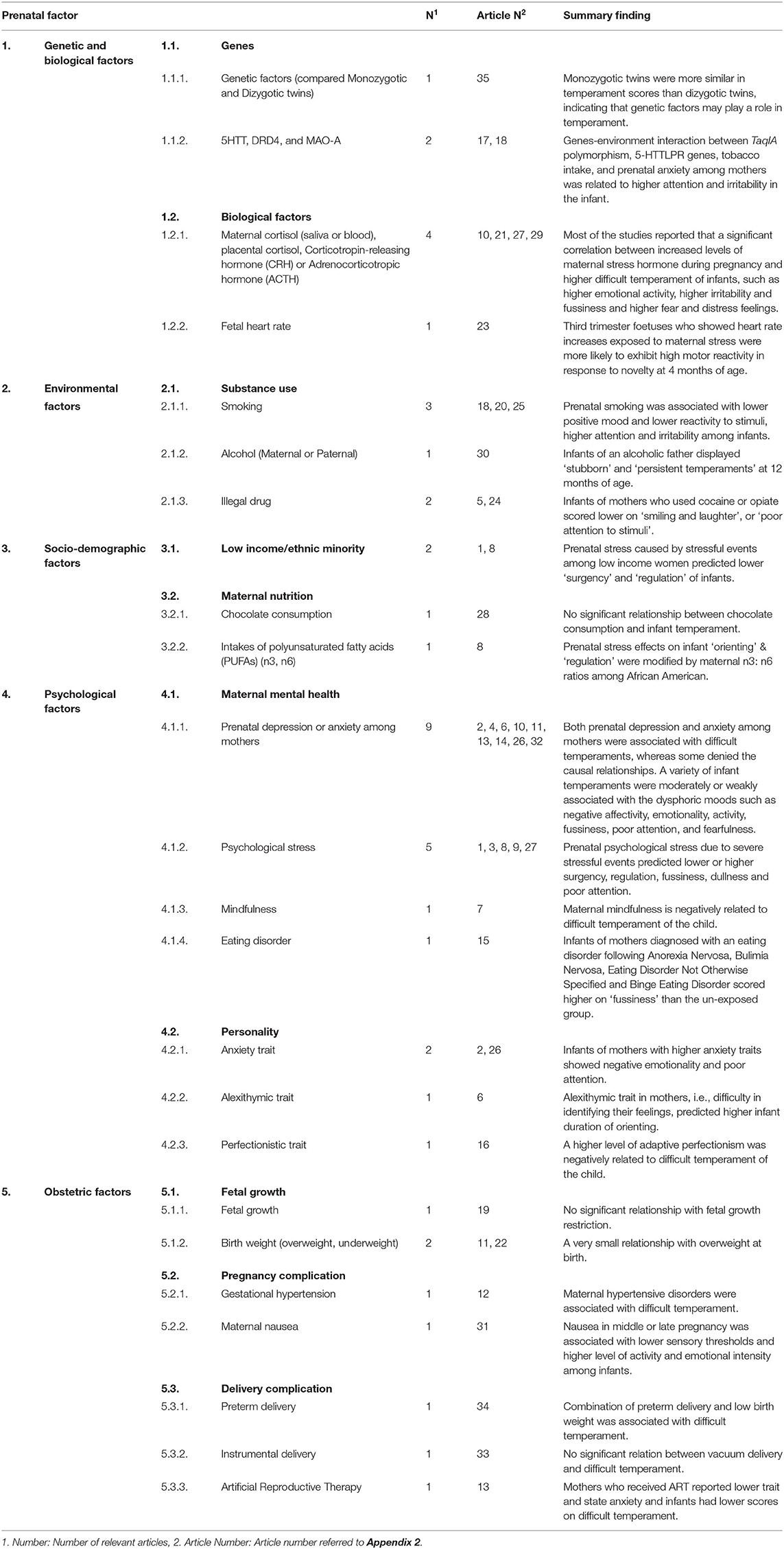
Table 2. Findings of literature review.
Genetic and Biological Factors
Three studies identified the association between the genetic factors of infants and their temperaments (30, 37, 38). Torgersen and Kringlen (30) found that monozygotic (MZ) twins were more similar in temperament scores than dizygotic (DZ) twins, indicating that genetic factors may play a role in temperament (30). Wiebe et al. (37) claimed that the gene–environment (G-E) interaction between TaqIA polymorphism, which is related to the D2 dopamine receptor, and prenatal exposure to tobacco were observed for higher ‘attention' and ‘irritable reactivity' among 4-week old neonates (37). These authors concluded that the interplay between genetic and prenatal environmental factors might affect development patterns of the offspring. Ivorra et al. (38) reported that there were positive correlations between the 5-HTTLPR gene of infants and the postnatal anxiety state of their mothers, and higher ‘irritability' among infants both at 2 and 8 months of age (38).
Out of the five studies that investigated the association of biological factors with infant temperament (14, 39–42), four measured stress hormones, such as maternal or placental cortisol, maternal corticotropin-releasing hormone (CRH), or adrenocorticotropic hormone (ACTH) (39–42), and one focused on foetal heart rate (FHR) (14). First, concerning stress hormones, most of the studies reported a significant correlation between increased levels of maternal stress hormones during pregnancy and difficult temperament in infants, such as higher levels of ‘emotional activity' (40) and higher levels of ‘fear and distress feeling', and ‘negative reactivity' (39, 42). Although most of these earlier studies hypothesised the role of maternal stress hormones as a mediator between maternal psychological distress during pregnancy and infant temperament (39, 40, 42), one study showed the insignificance of its mediating role using pathway analysis (41). Additionally, Davis et al. (39) measured placental cortisol and CRH in mothers' blood at 19, 25, and 31 gestational weeks, and found a significant association between both placental cortisol and CRH at 25 gestational weeks with higher ‘fear and distress feeling' among infants, but not at 19 or 31 gestational weeks (39).
Concerning FHR, Werner et al. (14) targeted 50 dyads of pregnant mothers and their unborn infants to assess FHR change. The authors found that foetuses during the third trimester of pregnancy who showed FHR increases during exposure to maternal psychological stress were more likely to exhibit higher ‘motor reactivity' in response to novelty at 4 months of age. However, Werner et al. (14) also reported no significant relationship between FHR change and ‘cry reactivity' of infants.
Environmental Factors
Six studies focused on maternal substance use during pregnancy; three assessed maternal smoking (37, 43, 44), one investigated paternal alcohol intake (45), and two measured maternal use of illegal drugs (46, 47).
The three studies that focused on maternal smoking reported that heavy or constant smoking by pregnant mothers predicted lower ‘positive mood' (43) and lower ‘reactivity to stimuli' (44) among infants, whereas Wiebe et al. (37) claimed that gene-environment interaction with exposure to tobacco caused higher ‘attention' and ‘irritability' as mentioned above. Picket et al. (43) also claimed that pregnant mothers who quit smoking early exerted a protective effect with decreased risk of ‘distress to novelty' and ‘irregularity' among infants. One study revealed that infants of alcoholic fathers displayed ‘stubborn' and ‘persistent temperament' at the age of 12 months (45). Edwards et al. (45) concluded that internalising problems are attributed to paternal depression comorbid to paternal alcoholism. Regarding maternal use of illegal drug, the use of illegal drugs was studied for cocaine or opiates (46), amphetamines, barbiturates, marijuana, and methamphetamine, as well as for alcohol (47). Locke et al. (46) reported that the infants of mothers who used cocaine or opiates scored lower in ‘smiling and laughter'. Weiss et al. (47) also concluded that infants, who were exposed to illegal substances during pregnancy, were more likely to be distracted by objects or events (‘poor attention to stimuli') in the environment.
Socio-Demographic Factors
Four studies investigated socio-demographic factors, namely low-income ethnic minorities and maternal nutrition (18, 48–50). Bush et al. (18) reported that prenatal stress caused by negative life events (NLE) among low-income women predicted greater respiratory sinus arrhythmia (RSA) reactivity and weaker recovery in foetuses, resulting in lower ‘surgency' and ‘regulation' of infants for weak effect but not negativity at the age of 6 months.
Chocolate consumption of mothers during pregnancy was related to prenatal stress; however, it was not associated with infant temperament (49). Brunst et al. (48) investigate the association between NLE, daily intake of polyunsaturated fatty acids (PUFAs) n3 and n6 during pregnancy, and infant temperament at 6 months postpartum. The authors found that higher n3:n6 ratios attenuated the effect of prenatal stress on ‘orienting' and ‘regulation' temperaments of infants in the African American population (48).
Psychological Factors
Seventeen articles investigated the association between prenatal mental health disorders of mothers and the temperament of infants longitudinally, nine focused on antenatal depression or anxiety in pregnancy (41, 50–57), five investigated prenatal stress (18, 48, 49, 58, 59), and one investigated eating disorders (60) and another investigated mindfulness (61). First, maternal antenatal depression and anxiety were assessed using the Structured Clinical Interview for the DSM (SCID) or parent-administered questionnaire. Six studies identified a significant association between maternal depressive or anxiety symptoms with ‘difficult temperament' in their child (41, 50–52, 56, 62). Antenatal depression in mothers was moderately associated with lower ‘affectivity' (41), lower ‘consolability' and higher ‘excessive crying' in their infants (56). Furthermore, one study suggested that a combination of maternal antenatal depression and lower family income was weakly associated with higher ‘emotionality and activity' among infants (50). The anxiety state of pregnant mothers was weakly associated with higher ‘emotional reactivity' (51, 52) and ‘poor attention to stimuli' among infants (51). However, three studies were unable to find an association between antenatal depression or anxiety in mothers and infant temperament (54, 57, 63).
Five articles focused on prenatal stress caused by severe stressful events (18, 48, 49, 58, 59). Contrary to the association between the combination of lower economic status and prenatal stress and lower ‘surgency' and ‘regulation' of infants as mentioned earlier (18), Lin et al. (59) reported that prenatal stress predicted higher ‘surgency' and ‘negativity', both of which directly and interactively predicted later engagement in regulatory behaviours. Laplante et al. (58) investigated the relationship between perceived maternal stress due to a disaster and infant temperament. Maternal distress was weakly associated with higher ‘fussiness' and ‘dullness' in infants. Raikonnen et al. (49) reported that ‘fear' in infants was higher for mothers who experienced severe stressful events prenatally than those who had not. One paper found a positive factor of infant temperament (61). Van den Heuvel et al. (61) found that mothers who were more mindful tended to score lower on self-regulation problems. Regarding eating disorders, infants of mothers who were diagnosed with an eating disorder such as Anorexia Nervosa (AN), Bulimia Nervosa (BN), Eating Disorder Not Otherwise Specified (EDNOS) and/or Binge Eating Disorder (BED), scored higher on ‘fussiness' than the un-exposed group (60).
The personality of mothers was studied in four articles. Two found that prenatal anxiety trait of mothers was associated with higher ‘negative emotionality' and ‘poor attentions' among infants (51, 57). One article targeting women with alexithymia (difficulty in identifying feelings) predicted higher infant duration for orienting (53). Another paper identified a higher level of adaptive perfectionism that was negatively related to difficult temperament in infants (64).
Obstetric Factors
Eight studies investigated an association between pregnancy or delivery complications and infant temperament (54, 55, 65–70). Concerning pregnancy complications, three studies assessed infants' weight at birth (54, 65, 66). Niegel et al. (65) found that a child with an overweight status at birth was more likely to show a difficult temperament (66). Baibazarova et al. (54) found that infants born with lower birth weight were more likely to show increased ‘fear' and ‘distress to limitation' (54). However, Roza et al. (64) concluded that there was no significant association between intrauterine growth and temperament after full adjustment (65). One study found that infants of mothers diagnosed with hypertensive disorders showed a difficult temperament for weak effect; however, the risk increased in the case of preeclampsia (70). Another study reported that nausea among mothers during pregnancy was associated with lower sensory thresholds and higher levels of activity and emotional intensity among infants (68). Ross (66) investigated the association between preterm delivery (highly correlated with lower birth weight) and difficult temperament (67). One study found no significant association between the mode of delivery (vacuum delivery) and infant temperament (69). Regarding pregnancy due to Artificial Reproductive Treatment (ART), mothers who received ART reported lower trait and state anxiety, and infants had lower scores on difficult temperament (55).
Discussion
A variety of predisposing factors such as genetic, biological, environmental, socio-demographic, and psychological factors of parents were identified. Additionally, both pregnancy and delivery complications weakly or moderately affected infant temperament. Because of different study designs and statistical analysis methods in the reviewed papers, further studies are required to draw more accurate conclusions. However, this systematic review helps to clarify the overall picture concerning prenatal and intrapartum factors of infant temperament and its possible mechanisms.
Regarding the characteristics of the reviewed studies, different assessment tools for measuring infant temperament were used in the reviewed studies due to disagreements about the concept of temperament among researchers. As stated previously, the dimensions of temperament, the criteria of behavioural style, the relationship with emotional behaviour, relative stability, and inheritance were controversial among theorists (1). Therefore, different assessment tools were developed: IBQ, ICQ, CITQ, TTQ, and others. Associations between these temperament measures need to be studied in further investigations. Almost all the reviewed studies treated infant temperament as a dimension. However, children may be grouped according to the patterns of their temperaments. This is a shift of emphasis from variable-centred to person-centred approaches. Different types of children may show different associations with the predictors discussed in the review (71–76).
This systematic review found that only a few studies investigated outcomes during the neonatal period, whereas others assessed outcomes between 2 and 12 months of age. Although temperament is regarded as relatively stable during infancy, some specialists emphasised that the expression of temperament is changeable throughout the period. Rothbart mentioned that ‘bio-behavioural shift is marked during 2 to 3 months of age by increases in orienting, smiling, and laughter, but at a relatively stable activity level from 3 to 12 months' (10). Goldsmith also referred the temperament as primary emotions based on presumably neurophysiological underpinnings; however, some degree of preservation of rank order are present among individuals until the various facets of feeling states, action tendencies, and response systems become integrated into a functional system. Hence, this is the reason why only a few studies in this systematic review collected data in the neonatal period, as the expression of temperament may be unstable during this period.
How temperament is formed and affected by environmental factors during pregnancy is still unclear. Our systematic review revealed that infants with a certain genotype, such as TaqIA polymorphism or 5-HTTLPR genes, who were prenatally exposed to tobacco (37) or psychological stress of their mothers (38), were more likely to show higher ‘irritability' and ‘fussiness'. The findings support the evidence that a child's temperament starts to form with a complex interaction of genes and biological reactions with the outer environment (G-E interactions) from the beginning of pregnancy (77).
Whether the environmental or psychological factors, including substance use or psychological distress, work as a modulator between gene and forms of temperament to affect directly or directly the development of temperament is also unclear. One research study showed two different trajectories through genetic factors as well as other factors of maternal stress hormonal activity called ‘biological embedding' (78). Influenced by the activation of the maternal HPA axis due to psychological/physical stress, the bio-physiologic functions of the foetus also change (79–81) and may result in a higher risk of infant negativity characterised by sadness, anger/frustration, fear, and poor soothability (39–42). Many of the reviewed studies included here focused on maternal psychological symptoms such as anxiety and depression during pregnancy and/or biomarkers of maternal stress such as cortisol, CRH, and ACTH. The increased levels of biomarkers, which are also closely linked with maternal psychological and physical symptoms, showed significant associations with difficult temperament such as higher emotionality, activity, lower surgency, poor attention, and higher levels of fear and fussiness. The biological response of increased stress hormone may play as a moderator interacting with psychological distress and temperament rather than a mediator (82). Additionally, recent studies have shown that psychological distress of mothers during pregnancy not only activates the foetal stress response directly but also indirectly causes an adverse intrauterine environment, such as pregnancy complications, including hypertensive disorders and foetal growth restriction, leading to negative consequences for infant temperament. Although our review did not cover posttraumatic stress disorders (PTSD), some previous studies indicated PTSD symptoms of mothers, cortisol, and difficult temperament of child (82, 83). Hence, ensuring mental and physical health of pregnant mothers is regarded as increasingly important by both clinical health professionals and researchers.
Moreover, it seems that substance use, such as the intake of tobacco, alcohol, and/or illegal drugs, by pregnant mothers directly impacts the neuropsychiatric development of their child because expressions of temperament are different depending on the substance used by the mother. For example, infants of mothers who had a habit of smoking showed higher ‘attention' and ‘irritability' (37), whereas infants of mothers who used cocaine or opiates scored lower on ‘smiling and laughter' and ‘poor attention to stimuli' (46). Due to the limited number of available articles, the differences in temperament due to the types of drugs are uncertain. Conversely, our review revealed the association between NLE, daily intake of PUFAs n3 and n6 during pregnancy, and infant temperament at 6 months postpartum, which supports the evidence that some kinds of nutrition buffer the adverse effect of psychological distress on the cognitive and neurological development (27, 28). However, considering mothers who are psychologically depressed, may take insufficient nutrition, the psychological distress may work as a confounder. Furthermore, whether paternal intake affects the temperament of the child is still unclear due to the very small number of studies (45). Further studies are required.
Interestingly, our systematic review identified that some significant obstetric factors were correlated with infants' temperament characteristics. They included foetal growth (birth weight), hypertension among mothers, nausea (emesis), and preterm birth. Further studies should confirm if low or high birth weight (66, 67) or if prematurity or low birth weight is important (67). Nausea (68) and dietary habits may also have an association with infant temperament. Furthermore, s other psychological and biological factors, the number of studies that focused on obstetric factors was insufficient; therefore, it is difficult to draw any conclusions from these results.
Some limitations should be noted. First, most of the reviewed studies adopted parent-administered questionnaires rather than objective measures to assess infant temperament. Although we excluded cross-sectional studies assessing psychological distress of parents and infant temperament simultaneously, perceived infant temperament may be biased due to parental mood at the time of observation (observer bias). Mothers with mental distress may have more negative views of parenting than others, such as a negligent attitude with decreased visual and physical contact with their infants (84, 85). Since depressed mothers are often more likely to perceive their child as difficult, caution should be taken regarding the causal relationship between infant temperament and parenting distress (8). Second, most of the significant factors identified in these longitudinal studies were only weakly or moderately associated with temperament. Considering the possibility that the expression of temperament may change along with social maturation in infancy (1), more underlying confounders in the postnatal period, such as bonding between the mother and infant, may affect the results. Third, the data search engines used were restricted to MEDLINE, PubMed, and SCOPUS because there was limited access to other databases in our institute. More published papers might have been obtained if we included other data search engines such as PsychINFO.
For future studies, study designs such as a prospective cohort study and adopting both subjective and objective measures may be recommended to avoid bias. Additionally, because most of the studies were conducted in Western societies targeting Caucasian children, more evidence needs to be accumulated in other ethnic groups because temperament is believed to be formed by genetic and biological functions. Furthermore, more evidence regarding pregnancy complications such as hypertensive disorders, nutrition status, delivery complications, and exposure to chemical factors (for example heavy metals, pesticides, and air pollutants) is needed to confirm the link with temperament (27).
Regardless of these limitations, this systematic review helps us understand prenatal and intrapartum factors of temperament, including genetic, biological, socio-demographic, psychological, and obstetric aspects in the complex mechanism of development. The findings from this systematic review imply the necessity of ensuring and promoting a safe and comfortable pregnancy and childbirth by health care professionals. Raising awareness of the risks of substance use and providing health education for a healthy pregnancy and childbirth to mothers and family members are recommended along with psychological support by nurses and midwives. However, it should be noted that infant temperament would, directly and indirectly, be associated with parent-child interactions as well as other confounders in childhood, subsequently helping to form their personality that would lead to positive or negative consequences later in their life (8). Hence, the expression of temperament may change flexibly, with positive consequences influenced by positive interactions between parent and child.
Conclusions
This systematic review identified a variety of prenatal and intrapartum factors that are significantly associated with the temperament of infants: (1) genetic and biological factors: certain genotypes, maternal cortisol and ACTH, and CRHs, (2) environmental factors: substance use such as tobacco, alcohol, and illegal drugs, (3) socio-demographic factor: lower-income, (4) psychological factors: depression or anxiety, eating disorders, personality types of mothers, and domestic violence, and (5) obstetric factors: foetal growth (birth weight), hypertension in mothers, nausea (emesis), and preterm birth. These findings support the gene-environment interaction and biological mechanisms for developing infant temperament, suggesting the importance of ensuring a safe and comfortable environment for pregnant mothers, the unborn child, and families during pregnancy and delivery in society.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
MTa contributed to the conception and designs of work, selection and review of articles, drafted and revised the manuscript. AM contributed to the selection of reviewed articles, drafted the manuscript. YO and TK contributed to the conception and designs of work, interpretation of data, supervision for drafting and revising the manuscript. MTo and LY contributed to supervision for drafting and revising the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study is supported by MEXT/JSPS KAKENHI Grant-in-Aid for Early-Career Scientists (18K17558).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.609020/full#supplementary-material
References
1. Goldsmith HH, Buss AH, Plomin R, Rothbart MK, Thomas A, Chess S, et al. Roundtable: what is temperament? Four approaches. Child Dev. (1987) 58:505–29.
2. Chess S, Thomas A. Temperamental Individuality from Childhood to Adolescence. J Am Acad Child Psychiatry. (1977) 16:218–26. doi: 10.1016/S0002-7138(09)60038-8
3. Buss AH, Plomin R. A Temperament Theory of Personality Development. New York, NY: Willey Interscience (1975).
4. Rothbart MK, Derryberry D. Development of Individual Difference in Temperament. In Lamb MR, Brown AL, editors. Advances in Developmental Psychology. Hillsdale: Lawrence Erlbaum Associates (1981). p. 33–86.
5. Rothbart MK. Measurement of temperament in infancy. Child Dev. (1981) 52:569–78. doi: 10.2307/1129176
6. Abulizi X, Pryor L, Michel G, Melchior M, van der Waerden J. Temperament in infancy and behavioral and emotional problems at age 5.5: The EDEN mother-child cohort. PLoS ONE. (2017) 12:e0171971. doi: 10.1371/journal.pone.0171971
7. Nigg JT. Temperament and developmental psychopathology. J Child Psychol Psychiatry. (2006) 47:395–422. doi: 10.1111/j.1469-7610.2006.01612.x
8. Rettew DC, McKee L. Temperament and its role in developmental psychopathology. Harv Rev Psychiatry. (2005) 13:14–27. doi: 10.1080/10673220590923146
9. Escalona SK. The Roots of Individuality: Normal Patterns of Development in Infancy. Oxford, England: Aldine (1969).
10. Goldsmith HH. Genetic influences on personality from infancy to adulthood. Child Dev. (1983) 54:331–55. doi: 10.2307/1129695
11. Marshall PJ, Fox NA, Henderson HA. Temperament as an organizer of development. Infancy. (2000) 1:239–44. doi: 10.1207/S15327078IN0102_5
12. Monk C, Spicer J, Champagne FA. Linking prenatal maternal adversity to developmental outcomes in infants: the role of epigenetic pathways. Dev Psychopathol. (2012) 24:1361–76. doi: 10.1017/s0954579412000764
13. O'Connor TG, Heron J, Golding J, Glover V. Maternal antenatal anxiety and behavioural/emotional problems in children: a test of a programming hypothesis. J Child Psychol Psychiatry. (2003) 44:1025–36. doi: 10.1111/1469-7610.00187
14. Werner EA, Myers MM, Fifer WP, Cheng B, Fang Y, Allen R, et al. Prenatal predictors of infant temperament. Dev Psychobiol. (2007) 49:474–84. doi: 10.1002/dev.20232
15. Caspi A, Moffitt TE. Gene-environment interactions in psychiatry: joining forces with neuroscience. Nat Rev Neurosci. (2006) 7:583–90. doi: 10.1038/nrn1925
16. Hanson M, Godfrey KM, Lillycrop KA, Burdge GC, Gluckman PD. Developmental plasticity and developmental origins of non-communicable disease: theoretical considerations and epigenetic mechanisms. Prog Biophys Mol Biol. (2011) 106:272–80. doi: 10.1016/j.pbiomolbio.2010.12.008
17. Hertzman C. The biological embedding of early experience and its effects on health in adulthood. Ann N Y Acad Sci. (1999) 896:85–95. doi: 10.1111/j.1749-6632.1999.tb08107.x
18. Bush NR, Jones-Mason K, Coccia M, Caron Z, Alkon A, Thomas M, et al. Effects of pre- and postnatal maternal stress on infant temperament and autonomic nervous system reactivity and regulation in a diverse, low-income population. Dev Psychopathol. (2017) 29:1553–71. doi: 10.1017/s0954579417001237
19. Nist MD. Biological embedding: evaluation and analysis of an emerging concept for nursing scholarship. J Adv Nurs. (2017) 73:349–60. doi: 10.1111/jan.13168
21. Barker DJ. The origins of the developmental origins theory. J Intern Med. (2007) 261:412–7. doi: 10.1111/j.1365-2796.2007.01809.x
22. Field T. Prenatal depression effects on early development: a review. Infant Behav Dev. (2011) 34:1–14. doi: 10.1016/j.infbeh.2010.09.008
23. Korja R, Nolvi S, Grant KA, McMahon C. The relations between maternal prenatal anxiety or stress and child's early negative reactivity or self-regulation: a systematic review. Child Psychiatry Hum Dev. (2017) 48:851–69. doi: 10.1007/s10578-017-0709-0
24. Erickson NL, Gartstein MA, Dotson JAW. Review of prenatal maternal mental health and the development of infant temperament. JOGNN. (2017) 46:588–600. doi: 10.1016/j.jogn.2017.03.008
25. Schoeps A, Peterson ER, Mia Y, Waldie KE, Underwood L, D'Souza S, et al. Prenatal alcohol consumption and infant and child behavior: evidence from the growing up in New Zealand cohort. Early Hum Dev. (2018) 123:22–9. doi: 10.1016/j.earlhumdev.2018.06.011
26. Knight AK, Craig JM, Theda C, Bækvad-Hansen M, Bybjerg-Grauholm J, Hansen CS, et al. An epigenetic clock for gestational age at birth based on blood methylation data. Genome Biol. (2016) 17:206. doi: 10.1186/s13059-016-1068-z
27. Gartstein MA, Skinner MK. Prenatal influences on temperament development: the role of environmental epigenetics. Dev Psychopathol. (2018) 30:1269–303. doi: 10.1017/S0954579417001730
28. Lindsay KL, Buss C, Wadhwa PD, Entringer S. The interplay between nutrition and stress in pregnancy: implications for fetal programming of brain development. Biol Psychiatry. (2019) 85:135–49. doi: 10.1016/j.biopsych.2018.06.021
29. Najman JM, Williams GM, Nikles J, Spence S, Bor W, O'Callaghan M, et al. Bias influencing maternal reports of child behaviour and emotional state. Soc Psychiatry Psychiatr Epidemiol. (2001) 36:186–94.
30. Torgersen AM, Kringlen E. Genetic aspects of temperamental differences in infants. A study of same-sexed twins. J Am Acad Child Psychiatry. (1978) 17:433–44. doi: 10.1016/s0002-7138(09)62299-8
31. Gartstein MA, Rothbart MK. Studying infant temperament via the Revised Infant Behavior Questionnaire. Infant Behav Dev. (2003) 26:64–86. doi: 10.1016/S0163-6383(02)00169-8
32. Putnam S, Helbig A, Gartstein M, Rothbart M, Leerkes E. Development and assessment of short and very short forms of the infant behavior questionnaire-revised. J Pers Assess. (2013) 96:445–58. doi: 10.1080/00223891.2013.841171
33. Bates JE, Freeland CAB, Lounsbury ML. Infant characteristics questionnaire. Child Dev. (1979) 50:794–803. doi: 10.2307/1128946
34. Carey WB, McDevitt SC. Revision of the infant temperament questionnaire. Pediatrics. (1978) 61:735.
35. Thomas A, Chess S, Birch HG. The origin of personality. Sci Am. (1970) 223:102–9. doi: 10.1038/scientificamerican0870-102
36. Kagan J, Snidman N. Temperamental factors in human development. Am Psychol. (1991) 46:856–62. doi: 10.1037/0003-066X.46.8.856
37. Wiebe SA, Espy KA, Stopp C, Respass J, Stewart P, Jameson TR, et al. Gene-environment interactions across development: exploring DRD2 genotype and prenatal smoking effects on self-regulation. Dev Psychol. (2009) 45:31–44. doi: 10.1037/a0014550
38. Ivorra JL, Sanjuan J, Jover M, Carot JM, Frutos R, Molto MD. Gene-environment interaction of child temperament. JDBP. (2010) 31:545–54. doi: 10.1097/DBP.0b013e3181ee4072
39. Davis EP, Glynn LM, Dunkel Schetter C, Hobel C, Chicz-Demet A, Sandman CA. Corticotropin-releasing hormone during pregnancy is associated with infant temperament. Dev Neurosci. (2005) 27:299–305. doi: 10.1159/000086709
40. de Weerth C, Buitelaar JK, Beijers R. Infant cortisol and behavioral habituation to weekly maternal separations: links with maternal prenatal cortisol and psychosocial stress. Psychoneuroendocrinology. (2013) 38:2863–74. doi: 10.1016/j.psyneuen.2013.07.014
41. Rouse MH, Goodman SH. Perinatal depression influences on infant negative affectivity: timing, severity, and co-morbid anxiety. Infant Behav Dev. (2014) 37:739–51. doi: 10.1016/j.infbeh.2014.09.001
42. Davis EP, Glynn LM, Schetter CD, Hobel C, Chicz-Demet A, Sandman CA. Prenatal exposure to maternal depression and cortisol influences infant temperament. J Am Acad Child Adolesc Psychiatry. (2007) 46:737–46. doi: 10.1097/chi.0b013e318047b775
43. Pickett KE, Wood C, Adamson J, D'Souza L, Wakschlag LS. Meaningful differences in maternal smoking behaviour during pregnancy: implications for infant behavioural vulnerability. J Epidemiol Community Health. (2008) 62:318–24. doi: 10.1136/jech.2006.058768
44. Martin RP, Dombrowski SC, Mullis C, Wisenbaker J, Huttunen MO. Smoking during pregnancy: association with childhood temperament, behavior, and academic performance. J Pediatr Psychol. (2006) 31:490–500. doi: 10.1093/jpepsy/jsj041
45. Edwards EP, Leonard KE, Eiden RD. Temperament and behavioral problems among infants in alcoholic families. Infant Ment Health J. (2001) 22:374–92. doi: 10.1002/imhj.1007
46. Locke RL, Lagasse LL, Seifer R, Lester BM, Shankaran S, Bada HS, et al. Effects of prenatal substance exposure on infant temperament vary by context. Dev Psychopath. (2016) 28:309–26. doi: 10.1017/s0954579415000504
47. Weiss SJ, St Jonn-Seed M, Harris-Muchell C. The contribution of fetal drug exposure to temperament: potential teratogenic effects on neuropsychiatric risk. J Child Psychol Psychiatry. (2007) 48:773–84. doi: 10.1111/j.1469-7610.2007.01745.x
48. Brunst KJ, Enlow MB, Kannan S, Carroll KN, Coull BA, Wright RJ. Effects of prenatal social stress and maternal dietary fatty acid ratio on infant temperament: does race matter? Epidemiology. (2014) 4:1000167. doi: 10.4172/2161-1165.1000167
49. Raikkonen K, Pesonen AK, Jarvenpaa AL, Strandberg TE. Sweet babies: chocolate consumption during pregnancy and infant temperament at six months. Early Human Dev. (2004) 76:139–45. doi: 10.1016/j.earlhumdev.2003.11.005
50. Melchior M, Chastang JF, de Lauzon B, Galera C, Saurel-Cubizolles MJ, Larroque B. Maternal depression, socioeconomic position, and temperament in early childhood: the EDEN Mother-Child Cohort. J Affect Disord. (2012) 137:165–9. doi: 10.1016/j.jad.2011.09.018
51. Chong SC, Broekman BF, Qiu A, Aris IM, Chan YH, Rifkin-Graboi A, et al. Anxiety and depression during pregnancy and temperament in early infancy: findings from a multi-ethnic, asian, prospective birth cohort study. Infant Ment Health J. (2016) 37:584–98. doi: 10.1002/imhj.21582
52. Nolvi S, Karlsson L, Bridgett DJ, Korja R, Huizink AC, Kataja EL, et al. Maternal prenatal stress and infant emotional reactivity six months postpartum. J Affect Disord. (2016) 199:163–70. doi: 10.1016/j.jad.2016.04.020
53. Kantonen T, Karlsson L, Nolvi S, Karukivi M, Tolvanen M, Karlsson H. Maternal alexithymic traits, prenatal stress, and infant temperament. Infant Behav Dev. (2015) 41:1–6. doi: 10.1016/j.infbeh.2015.06.013
54. Baibazarova E, van de Beek C, Cohen-Kettenis PT, Buitelaar J, Shelton KH, van Goozen SH. Influence of prenatal maternal stress, maternal plasma cortisol and cortisol in the amniotic fluid on birth outcomes and child temperament at 3 months. Psychoneuroendocrinology. (2013) 38:907–15. doi: 10.1016/j.psyneuen.2012.09.015
55. McMahon CA, Boivin J, Gibson FL, Hammarberg K, Wynter K, Saunders D, et al. Pregnancy-specific anxiety, ART conception and infant temperament at 4 months post-partum. Hum Reprod. (2013) 28:997–1005. doi: 10.1093/humrep/det029
56. Zuckerman B, Bauchner H, Parker S, Cabral H. Maternal depressive symptoms during pregnancy, and newborn irritability. J Dev Behav Pediatr. (1990) 11:190–4.
57. Austin MP, Hadzi-Pavlovic D, Leader L, Saint K, Parker G. Maternal trait anxiety, depression and life event stress in pregnancy: relationships with infant temperament. Early Hum Dev. (2005) 81:183–90. doi: 10.1016/j.earlhumdev.2004.07.001
58. Laplante DP, Brunet A, King S. The effects of maternal stress and illness during pregnancy on infant temperament: project Ice Storm. Pediatr Res. (2016) 79:107–13. doi: 10.1038/pr.2015.177
59. Lin B, Crnic KA, Luecken LJ, Gonzales NA. Maternal prenatal stress and infant regulatory capacity in Mexican Americans. Infant Behav Dev. (2014) 37:571–82. doi: 10.1016/j.infbeh.2014.07.001
60. Zerwas S, Von Holle A, Torgersen L, Reichborn-Kjennerud T, Stoltenberg C, Bulik CM. Maternal eating disorders and infant temperament: findings from the Norwegian mother and child cohort study. Int J Eat Disord. (2012) 45:546–55. doi: 10.1002/eat.20983
61. van den Heuvel MI, Johannes MA, Henrichs J, Van den Bergh BR. Maternal mindfulness during pregnancy and infant socio-emotional development and temperament: the mediating role of maternal anxiety. Early Hum Dev. (2015) 91:103–8. doi: 10.1016/j.earlhumdev.2014.12.003
62. McMahon CA, Ungerer JA, Tennant C, Saunders D. Psychosocial adjustment and the quality of the mother-child relationship at four months postpartum after conception by in vitro fertilization. Fertil Steril. (1997) 68:492–500.
63. Macedo A, Marques M, Bos S, Maia BR, Pereira T, Soares MJ, et al. Mother's personality and infant temperament. Infant Behav Dev. (2011) 34:552–68. doi: 10.1016/j.infbeh.2011.06.009
64. Roza SJ, PAC VANL, Jaddoe VWV, Steegers EAP, Moll HA, Mackenbach JP, et al. Intrauterine growth and infant temperamental difficulties: the Generation R Study. J Am Acad Child Adolesc Psychiatry. (2008) 47:264–72. doi: 10.1097/CHI.0b013e318160b3df
65. Niegel S, Ystrom E, Vollrath ME. Is difficult temperament related to overweight and rapid early weight gain in infants? A prospective cohort study. JDBP. (2007) 28:462–6. doi: 10.1097/DBP.0b013e31811431e8
66. Ross G. Temperament of preterm infants: its relationship to perinatal factors and one-year outcome. J Dev Behav Pediatr. (1987) 8:106–10.
67. Martin RP, Wisenbaker J, Huttunen MO. Nausea during pregnancy: relation to early childhood temperament and behavior problems at twelve years. J Abnorm Child Psychol. (1999) 27:323–9. doi: 10.1023/A:1022662726587
68. Persson-Blennow I, McNeil TF, Blennow G. Temperament in children delivered by vacuum extraction. Am J Orthopsychiatry. (1988) 58:304–9. doi: 10.1111/j.1939-0025.1988.tb01592.x
69. Robinson M, Oddy WH, Whitehouse AJ, Pennell CE, Kendall GE, McLean NJ, et al. Hypertensive diseases of pregnancy predict parent-reported difficult temperament in infancy. J Dev Behav Pediatr. (2013) 34:174–80. doi: 10.1097/DBP.0b013e31827d5761
70. Aksan N, Goldsmith HH, Smider NA, Essex MJ, Clark R, Hyde JS, et al. Derivation and prediction of temperamental types among preschoolers. Dev Psychol. (1999) 35:958–71. doi: 10.1037//0012-1649.35.4.958
71. Caspi A, Silva PA. Temperamental qualities at age three predict personality traits in young adulthood: longitudinal evidence from a birth cohort. Child Dev. (1995) 66:486–98. doi: 10.1111/j.1467-8624.1995.tb00885.x
72. Ohashi Y, Kitamura T. Typology of Temperament of Japanese Children Aged 3 and 4. Psychology. (2020) 11:955–65. doi: 10.4236/psych.2020.116061
73. Prokasky A, Rudasill K, Molfese VJ, Putnam S, Gartstein M, Rothbart M. Identifying child temperament types using cluster analysis in three samples. J Res Personality. (2017) 67:190–201. doi: 10.1016/j.jrp.2016.10.008
74. Robins RW, John OP, Caspi A, Moffitt TE, Stouthamer-Loeber M. Resilient, overcontrolled, and undercontrolled boys: three replicable personality types. J Pers Soc Psychol. (1996) 70:157–71. doi: 10.1037/0022-3514.70.1.157
75. Sanson A, Letcher P, Smart D, Prior M, Toumbourou J, Oberklaid F. Associations between Early childhood temperament clusters and later psychosocial adjustment. Merrill-Palmer Quarterly. (2008) 55:26–54. doi: 10.1353/mpq.0.0015
76. Bronfenbrenner U, Ceci SJ. Nature-nurture reconceptualized in developmental perspective: a bioecological model. Psychol Rev. (1994) 101:568–86. doi: 10.1037/0033-295x.101.4.568
77. Rice F, Harold GT, Boivin J, van den Bree M, Hay DF, Thapar A. The links between prenatal stress and offspring development and psychopathology: disentangling environmental and inherited influences. Psychol Med. (2010) 40:335–45. doi: 10.1017/S0033291709005911
78. Benediktsson R, Seckl JR. Understanding human parturition. Lancet. (1998) 351:913–4. doi: 10.1016/s0140-6736(05)70335-4
79. Radtke KM, Ruf M, Gunter HM, Dohrmann K, Schauer M, Meyer A, et al. Transgenerational impact of intimate partner violence on methylation in the promoter of the glucocorticoid receptor. Transl Psychiatry. (2011) 1:e21. doi: 10.1038/tp.2011.21
80. Weinstock M. Does prenatal stress impair coping and regulation of hypothalamic-pituitary-adrenal axis? Neurosci Biobehav Rev. (1997) 21:1–10. doi: 10.1016/S0149-7634(96)00014-0
81. Enlow MB, Egeland B, Carlson E, Blood E, Wright RJ. Mother-infant attachment and the intergenerational transmission of posttraumatic stress disorder. Dev Psychopathol. (2014) 26:41–65. doi: 10.1017/S0954579413000515
82. Enlow MB, Devick KL, Brunst KJ, Lipton LR, Coull BA, Wright RJ. Maternal lifetime trauma exposure, prenatal cortisol, and infant negative affectivity. Infancy. (2017) 22:492–513. doi: 10.1111/infa.12176
83. Burney RV, Leerkes EM. Links between mothers' and fathers' perceptions of infant temperament and coparenting. Infant Behav Dev. (2010) 33:125–35. doi: 10.1016/j.infbeh.2009.12.002
84. van den Bloom DC, Hoeksma JB. The effect of infant irritability on mother-infant interaction: a growth-curve analysis. Dev Psychol. (1994) 30:581–90. doi: 10.1037/0012-1649.30.4.581
Keywords: infant, temperament, systematic review, prenatal factor, intrapartum factor
Citation: Takegata M, Matsunaga A, Ohashi Y, Toizumi M, Yoshida LM and Kitamura T (2021) Prenatal and Intrapartum Factors Associated With Infant Temperament: A Systematic Review. Front. Psychiatry 12:609020. doi: 10.3389/fpsyt.2021.609020
Received: 22 September 2020; Accepted: 08 March 2021;
Published: 08 April 2021.
Edited by:
David Cohen, Université Pierre et Marie Curie, FranceReviewed by:
Maria Muzik, University of Michigan, United StatesRosalind Wright, Icahn School of Medicine at Mount Sinai, United States
Copyright © 2021 Takegata, Matsunaga, Ohashi, Toizumi, Yoshida and Kitamura. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mizuki Takegata, bXRha2VnYXRhLXRreUB1bWluLmFjLmpw