 Juan P. Sanabria-Mazo1,2
Juan P. Sanabria-Mazo1,2 Adrián Pérez-Aranda2,3*
Adrián Pérez-Aranda2,3* Carilene Armas-Landaeta4
Carilene Armas-Landaeta4 Estíbaliz Royuela-Colomer2,3Corel Mateo-Canedo5Itxaso Cabrera-Gil6
Estíbaliz Royuela-Colomer2,3Corel Mateo-Canedo5Itxaso Cabrera-Gil6 Alicia Monreal-Bartolomé6,7,8
Alicia Monreal-Bartolomé6,7,8 Javier García-Campayo4,7,8
Javier García-Campayo4,7,8 Yolanda López-del-Hoyo6,7,8
Yolanda López-del-Hoyo6,7,8- 1Teaching, Research, and Innovation Unit, Parc Sanitari Sant Joan de Déu, Sant Boi de Llobregat, Spain
- 2Center for Biomedical Research in Epidemiology and Public Health (CIBERESP), Madrid, Spain
- 3Department of Clinical and Health Psychology, Autonomous University of Barcelona, Cerdanyola del Vallès, Spain
- 4Faculty of Medicine, University of Zaragoza, Zaragoza, Spain
- 5Department of Basic, Developmental, and Educational Psychology, Autonomous University of Barcelona, Cerdanyola del Vallès, Spain
- 6Department of Psychology and Sociology, University of Zaragoza, Zaragoza, Spain
- 7Institute of Health Research of Aragon (IIS Aragón), Miguel Servet University Hospital, Zaragoza, Spain
- 8Research Network on Chronicity, Primary Care and Health Promotion (RICAPPS), Zaragoza, Spain
Background: Many adolescents face significant mental health challenges, including anxiety, depression, and substance-related and addictive disorders, with a growing need for school-based preventive strategies. Traditional classroom interventions often struggle to engage adolescents, prompting the exploration of game-based approaches to improve mental health knowledge and foster healthier attitudes.
Objective: This systematic review evaluates the effectiveness of game-based interventions implemented in classroom settings to enhance mental health knowledge and promote positive attitudes among adolescents.
Methods: A comprehensive search was conducted across Medline, PsycINFO, Web of Science, and SCOPUS, yielding 1,152 articles. After screening, 17 studies were included, most using cluster randomized controlled trial designs. These interventions addressed topics of mental health such as substance-related and addictive disorders, anxiety, and depression, employing playful activities like video games, virtual reality simulations, quizzes, and collaborative tasks.
Results: The interventions showed positive effects on knowledge acquisition and attitude change, with high satisfaction reported by participants. Those programs targeting alcohol and tobacco use were particularly effective in improving knowledge and attitudes. However, the quality of evidence varied, and long-term effects were not widely assessed due to a lack of follow-up in most studies. Some interventions had a limited impact on self-efficacy and behavior change.
Conclusions: Game-based classroom interventions show promise in promoting mental health literacy and healthier attitudes among adolescents. While short-term outcomes are encouraging, more rigorous studies with extended follow-up periods are necessary to understand their long-term effectiveness. Future interventions should focus on practical skill development and personalization to maximize impact.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/, identifier CRD42024531914.
1 Introduction
Adolescence, a critical phase in human development, is marked by significant biological and social changes that have lasting effects on long-term well-being (1). Mental health in adolescents is an area of growing concern: a recent report by the United Nations (2) indicated that 1 in 7 children and teens are impacted by mental health conditions. The neurodevelopmental transformations during this period, combined with the unique challenges of adolescence—such as evolving relationships with parents, exploration of social and sexual roles, identity formation, and planning for the future—heighten the risk of psychological distress. In some cases, this distress can manifest in mental health conditions such as anxiety, depression, and substance-related and addictive disorders (3). Recent evidence suggests that the COVID-19 pandemic has exacerbated mental health issues within this demographic (4–6), with substance-related and addictive disorders emerging as particularly concerning due to their association with long-term negative consequences, including a higher risk of mood disorders, academic difficulties, and social impairments (7).
This life stage constitutes a period of vulnerability to mental health issues, which represents a propitious time for prevention and intervention (8). Universal preventive strategies delivered in schools, designed to reach all adolescents irrespective of their individual risk factors or symptomatology, present a hopeful avenue for fostering mental well-being (9). By targeting a diverse range of adolescents, regardless of their initial susceptibility, these universal interventions hold the potential to mitigate the onset of problematic behaviors while concurrently enhancing overall mental health outcomes by increasing knowledge and modifying attitudes. Such school-based strategies can effectively reach a broader spectrum of adolescents, potentially reducing barriers associated with seeking professional help and minimizing stigma surrounding mental health treatment (10).
Traditionally, interventions delivered in the classroom involved educational programs designed to provide knowledge about mental health disorders, reduce stigma, and prevent risky behaviors related to addictive substances. However, while some classroom-delivered interventions have shown a certain degree of effectiveness (11), these programs are not exempt from challenges. A primary hurdle lies in the capacity of traditional educational models to truly engage and positively impact the target audience. Adolescents often perceive conventional teaching methods as outdated or disconnected from their daily experiences, which can diminish the impact of these interventions (12, 13).
To overcome the limitations of traditional approaches, it is crucial to adopt innovative strategies that bridge the gap between educational content and the lived experiences of adolescents. One promising method involves incorporating interactive elements, such as games, that directly address adolescents’ concerns and interests. Some game-based interventions are characterized by the incorporation of game elements but cannot fully qualify as stand-alone games (14). In contrast, other interventions, including serious games, educational games, and game-based learning strategies, are explicitly designed to educate players, enhance their skills, or enrich their knowledge (15).
By integrating dynamics such as points, levels, and rewards, gamification transforms educational content into a format that feels less like traditional learning and more like an engaging activity (15, 16). This game-based approach not only boosts participation and sustained interest but also allows for personalized learning experiences tailored to individual preferences and learning styles. Although previous systematic reviews have identified positive effects of gamified interventions in specific populations, such as adolescents with obesity (17), adolescents with attention-deficit hyperactivity disorder (18), or individuals from the general population (19), the specific impact of game-based interventions on promoting mental health knowledge and fostering healthy attitudes in adolescents has not been systematically explored.
Given the gaps in current research, an updated systematic review is needed to examine the available evidence on this topic. To date, the existing literature has not determined the extent to which game-based interventions can improve adolescents’ knowledge of mental health problems or encourage positive attitudes toward mental health. The objective of this study was to conduct a comprehensive systematic review examining various forms of game-based interventions implemented within classroom settings. These interventions are hypothesized to be effective and engaging tools for promoting mental health awareness. The reviewed interventions were required to include playful activities and be designed to enhance mental health knowledge dissemination and behavior change across diverse mental health conditions in adolescent populations. By scrutinizing the gamified approaches utilized and their corresponding outcomes, this study aims to provide valuable insights into the potential of playful interventions as effective tools for fostering mental health awareness and encouraging positive behavioral changes in adolescents.
2 Method
2.1 Study design
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines (20). The review protocol was registered in the Prospective Register of Systematic Review (PROSPERO) with the identification code CRD42024531914.
2.2 Data sources and search strategy
A search strategy using Medline, PsycINFO, Web of Science, and SCOPUS was conducted. This search strategy combined terms related to population (adolescent OR teenager OR youth OR juvenile OR young OR minor), games (game OR gaming OR gamified OR gamification), interventions (intervention OR program OR treatment OR therapy OR trial), and classrooms (classroom OR school OR education institution). All searches were performed based on titles, abstracts, and keywords. The bibliographic database searches are detailed in Supplementary Table 1.
The search terms were selected considering the search strategies in previous systematic reviews on game-based interventions (21–23). The following limits and filters were activated in all databases, if possible: (1) publication date (from inception until 2024), (2) document type (only articles), and (3) languages (English and Spanish). In addition, gray literature—such as dissertations, conference abstracts, or reports—was excluded to ensure methodological consistency across included studies. The reference list of included studies was examined through a reverse citation search.
2.3 Eligibility criteria
The eligibility criteria were selected using the “Population”, “Intervention”, “Comparison”, “Outcomes”, and “Study” (PICOS) approach (24):
● [P] Population: Adolescents aged between 11 and 18 years. Studies that did not specify age or did not indicate the age range of the sample were excluded. No additional exclusion criteria were established for the population.
● [I] Intervention: Those delivered in the classroom that incorporate playful activities to promote mental health knowledge and behavior change directed at diverse mental health conditions. Interventions could be fully or partially gamified, cooperative or competitive, and conducted face-to-face or using a digital device (if performed in the classroom). Blended interventions (i.e., a combination of face-to-face and digital device sessions) were also included. Interventions that did not include playful elements or were not conducted in the classroom were excluded.
● [C] Comparison: To explore all available evidence in the literature, single-, two-, or multi-arm interventions were included. No inclusion or exclusion criteria were established for controls.
● [O] Outcomes: Mental health-related outcomes were explored in this systematic review, such as mental health problems, knowledge about mental health problems, attitudes towards mental health problems, frequency of risk behaviors, or symptomatology, among others. Participants’ satisfaction with the interventions was also explored. Studies with outcomes not directly related to mental health were excluded.
● [S] Study design: Randomized controlled trials (RCTs), non-RCTs, and open trials of any length of follow-up were included. Pilot studies were also included if they followed one of the previous study designs. No trials were excluded based on publication status.
2.4 Study selection
Duplicate articles in the databases were automatically removed by Mendeley. Then, 2 authors (CAL and APA) independently screened all articles in Rayyan QCRI. Abstracts and titles were screened to identify those relevant to the research question. When insufficient information was available to determine eligibility, full articles were reviewed. The selected articles were examined for their reference lists to identify additional relevant studies that might not have appeared in the initial database search. Initial disagreements among the authors were resolved by consensus. No additional reviewer was needed to resolve the initial disagreement.
2.5 Quality appraisal
The quality appraisal (QA) of the studies was evaluated independently by 3 authors (CAL, APA, and JPSM) using the National Heart, Lung, and Blood Institute (NHLBI) tools for quality assessment (25). Considering the characteristics of the studies included in this systematic review, two tools were used: one for controlled intervention studies, and another for single-arm studies.
The total score range was 0–14 for the “Quality Assessment of Controlled Intervention Studies” tool: good QA (11-14), fair QA (6-10), and low QA (≤ 5); and 0–12 for the “Quality Assessment Tool for Before-After Studies with No Control Group” tool: good QA (9-12), fair QA (5-8), and low QA (≤ 4). The answer options were scored with 1 when the criterion was met and with a 0 when the criterion was not met, could not be determined, was not applicable, or was not reported. Discordances in quality rating were resolved through discussion between the authors.
2.6 Data extraction and synthesis
A data extraction form was developed based on the Centre for Reviews and Dissemination templates. Data collected included information on authors, publication date, country of study, study design, sample size, setting, outcomes, and results. In addition, the name, reference(s), objective, format, and games of the interventions included in this systematic review were extracted. A narrative synthesis was carried out to describe the main characteristics of game-based interventions, the quality of evidence, and the relationship of the findings within and between the included studies. A summary of each study and its main features was provided in the tables.
3 Results
3.1 Selection and inclusion of studies
As shown in Figure 1, the initial database search yielded a total of 1,152 published articles. In addition, 4 articles were included from other resources (i.e., reverse citation search). After removing duplicates, 1,130 titles and abstracts were reviewed, of which 41 were chosen for full-text review. Finally, 17 articles were included in this systematic review.
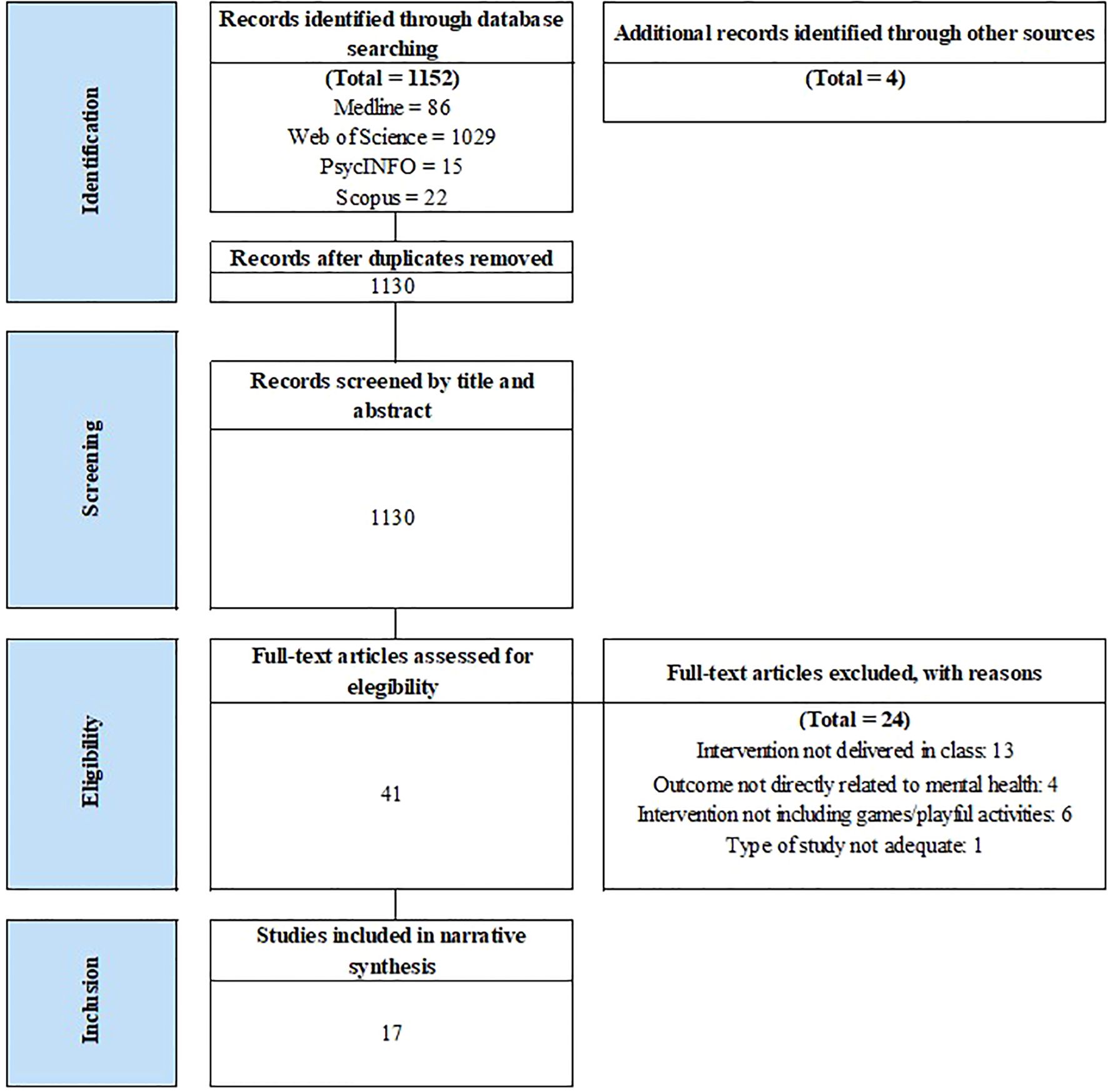
Figure 1. PRISMA flowchart from record identification to study inclusion. Source: PRISMA, https://www.prisma-statement.org/prisma-2020-flow-diagram, reproduced under CC BY 4.0 license.
3.2 Summary of the findings
Among the 17 studies, the cluster randomized controlled trial design was the most common (n = 12), where the whole classrooms were randomly assigned either to the intervention or control condition. Only six studies included a follow-up assessment. The sample sizes ranged from 40 to more than 14,000 adolescents, and participants’ ages ranged from 11 to 18. Gender distribution was balanced in most cases, although one study was conducted on a female-only education center. Regarding the outcomes, most studies (n = 12) included some measure of knowledge acquisition (regarding the aspects that the intervention targeted), attitudes, and intentions, among others. In addition, eight studies reported users’ opinions and/or satisfaction with the intervention. These outcomes were predominantly measured using ad hoc questionnaires—some previously employed in other studies, others specifically developed for the current research—while only 7 studies used some validated instruments. The description of each study can be found in Table 1.
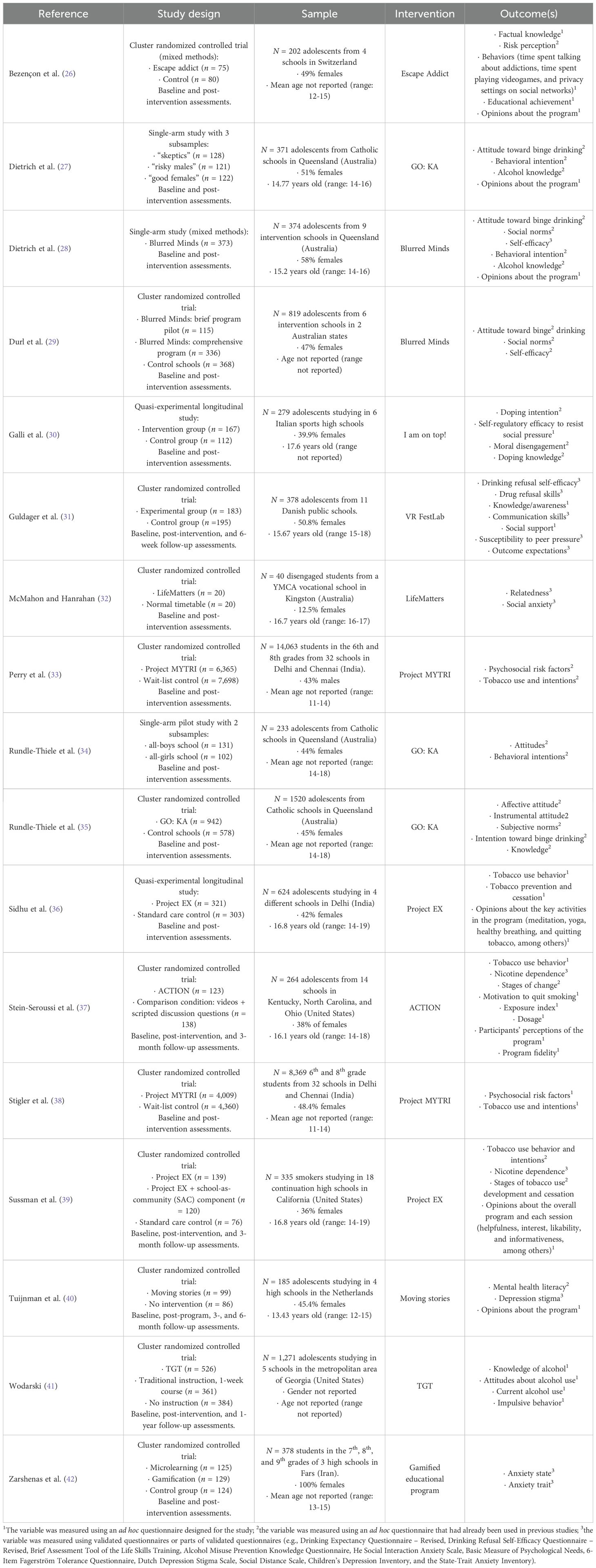
Table 1. Description of the 17 studies reviewed.
The studies reviewed tested the effects of 12 interventions that included some kind of game in the classroom to increase knowledge and/or promote healthy attitudes related to mental health: four interventions aimed at promoting responsible drinking; three focused on preventing/reducing tobacco use among adolescents; two programs targeted different types of substance-related and addictive disorders (doping, tobacco, alcohol, cannabis, and screen use); two focused on reducing anxiety; and one was addressed at increasing knowledge about depression and reducing its associated stigma. While some interventions were delivered in a single session (n = 3), most of them (n = 8) included at least four that took place once per week during consecutive weeks. The playful activities delivered in the classroom were diverse: videogames in which the students had to make decisions regarding the behavior of the main character and see the consequences (n = 2), virtual reality games that simulated social situations and bodily sensations (n = 2), interactive games and competitive quizzes to increase knowledge (n = 6), and a collaborative digital escape room to learn about different types of risky behaviors (n = 1). A description of the interventions, detailing the playful activity that each one included, can be found in Table 2.
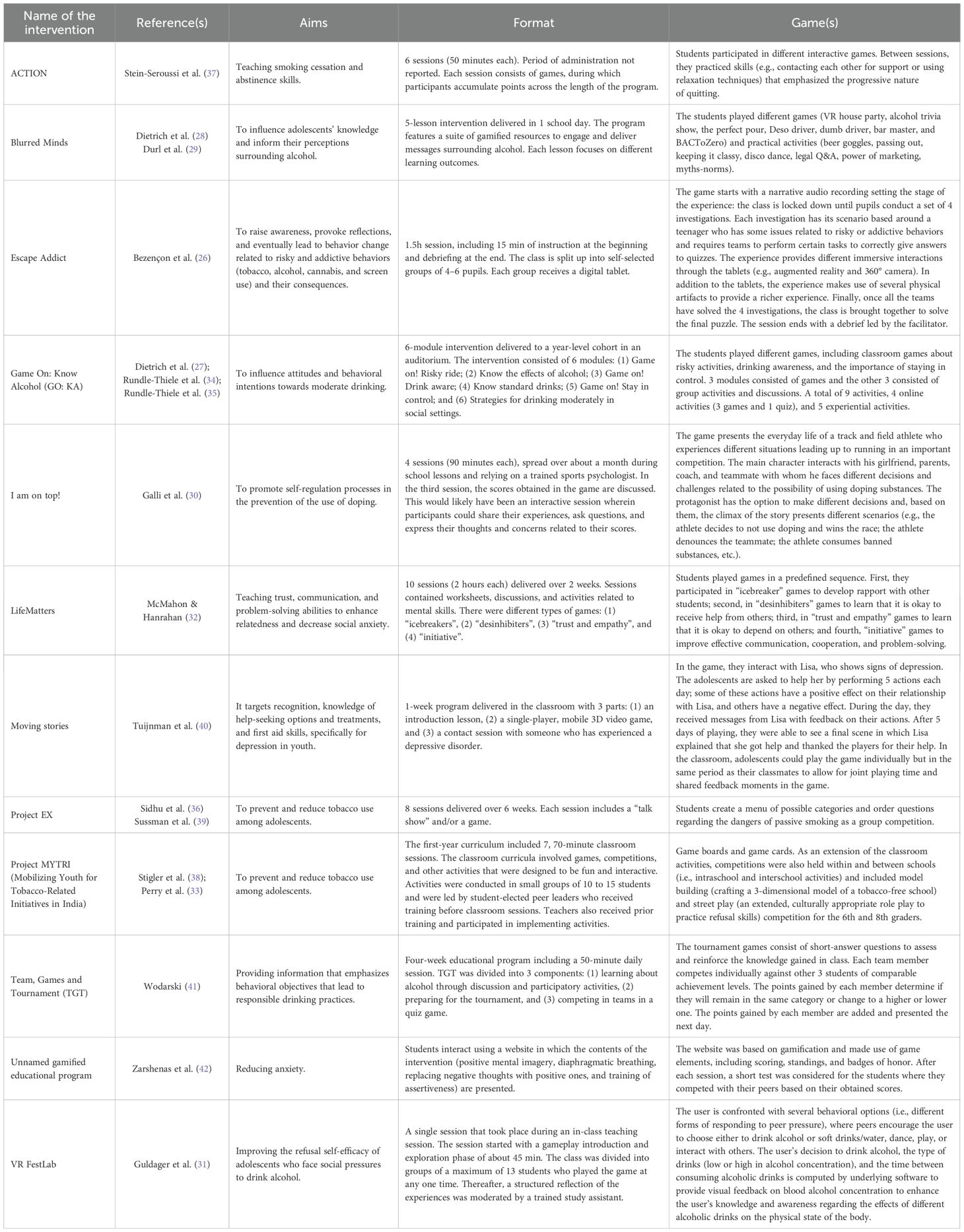
Table 2. Interventions included in the systematic review.
3.3 Study quality
The overall quality of the studies included was rated as fair. No studies were rated as good, while 4 presented low quality. The risk of bias was mainly due to a lack of blinding in controlled studies, while single-arm studies did not report information on the sample’s representativeness and sample size calculation. The quality assessment of the included studies is detailed in Supplementary Table 2.
3.4 Effects of the interventions on mental health promotion
3.4.1 Drinking behaviours
Four interventions were specifically designed to target risky drinking behaviors: Blurred Minds (28, 29), Game on: Know Alcohol (GO: KA; 27, 34, 35), Team-Games-Tournaments (TGT; 41), and VR FestLab (31). Another one, Escape Addict, included content related to alcoholism along with other types of addictive disorders (26). The effects of these interventions are summarized in Table 3.
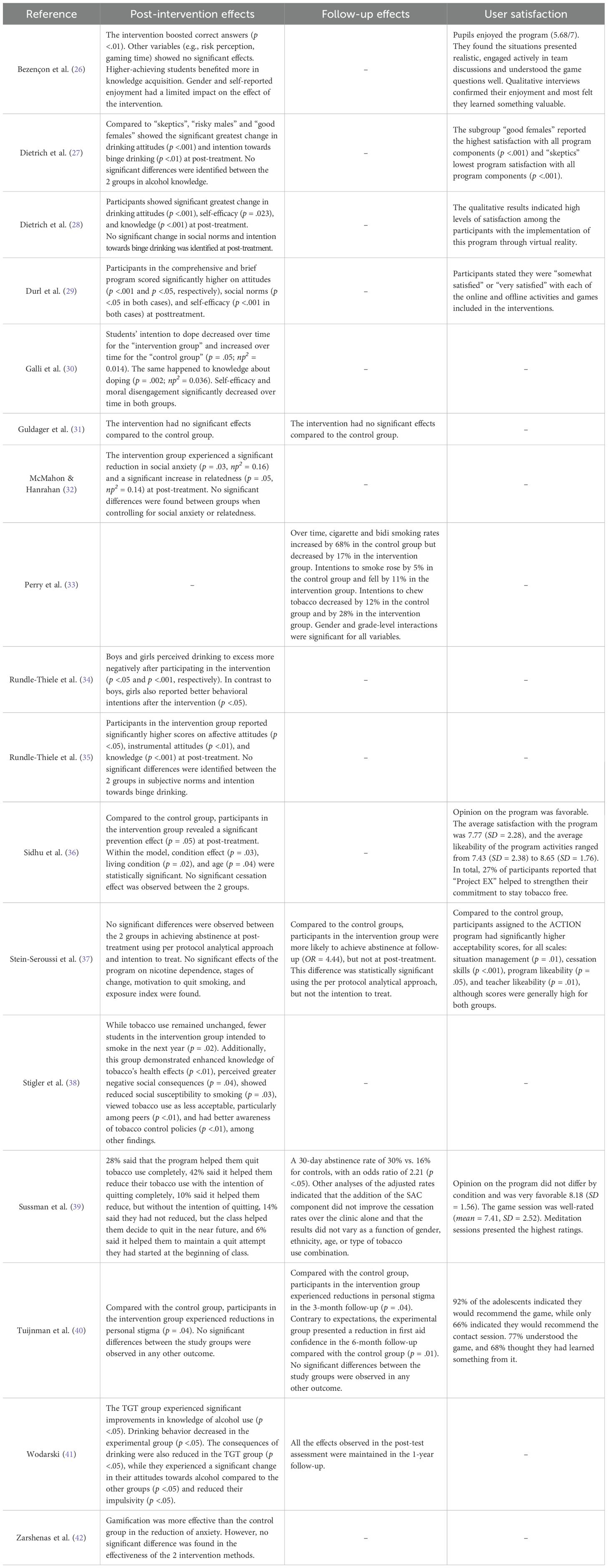
Table 3. Effects of the intervention.
Most studies reported positive findings regarding knowledge acquisition: five (26–28, 35, 41) observed significant increases in knowledge about alcohol (e.g., low-risk alcohol consumption levels or consequences of drink driving), while one found no effects on this outcome (31). Attitudes related to drinking were assessed in six studies, all of which found significant positive changes (27–29, 34, 35, 41).
Drinking intentions were assessed in four studies, but only one reported a significant positive change in their subsample of females (34). Self-efficacy was evaluated in three studies: the two studies testing Blurred Minds (28, 29) reported positive findings, while Guldager et al. (31) found no significant effect of VR FestLab on self-efficacy. Other outcomes that experienced significant improvements post-intervention were social norms in Blurred Minds (29), and drinking behavior and impulsivity in TGT (41). The remaining outcomes did not experience significant changes (e.g., risk perception, subjective norms, communication skills, social support, and susceptibility to peer pressure).
Only two studies included follow-up assessments regarding the long-term effects of the interventions: Wodarski (41) found that the changes experienced after the TGT intervention were maintained after one year, while no significant effects were found after six weeks, in the case of VR FestLab (31).
3.4.2 Tobacco use
Three interventions were designed to prevent tobacco use: ACTION (37), Project EX (36, 39), and Project MYTRY (33, 38). Again, the Escape Addict program also included content related to smoking prevention (26). The summary of these findings can be found in Table 3.
The effects on knowledge acquisition were assessed in Escape Addict and Project MYTRY, both with positive outcomes (26, 38). Project MYTRY’s effect on attitudes (e.g., perceiving tobacco use as acceptable) was also evaluated with significant changes after the 1-year assessment (38), as well as its effect on intentions to smoke or chew tobacco, both in the 1-year and 2-year assessments (33, 38).
Three interventions targeted quitting smoking as a main outcome: while ACTION produced no significant changes (37), Project EX produced higher rates of cessation than a control condition (39), as well as preventive effects (36). Project MYTRY did not produce an effect in the 1-year assessment, but in the second year, cigarette and bidi smoking rates increased by 68% in the control group but decreased by 17% in the intervention group (33). Other outcomes, such as motivation to quit smoking, exposure to tobacco, or stages of change, were assessed in one study, but none of them experienced a significant change in the intervention group (37).
Long-term effects were assessed for three of these interventions: after three months, the ACTION program achieved a significant rate of abstinence compared to the control group (37); similarly, Project MYTRY increased its effect in the 2-year assessment, finding significant cessation rates that were not present in the previous evaluation (33). Project EX, on its part, maintained its effects in the 3-month follow-up assessment.
3.4.3 Other substance-related and addictive behaviours
Two studies addressed risky behaviors associated with different types of addictive disorders: Galli et al. (30) observed that the I am on top! program had a significant impact on knowledge regarding doping and decreased doping intentions compared to the control group. No effects on self-efficacy or moral disengagement were found. On the other hand, Bezençon et al. (26) also reported that the Escape addict program increased the proportion of correct answers by around ten percentage points on average and had a positive impact on the variety of interlocutors with whom the themes of the intervention were discussed, which could be related to a change in attitudes. Risk perception and other behaviors did not experience significant changes. As shown in Table 3, no follow-up assessments were included in these 2 studies.
3.4.4 Anxiety
Two interventions addressed anxiety: LifeMatters produced a significant increase in relatedness, as well as a reduction in social anxiety, although both effects were not significant when including the other variable as a covariate in the model (32). In the same line, the intervention tested by Zarshenas et al. (42) reduced anxiety, but not more than the active control condition. These studies did not include any measures of knowledge, attitudes, or intentions. As shown in Table 3, the long-term effects of the interventions were not assessed.
3.4.5 Depression
Only 1 study focused on teaching about depression to reduce its associated stigma (40): the Moving Stories program did not produce significant changes in knowledge regarding depression (e.g., symptom recognition), and help-seeking intentions, as well as first aid intentions, were also not improved. However, it did produce a significant decrease in stigma that was maintained in the 3-month follow-up assessment, but not after six months. Other outcomes did not experience significant changes after the intervention: first-aid confidence (which experienced a significant decrease in the 6-month follow-up evaluation), help-seeking behavior, and first-aid behavior. The summary of these findings can be found in Table 3.
3.5 User satisfaction with the intervention
Eight studies reported users’ opinions about the program, and these were favorable in all cases (see Table 3): Escape Addict obtained a 5.68 out of 7, and students provided positive feedback about the contents and dynamics of the intervention. GO: KA, on its part, presented moderate levels of satisfaction (average of 3 out of 5), with one subsample (“good females”) showing more favorable opinions towards it. The Blurred Minds program received positive feedback from the participants in two studies (28, 29). Project EX had an average of around 8 points out of 10 in two studies (36, 39), and the game session was well-rated (7.41/10), although the meditation session was the most liked one. ACTION received better acceptability scores than the control intervention, although they were high for both groups (37). Finally, as reported by Tuijnman et al. (40), 92% of the adolescents who participated in the study indicated they would recommend Moving Stories.
4 Discussion
The identification of effective interventions with innovative approaches is necessary to awaken the interest, motivation, and commitment of adolescents toward their physical and mental health (43). This systematic review examined, for the first time, the efficacy of game-based classroom interventions to promote knowledge and healthy attitudes related to mental health among adolescents. Although effects varied by intervention type and context, findings from the 17 included studies (mostly from cluster-randomized controlled trial designs) suggest that these interventions are potentially effective resources for improving mental health knowledge and modifying risk behaviors. They also provide evidence about adolescents’ satisfaction with the content, dynamics, and methodology of these programs.
Despite notable heterogeneity in content, format, and targeted outcomes, certain features appear to enhance intervention effectiveness. Interventions incorporating interactive and immersive elements—such as role-playing scenarios or decision-making with real-time feedback—tended to show stronger post-intervention effects (e.g., Blurred Minds, Escape Addict, Moving Stories, I Am on Top!). Another key factor for sustained impact is multiple sessions with repeated exposure, which seems crucial for maintaining long-term effects (e.g., Project MYTRI, TGT). Similarly, combining game-based activities with guided discussions (e.g., GO: KA, Project MYTRI, LifeMatters) appears more effective than interventions relying solely on self-guided play. Finally, peer interaction also plays an important role in enhancing learning experiences: team-based components boost motivation and engagement, while competitive elements can further reinforce knowledge and behavior change.
For what concerns to those interventions aimed at reducing alcohol consumption, the four of them had positive effects in terms of knowledge acquisition and attitude change. Consistently, programs such as Blurred Minds (28, 29) and GO: KA (27, 34, 35) achieved significant improvements in alcohol knowledge and attitudes towards responsible drinking. However, changes in drinking intentions and self-efficacy were less consistent. Among these interventions, no significant changes were found in outcomes such as risk perception, subjective norms, communication skills, social support, and susceptibility to peer pressure. The lack of change in some outcomes may suggest that these programs need additional components that reinforce the practical skills and confidence of adolescents to apply what they have learned in real-life situations. In addition, most of the studies did not include long-term assessments, which limits the ability to determine the persistence of the effects detected over time.
Two of the three interventions aimed at preventing tobacco use, i.e., Project EX (36, 39) and Project MYTRI (33, 38), also showed improvements in knowledge and changes in attitudes toward tobacco use. Nevertheless, the effects on smoking cessation were heterogeneous, with some studies reporting higher abstinence rates (36, 39) and others finding no significant differences (37). Follow-up results from Project MYTRI (33, 38) showed sustained effects on reducing smoking intention. The variability detected in these interventions could be due to differences in the implementation, duration, and cultural context of the programs, as well as the level of support provided.
On the other hand, the two interventions focused on other substance-related and addictive disorders and the three interventions focused on mental health problems such as anxiety and depression indicated heterogeneous findings. For instance, the I am on top! (30) program succeeded in reducing doping intention and increasing knowledge about its risks but did not have a significant impact on self-efficacy. Similarly, the Moving Stories (40) program reduced depression’s stigma after treatment and at three months, although it did not significantly improve other aspects, such as knowledge about depression or intentions to seek help. Before including covariates in the model, the LifeMatters (32) program produced a significant increase in relatedness and a reduction in social anxiety. Escape Addict (26), which consists of a escape room implemented in the classroom, was effective for improving literacy towards substance-related and addictive disorders, but had no impact on other outcomes such as risk perception of gaming time. More evidence is needed to determine the efficacy of these interventions.
To date, game-based interventions have shown a diverse approach to addressing different health problems in adolescents (17, 18) and in the general population (19). As observed in the studies included in this systematic review, game-based interventions delivered in the classroom have varied according to format and activities, including videogames, virtual reality, interactive games, and collaborative competitions. Over the past three decades, classrooms have evolved significantly, moving from traditional paper-and-pencil activities and whiteboard illustrations to environments equipped with internet connectivity, social media, computer applications, and various technological adaptations. These advancements have likely influenced the design and delivery of game-based interventions. With the vast array of technology available today, it is crucial to continue exploring how to develop games that can successfully engage adolescents while also educating them on important topics such as mental health (44). As the digital landscape grows, researchers should focus on optimizing game design to ensure these interventions are not only engaging but also effective in promoting behavioral change.
4.1 Future research
This systematic review highlights the need for further research on the effects of game-based interventions implemented within classroom settings to promote knowledge and healthy attitudes related to mental health in adolescents. So far, most of the studies published in the literature have focused on exploring the benefits of these programs to prevent or intervene in different substance-related disorders (e.g., drinking behaviors, tobacco use, and doping). However, it would be pertinent for future lines of research to explore the efficacy of these interventions in addressing other prevalent mental health problems in adolescents, such as affective or eating disorders, among others (11). Additionally, it is crucial for such studies to explore the long-term effects of interventions targeting adolescents, particularly regarding their impact on knowledge, attitudes, and healthy behaviors.
Identifying potential mediating or moderating factors that may influence the effectiveness of game-based interventions could be key in customizing programs to meet the unique needs of different adolescent groups. Personalization of interventions seems essential to improve the effectiveness of school-based programs (45). Considering factors such as the age, gender, and socioeconomic context of adolescents, among others, could help to design interventions more in line with their needs and interests (46–48). In this regard, exploring diversity emerges as a fundamental aspect of understanding how game-based interventions can be better adapted to meet adolescents’ needs. For instance, Bezençon et al. (26) observed that gender and academic performance played a role in knowledge acquisition. Future research should investigate how diversity-related factors, such as socioeconomic status, race, ethnicity, gender identity, and cultural background, might influence the effectiveness of these programs. Recognizing these elements is essential to developing inclusive and culturally sensitive interventions that can be applied to diverse adolescent populations. Therefore, it is crucial to ensure that these interventions are accessible and relevant to all adolescents, regardless of their background or identity.
For educators, it is considered essential to create interventions that not only inform but also actively involve adolescents through interactive elements and relevant contexts. It would also be necessary for public policies to support the integration of these programs into the school curriculum, providing the necessary resources for their implementation and continuous evaluation. In addition, training educators in the use of these tools could contribute to maximizing their impact (49, 50). Encouraging the consistent practice of acquired skills over time, as well as adapting game content to be resonant with adolescents’ daily experiences could be elements that contribute to increasing their impact and sustainability (15, 16). This, along with the integration of playful elements that promote collaboration and mutual support, could facilitate the creation of more inclusive and motivating learning environments (51). Finally, assessing how different game elements, such as narrative, interactivity, and rewards, influence mental health outcomes could provide valuable information for designing effective interventions. All these improvements could help maximize the potential of games as intervention tools in promoting mental health among adolescents.
4.2 Limitations
One limitation of our review is the lack of a meta-analysis. While this approach was considered, it was deemed not feasible for several reasons. Primarily, there is a lack of standardized and validated operational definitions for mental health outcomes in game-based interventions. This heterogeneity in both outcome conceptualization and measurement tools significantly reduced comparability across studies, limiting the potential for data synthesis. Furthermore, outcomes such as knowledge, intentions, and attitudes were measured inconsistently across studies. Specifically, only five studies reported the necessary data, and the wide variety of instruments used rendered the data non-comparable. Additionally, the small number of available datasets would result in low statistical power and unreliable pooled estimates.
Another limitation is the generally low or fair quality of the studies included in this systematic review. The characteristics of the programs (i.e., number of sessions, intervention components, and measures) and targets (i.e., addictive behaviors, depression, and anxiety) were heterogeneous. For what concerns to outcomes, most of them were assessed using ad hoc questionnaires which, although sometimes showing acceptable internal consistency, lacked validation—thereby reducing the precision and reliability of the findings. Furthermore, in several cases, the description of the games used was incomplete, limiting the ability to analyze the contribution of specific program components. Only one-third of the studies included follow-up assessments, which hinders understanding of the long-term effects of these interventions. Taken together, these limitations suggest that it is still premature to draw strong conclusions about the effects of classroom-based game interventions to promote mental health among adolescents.
The variability in cohort characteristics across the studies included (e.g., periods of implementation, regional differences, and adolescent population variations) may have influenced the results. Such factors, including social, cultural, and educational changes over time, could limit the generalizability of the findings. Also, studies from the earliest available research were included in the systematic review to offer a comprehensive overview of the evidence on this topic. While this approach enabled the capture of the field’s evolution, it may also present a limitation, as older studies may vary significantly in methodology, context, and outcomes, potentially impacting the overall interpretation of the findings. Moreover, this systematic review included only studies published in English or Spanish, so other relevant evidence could have been excluded.
One last limitation of this review is the limited identification of theoretical frameworks underpinning the interventions. Most studies did not explicitly report the psychological theories guiding their design, which hinders the understanding of the causal mechanisms through which game elements might influence mental health outcomes. This gap limits the ability to draw conclusions about why certain intervention components may be more effective than others. Future research should place greater emphasis on grounding interventions in established theoretical models, which would help clarify the mechanisms of change and inform the development of more effective and targeted game-based strategies.
4.3 Conclusion
Game-based interventions represent a promising strategy to address adolescent mental health challenges, particularly in relation to substance-related and addictive disorders. This systematic review found evidence supporting their effectiveness in improving knowledge and attitudes toward alcohol and tobacco use, as well as in reducing the intention to consume these substances. Although further research is needed in areas such as anxiety and depression, the high levels of satisfaction and engagement reported by adolescents highlight the acceptability of these interventions in educational settings. Based on these findings, we recommend that teachers consider integrating evidence-informed game-based activities into health education curricula; that intervention designers align game content with specific psychological targets and employ validated outcome measures; and that policymakers support the implementation and evaluation of these programs by providing resources and training in schools. These recommendations can guide the development of more rigorous, theory-driven interventions and promote mental health literacy among adolescents.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
JS-M: Data curation, Writing – original draft, Methodology, Software, Conceptualization. AP-A: Conceptualization, Visualization, Methodology, Writing – original draft, Software, Data curation. CA-L: Writing – original draft, Data curation, Conceptualization, Methodology. ER-C: Writing – review & editing. CM-C: Writing – review & editing. IC-G: Writing – review & editing. AM-B: Writing – review & editing. JG-C: Writing – review & editing. YL-D-H: Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This research was supported by Carlos III Health Institute (ISCIII) of the Spanish Ministry of Economy and Competitiveness with group funds the Research Network on Chronicity, Primary Care and Health Promotion (RICAPPS, RD21/0016/0005) that is part of the Results-Oriented Cooperative Research Networks in Health (RICORS; ISCIII), funded by the European Union “NextGeneration EU/PRTR” funds and Mental Health Research Group in Primary Care (B17_23R) which is part of the Department of Employment, Science and Universities at the Government of Aragón (Spain).
Acknowledgments
The authors thank the Centre for Biomedical Research in Epidemiology and Public Health (CIBERESP; CB22/02/00052; ISCIII), the Research Network on Chronicity, Primary Care and Health Promotion, and the Instituto de Investigación Sanitaria Aragón for their support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1622099/full#supplementary-material
References
1. Sawyer SM, Afifi RA, Bearinger LH, Blakemore SJ, Dick B, Ezeh AC, et al. Adolescence: a foundation for future health. Lancet (London England). (2012) 379:1630–40. doi: 10.1016/S0140-6736(12)60072-5
2. United Nations. 1 in 7 children and teens impacted by mental health conditions. UN News (2024). Available online at: https://news.un.org/en/story/2024/10/1155536 (Accessed May 2, 2024).
3. Aguilera P, Navarro-Gil M, Pérez-Aranda A, Armas-Landaeta C, Beltrán-Ruiz M, Rodríguez-Freire C, et al. Applying a school-based mindfulness and compassion program (“Escuelas despiertas”) in spanish secondary schools to reduce psychological distress in adolescents: A randomized controlled trial. School Ment Health. (2025) 17:234–46. doi: 10.1007/s12310-024-09722-1
4. Dodge KA, Skinner AT, Godwin J, Bai Y, Lansford JE, Copeland WE, et al. Impact of the COVID-19 pandemic on substance use among adults without children, parents, and adolescents. Addictive Behav Rep. (2021) 14:100388. doi: 10.1016/j.abrep.2021.100388
5. Oliveira JMD, Butini L, Pauletto P, Lehmkuhl KM, Stefani CM, Bolan M, et al. Mental health effects prevalence in children and adolescents during the COVID-19 pandemic: A systematic review. Worldviews Evidence-Based Nurs. (2022) 19:130–7. doi: 10.1111/WVN.12566
6. Temple JR, Baumler E, Wood L, Guillot-Wright S, Torres E, and Thiel M. The impact of the COVID-19 pandemic on adolescent mental health and substance use. J Adolesc Health. (2022) 71:277–84. doi: 10.1016/j.jadohealth.2022.05.025
7. Jordan CJ and Andersen SL. Sensitive periods of substance abuse: Early risk for the transition to dependence. Dev Cogn Neurosci. (2017) 25:29–44. doi: 10.1016/J.DCN.2016.10.004
8. Kutcher S and Wei Y. Mental health and the school environment: Secondary schools, promotion and pathways to care. Curr Opin Psychiatry. (2012) 25:311–6. doi: 10.1097/YCO.0b013e3283543976
9. Weisz JR and Kazdin AE. Evidence-Based Psychotherapies For Children and Adolescents. New York, US: Guilford Press (2017).
10. Johnstone KM, Kemps E, and Chen J. A meta-analysis of universal school-based prevention programs for anxiety and depression in children. Clin Child Family Psychol Rev. (2018) 21:466–81. doi: 10.1007/S10567-018-0266-5
11. Nobre J, Oliveira AP, Monteiro F, Sequeira C, and Ferré-Grau C. Promotion of mental health literacy in adolescents: A scoping review. Int J Environ Res Public Health. (2021) 18:9500. doi: 10.3390/IJERPH18189500
12. Cairns K and Rossetto A. School-based mental health literacy interventions. In: Okan O, Bauer U, Levin-Zamir D, Pinheiro P, and Sorensen K, editors. International Handbook Of Health Literacy: Research, Practice And Policy Across the Life-Span. Bristol, United Kingdom: Policy Press (2019). p. 1–768.
13. Monreal-Bartolomé A, Barceló-Soler A, García-Campayo J, Bartolomé-Moreno C, Cortés-Montávez P, Acon E, et al. Preventive gambling programs for adolescents and young adults: A systematic review. Int J Environ Res Public Health. (2023) 20:4691. doi: 10.3390/IJERPH20064691
14. Fitz-Walter Z. Achievement Unlocked: Investigating the Design of Effective Gamification Experiences for Mobile Applications and Devices. Brisbane, Australia: Queensland University of Technology (2015).
15. Ritterfeld U, Cody M, and Vorderer P. Serious games: Mechanisms and effects. New York, US: Routledge (2009).
16. Tori AA, Tori R, and Nunes F. D. L. D. S. Serious game design in health education: A systematic review. IEEE Trans Learn Technol. (2022) 15:827–46. doi: 10.1109/TLT.2022.3200583
17. Ameryoun A, Sanaeinasab H, Saffari M, and Koenig HG. Impact of game-based health promotion programs on body mass index in overweight/obese children and adolescents: A systematic review and meta-analysis of randomized controlled trials. Childhood Obes (Print). (2018) 14:67–80. doi: 10.1089/CHI.2017.0250
18. Caselles-Pina L, Sújar A, Quesada-López A, and Delgado-Gómez D. Adherence, frequency, and long-term follow-up of video game-based treatments in patients with attention-deficit/hyperactivity disorder: A systematic review. Brain Behav. (2023) 13:e3265. doi: 10.1002/BRB3.3265
19. DeSmet A, Van Ryckeghem D, Compernolle S, Baranowski T, Thompson D, Crombez G, et al. A meta-analysis of serious digital games for healthy lifestyle promotion. Prev Med. (2014) 69:95–107. doi: 10.1016/J.YPMED.2014.08.026
20. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
21. Cuevas-Lara C, Izquierdo M, Sáez de Asteasu ML, Ramírez-Vélez R, Zambom-Ferraresi F, Zambom-Ferraresi F, et al. Impact of game-based interventions on health-related outcomes in hospitalized older patients: A systematic review. J Am Med Directors Assoc. (2021) 22:364–371.e1. doi: 10.1016/j.jamda.2020.07.027
22. Li J, Theng YL, and Foo S. Game-based digital interventions for depression therapy: A systematic review and meta-analysis. Cyberpsychology Behav Soc Networking. (2014) 17:519. doi: 10.1089/CYBER.2013.0481
23. Suleiman-Martos N, García-Lara RA, Membrive-Jiménez MJ, Pradas-Hernández L, Romero-Béjar JL, Dominguez-Vías G, et al. Effect of a game-based intervention on preoperative pain and anxiety in children: A systematic review and meta-analysis. J Clin Nurs. (2022) 31:3350. doi: 10.1111/JOCN.16227
24. Perestelo-Perez L. Standards on how to develop and report systematic reviews in psychology and health. Int J Clin Health Psychol. (2013) 13:49–57. doi: 10.1016/s1697-2600(13)70007-3
25. NIH. Study Quality Assessment Tools. National Heart, Lung, and Blood Institute (2014). Available online at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (Accessed October 10, 2024). NHLBI, NIH.
26. Bezençon V, De Santo A, Holzer A, and Lanz B. Escape Addict: A digital escape room for the prevention of addictions and risky behaviors in schools. Comput Educ. (2023) 200:104798. doi: 10.1016/j.compedu.2023.104798
27. Dietrich T, Rundle-Thiele S, Leo C, and Connor J. One size (Never) fits all: Segment differences observed following a school-based alcohol social marketing program. J School Health. (2015) 85:251–9. doi: 10.1111/josh.12244
28. Dietrich T, Rundle-Thiele S, Kubacki K, Durl J, Gullo MJ, Arli D, et al. Virtual reality in social marketing: a process evaluation. Marketing Intell Plann. (2019) 37:806–20. doi: 10.1108/MIP-11-2018-0537
29. Durl J, Dietrich T, and Kubacki K. Effectiveness of a brief versus a comprehensive social marketing program. J Soc Marketing. (2020) 10:377–94. doi: 10.1108/JSOCM-11-2019-0199
30. Galli F, Chirico A, Codella R, Zandonai T, Deplano V, De Maria A, et al. I am on top!”: an interactive intervention program to promote self-regulation processes in the prevention of the use of doping in sports high schools. Eur J Invest Health Psychol Educ. (2023) 13:2630–41. doi: 10.3390/ejihpe13110183
31. Guldager JD, Kjær SL, Grittner U, and Stock C. Efficacy of the virtual reality intervention VR festLab on alcohol refusal self-efficacy: A cluster-randomized controlled trial. Int J Environ Res Public Health. (2022) 19:3293. doi: 10.3390/ijerph19063293
32. McMahon MG and Hanrahan SJ. Life matters: exploring the influence of games and mental skills on relatedness and social anxiety levels in disengaged adolescent students. J Appl Sport Psychol. (2020) 32:205–19. doi: 10.1080/10413200.2018.1557764
33. Perry CL, Stigler MH, Arora M, and Reddy KS. Preventing tobacco use among young people in India: Project MYTRI. Am J Public Health. (2009) 99:899–906. doi: 10.2105/AJPH.2008.145433
34. Rundle-Thiele S, Russell-Bennett R, Leo C, and Dietrich T. Moderating teen drinking: Combining social marketing and education. Health Educ. (2013) 113:392–406. doi: 10.1108/HE-07-2012-0041
35. Rundle-Thiele S, Schuster L, Dietrich T, Russell-Bennett R, Drennan J, Leo C, et al. Maintaining or changing a drinking behavior? GOKA’s short-term outcomes. J Business Res. (2015) 68:2155–63. doi: 10.1016/j.jbusres.2015.03.015
36. Sidhu AK, Sussman S, Tewari A, Bassi S, and Arora M. Project EX-India: A classroom-based tobacco use prevention and cessation intervention program. Addictive Behav. (2016) 53:53–7. doi: 10.1016/j.addbeh.2015.09.005
37. Stein-Seroussi A, Stockton L, Brodish P, and Meyer M. Randomized controlled trial of the ACTION smoking cessation curriculum in tobacco-growing communities. Addictive Behav. (2009) 34:737–43. doi: 10.1016/j.addbeh.2009.04.016
38. Stigler MH, Perry CL, Arora M, Shrivastav R, Mathur C, and Reddy KS. Intermediate outcomes from project MYTRI: Mobilizing youth for tobacco-related initiatives in India. Cancer Epidemiol Biomarkers Prev. (2007) 16:1050–6. doi: 10.1158/1055-9965.EPI-06-0929
39. Sussman S, Dent CW, and Lichtman KL. Project EX. Outcomes of a teen smoking cessation program. Addictive Behav. (2001) 26:425–38. doi: 10.1016/S0306-4603(00)00135-0
40. Tuijnman A, Kleinjan M, Olthof M, Hoogendoorn E, Granic I, and Engels RCME. A game-based school program for mental health literacy and stigma on depression (Moving stories): cluster randomized controlled trial. JMIR Ment Health. (2022) 9:1–26. doi: 10.2196/26615
41. Wodarski JS. A social learning approach to teaching adolescents about alcohol and driving: A multiple variable follow-up evaluation. J Behav Ther Exp Psychiatry. (1987) 18:51–60. doi: 10.1016/0005-7916(87)90071-1
42. Zarshenas L, Saranjam E, Mehrabi M, and Setoodeh G. Microlearning and Gamification in Anxiety Management among girl adolescents in Iran: An interventional study. Pakistan J Med \& Health Sci. (2020) 14:689–94.
43. Chen T, Ou J, Li G, and Luo H. Promoting mental health in children and adolescents through digital technology: a systematic review and meta-analysis. Front Psychol. (2024) 15:1356554/BIBTEX. doi: 10.3389/FPSYG.2024.1356554/BIBTEX
44. Fleming TM, Bavin L, Stasiak K, Hermansson-Webb E, Merry SN, Cheek C, et al. Serious games and gamification for mental health: Current status and promising directions. Front Psychiatry. (2017) 7:215. doi: 10.3389/fpsyt.2016.00215
45. Jahedi F, Fay Henman PW, and Ryan JC. Personalization in digital psychological interventions for young adults. Int J Human–Computer Interaction. (2024) 40:2254–64. doi: 10.1080/10447318.2022.2158261
46. Gómez-Odriozola J and Calvete E. Effects of a mindfulness-based intervention on adolescents’ Depression and self-concept: the moderating role of age. J Child Family Stud. (2021) 30:1501–15. doi: 10.1007/S10826-021-01953-Z/METRICS
47. Macintyre AK, Torrens C, Campbell P, Maxwell M, Pollock A, Biggs H, et al. Socioeconomic inequalities and the equity impact of population-level interventions for adolescent health: an overview of systematic reviews. Public Health. (2020) 180:154–62. doi: 10.1016/J.PUHE.2019.11.008
48. Meneses C and Charro B. ¿Es necesaria una intervención diferencial de género en la prevención universal y selectiva del consumo de drogas en adolescentes? Rev Psiquiatría y Salud Ment. (2014) 7:5–12. doi: 10.1016/J.RPSM.2013.01.003
49. Hart LM, Morgan AJ, Rossetto A, Kelly CM, Mackinnon A, and Jorm AF. Helping adolescents to better support their peers with a mental health problem: A cluster-randomised crossover trial of teen Mental Health First Aid. Aust New Z J Psychiatry. (2018) 52:638–51. doi: 10.1177/0004867417753552
50. Hart LM, Bond KS, Morgan AJ, Rossetto A, Cottrill FA, Kelly CM, et al. Teen Mental Health First Aid for years 7-9: A description of the program and an initial evaluation. Int J Ment Health Syst. (2019) 13:1–13. doi: 10.1186/S13033-019-0325-4/TABLES/7
Keywords: adolescents, classroom, game-based interventions, public mental health, systematic review
Citation: Sanabria-Mazo JP, Pérez-Aranda A, Armas-Landaeta C, Royuela-Colomer E, Mateo-Canedo C, Cabrera-Gil I, Monreal-Bartolomé A, García-Campayo J and López-del-Hoyo Y (2025) The use of games in the classroom to promote mental health knowledge and healthy attitudes in adolescents: a systematic review. Front. Psychiatry 16:1622099. doi: 10.3389/fpsyt.2025.1622099
Received: 02 May 2025; Accepted: 11 August 2025;
Published: 01 September 2025.
Edited by:
Bruno Bonnechère, University of Hasselt, BelgiumReviewed by:
Matias E. Rodriguez-Rivas, Universidad de las Américas, ChileSiti Irma Fadhilah Ismail, Universiti Putra Malaysia, Malaysia
Copyright © 2025 Sanabria-Mazo, Pérez-Aranda, Armas-Landaeta, Royuela-Colomer, Mateo-Canedo, Cabrera-Gil, Monreal-Bartolomé, García-Campayo and López-del-Hoyo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adrián Pérez-Aranda, YWRyaWFuLnBlcmV6QHVhYi5jYXQ=