 Stefano Cardullo1
Stefano Cardullo1 Luis J. Gómez Pérez1
Luis J. Gómez Pérez1 Diego Cuppone1
Diego Cuppone1 Michela Sarlo2
Michela Sarlo2 Nicola Cellini3,4Alberto Terraneo1Luigi Gallimberti1
Nicola Cellini3,4Alberto Terraneo1Luigi Gallimberti1 Graziella Madeo1*
Graziella Madeo1*- 1Fondazione Novella Fronda, Piazza Castello, Padova, Italy
- 2Department of Communication Sciences, Humanities and International Studies, University of Urbino Carlo Bo, Urbino, Italy
- 3Department of General Psychology, University of Padova, Padova, Italy
- 4Padova Neuroscience Center, University of Padova, Padova, Italy
Background: Adult attention-deficit/hyperactivity disorder (ADHD) is associated with high comorbidity with other psychiatric diseases, including cocaine use disorder (CocUD). Given the common fronto-striatal dysfunction, ADHD patients often use cocaine as self-medication for ameliorating symptoms by increasing striatal dopamine release. Yet, comorbidity with ADHD is related to poor treatment outcomes. CocUD has been treated with transcranial magnetic stimulation (TMS), but no studies investigated the outcomes in patients comorbid with ADHD.
Methods: Twenty-two ADHD/CocUD and 208 CocUD-only participants received a high-frequency (15 Hz) rTMS treatment stimulating the left-DLPFC. We investigated whether both groups of patients shared similar demographic and clinical characteristics at baseline. Then, we monitored the effect of treatment testing for potential differences between groups.
Results: At baseline demographic, toxicology and clinical features were not different between the two groups except for global severity index (GSI from SCL-90): patients of ADHD/CocUD group reported higher general symptomatology compared to the CocUD-only group. Concerning the effect of treatment, both groups significantly improved over time regarding cocaine use, craving, and other negative affect symptoms. No differences were observed between groups.
Conclusions: To our knowledge, this is the first study comparing the demographic characterization and rTMS clinical improvements of patients with a dual diagnosis of ADHD and CocUD against CocUD-only patients. Cocaine use and common self-reported withdrawal/abstinence symptoms appear to benefit from rTMS treatment with no differences between groups. Future studies are needed to further investigate these preliminary results.
Introduction
Attention deficit hyperactivity disorder (ADHD) is a neurobehavioral disorder characterized by a persistent pattern of inattention and/or hyperactivity-impulsivity interfering with functioning or development (1). ADHD symptomatology begins in childhood but often persists into adulthood (2), with high comorbidity rates with other mental disorders (3) such as substance use disorders (SUDs). Indeed, the prevalence of ADHD is considerably higher among individuals with SUDs than in the general population (4–14). The co-occurrence of these disorders has relevant prognostic implications, as it is associated with a more severe course of substance use, a higher rate of psychiatric comorbidity, and poorer treatment outcome (4, 5, 7, 15–19). Several studies show similar disruptions of the brain dopamine (DA) fronto-striatal system and executive control impairments in adults with ADHD (20) and in people who chronically use drugs, as cocaine (21, 22). The impairment of dopamine signaling in individuals with ADHD may explain the higher risk of taking addictive drugs, as substances of abuse acutely increase brain DA concentration, and might transitorily improve ADHD symptoms (23). Moreover, these DA dysfunctions have been linked to the initiation and maintenance of addictive behaviors (24), indicating that drug addiction represents a dramatic dysregulation of brain motivational circuits (25). This evidence has led to the development of neurobiology-based interventions to modify functions of the affected neurocircuitry (26). Repetitive transcranial magnetic stimulation (rTMS) appears a novel and promising neuromodulation approach to the treatment of SUDs (27). rTMS influences neural electrical activity at the network level by inducing either short-or long-term effects through the application of magnetic pulses (28). Long-lasting rTMS-induced changes may impact behavioral manifestations of addictive disorders as craving, intake, or relapse (29). Preliminary clinical studies have shown reductions in cocaine craving and intake after rTMS treatments (30–35). In addition, it was reported a positive effect of rTMS on other symptoms connected to substance use and deeply related to the fronto-striatal functioning (36). The modulation of relevant addiction dimensions (e.g., anhedonia) was found to play a key role in modulating the response to the rTMS treatment (37, 38). Considering the evidence of cortical disinhibition across different psychiatric conditions (39), this brain stimulation technique has shown to provide some benefits also in ADHD subjects improving the core symptoms, including attention deficits, hyperactivity/impulsivity, and oppositional defiance (40, 41). Thus, considering that ADHD comorbidity negatively affects conventional treatment results for SUDs as cocaine use disorders (CocUD) (17), the present study aimed to assess the therapeutic response in terms of substance use and accompanying withdrawal symptoms in a sample of CocUD patients with and without ADHD symptoms who underwent a high frequency rTMS stimulation protocol over the left dorsolateral prefrontal cortex (L-DLPFC).
Methods
Participant Selection
Two-hundred and thirty participants diagnosed as suffering from cocaine use disorder (CocUD) were recruited after they voluntarily referral to a specialty outpatient clinic, Center for Addiction in Padua (Italy). Patients signed informed consent on the day of clinic intake and agreed that their data could be used for research. Patients were informed that the data collected would be processed in accordance with the law on privacy and compliance with Legislative Decree No. 196 of June 30, 2003, “Personal Data Protection Code” ensuring anonymity. The data were extracted from patient clinical records and anonymized for analysis. All subjects gave their informed consent for inclusion before they participated in the study. This is a retrospective chart review of data from 230 patients with CocUD who were treated with an rTMS protocol from 2015 to 2019 in an open-label, no sham control study investigating sleep disturbances. The protocol, limited to the retrospective chart review, was approved by the Ethical Committee for the Psychological Research, Departments of Psychology, University of Padua (Protocol no. 3185, code 82F319362FA08A4C9498620BF072CB72), and the study was conducted in accordance with the Declaration of Helsinki. The current retrospective analysis is listed at ClinicalTrials.gov (identifier: NCT03733821).
Participants were 22 to 59 years old and met diagnostic criteria for CocUD according to the Diagnostic and Statistical Manual of Mental Disorders – 5 (DSM 5) (1), as assessed by a clinical psychiatrist specializing in substance use disorders (SUDs). Exclusion criteria included a prior history of other psychiatric diseases, including major depression, schizophrenia, bipolar disorder or other psychosis, current alcohol and other substance abuse or dependence (excluding nicotine, and caffeine), pregnancy or breastfeeding, personality disorders or sleep disturbances deemed to be the primary disease, current unstable medical illness, substantial neurological illness, and any contraindication for rTMS (including implanted metal and devices in the body, or history of epilepsy). From the entire sample of 230 participants, we identified 22 patients diagnosed as suffering from ADHD as assessed by the structured Diagnostic Interview for ADHD in adults (DIVA 2.0) (42). The clinical suspicion of adult-ADHD arises from the evidenced role of self-medication in symptom control of cocaine rather than a research of the euphoric properties of the substance. As confirmation of the diagnosis, 19 out of 22 ADHD patients were pharmacologically treated with atomoxetine (mean: 34 mg/die, range: 18–80 mg/die), in addition to the rTMS treatment, with a significant reduction of inattentive and hyperactive symptoms. Thus, we benchmarked the outcomes of the sample of 22 CocUD patients in comorbidity with ADHD against a large cohort of 208 CocUD patients. All participants were required to keep medication use stable throughout the study. During the whole period of observation, cocaine use was assessed either via a urine drug test, at each visit, or via reports from the patient or significant others. The urine drug screen panel also included the following: morphine, methadone, THC, phencyclidine, amphetamine, and methamphetamine.
Treatment
Each patient underwent rTMS using a medical device (MagPro R30) targeting the L-DLPFC. The stimulation parameters, in accord with international recommendations for patient safety and ethics (43), were: frequency 15 Hz, intensity 100% of the motor threshold, 60 impulses per stimulation train, inter-train interval 15 s, and 40 total trains, for a session duration of 13 min. To best identify the L-DLPFC [Montreal Neurological Institute (MNI) coordinates x: −50, y: 30, z: 36], we used an optical TMS navigator (Localite, St. Augustin, Germany) and a magnetic resonance image (MRI) template. Treatment characteristics are the same described in our previous studies (30, 34): twice-daily rTMS sessions for the first five consecutive days of treatment, followed by twice-daily rTMS sessions once a week over eleven weeks. The time interval between the two sessions within each day was 45–60 min. Then, rTMS was re-administered throughout follow-up on an individualized basis to patients who reported lapses to cocaine use, and to patients whose clinical evaluations showed ongoing cocaine craving, including stress-induced craving. At each session, adverse events, including seizures, syncopes, neurological complications, or subjective complaints about memory, concentration, pain, headache, vertigo, or fatigue were assessed with a self-report questionnaire specifically developed by us for this purpose.
Measures
The primary outcome measure was cocaine use. It was assessed through a combination of urine screening, self-report, and reports by collateral informants (typically family members). Firstly, we considered the lapse to cocaine use. In this analysis, for consistency with our previous works (30, 34), the “zero” day for follow-up monitoring was set at 8 days after the initial 5-day course of rTMS. After that 8-day grace period, any indication of cocaine use was coded as a lapse.
In addition to lapse to cocaine use during follow-up, we evaluated the categorical reduction in cocaine frequency level. We adopted a harm reduction approach already validated for alcohol and cocaine consumption (44, 45). Based on the cocaine use during the 30 days before the assessment, we specified three frequency levels at baseline and day 90: abstinence, low-frequency use (one to 4 days of cocaine use in the past month), and high-frequency use (5 or more days of cocaine use in the past month). We also created a “change” variable to indicate a variation in cocaine frequency level from baseline to day 90: increase one level, no change, decrease one level, decrease two levels.
Secondary outcome measures were craving, perceived sleep quality, depression, anxiety, and other negative affect symptoms, assessed with the following scales: Cocaine Craving Questionnaire (CCQ) (46), Pittsburgh Sleep Quality Index (PSQI) (47), Beck Depression Inventory–II (BDI-II) (48), Self-rating Anxiety Scale (SAS) (49), and Symptoms checklist 90 - Revised (SCL-90-R) (50). Participants were assessed at baseline, immediately after completion of the first week of treatment (Day 5), and 30, 60, and 90 days after the beginning of treatment (Day 30–Day 60–Day 90). The instructions of BDI-II require the participant to consider the last 2 weeks preceding the test; thus, it was not included in the assessment on Day 5. Several participants did not complete every scale at every time point, for the main following reasons: clinical response, missing follow-up visit, missing TMS session, and refusal.
Statistical Analyses
Independent sample t-tests and chi-squares were performed to evaluate differences in the demographic and clinical characterization of patients at baseline.
Concerning the treatment primary outcomes, we used Kaplan- Meier survival analysis to calculate the median number of days until the first lapse to cocaine use. Data were coded as right-censored for patients who were still abstinent at the end of monitoring or with whom the clinic lost contact. We also performed chi-squares for assessing differences in Day 90 functioning by cocaine frequency level and frequency changes compared to baseline.
Linear mixed models, with a random intercept for each subject, using the time-point as a 5 levels independent variable (“Baseline,” “Day 5,” “Day 30,” “Day 60,” “Day 90,”) were computed for each secondary outcome (CCQ, PSQI, BDI-II, SAS, GSI). To estimate the overall effect of treatment, group, and their interaction it was performed a type III analysis of variance with Satterthwaite's method for computing the denominator degrees of freedom of each F-test. We corrected multiple pairwise comparisons between time points using the Bonferroni method.
Thereafter, for examining the best predictor of change in cocaine frequency level we performed an ordinal logistic regression, testing the following predictors: group (ADHD/CocUD vs. CocUD), cocaine frequency level at baseline (abstinence vs. Low use vs. High use), age at the beginning of treatment, age at the first experience with cocaine, age at the time of addiction to cocaine, years of education, and baseline scores at CCQ, PSQI, BDI, SAS and GSI. We did not test for sex differences because most participants were male. To perform this analysis, we removed missing values in any of the predictors: the final sample consisted of 22 patients with ADHD in comorbidity with CocUD, and 156 CocUD patients.
Data were expressed as mean ± standard deviation (SD), unless otherwise specified; alpha was set at <0.05, two-tailed. All the analyses were performed using RStudio versions 1.2.5001 (51) with R version 3.6.1 (52) and the packages MASS (53), survival (54), lme4 (55), lmerTest (56), and emmeans (57).
Results
Patients Characteristics at Baseline
Demographic and clinical characteristics at baseline of the participants are presented in Table 1 divided by group. The sample of ADHD/CocUD consisted of 22 patients, 1 female and 21 males, aged between 25 and 53 (37.91 ± 8.71). The sample of CocUD-only consisted of 208 patients, 5 females 203 males, aged between 22 and 59 (37.67 ± 7.05). Table 1 shows the results of the independent sample t-test for assessing differences between groups. ADHD/CocUD patients were not significantly different compared to CocUD-only patients in demographic characteristics such as age, education, age at the first experience with cocaine, and age at the onset of addiction (all ps ≥ 0.37). Moreover, there were no significantly differences in craving for cocaine (CCQ, p = 0.82), self-perceived sleep quality (PSQI, p = 0.36), depression (BDI, p = 0.10), and anxiety (SAS, p = 0.06). However, a broader measure of clinical symptomatology such as the GSI, from SCL-90, revealed higher scores in ADHD/CocUD patients compared to CocUD-only patients (GSI, p = 0.03).
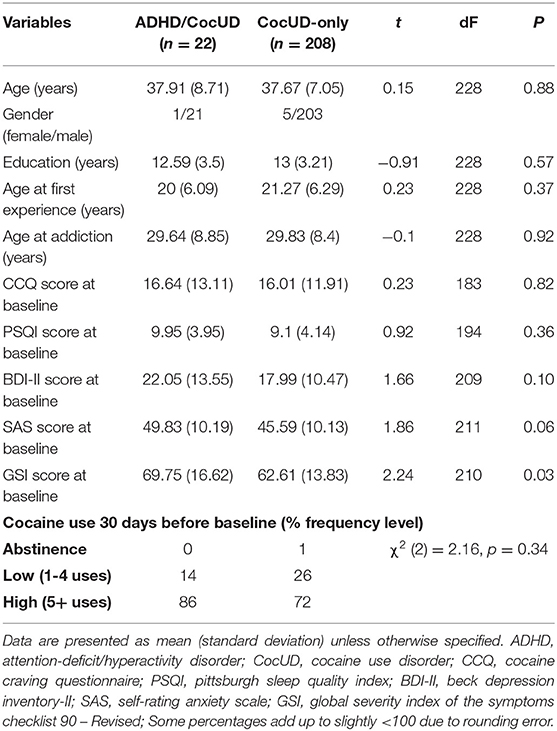
Table 1. Demographic and clinical characteristics of participants.
Regarding the cocaine use frequency level, most of the patients used 5 or more times in the 30 days before the beginning of treatment (ADHD/CocUD: 86%; CocUD-only: 72%). Only 1% of patients in the CocUD-only group was already abstinent at the beginning of treatment. A chi-square test of independence showed that there was no significant association between group and cocaine frequency level, χ2 (2) = 2.16, p = 0.34.
Primary Outcome: Cocaine Use
The Time to the first lapse is shown in Figure 1. The median time to the first use of cocaine use in the ADHD/CocUD group was 58 days (95% confidence interval: 17–267); in the CocUD-only group it was 93 days (95% confidence interval: 63–136). The difference between the two groups was not statistically significant (p = 0.34).
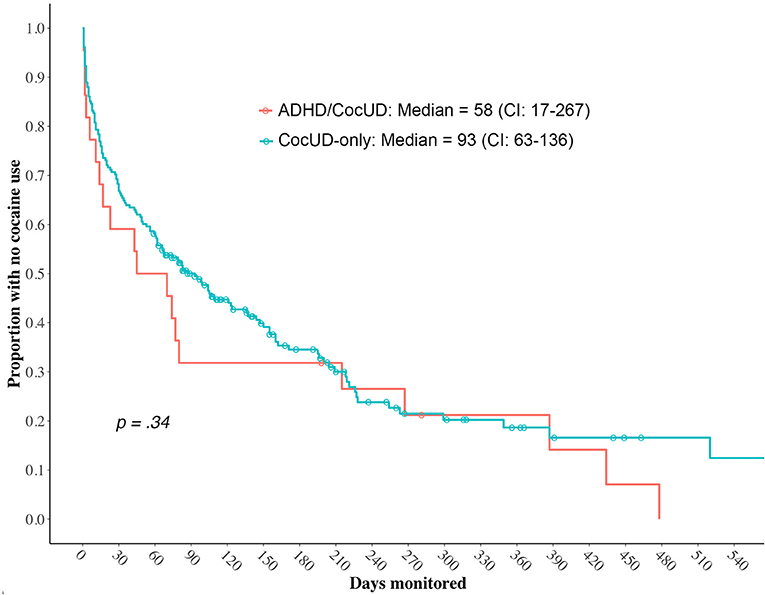
Figure 1. Time to the first resumption of cocaine in ADHD/CocUD and CocUD-only groups. ADHD, attention-deficit/hyperactivity disorder; CocUD, cocaine use disorder.
At the end of the standard protocol of treatment (Day 90), based on the cocaine use during the 30 days before the assessment, we specified three frequency levels as we did at baseline (Figure 2A). The proportion of abstinent patients significantly increased over time in both the ADHD/CocUD group [χ2 (2) = 24.9, p < 0.001] and the CocUD-only group [χ2 (2) = 229.33, p < 0.001]: respectively 50 and 63% of patients were abstinent during the 30 days prior to Day 90. There were no differences between groups [χ2 (2) = 1.69, p = 0.42]. Concerning the variation in cocaine frequency level from baseline to Day 90, 86% of ADHD/CocUD and 82% of CocUD-only patients reported an improvement (decrease one or two levels) (Figure 2B). Again, the chi-square test of independence showed that there was no significant association between groups and the variation in cocaine frequency level [χ2 (3) = 0.91, p = 0.82].
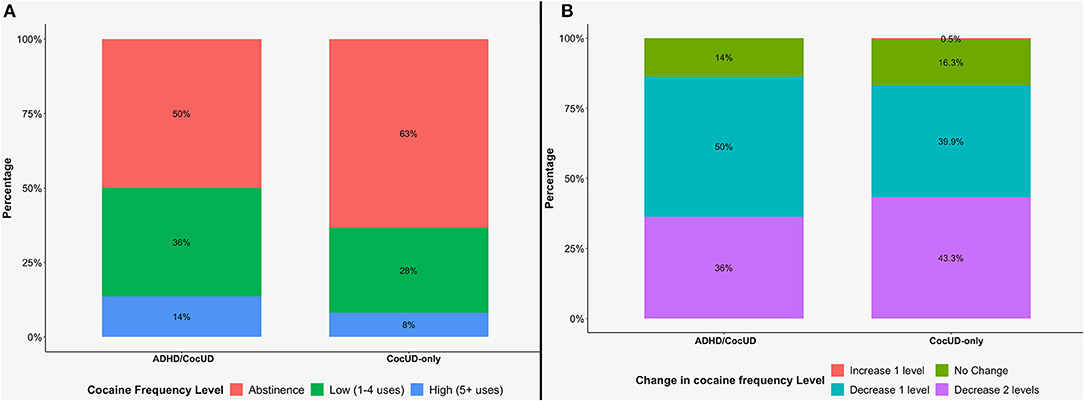
Figure 2. Distribution of patients according to cocaine frequency level at Day 90 (A), and change in cocaine frequency level in comparison to baseline (B). ADHD, attention-deficit/hyperactivity disorder; CocUD, cocaine use disorder.
Secondary Outcome: Changes in Craving, Sleep, Depression, and Anxiety
The second goal of our analyses was to investigate changes in clinical outcomes over time and whether there were differences between ADHD/CocUD and CocUD-only patients undergoing rTMS over the L-DLPFC. Using type III analyses of variance, we tested the main effect of Time and Group and their interaction in each linear mixed model for the different clinical outcomes.
CCQ scores significantly improved at each timepoint after the first week of rTMS treatment [F(4, 638) = 50.35, p < 0.001]. There were no differences between groups and there was not a significant effect of the Time × Group interaction [F(4, 638) = 0.43, p = 0.78]. Pairwise comparisons showed that CCQ scores at Day 5 were significantly lower than those at baseline in both the ADHD/CocUD group (Day 5: 5.59 ± 7.53; Baseline: 16.64 ± 13.11; p < 0.001), and CocUD-only group (Day 5: 3.81 ± 4.95; Baseline: 16.01 ± 11.9; p < 0.001). This improvement was maintained through the three subsequence time points in both the groups: ADHD/CocUD Day 30 (6.64 ± 8.17; p < 0.001), CocUD-only Day 30 (3.12 ± 5.67; p < 0.001), ADHD/CocUD Day 60 (5.55 ± 8.54; p < 0.001), CocUD-only Day 60 (3.62 ± 7.25; p < 0.001), ADHD/CocUD Day 90 (4.71 ± 5.46; p < 0.001), CocUD-only Day 90 (3.19 ± 5.45; p < 0.001).
Like craving, we observed a significant reduction over time of sleep disturbances and affective symptoms as reflected by the significant main effect of Time in each linear mixed model: PSQI [F(4, 682) = 28.99, p < 0.001], BDI-II [F(3, 518) = 101.88, p < 0.001], SAS [F(4, 676) = 43.87, p < 0.001], and GSI [F(4, 735) = 92.73, p < 0.001]. Also, for all these measures it was observed a main effect of Group: PSQI [F(1, 204) = 8.01, p < 0.01], BDI-II [F(1, 200) = 4.48, p < 0.05], SAS [F(1, 217) = 13.13, p < 0.001], and GSI [F(1, 220) = 11.26, p < 0.001]. Pairwise comparison allowed to highlight the differences between groups at the different time points. As previously observed, and here confirmed, at baseline groups were significantly different only for GSI scores [t(566) = 3.03, adjusted p = 0.01]. After the first week of treatment both the groups significantly improved in all the scores, and pairwise comparison showed no significant differences for any of the clinical measures, neither at GSI [t(566) = 2.37, adjusted p = 0.09]. At Day 30, pairwise comparison highlighted significant differences between groups for PSQI [t(672) = 2.99, adjusted p = 0.01], SAS [t(633) = 2.77, adjusted p = 0.02], and GSI scores [t(709) = 2.59, adjusted p = 0.04]. Other comparison showed that PSQI scores at Day 30 in ADHD/CocUD patient were no longer different from baseline [t(678) = 2.28, adjusted p = 0.26]. However, in all the other cases the scores at Day 30 were still significantly lower than those at baseline in both groups. At Day 60 and Day 90 the differences between groups returned to be not significant for all the clinical measure but SAS [Day 60: t(585) = 2.93, adjusted p = 0.02; Day 90 t(628) = 3.06, adjusted p = 0.01]. Also, PSQI score of ADHD/CocUD patients improved and turned again to be significantly lower than those at baseline [Day 60: t(683) = 3.74, adjusted p = 0.002; Day 90 t(679) = 3.77, adjusted p = 0.001].
For none of the clinical outcomes significant Time × Group interactions (all ps ≥ 0.27) were observed.
Best Predictor of Change in Cocaine Frequency Level
In a separate model, we examined the best predictor of change in cocaine frequency level from baseline to day 90 performing an ordinal logistic regression. The results are summarized in Table 2. Above all the predictors, only the cocaine frequency level at baseline and the CCQ score reached the defined alpha level (α = 0.05). Higher cocaine frequency level at baseline was associated with higher odds of moving from no change to decrease one level or decrease two levels (OR = 9.76; 95% CI: 4.61–21.77). Also, for a one-unit increase in CCQ score, the odds of moving from no change to decrease one level or decrease two levels were 4% less, given that the other variables in the model are held constant.
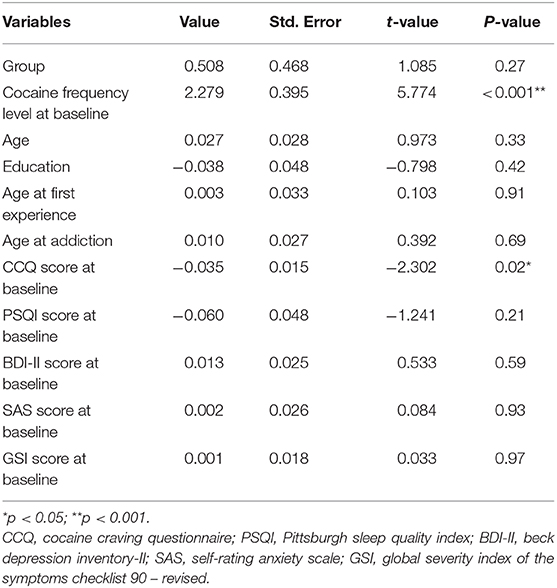
Table 2. Coefficient table of the ordinal logistic regression for examining the best predictor of change in cocaine frequency level.
Safety
None of these 230 patients reported any serious adverse event during the study. There were no seizures, syncopes, neurological complications, or subjective complaints about memory or concentration impairment limiting the treatment and no patient discontinued treatment prematurely due to intolerable stimulation, pain, or other adverse effects such as headache, vertigo, or fatigue.
Discussion
The main aim of the present study was to determine whether attention deficit hyperactivity disorder (ADHD) comorbidity among patients with cocaine addiction is associated with higher clinical symptomatology or less successful results of rTMS treatment.
In our sample the prevalence of ADHD was 9.5%, which is very close to what was found in other populations of cocaine abusers (9), and higher than the one reported in the Italian population (2.8%) (58). In opposite to already published studies and meta-analyses (5, 15, 16), in our cohort cocaine abusers with adult ADHD, compared to those without such comorbidity, were not younger at the clinical admission and did not report an earlier onset of cocaine abuse or a more frequent use in the 30-days before treatment. Moreover, they did not report worse depressive symptomatology, self-perceived quality of sleep, or anxiety as assessed by BDI-II, PSQI, and SAS. At baseline, the only clinical measure which was significantly different between the two groups was the Global Severity Index, indicating a generical status with severe symptoms. The lack of differences between groups may be due to an uncontrolled bias regarding the intrinsic characteristics of the patients who voluntarily refers to the specialty outpatient private clinic in which data were collected. They may have a higher socio-economic status or higher level of education compared to the generic population of cocaine abusers. These elements may flatten the differences found in the already published studies. Further studies are needed to test this hypothesis.
Several studies suggested that psychiatric comorbidity could play a role in determining a worse prognosis (5, 17, 18). Thus, we predicted that co-occurring ADHD would have a negative impact on the outcome of treatment (e.g., cocaine use). In our study, we adopted a harm reduction approach already validated for alcohol and cocaine consumption (44, 45). As reported by other groups, other than abstinence, a reduction in cocaine frequency by the end of treatment might be meaningful for a sustained clinical benefit up to 1 year following treatment (45). Surprisingly, our findings did not replicate the negative prognostic effect: concerning the variation in cocaine frequency level from baseline to Day 90, 86% of ADHD/CocUD and 82% of CocUD-only patients reported an improvement (decrease one or two levels) with no significant differences between groups. Both groups also showed an overall significant improvement of other accompanying symptoms, including depression and perceived sleep quality. On Day 90 there were no differences between groups in none measure, except for SAS scores. Indeed, patients with ADHD comorbidity showed higher anxiety levels compared to CocUD-only patients at Day 60 and Day 90. However, the mean SAS score in ADHD patients was above the clinical level set to 45, indicating a normal range of anxiety in both groups.
In our sample of ADHD/CocUD patients, 19 out of 22 subjects were pharmacologically treated with atomoxetine, and all received an rTMS treatment in addition to a conventional psychosocial intervention. This integrative multidimensional approach could account for the positive outcome observed in the ADHD/CocUD patient population, that did not differ from the CocUD-only group. However, despite atomoxetine treatment has been associated with clinical improvements in quality of life and executive functions in subjects with ADHD (59), a randomized double-blind placebo-controlled study failed to provide evidence supporting the utility of atomoxetine in treating cocaine dependence (60, 61). Moreover, it has been reported that atomoxetine increases extracellular levels of DA in prefrontal cortex, but not in the striatum and nucleus accumbens (62–65). The rTMS neuromodulatory effect within the reward circuitry may induce significant changes within the dysfunctional dopaminergic signaling underlying ADHD pathophysiology. Functional imaging studies showed a significant reduction dopamine transporter (DAT) and D2/D3 receptors within the reward/motivation brain areas in both ADHD and CocUD patients compared to healthy subjects (21, 22, 66, 67). The rTMS protocol over the left DLPFC might restore the aberrant dopaminergic signaling through the dopamine release induced in the caudate nucleus, cingulate cortex, and other regions of the dopamine pathway (68, 69) in both ADHD and addiction conditions. Thus, the modulation of dopamine signaling and the effects on executive functioning due to the rTMS treatment, rather than atomoxetine, may lead to the significant clinical effects we observed indiscriminately in both ADHD/CocUD and CocUD-only patients. This may open a new view in the investigation of the therapeutic effect of high-frequency stimulation on ADHD symptoms. Indeed, conflicting results have been reported regarding the use of rTMS as an effective tool for ADHD treatment (40, 41, 70–72). However, none of these studies stimulated the left DLPFC and further studies are needed to examine his role.
Another aim of our study was to explore the better predictor of treatment outcome. Specifically, we examined the best predictor of change in cocaine frequency level from baseline to day 90 performing an ordinal logistic regression. Above all the predictors, only the cocaine frequency level at baseline and the craving were significant. In previous studies, both of these variables were the most important predictors of successful detoxification from cocaine (73–77). Our results extend these findings to the context of an rTMS treatment. Again, there were no differences between groups: having ADHD in comorbidity is not related to a decreased odd of improvement.
To our knowledge, this is the first study comparing the demographic characterization and rTMS clinical improvements of patients with a dual diagnosis of ADHD and CocUD against CocUD-only patients. Cocaine use and common self-reported withdrawal/abstinence symptoms appear to benefit from rTMS treatment with no differences between groups.
We are aware of the limitations of the naturalistic clinical setting in which our cohort of patients received an rTMS treatment. Considering the absence of a control group or a sham-controlled double-blind design, we cannot rule out a possible placebo effect. Moreover, the unbalanced samples and the lack of a priori power analysis could have influenced the final outcome. Future studies using a more standardized approach are needed to further investigate these preliminary results.
Data Availability Statement
The dataset used in this study is not publicly available due to the sensitive and personal nature of the information included. However, the corresponding author is willing to respond to any reasonable requests for de-identified data.
Ethics Statement
The protocol, limited to the retrospective chart review, was reviewed and approved by Ethical Committee for the Psychological Research, Departments of Psychology, University of Padua (Protocol no. 3185, code 82F319362FA08A4C9498620BF072CB72). The patients provided their written informed consent to participate in this study.
Author Contributions
SC: data curation, methodology, formal analysis, and writing the original draft. GM and LG: conceptualization, supervision, review and editing original draft. LGP and DC: methodology and data curation. MS, NC, and AT: review and editing the original draft and designed the study. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank all personnel of the addiction specialty outpatient clinic from Padua (Italy) for their invaluable collaboration in the collection of data. Also, the authors would like to thank the Zardi-Gori Foundation for the fellowship bursary funded to SC.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.659527/full#supplementary-material
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Washington, DC: American Psychiatric Association (2013).
2. Biederman J. Attention-deficit/hyperactivity disorder: a selective overview. Biol Psychiatry. (2005) 57:1215–20. doi: 10.1016/j.biopsych.2004.10.020
3. Kessler RC, Adler L, Berkley R, Biederman J, Conners CK, Demler O, et al. The prevalence and correlates of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. Am J Psychiatry. (2006) 163:716–23. doi: 10.1176/ajp.2006.163.4.716
4. Arias AJ, Gelernter J, Chan G, Weiss RD, Brady KT, Farrer L, et al. Correlates of co-occurring ADHD in drug-dependent subjects: prevalence and features of substance dependence and psychiatric disorders. Addict Behav. (2008) 33:1199–207. doi: 10.1016/j.addbeh.2008.05.003
5. Carroll KM, Rounsaville BJ. History and significance of childhood attention deficit disorder in treatment-seeking cocaine abusers. Compr Psychiatry. (1993) 34:75–82.
6. Huntley Z, Maltezos S, Williams C, Morinan A, Hammon A, Ball D. Rates of undiagnosed attention deficit hyperactivity disorder in London drug and alcohol detoxification units. BMC Psychiatry. (2012) 12:223. doi: 10.1186/1471-244X-12-223
7. Kalbag AS, Levin FR. Adult ADHD and substance abuse: diagnostic and treatment issues. Subst Use Misuse. (2005) 40:1955–81. doi: 10.1080/10826080500294858
8. Falck RS, Wang J, Siegal HA, Carlson RG. The prevalence of psychiatric disorder among a community sample of crack cocaine users: an exploratory study with practical implications. J Nerv Ment Dis. (2004) 192:503–7. doi: 10.1097/01.nmd.0000131913.94916.d5
9. Levin FR, Evans SM, Kleber HD. Prevalence of adult attention-deficit hyperactivity disorder among cocaine abusers seeking treatment. Drug Alcohol Depend. (1998) 52:15–25.
10. Rounsaville BJ, Anton SF, Carroll K, Budde D, Prusoff BA, Gawin F. Psychiatric diagnoses of treatment-seeking cocaine abusers. Arch Gen Psychiatry. (1991) 48:43–51.
11. Tang Y-L, Kranzler HR, Gelernter J, Farrer LA, Cubells JF. Comorbid psychiatric diagnoses and their association with cocaine-induced psychosis in cocaine-dependent subjects. Am J Addict. (2007) 16:343–51. doi: 10.1080/10550490701525723
12. van de Glind G, Konstenius M, Koeter MWJ, van Emmerik-van Oortmerssen K, Carpentier P-J, Kaye S, et al. Variability in the prevalence of adult ADHD in treatment seeking substance use disorder patients: results from an international multi-center study exploring DSM-IV and DSM-5 criteria. Drug Alcohol Depend. (2014) 134:158–66. doi: 10.1016/j.drugalcdep.2013.09.026
13. van Emmerik-van Oortmerssen K, van de Glind G, van den Brink W, Smit F, Crunelle CL, Swets M, et al. Prevalence of attention-deficit hyperactivity disorder in substance use disorder patients: a meta-analysis and meta-regression analysis. Drug Alcohol Depend. (2012) 122:11–9. doi: 10.1016/j.drugalcdep.2011.12.007
14. Ziedonis DM, Rayford BS, Bryant KJ, Rounsaville BJ. Psychiatric comorbidity in white and African-American cocaine addicts seeking substance abuse treatment. Psychiatr Serv. (1994) 45:43–9.
15. Wilens TE. Impact of ADHD and its treatment on substance abuse in adults. J Clin Psychiatry. (2004) 65:38–45.
16. Wilens TE, Fusillo S. When ADHD and substance use disorders intersect: relationship and treatment implications. Curr Psychiatry Rep. (2007) 9:408–14. doi: 10.1007/s11920-007-0053-3
17. Levin FR, Evans SM, Vosburg SK, Horton T, Brooks D, Ng J. Impact of attention-deficit hyperactivity disorder and other psychopathology on treatment retention among cocaine abusers in a therapeutic community. Addict Behav. (2004) 29:1875–82. doi: 10.1016/j.addbeh.2004.03.041
18. Levin FR, Bisaga A, Raby W, Aharonovich E, Rubin E, Mariani J, et al. Effects of major depressive disorder and attention-deficit/hyperactivity disorder on the outcome of treatment for cocaine dependence. J Subst Abuse Treat. (2008) 34:80–9. doi: 10.1016/j.jsat.2006.11.012
19. Wise BK, Cuffe SP, Fischer T. Dual diagnosis and successful participation of adolescents in substance abuse treatment. J Subst Abuse Treat. (2001) 21:161–5. doi: 10.1016/S0740-5472(01)00193-3
20. Volkow ND, Wang G-J, Newcorn J, Telang F, Solanto MV, Fowler JS, et al. Depressed dopamine activity in caudate and preliminary evidence of limbic involvement in adults with attention-deficit/hyperactivity disorder. Arch Gen Psychiatry. (2007) 64:932–40. doi: 10.1001/archpsyc.64.8.932
21. Volkow ND, Fowler JS, Wolf AP, Schlyer D, Shiue C-Y, Alpert R, et al. Effects of chronic cocaine abuse on postsynaptic dopamine receptors. Am J Psychiatry. (1990) 147:719–24. doi: 10.1176/ajp.147.6.719
22. Volkow ND, Fowler JS, Wang GJ, Swanson JM. Dopamine in drug abuse and addiction: results from imaging studies and treatment implications. Mol Psychiatry. (2004) 9:557–69. doi: 10.1038/sj.mp.4001507
23. Volkow ND, Swanson JM. Does childhood treatment of ADHD with stimulant medication affect substance abuse in adulthood? Am J Psychiatry. (2008) 165:553–5. doi: 10.1176/appi.ajp.2008.08020237
24. Goldstein RZ, Volkow ND. Drug addiction and its underlying neurobiological basis: neuroimaging evidence for the involvement of the frontal cortex. Am J Psychiatry. (2002) 159:1642–52. doi: 10.1176/appi.ajp.159.10.1642
25. Koob GF, Volkow ND. Neurobiology of addiction: a neurocircuitry analysis. Lancet Psychiatry. (2016) 3:760–73. doi: 10.1016/S2215-0366(16)00104-8
26. Spagnolo PA, Goldman D. Neuromodulation interventions for addictive disorders: challenges, promise, and roadmap for future research. Brain. (2017) 140:1183–203. doi: 10.1093/brain/aww284
27. Ekhtiari H, Tavakoli H, Addolorato G, Baeken C, Bonci A, Campanella S, et al. Transcranial electrical and magnetic stimulation (tES and TMS) for addiction medicine: a consensus paper on the present state of the science and the road ahead. Neurosci Biobehav Rev. (2019) 104:118–40. doi: 10.1016/j.neubiorev.2019.06.007
28. Diana M, Raij T, Melis M, Nummenmaa A, Leggio L, Bonci A. Rehabilitating the addicted brain with transcranial magnetic stimulation. Nat Rev Neurosci. (2017) 18:685–93. doi: 10.1038/nrn.2017.113
29. Pettorruso M, Martinotti G, Montemitro C, Miuli A, Spano MC, Lorusso M, et al. Craving and other transdiagnostic dimensions in addiction: toward personalized neuromodulation treatments. J ECT. (2020) 36:e8. doi: 10.1097/YCT.0000000000000643
30. Terraneo A, Leggio L, Saladini M, Ermani M, Bonci A, Gallimberti L. Transcranial magnetic stimulation of dorsolateral prefrontal cortex reduces cocaine use: a pilot study. Eur Neuropsychopharmacol. (2016) 26:37–44. doi: 10.1016/j.euroneuro.2015.11.011
31. Rapinesi C, Del Casale A, Di Pietro S, Ferri VR, Piacentino D, Sani G, et al. Add-on high frequency deep transcranial magnetic stimulation (dTMS) to bilateral prefrontal cortex reduces cocaine craving in patients with cocaine use disorder. Neurosci Lett. (2016) 629:43–7. doi: 10.1016/j.neulet.2016.06.049
32. Politi E, Fauci E, Santoro A, Smeraldi E. Daily sessions of transcranial magnetic stimulation to the left prefrontal cortex gradually reduce cocaine craving. Am J Addict. (2008) 17:345–6. doi: 10.1080/10550490802139283
33. Bolloni C, Panella R, Pedetti M, Frascella AG, Gambelunghe C, Piccoli T, et al. Bilateral transcranial magnetic stimulation of the prefrontal cortex reduces cocaine intake: a pilot study. Front Psychiatry. (2016) 7:133. doi: 10.3389/fpsyt.2016.00133
34. Madeo G, Terraneo A, Cardullo S, Gómez Pérez LJ, Cellini N, Sarlo M, et al. Long-term outcome of repetitive transcranial magnetic stimulation in a large cohort of patients with cocaine-use disorder: an observational study. Front Psychiatry. (2020) 11:158. doi: 10.3389/fpsyt.2020.00158
35. Pettorruso M, Martinotti G, Santacroce R, Montemitro C, Fanella F, Di Giannantonio M. rTMS reduces psychopathological burden and cocaine consumption in treatment-seeking subjects with Cocaine Use Disorder: an open label, feasibility study. Front psychiatry. (2019) 10:621. doi: 10.3389/fpsyt.2019.00621
36. Gómez Pérez LJ, Cardullo S, Cellini N, Sarlo M, Monteanni T, Bonci A, et al. Sleep quality improves during treatment with repetitive transcranial magnetic stimulation (rTMS) in patients with cocaine use disorder: a retrospective observational study. BMC Psychiatry. (2020) 20:1–12. doi: 10.1186/s12888-020-02568-2
37. Pettorruso M, Spagnolo PA, Leggio L, Janiri L, Di Giannantonio M, Gallimberti L, et al. Repetitive transcranial magnetic stimulation of the left dorsolateral prefrontal cortex may improve symptoms of anhedonia in individuals with cocaine use disorder: a pilot study. Brain Stimul. (2018) 11:1195–7. doi: 10.1016/j.brs.2018.06.001
38. Pettorruso M, di Giannantonio M, De Risio L, Martinotti G, Koob GF. A light in the darkness: repetitive transcranial magnetic stimulation (rTMS) to treat the hedonic dysregulation of addiction. J Addict Med. (2020) 14:272–4. doi: 10.1097/ADM.0000000000000575
39. Bunse T, Wobrock T, Strube W, Padberg F, Palm U, Falkai P, et al. Motor cortical excitability assessed by transcranial magnetic stimulation in psychiatric disorders: a systematic review. Brain Stimul. (2014) 7:158–69. doi: 10.1016/j.brs.2013.08.009
40. Bloch Y, Harel EV, Aviram S, Govezensky J, Ratzoni G, Levkovitz Y. Positive effects of repetitive transcranial magnetic stimulation on attention in ADHD Subjects: a randomized controlled pilot study. World J Biol Psychiatry. (2010) 11:755–8. doi: 10.3109/15622975.2010.484466
41. Cao P, Xing J, Cao Y, Cheng Q, Sun X, Kang Q, et al. Clinical effects of repetitive transcranial magnetic stimulation combined with atomoxetine in the treatment of attention-deficit hyperactivity disorder. Neuropsychiatr Dis Treat. (2018) 14:3231–40. doi: 10.2147/NDT.S182527
42. Kooij JJS, Francken MH. DIVA 2.0. Diagnostic Interview Voor ADHD Adults bij volwassenen [DIVA 2 0 Diagnostic Interview ADHD Adults] DIVA Found (https://www.divacenter.eu/DIVA.aspx?id=461) (2010).
43. Rossi S, Hallett M, Rossini PM, Pascual-Leone A, Avanzini G, Bestmann S, et al. Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin Neurophysiol. (2009) 120:2008–39. doi: 10.1016/j.clinph.2009.08.016
44. Witkiewitz K, Hallgren KA, Kranzler HR, Mann KF, Hasin DS, Falk DE, et al. Clinical validation of reduced alcohol consumption after treatment for alcohol dependence using the world health organization risk drinking levels. Alcohol Clin Exp Res. (2017) 41:179–86. doi: 10.1111/acer.13272
45. Roos CR, Nich C, Mun CJ, Babuscio TA, Mendonca J, Miguel AQC, et al. Clinical validation of reduction in cocaine frequency level as an endpoint in clinical trials for cocaine use disorder. Drug Alcohol Depend. (2019) 205:107648. doi: 10.1016/j.drugalcdep.2019.107648
46. Weiss RD, Griffin ML, Hufford C, Muenz LR, Najavits LM, Jansson SB, et al. Early prediction of initiation of abstinence from cocaine. Am J Addict. (1997) 6:224–31. doi: 10.1111/j.1521-0391.1997.tb00401.x
47. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
48. Beck A, Steer R, Brown G. Beck depression inventory-II. San Antonio: San Antonio, TX: Psychological Corporation. (1996).
49. Zung WWK. A rating instrument for anxiety disorders. Psychosomatics. (1971) 12:371–9. doi: 10.1016/S0033-3182(71)71479-0
50. Derogatis LR. Symptom checklist-90-R (SCL-90-R): administration, scoring, and procedures manual. 3rd ed. Minneapolis, MN: NCS Pearson (1994).
52. R Core Team. R: A language and environment for statistical computing. Vienna: R Found Stat Comput (2019).
53. Venables WN, Ripley BD. Modern Applied Statistics with S. 4th ed. New York, NY: Springer (2002).
54. Therneau TM, Grambsch PM. Modeling Survival Data: Extending the Cox Model. New York, NY: Springer (2000).
55. Bates D, Mächler M, Bolker B, Walker S. Fitting linear mixed-effects models using lme4. J Stat Softw. (2015). doi: 10.18637/jss.v067.i01
56. Kuznetsova A, Brockhoff PB, Christensen RHB. lmerTest package: tests in linear mixed effects models. J Stat Softw. (2017) 82:1–26. doi: 10.18637/jss.v082.i13
57. Lenth R. emmeans: Estimated Marginal Means, aka Least-Squares Means. R package version 1.5.0 (2020). Available online at: https://CRAN.R-project.org/package=emmeans
58. Fayyad J, Sampson NA, Hwang I, Adamowski T, Aguilar-Gaxiola S, Al-Hamzawi A, et al. The descriptive epidemiology of DSM-IV Adult ADHD in the World Health Organization World Mental Health Surveys. ADHD Atten Deficit Hyperact Disord. (2017) 9:47–65. doi: 10.1007/s12402-016-0208-3
59. Elliott J, Johnston A, Husereau D, Kelly SE, Eagles C, Charach A, et al. Pharmacologic treatment of attention deficit hyperactivity disorder in adults: a systematic review and network meta-analysis. (2020) 15:e0240584. doi: 10.1371/journal.pone.0240584
60. Walsh SL, Middleton LS, Wong CJ, Nuzzo PA, Campbell CL, Rush CR, et al. Atomoxetine does not alter cocaine use in cocaine dependent individuals: a double blind randomized trial. Drug Alcohol Depend. (2013) 130:150–7. doi: 10.1016/j.drugalcdep.2012.10.024
61. Levin FR, Mariani JJ, Secora A, Brooks D, Cheng WY, Bisaga A, et al. Atomoxetine treatment for cocaine abuse and adult attention deficit/hyperactivity disorder (ADHD): a preliminary open trial. J Dual Diagn. (2009) 5:41–56. doi: 10.1080/15504260802628767
62. Suzuki C, Ikeda Y, Tateno A, Okubo Y, Fukayama H, Suzuki H. Acute atomoxetine selectively modulates encoding of reward value in ventral medial prefrontal cortex. J Nippon Med Sch. (2019) 86:98–107. doi: 10.1272/jnms.JNMS.2019_86-205
63. Bymaster FP, Katner JS, Nelson DL, Hemrick-Luecke SK, Threlkeld PG, Heiligenstein JH, et al. Atomoxetine increases extracellular levels of norepinephrine and dopamine in prefrontal cortex of rat: a potential mechanism for efficacy in attention deficit/hyperactivity disorder. Neuropsychopharmacology. (2002) 27:699–711. doi: 10.1016/S0893-133X(02)00346-9
64. Swanson CJ, Perry KW, Koch-Krueger S, Katner J, Svensson KA, Bymaster FP. Effect of the attention deficit/hyperactivity disorder drug atomoxetine on extracellular concentrations of norepinephrine and dopamine in several brain regions of the rat. Neuropharmacology. (2006) 50:755–60. doi: 10.1016/j.neuropharm.2005.11.022
65. Kowalczyk OS, Cubillo AI, Smith A, Barrett N, Giampietro V, Brammer M, et al. Methylphenidate and atomoxetine normalise fronto-parietal underactivation during sustained attention in ADHD adolescents. Eur Neuropsychopharmacol. (2019) 29:1102–16. doi: 10.1016/j.euroneuro.2019.07.139
66. Volkow ND, Wang GJ, Newcorn JH, Kollins SH, Wigal TL, Telang F, et al. Motivation deficit in ADHD is associated with dysfunction of the dopamine reward pathway. Mol Psychiatry. (2011) 16:1147–54. doi: 10.1038/mp.2010.97
67. Volkow ND, Wang GJ, Kollins SH, Wigal TL, Newcorn JH, Telang F, et al. Evaluating dopamine reward pathway in ADHD: clinical implications. J Am Med Assoc. (2009) 302:1084–91. doi: 10.1001/jama.2009.1308
68. Strafella AP, Paus TT, Fraraccio M, Dagher A. Striatal dopamine release induced by repetitive transcranial magnetic stimulation of the human motor cortex. Brain. (2003) 126:2609–15. doi: 10.1093/brain/awg268
69. Cho SS, Strafella AP. rTMS of the left dorsolateral prefrontal cortex modulates dopamine release in the ipsilateral anterior cingulate cortex and orbitofrontal cortex. PLoS ONE. (2009) 4:e6725. doi: 10.1371/journal.pone.0006725
70. Weaver L, Rostain AL, MacE W, Akhtar U, Moss E, O'Reardon JP. Transcranial magnetic stimulation (TMS) in the treatment of attention-deficit/hyperactivity disorder in adolescents and young adults: a pilot study. J ECT. (2012) 28:98–103. doi: 10.1097/YCT.0b013e31824532c8
71. Paz Y, Friedwald K, Levkovitz Y, Zangen A, Alyagon U, Nitzan U, et al. Randomised sham-controlled study of high-frequency bilateral deep transcranial magnetic stimulation (dTMS) to treat adult attention hyperactive disorder (ADHD): Negative results. World J Biol Psychiatry. (2017) 19:561–6. doi: 10.1080/15622975.2017.1282170
72. Niederhofer H. Effectiveness of the repetitive transcranical magnetic stimulation (rTMS) of 1 Hz for attention-deficit hyperactivity disorder (ADHD). Psychiatr Danub. (2008) 20:91–2.
73. Sofuoglu M, Gonzalez G, Poling J, Kosten TR. Prediction of treatment outcome by baseline urine cocaine results and self-reported cocaine use for cocaine and opioid dependence. Am J Drug Alcohol Abuse. (2003) 29:713–27. doi: 10.1081/ADA-120026256
74. Carroll KM, Power M-ED, Bryant KJ, Rounsaville BJ. One-year follow-up status of treatment-seeking cocaine abusers: psychopathology and dependence severity as predictors of outcome. J Nerv Ment Dis. (1993) 181:71–9. doi: 10.1097/00005053-199302000-00001
75. Weiss RD, Griffin ML, Hufford C. Craving in hospitalized cocaine abusers as a predictor of outcome. Am J Drug Alcohol Abuse. (1995) 21:289–301. doi: 10.3109/00952999509002698
76. Bordnick PS, Schmitz JM. Cocaine craving: an evaluation across treatment phases. J Subst Abuse. (1998) 10:9–17. doi: 10.1016/S0899-3289(99)80136-9
Keywords: attention deficit hyperactivity disorder, cocaine use disorder, craving, repetitive transcranial magnetic stimulation, dorsolateral prefrontal cortex, dopamine
Citation: Cardullo S, Gómez Pérez LJ, Cuppone D, Sarlo M, Cellini N, Terraneo A, Gallimberti L and Madeo G (2021) A Retrospective Comparative Study in Patients With Cocaine Use Disorder Comorbid With Attention Deficit Hyperactivity Disorder Undergoing an rTMS Protocol Treatment. Front. Psychiatry 12:659527. doi: 10.3389/fpsyt.2021.659527
Received: 27 January 2021; Accepted: 22 February 2021;
Published: 25 March 2021.
Edited by:
Giovanni Martinotti, University of Studies G. d'Annunzio Chieti and Pescara, ItalyReviewed by:
Mauro Pettorruso, University of Studies G. d'Annunzio Chieti and Pescara, ItalyGeorgios Demetrios Kotzalidis, Sapienza University of Rome, Italy
Copyright © 2021 Cardullo, Gómez Pérez, Cuppone, Sarlo, Cellini, Terraneo, Gallimberti and Madeo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Graziella Madeo, Z3JhemllbWFkZW9AZ21haWwuY29t