 Xiaomei Hu
Xiaomei Hu Yanying Pan1
Yanying Pan1 You Zhang
You Zhang- 1College of Acupuncture, Massage, and Rehabilitation, Hunan University of Chinese Medicine, Changsha, Hunan, China
- 2College of Medical Imaging Laboratory and Rehabilitation, Xiangnan University, Chenzhou, Hunan, China
Objective: This research aims to assess the therapeutic effects and safety of treatments for PSD by conducting a thorough systematic review and meta-analysis.
Methods: Randomized controlled trials (RCTs) were retrieved from PubMed, Embase, Web of Science, The Cochrane Library, China National Knowledge Infrastructure (CNKI), and Wan Fang, covering all available records up to September 30, 2024. RCTs evaluating on the efficacy and safety of electroacupuncture in individuals with PSD were included. The robustness of the findings and possible contributors to heterogeneity were examined via sensitivity and subgroup analyses. Statistical analyses were conducted utilizing STATA 15.0 and Review Manager 5.4.
Results: This study included 65 RCTs with a total of 5,362 participants. The results showed that electroacupuncture exhibited significantly greater clinical effectiveness compared to the control group (RR = 1.16, 95% CI [1.11, 1.22], I² = 59%, p < 0.00001), effectively reducing HAMD scores (SMD = -0.56, 95% CI [-0.72, -0.40], I² = 87%, p < 0.00001), SDS scores (SMD = -0.56, 95% CI [-0.87, -0.24], I² = 90%, p = 0.006), and TCM-DS scores (SMD = -0.52, 95% CI [-0.78, -0.27], I² = 0%, p < 0.0001). The incidence of adverse reactions was lower in the electroacupuncture (EA) intervention group (RR = 0.54, 95% CI [0.35, 0.83], I² = 0%, p = 0.004).The most commonly used acupoints were primarily located along the Gallbladder, Bladder, and Du Meridian, with the five most frequently used acupoints being: Baihui (GV20, 41 times), Shenting (DU24, 28 times), Taichong (LV3, 28 times), Shenmen (HT7, 26 times), and Neiguan (PC6, 22 times).
Conclusion: Electroacupuncture could serve as a safe and effective complementary therapy for PSD. It is recommended that multicenter, large-scale, and high-quality RCTs be conducted to further validate these findings.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024618618, identifier CRD42024618618
1 Introduction
Stroke ranks among the leading causes of death and long-term disability globally, causing significant neurological damage and functional limitations that greatly affect patients’ quality of life and recovery. In addition to neurological impairments, post-stroke depression (PSD) is a prevalent and concerning neuropsychiatric issue following a stroke (1). PSD is characterized by persistent depressive symptoms, emotional disturbances, and cognitive impairment, with a global prevalence estimated to range from 27% to 30% (2). The pathogenesis of PSD is complex, involving factors such as gender, a history of mental illness, the type of stroke, damage to the frontal and temporal lobes, insufficient social support, and severe physical disability, among others (3, 4). PSD often leads to a chronic and recurrent course, significantly impairing patients’ quality of life, delaying functional recovery, and increasing the risk of stroke recurrence and mortality. Current mainstream treatments still rely primarily on antidepressant medications and psychological therapies; however their efficacy is limited, and they are often accompanied by notable side effects—such as sleep disturbances, gastrointestinal discomfort, and sexual dysfunction—and even carry a risk of suicide triggered by overdose (5). Consequently, an increasing number of patients are turning to complementary and alternative therapies for managing PSD.
Electroacupuncture (EA), a modern technique combining traditional acupuncture with the delivery of low-frequency electrical pulses to specific acupoints, regulates the body’s electrical activity and energy flow, thereby achieving therapeutic benefits (6). Clinical studies have demonstrated that EA stimulation at acupoints on both the head—such as Baihui (GV20) and Yintang (GV29)—and the limbs—such as Taichong (LR3) and Hegu (LI4)—can significantly alleviate clinical symptoms in patients with mild to moderate post-stroke depression (PSD) (7, 8). Although the precise mechanism of action of EA is not yet fully understood, studies suggest that it may help restore neurological function and potentially stabilize post-stroke mood and cognition by modulating the central nervous system (9), reducing inflammation (10), and improving blood circulation (11).
To date, two systematic reviews on EA for the treatment of PSD have been published, one in 2018 (12) and the other in 2021 (13). These studies have summarized the existing evidence but ultimately reached contradictory conclusions. In addition, several new randomized controlled trials (RCTs) on EA for PSD have been conducted in recent years (7, 14). Accordingly, we conducted a meta-analysis and systematic review to assess safety and efficacy of EA in management of PSD, aiming to offer evidence-based guidance for its clinical use.
2 Materials and methods
2.1 Protocol and registration
This study followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), including its protocols and extension statements for meta-analysis. The meta-analysis was registered in the International Prospective Register of Systematic Reviews (PROSPERO) with the registration number CRD42024618618.
2.2 Search methods
A thorough literature search was conducted across multiple databases, including PubMed, Embase, Web of Science (WOS), The Cochrane Library, Wan Fang, and China National Knowledge Infrastructure (CNKI), to identify RCTs published up to September 20, 2024. The focus was on studies evaluating the use of electroacupuncture as a complementary therapy for post-stroke depression. No language or geographical restrictions were applied to the search. The search terms included: “Electroacupuncture” and “Stroke” OR “Cerebrovascular Accident” OR “Cerebral Stroke” OR “Cerebrovascular Apoplexy” OR “Brain Vascular Accident” OR “Apoplexy” OR “CVA” (Cerebrovascular Accident) OR “Acute Stroke” OR “Acute Cerebrovascular Accident” AND “Depression” OR “Depressive Symptoms” OR “Depressive Disorder” AND “Randomized Controlled Trial” OR “Randomized Trials”. To ensure a comprehensive review, additional relevant studies were identified through a manual examination of the reference lists of articles meeting the inclusion criteria. The full search strategies can be found in Supplementary Table S1.
2.3 Study selection
Following a comprehensive evaluation process, RCTs were selected based on an assessment of titles, abstracts, and full texts. The selection process was guided by specific inclusion and exclusion criteria, outlined as follows:
Inclusion Criteria:
a. Participants: The studies included adults aged 18 or older who were clinically diagnosed with PSD, with no restrictions on gender or ethnicity.
b. Intervention: The experimental group must have used EA or EA combined with other therapies, such as traditional Chinese medicine, antidepressant medication, or rehabilitation.
c. Control: The control group must have received non-electroacupuncture interventions.
d. Outcomes: The study was required to report minimum one of the following primary outcome measures: HAMDS, SDS, or TCM-DS. The secondary outcome measures included the overall efficacy rate and adverse reaction rate. The criteria for the overall efficacy rate are provided in Supplementary Table S2.
Exclusion Criteria:
a. Studies that are not RCTs, such as retrospective studies, animal experiments, or review articles.
b. Studies involving participants diagnosed with depression unrelated to stroke, or who did not show depressive symptoms after having a stroke.
c. Interventions in which the experimental group received EA in combination with other therapies not specified in the inclusion criteria.
d. Studies with inaccurate data or incomplete outcome measurements, where missing data could not be obtained from the authors.
e. Duplicate publications.
2.4 Data extraction
Two reviewers (PYY and TYS) independently conducted the initial screening of all retrieved literature using EndNote 9.0 software to eliminate duplicate studies. Subsequently, data were collected from the eligible studies, which included the following details:
Publication Details: Title, first author, and publication year.
Study Characteristics: Study design and duration of treatment.
Participant Information: Sample size gender, age, disease duration,
Intervention and Control: The intervention group reveived EA treatment, including specific acupoints, intensity, and frequency; the control group underwent alternative treatments, with specifications on dosage and frequency of administration.
For continuous data, the mean and standard deviation were recorded, whereas for categorical data, the number of events and total sample size were extracted.
A second round of screening was performed to identify studies meeting the inclusion criteria through a review of titles and abstracts. For studies where eligibility was unclear, the full texts were reviewed. In cases of disagreement, the final decision was made by a third reviewer (ZY). Once the final set of studies was determined, relevant data were extracted and synthesized.
2.5 Quality assessment
The quality of the included studies and the data extraction process were assessed using the Cochrane Collaboration’s Risk of Bias Tool for RCTs. Two reviewers (ZY and ZH) assessed the quality of the selected studies separately, and their assessments were cross-checked. The evaluation covered seven domains: random sequence generation, allocation concealment, blinding of participants and personnel, completeness of outcome data, reporting bias, and other potential biases. The methodological quality of the studies was classified into three categories: “high risk of bias,” “low risk of bias,” and “unclear risk of bias.” If the two reviewers disagreed, the final decision was made by a third reviewer (LZP).
2.6 Statistical analysis
EndNote 9.0 was used for reference management, Excel for data organization, and RevMan 5.4 and Stata 15.0 for statistical analysis. For binary outcomes, the risk ratio (RR) was employed as the effect size statistic, while for continuous outcomes, the standardized mean difference (SMD) was calculated. Heterogeneity was assessed using Cochrane’s Q test and I² statistics, with a significance level of α = 0.05 for the meta-analysis. Sensitivity analysis was performed by excluding studies one at a time. Publication bias was assessed using funnel plots and Egger’s test. Furthermore, subgroup analyses were conducted to evaluate the stability of outcomes and identify potential sources of heterogeneity.
3.Results
3.1Literature search and selection results
Through database searches, 625 relevant studies were initially identified. Following the removal of 206 duplicates, 419 studies were evaluated based on their titles and abstracts, leading to the exclusion of 233. The full-text review of the remaining 186 studies was conducted, resulting in the inclusion of 65 studies (14–78) (Figure 1).
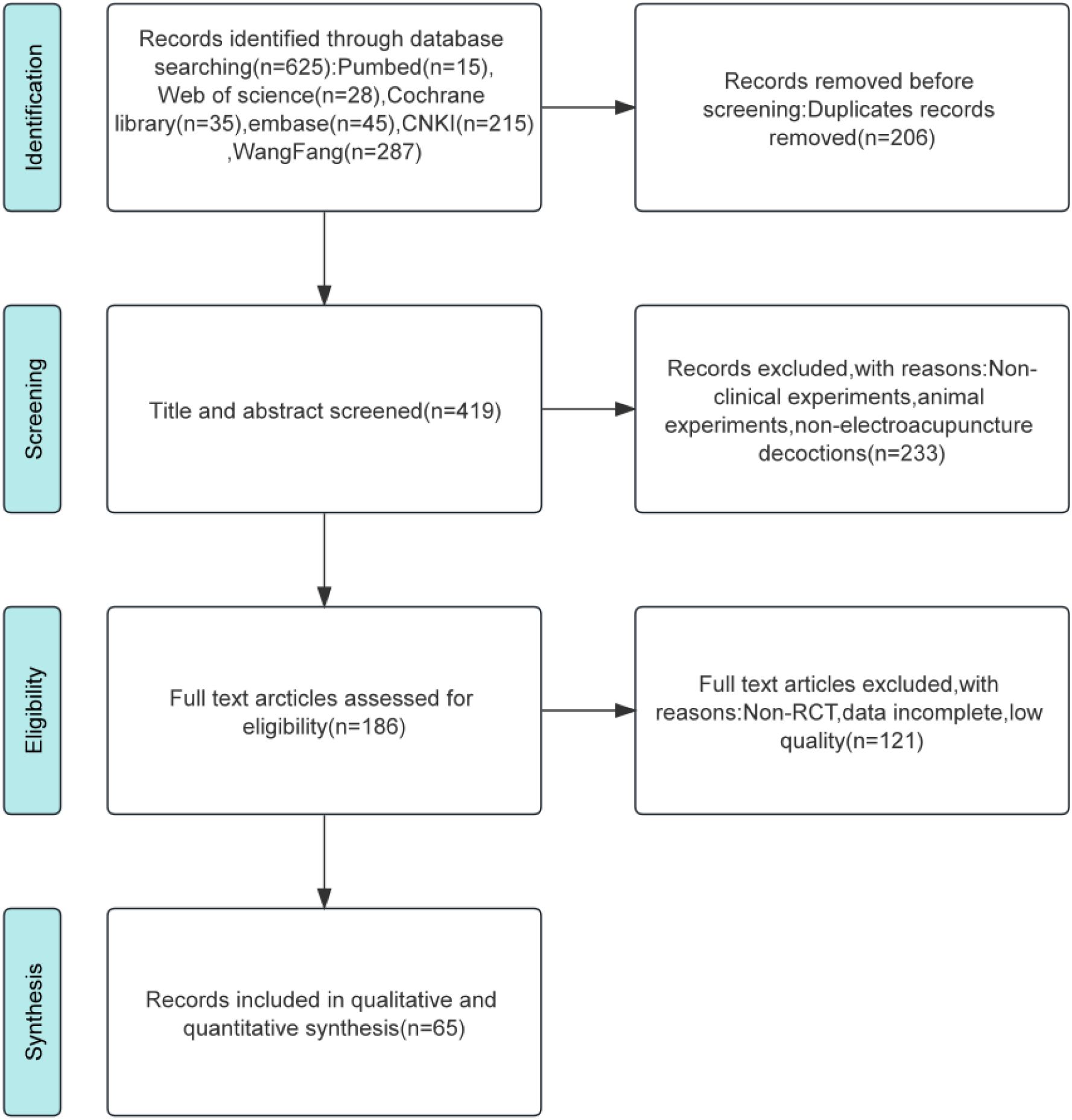
Figure 1. Flow chart of literature selection.
3.2 Study characteristics
A total of 65 relevant studies were obtained through database retrieval, with 2,823 participants in the EA intervention group and 2,539 participants in the control group. Both the intervention and control groups each had sample sizes exceeding 40 participants. The average age of patients in the EA intervention group ranged from 42.38 to 72 years, and in the control group, it ranged from 43.17 to 73.7 years. The treatment duration varied between 4 and 12 weeks. The interventions in the EA intervention group included EA alone, EA combined with Chinese herbal medicine, EA combined with antidepressants, EA combined with conventional medicine, and EA combined with rehabilitation therapy, among others. The control group received treatments such as standard pharmacotherapy, rehabilitation, Chinese herbal medicine, or non-electroacupuncture needle therapy. Across the studies, a total of 57 acupuncture points were utilized for EA therapy, with the five most frequently used points being Bai Hui (GV 20), Shen Ting (GV 24), Tai Chong (LR 3), Shen Men (HT 7), and Nei Guan (PC 6). Details on study characteristics, criteria for clinical efficacy evaluation, intervention measures, outcomes, and acupuncture points are provided in Supplementary Table S3, S4. All acupuncture points referenced in the formulas adhered to the international standard nomenclature for acupuncture (79).
3.3 Bias risk assessment results
The Cochrane Risk of Bias Assessment Tool was used to evaluate the quality of the included studies. Out of 65 studies, 60 employed random number tables for allocation, which were categorised as low risk of bias. One study (27) did not disclose the allocation method and was rated as unknown risk. Three studies (46, 47, 50) allocated participants by order of enrollment, and one study (67) allocated based on treatment, both rated as high risk of bias. Ten studies (14, 16–18, 41, 54–56, 70) explicitly reported allocation concealment and were categorized as low risk, while the remaining 55 studies were categorized as unknown risk. Two studies (18, 41) had non-blinding of participants and personnel, indicating high risk of bias, while 63 studies did not report blinding, rated as unknown risk. Additionally, five studies (17, 18, 24, 25, 46) reported blinding of outcomes and were rated low risk, while two studies (25, 52) had non-blinding of outcomes, rated high risk. Complete outcome data were available for all studies, which were rated as having a low risk of bias, with no other sources of bias identified (Figure 2).
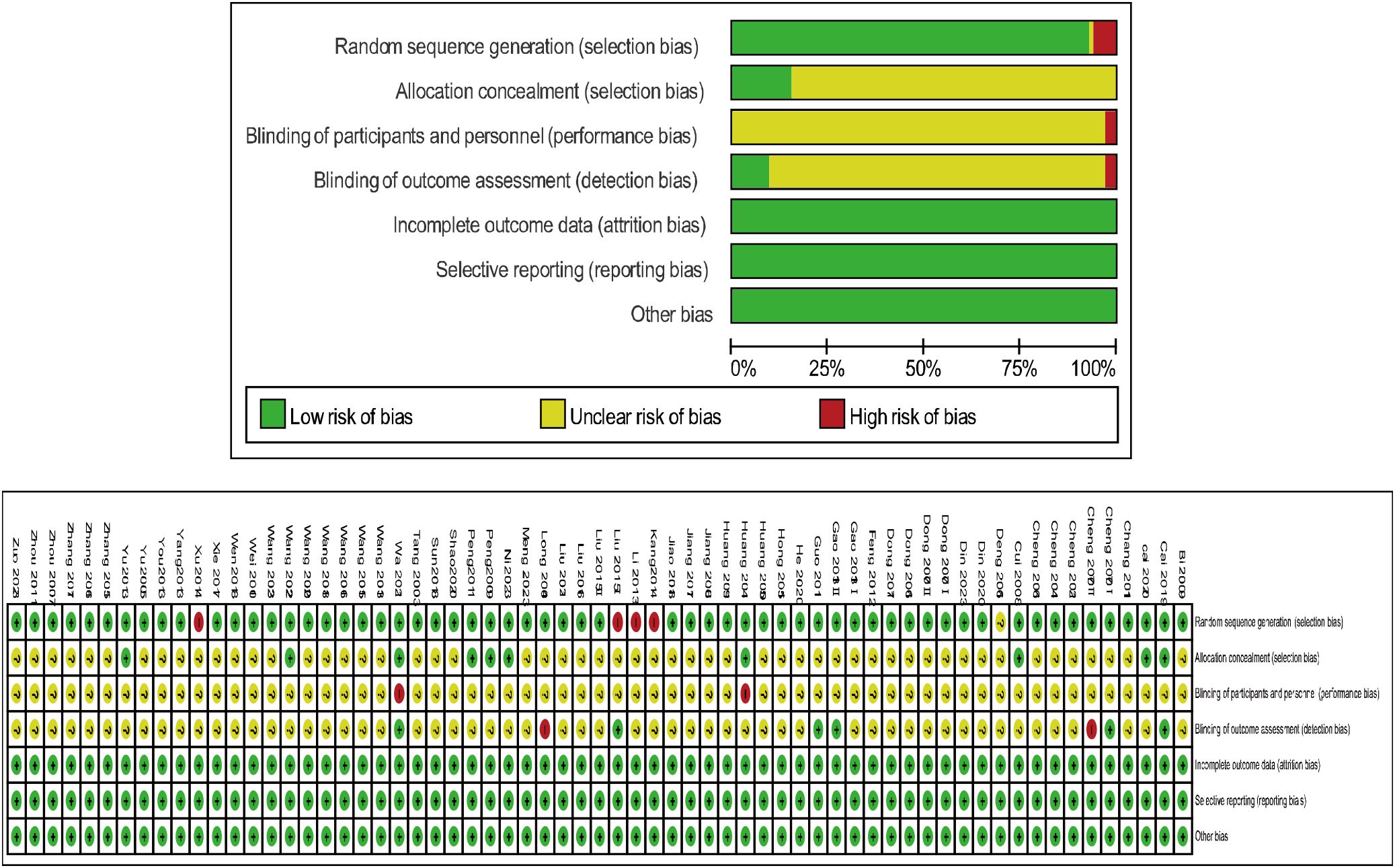
Figure 2. Bias risk assessment results.
3.4 Change in HAMD
The analysis of clinical efficacy outcomes included a total of 75 studies. The findings showed that the EA intervention group exhibited a greater reduction in HAMD scores in individuals with PSD in comparison to the control group (SMD = -0.56, 95% CI [-0.72, -0.40], I² = 87%, p < 0.00001) (Figure 3).
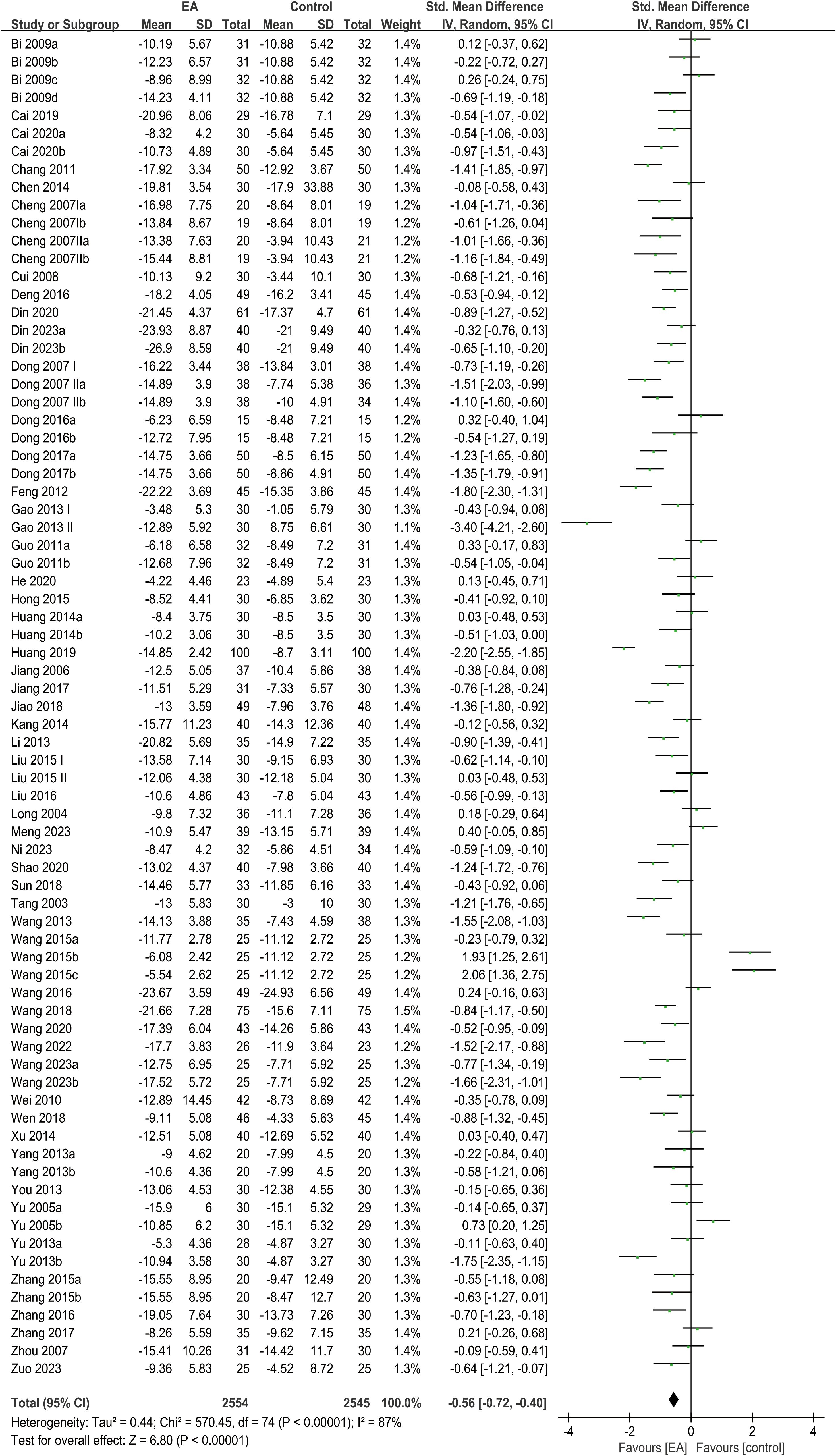
Figure 3. Forest plot of HAMD.
Subgroup analyses were performed according to intervention types, treatment duration, and patient age. The results of the analysis revealed no significant difference in HAMD score reduction between the intervention and control groups in the EA combined with rehabilitation group, the EA combined with conventional medicine group, or the subgroup with an intervention duration greater than 6 weeks. In contrast, significant reductions in HAMD scores were observed in other subgroups, including the standalone EA group, EA combined with antidepressants, EA combined with both antidepressants and rehabilitation, EA combined with Chinese herbal medicine, and subgroups with intervention durations of 6 weeks or less, as well as those stratified by age (> 60 years and ≤ 60 years) (Table 1).
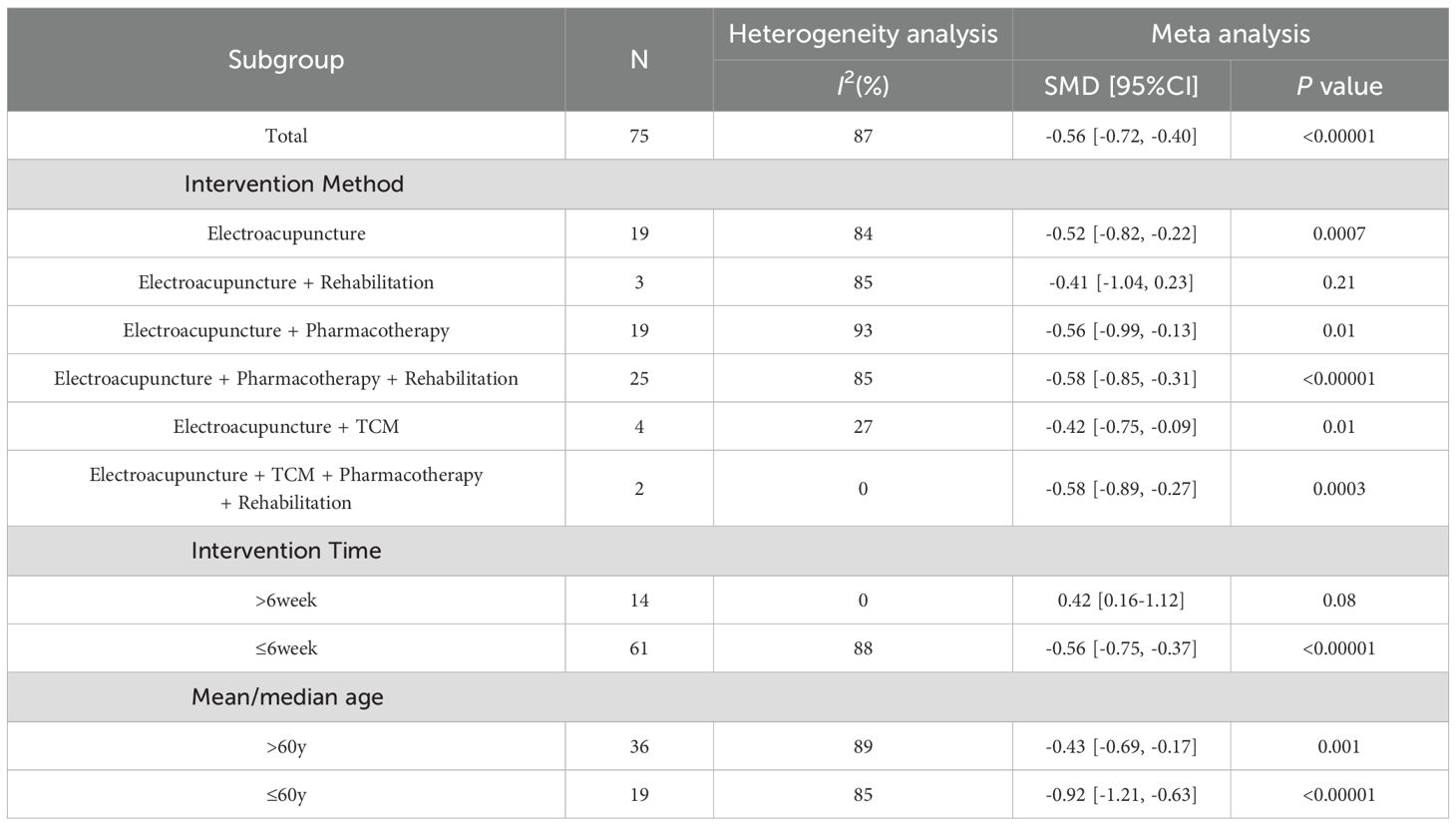
Table 1. HAMD subgroup analysis.
3.5 Change in SDS
The analysis of clinical efficacy outcomes included 24 studies in total. The results indicated that the EA intervention group achieved a significantly greater reduction in SDS scores in patients with PSD compared to the control group (SMD = -0.56, 95% CI [-0.87, -0.24], I² = 90%, p = 0.006) (Figure 4).
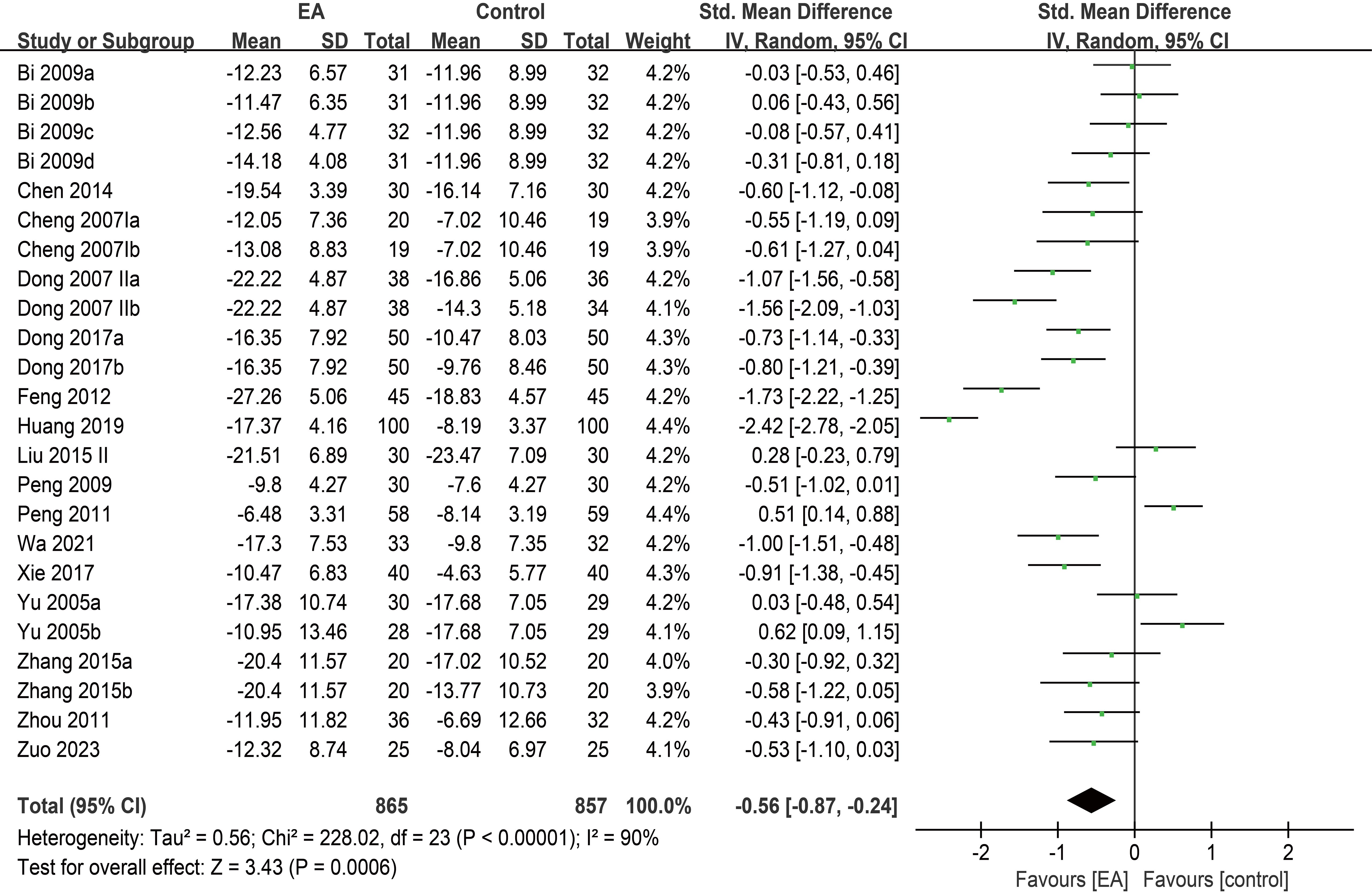
Figure 4. Forest plot of SDS.
Subgroup analyses showed no statistically significant difference in SDS improvement between the intervention and control groups in the EA combined with rehabilitation group, the EA combined with antidepressants and rehabilitation group, the EA combined with Chinese herbal medicine group, the EA combined with conventional medicine group, and the subgroup with age > 60 years. In contrast, statistically significant reduction in SDS scores was observed in the remaining subgroups, including the standalone EA group, the EA combined with antidepressants group, the subgroup with intervention duration > 6 weeks, the subgroup with intervention duration ≤ 6 weeks, and the subgroup with age ≤ 60 years (Table 2).
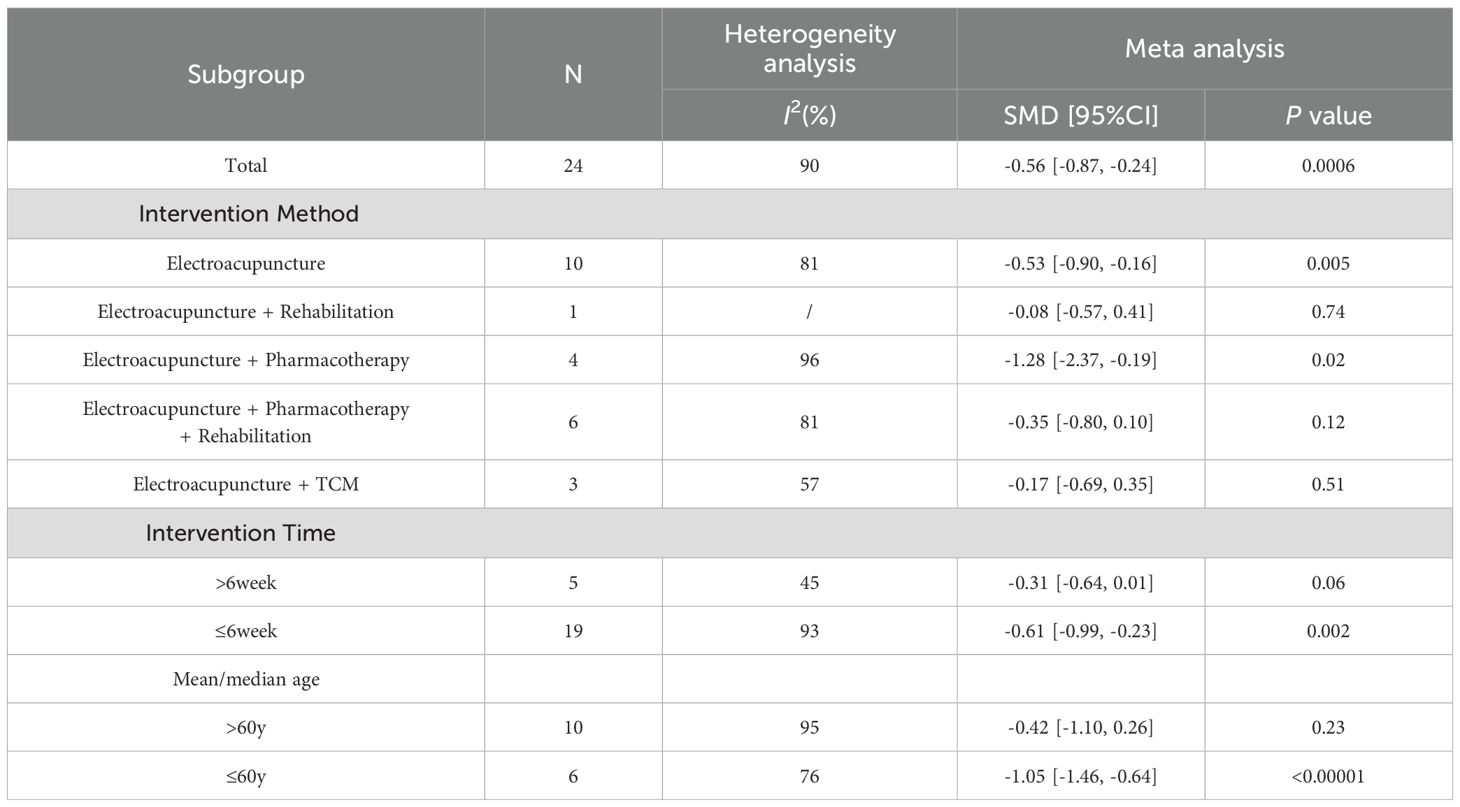
Table 2. SDS subgroup analysis.
3.6 Change in TCM-DS
The analysis of clinical efficacy outcome measures included a total of 4 studies. The results indicated that the reduction in TCM-DS scores was more pronounced in the EA intervention group compared to the control group in patients with post-stroke depression (SMD = -0.52, 95% CI [-0.78, -0.27], I² = 0%, p < 0.0001) (Figure 5).
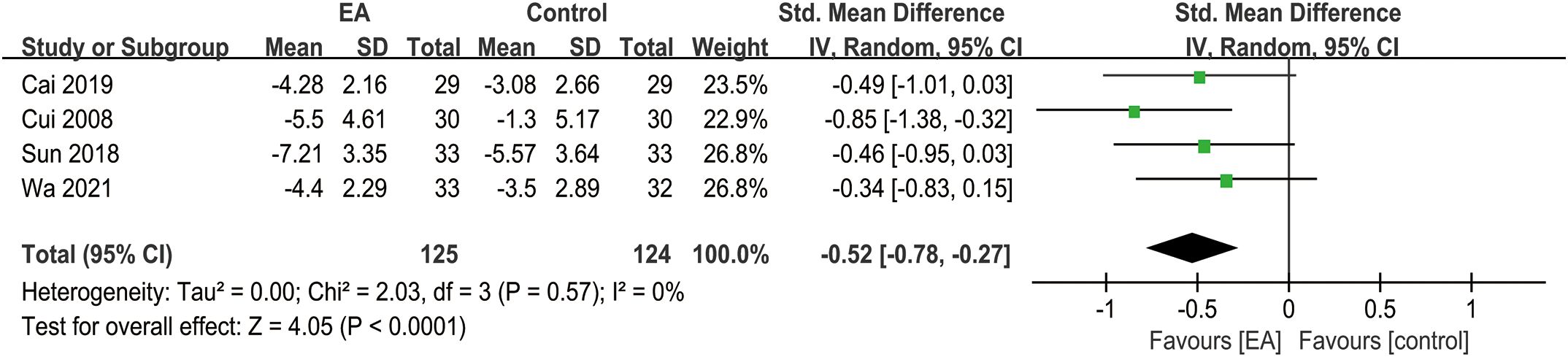
Figure 5. Forest plot of TCM-DS.
3.7 Overall efficacy rate
The analysis of clinical efficacy outcomes included 43 studies in total. The EA intervention group and control groups showed no significant difference in improving the overall efficacy rate for post-stroke depression. (RR = 1.16, 95% CI [1.11, 1.22], I² = 59%, p < 0.00001) (Figure 6).
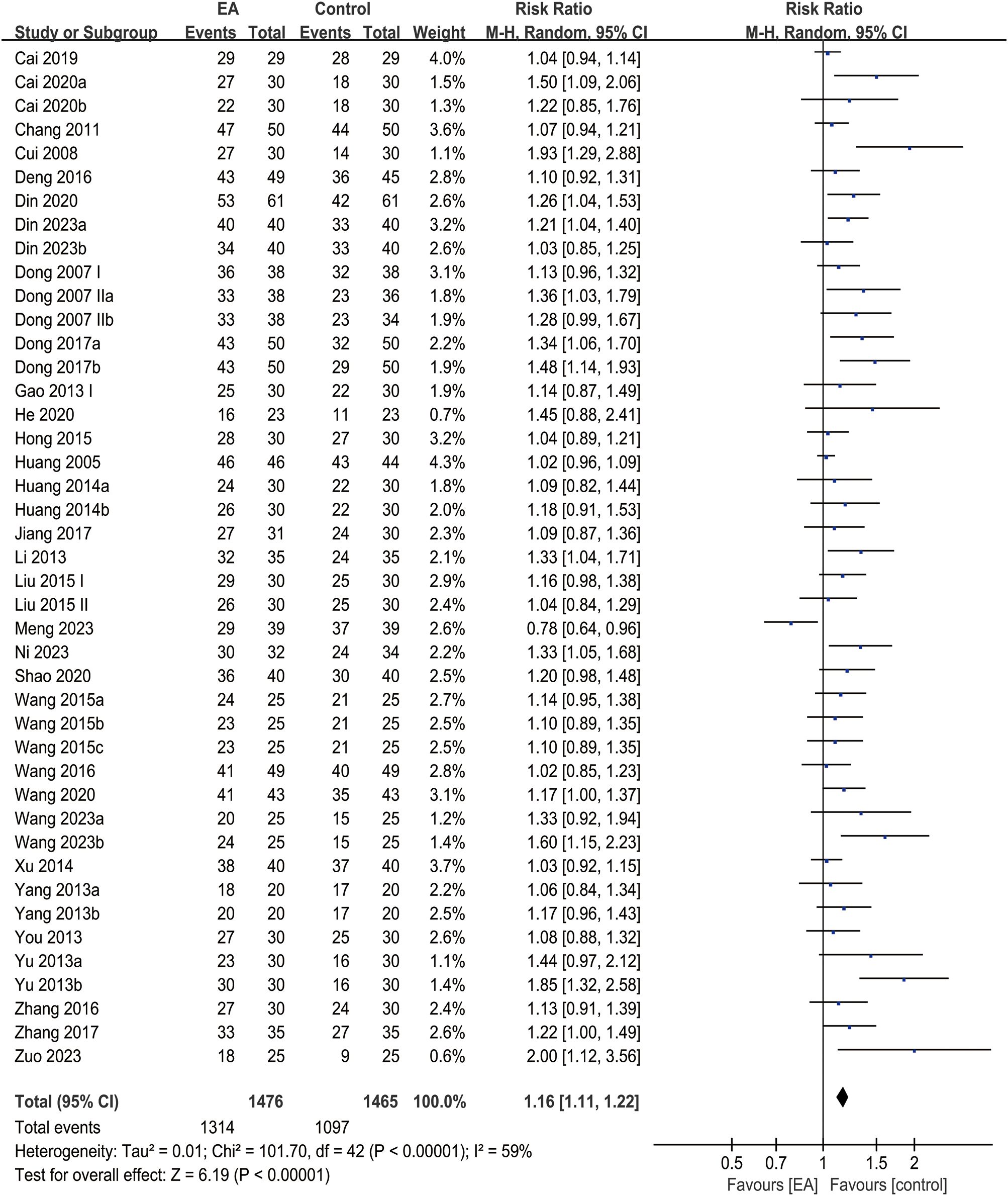
Figure 6. Forest plot of overall efficacy rate.
3.8 Adverse reaction rate
The analysis of clinical efficacy outcomes included a total of 18 studies. The results indicated that the adverse reaction rate of EA for post-stroke depression was significantly lower than that of the control group (RR = 0.54, 95% CI [0.35, 0.83], I² = 0%, p = 0.004) (Figure 7).
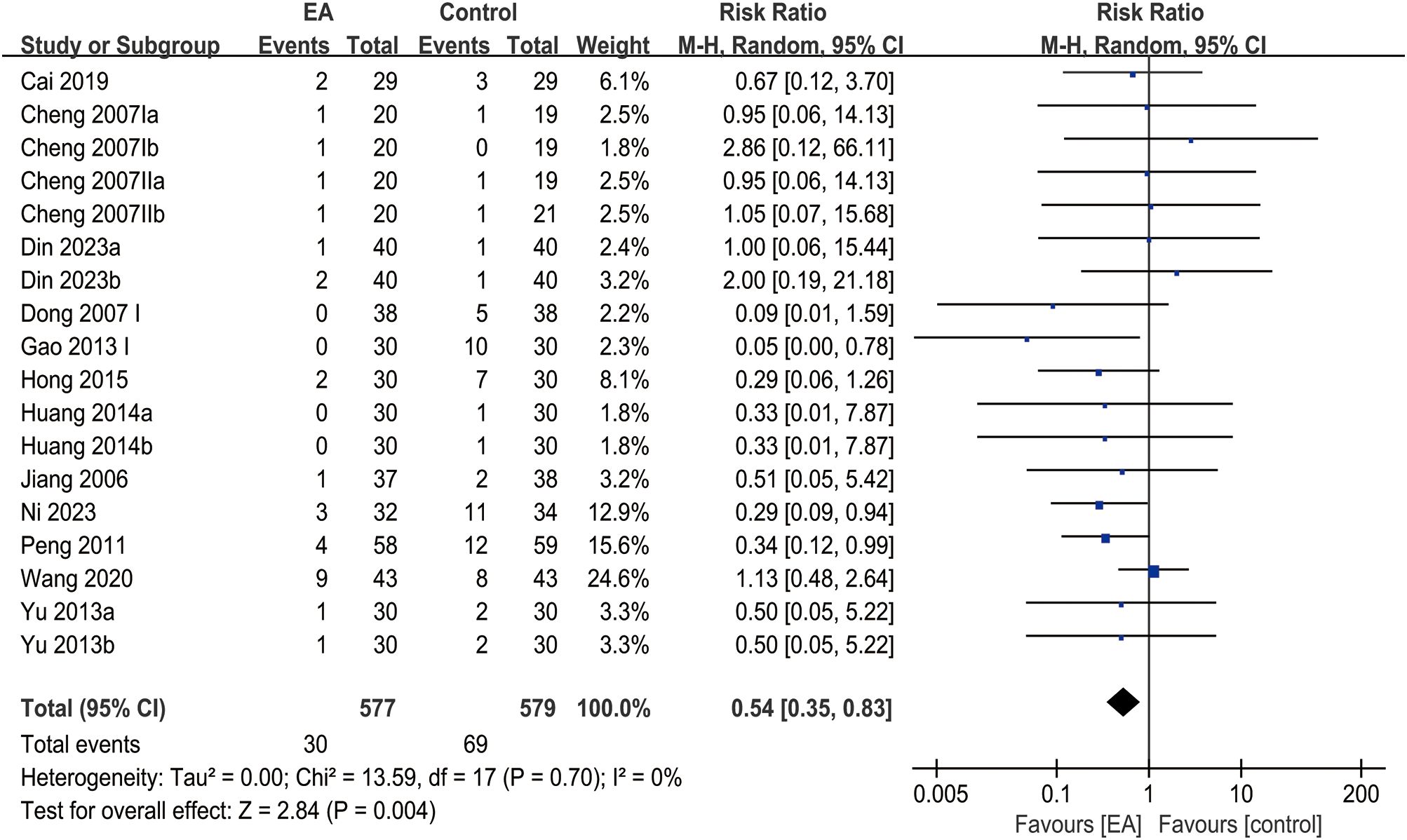
Figure 7. Forest plot of adverse reaction rate.
3.9 Publication bias and sensitivity analysis
The funnel plots for the overall efficacy rate displayed asymmetry (Figure 8D), suggesting potential publication bias. However, the funnel plots for other indicators, such as HAMD (Figure 8A), SDS (Figure 8B), TCM-DS (Figure 8C), and adverse reaction rate (Figure 9E), demonstrated acceptable symmetry. Egger’s test was used to evaluate publication bias, which revealed significant bias for the overall efficacy rate. (p = 0.0000), No bias was observed for HAMD, SDS, TCM-DS, or adverse reaction rate (p = 0.372, p = 0.334, p = 0.215, p = 0.163, p = 0.695). To assess the robustness of the results, sensitivity analyses were performed, and the results indicated that the sensitivity of all indicators, including HAMD (Figure 9A), SDS (Figure 9B), TCM-DS (Figure 9C), overall efficacy rate (Figure 9D), and adverse reaction rate (Figure 9E), remained stable. Sensitivity analysis details are provided in Supplementary Table S5.
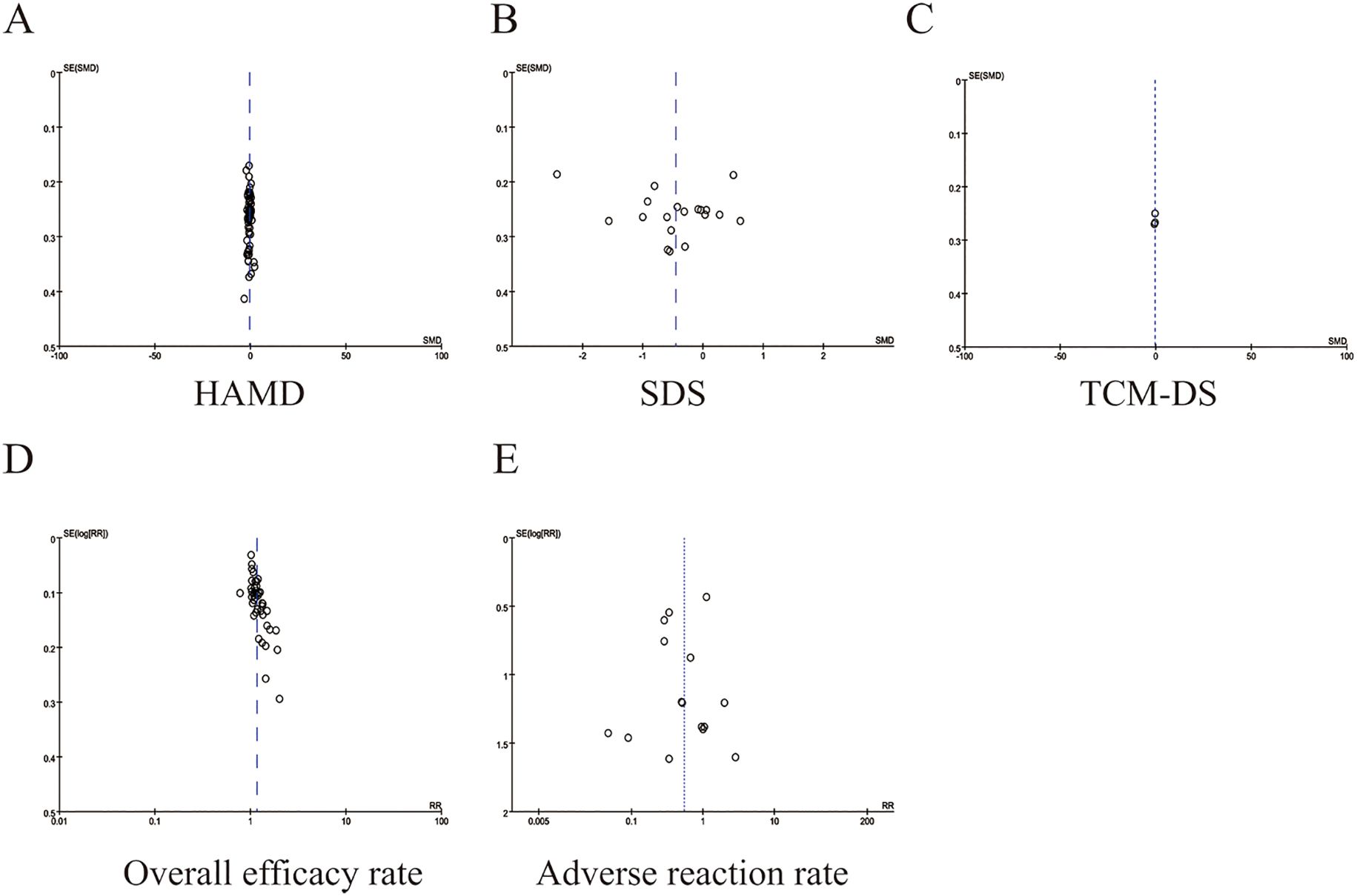
Figure 8. Funnel plots of outcomes. (A) HAMD (B) SDS (C) TCM-DS (D) Overall efficicacy rate (E) Aderverse reaction rate.
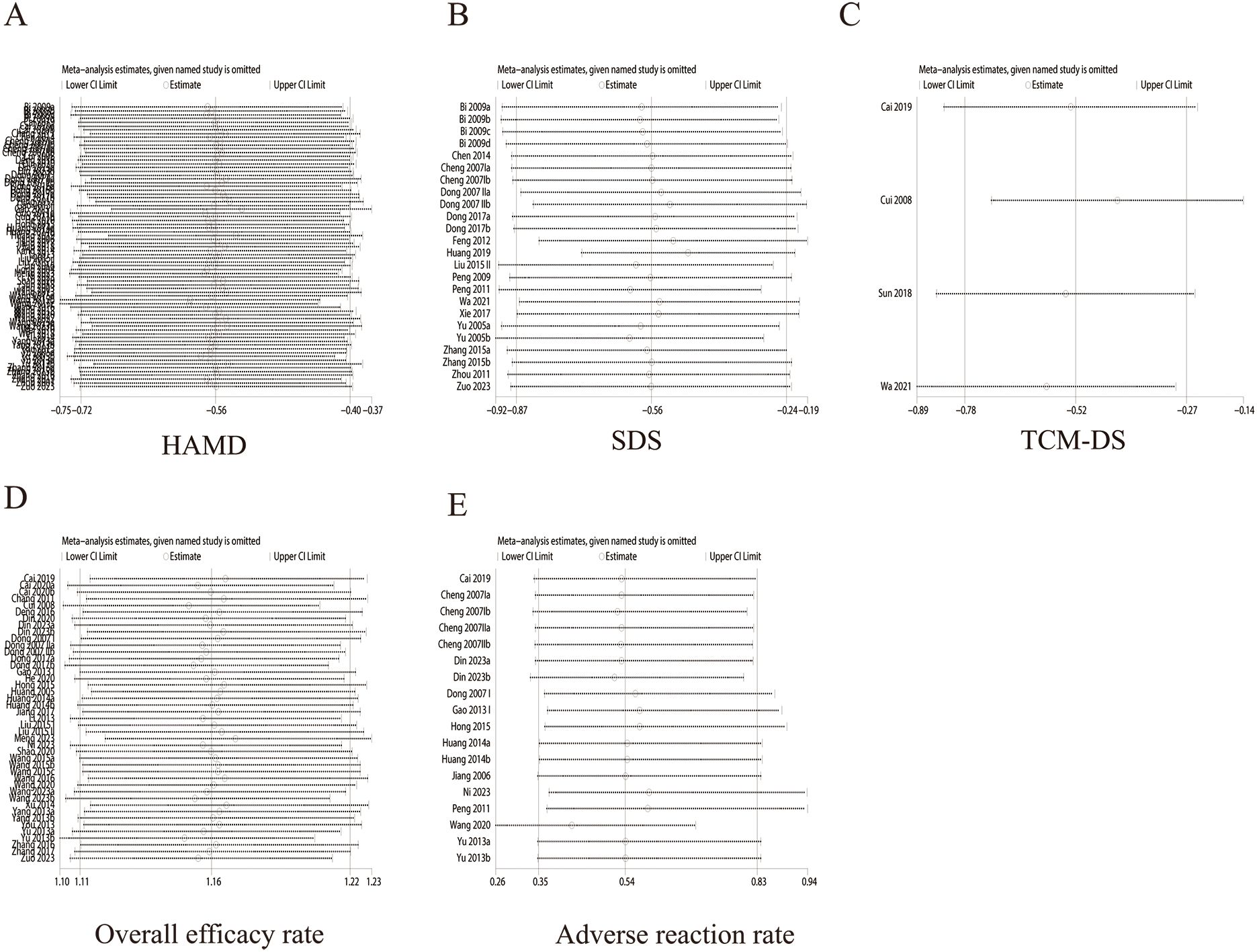
Figure 9. Sensitivity analysis of outcomes. (A) HAMD (B) SDS (C) TCM-DS (D) Overall efficicacy rate (E) Aderverse reaction rate.
4 Discussion
This meta-analysis provides several important findings. The EA intervention group demonstrated significant clinical improvements for patients with PSD, including reductions in HAMD, SDS and TCM-DS scores. Moreover, The EA intervention group showed a significantly lower incidence of adverse events compared to the control group. These results imply that EA may be an effective and safe treatment for alleviating depressive symptoms. Although the overall safety profile of EA was favorable, several trials reported mild and transient adverse effects, such as local redness, subcutaneous bruising, and vasovagal dizziness (17, 21, 22). These events were typically self-limiting and resolved with simple rest or local care. Therefore, ensuring proper aseptic technique, accurate point location, and standardized needle manipulation by trained practitioners is essential to minimize the occurrence of such adverse events (80).
To place our findings in the context of existing evidence, we reviewed two previously published meta-analyses on the efficacy of acupuncture for PSD.The first study (12) reported that no notable difference was identified between acupuncture and antidepressants in terms of improving depressive symptoms; the second study (13). indicated that acupuncture had effects on improving PSD that were comparable to those of antidepressants. Therefore, there is still no consensus regarding the efficacy of acupuncture in improving depressive symptoms. However, there are several notable differences between our study and these earlier analyses. First, the previous studies included 18 RCTs (n = 1,536 patients) and 19 RCTs (n = 1,606 patients), whereas our study incorporated 65 RCTs with a total of 5,362 participants. This substantial difference in sample size and study population could account for the differing results. Second, the earlier studies qualitatively assessed only one outcome (HAMD) and conducted subgroup analyses based solely on intervention duration. In contrast, our study evaluated quantitatively HAMD, SDS and TCM-DS outcomes and employed subgroup analyses based on intervention methods, intervention duration, and patient age, providing a more comprehensive understanding of EA’s efficacy. Third, we conducted sensitivity analyses and Egger’s tests to validate the robustness of our pooled results and assess the quality of evidence, which were not performed in the previous studies. Given these methodological advancements, the results of this analysis provide preliminary evidence supporting the efficacy of EA in the treatment of PSD; however, this evidence is limited by the overall quality of the included studies. High-quality randomized controlled trials are still needed to confirm these findings.
In clinical practice, both the HAMD and SDS scales are crucial tools for assessing the severity of depressive symptoms and the effectiveness of treatment in individuals with depression (81)Therefore, this study conducted subgroup analyses to comprehensively evaluate these two scales, identifying and exploring consistent trends in the changes observed in both the HAMD and SDS scores. Subgroup analysis, with intervention methods as a covariate, indicated the greatest improvements in both scales for the EA combined with antidepressants group, while the standalone EA group demonstrated the least improvement. This finding aligns with certain perspectives in complementary and alternative therapies for treating PSD (82, 83), reinforcing the potential benefits of EA in managing depression. Additionally, subgroup analysis based on intervention duration indicated that in the subgroup with intervention durations of ≤6 weeks, EA intervention group demonstrated consistent and significant improvements in both HAMD and SDS scores. Some clinical studies have found that EA for depression has a rapid onset, with effective symptom improvement occurring within 2 to 4 weeks (84, 85). However, at 8 weeks, although EA remains effective, some studies found no statistically significant differences (86). It is still difficult to determine to determine whether intervention durations of ≤ 6 weeks are indeed a key factor contributing to better outcomes, as there was a large discrepancy in sample sizes between the two subgroups. Therefore, further high-quality RCTs are neededto establish the optimal duration of EA treatment for PSD. Further analysis revealed that the duration of the intervention was a significant contributor to heterogeneity in this study. Finally, subgroup analysis by patient age indicated that the EA intervention group also had a notable therapeutic effect in the ≤ 60 years age group. Age is an important factor influencing the severity of depression and the effectiveness of acupuncture. Younger patients tend to have a lower incidence and severity of depression (87), Furthermore, some studies suggest that electroacupuncture may treat cerebrovascular diseases by affecting brain plasticity, while aging reduces brain plasticity, leading to a diminished therapeutic effect of electroacupuncture (88).
This study found that acupoints commonly used to alleviate PSD are primarily located along the Gallbladder, Bladder, and Du Meridians, and function to regulate Qi and blood, calm the mind, and relieve depression. The most frequently utilized acupoints included Bai hui (GV20, 41 times), Shen ting (DU24, 28 times), Tai chong (LR3, 28 times), Shen men (HT7, 26 times), and Nei guan (PC6, 22 times).
Bai hui (GV20)
GV20 is located on the Governing Vessel and is considered a critical convergence point of all meridians. Modern studies have demonstrated that EA stimulation of GV 20 can alleviate depressive symptoms by acutely activating the somatosensory and visual networks and, during the sustained phase, inhibiting the overactivation of the default mode network, suggesting both immediate and long-term therapeutic effects (89). Another study found that EA targeting GV20, LR3, Yintang (GV24), and Hegu (LI4) may reduce HAMD-17 scores by suppressing pro-inflammatory cytokines, with efficacy comparable to escitalopram oxalate (90).
Shenting (DU24)
DU 24, another acupoint on the Governing Vessel, is traditionally used to regulate emotions and is often combined with Baihui in the treatment of mood disorders. Studies have shown that EA stimulation of GV20 and DU24 alleviates depressive symptoms by modulating the expression of key proteins in the hippocampus, such as CaMKII, CaMKIV, and CaM, thereby reducing stress related to work and daily life (91). Electroacupuncture targeting GV20 and GV24 also alleviates depressive symptoms by activating the mesolimbic dopamine reward circuit, enhancing pain relief and emotional regulation (92).
Taichong (LR 3)
LR3 is located on the Liver meridian. Electroacupuncture at GV20 and LR3 alleviates depression through RNA sequencing technology, which identified changes in gene expression in the medial prefrontal cortex—including genes such as Casr, Bdkrb2, Gnb3, and Ccl1—suggesting that electroacupuncture modulates multiple biological pathways involved in the treatment of depression (93).
Shenmen (HT7)
HT7, located on the Heart meridian, is associated with calming the mind, benefiting the heart, and unblocking meridians. Research has shown that EA stimulation on HT7 alleviates anxiety and negative emotions induced by repeated alcohol administration by reducing plasma corticosterone levels, increasing amygdala expression of mature brain-derived neurotrophic factor and phosphorylated TrkB, and decreasing corticotropin-releasing hormone levels in the paraventricular nucleus, thereby modulating stress-related pathways (94).
Neiguan (PC6)
PC6, located on the Pericardium meridian, is known for its sedative and meridian-unblocking properties. Studies have shown that acupuncture stimulation of PC6 effectively alleviates depressive symptoms induced by chronic mild stress, including anxiety and anhedonia. This intervention restored behavioral indicators, such as open-arm latency in the elevated plus maze (EPM) test and sucrose intake, while significantly reducing the expression of c-fos in the paraventricular nucleus of the hypothalamus (95)
This study has certain limitations. Owing to the inherent characteristics of acupuncture interventions, most included trials lacked clear reporting of blinding and allocation procedures, as reflected in the quality assessment. Nevertheless, these methodological limitations did not substantially affect the overall findings. A large proportion of studies were sourced from Chinese databases, with small sample sizes and single-centre designs, potentially introducing publication and regional selection biases. Although acupuncture demonstrated a favourable safety profile across studies, it is noteworthy that only a small proportion of trials used sham acupuncture as a control, with the majority adopting active pharmacological comparators (Supplementary Table S3). This choice of control may have introduced selection bias and led to an overestimation of acupuncture’s relative safety. Further high-quality, rigorously designed trials are warranted to strengthen the evidence base.
5 Conclusion
Our analysis suggests that EA can alleviate PSD symptoms and enhance clinical efficacy, particularly when used in conjunction with antidepressants. However, the supporting evidence is limited due to the generally low quality of the RCTs considered, which reduces confidence in the observed benefits. EA also showed significant improvements in HAMD, SDS, and TCM-DS scores. Future research should prioritize high-quality, rigorously designed RCTs with robust controls, such as sham acupuncture, and longer follow-up periods to better evaluate long-term effects. Given the current evidence, the possible benefits of acupuncture for PSD should be approached with caution.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Author contributions
XH: Methodology, Data curation, Investigation, Conceptualization, Writing – original draft, Formal Analysis, Writing – review & editing, Resources. YP: Visualization, Validation, Writing – original draft, Supervision, Software. YT: Writing – original draft, Resources, Investigation, Supervision, Formal Analysis. YoZ: Software, Investigation, Validation, Writing – original draft, Supervision. ZL: Writing – original draft, Formal Analysis, Resources, Visualization, Data curation. YuZ: Formal Analysis, Supervision, Software, Writing – original draft, Investigation. HZ: Writing – original draft, Resources, Formal Analysis, Writing – review & editing, Visualization, Supervision, Conceptualization. XY: Methodology, Conceptualization, Writing – review & editing, Funding acquisition, Formal Analysis, Writing – original draft, Project administration.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by supported by National Natural Science Foundation of China(82274666), Provincial Natural Science Foundation of Hunan (2023JJ50375), Scientific Research Fund of Hunan Provincial Education Department (23B0350)
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1610032/full#supplementary-material
References
1. Vestergaard SB, Valentin JB, Dahm CC, Gottrup H, Johnsen SP, Andersen G, et al. Socioeconomic disparities in rate of poststroke dementia: A nationwide cohort study. Stroke. (2025) 56:65–73. doi: 10.1161/strokeaha.124.048380
2. Xiao W, Liu Y, Huang J, Huang LA, Bian Y, and Zou G. Analysis of factors associated with depressive symptoms in stroke patients based on a national cross-sectional study. Sci Rep. (2024) 14:9268. doi: 10.1038/s41598-024-59837-3
3. Eng PC, Tan LLY, Kimball TN, Prapiadou S, and Tan BYQ. Ischemic stroke in women: Understanding sex-specific risk factors, treatment considerations, and outcomes. J Cardiovasc Dev Dis. (2024) 11:382. doi: 10.3390/jcdd11120382
4. Huang H, Lu M, Zhang P, Xiao L, Zhang W, Xu Y, et al. Association between malnutrition, depression, anxiety and fatigue after stroke in older adults: A cross-lagged panel analysis. Aging Clin Exp Res. (2024) 37:4. doi: 10.1007/s40520-024-02892-7
5. Heinz A, Daedelow LS, Wackerhagen C, and Di Chiara G. Addiction theory matters-Why there is no dependence on caffeine or antidepressant medication. Addict Biol. (2020) 25:e12735. doi: 10.1111/adb.12735
6. Lu XY, Lv QY, Li QL, Zhang H, Chen CT, and Tian HM. Impact of acupuncture on ischemia/reperfusion injury: Unraveling the role of mir-34c-5p and autophagy activation. Brain Res Bull. (2024) 215:111031. doi: 10.1016/j.brainresbull.2024.111031
7. Ma F, Cao G, Lu L, Zhu Y, Li W, and Chen L. Electroacupuncture versus escitalopram for mild to moderate post-stroke depression: A randomized non-inferiority trial. Front Psychiatry. (2024) 15:1332107. doi: 10.3389/fpsyt.2024.1332107
8. Chen LY, Yen HR, Sun MF, Lin CL, Chiang JH, and Lee YC. Acupuncture treatment is associated with a decreased risk of developing stroke in patients with depression: A propensity-score matched cohort study. J Affect Disord. (2019) 250:298–306. doi: 10.1016/j.jad.2019.03.020
9. Gao J, Song X, Feng Y, Wu L, Ding Z, Qi S, et al. Electroacupuncture ameliorates depression-like behaviors in rats with post-stroke depression by inhibiting ferroptosis in the prefrontal cortex. Front Neurosci. (2024) 18:1422638. doi: 10.3389/fnins.2024.1422638
10. Yang P, Chen H, Wang T, Su H, Li J, He Y, et al. Electroacupuncture promotes synaptic plasticity in rats with chronic inflammatory pain-related depression by upregulating bdnf/trkb/creb signaling pathway. Brain Behav. (2023) 13:e3310. doi: 10.1002/brb3.3310
11. Han Q and Wang F. Electroacupuncture at gb20 improves cognitive ability and synaptic plasticity via the cam-camkii-creb signaling pathway following cerebral ischemia-reperfusion injury in rats. Acupuncture medicine: J Br Med Acupuncture Soc. (2024) 42:23–31. doi: 10.1177/09645284231202805
12. Li XB, Wang J, Xu AD, Huang JM, Meng LQ, Huang RY, et al. Clinical effects and safety of electroacupuncture for the treatment of post-stroke depression: A systematic review and meta-analysis of randomised controlled trials. Acupuncture medicine: J Br Med Acupuncture Soc. (2018) 36:284–93. doi: 10.1136/acupmed-2016-011300
13. Wang X, Cai W, Wang Y, Huang S, Zhang Q, and Wang F. Is electroacupuncture an effective and safe treatment for poststroke depression? updated systematic Rev meta-analysis BioMed Res Int. (2021) 2021:8661162. doi: 10.1155/2021/8661162
14. Wang H and Li Y. A pilot controlled trial of a combination of electroacupuncture and psychological intervention for post-stroke depression. Complementary therapies Med. (2022) 71:102899. doi: 10.1016/j.ctim.2022.102899
15. Bi CX, Lin SH, and Jiang L. Effects of various therapies on post-stroke depression: A comparative study. China Pract Med. (2010) 5:71–3. doi: 10.14163/j.cnki.11-5547/r.2010.02.174
16. Cai QX. Clinical observation of tong du regulating electroacupunctureand si-hua point moxibustion on post stroke depression with qidepression transforming into fire. Guangzhou, Guangdong, China: Guangzhou University of Chinese Medicine (2020).
17. Cai W. Clinical efficacy of electroacupuncture in post-stroke depression and mechanistic study based on the shh-gli1 signaling pathway. Shanghai, China: Shanghai University of Chinese Medicine (2019).
18. Cai W, Ma W, Li YJ, Wang GT, Yang H, and Shen WD. Efficacy and safety of electroacupuncture for post-stroke depression: A randomized controlled trial. Acupuncture medicine: J Br Med Acupuncture Soc. Beijing, China: Beijing University of Chinese Medicine (2022) 40:434–42. doi: 10.1177/09645284221077104
19. Ceng XL. Clinical observation of the therapeutic effect of electroacupuncture on anxiety and depression disorders after stroke. Beijing, China: Beijing University of Chinese Medicine (2009).
20. Chang XH and Zhang LZ. Clinical observation of acupuncture combined with medicine in treating post-stroke depression. New Chin Med. Guangzhou, Guangdong, China: Guangzhou University of Chinese Medicine (2011) 43:111–2. doi: 10.13457/j.cnki.jncm.2011.02.083
21. Chen C. Effect of scalp electroacupuncture point-through-point for stroke patients with depression on eeg changes before and after treatment. Harbin, Heilongjiang, China: Heilongjiang University of Chinese Medicine (2014).
22. Chen D and Sun YZ. Clinical observation on treating post-stroke depression by electropuncture plus auricular pressure. Clin J Chin Med. Qingdao, Shandong, China: Qingdao University (2016) 8:35–6. doi: 10.3969/cma.j.issn.1674-7860.2016.02.015
23. Chen S. Observation of the therapeutic efficacy of electroacupuncture for post-stroke depression. Chin J Primary Med Pharm. Zhengzhou, Henan, China: Henan University of Chinese Medicine (2012) 19:3094–5. doi: 10.3760/cma.j.issn.1008-6706.2012.20.034
24. Chen Y and Tang QS. Abdominal acupunctur e in treating liver -qi stagnation and spleen deficiency in the elder lywith post-str oke depr ession: A randomized and contr olled obser vation. Chin J Tissue Eng Res. (2007) 39):7791–4.
25. Chen Y and Zhao JJ. Clinical random control study of abdomen acupuncture on treating the post stroke depression. Chin Arch Traditional Chin Med. (2007) 09):1888–91. doi: 10.13193/j.archtcm.2007.09.129.chengy.034
26. Cui MN. Influence of electroacupuncture using dredging governor vessel and regulating mind on depression symptoms and quality of life in patients with post-stroke depression. Guangzhou, Guangdong, China: Guangzhou University of Chinese Medicine (2008).
27. Deng LP and Li HA. Exploration of the mechanism of acupuncture with dredging governor vessel and regulating mind in the treatment of post-stroke depression. Asia-Pacific Traditional Med. (2016) 12:118–9. doi: 10.11954/ytctyy.201609052
28. Din HQ, Dong HD, and Yang JJ. Clinical study of scalp point- through- point electroacupuncture and body acupuncture combined with fluoxetine for post-stroke depression. New Chin Med. (2020) 52:143–6. doi: 10.13457/j.cnki.jncm.2020.03.042
29. Ding XJ, Li H, Qu JL, and Yang LF. Research of siqi decoction combined with electroacupuncture baihui and shenting in treatment of depression after ischemic stroke. Traditional Chin Medicinal Res. (2023) 36:52–5.
30. Dong FC. Observation of the effect of electroacupuncture combined with paroxetine in the treatment of post-stroke depression. China Med Herald. 31:112.
31. Dong JP, Sun WY, Wang S, Wu ZQ, and Liu F. clinical observation on head point-through-point electroacupuncture for treatment of poststroke depression. Zhongguo zhen jiu = Chin acupuncture moxibustion. (2007) 27:241–4. doi: 10.21037/j.acu.2023.07.004
32. Dong JP, Wang DD, and Tan JH. Clinical study of scalp electroacupuncture with through-point needling in the treatment of post-stroke depression. Heilongjiang J Traditional Chin Med. (2017) 46:42–4.
33. Dong ZH, Liu YL, Zhang YT, and Bai YF. The effect of electroacupuncture combined with escitalopram on depression and neurological function in patients with post-stroke depression. China Health Care Nutr. (2016) 26:92.
34. Feng WX, Yan YM, and Liao XY. Clinical observation on combo therapy of electroacupuncture and xingnao jieyu capsule for 45 cases of post-stroke depression. J Traditional Chin Med. (2012) 53:1750–2. doi: 10.13288/j.11-2166/r.2012.20.013
35. Gao S. Clinical study of scalp electroacupuncture with through-point needling in the treatment of post-stroke depression. Harbin, Heilongjiang, China: Heilongjiang University of Chinese Medicine (2013).
36. Gao YY. Effects of electroacupuncture on serum levels of rbp-4 and hp in patients with post-stroke depression. Qingdao, Shandong, China: Qingdao University (2013).
37. Guo AS, Li AH, Chen X, Cai JY, and Wu QF. Effects of electric-acupuncture and fluoxetine on depression andneurological function of post-stroke depression patients. Shandong Med J. (2011) 51:9–11.
38. He L and Ouyang JB. Psychological effects of scalp electroacupuncture combined with transcranial magnetic stimulation on patients with intracerebral hemorrhage. Hunan J Traditional Chin Med. (2021) 37:75–7. doi: 10.16808/j.cnki.issn1003-7705.2021.03.026
39. Hong MZ, Wang ZL, Zhang SQ, and Ma RJ. Observation on effect of “xingshen jieyu” acupuncture method in treating post stroke depression. J Zhejiang Chin Med Univ. (2015) 39:621–4. doi: 10.16466/j.issn1005-5509.2015.08.013
40. Huang Y, Chen J, and Zou J. Effect of sclap electro-acupuncture on post-stroke depression. Chin J Tissue Eng Res. (2005) 40):172–3.
41. Huang SL, Wei Y, and Zhang Z. Combination of electroacupuncture on shen-wu-xing points”and western medicine for poststroke depression: A randomized controlled trial. Shanghai J Traditional Chin Med. (2014) 48:33–6. doi: 10.16305/j.1007-1334.2014.07.034
42. Huang YS. Exploratory study on the application of traditional chinese medicine scalp electroacupuncture in reducing the incidence of post-stroke depression (psd). Health Guide. (2019) 30):313.
43. Jiang H, Wen XY, Shi TH, and Ming ZS. The therapeutic effects of electroacupuncture on post-stroke depression after lacunar infarct. Chin J Phys Med Rehabil. (2006) 12):807–10.
44. Jiang ZY, Gao L, Li CD, and Cun LJ. Clinical study on the treatment of post-stroke depression with electroacupuncture of “niwan bazhen” points. World J Acupuncture-Moxibustion. (2007) 01):11–6.
45. Jiao YG and Xing YL. Effect of auricular electroacupuncture on depression after stroke in patients with type 2 diabetes mellitus. J New Med. (2018) 49:889–93.
46. Kang WG and Yang BG. Electro-acupuncture therapy for the post-stroke depression. J Clin Acupuncture Moxibustion. (2014) 30:35–7.
47. Li XY, Shi GC, and Dong QJ. Electroacupuncture at head san shen and si guan points for the treatment of 70 post-stroke depression patients. Heilongjiang J Traditional Chin Med. (2013) 42:31–2.
48. Liu G, Zhao S, Shi W, Su H, and Sheng G. Effect of acupuncture combined with medication on depressive state in patients with post-stroke motor aphasia. Shanghai J Acupuncture Moxibustion. (2021) 40:298–302. doi: 10.13460/j.issn.1005-0957.2021.03.0298
49. Liu YF, Meng Y, Jia LY, and Chang XH. Clinical research of electroacupuncture and traditional chinese medicine in the treatment of post stroke depression. Acta Chin Med. (2015) 30:146–8. doi: 10.16368/j.issn.1674-8999.2015.01.049
50. Liu YF. Observation of the curative effect on the treatment of psd by a comprehensive scheme of combined acupuncture with medicine. Zhengzhou, Henan, China: Henan University of Chinese Medicine (2015).
51. Liu YH. Acusector combined with deanxit in the treatment of post-stroke depression for 43 cases. Chin Med Modern Distance Educ China. (2016) 14:107–8. doi: 10.3969/j.issn.1672-2779.2016.04.051
52. Long HW, Tan PZ, Feng JH, and Li MZ. Clinical observation of electroacupuncture in the treatment of post-stroke depression. J Clin Psychiatry. (2004) 14:173–4. doi: 10.3969/j.issn.1005-3220.2004.03.040
53. Meng FP, Lu JJ, Zhou YX, Wu XB, and Jin GH. A clinical randomized controlled trial studyof electroacupuncture combined with repetitive transcranial magnetic stimulation in the treatment of moderate-to-severe post-stroke depression in elderly patients. Geriatrics Health Care. (2023) 29:696–699 + 715.
54. Ni SM, Jiang XZ, and Peng YJ. tiaoshen jieyu acupuncture combined with sertraline hydrochloride tab let for post-stoke depression: A randomized controlled trial. Zhongguo zhen jiu = Chin acupuncture moxibustion. (2023) 43:19–22. doi: 10.13703/j.0255-2930.20220520-0006
55. Peng HY, Tan JL, Wang BG, and Zhai MH. Clinical study on the treatment of post-stroke depression with electroacupuncture at temporal three-needle as the primary method. New Chin Med. (2009) 41:89–90 + 8. doi: 10.13457/j.cnki.jncm.2009.10.042
56. Peng HY, Ye JS, He XJ, Tan JL, and Zhang ZQ. Clinical randomized controlled study of electroacupuncture and fluoxetine capsules in the treatment of post-stroke depression. Jilin J Chin Med. (2011) 31:990–2. doi: 10.13463/j.cnki.jlzyy.2011.10.007
57. Shao HW. Clinical effect of electro-acupuncture at auricular points in treating type 2 diabetes mellitus complicated with post-stroke depression. J Guangzhou Univ Traditional Chin Med. (2020) 37:457–64. doi: 10.13359/j.cnki.gzxbtcm.2020.03.015
58. Sun YH, Zhou JH, and Zhuang LX. Study of professor zhuang’s mind regulation acupuncture against post-stoke depression. J Liaoning Univ Traditional Chin Med. (2019) 21:71–4. doi: 10.13194/j.issn.1673-842x.2019.03.020
59. Tang JX, Guan LH, Li L, and Liu JF. Influence of electroacupuncture on life quality in patients with post-apoplectic depression. Shanghai J Acupuncture Moxibustion. (2003) 03):12–4. doi: 10.13460/j.issn.1005-0957.2003.03.004
60. Wang F, Pan W, and Li YF. Therapeutic observation of acupuncture plus auricular point electroacupuncture for post-stroke depression and its effect on the quality of life. Shanghai J Acupuncture Moxibustion. (2016) 35:1033–5. doi: 10.13460/j.issn.1005-0957.2016.09.1033
61. Wang N, Lin XW, Zhang XL, Feng QF, Zhang GC, and Zhao J. Study on clinical efficacy of jieyu decoction combined with electro-acupuncture at baihui(du20) and sishencong(ex - hn1) on depression and anxiety after cerebral infarction and its influence on neurological function. Chin Arch Traditional Chin Med. (2020) 38:40–3. doi: 10.13193/j.issn.1673-7717.2020.07.011
62. Wang XX, Zhao YD, and Wang ML. The clinical effect of electro-nape acupuncture combined xiaoyao powder on the treatment of post-stroke depression and part of the mechanism discussion. J Clin Exp Med. (2018) 17:155–9. doi: 10.3969/j.issn.1671-4695.2018.02.014
63. Wang XY and Gao M. To observe the curative effect of electroacupuncture on governor vessel combined with venlafaxine in the treatment of post-stroke depression. Traditional Chin Med Rehabil. (2013) 4:86–8.
64. Wei AH, Wang XM, and Li LY. The effect of paxil combined with psychological intervention and electroacupuncture on depression and cognitive function in stroke patients. Chin J Phys Med Rehabil. (2011) 33:287–9. doi: 10.3760/cma.j.issn.0254-1424.2011.04.013
65. Wen AB, Deng JH, and Qin YB. Clinical observation on treatment of post-stroke dysphagia combined with anxiety and depression with new triple therapy. J Guangxi Univ Chin Med. (2018) 21:25–8.
66. Xie C, Jiang DX, Wang N, and Ma DL. Clinical study on electroacupuncture for limb dysfunction and anxiety-depression in patients with cerebral hemorrhage. psychol Doctor. (2017) 23:134–5.
67. Xu G and Miao G. Observation of the therapeutic efficacy of electroacupuncture for post-stroke depression in the elderly. Chin J Convalescent Med. (2015) 24:384–6. doi: 10.13517/j.cnki.ccm.2015.04.021
68. Yang SQ and Wang WH. Observations on the efficacy of scalp acupuncture plus medication for post-stroke depression. Shanghai J Acupuncture Moxibustion. (2013) 32:9–11.
69. You Y. Curative effect observation on back shu point electroacupuncture and small dose of paxil treat post-stroke depression. Chin J Convalescent Med. (2013) 22:974–6. doi: 10.13517/j.cnki.ccm.2013.11.014
70. Yu F. Clinical observation of electroacupuncture at the cervical jiaji points for the treatment of post-stroke depression. Heilongjiang Provincial Acad Traditional Chin Med. (2005).
71. Yu JN. The clinicalstudyof post-stroke depression of heartand spleen deficiency treated withmusicelectro-acupuncture. Heilongjiang Univ Chin Med. (2013).
72. Zhang R and Yan P. Effect of electroacupuncture at acupoints jieyu formula on patients with post-stroke depression. J Shanxi Coll Traditional Chin Med. (2017) 18:39–41.
73. Zhang J, Wang W, Wu H.H., Liu SJ, and Wang YM. Clinical observation of 60 cases of cerebral apoplexy treated with electro acupuncture combined with jieyutongluotang. World Latest Med Inf. (2015) 15:52–53 + 59.
74. Zhang SL, Lou YM, and Huang YH. Observation of the effect of escitalopram combined with electroacupuncture in the treatment of post-stroke depression. Med Equip. (2016) 29:77–8.
75. Zhou HY and Zhao SM. Observation on the rehabilitation effect of acupuncture combined with music electrical therapy in patients with acute stroke. Int J Nurs. (2011) 30:1575–8. doi: 10.3760/cma.j.issn.1673-4351.2011.10.071
76. Zhou ZM. The comparative study of electroacupuncture treatment and pharmacological treatment for post-stroke depression. China Med Herald. (2007) 16):23 + 128.
77. Zuo YC, Lou BD, Liu K, and Gao YY. Effect of electro-needling acupoints of pericardium meridian on blood acth and cort in treatment of post-stroke depression. J Clin Acupuncture Moxibustion. (2023) 39:53–7. doi: 10.19917/j.cnki.1005-0779.023073
78. Wang ZX. Observations on the clinical efficacyof electroacupuncture with differentwaveforms in the treatment of post-strokedepression. Heilongjiang Univ Chin Med. (2023).
79. World Health Organization. A standard international acupuncture nomenclature: Memorandum from a who meeting. Bull World Health Organ. (1990) 68:165–9.
80. Leung PC, Zhang L, and Cheng KF. Acupuncture: Complications are preventab le not adverse events. Chin J Integr Med. (2009) 15:229–32. doi: 10.1007/s11655-009-0229-2
81. Xiao K, Li X, Hu W, and Li X. Acupuncture combined with repetitive transcranial magnetic stimulation for the treatment of post-stroke depression: A systematic evaluation and meta-analysis based on a randomised controlled trial. Front Neurol. (2024) 15:1360437. doi: 10.3389/fneur.2024.1360437
82. Yi Y, Zhao W, Lv S, Zhang G, Rong Y, Wang X, et al. Effectiveness of non-pharmacological therapies for treating post-stroke depression: A systematic review and network meta-analysis. Gen Hosp Psychiatry. (2024) 90:99–107. doi: 10.1016/j.genhosppsych.2024.07.011
83. Wang X, Xiong J, Yang J, Yuan T, Jiang Y, Zhou X, et al. Meta-analysis of the clinical effectiveness of combined acupuncture and western medicine to treat post-stroke depression. J traditional Chin Med = Chung i tsa chih ying wen pan. (2021) 41:6–16. doi: 10.19852/j.cnki.jtcm.2021.01.002
84. Qu SS, Huang Y, Zhang ZJ, Chen JQ, Lin RY, Wang CQ, et al. A 6-week randomized controlled trial with 4-week follow-up of acupuncture combined with paroxetine in patients with major depressive disorder. J Psychiatr Res. (2013) 47:726–32. doi: 10.1016/j.jpsychires.2013.02.004
85. Song Y, Zhou D, Fan J, Luo H, and Halbreich U. Effects of electroacupuncture and fluoxetine on the density of gtp-binding-proteins in platelet membrane in patients with major depressive disorder. J Affect Disord. (2007) 98:253–7. doi: 10.1016/j.jad.2006.07.012
86. Yang X, Gong W, Ma X, Wang S, Wang X, Guo T, et al. Factor analysis of electroacupuncture and selective serotonin reuptake inhibitors for major depressive disorder: An 8-week controlled clinical trial. Acupuncture medicine: J Br Med Acupuncture Soc. (2020) 38:45–52. doi: 10.1136/acupmed-2017-011412
87. Ignacio KHD, Muir RT, Diestro JDB, Singh N, Yu M, Omari OE, et al. Prevalence of depression and anxiety symptoms after stroke in young adults: A systematic review and meta-analysis. J stroke cerebrovascular diseases: Off J Natl Stroke Assoc. (2024) 33:107732. doi: 10.1016/j.jstrokecerebrovasdis.2024.107732
88. Huo BB, Zheng MX, Hua XY, Wu JJ, Xing XX, Ma J, et al. Effect of aging on the cerebral metabolic mechanism of electroacupuncture treatment in rats with traumatic brain injury. Front Neurosci. (2023) 17:1081515. doi: 10.3389/fnins.2023.1081515
89. Wei XY, Chen H, Guo C, Tan WL, and Zhan SH. The instant and sustained effect of electroacupuncture in postgraduate students with depression: an fMRI study. Neuropsychiatr Dis Treat. (2021) 17:873–83. doi: 10.2147/NDT.S307083
90. Ma FX, Gao GP, Lu L, Zhu YL, Li WL, and Li C. Electroacupuncture versus Escitalopram for mild to moderate Post-Stroke Depression: A randomized non-inferiority trial. Front Psychiatry. (2024) 15:1332107. doi: 10.3389/fpsyt.2024.1332107
91. Bai L, Zhang D, Cui TT, Li JF, Gao YY, Jia PL, et al. Mechanisms underlying the antidepressant effect of acupuncture via the caMK signaling pathway. Front Behav Neurosci. (2020) 14:563698. doi: 10.3389/fnbeh.2020.563698
92. Yang YN, Wei X.L., Tian J, Zhu Y, Jia SH, and Shu Q. Scalp electroacupuncture targeting the VTADA neurons to relieve negative emotions and promote the alleviation of chronic pain. Front Neurosci. (2023) 17:1323727. doi: 10.3389/fnins.2023.1323727
93. Zhang YJ, Zhang HY, Zheng XJ, Hou Y, Chang X.L., Zhang LL, et al. Identification of differentially expressed genes in the medial prefrontal cortex of rats subjected to chronic unpredicta ble mild stress and treated with electroacupuncture. Genomics. (2024) 116:110901. doi: 10.1016/j.ygeno.2024.110901
94. Seo SY, Bang SK, Kang SY, Cho SJ, Choi KH, and Ryu YH. Acupuncture alleviates anxiety and 22-kHz ultrasonic vocalizations in rats subjected to repeated alcohol administration by modulating the brain-derived neurotrophic factor/corticotropin-releasing hormone signaling pathway. Int J Mol Sci. (2021) 22:4037. doi: 10.3390/ijms22084037
Keywords: post stroke depression, electroacupuncture, meta-analysis, randomized controlled trial, acupoint application
Citation: Hu X, Pan Y, Tang Y, Zhang Y, Liu Z, Zhuo Y, Zhang H and Yi X (2025) Efficacy and safety of electroacupuncture-based comprehensive treatment for post-stroke depression: a systematic review and meta-analysis of randomized controlled trials. Front. Psychiatry 16:1610032. doi: 10.3389/fpsyt.2025.1610032
Received: 11 April 2025; Accepted: 23 July 2025;
Published: 15 August 2025.
Edited by:
Francesco Panza, University of Bari Aldo Moro, ItalyReviewed by:
Christian Bohringer, UC Davis Medical Center, United StatesJunying Wang, China Academy of Chinese Medical Sciences, China
Yin Huang, Sichuan University, China
Copyright © 2025 Hu, Pan, Tang, Zhang, Liu, Zhuo, Zhang and Yi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiqin Yi, OTk1MDEwNTY4QHFxLmNvbQ==; Hong Zhang, emg1MzgxMjcxQHNpbmEuY29t