 Giulio Perugi1Paola Calò2
Giulio Perugi1Paola Calò2 Sergio De Filippis3
Sergio De Filippis3 Gianluca Rosso4,5
Gianluca Rosso4,5 Antonio Vita6,7Marina Adami8Giuseppe Ascione8Joachim Morrens9
Antonio Vita6,7Marina Adami8Giuseppe Ascione8Joachim Morrens9 Dario Delmonte8*
Dario Delmonte8*- 1Department of Clinical and Experimental Medicine, University of Pisa, Pisa, Italy
- 2Mental Health Department, Azienda Sanitaria Locale Lecce, Lecce, Italy
- 3Neuropsychiatric Clinic, Villa Von Siebenthal, Genzano di Roma, Italy
- 4Department of Neurosciences ‘Rita Levi Montalcini’, University of Torino, Turin, Italy
- 5San Luigi Gonzaga University Hospital of Orbassano, Orbassano, Italy
- 6Department of Clinical and Experimental Sciences, University of Brescia, Brescia, Italy
- 7Department of Mental Health and Addiction Services, Spedali Civili Hospital, Brescia, Italy
- 8Janssen Italy, Cologno Monzese, Italy
- 9Janssen EMEA, Beerse, Belgium
Introduction: Treatment-resistant depression (TRD) is a debilitating condition affecting 20–30% of patients with major depressive disorders (MDD). Currently, there is no established standard of care for TRD, and wide variation in the clinical approach for disease management has been documented. Real-world data could help describe TRD clinical features, disease burden, and treatment outcome and identify a potential unmet medical need.
Methods: We analyzed the Italian data from a European, prospective, multicentric, observational cohort study of patients fulfilling TRD criteria by the European Medicine Agency, with moderate to severe major depressive episode, and starting a new antidepressant treatment according to routinary clinical practice. They were followed up for minimum 6 months. Treatments received throughout the study period, disease severity, health-related quality of life and functioning were prospectively recorded and analyzed.
Results: The Italian subcohort included 124 TRD patients (30.2% of patients of the European cohort; mean age 53.2 [sd = 9.8], women: 82, 66.1%). At enrollement, the mean (SD) duration of MDD was 16 years (sd = 11.1) and the mean duration of the ongoing major depressive episode (MDE) was 97.5 weeks (sd = 143.5); low scores of quality of life and functioning were reported. The most frequently antidepressant classes started at baseline (data available for 98 subjects) were selective serotonin reuptake inhibitors (SSRI, 42 patients [42.9%]) and serotonin-norepinephrine reuptake inhibitors (SNRI, 32 patients [32.7%]). In terms of treatment strategies, 50 patients (51%) started augmentation therapies, 18 (18.4%) combination therapies and 24 (24.5%) monoterapies (6 patients [6%] started a non-antidepressant drug only). Fourteen patients (11.3%) were treated with a psychosocial approach, including psychotherapy. After 6 months of treatment, clinical assessments were collected for 89 patients: 64 (71.9%) showed no response, 9 (10.1%) response without remission and 16 (18.0%) were in remission; non-responder patients showed lower quality of life and higher disability scores than responder patients.
Conclusions: In our sample of TRD patients, we documented substantial illness burden, low perceived quality of life and poor outcome, suggesting an unmet treatment need in TRD care in Italy.
Registration Number: ClinicalTrials.gov, number: NCT03373253.
Introduction
Major depressive disorder (MDD) is a highly prevalent and burdensome mental disorder (1). The lifetime risk of MDD ranges 5–18% in the general population, with considerable variations across countries (2, 3). A recent publication from the World Health Organization (WHO) reported a prevalence of about 5% for depression in the European region (4). MDD is associated with social withdrawal, functional and vocational impairment, medical morbidity and increased utilization of health care services (1). According to WHO, MDD is the main contributor to the global years lived with disability worldwide (4).
While the therapeutic goal of MDD is remission with complete functional recovery (5), a sizeable subgroup of patients reports residual or persistent symptoms of depression despite receiving evidence-based antidepressant treatments (6). Evidence indicates that the likelihood of remission decreases with consecutive treatment lines (7). In the large, US, multi-step Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study there was a significant reduction of remission chances after the second and the third treatment steps. Remission rates were 36.8% for the first and 30.6% for the second treatments, while in patients who had failed the first two treatments, the remission rate dropped to 13.7% with the third and 13% with the forth treatment steps (7). A similar pattern was observed for response rates. In addition the greatest illness burden (i.e., depression chronicity, psychiatric or general medical comorbidity) was characteristic of those who required more treatment steps.
According to the European regulatory authority, treatment resistant depression (TRD) is defined as a major depressive episode (MDE), in the context of MDD diagnosis, failing to achieve adequate response after treatment with at least two antidepressants given at adequate dose and duration (8). With this definition, TRD affects 20–30% of MDD patients (9). Other staging methods for TRD consider different parameters, precluding consensus on the prevalence of the condition (10–12).
Available evidence indicates that TRD patients experience a dramatically higher burden of illness compared to patients who respond to treatment, with more severe symptomatology, poorer quality of life, higher disability, reduced life expectancy, greater frequency of suicide attempts, and higher health care costs (13–15).
Since there are no approved drugs in Europe for the treatment of TRD, current pharmacological options in TRD are as much the same as those available for the treatment of MDD (1), and include selective serotonin reuptake inhibitors [SSRI], serotonin-norepinephrine reuptake inhibitors [SNRI], tricyclic antidepressants [TCA], monoamine oxidase inhibitors [MAOI], and atypical antidepressants (16, 17). Esketamine, in conjunction with a SSRI or SNRI, is the only drug recently approved specifically for TRD in Europe (2019) (18). Among non-pharmacological treatments, psychotherapy and neurostimulation therapies, such as transcranial magnetic stimulation (TMS) have been proposed, usually in combination with oral medications. However, their efficacy in TRD is still questionable (19). Electroconvulsive therapy (ECT) is highly effective but is not widely available in Italy (20). Other non-pharmacological approaches such as deep brain stimulation (DBS) and vagal nerve stimulation (VNS) are invasive, with safety and tolerability concerns (21).
In clinical practice, common treatment strategies to tackle non-response in MDD involve switching to an alternative antidepressant, adding an antidepressant (combination therapy) or adding an augmentation agent (usually lithium, second-generation antipsychotics [SGA] and thyroxine) to the ongoing pharmacological therapy (22). Combining antidepressants or augmenting with non-antidepressant medications are typically employed when patients achieve partial response to the initial medication regimen; however, combined therapy may be associated with more severe side effects and poor tolerability. In the case of non-response and/or poor tolerability of the initial therapy, switching to another antidepressant is a common clinical choice (23). An alternative approach is to combine common drugs with psychotherapy or neurostimulatory treatments. In any case, the optimal treatment sequence in TRD is yet to be defined.
Real-world evidence on patients with TRD is scarce (15, 24, 25), especially from European countries (26), and mainly derived from retrospective studies based on administrative databases or electronic health records (27–29). Within these studies, data on prescribing patterns and illness outcome are sparsely reported (24–26, 30). Real-world data are of paramount importance since patients included in randomized clinical trials (RCTs) of depression are poorly representative of the treatment-seeking depressive patients in routinary clinical practice. Indeed, patients included in RCT are relatively uncomplicated, without relevant medical and psychiatric comorbidities, with absent suicidality, and higher likelihood of responsiveness, as reflected by the high rate of placebo response (31). In addition, in the clinical trial setting patients are more extensively assessed and more frequently monitored than in clinical practice, and treatment adherence is not a major issue (32). Real-world studies in the MDD/TRD context are therefore needed to fill the gap between clinical research and routinary clinical practice.
In light of this need, a cohort study was established in 2018 to collect real-world data from TRD patients treated in clinical practice in several European countries (33, 34). Available data of 411 TRD patients with moderate-to-severe disease starting a new antidepressant treatment and followed for a minimum 6 months period were analyzed. Results from the overall European cohort showed the substantial impact of TRD on patients and society (33), and underlined the wide range of treatments used in clinical practice and the poor response rates of these patients (34).
Given the lack of a widely shared and consolidated standard of care and the possible difference among countries in the clinical approach to TRD, it is important to describe the country specific approach and prospective outcome in the management of TRD.
Therefore, the present investigation is aimed to describe the socio-demographic and clinical characteristics, treatment patterns and outcomes of the Italian patients included in the large European TRD cohort, considering that about one third of the patients of this cohort were recruited in Italy. The healthcare resource use of these patients was also documented.
Materials and Methods
Study Design and Participants
The present study is based on the Italian component of a European, prospective, multicentric, observational cohort study of TRD patients (ClinicalTrials.gov number, NCT03373253). Study methods for the overall European cohort have been previously described (33). The study was conducted in the period February 2018 (first patient in) and January 2020 (last visit of the last patient). Briefly, in- and outpatients aged 18 to 74 years, of both genders, with a diagnosis of MDD (according to the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition [DSM-5] or the International Statistical Classification of Diseases and Related Health Problems, 10th Revision [ICD-10] criteria for MDD or Depressive disorder) and fulfilling TRD criteria by the European Medicines Agency (EMA) (i.e., treatment failure on at least 2 different oral antidepressants, given at adequate dose and duration, as evaluated by the Massachusetts General Hospital-Antidepressant Treatment Response Questionnaire [MGH-ATRQ]) were enrolled in the study. To be enrolled, patients had to have moderate-to-severe depressive episode, as defined by a Montgomery-Åsberg Depression Rating Scale (35) (MADRS) ≥20 and needed to be initiating a new treatment regimen for MDD (i.e., any pharmacological or non-pharmacological treatment, including neurostimulation and psychotherapeutic interventions, prescribed to replace, or in addition to, the previous treatment; switches to biosimilars or changes in dose were not considered as new treatments) according to standard care; treatment choice, dose and method of administration was at the discretion of the prescribing physician.
Patients were excluded if they had: current or past psychotic disorders, MDD with psychotic features, bipolar disorders or intellectual disability according to DSM-5 or ICD-10; history of suicidal behavior within 1 year prior to enrolment; homicidal or suicidal ideation with intent within 1 month prior to entering the study; history of moderate or severe substance disorder (including alcohol) within 6 months prior to enrolment.
TRD patients were followed-up for a 12-month observation period with a minimum of 6-months and an extended observation period up to 6 months after enrollment of the last patients (end of study). In the overall cohort, patients were enrolled in multiple centers from Belgium (9 sites, 44 patients), Germany (23 sites, 59 patients), Italy (22 sites, 124 patients), the Netherlands (3 sites, 27 patients), Portugal (10 sites, 37 patients), Spain (16 sites, 71 patients) and the United Kingdom (15 sites, 49 patients); in the present study, the Italian sub-cohort was analyzed.
The study was conducted according to the Declaration of Helsinki, with the approval of the study Local ethics review boards. All patients provided written informed consent to participate in the study; their capability to give consent was judged by the treating physician.
Data Collection
Data were collected at baseline, at scheduled visits (every 6 months), and at study end. Data were also collected in case of premature study withdrawal and clinically relevant events, such as a change in treatment, admission to – or discharge from – inpatient care, symptoms relapse or MDE remission. Individual participant information was mainly recorded from patient's medical records; patients were also asked to complete questionnaires for the self-assessment of quality of life and functionality.
At baseline, patient's socio-demographic characteristics, history of the depressive disease, treatment history for the current MDE, and comorbidities were recorded. Clinical evaluation was performed at baseline and at each visit. Depression severity was assessed through the MADRS (35) (range: 0–60, with higher scores for higher depressive symptomology) and the Clinical Global Impression of Severity (CGI-S) (36) (range: 1–7, with higher scores for more severe mental illness). Change in depression severity was evaluated through the Clinical Global Impression of Change (CGI-C) (36) (range: 1–7, with lower scores for improvement and higher scores for worsening of depression). Patient's quality of life and functioning was collected at baseline and scheduled visits. Quality of life was assessed by the self-reported EuroQol 5-dimension 5-level (EQ-5D-5L) instrument (37). The EQ-5D-5L questionnaire assessed five dimensions (i.e., mobility, self-care, usual activities, pain/discomfort and anxiety/depression), with five levels of functioning (e.g., no problems, slight, moderate, severe and extreme problems). Results on each dimension were converted into a single utility index (generally ranging 0–1, with higher scores for a better state of health) according to standard methods; UK tariffs were used. The EQ-5D-5L questionnaire also included the EQ visual analog scale (EQ-VAS, range: 0–100, with higher scores for better quality of life). Functional impact and disability was evaluated by the self-reported Sheehan Disability Scale (SDS) (38). In the SDS, patients are asked to rate the extent to which (1) work, (2) social life or leasure activity, and (3) home life or family resposibilities are impaired on a 10-point visual analog scale, on which 0 is for normal function and 10 for severe funcional impairment; the total SDS score is calculated by summig up the 3 rates items, and thus ranges from 0 to 30, with higher scores for more severe impairment.
All pharmacological and non-pharmacological antidepressant therapies initiated at baseline and during the study period as for clinical practice were recorded.
Data on the healthcare resource utilization during the study period, including hospitalization, inpatient and outpatient visits, and intensive care unit (ICU) visits, were recorded.
Data Processing and Analyses
Analyses were based mainly on data collected at baseline (available for all 124 patients) and at 6 months after baseline (available for 98 patients).
Antidepressant pharmacological treatment classes were categorized as: SSRI, SNRI, TCA, MAOI, and “other” (e.g., trazodone, bupropion, mirtazapine, vortioxetine). Non-antidepressant drugs were categorized as add-on or augmentation medications (e.g., quetiapine, brexpiprazole, aripiprazole, lithium). Combination therapy was defined as more than one antidepressant medication in the absence of add-on medication. Augmentation therapy was defined as antidepressant medication(s) plus at least one add-on medication.
We derived treatment lines being received by patients from baseline onward. Specifically, every treatment started at baseline (between 7 days before and 14 days after baseline) was defined as “first treatment line”. To be included in an appropriate “treatment line,” a treatment had to last at least 30 days: patients who started a treatment line at baseline but were lost to follow-up within 1 month and/or had no post-baseline visit with MADRS assessment were not taken into account in this analysis.
Remission and response status were defined according to the MADRS score. In particular, remission was defined as a MADRS score ≤10 and response (without remission) was defined as an improvement ≥50% from baseline in the MADRS score, with a MADRS >10.
The main study outcomes were the rates of patients with remission and response status at 6 and 12 months after baseline (only the assessments done during the visits which occurred, respectively, between days 150 and 216 and between days 330 and 402 after baseline were taken into account). Change in patient' condition according to the CGI-C score (vs. the baseline visit) at 6 month was also analyzed. Quality of life and functioning at 6 months were also described, overall and by clinical response.
Statistical Analysis
Continuous variables were presented as mean values (±standard deviations) or median values (ranges), and categorical variables were reported as numbers and percentages. The Kaplan-Meier method was used to estimate the survival curve for time to treatment change.
Results
In total, 124 Italian patients with TRD from 22 sites participated in the TRD European cohort and were included in the present analysis.
Baseline Demographic Characteristics, Clinical Features and Medical History
At enrollment, the mean (SD) age was 53.2 (sd = 9.8) years and 82 patients (66.1%) were women (Table 1). Most patients had secondary (n = 50, 40.3%) or high school education (n = 44, 35.5%); 11 patients (8.9%) had University degrees. Seventy patients (56.5%) were married or had an official partner; 42 (33.9%) were employed, 52 (42.0%) unemployed and 17 (13.7%) were retired. The large majority of patients lived at home with cohabitants (n = 102, 82.3%); one patient lived at a psychiatric institution.
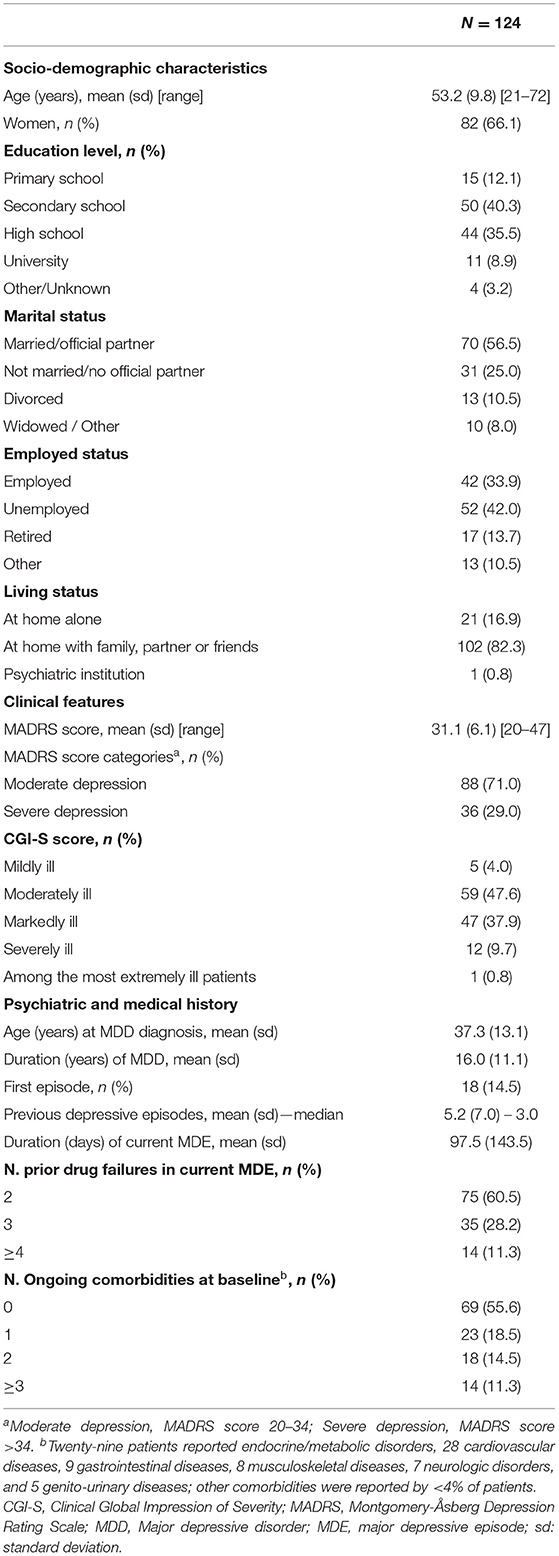
Table 1. Baseline socio-demographic characteristics and clinical features, psychiatric and medical history of patients with treatment-resistant depression (TRD).
The mean age at onset of MDD was 37.3 (sd = 13.1) years and the mean duration of the illness was 16.0 (sd = 11.1) years. The mean number of previous depressive episodes was 5.2, ranging from 0 to 43.
The current MDE had a mean duration of 97.5 (sd = 143.5) weeks, ranging from 13 to 1,304 weeks, and was a recurrent episode for over 85% of the patients; for treating it, 75 (60.5%), 35 (28.2%), and 14 (11.3%) patients had previously failed 2, 3 and ≥4 antidepressant drugs, respectively.
Fifty-five patients (44%) reported at least one ongoing comorbidity at baseline (32 patients 2 or more comorbidities), including both psychiatric and somatic ones; the most frequent ongoing conditions were endocrine and metabolic disorders (n = 29, 23.4%) and cardiovascular diseases (n = 28, 22.6%), followed by gastrointestinal (n = 9, 7.3%), musculoskeletal (n = 8, 6.5%), neurologic (n = 7, 5.6%), and genito-urinary diseases (n = 5, 4.0%). Other comorbidities were reported by <4% of patients.
The mean MADRS score at enrollment was 31.1 (sd = 6.1), with 88 patients (71.0%) being classified as having moderate depression (MADRS 20–34) and the remaining 36 (29.0%) as having severe depression (MADRS>34). Based on the CGI-S score (range: 1–7), 5 patients (4%) were categorized as mildly ill, 59 (47.6%) as moderately ill, 47 (37.9%) as markedly ill and 12 (9.7%) as severely ill; 1 patient had a CGI-S score of 7 (among the most extremely ill patients).
Prior Failed Treatments and Successive Treatment Lines
The most frequent failed antidepressant classes were SSRI (n = 96, 77.4%) and SNRI (n = 57, 46.0%), followed by TCA (n = 25, 20.2%); prior add-on drugs (SGAs) were reported by 17 patients (13.7%) (Figure 1).
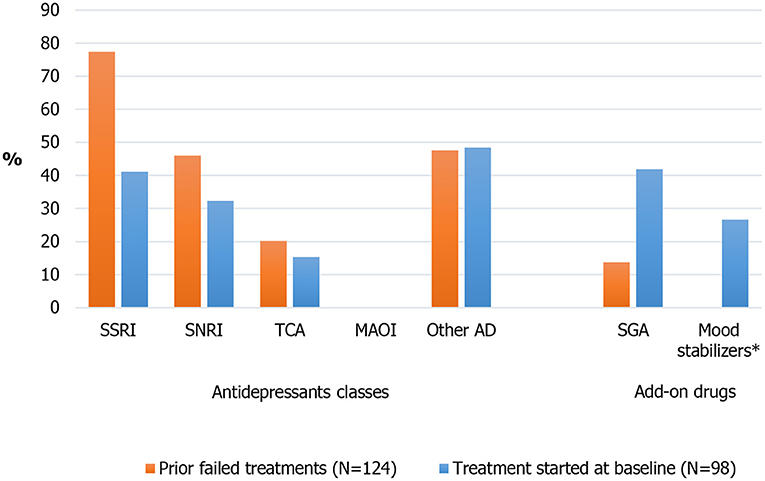
Figure 1. Prior failed antidepressive treatment and treatment started at baseline. *33 patients (26.6%) were treated with add-on mood stabilizers (16 patients [12.9%] with lithium) at baseline (not documented whether treatment onging at baseline or started at baseline). AD, antidepressants; MAOI, monoamine oxidase inhibitors; SGA, second-generation antipsychotics; SNRI, serotonin-norepinephrine reuptake inhibitors; SSRI, selective serotonin reuptake inhibitors; TCA, Tricyclic antidepressants.
Information about drugs started at baseline was available for 98 patients (Figure 1): 42 patients (42.9%) started a SSRI (mainly sertraline, paroxetine, and escitalopram), 32 (32.7%) a SNRI (venlafaxine and duloxetine), 15 (15.3%) a TCA (mainly clomipramine), and 46 (46.9%) “other” antidepressant classes (including 23 patients [23.5%] receiving vortioxetine, 14 [14.3%] bupropion and 10 [10.2%] trazodone); 42 (42.9%) and 25 (25.5%) patients started, respectively, add-on SGAs (mostly quetiapine and aripiprazole) and add-on mood stabilizers (mostly lithium). No patient was treated with MAOI drugs. Regarding non-pharmacological approaches, no patient was treated with a neurostimulation approach. According to baseline information, 14 Italian patients (11.3%) had been treated with a psychosocial approach, including psychotherapy; in particualar, 7 patients (5.6%) received cognitive behavioral therapy.
In terms of treatment strategies, 50 patients (51.0%) started at baseline augmentation therapies, 18 (18.4%) combination therapies, and 24 (24.5%) monotherapies; 6 patients (6.1%) received a non-antidepressant drug (e.g., SGA) only.
According to Kaplan-Meier analysis, 73% of patients were still on the treatment received at baseline after 6 months (Supplementary Figure 1).
In the successive treatment line (n = 28), 19 patients (68%) received augmentation therapy; combination therapy, monotherapy and a non-antidepressant drug only were prescribed to 3 patients each (data not shown).
Outcomes and Health Resource Utilization
At Month 6, 16 patients were reported as discontinued: 11 patients were lost to follow up; 2 died; 3 discontinued due to “other” reasons. Data were excluded from the 6 months outcome analysis for a further 18 patients who were still in the study but whose visits did not meet the defined cut-off dates for a Month 6 visit. We excluded one additional patient who had missing MADRS information at month 6. In total, 35 patients were not considered in the 6 month analysis (mean age: 52.2 years, % of women: 62.9%, mean MADRS: 29.9). All other 89 patients were included in this analysis, irrespective of treatment strategy. Among them, 64 (71.9%) showed no response, 9 (10.1%) response without remission and 16 (18.0%) remission (Figure 2). The MADRS score decreased, on average, by 31.6% (sd = 31.4), with a 6-month mean score of 21.5 (sd = 10.8): the mean score was 26.3 (sd = 8.6) in 64 non-responder patients, 13.8 (sd = 3.7) in 9 responder patients and 6.9 (SD 1.4) in 16 remitter patients.
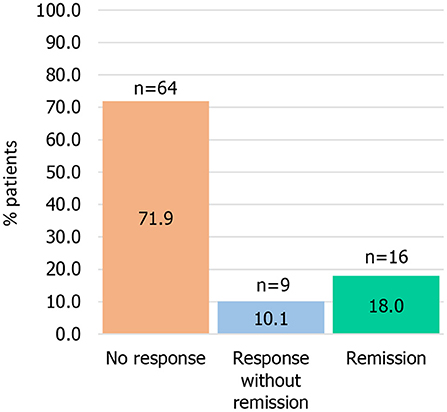
Figure 2. Treatment response* among patients with treatment-resistant depression at 6 months. *Remission: Montgomery-Åsberg Depression Rating Scale (MADRS) score ≤10; response (without remission): ≥50% improvement in the MADRS score, with MADRS>10.
At 6 months, 6 patients (6.7%) were classified as not at all ill, 10 (11.2%) as bordeline metally ill, 15 (16.9%) as mildly ill, 44 (49.4%) as moderately ill, 10 (11.2%) as markedly ill and 4 (4.5%) as severely ill based on the CGI-S score. The corresponding numbers were 0, 1, 12, 38, 9 and 4 in non-responder patients, 2, 1, 2, 3, 1, and 0 in responder patients, and 4, 8, 1, 3, 0, and 0 in remitter patients.
According to the CGI-C score, 30 patients improved much or very much (33.7%), 29 patients minimally improved (32.6%) and 30 (33.7%) did not benefit from treatment (no change or worse) at 6 months (Table 2). The means of EQ-5D-5L and EQ VAS were 0.44 (sd = 0.25) and 43.9 (sd = 19.0) at baseline and 0.6 (sd = 0.2) and 57.5 (sd = 22.3) at 6 months. The mean of the SDS scores decreased from 21.0 (sd = 5.7) at baseline to 15.0 (sd = 8.0) at 6 months. When patient-reported measures were analyzed according to clinical response, we found mean EQ-5D-5L scores of 0.6 in non-responder patients, 0.7 in responder patients and 0.9 in patients in remission; the corresponding mean values for EQ-VAS were, respectively, 50.1, 64.6 and 81.9 (Table 2). As for the disability, the mean SDS scores at 6 months was 18.6 in non-responder patients, 12.6 in responder patients, and 5.0 in patients with remission.
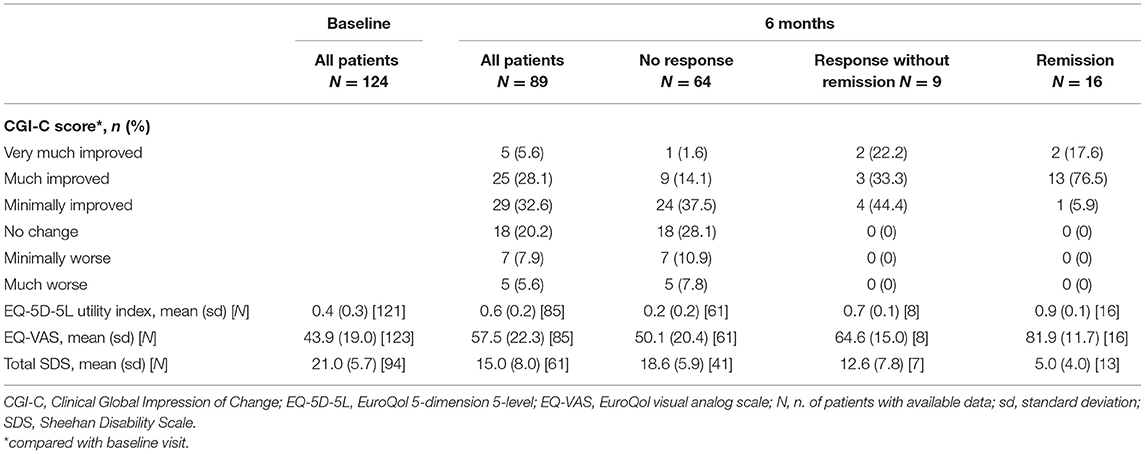
Table 2. Change in depression severity at 6 months compared to the baseline visit (CGI-C score), and quality of life and disability at baseline and at 6 months in patients with treatment-resistant depression (TRD), overall and by clinical response at 6 months.
Outcomes data at the 12-months follow-up were available for 44 patients; 27 (61.4%) had no response, 7 (15.9%) achieved response without remission and 10 (22.7%) achieved remission (Supplementary Figure 2).
During the first 6 months of study, 11 patients (12.4%) were hospitalized, with a median of 11 (range: 1–34) days spent in hospital (Table 3). Sixty-three patients (70.8%) had at least one outpatient consultation.
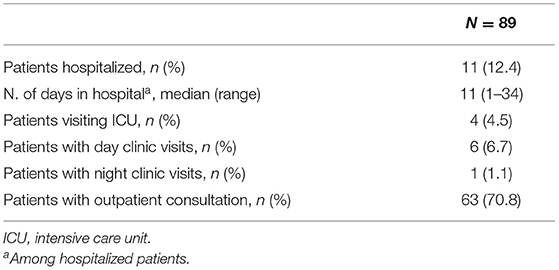
Table 3. Healthcare resource utilization between baseline and month 6 in patients with treatment-resistant depression.
Discussion
The present study provided original and interesting data on the characteristics, the naturalistic treatment pattern and the clinical outcome of a cohort of TRD patients with moderate to severe depression treated in Italian clinical practice. We also reported information on the health resource utilization of these patients.
A recent Italian study aimed at estimating the number of patients with TRD and at characterizing the pattern of drug use in the country (30). By applying TRD criteria by the EMA, the authors estimated over 101,000 Italian adults affected by TRD. They also reported frequent use of combination and augmentation therapy to treat the disease. That study was, however, a retrospective record-linkage study based on administrative databases and did not provided clinical outcome data (30). Collecting prospectively and ad hoc patient-level information on disease course, the current study represents, therefore, an important complementary source of data on TRD in Italy.
Our study showed the negative impact TRD has on patients in terms of employment status, quality of life and functioning, and documented the frequent use of SSRI and SNRI and of augmentation strategies in the everyday Italian clinical practice.
The moderate to severe MDE lasted on average almost 2 years, without any treatment response in more than 70% of the cases, suggesting a substantial disease burden over time. The poor response and remission rates observed at 6 and 12 months seem to reflect the difficult-to-treat nature of TRD: 71.9% of the patients were still non-responder to the treatment at month 6, with a mean MADRS score of 26.3, indicanting persistence of clinically relevant depressive symptoms. These results were similar to those observed in overall European cohort (34).
Given such negative outcomes, it is surprising that no patient in the Italian cohort was treated with neurostimulatory techniques and that the use of psychotherapy was very limited. In particular, psychosocial therapy was prescribed to 7% of our Italian patients but to 19.2% of patients in the overall Euoropean cohort (34). In a recent Danish study, psychotherapy was used in 18% of TRD patients (39). Our findings are aligned with the poor availability and spread of such techniques in Italian mental health departements; it is in any case worth to mention that information on the use of private psychotherapists is not available in the study.
In line with the overall European sample (33), at baseline, our patients had already suffered from MDD for over a decade. About 2 out of 3 of our patients were female, in line with the well-known sex ratio in the prevalence of depression (1). The mean duration of the MDE ongoing at baseline was almost 2 years and a considerable proportion of patients had experienced 3 or more previous drug failures during the ongoing MDE. A high proportion of patients, almost 50%, reported at least one ongoing comorbidity at baseline, either psychiatric or physical. The most frequent conditions were endocrine, metabolic disorders and cardiovascular diseases.
Long duration of current MDE together with the failure of several antidepressant treatments are main contributors to the high burden of disease of TRD condition, that is also associated with higher rates of psychiatric and physical comorbility, shorter life expectancy and higher mortality than non-TRD episodes (27, 28, 40, 41).
Confirming the high burden of TRD, our patients showed low quality of life and poor functioning, together with a substantial degree of disability. In particular, we observed a mean utility value derived from EQ-5D-5L of 0.44, similar to that reported in a recently published French TRD cohort (26). The much lower employment rate in our study (34%, which increased to 39% when calculated excluding retired patients) compared to that reported for the Italian population (63% among individuals aged 20–64 years in 2018 according to the Italian National Institute of Statistics) is not unexpected and confirms the personal and social burden of TRD. The negative impact of MDD in general, and TRD in particular, on work functioning, including employment status, has been widely reported in the literature (15, 42).
Describing the treatment approaches, we documented a widespread use of augmentation therapy, mostly with SGA, which increases as treatment changes. At enrolment, previously failed augmentation therapy was reported by ~14% of patients, while it was received by a considerable higher proportion of patient at baseline (51%) and at the successive treatment step (68%). An increase in the use of augmentation with successive treatment lines was reported also in the overall European cohort, but with lower prevalences (i.e., 36.7% at baseline and 47.2% at the successive treatment step) (34). Although a specific pharmacological treatment has not been established for TRD, augmentation is a mainstay in the pharmacotherapy of TRD and more severe/difficult to treat MDD (16), with multiple clinical trials and meta-analyses focused on the efficacy of SGA and lithium in MDD patients failing on an antidepressant (22, 23). Widespread use of a polypharmaceutical approach and augmentation in MDD was observed in a large, European, cross-sectional study, which also reported an association between augmentation/combination therapy and resistance to prior antidepressant therapy (43). In the only available Italian study on TRD 57% of patients were prescribed an add-on treatment starting from the third line of therapy (30).
An increasing prescription of SGA in MDD has been documented in the last years across various countries (44, 45), including European ones (46). Noteworthy, the SGA quetiapine got approval by the EMA as add-on medication to ongoing antidepressants in patients with MDD who have had sub-optimal response to treatment with other antidepressants [Quetiapine XR EPAR] (47). A recent meta-analysis showed a relatively limited efficacy of add-on treatment with SGA compared with placebo in TRD, with a pooled mean difference in the mean change from baseline in the MADRS score of 2.5 for SGA vs. placebo (48).
In our study, lithium augmentation was less frequently prescribed than SGA, as reported by others (43). Most of the available evidence is on the efficacy of lithium augmentation with TCAs, which are not widely used in contemporary clinical practice (49) (as also observed in the present study). On the contrary, the efficacy of lithium augmentation with SSRI and SNRI antidepressants is not well-documented (50). This observation, together with the diffuse negative perception of lithium side effects and safety concerns (51) and the need for monitoring of the serum lithium concentration and endocrine and renal function (50), may explain the lower use of lithium over SGA augmentation in clinical practice.
In terms of antidepressants, SSRI and SNRI represented the most frequently previously failed classes of antidepressants for the treatment of the index MDE as well as the treatments chosen most commonly at baseline in monotherapy or in combination; this indicates a still widespread use in clinical practice of these 2 antidepressant classes that are representative of the current Italian standard of care.
In general, we observed some improvements in depression severity, quality of life, functioning and disability at 6 months, with 32.6% of patients being classified as minimally improved, 28.1% as much improved and 5.6% as very much improved by the CGI-C score, and with scores of EQ-5D-5L and EQ-VAS increasing (respectively from 0.4 to 0.6 and from 43.9 to 57.5, on average) and scores of SDS decreasing (from 21.0 to 15.0, on average). However, response rates at 6 months were generally poor (remission: 19%, response: 10%); data at 12 months, limited to 44 patients with available information, did not demonstrate any meaningful improvement in outcomes with 6 additional months of treatment (remission: 15.9%, response: 22.7%). Notewhorty, disability evaluations with SDS and quality of life with EQ-5D-5L and EQ-VAS scores were consistent with MADRS outcomes, showing a substantial burden of disease in non-responder patients and suggesting a consistency between the physician's assessment of the disease and the patient's perception of their health and quality of life.
Although measures of function and quality of life are important secondary outcomes, remission, i.e., complete relief of depressive symptoms, is the most clinically relevant goal in MDD. Patients achieving remission have better functioning and prognosis and are much less likely to relapse than those achieving response with residual symptomatology (5). Low response and remission rates in TRD with standard care were reported by others (24, 25, 52). In particular, in a US, prospective, observational study of 124 TRD patients receiving treatment as usual, the 6-, 12- and 24-months remission (i.e., 30-item Inventory of Depressive Symptomatology-Self Report [IDS-SR-30] ≤14) rates were 2.5, 3.6, and 7.8%, respectively; the corresponding response (i.e, ≥50% IDS-SR-30 improvement) rates were, respectively, 8.4, 11.6, and 18.4% (24). Our results, consistently with those from other studies, underscore the unmet need for better treatment modalities for TRD, as the current options have a low chance to provide clinically desirable and long-term effects.
Because of the timeline of esketamine nasal spray approval (November 2019 by the EMA and March 2020 by the Italian Medicines Agency) and of its commercial availability in Italy (October 2020), our study did not capture data of this new treatment option for TRD patients, for which only data from RCT are available; it will be relevant to document its use and associated outcomes in more naturalistic settings.
This is the first real-world prospective study on TRD conducted in Italy; however, the sample size is relatively small compared to other studies. Among the other limitations, the diagnosis of MDD was made exclusively by clinical assessment according to standard criteria and no (semi)structured interview was administered. In addition, data collected in our study did not allow to associate outcomes to specific treatment strategies. Furthermore, outcomes data at 6 and 12 months of follow-up were available only for a proportion of patients; this was due to a number of reasons, including lost to follow up, patients drop out, study end (i.e., the study ended 6 months after the recruitment of the last patient), lack of MADRS and other clinical/patient reported outcome data, and the fact some patients did not have visits meeting criteria for a month 6 (i.e., occurred between day 150 and day 216 after baseline) or a month 12 visit (between day 330 and day 402). In particular, outcome data at 12 months were available for <40% of the originally recruited patients, and thus such results need to be interpreted with caution.
Our study has, however, major strengths, including the prospective design, the inclusion of patients encountered in routine clinical practice, the involvement of a number of sites across the various Italian Regions, and the ad-hoc prospective collection of clinical and patients reported outcomes through the observation period.
Conclusions
Results from the present study clearly showed the negative impact of TRD in terms of chronicity of the symptomatology, impairment in quality of life and functioning, and documented the substantial burden experienced by real-world TRD patients in Italy as in other European Countries. We also documented the widespread use of SSRI and SNRI and of augmentation strategies and the unfrequent use of a psychosocial approach, including psychotherapy, in the everyday Italian clinical practice. The study shows that, despite the multiple treatment options, the disease remains a complex and challenging condition and suggests an unmet treatment need in TRD care.
Data Availability Statement
The datasets presented in this article are not readily available because legal/commercial restriction. Requests to access the datasets should be directed to ZGRlbG1vbnRAaXRzLmpuai5jb20=.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethic Committees of the participating centers. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
DD, MA, GA, GP, and GR: substantial contributions to acquisition and analysis or interpretation of the data. GP, PC, SD, GR, AV, MA, GA, JM, and DD: drafting the article or revising it critically for important intellectual content. All authors contributed to the article and approved the submitted version.
Conflict of Interest
GP received grant/research support from Angelini; speaker/consultant for Angelini, Janssen, Lundbeck, Neuraxpharm, Sanofi Aventis. GR received speaker/consultant fees for Angelini, Innova Pharma, Janssen, Lundbeck and Otsuka. AV received grant/research support and speaker/consultant fees for Angelini, Boheringer Ingelheim, Innovapharma, Janssen-Cilag, Lundbeck, Otsuka, Pfizer, Recordati, Roche, Rovi Pharma, Takeda. JM was employed by Janssen EMEA. MA was employed by Janssen-Cilag SpA. GA was employed by Janssen-Cilag SpA. DD was employed by Janssen-Cilag SpA.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This article was based on the original study 54135419DEP4001 sponsored by Janssen EMEA. The funder had the following involvement with the study: study design, data collection and analysis, decision to publish, and preparation of the manuscript. Support for third-party writing assistance for this article, provided by Carlotta Galeone (Statinfo srl), was funded by Janssen-Cilag SpA in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank the patients, the investigators and their teams who took part in this study. The authors also acknowledge Carlotta Galeone, Ph.D., from Statinfo srl, for medical writing and editorial assistance based on the author's input and direction.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.769693/full#supplementary-material
References
2. Bromet E, Andrade LH, Hwang I, Sampson NA, Alonso J, de Girolamo G, et al. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. (2011) 9:90. doi: 10.1186/1741-7015-9-90
3. de Girolamo G, Polidori G, Morosini P, Scarpino V, Reda V, Serra G, et al. Prevalence of common mental disorders in Italy: results from the European study of the epidemiology of mental disorders (ESEMeD). Soc Psychiatry Psychiatr Epidemiol. (2006) 41:853–61. doi: 10.1007/s00127-006-0097-4
4. World Health Organization. Depression and Other Common Mental Disorder: Global Health Estimates. Geneva, World Health Organization (2017). p. 24. License: CC BY-NC-SA 3.0 IGO.
5. Rush AJ, Kraemer HC, Sackeim HA, Fava M, Trivedi MH, Frank E, et al. Report by the ACNP task force on response and remission in major depressive disorder. Neuropsychopharmacology. (2006) 31:1841–53. doi: 10.1038/sj.npp.1301131
6. Berlim MT, Turecki G. Definition, assessment, and staging of treatment-resistant refractory major depression: a review of current concepts and methods. Can J Psychiatry. (2007) 52:46–54. doi: 10.1177/070674370705200108
7. Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry. (2006) 163:1905–17. doi: 10.1176/ajp.2006.163.11.1905
8. European Medicines Agency. Guideline on Clinical Investigation of Medicinal Products in the Treatment of Depression. EMA/CHMP/185423/2010 Rev 2 (2013). Available online at: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-investigation-medicinal-products-treatment-depression_en.pdf (accessed June, 2021).
9. McLachlan G. Treatment resistant depression: what are the options? BMJ. (2018) 363:k5354. doi: 10.1136/bmj.k5354
10. Wiles N, Thomas L, Abel A, Barnes M, Carroll F, Ridgway N, et al. Clinical effectiveness and cost-effectiveness of cognitive behavioural therapy as an adjunct to pharmacotherapy for treatment-resistant depression in primary care: the CoBalT randomised controlled trial. Health Technol Assess. (2014) 18:1–167. doi: 10.3310/hta18310
11. Conway CR, George MS, Sackeim HA. Toward an evidence-based, operational definition of treatment-resistant depression: when enough is enough. JAMA Psychiatry. (2017) 74:9–10. doi: 10.1001/jamapsychiatry.2016.2586
12. Nemeroff CB. Prevalence and management of treatment-resistant depression. J Clin Psychiatry. (2007) (Suppl. 68)8:17–25.
13. Mrazek DA, Hornberger JC, Altar CA, Degtiar I. A review of the clinical, economic, and societal burden of treatment-resistant depression: 1996-2013. Psychiatr Serv. (2014) 65:977–87. doi: 10.1176/appi.ps.201300059
14. Olfson M, Amos TB, Benson C, McRae J, Marcus SC. Prospective service use and health care costs of medicaid beneficiaries with treatment-resistant depression. J Manag Care Spec Pharm. (2018) 24:226–36. doi: 10.18553/jmcp.2018.24.3.226
15. Jaffe DH, Rive B, Denee TR. The humanistic and economic burden of treatment-resistant depression in Europe: a cross-sectional study. BMC Psychiatry. (2019) 19:247. doi: 10.1186/s12888-019-2222-4
16. de Sousa RT, Zanetti MV, Brunoni AR, Machado-Vieira R. Challenging treatment-resistant major depressive disorder: a roadmap for improved therapeutics. Curr Neuropharmacol. (2015) 13:616–35. doi: 10.2174/1570159X13666150630173522
17. Voineskos D, Daskalakis ZJ, Blumberger DM. Management of treatment-resistant depression: challenges and strategies. Neuropsychiatr Dis Treat. (2020) 16:221–34. doi: 10.2147/NDT.S198774
18. Mahase E. Esketamine is approved in Europe for treating resistant major depressive disorder. BMJ. (2019) 367:l7069. doi: 10.1136/bmj.l7069
19. Martin JL, Barbanoj MJ, Schlaepfer TE, Clos S, Perez V, Kulisevsky J, et al. Transcranial magnetic stimulation for treating depression. Cochrane Database Syst Rev. (2002) CD003493.
20. Cattaneo CI, Ressico F, Fornaro M, Fazzari G, Perugi G. The shocking attitude toward electroconvulsive therapy in Italy. CNS Spectr. (2020) 1−3. doi: 10.1017/S1092852920002059
21. Milev RV, Giacobbe P, Kennedy SH, Blumberger DM, Daskalakis ZJ, Downar J, et al. Canadian network for mood and anxiety treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 4. Neurostimulation Treatments. Can J Psychiatry. (2016) 61:561–75. doi: 10.1177/0706743716660033
22. Ruberto VL, Jha MK, Murrough JW. Pharmacological treatments for patients with treatment-resistant depression. Pharmaceuticals (Basel). (2020) 13:116. doi: 10.3390/ph13060116
23. Ionescu DF, Rosenbaum JF, Alpert JE. Pharmacological approaches to the challenge of treatment-resistant depression. Dialogues Clin Neurosci. (2015) 17:111–26. doi: 10.31887/DCNS.2015.17.2/dionescu
24. Dunner DL, Rush AJ, Russell JM, Burke M, Woodard S, Wingard P, et al. Prospective, long-term, multicenter study of the naturalistic outcomes of patients with treatment-resistant depression. J Clin Psychiatry. (2006) 67:688–95. doi: 10.4088/JCP.v67n0501
25. Aaronson ST, Sears P, Ruvuna F, Bunker M, Conway CR, Dougherty DD, et al. A 5-year observational study of patients with treatment-resistant depression treated with vagus nerve stimulation or treatment as usual: comparison of response, remission, and suicidality. Am J Psychiatry. (2017) 174:640–8. doi: 10.1176/appi.ajp.2017.16010034
26. Yrondi A, Bennabi D, Haffen E, Quelard D, Samalin L, Maruani J, et al. Treatment-resistant depression in a real-world setting: first interim analysis of characteristics, healthcare resource use, and utility values of the fondamental cohort. Brain Sci. (2020) 10:962. doi: 10.3390/brainsci10120962
27. Amos TB, Tandon N, Lefebvre P, Pilon D, Kamstra RL, Pivneva I, et al. Direct and indirect cost burden and change of employment status in treatment-resistant depression: a matched-cohort study using a us commercial claims database. J Clin Psychiatry. (2018) 79:17m11725. doi: 10.4088/JCP.17m11725
28. Kubitz N, Mehra M, Potluri RC, Garg N, Cossrow N. Characterization of treatment resistant depression episodes in a cohort of patients from a US commercial claims database. PLoS ONE. (2013) 8:e76882. doi: 10.1371/journal.pone.0076882
29. Rizvi SJ, Grima E, Tan M, Rotzinger S, Lin P, McIntyre RS, et al. Treatment-resistant depression in primary care across Canada. Can J Psychiatry. (2014) 59:349–57. doi: 10.1177/070674371405900702
30. Perrone V, Sangiorgi D, Andretta M, Ducci G, Forti B, Francesa Morel PC, et al. Assessment of patients affected by treatment-resistant depression: findings from a real-world study in italy. J Affect Disord. (2020) 4:104–17.
31. Wisniewski SR, Rush AJ, Nierenberg AA, Gaynes BN, Warden D, Luther JF, et al. Can phase III trial results of antidepressant medications be generalized to clinical practice? A STAR*D report. Am J Psychiatr. (2009) 166:599–607. doi: 10.1176/appi.ajp.2008.08071027
32. Gaynes BN, Rush AJ, Trivedi MH, Wisniewski SR, Spencer D, Fava M. The STAR*D study: treating depression in the real world. Cleve Clin J Med. (2008) 75:57–66. doi: 10.3949/ccjm.75.1.57
33. Heerlein K, Young AH, Otte C, Frodl T, Degraeve G, Hagedoorn W, et al. Real-world evidence from a european cohort study of patients with treatment resistant depression: baseline patient characteristics. J Affect Disord. (2021) 283:115–22. doi: 10.1016/j.jad.2020.11.124
34. Heerlein K, Perugi G, Otte C, Frodl T, Degraeve G, Hagedoorn W, et al. Real-world evidence from a european cohort study of patients with treatment resistant depression: treatment patterns and clinical outcomes. J Affect Disord. (2021) 290:334–44. doi: 10.1016/j.jad.2021.03.073
35. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. (1979) 134:382–9. doi: 10.1192/bjp.134.4.382
36. Guy W. ECDEU Assessment Manual for Psychopharmacology. Rockville, MD: US Department of Health, Education, and Welfare Public Health Service Alcohol, Drug Abuse, and Mental Health Administration (1976).
37. EuroQol Research Foundation. EQ-5D-5L User Guide. (2019). Available online at: https://euroqol.org/publications/user-guides.
38. Sheehan DV, Harnett-Sheehan K, Raj BA. The measurement of disability. Int Clin Psychopharmacol. (1996) 11(Suppl. 3):89–95. doi: 10.1097/00004850-199606003-00015
39. Gronemann FH, Petersen J, Alulis S, Jensen KJ, Riise J, Ankarfeldt MZ, et al. Treatment patterns in patients with treatment-resistant depression in Danish patients with major depressive disorder. J Affect Disord. (2021) 287:204–13. doi: 10.1016/j.jad.2021.03.029
40. Ivanova JI, Birnbaum HG, Kidolezi Y, Subramanian G, Khan SA, Stensland MD. Direct and indirect costs of employees with treatment-resistant and non-treatment-resistant major depressive disorder. Curr Med Res Opin. (2010) 26:2475–84. doi: 10.1185/03007995.2010.517716
41. Souery D, Oswald P, Massat I, Bailer U, Bollen J, Demyttenaere K, et al. Clinical factors associated with treatment resistance in major depressive disorder: results from a European multicenter study. J Clin Psychiatry. (2007) 68:1062–70. doi: 10.4088/JCP.v68n0713
42. Patten SB, Wang JL, Williams JV, Lavorato DH, Bulloch A, Eliasziw M. Prospective evaluation of the effect of major depression on working status in a population sample. Can J Psychiatry. (2009) 54:841–5. doi: 10.1177/070674370905401207
43. Dold M, Bartova L, Mendlewicz J, Souery D, Serretti A, Porcelli S, et al. Clinical correlates of augmentation/combination treatment strategies in major depressive disorder. Acta Psychiatr Scand. (2018) 137:401–12. doi: 10.1111/acps.12870
44. Lenderts S., Kalali A. Treatment of depression: an update on antidepressant monotherapy and combination therapy. Psychiatry (Edgmont). (2009) 6:15–7.
45. Halfdanarson O, Zoega H, Aagaard L, Bernardo M, Brandt L, Fuste AC, et al. International trends in antipsychotic use: a study in 16 countries, 2005-2014. Eur Neuropsychopharmacol. (2017) 27:1064–76. doi: 10.1016/j.euroneuro.2017.07.001
46. Konstantinidis A, Papageorgiou K, Grohmann R, Horvath A, Engel R, Kasper S. Increase of antipsychotic medication in depressive inpatients from 2000 to 2007: results from the AMSP international pharmacovigilance program. Int J Neuropsychopharmacol. (2012) 15:449–57. doi: 10.1017/S1461145711000745
47. European Medicines Agency. Esketamine Summary of Product Characteristics. Available online at: https://www.ema.europa.eu/en/medicines/human/EPAR/spravato. (accessed June 07 2021).
48. Dold M, Bartova L, Kasper S. Treatment response of add-on esketamine nasal spray in resistant major depression in relation to add-on second-generation antipsychotic treatment. Int J Neuropsychopharmacol. (2020) 23:440–5. doi: 10.1093/ijnp/pyaa034
49. Bauer M, Monz BU, Montejo AL, Quail D, Dantchev N, Demyttenaere K, et al. Prescribing patterns of antidepressants in Europe: results from the factors influencing depression endpoints research (FINDER) study. Eur Psychiatry. (2008) 23:66–73. doi: 10.1016/j.eurpsy.2007.11.001
50. Bauer M, Adli M, Ricken R, Severus E, Pilhatsch M. Role of lithium augmentation in the management of major depressive disorder. CNS Drugs. (2014) 28:331–42. doi: 10.1007/s40263-014-0152-8
51. McKnight RF, Adida M, Budge K, Stockton S, Goodwin GM, Geddes JR. Lithium toxicity profile: a systematic review and meta-analysis. Lancet. (2012) 379:721–8. doi: 10.1016/S0140-6736(11)61516-X
52. Fonagy P, Rost F, Carlyle JA, McPherson S, Thomas R, Pasco Fearon RM, et al. Pragmatic randomized controlled trial of long-term psychoanalytic psychotherapy for treatment-resistant depression: the tavistock adult depression study (TADS). World Psychiatry. (2015) 14:312–21. doi: 10.1002/wps.20267
Keywords: treatment resistant depression, treatment outcome, health-related quality of life, cohort study, treatment pattern, real-world study, major depressive disorder
Citation: Perugi G, Calò P, De Filippis S, Rosso G, Vita A, Adami M, Ascione G, Morrens J and Delmonte D (2021) Clinical Features and Outcomes of 124 Italian Patients With Treatment Resistant Depression: A Real-World, Prospective Study. Front. Psychiatry 12:769693. doi: 10.3389/fpsyt.2021.769693
Received: 02 September 2021; Accepted: 13 October 2021;
Published: 05 November 2021.
Edited by:
Michele Fornaro, New York State Psychiatric Institute (NYSPI), United StatesReviewed by:
Michele De Prisco, Federico II University Hospital, ItalyMarit Therese Schmid, Western Norway University of Applied Sciences, Norway
Copyright © 2021 Perugi, Calò, De Filippis, Rosso, Vita, Adami, Ascione, Morrens and Delmonte. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dario Delmonte, ZGRlbG1vbnRAaXRzLmpuai5jb20=