 Alexandre Hudon1,2,3,4,5*
Alexandre Hudon1,2,3,4,5* Jean-Philippe Cloutier-Tanguay6
Jean-Philippe Cloutier-Tanguay6 Joshua Levy1
Joshua Levy1 William Dastous-Stampe1
William Dastous-Stampe1 Marie-Louise Daigneault7Cédric Lacombe1,2
Marie-Louise Daigneault7Cédric Lacombe1,2 François Noël1,2Stéphanie Borduas Pagé1,2
François Noël1,2Stéphanie Borduas Pagé1,2- 1Department of Psychiatry and Addictology, Faculty of Medicine, Université de Montréal, Montréal, QC, Canada
- 2Department of Psychiatry, Institut Universitaire en Santé Mentale de Montréal, Montréal, QC, Canada
- 3Centre de Recherche de l’Institut Universitaire en Santé Mentale de Montréal, Montréal, QC, Canada
- 4Department of Psychiatry, Institut National de Psychiatrie Légale Philippe-Pinel, Montréal, QC, Canada
- 5Groupe Interdisciplinaire de Recherche sur la Cognition et le Raisonnement Professionnel (GIRCoPRo), Université de Montréal, Montréal, QC, Canada
- 6Department of Psychiatry, Faculty of Medicine, Université Laval, Québec, QC, Canada
- 7Department of Family and Emergency Medicine, Faculty of Medicine, Université de Montréal, Montréal, QC, Canada
Objective: Substance use during psychiatric hospitalization compromises safety, treatment engagement, and post-discharge outcomes, but practical guidance for ward staff remains limited. This scoping review mapped the peer-reviewed literature on how psychiatric inpatient units detect, manage, and respond to alcohol or drug use that occurs on the ward itself, and summarized the effectiveness and breadth of reported strategies.
Methods: The review followed the PRISMA-ScR framework. PubMed, Embase, PsycINFO, and Google Scholar were searched from inception to April 2025 using controlled vocabulary and free-text terms for substance use, psychiatric inpatients, and management strategies. English- and French-language empirical studies, quality-improvement reports, policy evaluations, and scoping reviews were eligible if they described an intervention or protocol applied in an inpatient psychiatric setting. Reviewers independently screened titles/abstracts and full texts extracted data with a standardized spreadsheet, and applied Joanna Briggs Institute critical-appraisal tools.
Results: From the identified studies, 18 studies met inclusion criteria: 1 randomized trial, 3 quasi-experimental reports, 8 descriptive prevalence/cross-sectional studies, 2 policy case studies, 3 reviews/chapters, and 1 commentary. Seven recurring intervention domains were identified: systematic screening (n = 9 studies), brief motivational interventions, policy / protocol development, environmental or security measures, harm reduction strategies, staff training and culture change, and discharge planning. Structured screening improved detection rates up to two-fold; brief interventions such as SBIRT and BIMI increased post-discharge treatment engagement and reduced 30-day readmissions by up to 18%. Zero-tolerance security measures showed inconsistent effects on contraband entry or aggression. Overall methodological quality was moderate, with most evidence derived from single-site implementations.
Conclusions: Existing evidence suggests that standardized screening, ward-adapted brief interventions, clear patient-centered policies, and targeted harm-reduction measures can feasibly improve management of inpatient substance use, while purely punitive security tactics are insufficient. Research gaps include rigorous multi-site evaluations, adolescent and forensic settings, and integrated harm-reduction protocols for substances other than nicotine.
1 Introduction
Substance use and mental health disorders intersect in complex, bidirectional ways that challenge clinicians and policymakers alike. Large epidemiologic surveys show that mood or anxiety disorders approximately double the odds of meeting criteria for a substance-use disorder, underscoring the scale of the problem across community samples (1, 2). Recent work in neurosciences suggests that overlapping neurobiological circuits (particularly those governing reward salience and stress responsivity) create shared vulnerability, helping to explain why nearly half of adults entering treatment for addiction also meet criteria for another psychiatric diagnosis (3). Longitudinal data indicate that early-onset internalizing conditions markedly elevate later risk for nicotine, alcohol, and illicit-drug dependence, even after controlling for sociodemographic factors (4). Alcohol illustrates the bidirectionality: heavy drinking can precipitate depressive episodes while existing depression predicts escalation from hazardous to dependent use (5). The cannabis–psychosis link is similarly reciprocal; frequent high-potency consumption accelerates transition to first-episode psychosis, but psychotic disorders themselves are associated with higher rates of continued cannabis use and relapse (6). Comorbidity also complicates clinical trajectories: benzodiazepine misuse in anxiety or post-traumatic stress disorders is associated with poorer functional outcomes and greater healthcare utilization while co-occurring alcohol or drug misuse predicts lower adherence to antidepressants and mood stabilizers (7, 8). Nonetheless, recovery research highlights protective factors, often termed “recovery capital”, that buffer relapse and psychiatric recurrence, including stable housing, social support, and engagement in mutual-help groups (9). Harm-reduction frameworks further emphasize that partial improvements (such as nicotine-replacement therapy for smokers with schizophrenia) can yield measurable gains in cognition and quality of life even when abstinence is not immediately attainable (10). Contemporary translational models therefore call for integrated, stage-matched interventions that address neurocognitive deficits, social disadvantage, and psychiatric symptom burden in tandem (11).
International guidelines increasingly endorse a multifaceted approach to substance-use disorders (SUDs), combining evidence-based pharmacotherapies with psychosocial and harm-reduction interventions across the continuum of care (12–14). For opioid, alcohol, and nicotine use disorders, first-line treatments and preventive strategies are now well established in community and outpatient settings (15, 16). However, much less guidance exists on how to adapt these interventions for psychiatric inpatient units, where patients may be acutely unwell, pharmacologic regimens are often interrupted, and patterns of substance use differ. Screening and brief interventions are promoted as preventive services, but their implementation on psychiatric wards remains inconsistent, and few studies have addressed how best to manage co-occurring psychiatric and substance-use disorders during hospitalization itself (17). This demonstrates the need for unit-level protocols that can bridge evidence-based addiction care with the realities of acute psychiatric treatment.
Although inpatient psychiatric wards routinely report that between one-quarter and one-half of service users drink alcohol or use illicit drugs while admitted, authoritative guidance on how staff should respond remains strikingly sparse (18). National frameworks for SUDs (such as the Royal College of Psychiatrists’ quality standards or WHO’s Mental Health Gap Action Programme) devote only brief sidebars to acute-care settings and focus primarily on discharge planning rather than real-time use on the ward (19, 20). Most institutions therefore default to zero-tolerance rules that rely on random searches, yet observational audits show these measures neither prevent entry of substances nor reduce subsequent aggression (21, 22). Brief-intervention models such as Screening, Brief Intervention, and Referral to Treatment (SBIRT) have been tested in emergency departments but have not been adapted to locked or restricted-entry wards, leaving uncertainty about staffing ratios, confidentiality, and capacity to obtain informed consent from acutely unwell patients (23, 24). Similarly, contingency-management approaches have never been evaluated behind ward doors, largely due to ethical concerns about “rewarding” patients in coercive environments (25). In the absence of evidence-based direction, nurses report using ad-hoc strategies that vary by shift and rely on personal comfort levels, contributing to inconsistent practice and patient perceptions of arbitrariness (26). This gap highlights a need for consensus-driven protocols and high-quality implementation studies that address the unique legal, ethical, and clinical complexities of concurrent substance use and mental health problems occurring inside psychiatric hospitals.
This scoping review aims to identify the existing evidence on how psychiatric inpatient wards recognize and handle alcohol or drug use that occurs during admission. Specifically, the review will describe the types of strategies and note where these have been applied and what outcomes were recorded. A secondary objective is to outline practical, low-burden recommendations that emerge from the literature. These suggestions are intended as starting points for local quality-improvement efforts and to highlight areas where more focused research would be valuable.
2 Methods
2.1 Search strategies
A comprehensive search strategy was developed to identify studies addressing the management of substance use within psychiatric inpatient settings. Four electronic databases were searched from their inception through April 2025: PubMed (MEDLINE), Embase, PsycINFO, and the Google Scholar search engine. Search strategies combined controlled vocabulary terms (e.g., MeSH, Emtree, APA Thesaurus) with free-text keywords related to substance use and misuse (e.g., “substance use disorder,” “alcohol abuse,” “drug misuse”), psychiatric inpatient care (e.g., “psychiatric ward,” “mental health inpatient,” “locked unit”), and management or intervention strategies (e.g., “treatment,” “SBIRT,” “harm reduction,” “policy,” “discharge planning”). Boolean operators were used to combine concepts across the three core domains, and additional syntax refinements were applied in each database to optimize retrieval. The search strategy was iteratively refined in consultation with a health sciences librarian specialized in psychiatry and addiction medicine. No geographic or setting restrictions were applied. Only studies published in English or French were eligible. Reference lists of included articles and relevant reviews were manually screened to identify additional studies. The final search results were de-duplicated and screened in Rayyan by two reviewers independently, with discrepancies resolved through consensus. The complete database-specific search strings are presented in Supplementary Material. The Preferred Reporting Items for Systematic reviews and Meta-Analyses adapted for Scoping Review checklist (PRISMA-SRc) is also found in the provided Supplementary Material. This study was not registered.
2.2 Study eligibility
Studies were considered eligible if they examined the detection, management, intervention, or policy response to substance use or SUDs within psychiatric inpatient settings. Eligible settings included general adult psychiatric wards, adolescent psychiatric units, forensic psychiatric hospitals, emergency or brief-stay psychiatric beds, and specialized mental health in-patient programs. Also, eligible study designs included empirical research (quantitative, qualitative, or mixed-methods), quality-improvement projects, implementation studies, clinical audits, policy evaluations, and scoping reviews. To be included, studies needed to report on specific management strategies, such as structured screening (e.g., urine toxicology, drug screening questionnaires), brief interventions (e.g., SBIRT), harm-reduction measures (e.g., e-cigarettes, take-home naloxone), discharge planning, staff training, or unit-level policy implementation. Articles were required to include information on intervention design, implementation process, reported outcomes, or contextual barriers and facilitators. Considering the small amounts of studies on the topic, commentaries and perspectives were also included. Only publications available in English or French and published from inception of the databases onward were included.
Exclusion criteria encompassed studies focused exclusively on outpatient, community-based, or emergency department populations, unless psychiatric inpatients were explicitly included. Articles that described substance use solely as a background risk factor (without addressing detection or management) were excluded. Studies conducted in non-psychiatric hospital settings (e.g., internal medicine or surgical wards) were excluded unless they involved embedded psychiatric services. Other exclusions included single case reports, and papers without available full text. These criteria were established prior to screening and applied consistently during the title/abstract and full-text review phases.
2.3 Data extraction
Data extraction was performed using a structured Excel spreadsheet (Microsoft 365 version). For each included study, the following variables were charted (1): Author(s), year, and country (2), Sample population, including setting, sample size, and clinical context (3); Type of psychiatric inpatient unit (e.g., general adult, adolescent, forensic, brief-stay) (4); Substances examined, detailing the types of substance use addressed (e.g., alcohol, cannabis, opioids, nicotine) (5); Description of how substance use was addressed, including management strategies, screening tools, brief interventions, harm-reduction approaches, and institutional policies (6); Description of how substance use was problematic, as reported by the study (e.g., interference with care, safety concerns, diagnostic challenges) (7); Main outcomes, such as changes in detection rates, treatment engagement, readmissions, or policy impact; and (8) Main conclusions or implications drawn by the authors. Data extraction was conducted by one reviewer and verified by a second to ensure completeness and accuracy. Discrepancies were resolved through discussion. Discrepancies at both the title/abstract and full-text screening stages were resolved through discussion between the two primary reviewers. If consensus could not be reached, a third reviewer was consulted to adjudicate. This same process was applied during data extraction and quality appraisal to ensure accuracy and consistency.
2.4 Data analysis
During the synthesis phase, the research team conducted an inductive thematic grouping of the extracted interventions and policies. Through iterative review and consensus discussions, seven core domains were identified that reflect the principal areas of ward-level practice described in the literature (screening, brief interventions, policy frameworks, environmental and security measures, harm reduction, smoke-free strategies, and staff training/continuity of care). These domains were used to structure the summary table and guide the narrative synthesis.
2.5 Quality assessment
A structured quality appraisal was conducted to provide an overview of the methodological aspects and transparency of included studies. Each study was assessed using the Joanna Briggs Institute (JBI) critical appraisal checklists, selected based on study design (27). The JBI tools for randomized controlled trials, quasi-experimental studies, prevalence studies, qualitative research, text and opinion papers, and scoping reviews were applied as appropriate. Quality appraisal focused on elements such as clarity of research objectives, sampling procedures, validity of measurement tools, transparency in intervention description, and appropriateness of analytical methods. Two reviewers independently assessed each study, with disagreements resolved through discussion and consensus. No studies were excluded based on quality assessment; rather, appraisal findings were used to contextualize the strength and consistency of the evidence base across study types.
3 Results
3.1 Description of the identified studies
This scoping review examined published literature on the management of substance use within psychiatric inpatient units. A total of 4389 records were identified through comprehensive database searching, including PubMed (n = 1308), PsycINFO (n = 7), Embase (n = 64), and Google Scholar (n = 2010). After removing 1278 duplicates, 3389 unique records were screened by title and abstract. Of these, 3211 were excluded for not meeting the inclusion criteria. Full-text assessment was conducted for 178 studies. Following detailed review, 160 articles were excluded for the following reasons: focus on outpatient or community-based populations (n = 81), discussion of substance use only as a risk factor without management components (n = 69), or focus on interventions outside of psychiatric hospital settings (n = 10). Ultimately, 18 studies were included for analysis. The complete PRISMA flow diagram is presented in Figure 1. These studies represent a diverse body of literature, including randomized trials, quality-improvement reports, prevalence surveys, and hospital policy evaluations. Notably, most interventions were implemented in general adult psychiatric wards, although a few targeted adolescent or specialized brief-stay units. Approaches to managing substance use varied widely, including structured screening (e.g., urine toxicology, questionnaires), motivational interventions, policy reforms, and harm-reduction practices. Table 1 provides a detailed overview of each included study.
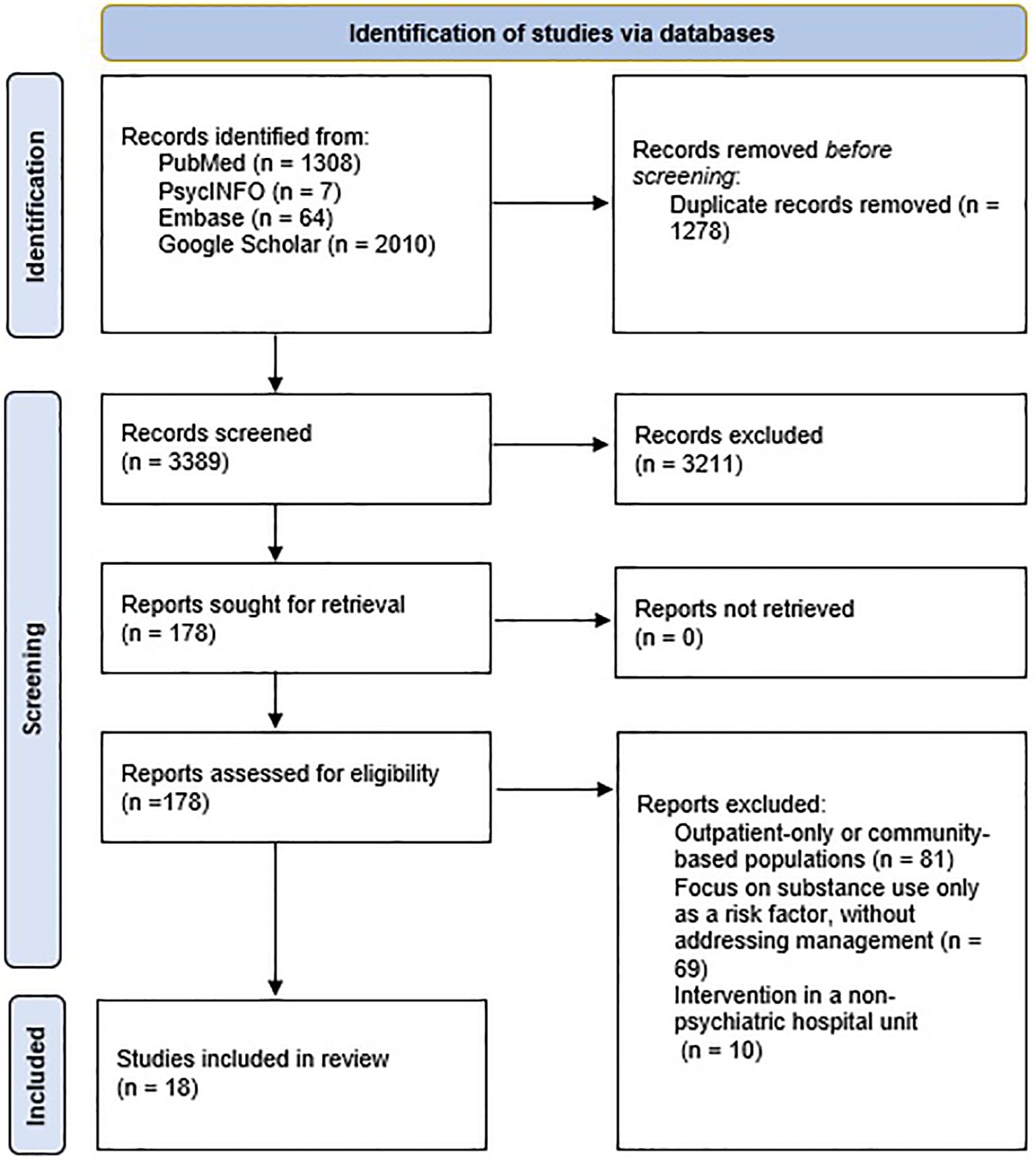
Figure 1. Flow diagram for the identification of studies.
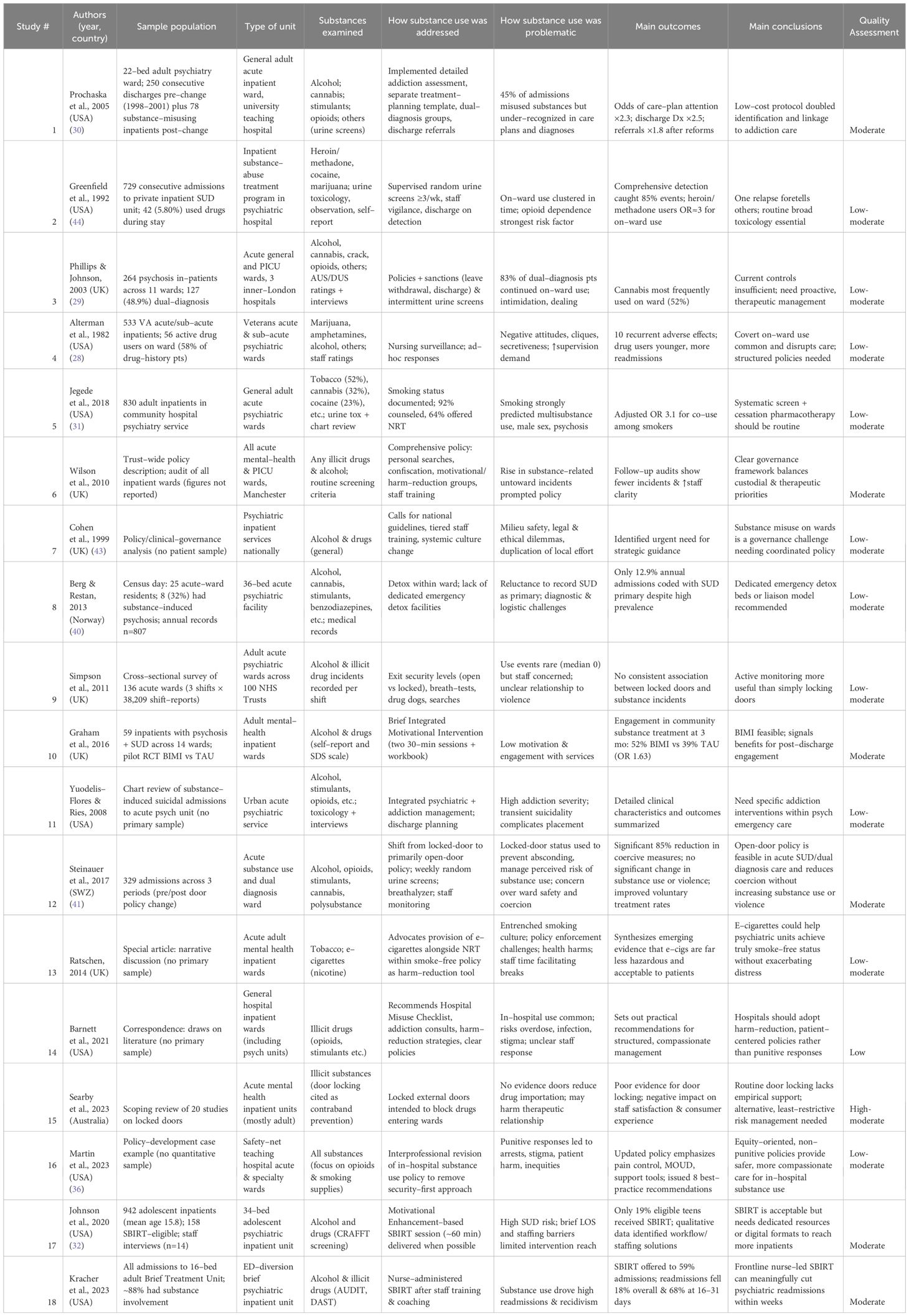
Table 1. Identified studies and detailed analysis.
3.2 Main themes
Seven themes, mapped as intervention domains, were identified across the 18 studies. Figure 2 outlines the number of studies found for each intervention domain. Each domain will be presented underneath to understand its key points and potential use and benefits.
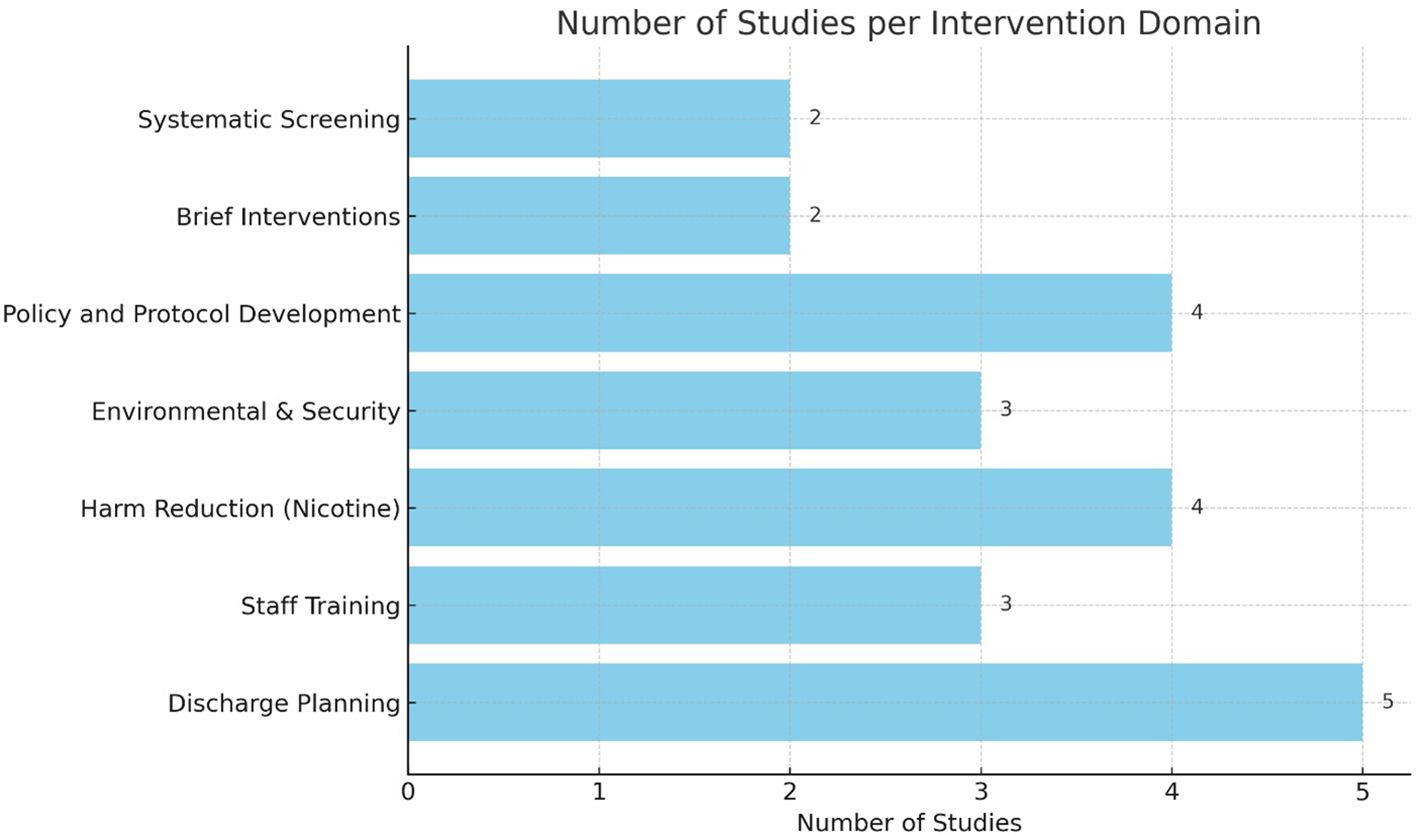
Figure 2. Number of studies identified per intervention domain.
3.2.1 Systematic screening & identification
A consistent message across the identified studies is that effective management begins with universal, structured case-finding at (and throughout) admission. Older prevalence studies (e.g., Alterman et al., 1982; Phillips et al., 2003) relied on clinician judgment and ad-hoc urine testing, but more recent work shows the benefit of formal tools such as the Alcohol Use Disorders Identification Test (AUDIT), Drug Abuse Screening Test (DAST), CRAFFT Screening Test for Adolescent Substance Use (CRAFFT), or single-question screeners embedded in the electronic chart (28, 29). Prochaska and colleagues demonstrated that adding a brief, algorithm-driven intake checklist doubled the proportion of in-patients whose substance use was recognized in care plans and discharge documents, while Jegede showed that routine urine toxicology uncovered polysubstance use in more than half of admissions (information that would otherwise have been missed) (30, 31). Adolescent services face unique challenges: Johnson et al. found that CRAFFT screening identified 158 at-risk youths in a single year, but time constraints meant that only one in five ultimately received an intervention, underscoring the need for streamlined digital or nurse-led workflows (32). At a systems level, the Joint Commission’s Hospital Based Inpatient Psychiatric Services (HBIPS-1) quality indicator now requires documented substance-use screening on every U.S. psychiatric admission, providing both an incentive and a benchmark for compliance monitoring. Together, these findings argue for standardized, auditable screening pathways, ideally hard-wired into admission orders and repeated after periods of leave or changes in mental state, to convert detection from a discretionary act into a routine standard of care.
3.2.2 Brief interventions & integrated therapeutic care
Once substance use is detected, the evidence favors brief, motivationally oriented interventions delivered on the ward and linked to post-discharge care. The pilot RCT by Graham et al. showed that a two-session Brief Integrated Motivational Intervention (BIMI) increased engagement with community addiction services from 39% to 52% three months post-discharge (33). In parallel, nurse-administered SBIRT programs have gained traction: Kracher et al. reported SBIRT uptake in 59% of admissions and an 18% reduction in readmissions within a month, while Johnson et al. confirmed its feasibility in adolescents despite staffing hurdles (32, 34). These programs are most effective when embedded in a broader dual-diagnosis model. For example, Prochaska et al., paired structured assessment with daily group therapy and dedicated discharge planning, doubling documentation of substance-related goals (30). The common elements across successful initiatives include: (a) a manualized, 10- to 60-minute counseling protocol grounded in motivational interviewing; (b) rapid referral pathways to community or hospital-based addiction specialists; and (c) routine outcome tracking (e.g., readmissions, engagement rates) to drive quality-improvement cycles. Ward teams therefore benefit from adopting a tiered intervention ladder, starting with bedside brief advice for low-risk users and scaling up to specialist addiction liaison for complex dependence.
3.2.3 Policy & governance frameworks
Empirical work and practice commentaries converge on the idea that clear, equity-oriented written policies are the backbone of sustainable substance-use management. Wilson 2010’s trust-wide guideline combined motivational approaches with explicit search and confiscation procedures, resulting in fewer substance-related incidents and improved staff confidence (35). Martin extended this by rewriting a hospital policy that had relied on security-led enforcement; the new version centered on harm-reduction, medication for opioid-use disorder (MOUD), and staff discretion grounded in trauma-informed care (36). At a national level, NICE Guideline NG58 mandates integrated care planning for co-existing severe mental illness and substance misuse, offering a template that units can adapt (16). Studies emphasize that governance goes beyond paperwork: Williams and Cohen showed that pairing policies with audit-feedback loops (tracking screening rates, incident reports, and patient complaints) creates a virtuous cycle of accountability (37). Importantly, policies should define graduated responses (from supportive counseling to, rarely, legal action) and outline staff roles, documentation standards, and escalation pathways. Where policies are co-produced with patients and community partners, units report greater legitimacy and fewer adversarial interactions, highlighting governance as both a procedural and relational endeavor.
3.2.4 Environmental & security measures
Physical controls remain the most controversial domain. Large multi-ward surveys and the recent scoping review by Searby et al. find no consistent link between locked external doors and reduced on-ward substance use; in fact, door locking may erode therapeutic alliance and staff morale (38, 39). Targeted measures (random breath-tests, urine toxicology, or passive drug-detection dogs) can detect contraband but risk a punitive tone if not paired with rapid therapeutic follow-up. Alterman documented how covert on-ward use created patient cliques and supervision burdens (28). However, Berg and colleagues showed that simply adding detox beds reduced illicit consumption by providing a safe, sanctioned space for withdrawal (40). The emerging consensus favors a least-restrictive, risk-responsive model: searches based on reasonable suspicion rather than blanket policies, locked doors used sparingly and reviewed daily, and environmental cues (visibility lines, staff presence) designed to dissuade dealing without creating a carceral atmosphere. Units implementing such nuanced strategies report stable incident rates, lower seclusion use, and better patient satisfaction, suggesting that environmental measures work best when they support (not substitute for) therapeutic engagement. Similarly, Steinauer and colleagues reported that shifting from locked to primarily open doors on a substance use and dual diagnosis ward led to a significant 85% reduction in coercive measures, without any increase in substance use or violence, further challenging assumptions that door-locking policies are necessary for safety or substance control (41).
3.2.5 Harm-reduction
An increasing number of inpatient units are adopting harm-reduction approaches for substances other than tobacco. For example, Martin details protocols that provide take-home naloxone, initiate MOUD during admission, and allow patients to store vaping devices (36). Barnett et al. proposes safe-use kits and no-punish frameworks for patients who disclose in-hospital drug use, arguing that punitive responses drive concealment and overdose risk (42). On the alcohol front, some units have implemented symptom-triggered benzodiazepine tapers and monitored consumption agreements rather than zero-tolerance bans, reporting fewer withdrawal complications. These initiatives seek to mitigate risks associated with ongoing substance use during hospitalization, aligning inpatient practice with broader public-health trends in harm reduction.
3.2.6 Staff training & culture change
Technical protocols are difficult to apply without a workforce that is both skilled and philosophically aligned with integrated care. Early ethnographic work revealed cultures of “us versus them,” where substance-using patients were judged more than helped (28, 43). Contemporary programs address this through multidisciplinary training, reflective practice, and ongoing coaching. Wilson and colleagues embedded an annual competency package covering motivational interviewing, trauma-informed search techniques, and de-escalation; staff surveys documented improved confidence and a 20% drop in incident reports (35). Kracher et al. paired SBIRT roll-out with bedside mentorship, finding that sustained coaching, rather than one-off workshops, predicted intervention fidelity (34). Senior-management ownership and peer champions are repeatedly cited as catalysts for shifting norms from rule enforcement to therapeutic alliance. Measuring culture is equally important: many trusts now incorporate staff attitudes toward dual diagnosis into routine dashboards, signaling that culture change, like any outcome, is audited, resourced, and rewarded.
3.2.7 Discharge planning & continuity of care
Inpatient success is fragile without seamless hand-off to community addiction services. Prochaska et al. and Graham et al. (both link structured discharge plans (and explicit substance-use referrals) to higher engagement rates and lower early readmissions (30, 33). Greenfield et al. showed that detecting on-ward relapse, coupled with a clear aftercare contract, mitigated the clustering of post-discharge use episodes (44). Nurse-led SBIRT models of Kracher et al. now include warm hand-offs to peer recovery coaches and digital reminders, achieving up to a 68% reduction in 16–31-day readmissions (34). Effective plans share three traits (1): documented linkage (appointment date/time or e-referral confirmation) (2), patient-centered goal-setting that integrates mental-health and addiction priorities, and (3) follow-up accountability, whether by community teams, virtual check-ins, or text-based support. Emerging digital solutions (secure messaging, tele-SBIRT) show promise for bridging the important first two weeks after discharge, a window repeatedly flagged as high-risk for relapse or overdose. Embedding these elements transforms discharge from an administrative act into a continuum of care that maintains therapeutic momentum beyond the ward.
3.3 Quality appraisal
Using the JBI suite of critical-appraisal tools matched to each study, the overall evidence base is moderate. The lone randomized study of Graham et al. met seven of thirteen RCT criteria, earning moderate quality: random-sequence generation and baseline comparability were clear, but allocation concealment, blinding, and power calculations were absent, and follow-up was under 80% (33). The three quasi-experimental or quality-improvement reports scored between six and eight on the nine-item checklist, also achieving a moderate rating: they provided clearly defined interventions, multiple pre-post measures, and parallel controls or statistical adjustments, but relied on convenience samples and were susceptible to history effects (30–32, 34). Among the seven descriptive prevalence or cross-sectional studies, half satisfied six to eight JBI reporting standardized measures, transparent inclusion criteria, and more than 80% participation, while the remainder lacked probability sampling or had substantial missing data, yielding low-to-moderate ratings (28, 29, 31, 38, 40, 44, 45). The two policy/governance case studies and the Lancet Psychiatry commentary were appraised with JBI’s “text and opinion” checklist: both policy papers articulated clear positional statements supported by referenced evidence and stakeholder consultation (scoring 4/6, moderate), whereas the commentary was more impressionistic (3/6, low) (35, 36, 42). The Searby et al. scoping review scored nine out of eleven criteria on the JBI comprehensive search strategy checklist, duplicate selection, and transparent charting, but did not register a protocol or appraise included evidence, so quality was classed as high-moderate (39). Finally, the earlier governance met only three out of the six applicable criteria (unclear search methods, unstructured synthesis), thus low quality (43). In sum, about one-third of the identified study are moderate-to-high quality. As a general appraisal, the field is limited by small samples, single-site designs, and often descriptive aims.
4 Discussion
4.1 Findings and comparison with prior works
The present scoping review identified 18 empirical and practice-oriented publications that describe how psychiatric wards attempt to detect, manage, or otherwise respond when patients consume alcohol or drugs during admission. Most studies originated from high-income countries and focused on general adult units; only a handful examined adolescent, forensic, or brief-stay settings. Seven broad management domains were identified: systematic screening, brief motivational care, policy and governance frameworks, environmental or security measures, harm-reduction initiatives, staff training and culture change, and discharge linkage. Many studies are descriptive, small-scale, or limited to single-site quality improvement efforts, with few rigorous trials or multi-site evaluations. This gap is particularly striking given the contrast between the prevalence of substance use in psychiatric settings and the lack of robust guidance for clinicians. Bridging this gap will require more systematic research efforts, drawing on both quantitative and qualitative methods to inform pragmatic, patient-centered approaches to care. Nevertheless, consistent signals emerged: structured screening improves detection, brief interventions are feasible, and purely punitive security tactics rarely prevents contraband entry or aggression.
One notable finding is the underutilization of structured screening tools in psychiatric settings. While nurse-led screening has proven effective in general hospitals (identifying unhealthy substance use in approximately 16% of patients), psychiatric units often lack standardized protocols (46). Implementing brief screening tools, such as the AUDIT, into routine assessments could enhance early detection and intervention efforts. Harm-reduction approaches, have also shown promise in mental health settings. As an example, despite the implementation of smoke-free policies, tobacco use remains highly prevalent on psychiatric wards, often leading to daily tensions, withdrawal symptoms, and patient agitation due to inconsistent enforcement and limited alternatives. Providing NRT and considering the supervised use of e-cigarettes can help manage withdrawal symptoms during hospitalization, reduce conflict on the ward, and support both patient comfort and adherence to smoke-free regulations (47). More broadly, staff attitudes toward patients with substance use disorders significantly influence care quality. Educational interventions have demonstrated effectiveness in improving nurses’ attitudes and perceptions, leading to more compassionate and effective care (48). Ongoing training and support for healthcare providers are essential to favorize a therapeutic environment conducive to recovery.
Harm-reduction approaches represent a particularly important yet underdeveloped area in this literature. Several studies describe promising ward-level strategies (including safe-use kits, monitored alcohol tapering, naloxone distribution, and permissive frameworks for disclosure) that help mitigate the risks of ongoing substance use during hospitalization (36, 42). However, such practices remain inconsistently implemented and are often hampered by prevailing abstinence-based or punitive ward cultures. A recurring theme across the studies reviewed is that harm reduction is not simply a set of protocols but a shift in clinical mindset: one that requires sustained investment in staff training, ongoing coaching, and reflective practice to be effective. One-time educational sessions alone appear insufficient to embed harm-reduction principles into daily care. Favorizing a culture of compassionate, risk-mitigating engagement (particularly in the face of entrenched stigma toward substance use) is important for improving patient outcomes and bridging the current evidence-practice gap in psychiatric inpatient settings.
From a policy perspective, the findings underscore the need for national and regional mental health frameworks to explicitly address substance use occurring within psychiatric inpatient settings, rather than focusing solely on discharge planning. Incorporating ward-level protocols into accreditation standards, hospital governance audits, and quality indicators could incentivize adoption of evidence-informed strategies. Policies that integrate harm-reduction principles and ensure funding for staff training and screening infrastructure are more likely to achieve sustainable impact. Finally, practical barriers reported included limited staffing, high patient acuity, competing clinical priorities, and restricted ward environments that limit privacy for interventions. Resistance from staff unfamiliar with harm-reduction principles and lack of leadership endorsement were also recurrent challenges. Implementation was more successful where interventions were embedded into routine workflows, supported by leadership, and accompanied by ongoing mentorship rather than one-off training sessions.
4.2 Limitations
This review is not without limitations. Only English- and French-language sources were included, and grey literature beyond peer-reviewed journals was not systematically searched, raising the possibility that effective local protocols remain unpublished. The evidence base itself is skewed toward descriptive reports with small samples; many lacked control groups, standardized outcome measures, or long-term follow-up, limiting confidence in causal inferences. Finally, heterogeneity in unit type, patient mix, and health-system context hindered direct comparison of interventions. These gaps underscore the need for multi-site implementation studies and consensus-building exercises that can translate promising but disparate strategies into coherent, evidence-informed guidance for psychiatric inpatient care. A limitation of the current evidence base is the absence of standardized outcome measures. Across studies, outcomes ranged from detection rates and patient engagement to qualitative staff perceptions, making cross-study comparison difficult. Future work would benefit from a core outcome set for inpatient substance-use interventions, encompassing both clinical (e.g., relapse, readmissions) and process measures (e.g., screening adherence, patient satisfaction). Such standardization would facilitate meta-analyses and guide quality-improvement benchmarks.
4.3 Recommendations
This scoping review highlights several areas where practical, evidence-informed improvements can be made to better manage substance use on psychiatric inpatient units. Recommendations are summarized in Table 2.
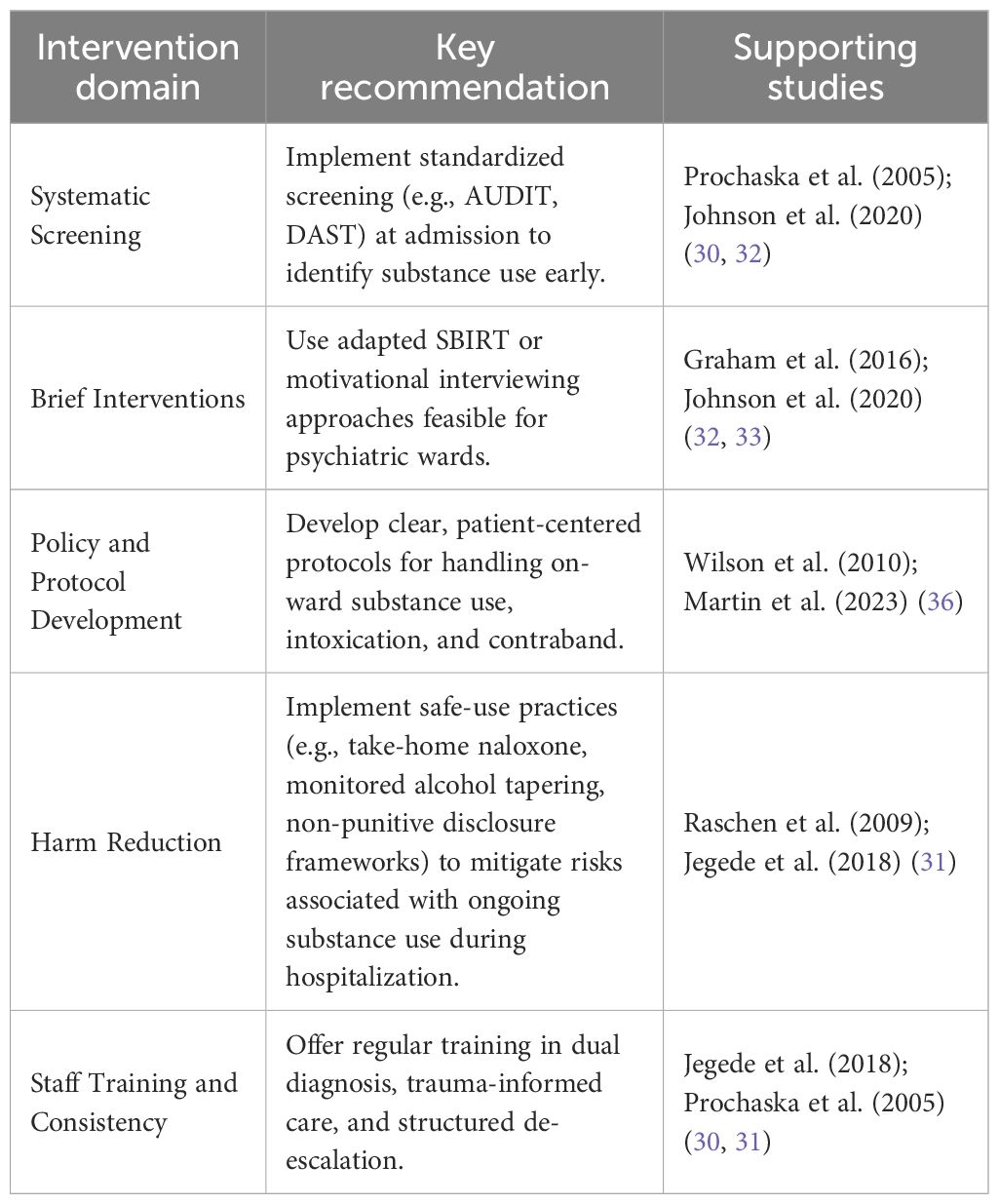
Table 2. Summary of recommendations.
1. The implementation of systematic screening procedures is both feasible and necessary. Several included studies, such as Prochaska et al. and Johnson et al. demonstrated that embedding brief screening tools like AUDIT and DAST at admission can identify substance use early and create an opportunity for timely intervention (30, 32). Where staffing allows, universal screening should be incorporated into routine nursing or medical assessments.
2. Brief motivational interventions tailored to psychiatric inpatients should be expanded. Interventions such as SBIRT, adapted for the ward environment, showed promising acceptability and early impact in adolescent and adult settings (32, 33). Although implementation challenges were reported (such as patient acuity and staff training needs) these approaches were found to be both low-cost and scalable when properly supported.
3. Third, there is a need for clear and consistently applied ward-level policies. Studies underscored the importance of having written protocols for managing suspected on-ward substance use, including guidance on searches, use of breathalyzers, and steps for managing intoxication (35, 36). These policies should be transparent, patient-centered, and include graduated responses rather than purely punitive approaches.
4. In line with harm-reduction principles, several reports recommend the provision of nicotine-replacement therapy and consideration of alternatives such as e-cigarettes in smoke-free psychiatric facilities (31, 45). These measures were associated with improved patient adherence to smoking bans and reduced conflict. While full harm-reduction programs for other substances are not yet widely implemented on inpatient units, these studies highlight a direction for future practice.
5. Finally, ongoing staff education and reflective practice are important to ensure consistent, stigma-free responses to substance use on the ward. Jegede et al. and Prochaska et al. both noted wide variability in how staff respond to substance-related incidents, with some staff expressing uncertainty or moral discomfort (30, 31). Regular training on dual diagnosis, trauma-informed care, and structured de-escalation can support therapeutic consistency and reduce reliance on containment measures. Incorporating principles of culturally safe care and cultural humility is also important, as substance use patterns, stigma, and treatment expectations can vary considerably across cultural groups. Attention to these dimensions can help tailor interventions, favorize trust, and improve engagement among diverse patient populations. Cultural context strongly shapes substance-use patterns, help-seeking behaviors, and perceptions of harm-reduction practices. Adapting interventions for cultural relevance (through co-design with service users, inclusion of culturally specific peer workers, and integration of Indigenous or community-based healing approaches) can improve engagement and trust. This is particularly important in diverse urban psychiatric settings and for Indigenous and minority populations, where historical mistrust of psychiatric institutions may affect intervention uptake.
Resource considerations are very important to implementation. Most strategies identified (such as brief motivational interventions, standardized screening tools, and staff training) are relatively low-cost when integrated into existing workflows, but require initial investment in training and change management. More resource-intensive measures, such as dedicated addiction liaison staff or environmental modifications, may be justified in high-prevalence settings but should be evaluated for cost-effectiveness.
5 Conclusion
This scoping review provides a comprehensive synthesis of the limited body of literature on how psychiatric inpatient units manage substance use that occurs during hospitalization. Although practices vary considerably across settings, the findings reveal several promising strategies. Such strategies include structured screening, brief motivational interventions, clear ward policies, harm-reduction tools, and staff education. These strategies can be feasibly adapted to psychiatric contexts. When implemented thoughtfully, they have the potential to improve detection, enhance therapeutic engagement, reduce conflict, and promote continuity of care after discharge. However, the evidence remains fragmented, methodologically heterogeneous, and heavily reliant on single-site or descriptive reports. Moving forward, there is a pressing need for multi-site implementation studies, consensus-driven protocols, and pragmatic evaluations that reflect the complex realities of psychiatric wards. Strengthening the evidence base in this area will be essential not only to support frontline clinicians but also to help shift away from punitive or control-based responses that risk undermining trust and recovery. Embedding compassionate, harm-reduction-oriented practices into inpatient care is a critical step toward greater alignment with contemporary public health and addiction treatment frameworks. Future research should prioritize multi-site pragmatic trials and hybrid implementation-effectiveness studies that assess both clinical outcomes and contextual determinants of success. Longitudinal designs with standardized outcome sets, inclusion of diverse cultural groups, and cost-effectiveness analyses will be essential. Mixed-methods approaches can capture both quantitative impact and qualitative insights into patient and staff experiences, informing scalable and context-sensitive protocols.
Author contributions
AH: Writing – review & editing, Funding acquisition, Writing – original draft, Supervision, Formal Analysis, Investigation, Data curation, Resources, Project administration, Validation, Methodology, Visualization, Conceptualization. J-PC-T: Methodology, Formal Analysis, Data curation, Investigation, Writing – original draft, Writing – review & editing. JL: Writing – review & editing, Formal Analysis, Data curation, Methodology, Writing – original draft, Investigation. WD-S: Formal Analysis, Data curation, Writing – original draft, Methodology, Investigation, Writing – review & editing. M-LD: Conceptualization, Writing – review & editing, Validation, Investigation, Writing – original draft, Formal Analysis. CL: Writing – original draft, Conceptualization, Validation, Writing – review & editing, Investigation, Formal Analysis. FN: Methodology, Writing – original draft, Conceptualization, Writing – review & editing, Investigation, Formal Analysis, Validation. SB: Methodology, Project administration, Conceptualization, Supervision, Investigation, Formal Analysis, Writing – review & editing, Writing – original draft.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. Indirectly funded by the Fondation de l’Institut universitaire en santé mentale de Montréal and the Fonds d’opérations IVADO of Dr. Alexandre Hudon.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. The author(s) declare that Generative AI was used to proof read this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1653093/full#supplementary-material
References
1. Grant BF, Stinson FS, Dawson DA, Chou SP, Dufour MC, Compton W, et al. Prevalence and co-occurrence of substance use disorders and independent mood and anxiety disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. (2004) 61:807–16. doi: 10.1001/archpsyc.61.8.807
2. Kessler RC, Crum RM, Warner LA, Nelson CB, Schulenberg J, and Anthony JC. Lifetime co-occurrence of DSM-III-R alcohol abuse and dependence with other psychiatric disorders in the National Comorbidity Survey. Arch Gen Psychiatry. (1997) 54:313–21. doi: 10.1001/archpsyc.1997.01830160031005
3. Volkow ND and Blanco C. Substance use disorders: a comprehensive update of classification, epidemiology, neurobiology, clinical aspects, treatment and prevention. World psychiatry: Off J World Psychiatr Assoc (WPA). (2023) 22:203–29. doi: 10.1002/wps.21073
4. Roberts RE, Roberts CR, and Xing Y. Comorbidity of substance use disorders and other psychiatric disorders among adolescents: evidence from an epidemiologic survey. Drug Alcohol Depend. (2007) 88 Suppl 1:S4–S13. doi: 10.1016/j.drugalcdep.2006.12.010
5. Rehm J, Gmel G. E. C.OMMAS.R.X.X.X, Gmel G, Hasan OSM, Imtiaz S, Popova S, et al. The relationship between different dimensions of alcohol use and the burden of disease-an update. Addict (Abingdon England). (2017) 112:968–1001. doi: 10.1111/add.13757
6. Connor JP, Stjepanović D, Le Foll B, Hoch E, Budney AJ, and Hall WD. Cannabis use and cannabis use disorder. Nat Rev Dis Primers. (2021) 7:16. doi: 10.1038/s41572-021-00247-4
7. Lader M. Benzodiazepines revisited–will we ever learn? Addict (Abingdon England). (2011) 106:2086–109. doi: 10.1111/j.1360-0443.2011.03563.x
8. Nunes EV and Levin FR. Treatment of depression in patients with alcohol or other drug dependence: a meta-analysis. JAMA. (2004) 291:1887–96. doi: 10.1001/jama.291.15.1887
9. Kelly JF, Bergman B, Hoeppner BB, Vilsaint C, and White WL. Prevalence and pathways of recovery from drug and alcohol problems in the United States population: Implications for practice, research, and policy. Drug Alcohol Depend. (2017) 181:162–9. doi: 10.1016/j.drugalcdep.2017.09.028
10. Moylan S, Jacka FN, Pasco JA, and Berk M. Cigarette smoking, nicotine dependence and anxiety disorders: a systematic review of population-based, epidemiological studies. BMC Med. (2012) 10:123. doi: 10.1186/1741-7015-10-123
11. Blanco C, Hasin DS, Wall MM, Flórez-Salamanca L, Hoertel N, Wang S, et al. Cannabis use and risk of psychiatric disorders: prospective evidence from a US national longitudinal study. JAMA Psychiatry. (2016) 73:388–95. doi: 10.1001/jamapsychiatry.2015.3229
12. American Society of Addiction Medicine. The ASAM national practice guideline for the treatment of opioid use disorder: 2020 focused update. (2020). Available online at: https://www.asam.org/quality-care/clinical-guidelines/national-practice-guideline (Accessed March 12, 2025).
13. Substance Abuse and Mental Health Services Administration. TIP 63: Medications for opioid use disorder (2021). Available online at: https://store.samhsa.gov/product/TIP-63-Medications-for-Opioid-Use-Disorder-Full-Document/PEP21-02-01-002 (Accessed March 12, 2025).
14. World Health Organization. Guidelines for the pharmacological treatment of opioid dependence. (2016). Available online at: https://www.who.int/publications/i/item/9789241547543 (Accessed March 12, 2025).
15. Canadian Research Initiative in Substance Misuse. National guideline for opioid agonist therapy (2021). Available online at: https://crism.ca/projects/opioid-agonist-therapy-guideline (Accessed March 12, 2025).
16. National Institute for Health and Care Excellence. Coexisting severe mental illness and substance misuse: Assessment and management in healthcare settings (NG58). (2016). Available online at: https://www.nice.org.uk/guidance/ng58 (Accessed March 12, 2025).
17. Preventive Services Task Force US. Screening for unhealthy drug use: U.S. Preventive Services Task Force recommendation statement. JAMA. (2020) 323:2301–9. doi: 10.1001/jama.2020.8020
18. Fazel S, Yoon IA, and Hayes AJ. Substance use disorders in prisoners: an updated systematic review and meta-regression analysis in recently incarcerated men and women. Addict (Abingdon England). (2017) 112:1725–39. doi: 10.1111/add.13877
19. Royal College of Psychiatrists. Co-occurring severe mental illness and substance misuse: Quality improvement guidance. (2017). Available online at: https://www.rcpsych.ac.uk (Accessed March 12, 2025).
20. World Health Organization. International standards for the treatment of drug use disorders (2020). World Health Organization. Available online at: https://www.who.int/publications/i/item/international-standards-for-the-treatment-of-drug-use-disorders (Accessed March 12, 2025).
21. Jaiteh C, Steinauer R, and Frei IA. Individuals with opioid dependence using polysubstances: how do they experience acute hospital care and what are their needs? A qualitative study. J Addict Nurs. (2019) 30:177–84. doi: 10.1097/JAN.0000000000000294
22. Forchuk C, Serrato J, Scott L, Rudnick A, Dickey C, and Silverman M. No Good Choice”: What are the Issues of Having no Harm Reduction Strategies in Hospitals?Substance abuse: research and treatment. 17. (2023) 11782218231186065. doi: 10.1177/11782218231186065
23. McCance-Katz EF and Satterfield J. SBIRT: a key to integrate prevention and treatment of substance abuse in primary care. Am J Addict. (2012) 21:176–7. doi: 10.1111/j.1521-0391.2011.00213.x
24. Karno MP, Rawson R, Rogers B, Spear S, Grella C, Mooney LJ, et al. Effect of screening, brief intervention and referral to treatment for unhealthy alcohol and other drug use in mental health treatment settings: a randomized controlled trial. Addiction. (2021) 116:159–69. doi: 10.1111/add.15114
25. Rash CJ, Stitzer M, and Weinstock J. Contingency management: new directions and remaining challenges for an evidence-based intervention. J Subst Abuse Treat. (2017) 72:10–8. doi: 10.1016/j.jsat.2016.09.008
26. Petersén E, Thurang A, and Berman AH. Staff experiences of encountering and treating outpatients with substance use disorder in the psychiatric context: a qualitative study. Addict Sci Clin Pract. (2021) 16:29. doi: 10.1186/s13722-021-00235-9
27. Munn Z, Barker TH, Moola S, Tufanaru C, Stern C, McArthur A, et al. Methodological quality of case series studies: an introduction to the JBI critical appraisal tool. JBI evidence synthesis. (2020) 18:2127–33. doi: 10.11124/JBISRIR-D-19-00099
28. Alterman AI, Erdlen DL, LaPorte DJ, and Erdlen FR. Effects of illicit drug use in an inpatient psychiatric population. Addictive Behav. (1982) 7:231–42. doi: 10.1016/0306-4603(82)90050-8
29. Phillips P and Johnson S. Drug and alcohol misuse among in-patients with psychotic illnesses in three inner-London psychiatric units. Psychiatr Bull. (2003) 27:217–20. doi: 10.1192/pb.27.6.217
30. Prochaska JJ, Gill P, Hall SE, and Hall SM. Identification and treatment of substance misuse on an inpatient psychiatry unit. Psychiatr Serv. (2005) 56:347–9. doi: 10.1176/appi.ps.56.3.347
31. Jegede O, Ranjith G, and Oyebode F. Managing illicit substance use on psychiatric wards: A survey of U.K. practice. BJPsych Bull. (2018) 42:206–12. doi: 10.1192/bjb.2018.27
32. Johnson SE, Lapomardo A, Thibeau HM, Altemus M, Hunt JI, and Wolff JC. A process evaluation of a substance-use brief intervention for adolescents in a psychiatric inpatient program. Subst Abuse: Res Treat. (2020) 14:1–14. doi: 10.1177/1178221820936666
33. Graham HL, Copello A, Griffith E, Freemantle N, McCrone P, Clarke L, et al. Pilot randomised trial of a brief intervention for comorbid substance misuse in psychiatric in-patient settings. Acta Psychiatrica Scandinavica. (2016) 133:298–309. doi: 10.1111/acps.12530
34. Kracher V and Welsh C. Utilisation of nurse-administered screening and brief intervention in acute psychiatric care. Issues Ment Health Nurs. (2023) 44:120–7. doi: 10.1080/01612840.2022.2137210
35. Wilson I, Holland M, Mason V, Reeve J, and Ash H. The management of substance misuse on psychiatric inpatient wards – A policy to promote effective good practice. Adv Dual Diagnosis. (2009) 2:12–9. doi: 10.5042/add.2010.0098
36. Martin RA, Donovan DM, and Wilsnack S. In-hospital substance-use policies: An opportunity for therapeutic engagement. Hosp Pract. (2023) 51:42–8. doi: 10.1080/21548331.2023.2180459
37. Williams R and Cohen J. Substance use and misuse in psychiatric wards: A model task for clinical governance? Psychiatr Bull. (2000) 24:43–6. doi: 10.1192/pb.24.2.43
38. Simpson A, Bowers L, Haglund K, Muir-Cochrane E, Nijman H, and Wijk H. Substance use and exit security on psychiatric wards: Associations with door-locking, ward-security and other factors. J Advanced Nurs. (2010) 66:513–22. doi: 10.1111/j.1365-2648.2009.05198.x
39. Searby A, Lake A, and Park E. Locked external doors on inpatient mental health units: A scoping review. Int J Ment Health Nurs. (2023) 32:49–63. doi: 10.1111/inm.13035
40. Berg JE and Restan A. Substance abusers in an acute psychiatric facility: A diagnostic and logistic challenge. ISRN Psychiatry. (2013) 2013. doi: 10.1155/2013/705657
41. Steinauer R, Huber CG, Petitjean S, Wiesbeck GA, Dürsteler KM, Lang UE, et al. Effect of door-locking policy on inpatient treatment of substance use and dual disorders. Eur Addict Res. (2017) 23:87–96. doi: 10.1159/000458757
42. Barnett P and Iyegbe C. Pharmacological management of substance misuse in psychiatric inpatients: A narrative review. Lancet Psychiatry. (2021) 8:310–22. doi: 10.1016/S2215-0366(20)30487-9
43. Cohen J, Runciman R, and Williams R. Substance use and misuse in psychiatric wards: A model task for clinical governance. Drugs: Education Prev Policy. (1999) 6:181–94. doi: 10.1080/09687639997924
44. Greenfield SF, Weiss RD, and Griffin ML. Patients who use drugs during inpatient substance-abuse treatment. Am J Psychiatry. (1992) 149:235–9. doi: 10.1176/ajp.149.2.235
45. Ratschen E, Britton J, Doody GA, and McNeill A. Smoke-free policy in acute mental health wards: avoiding the pitfalls. Gen Hosp Psychiatry. (2009) 31:131–6. doi: 10.1016/j.genhosppsych.2008.10.006
46. Roche AM, Freeman T, and Skinner N. From data to evidence, to action: findings from a systematic review of hospital screening studies for high-risk alcohol consumption. Drug Alcohol Depend. (2006) 83:1–14. doi: 10.1016/j.drugalcdep.2005.10.011
47. Lawn S. Cigarette smoking in psychiatric settings: Occupational health, safety, welfare and legal concerns. Aust New Z J Psychiatry. (2005) 39:886–91. doi: 10.1080/j.1440-1614.2005.01698.x
Keywords: psychiatric inpatient, substance use, management, drug screening, harm reduction, brief intervention, policy, dual diagnosis
Citation: Hudon A, Cloutier-Tanguay J-P, Levy J, Dastous-Stampe W, Daigneault M-L, Lacombe C, Noël F and Borduas Pagé S (2025) Managing substance abuse on psychiatric units: a scoping review. Front. Psychiatry 16:1653093. doi: 10.3389/fpsyt.2025.1653093
Received: 24 June 2025; Accepted: 20 October 2025;
Published: 29 October 2025.
Edited by:
Carlos Roncero, University of Salamanca, SpainReviewed by:
Erich Flammer, ZfP Südwürttemberg, GermanyJoan Ignasi Mestre-Pinto, Mar Institute of Medical Research (IMIM), Spain
Copyright © 2025 Hudon, Cloutier-Tanguay, Levy, Dastous-Stampe, Daigneault, Lacombe, Noël and Borduas Pagé. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandre Hudon, YWxleGFuZHJlLmh1ZG9uLjFAdW1vbnRyZWFsLmNh