 Yi Xie1†
Yi Xie1† Xiao-Fei Cheng1†Cong Wang1,2Jia Cai1,2Yu Wang1Yun-Fei Mu1,2
Xiao-Fei Cheng1†Cong Wang1,2Jia Cai1,2Yu Wang1Yun-Fei Mu1,2 Zhong-Yue Deng1,2Ai-Ping Deng1,3Hong-Jun Song1,3
Zhong-Yue Deng1,2Ai-Ping Deng1,3Hong-Jun Song1,3 Xue-Hua Huang1,2Lan Zhang1,2
Xue-Hua Huang1,2Lan Zhang1,2 Jun Zhang1,2
Jun Zhang1,2 Yi Huang1,2
Yi Huang1,2 Li Yin1,2Wen-Wu Shen4
Li Yin1,2Wen-Wu Shen4 Ming-Li Li1,2*
Ming-Li Li1,2* Mao-Sheng Ran1,2*
Mao-Sheng Ran1,2*- 1Mental Health Center, West China Hospital, Sichuan University, Chengdu, Sichuan, China
- 2Institute of Psychiatry, West China Hospital, Sichuan University, Chengdu, Sichuan, China
- 3West China School of Nursing, Sichuan University, Chengdu, Sichuan, China
- 4West China Hospital, Sichuan University, Chengdu, Sichuan, China
Background: Anxiety and Internet addiction (IA) are prevalent and exhibit a strong correlation among adolescents. This study aimed to (a) identify key symptoms and relationships of the anxiety-IA combined network in Chinese adolescents and (b) examine the differences in anxiety-IA symptoms between rural and urban adolescents.
Methods: The study was a cross-sectional survey conducted in 122 secondary schools in Sichuan Province, China, using the Generalized Anxiety Disorder Scale and the Internet Addiction Test. General network analysis and bridge network analysis were used to identify the most influential symptoms and key connectors by adopting expected influence and bridge expected influence values. Network comparison tests were conducted to explore the global strength and network structure differences between rural and urban adolescents.
Results: The study included 60,268 adolescents (mean age 15.90 ± 1.65 years; 54.44% females), stratified by residence: rural (n = 49,819) and urban (n = 10,449). In the general network, “Fantasize about being on the web” (IAT15), “Neglect household chores” (IAT2), and “Reluctant to be offline” (IAT16) were the most influential symptoms. Bridge network analysis revealed that “Use the web to escape from emotion” (IAT10), “Feeling afraid” (GAD7), and “Defensive or secretive about being on the web” (IAT9) served as key connectors that bridge the comorbid network of anxiety and IA. The network structure test detected residence-related differences, and the most influential and bridging symptoms diverged by residence. “Craving for next Internet use” (IAT11) and “Irritability” (GAD6) characterized rural adolescents, whereas “Excessive worry” (GAD3) and “Restlessness” (GAD5) typified urban adolescents.
Conclusions: This study offers new insights into the symptom-level interactions between anxiety and IA in adolescents. These findings also highlight the necessity of precisely addressing the comorbidity of anxiety and IA between rural and urban adolescents.
Introduction
With the advancement of informatization, the number of Internet users in China had reached 1.092 billion by 2023, with an Internet penetration rate of 77.5% (1). The astounding development of the Internet has given rise to Internet addiction (IA), which was identified as a critical public health concern (2). IA is characterized by an excessive or poorly controlled preoccupation, urge, or behavior of Internet use resulting in functional impairments or distress (3, 4). IA can lead to physical conditions such as hearing loss, dry eye syndrome, and vision problems, while mentally it is often related to anxiety, sleep issues, and social isolation (5).
Empirical research has consistently shown that IA is often comorbid with other psychological symptoms and mental disorders, such as anxiety and Generalized Anxiety Disorder (GAD) (5, 6). Fifteen years ago, Bernardi demonstrated that of a cohort of 50 outpatients screened for IA, 15% presented with comorbid GAD (7). Adolescence marks an essential developmental stage where individuals undergo significant emotional and behavioral transformations, heightening their vulnerability to mental disorders (8). Specifically, in China, the overall prevalence of adolescents diagnosed with anxiety disorders reaches 4.7% (9). Additionally, the prevalence of Chinese adolescents screened for IA ranged from 33.37% to 45.32% (10, 11). Given the high prevalence of adolescent anxiety and IA and their positive and robust interaction (12, 13), it’s imperative to conduct in-depth research on IA and co-occurring anxiety.
A meta-analytic review indicates that social anxiety serves as a precursor to the emergence of IA among adolescents and young adults (14). Additionally, longitudinal studies have documented a consistent positive relationship between anxiety symptoms and IA over six-month intervals, with anxiety demonstrating a significant predictive capacity for IA (15, 16). On the other hand, IA has been shown to worsen anxiety symptoms (17), with studies indicating a strong link between IA severity and increased anxiety levels in adolescents (18). A variety of studies conducted among adolescents in different regions, including Peru (19), India (17), and Vietnam (20), have demonstrated a significant and positive link between the severity of IA and anxiety symptoms. Furthermore, cross-sectional studies have indicated that individuals with IA face 1.26 to 7 times the risk of anxiety compared to those without IA (21, 22). These findings emphasized the robust positive associations between anxiety and IA in adolescents, suggesting the possibility of co-occurrence of the two disorders in the population.
However, previous studies often overlooked the symptom-level interactions between anxiety and IA. Network analysis introduces a fresh approach by suggesting that disorders emerge from the interactions among symptoms, allowing us to estimate relationships across the symptoms of mental disorders (23). General network analysis focuses on characterizing the overall architecture of the symptom network by quantifying how symptoms interconnect at the whole-network level, which guides optimization and management strategies aimed at the entire system. Bridge network analysis, in contrast, is specifically concerned with identifying the critical bridge nodes and edges that knit together otherwise separable subnetworks or distinct clusters (e.g., anxiety vs. IA symptoms). Targeting these key bridging symptoms is often more efficient, which can simultaneously dampen risk across multiple subnetworks, thereby preventing the spread of pathology. Thus, the two approaches are complementary and mutually indispensable.
In these network models, symptoms are represented as nodes linked by edges, where these edges reflect the connections between symptoms, considering the influence of all other nodes in the network (24). The central nodes within this network identify important symptoms that are essential to the underlying mechanisms of the disorder’s pathology (25). Moreover, symptoms that connect both disorders—known as bridge symptoms—determine comorbidity and offer prime targets for clinical interventions (26).
Previous research has shown that symptoms like “Academic decline due to Internet use” and “Feeling depressed, moody, or nervous only while offline” are essential to the underlying mechanisms of anxiety combined with IA network pathology in nursing students (27). Besides, an investigation involving children and adolescents through school recruitment identified “Feeling afraid” as a key connector that bridged the IA and anxiety combined network, suggesting that addressing fearfulness can disrupt the spread or exacerbation of symptoms across anxiety and IA (12). It’s observed that the symptoms most requiring intervention in the IA and anxiety comorbidity network vary across populations. Therefore, further investigation is warranted within a large, representative sample of Chinese adolescents to clarify which specific symptoms most critically demand intervention in the comorbid anxiety-IA.
Furthermore, recent research has also underscored residence-specific disparities in anxiety and IA. Among middle-school students in China, both the prevalence of social anxiety and IA are significantly higher in urban adolescents than in their rural counterparts (28). Among 692 Polish respondents (mean age = 20.8 years), those at risk for IA who lived in rural areas exhibited significantly more severe psychopathological symptoms, including phobic anxiety, than their urban counterparts (29). While analyses stratified by residence revealed no significant differences in the combined anxiety-IA network structure among nursing students (27). However, the symptom-level nuances of comorbid anxiety-IA networks across residential settings remain insufficiently explored. These mixed findings underscore the need to examine how specific symptom pathways differ between rural and urban adolescents, meriting targeted investigation in large, representative samples of adolescents.
Thus, in the present study, we used general and bridge network analysis to (a) identify the most influential symptoms and connectors in the anxiety and IA combined network and (b) compare the structure of anxiety-IA networks between rural and urban adolescent students in China. It could provide the most critical, precise targets for clinical intervention in adolescent students.
Methods
Research design and participants
This convenience-sampled cross-sectional study was conducted among adolescent students in Sichuan Province, China, from December 14, 2022, to February 28, 2023. A total of 122 middle schools and high schools participated in the survey, ensuring a broad and diverse sample that spans 20 of the 21 prefecture-level divisions in Sichuan Province, with a 95% coverage rate; only the Ganzi Tibetan Autonomous Prefecture was not represented. The criteria for inclusion included (1) middle and high school students in Sichuan Province, China, (2) being able to read and fill out the questionnaire, and (3) voluntarily participating in the study. The exclusion criteria included (1) not being enrolled in schools in Sichuan Province, (2) having difficulty filling out the questionnaire, and (3) being unwilling to take part in the study.
An online survey was distributed through SoJump.com (wjx.cn), a viable source of convenience samples in China (30). To enhance the quality of the data collection, the survey information was initially sent to teachers at the participating schools. These teachers then scheduled their classes into the schools’ computer rooms orderly, where students completed the survey under teacher supervision (31–33). A total of 65,509 students accessed the survey, and 60,268 (92.0%) completed the questionnaires after providing informed consent, while 5,241 (8.0%) declined to participate or did not complete the survey.
Informed consent was obtained from all participants themselves, their parents, and their teachers, who served as guardians in school, and the participants’ anonymity has been preserved. The study received ethical approval from the Research Ethics Committee of West China Hospital, Sichuan University (No. 2022 – 1790). All procedures conformed to the provisions of the Declaration of Helsinki (as revised in Brazil in 2013).
Measurements
Anxiety
In assessing anxiety, this study utilized the 7-item Generalized Anxiety Disorder Scale (GAD - 7), which rates symptoms on a scale from 0 (none) to 3 (almost every day), reflecting the frequency of anxiety symptoms experienced in the past two weeks (34). The total score ranges from 0 to 21, with higher scores denoting more severe anxiety (35). The GAD - 7 scale has demonstrated strong reliability among Chinese youth, with a Cronbach’s α range of 0.71 to 0.87 (36) and a higher Cronbach’s α range of 0.97 in our sample.
IA
This research applied Kimberly S. Young’s 20-item Internet Addiction Test (IAT - 20) for assessing IA, which was developed based on the DSM-IV-TR criteria for pathological gambling (4). Scored on a 5-point Likert scale, from “very rarely” to “very frequently,” the IAT - 20 yields a total score between 20 and 100 (4), with a higher score indicating a higher level of IA. The IAT - 20’s validity and reliability were confirmed among Chinese adolescents, with a Cronbach’s α reaching 0.93 (37) and a slightly higher Cronbach’s α reaching 0.96 in our study.
Given the controversial factor structure and potential issues within the original items, Khazaal’s modifications to the IAT - 20 were used for data analysis (38). Specifically, the modifications involved combining items 3 and 19 and items 6 and 8 and renaming them IAT3 and IAT6, respectively. For the combined items, the highest or only responses were used. Since item 4 focused on making friends online, it was considered outdated and deleted. In addition to these five items, other items from 1 to 20 were retained with their original names, resulting in a modified 17-item Internet Addiction Test scale (IAT - 17) (38). The IAT - 17 scale exhibited high reliability in our study, with a Cronbach’s α of 0.95.
Other features
We used a self-designed questionnaire to collect self-reported data like demographics (age, sex, grade, and ethnicity), academic satisfaction, and family background (single child, family monthly income, marital status of parents, and parenting style).
Statistical analysis
Descriptive and network analyses were carried out using R programming, version 4.5.1. Categorical variables were analyzed with chi-square tests and Mann-Whitney U tests, and continuous variables were assessed using independent-sample t-tests. A threshold of.05 was defined as significance for all two-tailed tests. Our main approaches included setting up general and bridge network models, assessing the accuracy and stability of our models, analyzing the most influential symptoms and connectors, and comparing the differences between the rural and urban areas.
General network model
As for general network analysis, we utilized the “glasso” package for modal estimation (39), with the “qgraph” package for the model visualization (40). The “EBICglasso” algorithm combines the Extended Bayesian Information Criterion (EBIC) with the graphical Least Absolute Shrinkage and Selection Operator (gLASSO). EBIC selects the penalty value that yields the most parsimonious yet well-fitting model, thereby minimizing false-positive edges and enhancing interpretability, and gLASSO introduces a penalty parameter that shrinks small partial-correlation estimates (0.001 in our study) to exactly zero, producing a sparse network (41).
When each node (a node represents a symptom) is connected to several other nodes through edges (an edge represents specific links between two symptoms) with different weights, the final network is constructed automatically and indicates the centrality indices of each node. We provided quantitative centrality indicators for each node based on the unique configuration of a network, including Expected Influence (EI), Strength, Betweenness, and Closeness. EI is the sum of the signed edge weights (EW) connected to a node, capturing both the magnitude and the valence (positive or negative) of its associations with all other nodes. Strength is the sum of the weight of all direct connections between a specific symptom and others. Betweenness indicates how often a symptom lies on the shortest indirect path to another node. Closeness indicates how strongly a node is indirectly connected to other nodes in a network (i.e., the inverse of the sum of the distances). Given the presence of both positive and negative correlations within the network, we opted for the EI measure to identify the most influential symptoms with the highest EI (25). Symptoms were considered influential if their EI value lay above the 80th percentile.
Bridge network model
In bridge network analysis, we removed all within-cluster edges of the general network so that only the connections between the independent disorder clusters remained. We employed the “networktools” package to reveal key connectors that link the comorbid anxiety and IA network (Cramer et al., 2010). Within this bridge network, we computed bridge centrality indices—Bridge Expected Influence (BEI), Bridge Strength, Bridge Closeness, and Bridge Betweenness—similar to those in the general network. Because BEI incorporates both the magnitude and the sign of the associations, we used it as the primary indicator of a symptom’s bridging importance. These key connecting symptoms were identified by applying an 80th percentile cut-off to BEI values (42). The symptoms serve as potential targets for precision medicine to address the comorbidity of anxiety and IA.
Network stability analysis
For assessing conventional network model reliability and stability, the “bootnet” package was applied (43). We calculated a correlation stability coefficient (CS coefficient) for these centrality, bridge centrality, and EW indices in networks, showing how much data could be dropped while keeping a correlation of at least 0.70, which requires a CS coefficient of at least 0.25; results above 0.5 indicate strong network stability (43). Besides, with 1,000 case-dropping bootstrap simulations to estimate 95% confidence intervals (95% CIs) for EI, BEI, and EW, non-overlapping 95% CIs indicated significant differences between two symptoms or two edges (43).
Network comparison test
We explored differences in the combined anxiety-IA networks between rural and urban adolescents using the “Network ComparisonTest” package, based on 1,000 bootstrap samples, with Benjamini–Hochberg adjustment (44). The global strength differences test evaluated whether the overall network topology differs between rural and urban adolescents by comparing the sum of weights of all edges connected to that node between groups. The maximum EW differences test identified the single edge with the largest absolute weight difference between the two groups and used this difference as the test statistic for the overall structural invariance test.
We also subsequently fitted dedicated general and bridge networks for the rural and urban subsamples. For each residence-specific network, we estimated the structure with EBICglasso, quantified accuracy and stability via 1,000 non-parametric bootstraps, and identified the most influential symptoms and key connectors.
Results
Demographics and symptom distributions
The study included 60,268 adolescents aged 12 – 19 years (mean age: 15.90 ± 1.65 years; 54.44% females; 40.08% junior high school students; and 88.7% Han ethnicity), stratified by residence: rural (n = 49,819) and urban (n = 10,449). Demographic characteristics are presented in Table 1.
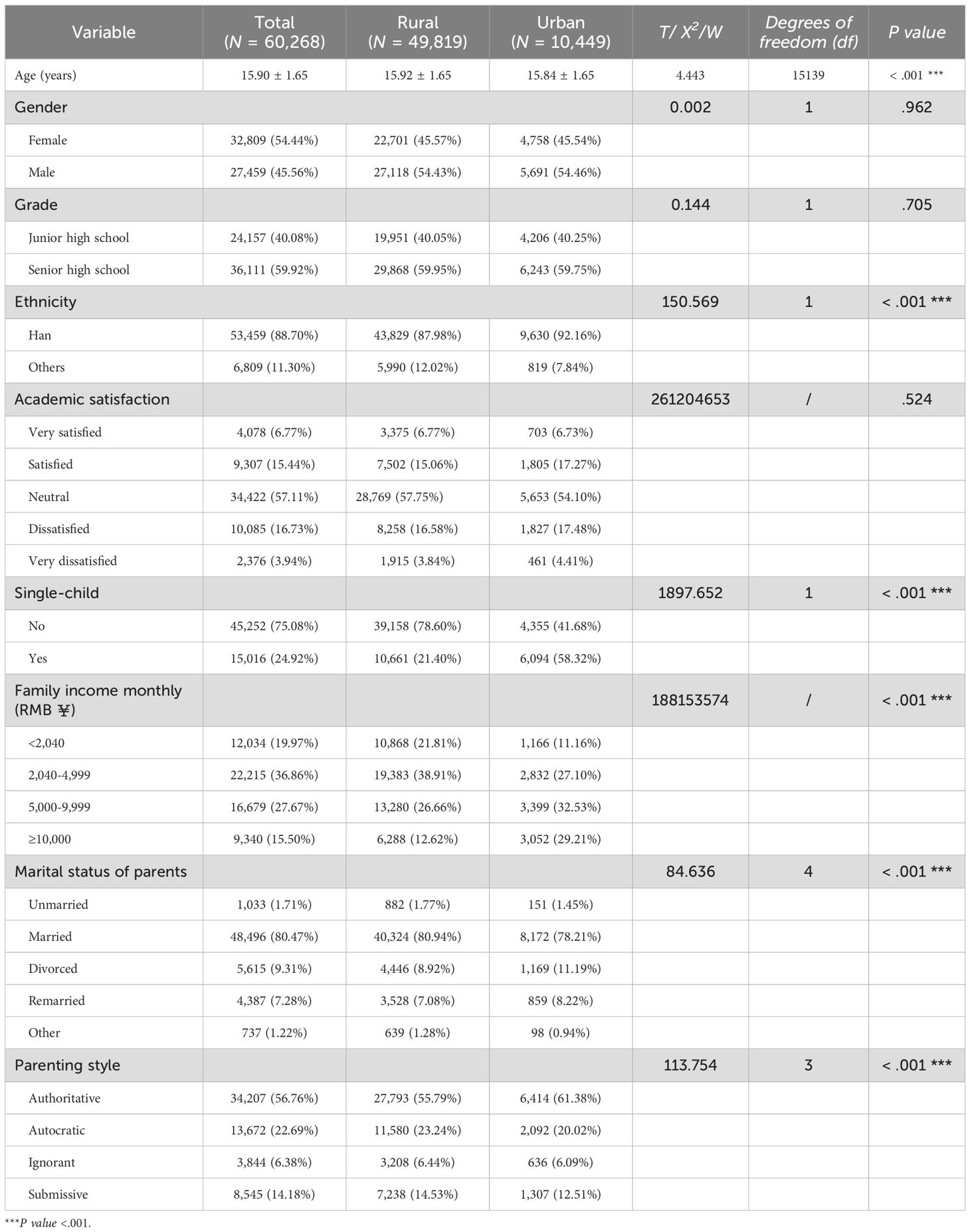
Table 1. Demographic characteristics and differences among groups by residence.
In the GAD - 7, “Nervousness” (GAD - 1) emerged as the most severe reported (0.54 ± 0.78). In the IAT - 20, “Complained about being on the web for very long” (IAT5) emerged as the predominant symptom (2.80 ± 1.22). The total score for the GAD - 7 Scale was 3.52 ± 5.03, showcasing the severity of the anxiety symptoms cluster. The composite score for the IAT - 20 Scale stood at 44.75 ± 17.07, reflecting a substantial severity of the IA symptoms cluster. Both total scores of the scales differed significantly between urban and rural adolescents (in GAD - 7, p = .001; in IAT - 20, p <.001), underscoring the need for residence-stratified analyses. Table 2 delineates the mean values and standard deviations (SDs) for the symptoms and overall scores of the GAD - 7 and IAT - 20 scales, with the details of the IAT - 17 scale in Supplementary Table S1 in the Supplementary Material.
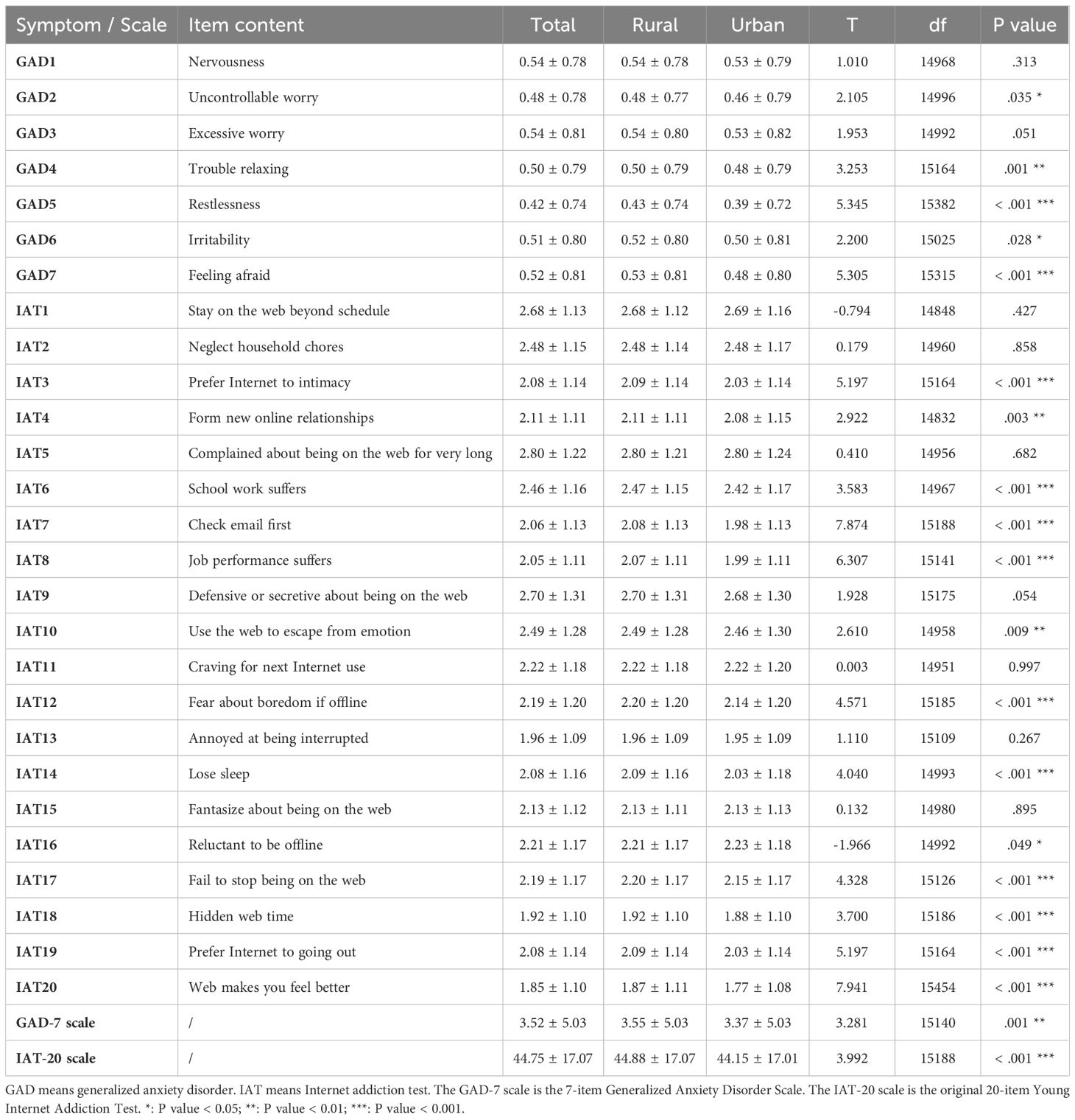
Table 2. Description and differences of the symptoms and overall scales of GAD-7 and IAT-20.
Network stability analysis
The 1,000-case-dropping bootstrap confirmed that the general and bridge networks for the overall population, as well as rural and urban subgroups, revealed acceptable stability, as evidenced by all CS coefficients of 0.750 for the main indices, including EI, BEI, and EW, indicating that the estimates did not fluctuate markedly when portions of the sample were removed. Supplementary Figure S1 presents the CS coefficients of all centrality, bridge centrality, and EW metrics in the Supplementary Materials.
The case-dropping difference test showed that most of the comparisons of main metrics between pairs of nodes or edges were statistically significant. Supplementary Figure S2 displays the resulting 95% CIs of all metrics in the Supplementary Materials; non-overlapping intervals denote significant differences, whereas overlapping intervals reflect non-significant differences.
General network model
Figure 1 illustrates the general comorbid network structure with the EI values for each symptom. The most influential symptoms were “Fantasize about being on the web” (IAT15, EI = 1.136), “Neglect household chores” (IAT2, EI = 1.094), “Reluctant to be offline” (IAT16, EI = 1.071), “Web makes you feel better” (IAT20, EI = 1.067), and “Uncontrollable worry” (GAD2, EI = 1.066).
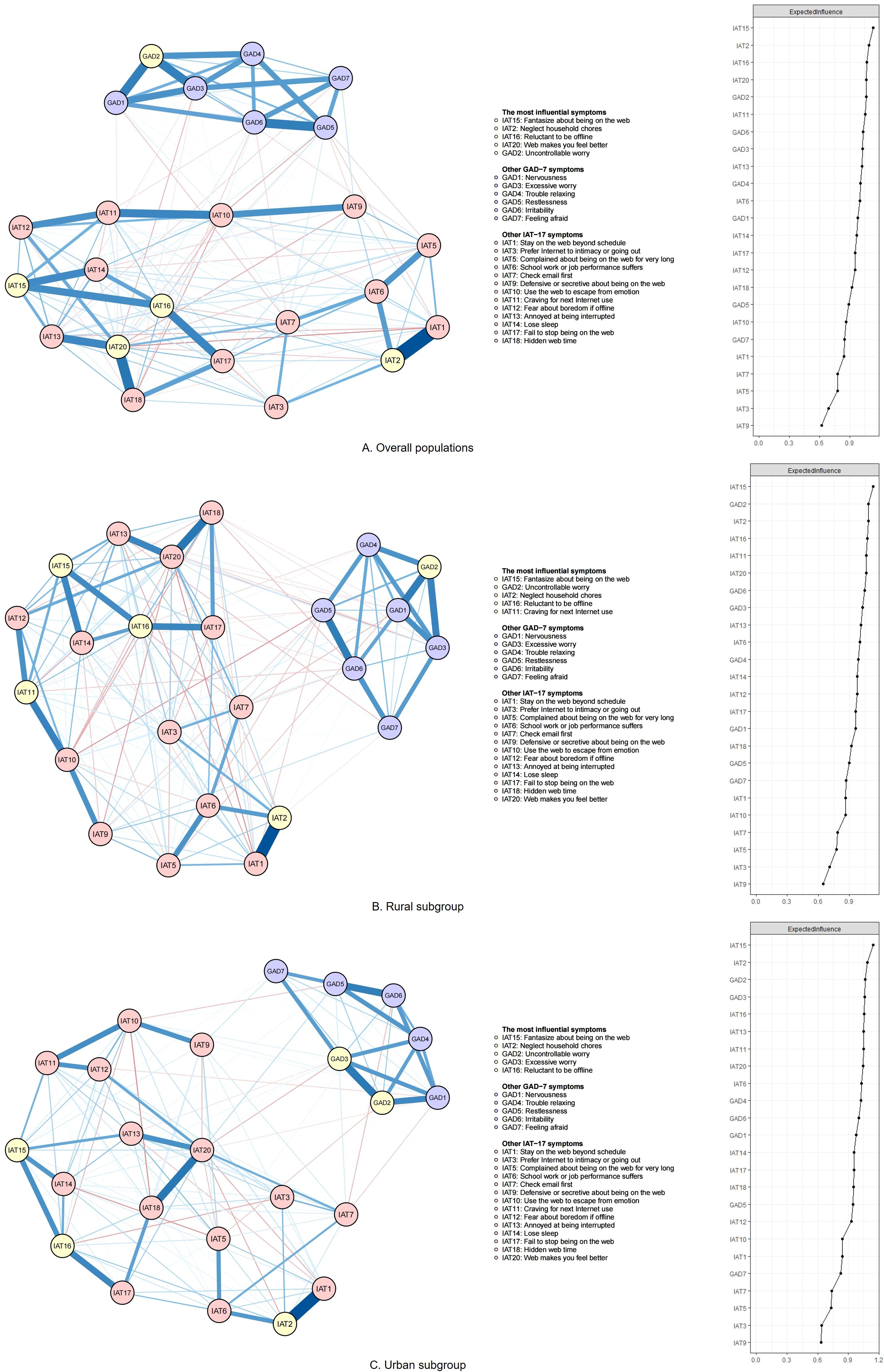
Figure 1. Network structure and expected influence (EI) value for each node of the combined anxiety-IA network. GAD - 7 means the 7-item Generalized Anxiety Disorder Scale. The IAT - 17 scale is the 17-item modified Internet Addiction Test. Nodes with EI values above the 80th percentile are identified as the most influential nodes. Blue lines represent positive correlations, while red lines indicate negative correlations. The edge’s thickness and saturation reflect the value of EI, with a higher absolute value of EI through greater thickness and saturation. (A) Overall populations; (B) Rural subgroup; (C) Urban subgroup.
The strongest positive edges linked “Fantasize about being on the web” with “Neglect household chores” (IAT1-IAT2, EW = 0.406), followed by “Hidden web time” and “Web makes you feel better” (IAT18-IAT20, EW = 0.301) and “restlessness” and “irritability” (GAD5-GAD6, EW = 0.279).
The strongest negative connections were between “Fantasize about being on the web” and “Web makes you feel better” (IAT1-IAT20, EW = -0.048), “Use the web to escape from emotion” and “hidden web time” (IAT10-IAT18, EW = -0.038), and “Defensive or secretive about being on the web” and “Web makes you feel better” (IAT9-IAT20, EW = -0.035). The specific values of all EW and centrality metrics are listed in Supplementary Tables S2 and S3, with the order in Supplementary Figure S3 in the Supplementary Materials, respectively.
Bridge network model
Figure 2 highlights the key connectors that link anxiety and IA comorbidity, along with their BEI values. “Use the web to escape from emotion” (IAT10, BEI = 0.068), “Feeling afraid” (GAD7, BEI = 0.066), “Defensive or secretive about being on the web” (IAT9, BEI = 0.051), “Nervousness” (GAD1, BEI = 0.046), and “Lose sleep” (IAT14, BEI = 0.045) were identified as bridge nodes, all of which are important in connecting the comorbidity network.
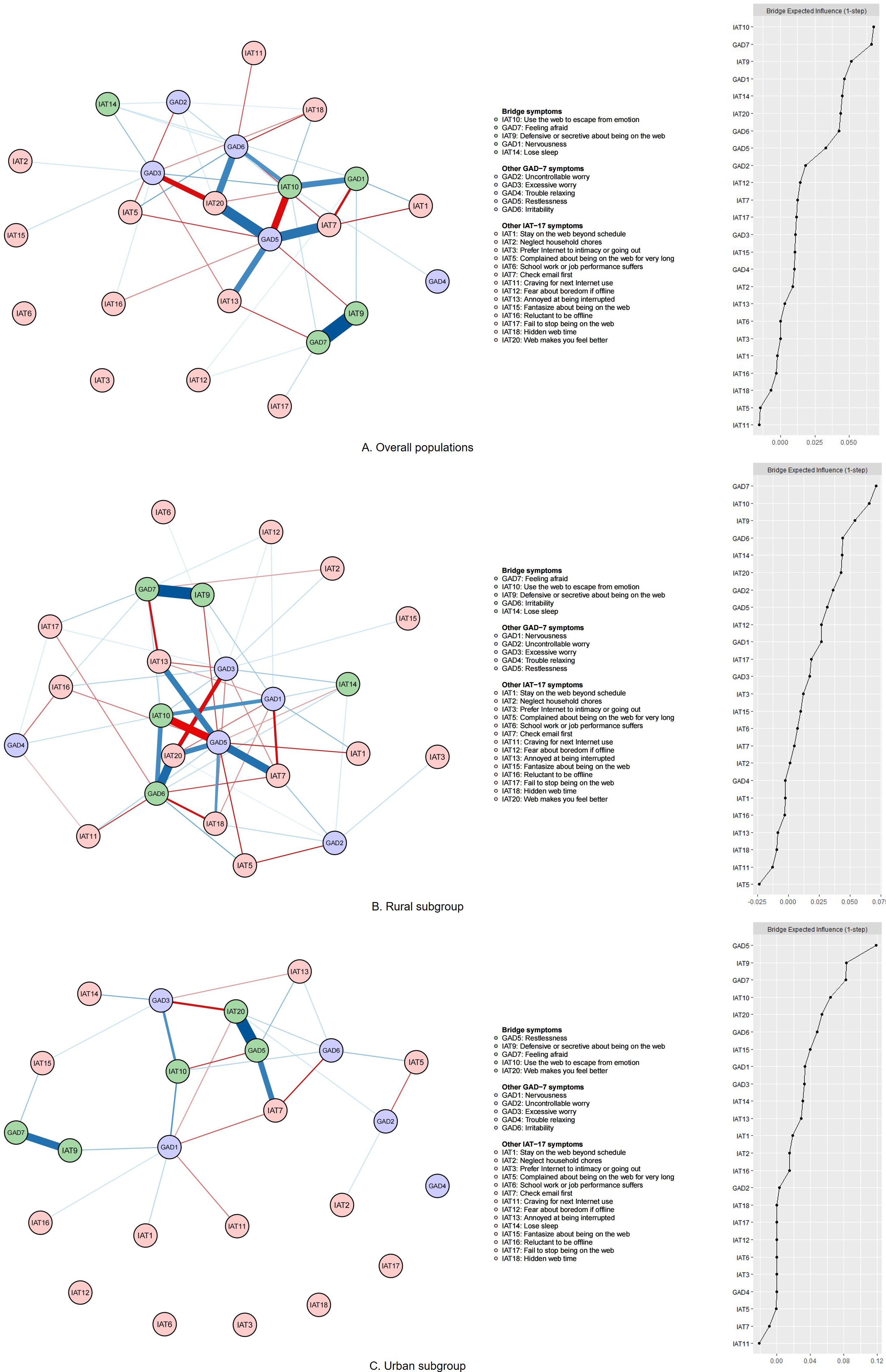
Figure 2. Bridge network structure and the bridge expected influence (BEI) value for each node of the combined anxiety and IA network. GAD-7 means the 7-item Generalized Anxiety Disorder Scale. The IAT-17 scale is the 17-item modified Internet Addiction Test. Nodes with BEI values above the 80th percentile are identified as bridge nodes. The item content, represented by node names, is displayed in the legend. Blue lines represent positive correlations, while red lines indicate negative correlations. The edge’s thickness and saturation reflect the value of EI, with a higher absolute value of EI through greater thickness and saturation. (A) Overall populations; (B) Rural subgroup; (C) Urban subgroup.
The strongest positive bridge connected “Feeling afraid” with “Defensive or secretive about being on the web” (GAD7-IAT9, EW = 0.054), “Restlessness” with “Web makes you feel better” (GAD5-IAT20, EW = 0.044), and “Restlessness” with “Check email first” (GAD5-IAT7, EW = 0.042).
The strongest negative associations were “Restlessness” and “Use the web to escape from emotion” (GAD5-IAT10, EW = -0.035), “Excessive worry” and “Web makes you feel better” (GAD3-IAT20, EW = -0.031), and “Nervousness” and “Check email first” (GAD1-IAT7, EW = -0.024). The specific values of all bridge centrality metrics are seen in Supplementary Table S3, with the order in Supplementary Figure S3 in the Supplementary Materials.
Network comparison test
Figure 3 presents the comparative analysis of the combined network models between rural and urban participants. The analysis of differences in global strength (rural: 11.844 vs. urban: 11.976) showed no significant differences between rural and urban participants (Test Statistic S = 4.834, p = .332), indicating the comparable overall symptom co-occurrence intensity between the two groups. However, the maximum EW difference test revealed resident differences in connectivity modal among adolescents (Test Statistic M = 0.096, p <.001). In other words, the entire network structure was not identical between rural and urban groups. However, there were no significant specific EW differences in the anxiety and IA combined network between rural and urban participants (all p >.05), as seen in Supplementary Table S4 in the Supplementary Materials.
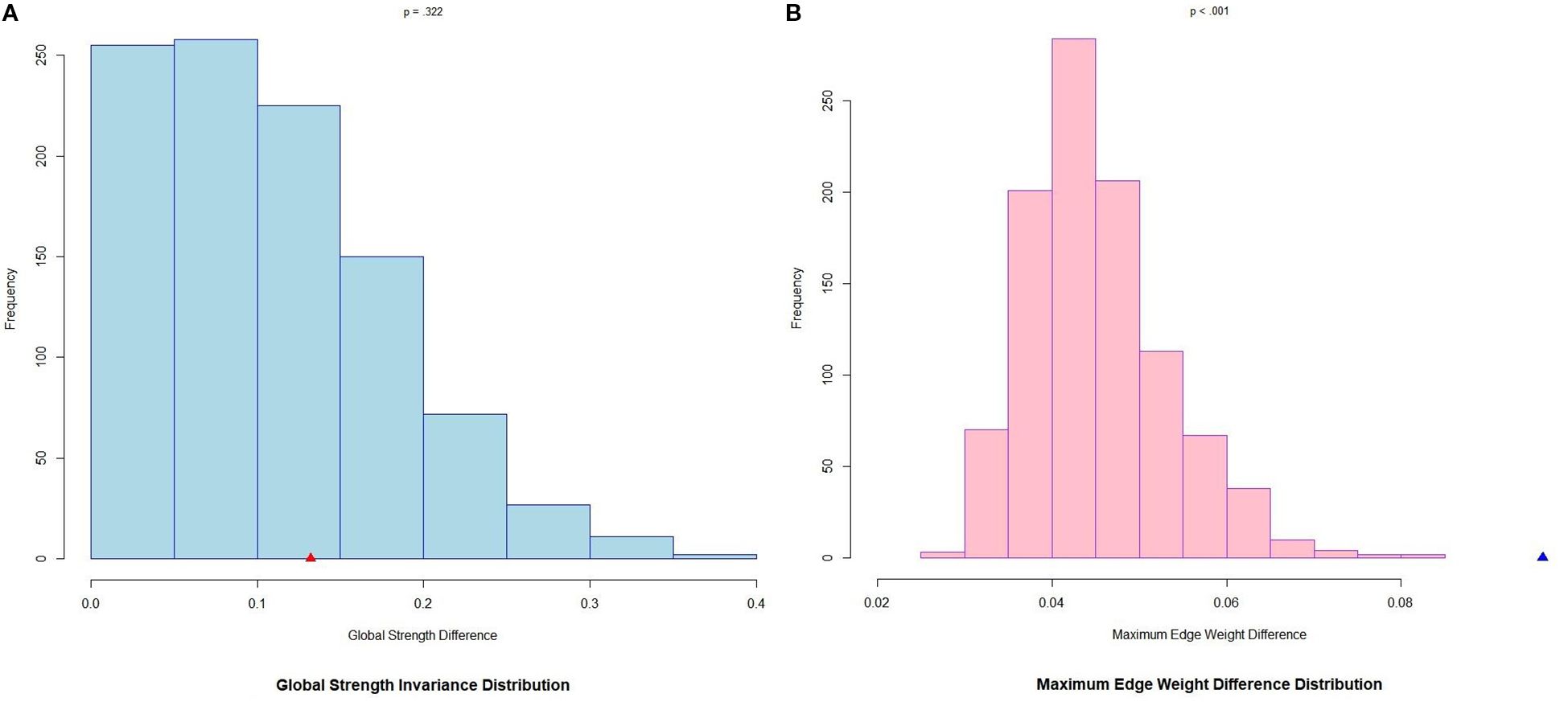
Figure 3. Global strength and edge weight comparisons between rural and urban networks of anxiety and IA symptoms. (A) Global strength (rural:11.844, urban:11.976) difference: point estimate of Test Statistic S = 0.132, p = .332. (B) Maximum edge weight difference: point estimate of Test Statistic M = 0.096, p <.001. Bars indicate the relative frequency of the test statistic under the null hypothesis of no group difference from 1,000 label-swapping permutations. The triangle denotes the observed point estimate from the original, unpermuted data. A triangle located far in the tail (outside the bars of the null distribution) signifies a significant group difference; a triangle falling within the bars of the distribution indicates that the observed difference is compatible with random fluctuation, and not statistically significant.
The most influential nodes and key bridge nodes differed between the two residence groups. In general networks, “Craving for next Internet use” (IAT11, EI = 1.062) only emerged as an influential symptom in rural adolescents, while “Excessive worry” (GAD3, EI = 1.061) only emerged as this symptom in urban adolescents. The residence-stratified groups shared the same strongest positive edges with the overall population (IAT1-IAT2, IAT18-IAT20, GAD5-GAD6). Notably, the most pronounced special negative edge in the rural network was linked to “Restlessness” with “Use the web to escape from emotion” (GAD5-IAT10, EW = -0.044). By contrast, the urban network exhibited two markedly strong negative connections: “Complained about being on the web for very long” and “Lose sleep” (IAT5-IAT14, EW = -0.056); and “Prefer Internet to intimacy or going out” and “Reluctant to be offline” (IAT3-IAT16, EW = -0.045).
In the bridge networks, there were key connectors only emerging in rural areas: “Irritability” (GAD6), with key connectors “Restlessness” (GAD5) and “Web makes you feel better” (IAT20) only emerging in urban areas. The different network models of the rural, urban, and overall populations shared the same strongest positive edge (GAD7-IAT9, GAD5-IAT20, GAD6-IAT20, and GAD5-IAT7). However, in urban adolescents, an additional strong negative edge emerged: “Irritability” and “Check email first” (GAD6-IAT7; EW = -0.035).
Discussion
In the present study, we found “Fantasize about being on the web,” “Neglect house chores,” “Reluctant to be offline,” “Web makes you feel better,” and “Uncontrollable worry” emerged as the most influential symptoms in the combined anxiety-IA network, while “Use the web to escape from emotion,” “Feeling afraid,” “Defensive or secretive about being on the web,” “Nervousness,” and “Lose sleep” served as key bridge nodes linking the anxiety-IA network in adolescents. In addition, the most influential and bridging symptoms diverged by residence: “Craving for next Internet use” and “Irritability” characterized rural adolescents, whereas “Excessive worry,” “Restlessness,” and “Web makes you feel better” typified urban adolescents.
General network model
“Fantasize about being on the web,” “Neglect household chores,” “Reluctant to be offline,” “Web makes you feel better,” and “Uncontrollable worry” emerged as the five most influential nodes, capturing intrusive cognition, functional impairment, withdrawal, emotional dependence, and the DSM - 5 core anxiety symptom, respectively. Specifically, fantasizing reflects intrusive daydreaming, which fuels IA and anxiety symptoms. It supports a previous study suggesting that day-to-day fluctuations in maladaptive daydreaming prospectively predicted simultaneous increases in negative emotion, whereas it also frequently co-occurs with anxiety and depression, indicating a positive-reinforcement loop akin to IA and anxiety (45). Neglecting chores is a highly visible marker of impairment of function for Chinese parents, who may routinely employ scolding and explicit expressions of disappointment—forms of psychological aggression and shaming discipline—to induce shame and guilt in their children when household duties or other filial expectations are neglected (46). In the context of emphasizing filial piety (47), these parental practices intensify children’s internalizing symptoms, creating a reciprocal loop in which anxiety and IA are both amplified. Reluctance to disconnect represents withdrawal and distress intolerance, reciprocally linked to physiological arousal (48) and fear-of-missing-out (49), thereby propagating symptoms rapidly across the anxiety-IA network. Feeling better embodies the reinforcement loop it creates—short-term mood repair by online immersion strengthens compulsive use, which then exacerbates offline stressors, such as schoolwork backlog and family tension, fueling new anxious conditions and motivation to IA (50). In addition to those, the result of uncontrollable worry aligns with previous adolescent comorbidity networks (51, 52) and confirms the criteria according to both DSM-5 and ICD-11 that “Uncontrollable worry” is one of the core symptoms of GAD (53, 54).
Except for these, fantasizing, reluctance, and feeling better might elucidate the fundamental neurobiological pathway implicated in IA. The “feels-better” pathway may activate the brain’s reward centers, such as the ventral striatum, illustrating how initial Internet use can offer pleasure or serve as an escape mechanism, potentially leading to addiction (55). Besides, the “must-do” pathway may become more prominent, influencing the dorsal striatum areas responsible for habit formation (55).
Furthermore, the results of this study showed that the strongest negative edge connected “Fantasize about being on the web” with “Web makes you feel better.” This inverse coupling suggests that the anticipatory craving and the consummatory reward do not co-activate; rather, they may represent distinct phases of the comorbidity cycle. These psychological dynamics highlight the probable transition from voluntary Internet use to a compulsive necessity, revealing the intricate relationship between reward, compulsion, and the development and persistence of IA and its comorbidity (50).
Bridge network model
In the bridge network, the results of this study showed that “Use the web to escape from emotion,” “Feeling afraid,” “Defensive or secretive about being on the web,” “Nervousness,” and “Lose sleep” were identified as bridge nodes, important in connecting the comorbidity of anxiety and IA symptoms, capturing emotion regulation, transdiagnostic emotion, behavioral concealment, physiological arousal bridge, and biobehavior, respectively. Negative emotions may lead adolescents to adopt a protective stance towards their online activities, viewing the Internet as a refuge from external criticism or judgment, directly linking compensatory use of the Internet with anxiety symptoms (56). Besides, individuals prone to emotions such as feeling afraid and nervous exhibit sensitivity that may escalate into anxiety and IA comorbidity, supporting previous research findings that the generalized fear or nervousness intensifies the urge to seek online safety cues. Meanwhile, excessive Internet use feeds back into new offline fears—missed deadlines, parental scolding—which in turn intensify IA and anxiety symptoms, sustaining the comorbidity loop (12, 54). Hiding usage generates interpersonal tension and guilt (57), further binding the two disorders into a self-perpetuating network. Besides, this finding of losing sleep as a bridge node provided empirical support for the mechanisms by which sleep issues can affect both IA and anxiety symptoms (58, 59). Sleep deprivation can impair the brain’s capacity to regulate emotions effectively (59), adversely impact impulse control function (60), and negatively alter social interactions (61), which may ultimately reinforce patterns of IA and anxiety.
Interestingly, the most pronounced negative connection was between “Nervousness” and “Check email first.” This negative association may reflect a tendency among those who are generally nervous not to necessarily prioritize checking emails. This is also indicative of a larger trend among Chinese adolescents, who primarily use immediate, interactive digital platforms like WeChat rather than conventional email for communication (62).
Network comparison test
The comparative analysis of the undirected combined networks between rural and urban adolescents revealed the insignificant influence of residence on these global network structures, which is consistent with previous research (27). However, conversely, the maximum EW difference test of the global network mode is significant.
In rural adolescents, the most influential symptoms, especially including “Craving for the next Internet use,” align with a network analysis of 1,009 Macua adolescents, in which the craving symptom was the central symptom linking IA and depression (63). Limited access to electronic devices in rural regions (64) is likely to amplify the salience of upcoming online rewards (65), because of which each opportunity to go online becomes highly valued. The heightened craving then triggers anxiety, reinforcing a feedback loop that makes craving the most efficient intervention target.
Notably, the most pronounced special negative edge in the rural bridge network was linked to “Restlessness” with “Use the web to escape from emotion,” indicating that when rural adolescents already feel physically agitated, they appear less inclined to turn to the Internet as an immediate emotional regulator. One plausible explanation is that the limited access to devices in rural settings makes online escape less available at the very moment restlessness peaks; instead, these adolescents may resort to non-digital coping (64, 65).
Excessive worry surfaced as a uniquely influential symptom of the general comorbid network only among urban adolescents. This may reflect the higher academic and social demands in cities (66), where unmet high-level needs become a central driver that simultaneously intensifies both anxiety and IA symptoms. The strongest negative edge linked complaints about prolonged Internet usage with losing sleep only in urban settings, where parental or school interventions intervene early and restrict late-night use of devices to protect sleep quality (67). On the other hand, the strongest negative edge connected a preference for online intimacy with reluctance to log off. For urban adolescents, digital closeness operates not as an irreplaceable emotional line but as an accessible form of entertainment (68), which can be turned off at will rather than feeling compelled to maintain.
The results of this study showed that restlessness and feeling better over the Internet served as bridge nodes in urban adolescents. Highly stressful city life constantly amplifies restlessness (66); when that restlessness is high, adolescents feel an immediate urge to go online, turning into a launching point for both anxiety and IA. The city-specific ecological and psychosocial factors—dense academic schedules (66) and high parental expectations (67)—make the “feels-better” pathway salient enough to function as a unique bridge between anxiety and IA symptoms, whereas rural adolescents—facing limited access and more stable routines (65)—do not experience this perception at comparable intensity. In addition to those, the strongest negative association includes a tendency among those who are generally irritable not to necessarily prioritize checking emails, indicating anger and the impulse to log on immediately do not rise together in urban adolescents.
Clinical implications
Beyond these findings, our research suggests that when treating adolescent symptoms of anxiety and IA, it’s important to help them find alternative activities that provide comfort and pleasure, reducing the feelings of negative emotion they may experience when offline. Physicians should advise adolescents to engage in regular exercise and participate in social clubs, which can decrease their psychological reliance on the Internet. This approach not only offers a substitute for Internet surfing but can also aid in the recovery of their impaired brain and social functions (69). They should be trained in emotional skills as well, to prevent them from excessively seeking emotional solace or refuge online or from passively allowing their IA and anxiety symptoms to escalate (70).
Limitations
However, the study had its limitations. The cross-sectional nature of the data collection limited our ability to draw rigorous causal links. Further longitudinal follow-up studies should be conducted to explore the causal relationship between anxiety and IA. Besides, the reliance on self-reported data and a sample limited to one province means that one should be cautious in generalizing these findings.
Conclusions
Our study offers new insights into the symptom-level interactions between anxiety and IA in adolescents. The research points out how psychological dependence on the Internet can trigger comorbidity of anxiety and IA. It also highlights the need for good sleep practices to prevent comorbid IA and anxiety. In addition, for rural and urban adolescents, some differentiated specific interventions should be adopted. Larger-scale longitudinal studies are warranted to further explore these relationships and their treatment and prevention strategies.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval was granted from the Research Ethics Committee of West China Hospital, Sichuan University (No. 2022–1790). All procedures followed were by the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 (5). The studies were conducted in accordance with the local legislation and institutional requirements. Informed consent was obtained from all participants, their parents, and their teachers, who served as their guardians in the school.
Author contributions
YX: Writing – original draft, Writing – review & editing. XF-C: Writing – original draft, Writing – review & editing. CW: Writing – review & editing. JC: Writing – review & editing. YW: Writing – review & editing. Y-FM: Writing – review & editing. Z-YD: Writing – review & editing. A-PD: Writing – review & editing. H-JS: Writing – review & editing. XH-H: Writing – review & editing. LZ: Writing – review & editing. JZ: Writing – review & editing. YH: Writing – review & editing. LY: Writing – review & editing. W-WS: Writing – review & editing. ML-L: Funding acquisition, Writing – original draft, Writing – review & editing. M-SR: Funding acquisition, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This study was supported by the Initial Research Fund, West China Hospital (WCH, No. 136220012, PI: M-SR), and the National Science and Technology Innovation 2030 “Brain Science and Brain Research” major project of China (2021ZD0202100, 2021ZD0202102). The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Acknowledgments
We thank all of the participants and their teachers for their help, willingness to participate in the study, and the time that they devoted to the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1558276/full#supplementary-material
Abbreviations
IA, Internet Addiction; GAD - 7, the 7-item Generalized Anxiety Disorder Scale; IAT - 20, the 20-item Young’s Internet Addiction Test; IAT - 17, the modified 17-item Internet Addiction Test; DSM - 5, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; ICD - 11, the International Classification of Diseases, Eleventh Revision; IAT, Internet Addiction Test; GAD, Generalized Anxiety Disorder; EBIC, the Extended Bayesian Information Criterion; gLASSO, the graphical Enhanced Least Absolute Shrinkage and Selection Operator; EI, Expected Influence; BEI, Bridge Expected Influence; EW, Edge Weight; 95% CI, 95% confidence intervals; CS coefficient, correlation stability coefficient; SD, standard deviation.
References
1. CNNIC. The 53rd China statistical report on internet development China (2024). Available online at: https://www3.cnnic.cn/n4/2024/0322/c88-10964.html (Accessed March 1, 2025).
2. Xu D-D, Lok K-I, Liu H-Z, Cao X-L, An F-R, Hall BJ, et al. Internet addiction among adolescents in Macau and mainland China: prevalence, demographics and quality of life. Sci Rep. (2020) 10:16222. doi: 10.1038/s41598-020-73023-1
3. Shaw M and Black DW. Internet addiction. CNS Drugs. (2008) 22:353–65. doi: 10.2165/00023210-200822050-00001
4. Young KS. Internet addiction: the emergence of a new clinical disorder. CyberPsychol Behav. (1998) 1:237–44. doi: 10.1089/cpb.1998.1.237
5. Zhou M, Zhu W, Sun X, and Huang L. Internet addiction and child physical and mental health: Evidence from panel dataset in China. J Affect Disord. (2022) 309:52–62. doi: 10.1016/j.jad.2022.04.115
6. Otsuka Y, Kaneita Y, Itani O, and Tokiya M. Relationship between internet addiction and poor mental health among Japanese adolescents. Iranian J Public Health. (2020) 49:2069–77. doi: 10.18502/ijph.v49i11.4722
7. Bernardi S and Pallanti S. Internet addiction: a descriptive clinical study focusing on comorbidities and dissociative symptoms. Compr Psychiatry. (2009) 50:510–6. doi: 10.1016/j.comppsych.2008.11.011
8. Mansfield R, Patalay P, and Humphrey N. A systematic literature review of existing conceptualisation and measurement of mental health literacy in adolescent research: current challenges and inconsistencies. BMC Public Health. (2020) 20:607. doi: 10.1186/s12889-020-08734-1
9. Li F, Cui Y, Li Y, Guo L, Ke X, Liu J, et al. Prevalence of mental disorders in school children and adolescents in China: diagnostic data from detailed clinical assessments of 17,524 individuals. J Child Psychol Psychiatry. (2021) 63:34–46. doi: 10.1111/jcpp.13445
10. Cui X and Chi X. The relationship between social support and internet addiction among chinese adolescents during the COVID - 19 pandemic: A multiple mediation model of resilience and post-traumatic stress disorder symptoms. Psychol Res Behav Manage. (2021) 14:1665–74. doi: 10.2147/PRBM.S305510
11. Dong H, Yang F, Lu X, and Hao W. Internet addiction and related psychological factors among children and adolescents in China during the coronavirus disease 2019 (COVID - 19) epidemic. Front Psychiatry. (2020) 11:00751. doi: 10.3389/fpsyt.2020.00751
12. Liu Y, Yuan H, Song C, Li L, Zhou W, and Wang W. Symptom relationships between internet addiction and anxiety across primary and middle school students during the Omicron lockdown. J Affect Disord. (2023) 329:251–6. doi: 10.1016/j.jad.2023.02.074
13. Servidio R, Bartolo MG, Palermiti AL, and Costabile A. Fear of COVID - 19, depression, anxiety, and their association with Internet addiction disorder in a sample of Italian students. J Affect Disord Rep. (2021) 4:100097. doi: 10.1016/j.jadr.2021.100097
14. Ding H, Cao B, and Sun Q. The association between problematic internet use and social anxiety within adolescents and young adults: a systematic review and meta-analysis. Front Public Health. (2023) 11:1275723. doi: 10.3389/fpubh.2023.1275723
15. Zhao L, Li X, Yang Q, Peng Y, Jiang L, Jia P, et al. The longitudinal association between internet addiction and depressive and anxiety symptoms among Chinese adolescents before and during the COVID - 19 pandemic. Front Public Health. (2022) 10:1096660. doi: 10.3389/fpubh.2022.1096660
16. Xie X, Cheng H, and Chen Z. Anxiety predicts internet addiction, which predicts depression among male college students: A cross-lagged comparison by sex. Front Psychol. (2022) 13:1102066. doi: 10.3389/fpsyg.2022.1102066
17. Kumar G, Dash P, Jnaneswar A, Suresan V, Jha K, and Ghosal S. Impact of internet addiction during COVID - 19 on anxiety and sleep quality among college students of Bhubaneswar city. J Educ Health Promot. (2022) 11:156. doi: 10.4103/jehp.jehp_396_21
18. Yfanti T, Zygouris NC, Chondropoulos I, and Stamoulis GI eds. Internet addiction and anxiety among greek adolescents: an online survey. In: The Challenges of the Digital Transformation in Education: Proceedings of the 21st International Conference on Interactive Collaborative Learning (ICL2018)-Volume 1. Cham: Springer.
19. Perez-Oyola JC, Walter-Chavez DM, Zila-Velasque JP, Pereira-Victorio CJ, Failoc-Rojas VE, Vera-Ponce VJ, et al. Internet addiction and mental health disorders in high school students in a Peruvian region: a cross-sectional study. BMC Psychiatry. (2023) 23:408. doi: 10.1186/s12888-023-04838-1
20. Dien TM, Chi PTL, Duy PQ, Anh LH, Ngan NTK, and Hoang Lan VT. Prevalence of internet addiction and anxiety, and factors associated with the high level of anxiety among adolescents in Hanoi, Vietnam during the COVID - 19 pandemic. BMC Public Health. (2023) 23:2441. doi: 10.1186/s12889-023-17348-2
21. Andrade ALM, Scatena A, Bedendo A, Enumo SRF, Dellazzana-Zanon LL, Prebianchi HB, et al. Findings on the relationship between Internet addiction and psychological symptoms in Brazilian adults. Int J Psychol. (2020) 55:941–50. doi: 10.1002/ijop.12670
22. Kim Y-J, Jang HM, Lee Y, Lee D, and Kim D-J. Effects of internet and smartphone addictions on depression and anxiety based on propensity score matching analysis. Int J Environ Res Public Health. (2018) 15:859. doi: 10.3390/ijerph15050859
23. Borsboom D. A network theory of mental disorders. World Psychiatry. (2017) 16:5–13. doi: 10.1002/wps.20375
24. Borsboom D and Cramer AO. Network analysis: an integrative approach to the structure of psychopathology. Annu Rev Clin Psychol. (2013) 9:91–121. doi: 10.1146/annurev-clinpsy-050212-185608
25. Robinaugh DJ, Millner AJ, and McNally RJ. Identifying highly influential nodes in the complicated grief network. J Abnorm Psychol. (2016) 125:747–57. doi: 10.1037/abn0000181
26. Cramer AO, Waldorp LJ, van der Maas HL, and Borsboom D. Comorbidity: a network perspective. Behav Brain Sci. (2010) 33:137–50; discussion 50-93. doi: 10.1017/S0140525X09991567
27. Cai H, Xi H-T, An F, Wang Z, Han L, Liu S, et al. The association between internet addiction and anxiety in nursing students: A network analysis. Front Psychiatry. (2021) 12:723355. doi: 10.3389/fpsyt.2021.723355
28. Tan Y, Deng J, Zhang D, Peng C, and Peng A. Social anxiety and suicidal ideation among middle-school students in China: a mediation model of internet addiction. Front Psychiatry. (2023) 14:1337577. doi: 10.3389/fpsyt.2023.1337577
29. Potembska E, Pawłowska B, and Szymańska J. Psychopathological symptoms in individuals at risk of Internet addiction in the context of selected demographic factors. Ann Agric Environ Med. (2019) 26:33–8. doi: 10.26444/aaem/81665
30. Del Ponte A, Li L, Ang L, Lim N, and Seow WJ. Evaluating SoJump.com as a tool for online behavioral research in China. J Behav Exp Finance. (2024) 41:100905. doi: 10.1016/j.jbef.2024.100905
31. Ran M-S, Wang C, Cai J, Deng Z-Y, Mu Y-F, Huang Y, et al. The mutual overlapping impact of stress and infection on mental health problems in adolescents and youths during and after COVID - 19 pandemic in China. J Affect Disord. (2024) 347:500–8. doi: 10.1016/j.jad.2023.12.009
32. Deng A-P, Wang C, Cai J, Deng Z-Y, Mu Y-F, Song H-J, et al. Effects of internet addiction and academic satisfaction on mental health among college students after the lifting of COVID - 19 restrictions in China. Front Psychiatry. (2023) 14:1243619. doi: 10.3389/fpsyt.2023.1243619
33. Song H-J, Mu Y-F, Wang C, Cai J, Deng Z-Y, Deng A-P, et al. Academic performance and mental health among Chinese middle and high school students after the lifting of COVID - 19 restrictions. Front Psychiatry. (2023) 14:1248541. doi: 10.3389/fpsyt.2023.1248541
34. Spitzer RL, Kroenke K, Williams JBW, and Löwe B. A brief measure for assessing generalized anxiety disorder. Arch Internal Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
35. Spitzer RL, Kroenke K, Williams JB, and Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
36. Zhang C, Wang T, Zeng P, Zhao M, Zhang G, Zhai S, et al. Reliability, validity, and measurement invariance of the general anxiety disorder scale among chinese medical university students. Front Psychiatry. (2021) 12:648755. doi: 10.3389/fpsyt.2021.648755
37. Lai CM, Mak KK, Watanabe H, Ang RP, Pang JS, and Ho RC. Psychometric properties of the internet addiction test in Chinese adolescents. J Pediatr Psychol. (2013) 38:794–807. doi: 10.1093/jpepsy/jst022
38. Khazaal Y, Achab S, Billieux J, Thorens G, Zullino D, Dufour M, et al. Factor structure of the internet addiction test in online gamers and poker players. JMIR Ment Health. (2015) 2:e12. doi: 10.2196/mental.3805
39. Friedman J, Hastie T, and Tibshirani R. Sparse inverse covariance estimation with the graphical lasso. Biostatistics. (2008) 9:432–41. doi: 10.1093/biostatistics/kxm045
40. Epskamp S, Cramer AOJ, Waldorp LJ, Schmittmann VD, and Borsboom D. qgraph: network visualizations of relationships in psychometric data. J Stat Software. (2012) 48:1–18. doi: 10.18637/jss.v048.i04
41. Ocloo IX and Chen H. Feature selection in high-dimensional models via EBIC with energy distance correlation. Entropy. (2023) 25:14. doi: 10.3390/e25010014
42. Jones PJ, Ma R, and McNally RJ. Bridge centrality: A network approach to understanding comorbidity. Multivariate Behav Res. (2019) 56:353–67. doi: 10.1080/00273171.2019.1614898
43. Epskamp S, Borsboom D, and Fried EI. Estimating psychological networks and their accuracy: A tutorial paper. Behav Res Methods. (2018) 50:195–212. doi: 10.3758/s13428-017-0862-1
44. Vargha A and Delaney HD. A critique and improvement of the CL common language effect size statistics of mcGraw and wong. J Educ Behav Stat. (2016) 25:101–32. doi: 10.2307/1165329
45. Soffer-Dudek N and Somer E. Trapped in a daydream: daily elevations in maladaptive daydreaming are associated with daily psychopathological symptoms. Front Psychiatry. (2018) 9:194. doi: 10.3389/fpsyt.2018.00194
46. Cheah C, Yu J, Hart C, Sun S, and Olsen J. Confirming the multidimensionality of psychologically controlling parenting among chinese-american mothers: love withdrawal, guilt induction, and shaming. Int J Behav Dev. (2015) 39:285–92. doi: 10.1177/0165025414562238
47. Dong X and Xu Y. Filial piety among global chinese adult children: A systematic review. Res Rev. (2016) 2:46–55.
48. Throuvala MA, Griffiths MD, Rennoldson M, and Kuss DJ. Perceived challenges and online harms from social media use on a severity continuum: A qualitative psychological stakeholder perspective. Int J Environ Res Public Health. (2021) 18:3227. doi: 10.3390/ijerph18063227
49. Zhu X, Lian W, and Fan L. Network analysis of internet addiction, online social anxiety, fear of missing out, and interpersonal sensitivity among chinese university students. Depress Anxiety. (2024) 2024:5447802. doi: 10.1155/2024/5447802
50. Lüscher C, Robbins TW, and Everitt BJ. The transition to compulsion in addiction. Nat Rev Neurosci. (2020) 21:247–63. doi: 10.1038/s41583-020-0289-z
51. Campbell S and Osborn TL. Adolescent psychopathology and psychological wellbeing: a network analysis approach. BMC Psychiatry. (2021) 21:333. doi: 10.1186/s12888-021-03331-x
52. He Y, Wu C, LeMoult J, Huang J, Zhao Y, Liang K, et al. Exploring symptom-level associations between anxiety and depression across developmental stages of adolescence: a network analysis approach. BMC Psychiatry. (2023) 23:941. doi: 10.1186/s12888-023-05449-6
53. American Psychiatric A. Diagnostic and statistical manual of mental disorders. Arlington, VA, US: American Psychiatric Publishing, Inc (2013) p. xliv, 947–xliv.
54. WHO. Anxiety disorders (2023). Available online at: https://www.who.int/news-room/fact-sheets/detail/anxiety-disorders (Accessed March 1, 2025).
55. Brand M. Can internet use become addictive? Science. (2022) 376:798–9. doi: 10.1126/science.abn4189
56. Santer ND, Manago A, Starks A, and Reich SM. Early adolescents’ perspectives on digital privacy. Algorithmic Rights Protect Children. (2021). doi: 10.1162/ba67f642.646d0673
57. Russo A, Santoro G, and Schimmenti A. Interpersonal guilt and problematic online behaviors: the mediating role of emotion dysregulation. Clin Neuropsych. (2022) 19:236–47. doi: 10.36131/cnfioritieditore20220406
58. Lam LT. Internet gaming addiction, problematic use of the internet, and sleep problems: A systematic review. Curr Psychiatry Rep. (2014) 16:444. doi: 10.1007/s11920-014-0444-1
59. Palmer CA, Bower JL, Cho KW, Clementi MA, Lau S, Oosterhoff B, et al. Sleep loss and emotion: A systematic review and meta-analysis of over 50 years of experimental research. psychol Bull. (2024) 150:440–63. doi: 10.1037/bul0000410
60. Krause AJ, Simon EB, Mander BA, Greer SM, Saletin JM, Goldstein-Piekarski AN, et al. The sleep-deprived human brain. Nat Rev Neurosci. (2017) 18:404–18. doi: 10.1038/nrn.2017.55
61. Mi Y, Duan H, Xu Z, and Lei X. The impact of sleep deprivation on brain networks in response to social evaluation tasks. Brain Sci. (2023) 13:1122. doi: 10.3390/brainsci13081122
62. Nie Z, Li M, Waheed M, Kasimon D, and Wan Abas WAB. The impact of the density of individual social networks on weChat usage in intimate relationships among chinese youngsters. Journal Media. (2023) 4:377–95. doi: 10.3390/journalmedia4010025
63. Cai H, Bai W, Sha S, Zhang L, Chow IHI, Lei SM, et al. Identification of central symptoms in Internet addictions and depression among adolescents in Macau: A network analysis. J Affect Disord. (2022) 302:415–23. doi: 10.1016/j.jad.2022.01.068
64. Bai C, Guan W, Wang D, and Chen X. Digital village construction and the quality of life of rural residents. Int Rev Econom Finance. (2024) 96:103729. doi: 10.1016/j.iref.2024.103729
65. Mamabolo MJ and Durodolu OO. Rural accessibility to digital libraries: requirements and challenges. Digital Library Perspect. (2023) 39:551–70. doi: 10.1108/DLP-04-2023-0025
66. Singh J and Kaur D. Academic pressure and its psychological impact on teenage boys and girls: A rural-urban comparative study. Int J Environ Sci. (2025) 11:758–62. doi: 10.64252/n5tgjw44
67. Luebbe AM, Bump KA, Fussner LM, and Rulon KJ. Perceived maternal and paternal psychological control: relations to adolescent anxiety through deficits in emotion regulation. Child Psychiatry Hum Dev. (2014) 45:565–76. doi: 10.1007/s10578-013-0425-3
68. Chan LS. Multiple uses and anti-purposefulness on Momo, a Chinese dating/social app. Inform Commun Society. (2020) 23:1515–30. doi: 10.1080/1369118X.2019.1586977
69. Mestre-Bach G, Fernandez-Aranda F, and Jiménez-Murcia S. Exploring Internet gaming disorder: an updated perspective of empirical evidence (from 2016 to 2021). Compr Psychiatry. (2022) 116:152319. doi: 10.1016/j.comppsych.2022.152319
Keywords: anxiety, internet addiction disorder, comorbidity, network analysis, adolescent, China
Citation: Xie Y, Cheng X-F, Wang C, Cai J, Wang Y, Mu Y-F, Deng Z-Y, Deng A-P, Song H-J, Huang X-H, Zhang L, Zhang J, Huang Y, Yin L, Shen W-W, Li M-L and Ran M-S (2025) Symptom-level interactions between anxiety and internet addiction in Chinese adolescents: a large-scale network and residence difference analysis. Front. Psychiatry 16:1558276. doi: 10.3389/fpsyt.2025.1558276
Received: 10 January 2025; Accepted: 20 August 2025;
Published: 16 September 2025.
Edited by:
Lei Shi, Guangzhou Medical University, ChinaReviewed by:
Ted C. T. Fong, The University of Hong Kong, Hong Kong SAR, ChinaSizhe Cheng, Air Force Harbin Flying College, China
Copyright © 2025 Xie, Cheng, Wang, Cai, Wang, Mu, Deng, Deng, Song, Huang, Zhang, Zhang, Huang, Yin, Shen, Li and Ran. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ming-Li Li, bGltaW5nbGlAd2Noc2N1LmNu; Mao-Sheng Ran, bXNyYW5jZEBvdXRsb29rLmNvbQ==
†These authors have contributed equally to this work