 Alexander Bäuerle1
Alexander Bäuerle1 Lisa Jahre1
Lisa Jahre1 Martin Teufel1*
Martin Teufel1* Christoph Jansen1
Christoph Jansen1 Venja Musche1
Venja Musche1 Adam Schweda1
Adam Schweda1 Madeleine Fink1
Madeleine Fink1 Hannah Dinse1
Hannah Dinse1 Benjamin Weismüller1
Benjamin Weismüller1 Nora Dörrie1Florian Junne2,3
Nora Dörrie1Florian Junne2,3 Johanna Graf2†
Johanna Graf2† Eva-Maria Skoda1†
Eva-Maria Skoda1†- 1Clinic for Psychosomatic Medicine and Psychotherapy, LVR-University Hospital Essen, University of Duisburg-Essen, Essen, Germany
- 2Department of Psychosomatic Medicine and Psychotherapy, University Hospital Tübingen, Eberhard Karls University Tübingen, Tübingen, Germany
- 3Department for Psychosomatic Medicine and Psychotherapy, Otto Von Guericke University Magdeburg, Magdeburg, Germany
Background: The SARS-CoV-2 pandemic poses immense challenges for health care systems and population-wide mental health. The e-mental health intervention “CoPE It” has been developed to offer standardized and manualized support to overcome psychological distress caused by the pandemic. The aim of this study was to assess the effectiveness of “CoPE It” in terms of reducing distress (primary outcome), depression and anxiety symptoms, and improving self-efficacy, and mindfulness (secondary outcomes). Furthermore, the intervention's usability, feasibility, and participants' satisfaction with “CoPE It” was evaluated (tertiary outcome). The study protocol has been published previously.
Methods: A bicentre longitudinal study was conducted from April 27th 2020 to May 3rd 2021. N = 110 participants were included in the analyses. The intervention consisted of four modules featuring different media promoting evidence-based methods of cognitive behavioral therapy and mindfulness-based stress reduction. Difference in psychological distress between baseline (T0) and post-intervention (T1) were analyzed by repeated measure analysis of covariance. Mixed linear models were applied to assess moderating effects. Depressive symptoms, generalized anxiety symptoms, self-efficacy, and mindfulness were compared between baseline (T0) and post-intervention (T1) via t-tests. Usability of the “CoPE It” intervention and participants' satisfaction was evaluated by calculation means and frequencies.
Results: Primary outcome: A significant effect of time on psychological distress at post-intervention (T1) after controlling for age, gender, education, mental illness and attitudes toward online interventions was found. Depressive and anxiety symptoms, and mindfulness were a significant moderators of the relationship between time and psychological distress for consistent wording. Secondary outcomes: There was a significant decrease in depressive symptoms and generalized anxiety, and a significant increase in self-efficacy and mindfulness between baseline (T0) and post-intervention (T1). Tertiary outcomes: 95.83% of the participants thought the “CoPE It” intervention was easy to use and 87.50% were satisfied with the “CoPE It” intervention in an overall, general sense.
Conclusion: The e-mental health “CoPE It” intervention seems to be an effective approach in reducing psychological distress, anxiety and depressive symptoms, and in enhancing self-efficacy and mindfulness during the COVID-19 pandemic. Participants' satisfaction and the program‘s feasibility, and usability were proven to be high.
Clinical Trial Registration: www.ClinicalTrials.gov, identifier: DRKS00021301.
Introduction
In December 2019 the first case of the novel SARS-CoV-2 virus was reported in China (1). Since then, the spread of the virus reached the status of a pandemic, with 212,357,898 people infected and 4,439,843 reported deaths worldwide to this date (2). COVID-19 describes the disease that is caused by infection with the SARS-CoV-2 virus (3). Over the course of time, different approaches to infection control have been implemented by governments all over the world. The government of Germany initiated two lockdowns and varying regional measurements in reaction to three waves of rising infections (4). Many of those restrictions had measurable effects on everyday life and general and psychological health care (5). New virus mutants increased the pace at which COVID-19 could spread (6) and first reports on the long-time effects of infection with COVID-19, a cluster of symptoms called “Long-COVID,” suggest that the pandemic will continue to impact the world in a decisive manner (7).
Several studies investigated the psychological burden that is caused by or goes along with the COVID-19 pandemic (8). Common reactions to the pandemic events are symptoms of anxiety and depression, self-reported distress and sleep disturbance (9). High rates of post-traumatic stress disorder and psychological distress in the general population are reported across different countries (10). These findings were reproduced in data from a large sample of the German population. Since the outbreak of the COVID-19 pandemic, symptoms of depression and anxiety have increased (11, 12). The exact causes of such elevated levels of psychological burden might be manifold. For instance, people who were in quarantine and self-isolated for two weeks showed high levels of anxiety and stress, as well as low sleep quality (13), underlining the negative impact of COVID-19 restrictions on mental health. Also, the pandemic appears to systematically put already vulnerable people at disadvantage: indeed, individuals with preexisting mental health issues are particularly affected by the pandemic, now reaching concerning levels of symptom outcomes (14, 15). COVID-19-related fear represents a pandemic specific stressor that can be found across different countries (16) and highly affects individuals with high-risk diseases (17) and oncological patients (18). In terms of mental health many individuals affected by the pandemic are not attainable in a timely manner. In Lancet Psychiatry, Duan and Zhu urged governments to establish mental health care for those negatively impacted by the COVID-19 pandemic (19). Most people infected with COVID-19 either quarantine at home or are under intensive care in the hospital. Treatment of somatic symptoms of infection with COVID-19 takes priority over treatment of psychological impact. The pandemic places patients in a poor position to access mental health care and psychological treatments were reduced during the early weeks of the pandemic (20). Additionally, waiting times for psychotherapy are long since capacities for outpatient care are limited (21). Overall, since the previous literature convergingly indicates high levels of psychological distress caused by the COVID-19 pandemic, low-threshold mental health support for the general population is required, in order to avert the negative impact of this public health crisis.
The psychological impact of the COVID-19 pandemic and the difficulties in providing psychological support have suggested the need for evidence-based and innovative situation-based approaches to endorse psychological well-being (22, 23). To ensure the acceptance of these new approaches, it is necessary that they are freely accessible, anonymous, and low-threshold (24). E-mental health approaches are versatile instruments that can reach multiple people at the same time. In direct comparison to face-to-face interventions, internet-delivered cognitive behavior therapy shows similar effects in several mental and somatic disorders (25). Nevertheless, establishing e-mental health approaches in health care face several barriers. A study conducted before the outbreak of the pandemic observed ambivalent or negative attitudes toward therapies that were delivered online and the intention to use such therapy approaches was low, even though the participants expected health care improvements if e-mental health approaches were implemented (26). Possible barriers to the use of e-mental health interventions may be concerns about data privacy, lack of quality standards and missing research regarding risks and side effects (27). Personal barriers include–among other factors–time and level of stress (28). For instance, one study assessing the intention to use digital psychodiabetology during the pandemic showed moderate acceptance of such interventions (29).
The ongoing pandemic has already constituted a collective stress test for the implementation of several different eHealth approaches into medical care in order to decrease risk of infection with COVID-19 in face-to-face health care. During the ongoing pandemic, new and digital patient care approaches (e.g., tele-rehabilitation) were rapidly established. These approaches have proven to be highly accepted, satisfying and feasible expansions to medical care (30–35). Regarding e-mental health approaches to face pandemic related distress there is only limited evidence. In fact, there is only one study assessing the efficacy of a therapist-guided online therapy compared to self-help internet-based therapy (36). The goal of this study was to reduce COVID-19-induced anxiety and depression. The study showed that in both groups the levels of anxiety and depression symptoms were reduced, although the reduction in the therapist-guided group was higher. However, it is important to highlight, that this study was not conceptualized to assess the efficacy of a self-guided e-mental health intervention. One different study provides an overview of the intervention protocol of an app-based psychological group intervention as well as preliminary baseline data (37). One study applying qualitative research methods showed overall good acceptance of telehealth to foster mental health. Nevertheless, positive experience of telehealth services were dependent on several factors, including assured support and, comfortable access (38).
These observations demonstrate that we are currently experiencing a shift in establishing new health care approaches, from mandatorily classic face-to-face treatments toward internet-based modalities. However, this development needs to be guided by evidence-based decisions regarding e-mental health interventions in order to quickly adapt to the psychological burden of the general population as well as different patient groups. Only by implementing innovative and easily accessible approaches can the negative impact of the COVID-19 pandemic be reduced at an early stage (39).
The self-guided e-mental health intervention “CoPE It” offers low-threshold support to those who are highly impacted by the psychological strain of the COVID-19 pandemic (40). “CoPE It” is part of the structured clinical approach “Coping with Corona: Extended Psychosomatic care in Essen” (CoPE), which targets psychologically burdened people in Essen, Germany (41). The aim of this study was to assess the effectiveness, usability, and participants' satisfaction with the e-mental health intervention “CoPE It” during the COVID-19 pandemic. The ongoing public health crisis has spotlighted the need for adaption to restrictions of social life and therefore the development of innovative, evidence-based interventions to offer care should be in the focus of clinical research (42). E-mental health interventions like “CoPE It” can bridge the supply gap for higher-threshold interventions like face-to-face therapy.
It was hypothesized that the e-mental health intervention “CoPE It” reduces participants' psychological distress (primary outcome). Secondary hypotheses were that “CoPE It” reduces anxiety and depression symptoms and increases self-efficacy and mindfulness among participants (secondary outcomes). It was further hypothesized that usability of “CoPE It” and satisfaction with the e-mental health intervention would be evaluated positively by participants (tertiary outcomes).
Materials and Methods
Procedure and Participants
The previously published study protocol offers an in-depth overview of the methods of the conducted study (43). To investigate the effectiveness of the low-threshold, e-mental health intervention “CoPE It” for psychological burdened individuals during the COVID-19 pandemic, a bicentre longitudinal study was conducted at the University Hospital Essen and University of Tübingen from April 27th 2020 to May 3rd 2021. Potential participants were recruited via the CoPE hotline [see CoPE concept for details (41)], other emergency support hotlines in Germany, via the Health Department Freudenstadt, via the distribution of flyers, from the publicly accessible website, and social media. Eligibility requirements were a good command of the German language, internet access and basic computer skills, and a minimum age of 18 years. Only participants who completed at least the first three modules (out of four) were included into imputation of missing data and statistical analysis. Electronic informed consent was obtained. The study was approved by the Ethics Committees of the University Hospital Essen (20-9243-BO) and University of Tübingen (469/2020BO).
“CoPE It” Intervention
The self-guided e-mental health intervention “CoPE It” was based on current literature regarding health issues and approaches toward support during the COVID-19 pandemic (44–50). The goal was a reduction of psychological distress by promoting adaptive coping strategies, self-efficacy, daily routines, sleep quality, and activating resources and physical exercises. Evidence-based methods of cognitive behavioral therapy and mindfulness-based stress reduction formed the foundation of “CoPE It” (51–53). The intervention consisted of four modules featuring different media, such as psychoeducational videos, audio-guided mindfulness exercises, and interactive skills training (e.g., planning a daily routine, stress management, activity skills, and individual skills for emotional emergencies). For an overview of the contents of the “CoPE It” intervention, see Table 1. The duration of each module was about 30 min and modules were unlocked in a two-day interval after the completion of the previous module. Details regarding the specific contents of the intervention are provided in the intervention concept and study protocol (40, 43).
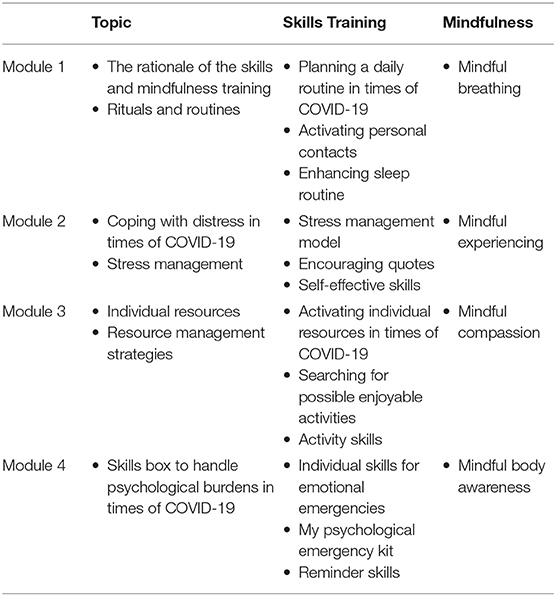
Table 1. COVID-19 adapted topics, contents, and exercises from the “CoPE It”.
Measurements
Data for outcome measures were collected via an online assessment tool integrated in the web-based “CoPE It” platform with an approximate completion time of 10–25 min before at baseline (T0) and after completion of the intervention (T1). Primary and secondary outcomes were assessed at both measure points. Attitudes toward e-mental health and demographics were assessed at baseline (T0) and the evaluation of “CoPE It” was assessed at post-intervention (T1). For each of the psychometric instruments, German versions were used. See Table 2 for the assessment schedule.
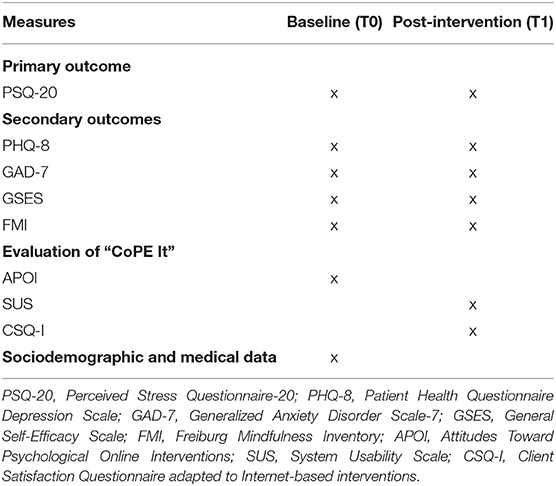
Table 2. Assessment schedule.
Primary Outcome Measures
The primary outcome is psychological distress at post-intervention (T1), assessed by the German version of the Perceived Stress Questionnaire-20 (PSQ-20) (54).
Secondary Outcome Measures
The Patient Health Questionnaire Depression Scale (PHQ-8) and the Generalized Anxiety Disorder Scale-7 (GAD-7) were used to assess depressive and anxiety symptoms (55, 56). To measure self-efficacy, the General Self-Efficacy Scale (GSE) (57) was used. The Freiburg Mindfulness Inventory (FMI) (58) was applied as a measurement of mindfulness.
Evaluation of the “CoPE It” E-Mental Health Intervention
The Attitudes Toward Psychological Online Interventions (APOI) instrument (59) was used to assess participants' attitudes toward e-mental health interventions and were considered as covariate. A modified version of the 10-item System Usability Scale (SUS) (60), the Client Satisfaction Questionnaire adapted to internet-based interventions (CSQ-I) (61) were applied for evaluation of usability and participants' satisfaction with the “CoPE It” intervention.
Sociodemographic and Medical Data
Self-generated items were used for assessment of participants' sociodemographic information. Demographic data, such as age, gender, marital status, having children, educational level, employment status, and community size were collected. Furthermore, participants were asked about their duration of internet use, prior experience with e-mental health interventions, their possible financial burden due to COVID-19 and if they were either personal affected by a COVID-19 infection or indirectly through infection in their household. Medical data consisted of somatic and mental illness and the use of psychiatric medication.
Statistical Analyses
Statistical analyses were performed using R (4.0.3). The overall percentage of missing values across the outcome and predictor variables varied between 1.33% and 1.44%, with 329 of 2,640 records (12.46%) incomplete in total. Under the assumption of missing at random, multiple imputation was used for the creation of 100 multiply imputed datasets. Incomplete outcome and predictor variables were imputed using the default settings for predictive mean matching of the ‘mice’ package (62). Repeated measure analysis of covariance (ANCOVA) was computed to determine the difference in psychological distress between baseline (T0) and post-intervention (T1). Age, gender, education, mental illness, and attitudes toward psychological online interventions were added as covariates. The variables age and attitudes toward psychological online interventions were included in the model in a standardized form. The variable somatic illness was excluded from the covariates because only 13 participants reported a somatic condition, leaving entire cells empty. Variance inflation factors (VIF) below 1.2 indicated that multicollinearity was not a concern. Partial η2 was used as effect size, with values around 0.01, 0.06, and 0.14 considered small, medium-sized, and large effects, respectively (63). Additionally, generalized estimating equations of the original model that actually could include somatic illness were calculated. Mixed linear models with the respective participant as a random intercept were applied to assess moderating effects of age, gender, education, mental illness, and baseline levels of depressive symptoms, generalized anxiety, mindfulness and attitudes toward online interventions on the effect of the intervention on the reduction of psychological distress (primary outcome). All continuous variables were standardized before analysis. There were no outliers, collinearity was low (for all variables: VIF = 1.00) and the error variance turned out to be homoscedastic, as revealed by a Breusch-Pagan-Test. Residuals were normally distributed, except for the model including mindfulness as a moderator. Shapiro-Wilk tests indicated normality of random effects for all models of significant moderating effects. For the secondary outcomes, two-sided paired t-test comparing depressive symptoms, generalized anxiety, self-efficacy, and mindfulness between baseline (T0) and post-intervention (T1) were conducted. Due to the sample size, normal distribution was assumed (64). Cohen's d was used as effect size, with values around 0.2, 0.5, and 0.8 being considered small, medium, and large effects, respectively (63). To evaluate the “CoPE It” e-mental health intervention, distributions, means and sum scores for SUS and CSQ-I were computed.
Results
Study Population
The baseline-data from 440 individuals was collected, of which 114 participants finished module 3 and 4. One hundred thirty-eight participants completed the T0 assessment but did not start the first module. One hundred twenty-eight participants dropped out of the study after the first module and 60 participants dropped out after the second module. The overall dropout rate of this study was 74.09%. Four participants were excluded because they did not fulfill the participation requirements and 110 participants were included into imputation of missing data and data analysis.
Of the 110 participants, 92 (83.6%) were female and the mean age was M = 45.09 (SD = 14.03). Ninety-three participants (84.5%) had general higher education or entrance qualification for general higher education. Sixty-three participants (57.3%) reported a diagnosis of mental illness in the past. Most participants (n = 97, 88.2%) had never used an e-mental health intervention before. For a more detailed sample size description, see Table 3.
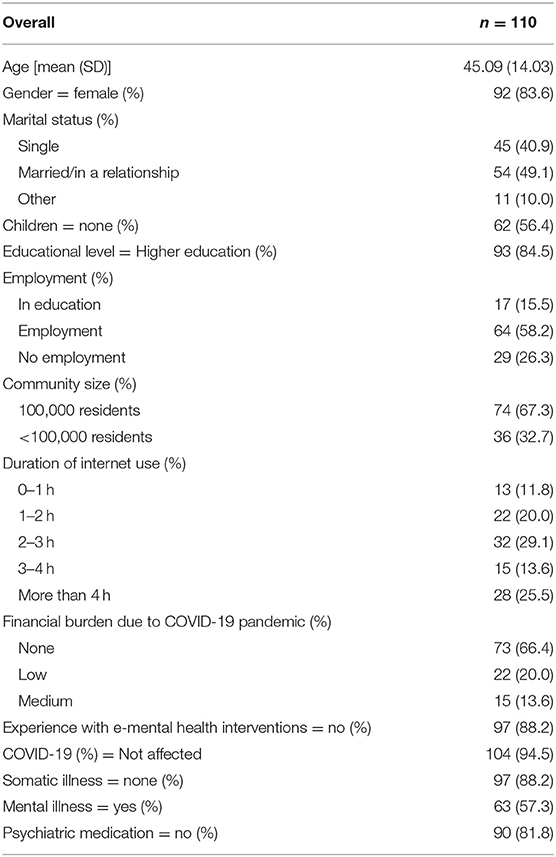
Table 3. Sociodemographic and medical data.
Primary Outcome Measure: Perceived Stress Questionnaire-20
PSQ-20 scores range between 20 and 80, with higher scores indicating a higher level of psychological distress. PSQ-20-scores were higher at baseline (M = 48.26, SD = 19.35) than at post-intervention (M = 31.95, SD = 21.51). An ANCOVA revealed a significant effect of time on psychological distress at post-intervention (T1) after controlling for age, gender, education, mental illness, and attitudes toward online interventions [F(1, 104) = 22.41, p < 0.001, = 0.18]. Similar results were found in the conducted generalized estimating equations (see Supplementary Material).
Moderation Analyses
Depressive and anxiety symptoms were a significant moderator of the relationship between time and psychological distress [coefficient PHQ-8*timepoint: β = 0.133, t(108) = 3.00, p = 0.003; coefficient GAD-7*timepoint: β = 0.136, t(108) = 3.08, p = 0.003]. Furthermore, mindfulness significantly moderated the relationship between time and psychological distress (coefficient FMI*timepoint: β = −0.145, t(108) = −3.39, p = 0.001). Estimated marginal effect analyses (see Supplementary Material) suggest that the higher the levels of depressive symptoms and anxiety at T0, and the lower the baseline mindfulness, the larger the effect of the “CoPE It” intervention was. For purposes of illustration of these moderation effects, the sample was divided into tertiles with regard to the respective PHQ-8-, GAD-7-, and FMI-scores and depicted in Figure 1.
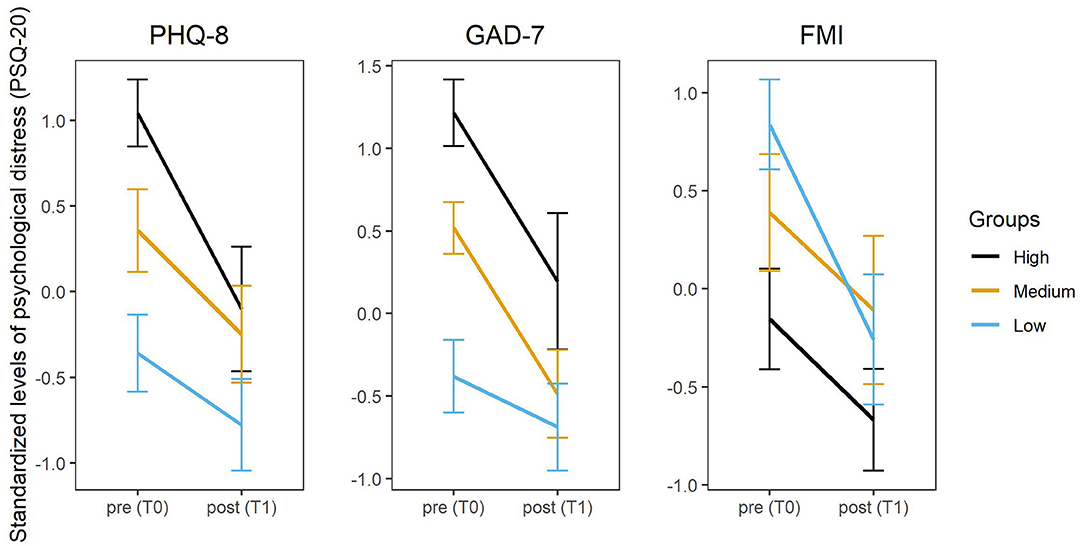
Figure 1. Change of psychological distress (PSQ-20) from baseline (T0) to post-intervention (T1) by group (high, medium, low scores for PHQ-8, GAD-7, and FMI). PHQ-8, Patient Health Questionnaire Depression Scale; GAD-7, Generalized Anxiety Disorder Scale-7; FMI, Freiburg Mindfulness Inventory.
Secondary Outcome Measures: Depressive Symptoms, Generalized Anxiety, Self-Efficacy, and Mindfulness
A measurable and significant change occurred between baseline (T0) and post-intervention (T1) in depressive symptoms [t(109) = 6.45, p < 0.001, d = 0.615], generalized anxiety [t(109) = 6.96, p < 0.001, d = 0.663], self-efficacy [t(109) = −4.59, p < 0.001, d = 0.438], and mindfulness [t(109) = −8.98, p < 0.001, d = 0.856]. The results are depicted in Table 4.
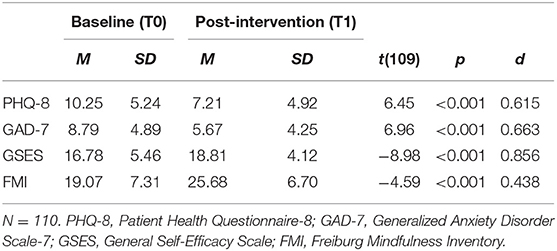
Table 4. Results of two-sided paired t-tests for secondary outcomes.
Evaluation of the “CoPE It” E-Mental Health Intervention
SUS scores range between 0 and 100, with higher scores indicating a higher level of usability. For this sample, the SUS score was M = 86.18 (SD = 10.20, Mdn = 86.25). 95.83% of the participants thought that “CoPE It” was easy to use and 87.50% found the various functions in the “CoPE It” intervention to be well-integrated. Further, 88.89% of the participants responded that they would imagine that most people would learn to use this intervention very quickly and 95.83% felt very confident using the system.
CSQ-I scores have a range from 8 to 32, with higher scores indicating higher satisfaction. In this study, the CSQ-I was M = 16.99 (SD = 5.61, Mdn = 18). 94.44% of the participants thought that the “CoPE It” intervention was of high quality. Furthermore, 87.50% of the participants were satisfied with the “CoPE It” intervention in an overall, general sense and 77.78% would come back to such an intervention if they were to seek help again.
Discussion
The aim of this study was to assess the effectiveness of the e-mental health “CoPE It” intervention, to assess its usability, and participants' satisfaction with the intervention. Participants in the “CoPE It” intervention reported a significant and relevant reduction in psychological distress after using the intervention. The effect was not dependent on age, gender, education, mental illness or attitudes toward online interventions. Higher levels of anxiety and depression at baseline, and lower levels of mindfulness before the intervention were associated with a larger effect of the “CoPE It” intervention. Further, after partaking in the e-mental health “CoPE It” intervention, depressive and anxiety symptoms were lower than before the intervention, while self-efficacy and mindfulness were increased afterwards. Participants evaluated the usability of the intervention as high and were satisfied with the intervention.
Given the results of this study, “CoPE It” seems to have enabled a reduction in psychological distress for individuals during the ongoing COVID-19 pandemic. A large effect was observed. The successful management of distress through evidence-based low-threshold instruments like “CoPE It” provides an innovative approach for prevention of mental health disorders and effective methods to reduce mental burden arising through crises affecting the whole population, such as the COVID-19 pandemic (65, 66). In this study, it was shown that “CoPE It” fulfills these demands and is a helpful intervention in the COVID-19 pandemic to face to increased psychological burden (12). This result is in line with previous research establishing mindfulness-based online interventions and internet-delivered cognitive behavior therapy as effective interventions for stress reduction (25, 53, 67). These new forms of interventions can be applied in everyday clinical practice, therefore lowering the barrier for accessible and low-threshold mental health care.
Even though all participants benefited from the intervention, the positive effect of psychological distress reduction was particularly evident for individuals with higher scores of depressive symptoms and anxiety, as well as participants who reported less mindfulness states at baseline assessment. Similar results were found in an Italian study with female teachers who received a mindfulness training (68). Those with low resilience showed a greater improvement in depression, anxiety, and psychological well-being than those with already high resilience. These observations suggest that “CoPE It” is a valid option to support individuals with a high burden of psychological distress and introduce mindfulness to those who experience less mindfulness in everyday life.
Further, the “CoPE It” intervention reduced symptoms of depression and anxiety. High effect sizes were observed. In accordance with other research, this study provides additional evidence that e-mental health interventions may be able to successfully alleviate the burden of depression and anxiety symptoms (69, 70). This is of particular value since most studies reported an increase in symptoms of depression and anxiety during the pandemic (10–12). The “CoPE It” intervention provides a benefit for those with an already high psychological burden who are in urgent need of support through mental health care.
After participating in the “CoPE It” study, an increase in self-efficacy and mindfulness could be observed. High to moderate effect sizes were found. These skills are important resources for good mental health and dealing with stressful life events (71, 72). Self-efficacy has been found to be a protective factor for nurses working in Wuhan from anxiety related to the COVID-19 pandemic (73). The positive effect of self-efficacy is not limited to health care workers, the general population benefits from self-efficacy as a protective factor against COVID-19 related anxiety, as well (74). High self-efficacy has also been associated with lower psychological distress caused by the COVID-19 pandemic (75). Another study could observe the negative effects of the ongoing pandemic on student's academic self-efficacy (76). Mindfulness has been found to increase well-being, even during the COVID-19 pandemic (77, 78) and was found to comprise a buffering influence on the relationship between fear of COVID-19 and hopelessness (79). Furthermore, there might be a direct impact on the infection risk for COVID-19 since mindfulness is associated with greater engagement in social distancing (80). Enhancing functional coping skills does not only provide protection for the general population but does also mitigate the psychological strain of those with depressive and anxiety symptoms.
Participants in this study reported that they would use the “CoPE It” intervention frequently and almost all participants found the “CoPE It” intervention easy to use and were confident in using the platform. Further, the “CoPE It” intervention was considered helpful for existing problems by a large proportion of participants and participants of this study expressed that it was likely that they would use the intervention again. These findings are in line with research regarding other e-mental health interventions which revealed participants' high satisfaction, usability and acceptance (81, 82). Satisfaction with the intervention was generally good. Regarding usability, responses were also very positive, indicate an user-friendly web-based approach. The results of satisfaction und usability assessment show that the acceptance of “CoPE It” is comparable to other low-threshold interventions.
Global health crises such as the COVID-19 pandemic present a risk for new onset of mental disorders and worsening of existing symptoms such as depression and anxiety. Additionally to these findings, increased psychological distress is a central result of a population-wide strain (74). The e-mental health “CoPE It” intervention addresses these pandemic related strains and offers substantial support to overcome these burdens. Evidence-based e-mental health interventions such as “CoPE It” are urgently needed and are of great value if they can provide relief in times of restrictions even without face to face contact.
Limitations
The primary limitation is the absence of a control group. Therefore, randomization of study participants could not be performed. Due to non-randomization it could not be ruled out that other factors besides the “CoPE It” intervention may have positively affected the participants. For example, the participants may have adapted to the challenges of the ongoing pandemic over time, thus decreasing the negative effect of pandemic stressors on their mental health. However, this consideration does not explain the increase in mindfulness observed in the study. The results of the e-mental health “CoPE It” intervention are promising, even though it is not yet possible to clearly evaluate its efficiency. A randomized controlled trial to clearly evaluate the effectiveness of the “CoPE It” intervention is needed. However, due to the high psychological distress caused by the pandemic, which affects most people, conducting a randomized controlled trial was ethical not reasonable from our point of view. Because only post-intervention effects were analyzed, no conclusion can be drawn about the long-term effects of the intervention. Further studies with longer follow-up periods are needed to investigate the duration of treatment effects. Moreover, the sample of this study was mostly composed of women with higher education, underlying the need for further studies with a more representative sample of participants. Women seem to be particularly psychologically burdened by the pandemic (8, 9, 12). Since only a few participants were affected by somatic illness or infection of COVID-19, the intervention may have been tested on a group that is less burdened than those in need of e-mental health interventions.
Conclusion
The e-mental health “CoPE It” intervention seems to be an effective approach in reducing psychological distress, anxiety and depressive symptoms, and enhancing self-efficacy and mindfulness during the COVID-19 pandemic. Participants' satisfaction, and the program‘s feasibility and usability were high. In times of public contact restriction and strain on the health care system, low-threshold e-mental health programs like “CoPE It” could potentially bridge the supply gap of interventions for mentally burdened people.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committees of the Medical Faculty of the University of Duisburg-Essen (20-9243-BO) and the Ethics Committees of the Medical Faculty of the University of Tübingen (469/2020BO). The participants provided their electronic informed consent to participate in this study.
Author Contributions
AB, E-MS, and MT initiated the study. AB, JG, E-MS, and MT contributed to designing the study and developing the intervention. AB administering the trial and drafted the manuscript with LJ. CJ developed the information technology structure for the study and intervention as well as contributing to preparing the manuscript. Statistical analyses were conducted by LJ, AS, and AB. JG, E-MS, MT, MF, VM, AS, BW, HD, ND, and FJ contributed to the preparation of the manuscript. All authors supported recruitment of the participants and read and approved the final manuscript.
Funding
We acknowledge support by the Open Access Publication Fund of the University of Duisburg-Essen.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.768132/full#supplementary-material
Abbreviations
APOI, Attitudes Toward Psychological Online Interventions; CoPE, Coping with Corona: Extended Psychosomatic care in Essen; FMI, Freiburg Mindfulness Inventory; GAD-7, Generalized Anxiety Disorder Scale-7; GSE, General Self-Efficacy Scale; PHQ-8, Patient Health Questionnaire Depression Scale; PSQ-20, Perceived Stress Questionnaire-20; SUS, System Usability Scale; CSQ-I, Client Satisfaction Questionnaire adapted to internet-based interventions.
References
1. Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. (2020) 382:727–33. doi: 10.1056/NEJMoa2001017
2. World Health Organization (WHO). WHO Coronavirus (COVID-19) Dashboard. Available online at: https://covid19.who.int/ (accessed August 25, 2021).
3. World Health Organization (WHO). Coronavirus Disease (COVID-19). Available online at: https://www.who.int/health-topics/coronavirus (accessed September 30, 2021).
4. Bundesgesundheitsministerium. Coronavirus-Pandemie (SARS-CoV-2): Chronik bisheriger Maßnahmen und Ereignisse. Available online at: https://www.bundesgesundheitsministerium.de/coronavirus/chronik-coronavirus.html (accessed August 25, 2021).
5. Sheridan Rains L, Johnson S, Barnett P, Steare T, Needle JJ, Carr S, et al. Early impacts of the COVID-19 pandemic on mental health care and on people with mental health conditions: framework synthesis of international experiences and responses. Soc Psychiatry Psychiatr Epidemiol. (2021) 56:13–24. doi: 10.1007/s00127-020-01924-7
6. Otto SP, Day T, Arino J, Colijn C, Dushoff J, Li M, et al. The origins and potential future of SARS-CoV-2 variants of concern in the evolving COVID-19 pandemic. Curr Biol. (2021) 31:R918–29. doi: 10.1016/j.cub.2021.06.049
7. Aiyegbusi OL, Hughes SE, Turner G, Rivera SC, McMullan C, Chandan JS, et al. Symptoms, complications and management of long COVID: a review. J R Soc Med. (2021) 114:428–42. doi: 10.1177/01410768211032850
8. Hossain MM, Tasnim S, Sultana A, Faizah F, Mazumder H, Zou L, et al. Epidemiology of mental health problems in COVID-19: a review. F1000Res. (2020) 9:636. doi: 10.12688/f1000research.24457.1
9. Rajkumar RP. COVID-19 and mental health: a review of the existing literature. Asian J Psychiatr. (2020) 52:102066. doi: 10.1016/j.ajp.2020.102066
10. Xiong J, Lipsitz O, Nasri F, Lui LMW, Gill H, Phan L, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. (2020) 277:55–64. doi: 10.1016/j.jad.2020.08.001
11. Bäuerle A, Steinbach J, Schweda A, Beckord J, Hetkamp M, Weismüller B, et al. Mental health burden of the COVID-19 outbreak in Germany: predictors of mental health impairment. J Prim Care Community Health. (2020) 11:2150132720953682. doi: 10.1177/2150132720953682
12. Bäuerle A, Teufel M, Musche V, Weismüller B, Kohler H, Hetkamp M, et al. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: a cross-sectional study in Germany. J Public Health (Oxf). (2020) 42:672–8. doi: 10.1093/pubmed/fdaa106
13. Xiao H, Zhang Y, Kong D, Li S, Yang N. Social capital and sleep quality in individuals who self-isolated for 14 days during the coronavirus disease 2019 (COVID-19) outbreak in January 2020 in China. Med Sci Monit. (2020) 26:e923921. doi: 10.12659/MSM.923921
14. Murphy L, Markey KCOD, Moloney M, Doody O. The impact of the COVID-19 pandemic and its related restrictions on people with pre-existent mental health conditions: a scoping review. Arch Psychiatr Nurs. (2021) 35:375–94. doi: 10.1016/j.apnu.2021.05.002
15. Skoda EM, Bäuerle A, Schweda A, Dörrie N, Musche V, Hetkamp M, et al. Severely increased generalized anxiety, but not COVID-19-related fear in individuals with mental illnesses: a population based cross-sectional study in Germany. Int J Soc Psychiatry. (2021) 67:550–8. doi: 10.1177/0020764020960773
16. Luo F, Ghanei Gheshlagh R, Dalvand S, Saedmoucheshi S, Li Q. Systematic review and meta-analysis of fear of COVID-19. Front Psychol. (2021) 12:661078. doi: 10.3389/fpsyg.2021.661078
17. Kohler H, Bäuerle A, Schweda A, Weismüller B, Fink M, Musche V, et al. Increased COVID-19-related fear and subjective risk perception regarding COVID-19 affects behavior in individuals with internal high-risk diseases. J Prim Care Community Health. (2021) 12:2150132721996898. doi: 10.1177/2150132721996898
18. Musche V, Kohler H, Bauerle A, Schweda A, Weismuller B, Fink M, et al. COVID-19-related fear, risk perception, and safety behavior in individuals with diabetes. Healthcare (Basel). (2021) 9:480. doi: 10.3390/healthcare9040480
19. Duan L, Zhu G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry. (2020) 7:300–2. doi: 10.1016/S2215-0366(20)30073-0
20. Probst T, Stippl P, Pieh C. Changes in provision of psychotherapy in the early weeks of the COVID-19 lockdown in Austria. Int J Environ Res Public Health. (2020) 17:3815. doi: 10.3390/ijerph17113815
21. Grunzig SD, Baumeister H, Bengel J, Ebert D, Kramer L. Effectiveness and acceptance of a web-based depression intervention during waiting time for outpatient psychotherapy: study protocol for a randomized controlled trial. Trials. (2018) 19:285. doi: 10.1186/s13063-018-2657-9
22. da Silva JA, Siegmund G, Bredemeier J. Crisis interventions in online psychological counseling. Trends Psychiatry Psychother. (2015) 37:171–82. doi: 10.1590/2237-6089-2014-0026
23. Moreno C, Wykes T, Galderisi S, Nordentoft M, Crossley N, Jones N, et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry. (2020) 7:813–24. doi: 10.1016/S2215-0366(20)30307-2
24. Fiorillo A, Gorwood P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur Psychiatry. (2020) 63:e32. doi: 10.1192/j.eurpsy.2020.35
25. Andersson G. Internet-delivered psychological treatments. Annu Rev Clin Psychol. (2016) 12:157–79. doi: 10.1146/annurev-clinpsy-021815-093006
26. Apolinario-Hagen J, Vehreschild V, Alkoudmani RM. Current views and perspectives on e-mental health: an exploratory survey study for understanding public attitudes toward internet-based psychotherapy in Germany. JMIR Ment Health. (2017) 4:e8. doi: 10.2196/mental.6375
27. Kohnen M, Dirmaier J, Harter M. [Potentials and Challenges of E-Mental Health Interventions in Mental Health Care]. Fortschr Neurol Psychiatr. (2019) 87:160–4. doi: 10.1055/a-0853-2568
28. Eccles H, Nannarone M, Lashewicz B, Attridge M, Marchand A, Aiken A, et al. Barriers to the use of web-based mental health programs for preventing depression: qualitative study. JMIR Form Res. (2021) 5:e16949. doi: 10.2196/16949
29. Damerau M, Teufel M, Musche V, Dinse H, Schweda A, Beckord J, et al. Determining acceptance of e-mental health interventions in digital psychodiabetology using a quantitative web-based survey: cross-sectional study. JMIR Form Res. (2021) 5:e27436. doi: 10.2196/27436
30. Magliah SF, Alsabban AS, Turkistani HA, Abulaban BA, Alsharif AH, Alsharif SS, et al. Perception of virtual clinics among Saudi adults with type 1 diabetes during the COVID-19 pandemic. Diabetes Metab Syndr. (2021) 15:102175. doi: 10.1016/j.dsx.2021.06.012
31. Houston E, Kennedy AG, O'Malley D, Rabinowitz T, Rose GL, Boyd J. Telemedicine in neurology: a scoping review of key outcomes in movement disorders. Telemed J E Health. (2021). doi: 10.1089/tmj.2021.0117
32. Mukaino M, Tatemoto T, Kumazawa N, Tanabe S, Katoh M, Saitoh E, et al. Staying active in isolation: telerehabilitation for individuals with the severe acute respiratory syndrome coronavirus 2 infection. Am J Phys Med Rehabil. (2020) 99:478–9. doi: 10.1097/PHM.0000000000001441
33. Deeb W, Hess CW, Gamez N, Patel B, Moore K, Armstrong MJ. Response to telemedicine visits from patients with parkinsonism during the covid-19 pandemic on postvisit surveys. J Patient Exp. (2021) 8:2374373521997224. doi: 10.1177/2374373521997224
34. Mortezavi M, Lokineni S, Garg M, Chen YL, Ramsey A. Rheumatology patient satisfaction with telemedicine during the COVID-19 pandemic in the United States. J Patient Exp. (2021) 8:23743735211008825. doi: 10.1177/23743735211008825
35. Micallef M, Hurley S, Brell N, Cook R, Post J, Overton K. Telehealth outpatient coronavirus disease 2019 case management at a tertiary hospital in Sydney. J Telemed Telecare. (2021) 1357633X211024097. doi: 10.1177/1357633X211024097
36. Al-Alawi M, McCall RK, Sultan A, Al Balushi N, Al-Mahrouqi T, Al Ghailani A, et al. Efficacy of a six-week-long therapist-guided online therapy versus self-help internet-based therapy for COVID-19-induced anxiety and depression: open-label, pragmatic, randomized controlled trial. JMIR Ment Health. (2021) 8:e26683. doi: 10.2196/26683
37. Parolin LAL, Benzi IMA, Fanti E, Milesi A, Cipresso P, Preti E. Italia Ti Ascolto [Italy, I am listening]: an app-based group psychological intervention during the COVID-19 pandemic. Res Psychother. (2021) 24:517. doi: 10.4081/ripppo.2021.517
38. Venville A, O'Connor S, Roeschlein H, Ennals P, McLoughlan G, Thomas N. Mental health service user and worker experiences of psychosocial support via telehealth through the COVID-19 pandemic: qualitative study. JMIR Ment Health. (2021) 8:e29671. doi: 10.2196/29671
39. Wind TR, Rijkeboer M, Andersson G, Riper H. The COVID-19 pandemic: the 'black swan' for mental health care and a turning point for e-health. Internet Interv. (2020) 20:100317. doi: 10.1016/j.invent.2020.100317
40. Bäuerle A, Graf J, Jansen C, Dörrie N, Junne F, Teufel M, et al. An e-mental health intervention to support burdened people in times of the COVID-19 pandemic: CoPE It. J Public Health (Oxf). (2020) 42:647–8. doi: 10.1093/pubmed/fdaa058
41. Bäuerle A, Skoda EM, Dörrie N, Böttcher J, Teufel M. Psychological support in times of COVID-19: the Essen community-based CoPE concept. J Public Health (Oxf). (2020) 42:649–50. doi: 10.1093/pubmed/fdaa053
42. Liu S, Yang L, Zhang C, Xiang Y-T, Liu Z, Hu S, et al. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry. (2020) 7:e17–e8. doi: 10.1016/S2215-0366(20)30077-8
43. Bäuerle A, Graf J, Jansen C, Musche V, Schweda A, Hetkamp M, et al. E-mental health mindfulness-based and skills-based 'CoPE It' intervention to reduce psychological distress in times of COVID-19: study protocol for a bicentre longitudinal study. BMJ Open. (2020) 10:e039646. doi: 10.1136/bmjopen-2020-039646
44. Hao F, Tan W, Jiang L, Zhang L, Zhao X, Zou Y, et al. Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain Behav Immun. (2020) 87:100–6. doi: 10.1016/j.bbi.2020.04.069
45. Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. (2020) 17:1729. doi: 10.3390/ijerph17051729
46. Wang C, Pan R, Wan X, Tan Y, Xu L, McIntyre RS, et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav Immun. (2020) 87:40–8. doi: 10.1016/j.bbi.2020.04.028
47. Behan C. The benefits of meditation and mindfulness practices during times of crisis such as COVID-19. Ir J Psychol Med. (2020) 37:256–8. doi: 10.1017/ipm.2020.38
48. Chew NWS, Lee GKH, Tan BYQ, Jing M, Goh Y, Ngiam NJH, et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav Immun. (2020) 88:559–65. doi: 10.1016/j.bbi.2020.04.049
49. Zhou X, Snoswell CL, Harding LE, Bambling M, Edirippulige S, Bai X, et al. The role of telehealth in reducing the mental health burden from COVID-19. Telemed J E Health. (2020) 26:377–9. doi: 10.1089/tmj.2020.0068
50. Ho CS, Chee CY, Ho RC. Mental health strategies to combat the psychological impact of COVID-19 beyond paranoia and panic. Ann Acad Med Singapore. (2020) 49:1–3. doi: 10.47102/annals-acadmedsg.202043
51. Dobson D, Dobson KS. Evidence-Based Practice of Cognitive-Behavioral Therapy. New York, NY: Guilford Publications (2018).
52. Mak WW, Tong AC, Yip SY, Lui WW, Chio FH, Chan AT, et al. Efficacy and moderation of mobile app-based programs for mindfulness-based training, self-compassion training, and cognitive behavioral psychoeducation on mental health: randomized controlled noninferiority trial. JMIR Ment Health. (2018) 5:e60. doi: 10.2196/mental.8597
53. Spijkerman MP, Pots WT, Bohlmeijer ET. Effectiveness of online mindfulness-based interventions in improving mental health: a review and meta-analysis of randomised controlled trials. Clin Psychol Rev. (2016) 45:102–14. doi: 10.1016/j.cpr.2016.03.009
54. Fliege H, Rose M, Arck P, Levenstein S, Klapp BF. Validierung des “perceived stress questionnaire”(PSQ) an einer deutschen Stichprobe [Validation of the “helidatio Stress Questionnaireased:/ in a German sample]. Diagnostica. (2001) 47:142–52. doi: 10.1026//0012-1924.47.3.142
55. Kroenke K, Strine TW, Spitzer RL, Williams JB, Berry JT, Mokdad AH. The PHQ-8 as a measure of current depression in the general population. J Affect Disord. (2009) 114:163–73. doi: 10.1016/j.jad.2008.06.026
56. Spitzer RL, Kroenke K, Williams JB, Lowe B, A. brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
57. Schwarzer R, Jerusalem M editors. Skalen zur erfassung von Lehrer-und schülermerkmalen. Dokumentation der psychometrischen Verfahren im Rahmen der Wissenschaftlichen Begleitung des Modellversuchs Selbstwirksame Schulen. Berlin: Freie Universität Berlin (1999).
58. Walach H, Buchheld N, Buttenmüller V, Kleinknecht N, Schmidt S. Measuring mindfulness—the Freiburg Mindfulness Inventory (FMI). Pers Individ Dif. (2006) 40:1543–55. doi: 10.1016/j.paid.2005.11.025
59. Schroder J, Sautier L, Kriston L, Berger T, Meyer B, Spath C, et al. Development of a questionnaire measuring attitudes towards psychological online interventions-the APOI. J Affect Disord. (2015) 187:136–41. doi: 10.1016/j.jad.2015.08.044
61. Boss L, Lehr D, Reis D, Vis C, Riper H, Berking M, et al. Reliability and validity of assessing user satisfaction with web-based health interventions. J Med Internet Res. (2016) 18:e234. doi: 10.2196/jmir.5952
62. van Buuren S, Groothuis-Oudshoorn K. Mice: multivariate imputation by chained equations in R. J Stat Softw. (2011) 45:1–67. doi: 10.18637/jss.v045.i03
63. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Cambridge, MA: Academic Press (2013).
64. Schmidt AF, Finan C. Linear regression and the normality assumption. J Clin Epidemiol. (2018) 98:146–51. doi: 10.1016/j.jclinepi.2017.12.006
65. Drissi N, Ouhbi S, Marques G. de la Torre Diez I, Ghogho M, Janati Idrissi MA. A Systematic Literature Review on e-Mental Health Solutions to Assist Health Care Workers During COVID-19. Telemed J E Health. (2021) 27:594–602. doi: 10.1089/tmj.2020.0287
66. Torous J, Jan Myrick K, Rauseo-Ricupero N, Firth J. Digital mental health and COVID-19: using technology today to accelerate the curve on access and quality tomorrow. JMIR Ment Health. (2020) 7:e18848. doi: 10.2196/18848
67. Jayewardene WP, Lohrmann DK, Erbe RG, Torabi MR. Effects of preventive online mindfulness interventions on stress and mindfulness: a meta-analysis of randomized controlled trials. Prev Med Rep. (2017) 5:150–9. doi: 10.1016/j.pmedr.2016.11.013
68. Matiz A, Fabbro F, Paschetto A, Cantone D, Paolone AR, Crescentini C. Positive impact of mindfulness meditation on mental health of female teachers during the COVID-19 outbreak in Italy. Int J Environ Res Public Health. (2020) 17:6450. doi: 10.3390/ijerph17186450
69. Saddichha S, Al-Desouki M, Lamia A, Linden IA, Krausz M. Online interventions for depression and anxiety–a systematic review. Health Psychol Behav Med. (2014) 2:841–81. doi: 10.1080/21642850.2014.945934
70. Wei N, Huang BC, Lu SJ, Hu JB, Zhou XY, Hu CC, et al. Efficacy of internet-based integrated intervention on depression and anxiety symptoms in patients with COVID-19. J Zhejiang Univ Sci B. (2020) 21:400–4. doi: 10.1631/jzus.B2010013
71. Janssen M, Heerkens Y, Kuijer W, van der Heijden B, Engels J. Effects of mindfulness-based stress reduction on employees' mental health: a systematic review. PLoS ONE. (2018) 13:e0191332. doi: 10.1371/journal.pone.0191332
72. Penacoba C, Catala P, Velasco L, Carmona-Monge FJ, Garcia-Hedrera FJ, Gil-Almagro F. Stress and quality of life of intensive care nurses during the COVID-19 pandemic: self-efficacy and resilience as resources. Nurs Crit Care. (2021) doi: 10.1111/nicc.12690
73. Mo Y, Deng L, Zhang L, Lang Q, Pang H, Liao C, et al. Anxiety of nurses to support Wuhan in fighting against COVID-19 epidemic and its correlation with work stress and self-efficacy. J Clin Nurs. (2021) 30:397–405. doi: 10.1111/jocn.15549
74. Petzold MB, Bendau A, Plag J, Pyrkosch L, Mascarell Maricic L, Betzler F, et al. Risk, resilience, psychological distress, and anxiety at the beginning of the COVID-19 pandemic in Germany. Brain Behav. (2020) 10:e01745. doi: 10.1002/brb3.1745
75. Shacham M, Hamama-Raz Y, Kolerman R, Mijiritsky O, Ben-Ezra M, Mijiritsky E. COVID-19 factors and psychological factors associated with elevated psychological distress among dentists and dental hygienists in Israel. Int J Environ Res Public Health. (2020) 17:2900. doi: 10.3390/ijerph17082900
76. Alemany-Arrebola I, Rojas-Ruiz G, Granda-Vera J, Mingorance-Estrada AC. Influence of COVID-19 on the perception of academic self-efficacy, state anxiety, and trait anxiety in college students. Front Psychol. (2020) 11:570017. doi: 10.3389/fpsyg.2020.570017
77. Conversano C, Di Giuseppe M, Miccoli M, Ciacchini R, Gemignani A, Orru G. Mindfulness, age and gender as protective factors against psychological distress during COVID-19 pandemic. Front Psychol. (2020) 11:1900. doi: 10.3389/fpsyg.2020.01900
78. Zheng MX, Masters-Waage TC, Yao J, Lu Y, Tan N, Narayanan J. Stay mindful and carry on: mindfulness neutralizes COVID-19 stressors on work engagement via sleep duration. Front Psychol. (2020) 11:610156. doi: 10.3389/fpsyg.2020.610156
79. Saricali M, Satici SA, Satici B, Gocet-Tekin E, Griffiths MD. Fear of COVID-19, mindfulness, humor, and hopelessness: a multiple mediation analysis. Int J Ment Health Addict. (2020) 1–14. doi: 10.1007/s11469-020-00419-5
80. Haliwa I, Lee J, Wilson J, Shook NJ. Mindfulness and engagement in COVID-19 preventive behavior. Prev Med Rep. (2020) 20:101246. doi: 10.1016/j.pmedr.2020.101246
81. Kohnen M, Dreier M, Freuck J, Harter M, Dirmaier J. [Acceptance and Use of the e-Mental Health Website–www.psychenet.de]. Psychiatr Prax. (2021). doi: 10.1055/a-1502-0961
82. van der Aa HP, van Rens GH, Verbraak FD, Bosscha M, Comijs HC, van Nispen RM. Anxiety and depression in patients who receive anti-VEGF treatment and the usability and feasibility of e-mental health support: the E-PsEYE pilot study. Ophthalmic Physiol Opt. (2021) 41:808–19. doi: 10.1111/opo.12837
Keywords: COVID-19, e-mental health, psychological distress, mindfulness, self-efficacy, online intervention, anxiety, depression
Citation: Bäuerle A, Jahre L, Teufel M, Jansen C, Musche V, Schweda A, Fink M, Dinse H, Weismüller B, Dörrie N, Junne F, Graf J and Skoda E-M (2021) Evaluation of the E-Mental Health Mindfulness-Based and Skills-Based “CoPE It” Intervention to Reduce Psychological Distress in Times of COVID-19: Results of a Bicentre Longitudinal Study. Front. Psychiatry 12:768132. doi: 10.3389/fpsyt.2021.768132
Received: 01 September 2021; Accepted: 11 October 2021;
Published: 04 November 2021.
Edited by:
Charlotte R. Blease, Beth Israel Deaconess Medical Center and Harvard Medical School, United StatesReviewed by:
Wanderson Moreira, University of São Paulo, BrazilLing Wang, King's College London, United Kingdom
Copyright © 2021 Bäuerle, Jahre, Teufel, Jansen, Musche, Schweda, Fink, Dinse, Weismüller, Dörrie, Junne, Graf and Skoda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martin Teufel, bWFydGluLnRldWZlbEB1bmktZHVlLmRl
†These authors have contributed equally to this work and share last authorship