 Fredrik Gustafsson1*
Fredrik Gustafsson1* Adrian Desai Boström1,2
Adrian Desai Boström1,2 Alexander Wilczek3
Alexander Wilczek3 Matilda Naesström1Mia Rajalin1
Matilda Naesström1Mia Rajalin1 Marie Åsberg3
Marie Åsberg3 Jussi Jokinen1,2
Jussi Jokinen1,2- 1Department of Clinical Sciences/Psychiatry, Umeå University, Umeå, Sweden
- 2Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden
- 3Department of Clinical Sciences, Karolinska Institutet, Stockholm, Sweden
Background: Patients with emotionally unstable personality disorder (EUPD) report increased use and exposure to interpersonal violence and experience significant interpersonal difficulties. The relationship between the type of self-reported interpersonal problems and interpersonal violence among individuals with EUPD remains unclear. This study investigates the association between interpersonal problems and the cumulative lifetime violence burden among suicidal women with EUPD.
Methods: The study included 103 women diagnosed with EUPD who had attempted suicide at least twice. The inventory of Interpersonal problems (IIP) and the Karolinska Interpersonal Violence Scale (KIVS) were used to assess interpersonal problems and lifetime violence load. The eight IIP subscales were grouped into two factors: Factor 1 (Domineering; Vindictive; Cold; Social avoidant) and Factor 2 (Nonassertive; Exploitable; Overly nurturant, and Intrusive).
Results: The mean T-scores for IIP subscales ranged from 56 to 63, while the KIVS total score varied from 0 to 19, with a mean of 7.63. Cumulative lifetime violence burden was significantly associated with IIP Factor 1 (Spearman’s rho=0.26, p=0.0081), but not with IIP Factor 2 (r=0.014, p=0.89). Linear regression analysis revealed that Factor 1 (t=2.99, p=0.0039) and global assessment of functioning (GAF) (t=-2.26, p=0.027) significantly predicted accumulated lifetime interpersonal violence. Further post-hoc analysis showed that individuals with higher violence burdens exhibited significantly greater interpersonal problems in the three domains of Factor 1 - Domineering/Controlling, Vindictive/Self-centered, and Cold/Distant.
Conclusions: Specific Interpersonal problems and low functioning seem to be associated with cumulative lifetime violence burden among suicidal women with EUPD. These interpersonal traits may serve as key targets for treatment and prevention.
Highlights
● Women with emotionally unstable personality disorder report high levels of interpersonal violence and interpersonal problems.
● High violence burden is associated with being controlling, self-centered and distant in interpersonal relationships.
● Low global functioning is associated with cumulative lifetime violence burden among suicidal women with emotionally unstable personality disorder.
1 Introduction
Emotionally unstable personality disorder (EUPD), also known as Borderline Personality Disorder, one of cluster B disorders, is characterized by nine symptoms/criteria such as emotional dysregulation, chronic feelings of emptiness, self-destructive impulsivity and instability in interpersonal relationships (1). The disorder is associated with increased mortality, including a nearly five-fold increase in all-cause mortality and a 50-fold increase in suicide risk (2, 3). Interpersonal problems are central to EUPD pathology and play a crucial role in treatment outcomes (4). Difficulties in interpersonal relationships have also proved to be a trigger for suicidal behavior, and even important in the familial transmission of suicidal behavior (5, 6).
Exposure to violence during childhood and violent behavior in adulthood are risk factors for later completed suicide in suicide attempters (7) and women with EUPD report high life-time interpersonal violence exposure (8). People with EUPD are more prone to use violence according to a recent systematic and meta-regression analysis (Odds ratio 2.6) (9). EUPD is characterized by a wide variety of interpersonal problems related to symptom severity and therapeutic alliance (10). Whether interpersonal violence is associated with specific types of interpersonal problems among individuals with EUPD is to our knowledge not known. This study investigates the association between interpersonal problems and cumulative lifetime interpersonal violence burden among women with EUPD and a history of repeated suicidal behavior.
2 Materials and methods
2.1 Participants
This study utilized data from 106 women diagnosed with EUPD who participated in the “Stockholm County Council and Karolinska Institute Psychotherapy Project for Suicide-Prone Women” (SKIP). Participants were recruited between 1999 and 2004 as part of a randomized controlled trial comparing dialectic behavioral therapy, psychodynamic therapy and treatment as usual. Inclusion criteria required a verified EUPD diagnosis and a history of at least two potentially lethal suicide attempts, with one occurring within six months before referral. Participants were excluded if they had a current life-threatening eating disorder, current psychotic disorder or major depressive illness with melancholic features, evidence of dementia or other irreversible organic brain syndrome or a current diagnosis of substance dependence. Details on the EUPD cohort have been previously published (8, 11). The original study protocol was approved by the Committee for Ethical Research at Karolinska Institutet (Dnrs: 95–283; 2021-06929-01). Patients were referred from all the psychiatric clinics in Stockholm County Council (encompassing care of 1.8 million inhabitants). A total of 162 women with EUPD were invited to take part in the SKIP project. Of these individuals, 14 (8.7%) declined to join the study, 41 (25.3%) were excluded due to not fulfilling inclusion criteria or to fulfilled exclusion criteria. One completed suicide before joining the study. All participants were checked in Swedish cause of death registry until 2011, and eight had died by suicide.
2.2 Assessments
The participants were interviewed by trained clinicians using a range of semi-structured psychiatric diagnostic and assessment tools, the SCID I research version interview to establish the DSM–IV diagnoses (12), and DIP–I to establish Axis II diagnoses (13). To measure the participants overall psychosocial impairment the Global Assessment of Functioning (GAF) was used (14). Non-violent suicide attempt method included tablet intoxications while all other methods were defined as violent (hanging, drowning, jumping from a height for example). The two questionnaires used to examine interpersonal problems and interpersonal violence are presented below.
2.2.1 Inventory of interpersonal problems
The Inventory of Interpersonal Problems (IIP), a 64-item questionnaire measuring interpersonal problems has been extensively validated and has shown strong reliability (Cronbach’s alpha of 0.78) (15). Validity of the IIP has been confirmed in Sweden as well (16).
The inventory comprises eight subscales, each representing distinct interpersonal difficulties, with updated names provided in parentheses: Domineering (Domineering/Controlling), Vindictive (Vindictive/Self-centered), Cold (Cold/Distant), Social avoidant (Social inhibited), Non-assertive (Non-assertive), Exploitable (Overly Accommodating), Overly nurturant (Self-sacrificing), and Intrusive (Intrusive/Needy). Respondents indicate the extent to which they find it challenging to handle distressing interpersonal situations using statements like “it is hard for me to…” and “these are things I do too much or too often.” Responses are recorded on a Likert scale ranging from 0 (not at all) to 4 (extremely).
For instance, the Domineering scale assesses difficulties in maintaining control and exhibiting aggressive behaviors, such as “I try to change people too much.” High scores on the Vindictive scale indicate struggles with harboring vindictive thoughts and managing frustration and anger, as evidenced by statements like “it’s hard for me to put someone else’s needs before my own.” Similarly, a high score on the Cold scale suggests challenges in forming connections with others, with items such as “I keep other people at a distance too much.” The Social avoidant scale reflects a tendency to shy away from social interaction and express feelings, as seen in statements like “it’s hard for me to show my feelings.”
Scores on the Non-assertive scale reveal issues related to low self-confidence and difficulty in expressing needs assertively, exemplified by statements like “it’s hard for me to be firm when I need to be.” High scores on the Exploitable scale indicate a propensity to prioritize others’ needs over one’s own and difficulties in expressing anger, as demonstrated by statements like “it is hard for me to let other people know when I’m angry.”
In contrast, the Overly nurturant scale highlights struggle with setting boundaries and prioritizing others’ needs excessively, as shown in statements like “I put other people’s needs before my own too much.” Lastly, the Intrusive scale assesses challenges in respecting others’ boundaries, as evidenced by statements like “I tell personal things to other people too much.”
The total score, transformed into a normative T-score, reflects an individual’s overall level of interpersonal issues compared to the general population. Scores on the eight scales delineate specific problematic areas and types of interpersonal problems. Additionally, an ipsative T-score can offer insights into an individual’s personal level of interpersonal difficulties. These scores can be utilized to assess a patient’s interpersonal issues, compare different groups, or measure changes in interpersonal problems pre- and post-treatment.
The eight IIP subscales are known to intercorrelate and to reduce the risk of multicollinearity, the scales could be grouped into two factors as follows: Factor 1 (Domineering; Vindictive; Cold; Social avoidant) and Factor 2 (Nonassertive; Exploitable; Overly nurturant, and Intrusive) using normative T-scores (15, 17).
2.2.2 Karolinska interpersonal violence scale
The Karolinska Interpersonal Violence Scale (KIVS): a structured interview measuring both exposure and expressed violent behavior in childhood (defined as 6–14 years of age) and during adult life (defined as age 15 or older). The ratings are based on a structured interview with concrete examples of interpersonal violence performed and assessed by trained clinicians. It was first published in 2010 (7) and validated using the Buss-Durkee Hostility Inventory (BDHI) (18), “Urge to act out hostility” subscales from the Hostility Questionnaire (HDHQ) (19) and the Early Experience Questionnaire (EEQ) (20). The complete scale is presented in Appendix 1.
In brief, the first step of the KIVS explores the subjects experience of using violence as a child and as an adult and is rated 0–5 where a high number indicate a history of violent behavior. The total maximal score is 20. For example, the score “3” for used violence as a child were stated as “Often started fights. Hit comrade who had been bullied. Continued hitting when other had surrendered” and the highest score “5” was defined as “Caused serious physical injury. Violent toward adult(s). Violent behavior that led to intervention by social welfare authorities”. The second part on the other hand focuses on the subject as a victim of violence, again divided by experience as a child and as an adult. The “5” score for being a victim of violence during adulthood were stated as “Repeatedly raped. Repeatedly battered. Severely battered, resulting in serious bodily harm”.
2.3 Statistical methods
Shapiro Wilks test evaluated data distribution. Correlational analyses were used to determine associations between the total score of interpersonal violence (KIVS total score) and the two IIP factors, age at first suicide attempt, GAF score as well as the number of EUPD criteria, as continuous variables. Pearson’s r was applied for parametric correlation analyses and Spearman´s rho was applied for non-parametric correlation analyses. Depending on whether the data was normally distributed or not we used Student’s t-test or Kruskal-Wallis’ test to assess group differences (suicide attempters with and without violent suicide attempt method, respectively) in continuous variables.
From the results of the bivariate analyses of the two IIP factors, a multiple linear regression analysis was conducted to determine whether accumulated interpersonal violence was associated with specific domain of interpersonal problems adjusted for the number of EUPD criteria and the GAF score. The Durbin—Watson test statistic expressed no correlation in adjacent residuals. All statistical tests were two-tailed.
Statistical significance was set at p <0.05. We used the Statistical Package JMP 9.0.3 software, SAS Institute Inc., Cary, NC, USA.
3 Results
3.1 Participants characteristics
The mean age was 30 years (range 19–50 years, SD=7.8). 85% (n=90)of the patients had a mood disorder diagnosis and 83% (n=88) met criteria for anxiety disorders. 57% (n=60) of the patients had post-traumatic stress disorder (PTSD) and 26% (n=27) had a comorbid eating disorder. 54% (n=57) of the patients fulfilled the criteria for substance use disorder past or present (all substances, alcohol included). Fifty women had an additional personality disorder and 24% (25%) of women had three or more personality disorders. The mean age at first suicide attempt was 20 years (range 5-46, SD=7.6). Eleven percent of women with EUPD reported having used a violent suicide attempt method. The mean T-scores for IIP subscales ranged between 56–63 and are shown in Table 1. More on participants characteristics can be found in Table 2. The mean KIVS total score was 7.63 (range 0-19, SD=4). Mean number of EUPD criteria was 6.2 and 36 percent fulfilled 7 or more EUPD criteria. Mean score of the Global Assessment of Functioning (GAF) was 49.
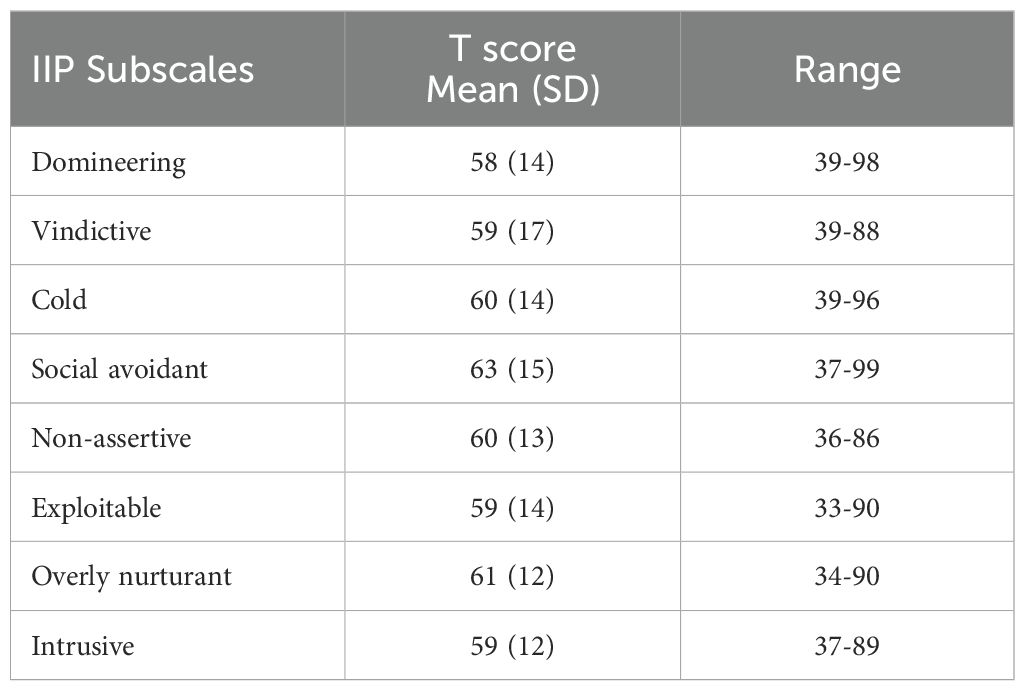
Table 1. IIP-ratings in suicidal women with EUPD (n=103), T-score mean, standard deviation (SD), range.
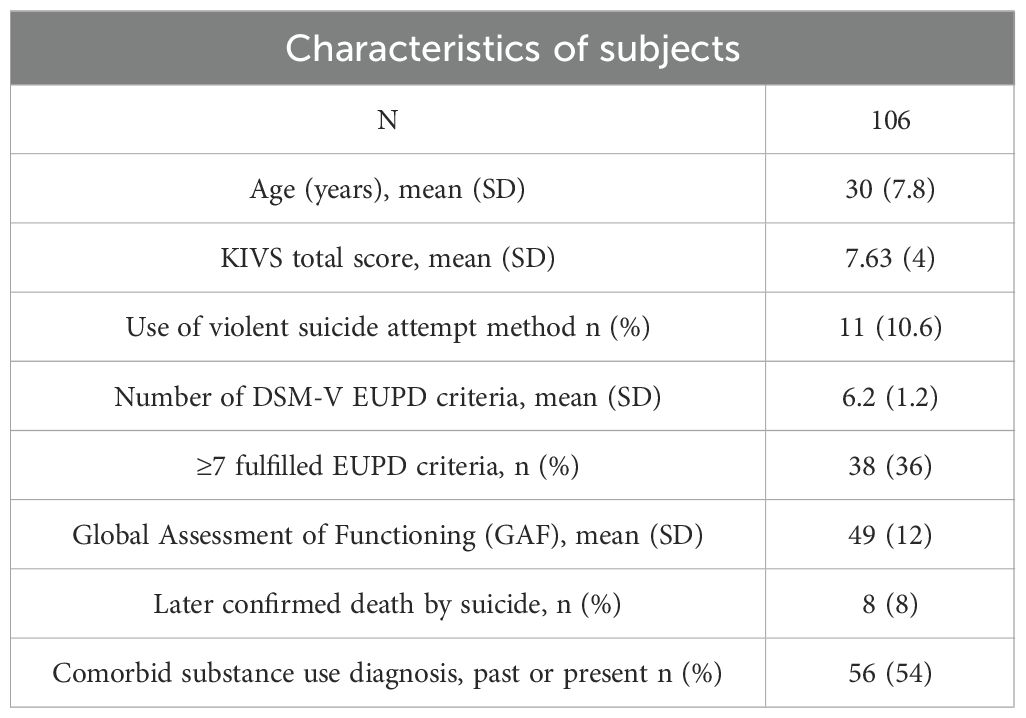
Table 2. Characteristics of subjects.
3.2 Correlations and regression analysis
The cumulative lifetime interpersonal violence was significantly associated with IIP Factor 1 (r=0.26, p=0.0071), but not with Factor 2 (r=0.014, p=0.89), Figure 1. Higher number of EUPD criteria was significantly associated both with both Factor 1 (r=0.38, p<0.0001) and cumulative lifetime interpersonal violence (r=0.26, p=0.0075). The correlation between Factor 1 and Factor 2 was significant (r=0.28, p=0.0049). GAF ratings showed significant negative correlation with the cumulative lifetime interpersonal violence (r= -0.25, p=0.025) Patients who had used a violent suicide attempt method (e.g. hanging, strangulation/suffocation, or firearms use) or patients with substance use disorder (past or present) did not have significantly different ratings in Factors 1 or 2 or KIVS total score or number of EUPD criteria. Table 3 shows correlations between the KIVS total score, Interpersonal problems grouped into Factor 1 and Factor 2, number of EUPD criteria, age at onset of suicidal behavior and GAF.
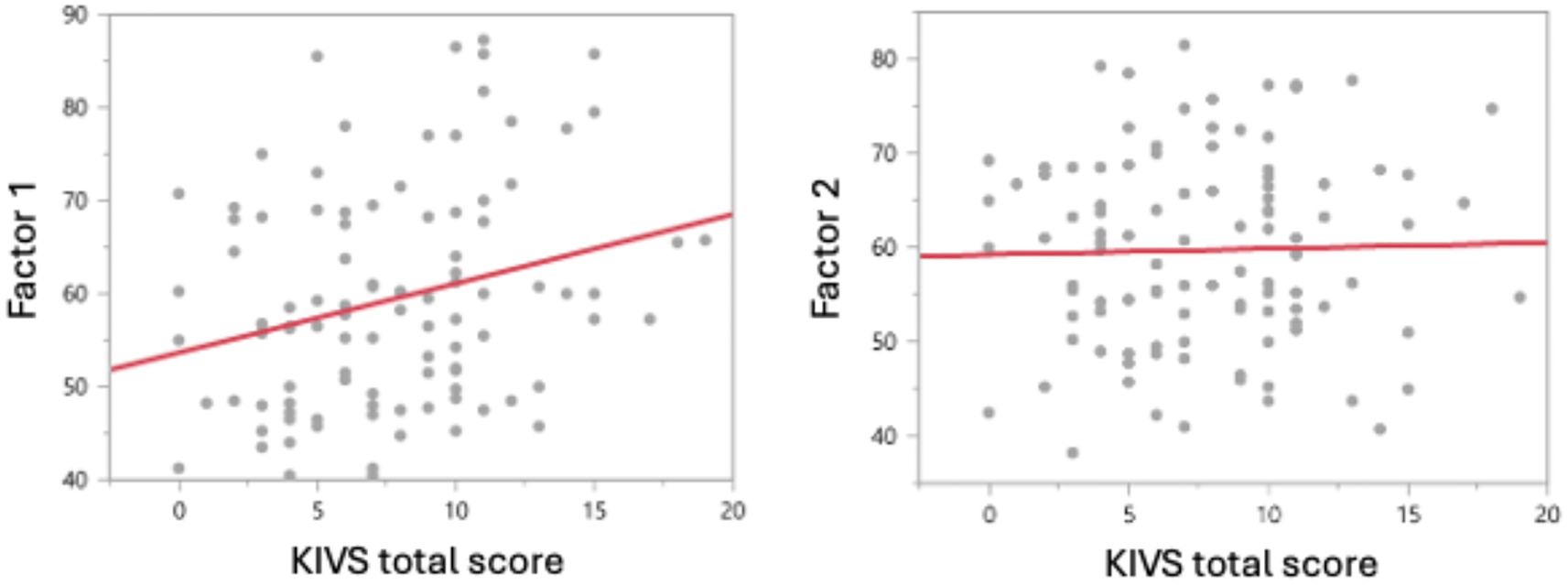
Figure 1. Bivariate correlation analysis of the Cumulative lifetime burden of violence, as measured by the total KIVS score, is significantly positively associated with Factor 1 (Spearman’s rho=0.26, p=0.0081), but not with Factor 2 (r=0.014, p=0.89).

Table 3. Correlations (Spearman’s p) between lifetime accumulated violence load and interpersonal problems grouped into Factor 1 vs Factor 2, age at first suicide attempt (SA) and number of EUPD criteria.
A multiple linear regression analysis based on the results in correlation analyses was conducted with Factor 1, Factor 2, GAF and number of EUPD criteria as predictors of accumulated lifetime interpersonal violence, entered simultaneously as predictors. The regression model was significant, adjusted RSq=0.15, df=4, p=0.004. Factor 1 and GAF were significant predictors of accumulated lifetime interpersonal violence in the regression model, Table 4.
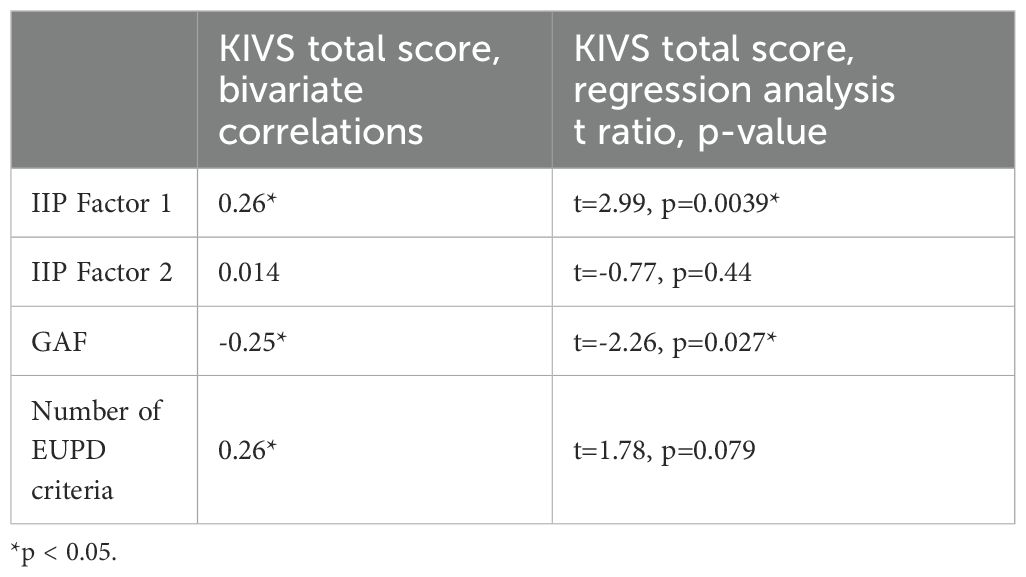
Table 4. Multiple linear regression analysis based on the results in Table 3.
Further posthoc subscale analysis revealed that suicidal women with EUPD with a high burden of violence exhibited significantly greater interpersonal problems in the domains of Domineering/Controlling, Vindictive/Self-centered, and Cold/Distant, but not in the remaining five domains of interpersonal problems, Table 5.
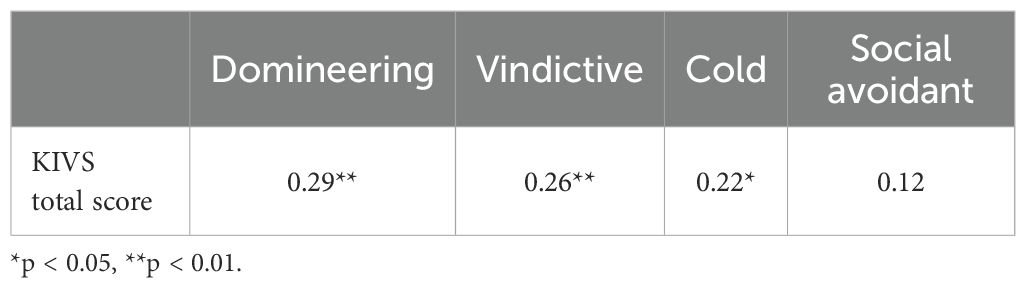
Table 5. Subscale analysis of the Interpersonal problems in Factor 1 in correlation to lifetime accumulated violence load.
4 Discussion
In this study we assessed the association between Interpersonal problems and lifetime accumulated violence load among suicidal women with EUPD. The participants rated high levels of interpersonal problems, with a mean t-scores between 58 and 63 which is higher compared to a similar study that investigated exposure to early life adversity and interpersonal functioning in attempted suicide among both men and women where the mean t-score for the eight interpersonal problems ranged between 49-61 (5). The level of interpersonal violence was also high, which is in line with previous research that concluded that combined violence (self- and other directed violence) is more common among EUPD patients compared to a normal population with a prevalence of 70.7% (21). Patients were severely ill with high level of psychiatric comorbidity as well as a high number of EUPD criteria and low global functioning.
The main finding was that Factor 1 and GAF were significant predictors of accumulated lifetime interpersonal violence. Within Factor 1, three specific domains of interpersonal problems - Domineering, Vindictive and Cold – were significantly associated with the lifetime burden of interpersonal violence in suicidal women with EUPD. The remaining interpersonal problems mainly clustered in factor 2 – Social avoidant, Non-assertive, Exploitable, Overly nurturant and Intrusive - showed no significant correlations with interpersonal violence load. This indicates that suicidal women with EUPD and a history of violence both as a victim and a perpetrator have severe specific interpersonal difficulties. They show features as difficulties to let go of control and a proneness to aggression towards others (Domineering), emotional dysregulation reflecting problems with anger, frustration and vindictive thoughts (Vindictive) and problems in connecting to others and having problems to get along with other people (Cold).
We adjusted the analysis for the number of EUPD criteria since the number of criteria was significantly positively associated with both the total interpersonal violence load and Factor 1 in bivariate analysis. In the regression analysis, the more severe EUPD, e.g. higher number of met criteria for EUPD, showed a trend to be significantly associated with IIP Factor 1. This is partly in line with the results from another study which found that childhood trauma severity positively predicted EUPD symptom severity (22).
Interestingly, neither accumulated lifetime burden of interpersonal violence or interpersonal problems were significantly associated with earlier onset of suicide attempts or use of violent suicide attempt method in this cohort of women with EUPD. Earlier study on suicide attempters found higher levels of interpersonal violence among patients who had used a violent suicide attempt method (7). Violent suicide attempt methods are more common among men and our finding in this study may reflect the fact that all participants were women. Interestingly an earlier study reported significant correlations between specific interpersonal problems like being more intrusive (clustered in Factor 2) and family history of suicide among patients with a major depressive disorder and a recent suicide attempt (6) indicating that proneness to certain type of interpersonal problems can be related to certain phenotypes of suicidal behaviors maybe in a gender specific manner. In another study specific interpersonal problems in patients with EUPD seem to affect aggressive behaviors (23).
With all this in mind, different interpersonal problems, and lifetime violence burden are part of very complex intermediate phenotypes underlying EUPD and suicidal behavior. Whether the development of specific interpersonal problems is a consequence of accumulated interpersonal violence burden or vice versa cannot be concluded from this study. However, knowledge about these associations could be important when developing treatment strategies. Future research discovering neural correlates of aggression in personality disorders could also benefit from our results, where e.g. our finding considering low global functioning and its association to interpersonal violence and EUPD symptom severity seems to be a highly relevant area in neuroimaging research aiming to examine personality disorder traits relevant to aggressive behavior (24).
Due to the available data set males were not represented in this study. This could be seen both as a strength and a limitation. The strength is by reducing potential gender confounders and the limitation is that no conclusion or treatment direction can be stated for male individuals with EUPD which may act as a knowledge gap for future research.
Since the study design is cross-sectional, it does not allow for establishing causal relationships between cumulative violence and interpersonal problems or the direction of these relationships. The Karolinska Interpersonal Violence Scale does not assess different types of violence (physical, sexual, emotional) or their context (family, intimate partner, institutional) separately, which can be seen as a limitation since a more detailed information could be clinically relevant.
The data collection was performed between 1999 and 2004, more than 20 years ago. This means that the EUPD diagnoses were set according to the DSM-IV manual, which in present clinical practice is replaced by DSM-5, which could affect the generalizability of the results to current clinical settings and social context. However, all diagnoses were established by using DSM criteria based structured interviews (research versions) by trained psychiatrists and psychologists. One could also argue that the patients fulfill the criteria for the alternative model of personality disorders (AMPD) (1), given the fact that they also showed low global functioning which is highlighted in criterion A where interpersonal functioning is highly relevant. Our results on certain interpersonal problems related to accumulated interpersonal violence burden add to the literature on the interpersonal functioning in women with EUPD.
5 Conclusion
Specific Interpersonal problems seem to be associated with cumulative lifetime violence burden among suicidal women with EUPD. These interpersonal traits may serve as key targets for treatment and suicide prevention.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Committee for Ethical Research at Karolinska Institutet (Dnrs: 95–283; 2021-06929-01). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
FG: Writing – original draft, Writing – review & editing. AD: Writing – original draft, Writing – review & editing. AW: Writing – original draft, Writing – review & editing. MN: Writing – original draft, Writing – review & editing. MS: Writing – original draft, Writing – review & editing. MÅ: Writing – original draft, Writing – review & editing. JJ: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. Funding for this study was provided by the Swedish Research Council (Project numbers: 5454 (MÅ); K2009–61P-21304-04-4 (JJ); K2009-61X-21305-01-1 (JJ)) and through a regional agreement between Umeå University and Västerbotten County Council (ALF)(JJ) and by grants provided by the Stockholm County Council (ALF)(JJ).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1646158/full#supplementary-material
References
1. APA American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th Edition. Washington, D.C.: American Psychiatric Association Publishing (2013).
2. Kjær JNR, Biskin R, Vestergaard C, and Munk JRP. All-cause mortality of hospital-treated borderline personality disorder: A nationwide cohort study. J Pers Disord. (2020) 34:723–35. doi: 10.1521/pedi_2018_32_403
3. Leichsenring F, Leibing E, Kruse J, New AS, and Leweke F. Borderline personality disorder. Lancet. (2011) 377:74–84. doi: 10.1016/s0140-6736(10)61422-5
4. Euler S, Nolte T, Constantinou M, Griem J, Montague PR, and Fonagy P. Interpersonal problems in borderline personality disorder: associations with mentalizing, emotion regulation, and impulsiveness. J Pers Disord. (2021) 35:177–93. doi: 10.1521/pedi_2019_33_427
5. Rajalin M, Hirvikoski T, Renberg ES, Åsberg M, and Jokinen J. Exposure to early life adversity and interpersonal functioning in attempted suicide. Front Psychiatry. (2020) 11:552514. doi: 10.3389/fpsyt.2020.552514
6. Rajalin M, Hirvikoski T, Salander Renberg E, Åsberg M, and Jokinen J. Family history of suicide and interpersonal functioning in suicide attempters. Psychiatry Res. (2017) 247:310–4. doi: 10.1016/j.psychres.2016.11.029
7. Jokinen J, Forslund K, Ahnemark E, Gustavsson JP, Nordström P, and Asberg M. Karolinska Interpersonal Violence Scale predicts suicide in suicide attempters. J Clin Psychiatry. (2010) 71:1025–32. doi: 10.4088/JCP.09m05944blu
8. Sinai C, Hirvikoski T, Nordström AL, Nordström P, Nilsonne Å., Wilczek A, et al. Thyroid hormones and adult interpersonal violence among women with borderline personality disorder. Psychiatry Res. (2015) 227:253–7. doi: 10.1016/j.psychres.2015.03.025
9. Chow RTS, Yu R, Geddes JR, and Fazel S. Personality disorders, violence and antisocial behaviour: updated systematic review and meta-regression analysis. Br J Psychiatry. (2024) 227:1–11. doi: 10.1192/bjp.2024.226
10. Salzer S, Streeck U, Jaeger U, Masuhr O, Warwas J, Leichsenring F, et al. Patterns of interpersonal problems in borderline personality disorder. J Nerv Ment Dis. (2013) 201:94–8. doi: 10.1097/NMD.0b013e3182532b59
11. Zaboli G, Gizatullin R, Nilsonne A, Wilczek A, Jönsson EG, Ahnemark E, et al. Tryptophan hydroxylase-1 gene variants associate with a group of suicidal borderline women. Neuropsychopharmacology. (2006) 31:1982–90. doi: 10.1038/sj.npp.1301046
12. First MB, Gibbon M, Spitzer RL, Williams JBW, and Benjamin LS. Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II). Washington, D.C.: American Psychiatric Press, Inc. (1997).
13. Ottosson H, Bodlund O, Ekselius L, Knorring L, Kullgren G, Lindström E, et al. The DSM-IV and ICD-10 personality questionnaire (DIP-Q): Construction and preliminary validation. Nordic J Psychiatry. (1995) 49:285–92. doi: 10.3109/08039489509011918
14. APA American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, D.C: American Psychiatric Publishing (1994).
15. Horowitz LM, Rosenberg SE, Baer BA, Ureño G, and Villaseñor VS. Inventory of interpersonal problems: psychometric properties and clinical applications. J Consult Clin Psychol. (1988) 56:885–92. doi: 10.1037//0022-006x.56.6.885
16. Weinryb RM, Gustavsson JP, Hellström C, Andersson E, Broberg A, and Rylander G. Interpersonal Problems and personality characteristics: Psychometric studies of the Swedish version of the IIP. Pers Individ Dif. (1996) 20:13–23. doi: 10.1016/0191-8869(95)00137-U
17. Alden LE, Wiggins JS, and Pincus AL. Construction of circumplex scales for the Inventory of Interpersonal Problems. J Pers Assess. (1990) 55:521–36. doi: 10.1080/00223891.1990.9674088
18. Buss AH and Durkee A. An inventory for assessing different kinds of hostility. J Consult Psychol. (1957) 21:343–9. doi: 10.1037/h0046900
19. Foulds GA, Caine TM, Adams A, and Owen A. Personality and Personal Illness. London: Tavistock Publications London (1965).
20. Fishbein DH, Lozovsky D, and Jaffe JH. Impulsivity, aggression, and neuroendocrine responses to serotonergic stimulation in substance abusers. Biol Psychiatry. (1989) 25:1049–66. doi: 10.1016/0006-3223(89)90293-x
21. Harford TC, Chen CM, Kerridge BT, and Grant BF. Borderline personality disorder and violence toward self and others: A national study. J Pers Disord. (2019) 33:653–70. doi: 10.1521/pedi_2018_32_361
22. Goldbach RE, Neukel C, Panizza A, Reinken A, and Krause-Utz A. Differentiating between intrapsychic symptoms and behavioral expressions of borderline personality disorder in relation to childhood emotional maltreatment and emotion dysregulation: an exploratory investigation. Eur J Psychotraumatol. (2023) 14:2263317. doi: 10.1080/20008066.2023.2263317
23. Stepp SD, Smith TD, Morse JQ, Hallquist MN, and Pilkonis PA. Prospective associations among borderline personality disorder symptoms, interpersonal problems, and aggressive behaviors. J Interpers Violence. (2012) 27:103–24. doi: 10.1177/0886260511416468
Keywords: emotionally unstable personality disorder, women, suicide attempt, suicide, victims of violence, perpetrators of violence, interpersonal problems, childhood trauma
Citation: Gustafsson F, Boström AD, Wilczek A, Naesström M, Rajalin M, Åsberg M and Jokinen J (2025) Accumulated lifetime violence load and interpersonal problems among suicidal women with emotionally unstable personality disorder. Front. Psychiatry 16:1646158. doi: 10.3389/fpsyt.2025.1646158
Received: 12 June 2025; Accepted: 13 August 2025;
Published: 28 August 2025.
Edited by:
Francesca Strappini, Foro Italico University, ItalyReviewed by:
Massimiliano Beghi, Azienda Unità Sanitaria Locale (AUSL) della Romagna, ItalyMaría Isabel Perea González, Sevilla University, Spain
Copyright © 2025 Gustafsson, Boström, Wilczek, Naesström, Rajalin, Åsberg and Jokinen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fredrik Gustafsson, RnJlZHJpay5ndXN0YWZzc29uQHVtdS5zZQ==