 André Beyer Mathiassen1,2*
André Beyer Mathiassen1,2* Christoffer Cramer Lundsgaard1,2Krzysztof Gbyl1,2
Christoffer Cramer Lundsgaard1,2Krzysztof Gbyl1,2 Kamilla Miskowiak2,3Birgitte Fagerlund4,5Henrik B. Wiberg Larsson6
Kamilla Miskowiak2,3Birgitte Fagerlund4,5Henrik B. Wiberg Larsson6 Ulrich Lindberg6Poul Videbech1,2
Ulrich Lindberg6Poul Videbech1,2- 1Center for Neuropsychiatric Depression Research, Mental Health Center Glostrup, Copenhagen University Hospital – Mental Health Services CPH, Glostrup, Denmark
- 2Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
- 3Neurocognition and Emotion Across Disorders of the Brain Centre (NEAD), Psychiatric Centre Copenhagen, Frederiksberg, Denmark
- 4Department of Psychology, University of Copenhagen, Copenhagen, Denmark
- 5Child and Adolescent Mental Health Center, Mental Health Services CPH, Copenhagen, Denmark
- 6Functional Imaging Unit, Department of Clinical Physiology and Nuclear Medicine, Copenhagen University Hospital – Rigshospitalet, Copenhagen, Denmark
Background: Electroconvulsive therapy (ECT) may cause anterograde and autobiographical amnesia. Identifying reliable predictive biomarkers for the risk of this memory loss may assist clinicians in their decision to use this treatment. We aimed to investigate whether the baseline volume or the cortical thickness of the predetermined regions of interest (ROIs) involved in memory recall is correlated with the degree of amnesia after ECT.
Method: In this longitudinal study, we followed 19 inpatients receiving ECT for depression. Using 3-T MRI, we performed structural brain scans prior to ECT. We also assessed the autobiographical, verbal, and visual anterograde memory both before and after ECT. We conducted one-sided partial correlation analyses between the volume or the cortical thickness of the ROIs at baseline and the memory decline following ECT (ClinicalTrials.gov: NCT04160286).
Results: As hypothesized, a larger baseline cortical thickness of the right parahippocampal gyrus (r = 0.517, p = 0.014) and the left ventrolateral prefrontal cortex (r = 0.530, p = 0.012) correlated with less ECT-related decline in autobiographical memory, respectively explaining 26.7% and 28.1% of the variance. Unexpectedly, a smaller volume of the right hippocampus also correlated with less autobiographical memory decline (r = −0.416, p = 0.048). None of the ROIs predicted anterograde memory impairment.
Conclusion: These early findings suggest that a pre-ECT neural reserve in the brain regions subserving memory might act protectively against the development of autobiographical memory loss after ECT. If replicated in larger samples, our findings may have promising clinical implications as a structural MRI scan prior to ECT might contribute to determining the individual risk of autobiographical memory loss following ECT.
1 Introduction
Electroconvulsive therapy (ECT) is remarkably effective in the treatment of severe uni- and bipolar depression (1) and is widely used across the globe (2, 3). Unfortunately, ECT is associated with anterograde and retrograde (autobiographical) amnesia, which may be severe in some cases (4–6). Therefore, the ability to predict such side effects prior to treatment initiation would be highly valuable in the clinical setting as it would enable clinicians to identify patients at high risk of developing adverse amnesic effects following ECT. This may facilitate the shared decision-making between patients, their relatives, and their physician.
The concept of brain reserve refers to the observation that larger brains tolerate more detrimental effects before cognitive impairment emerges (7, 8). Brain reserve has been found to be protective against cognitive impairment in relation to various pathological brain changes, including traumatic brain injury (8), multiple sclerosis (9), and Alzheimer’s disease (7). Brain volume and cortical thickness are considered direct measures of such brain reserve (10). Retrograde memory recall has been found to be positively correlated with the cortical thickness of the brain regions important for autobiographical memory function (11). These observations are further substantiated by functional imaging studies that found the activation of these and other pertinent regions to be correlated with autobiographical memory recall. Specifically, the recall of autobiographical memories has most frequently been associated with the hippocampus (HC), the medial prefrontal cortex (mPFC), the parahippocampal gyrus (PHG), the posterior cingulate cortex (PCC), the ventrolateral prefrontal cortex (vlPFC), and the angular gyrus (AG) (12–14). The anterograde memory function is positively correlated with the hippocampal volume in various patient populations, including depression (15, 16). Thus, it is plausible that a brain reserve in these regions may act protectively against the development of amnesia following ECT. If so, such a measure may have potential to serve as a useful predictive biomarker for this amnesia. To the best of our knowledge, this has never been investigated before.
1.1 Aims
The aim of this study was to explore potential predictive biomarkers in the brain for the risk of developing amnesia following ECT by studying how the baseline brain structure relates to this amnesia. Based on the literature, we hypothesized the following:
1. Less autobiographical amnesia will be correlated with a larger baseline hippocampal volume and a larger baseline thickness of the following cortical regions: mPFC, PHG, PCC, vlPFC, and AG (12–14).
2. Less anterograde amnesia will be correlated with a larger hippocampal volume at baseline. Verbal and visual anterograde amnesia will be more strongly correlated with the left and the right HC, respectively (17, 18).
2 Materials and methods
This manuscript was conducted in agreement with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidance. The study was part of The Danish Neuropsychological Study of the Adverse Effects of ECT (DANSECT), which was registered on ClinicalTrials.gov (ID: NCT04160286) before patient recruitment commenced. It was approved by the Ethical Committee of the Capital Region of Denmark (H-19038861).
2.1 Study design and sample
DANSECT was designed as an extension of the Danish ECT/MRI project (ClinicalTrials.gov ID: NCT03040388), as the magnetic resonance imaging (MRI) techniques were the same as those in this project and complemented with neuropsychological measurements (19–23).
This longitudinal study is prospective and observational. We examined inpatients with moderate-to-severe depression who received a series of ECT. Patients were consecutively recruited from mental health centers in the Capital Region of Denmark between December 2020 and July 2023.
Inpatients between 18 and 95 years of age, fluent in Danish, and referred for ECT with moderate-to-severe uni- or bipolar depression according to ICD-10 (24) were eligible for inclusion. Patients with one or more of the following characteristics were excluded: 1) showing severe psychotic symptoms or suicidality, making transportation to MRI hazardous; 2) undergoing maintenance ECT or having already received ECT during the past 6 months; 3) with schizophrenia or other psychotic disorder, apart from psychotic depression; 4) with dependency syndrome cf. ICD-10 (24); 5) with a history of head trauma causing unconsciousness for more than 5 min; 6) with severe somatic or neurological illness affecting the brain; and 7) requiring compulsory treatment. Written and verbal informed consent was obtained from the patients prior to inclusion in our study.
The depression diagnosis giving rise to referral to this project was initially made by a psychiatrist at the psychiatric ward. Subsequently, this diagnosis was confirmed by the project neuropsychologist (AM) or the project medical doctor (CL) using the Mini-International Neuropsychiatric Interview (M.I.N.I.) (25). In order to verify that the symptoms of depression were not due to organic causes, a physical examination, blood tests, electrocardiogram, and urine screening for drugs were performed.
The MRI scans were conducted at pre-ECT (baseline): 1–2 days before ECT. The Wechsler Adult Intelligence Scale IV (WAIS-IV) Vocabulary (26) was applied at post-ECT: 5 (±2) days after the last ECT session. The remaining clinical assessments were performed at both pre- and post-ECT.
2.2 Clinical assessments
The depression severity was measured using the six-item Hamilton Rating Scale for Depression (HAM-D6) (27). The six-item version was chosen as it has been proven to be as sensitive as the longer versions while also being superiorly equidistant (28). Autobiographical memory was measured using the Columbia Autobiographical Memory Interview—Short Form (CAMI-SF) (29), which is the most frequently used tool for assessment of autobiographical memory performance in the ECT literature. Verbal anterograde memory was measured with the Verbal Learning Test—Delayed (VLT-D), which is a subtest of the Screen for Cognitive Impairment in Psychiatry (SCIP-D) (30). Parallel versions were employed at different time points. Visual anterograde memory was measured using the Rey Complex Figure Test (RCFT) 3-min recall (31). The RCFT was administered at both time points due to the different psychometric properties of alternative complex figures (32–34). Premorbid level of intelligence was assessed using the WAIS-IV Vocabulary.
2.3 MRI data
2.3.1 MRI scanner
All MRI scans were carried out on a Philips Achieva dStream (Philips Healthcare, Best, Netherlands) with 3 T. The scanner was equipped with a phased-array receive-only head coil with 32 channels. High-resolution anatomical scans, both T1- and T2-weighted, were conducted using the following parameters: field of view = 256 × 240 × 180 mm3, acquisition time = 335 s, repetition time = 11 ms, echo time = 5.08 ms, inversion delay = 950 ms, flip angle = 8°, no. of slices = 257, turbo factor = 159, and voxel size = 0.7 × 0.7 × 0.7 mm3 for T1-weighted and field of view = 256 × 240 × 180 mm3, acquisition time = 305 s, repetition time = 2,500 ms, echo time = 330 ms, flip angle = 90°, no. of slices = 257, turbo factor = 113, and voxel size = 0.7 × 0.7 × 0.7 mm3 for T2-weighted.
2.3.2 MRI data processing
MRI data were based on T1- and T2-weighted images. These were automatically processed in FreeSurfer (version 7.4.1) (35) using the longitudinal stream (36). Cortical parcellation was automatically performed using the Desikan–Kiliany (37) and the Destrieux atlas (38). The latter atlas was only used for parcellation of the AG as the Desikan–Kiliany atlas does not offer a parcellation corresponding appropriately to this region. Hippocampal segmentation was automatically conducted using the hippocampal module (39). Since the thickness of the perirhinal cortex is not automatically extracted in FreeSurfer, these values were manually extracted from ex vivo data. Quality control was performed through visual inspection of the coronal slices, ensuring correct delineation of the boundaries between gray and white matter. None of the slices gave rise to manual corrections.
2.3.3 Regions of interest
2.3.3.1 ROIs associated with autobiographical memory performance
The selection of the gray matter brain regions for which we expected the baseline volume or thickness to be associated with post-ECT changes in autobiographical memory performance was based on the convergence between three meta-analyses of functional MRI (fMRI) and PET studies (12–14). These studies attempted to identify the core brain regions involved in autobiographical memory recall. The selected regions of interest (ROIs) were the HC, PHG, PCC, mPFC, vlPFC, and AG. The PHG, mPFC, and vlPFC were composite measures comprising the following FreeSurfer parcellations: parahippocampal, entorhinal, and perirhinal cortices (PHG); medial orbitofrontal cortex and rostral anterior cingulate cortex (mPFC); and pars opercularis, triangularis, and orbitalis (vlPFC). Figure 1 presents an overview of the selected ROIs.
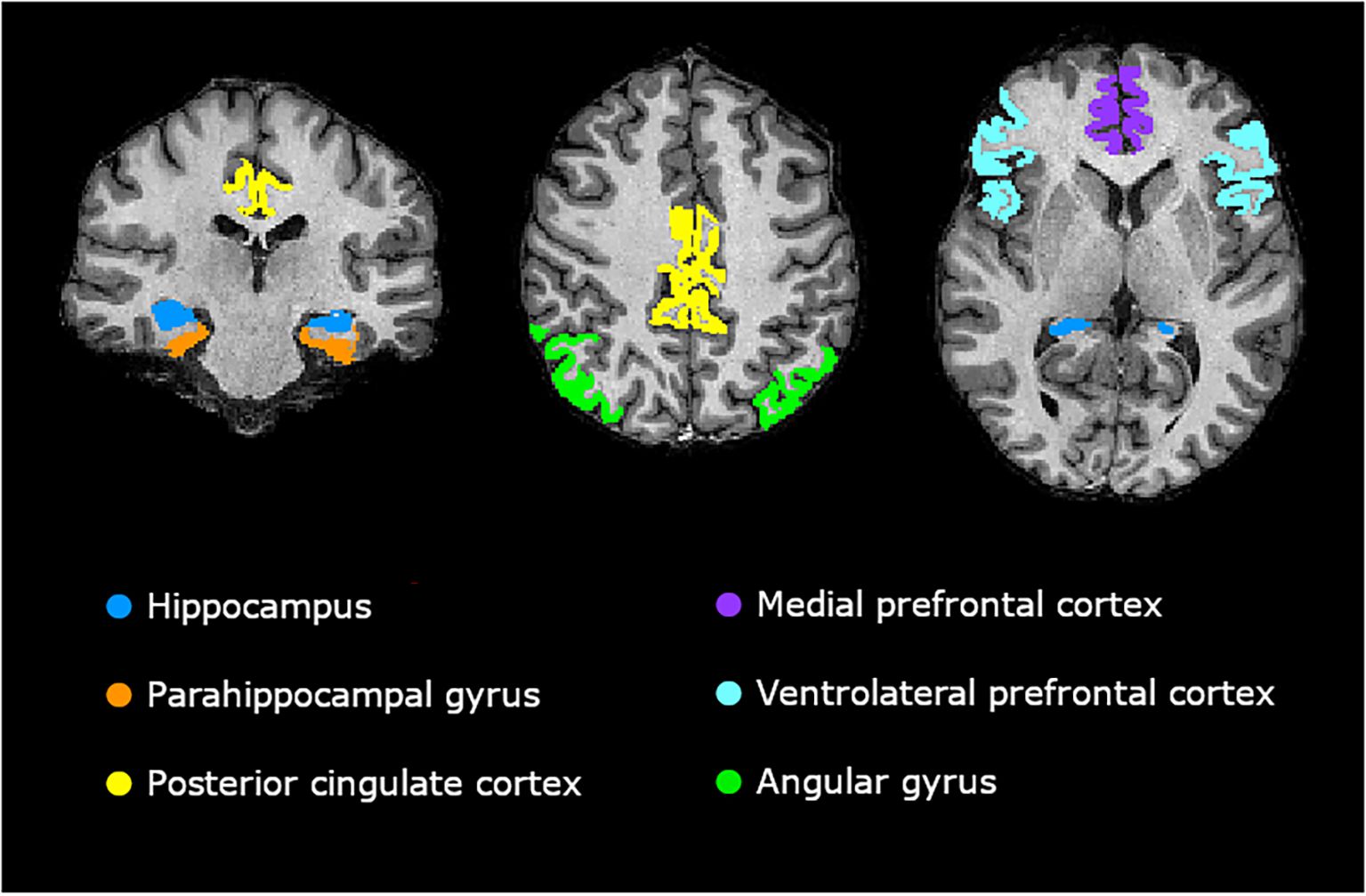
Figure 1. Visualization of the regions of interest (ROIs). Visualizations were rendered in FreeView (35).
2.3.3.2 ROIs associated with anterograde memory performance
The selection of the HC as the ROI, for which we expected the baseline volume to be associated with the changes in anterograde memory performance after ECT, was based on the vast literature linking this structure to anterograde memory from the first study of patient H.M (17) until recent years (18).
2.4 Electroconvulsive therapy
The ECT treatment followed the standard clinical procedures of the Mental Health Service of the Capital Region of Denmark. Bilateral (bitemporal) electrode placement was applied as standard. However, the treating physician could change to right unilateral electrode placement if cognitive side effects were intolerable. Treatment was given three times per week. The treating physicians in the clinic made all decisions regarding patient treatment, and the research group did not participate in these.
ECT was delivered using a Thymatron IV apparatus. The initial treatment charge was calculated according to the half-age method, and the charges used in subsequent treatments were decided according to the clinical effect and the seizure quality as evaluated using electroencephalograms. The pulse width used was brief pulse (0.5–1.0 ms). Anesthesia was performed with thiopental (2–4 mg/kg) and muscle relaxation with suxamethonium (0.75 mg/kg).
2.5 Statistical analyses
As all hypotheses had specific a priori directional predictions based on prior literature, we reported one-sided p-values. Both our hypotheses were tested with partial correlation analyses, conducted using SPSS (version 29.0.1.0) (40). All analyses were controlled for age due to an expectation of age-related atrophy. The analyses involving hippocampal volume were controlled for baseline total brain volume, while the analyses involving cortical thickness were not as cortical thickness is largely independent of head size (https://surfer.nmr.mgh.harvard.edu/fswiki/eTIV). The variables representing amnesia following ECT were computed as the percentage change from pre- to post-ECT (Δ%) as follows:
where Mempost is the post-ECT memory score and Mempre is the pre-ECT memory score.
We correlated the baseline volume or thickness of the ROIs with Δ% in autobiographical memory performance, Δ% in verbal, and Δ% in visual anterograde memory performance. For explorative purposes, these analyses were also run with the subregions (individual parcels) constituting the ROI in question. This was done in order to examine potential drivers of the association between ROI and amnesia.
For an overview of the applied independent and dependent variables, see Supplementary Table S1.
3 Results
3.1 Patient inclusion
For an overview of the inclusion process, see the flowchart in Figure 2.

Figure 2. Flowchart of the patient inclusion process. CAMI-SF, Columbia Autobiographical Memory Interview—Short Form; RCFT, Rey Complex Figure Test; VLT-D, Verbal Learning Test—Delayed.
3.2 Demographic and clinical characteristics
The demographic and clinical characteristics of the included subjects are listed in Table 1.
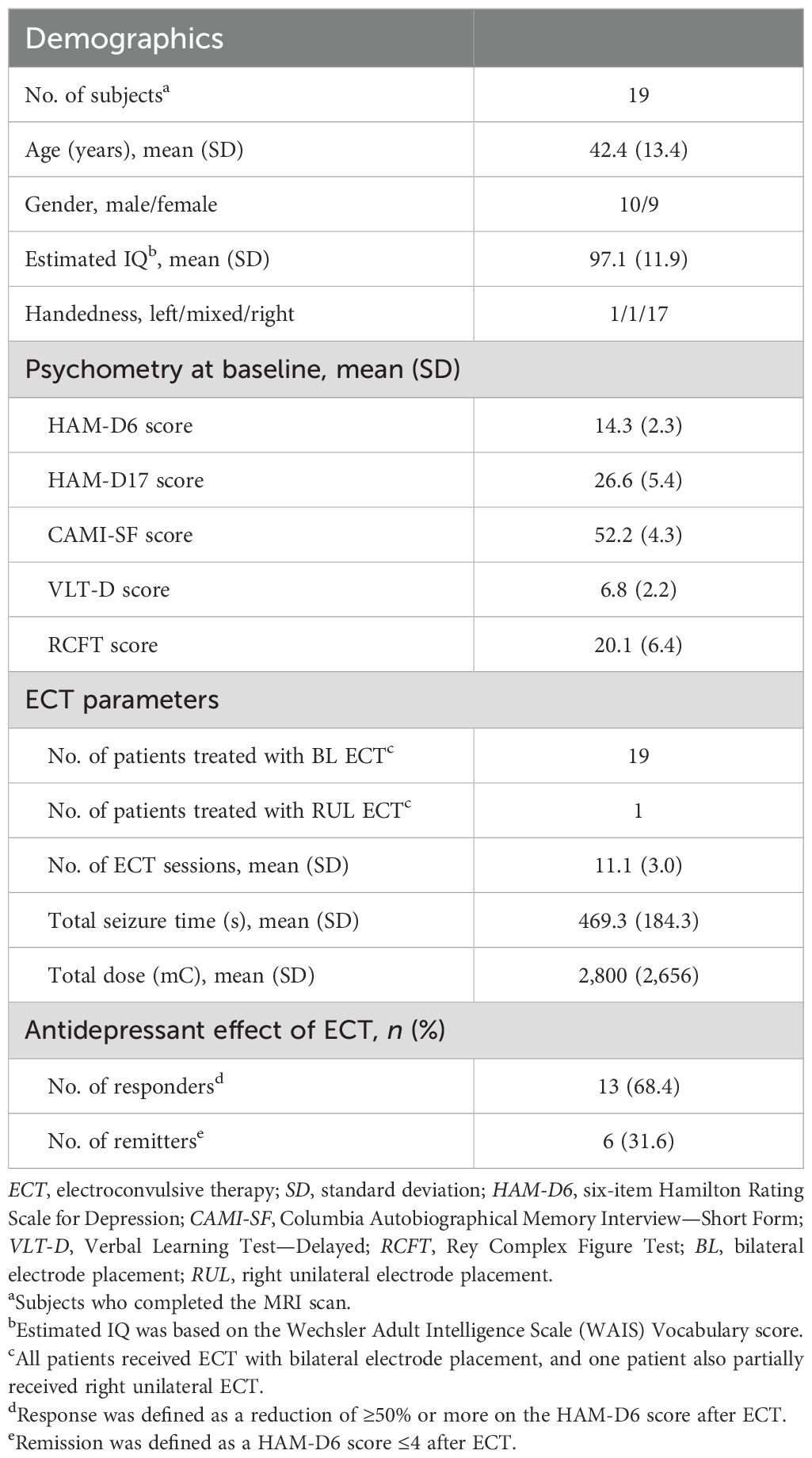
Table 1. Demographic and clinical characteristics of the included subjects.
3.3 Memory decline following ECT
Performance on all three memory tests was approximately normally distributed based on inspection of the histograms. Paired-samples t-tests showed that both autobiographical [t(23) = 9.146, one-sided p < 0.001] and verbal anterograde [t(20) = 3.101, one-sided p = 0.003) memory performance decreased significantly from pre- to post-ECT on group levels. In contrast, there was no significant difference between pre- and post-ECT visual anterograde memory performance on group level (one-sided p = 0.352). For an overview of the individual trajectories, see Figure 3. Post-ECT memory assessment was conducted 177 h after the last ECT session, on average (SD = 141, range = 51–601).
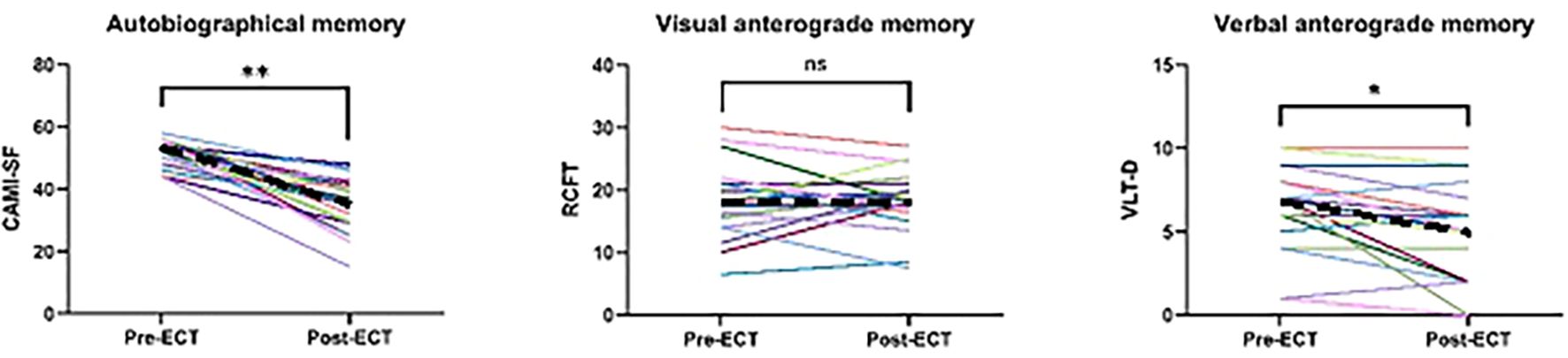
Figure 3. Change in memory performance from pre- to post-electroconvulsive therapy (ECT) across memory modalities. CAMI-SF, Columbia Autobiographical Memory Interview—Short Form; ns, not significant; RCFT, Rey Complex Figure Test; VLT-D, Verbal Learning Test—Delayed. *p = 0.003; **p < 0.001. Dashes denote the median value.
3.4 Prediction of memory decline from baseline brain volume and cortical thickness
For an overview of the main results, see Table 2.

Table 2. Correlation analyses between baseline regions of interest (ROIs) and post-electroconvulsive therapy (ECT) memory loss.
3.4.1 Prediction of autobiographical memory loss
The baseline hippocampal volume and the thickness of the cortical ROIs showed approximate normal distributions based on inspection of the histograms. Less severe post-ECT autobiographical memory loss was correlated with a larger baseline thickness of the left vlPFC (r = 0.530, p = 0.012, R2 = 0.281) and the right PHG (r = 0.517, p = 0.014, R2 = 0.267) (see Figure 4). The correlation with vlPFC was driven by its anterior subregion, pars orbitalis (r = 0.681, p < 0.001, R2 = 0.464), while the PHG was driven by the subregions entorhinal (r = 0.565, p = 0.007, R2 = 0.319) and perirhinal (r = 0.483, p = 0.021, R2 = 0.233) cortices. In the opposite direction of the analyses above, and against our hypothesis, less severe autobiographical memory loss was correlated with a smaller baseline hippocampal volume in the right hemisphere (r = −0.416, p = 0.048, R2 = 0.173).

Figure 4. Baseline cortical thickness and post-electroconvulsive therapy (ECT) autobiographical memory loss. CAMI-SF, Columbia Autobiographical Memory Interview—Short Form; LH, left hemisphere; PHG, parahippocampal gyrus; RH, right hemisphere; vlPFC, ventrolateral prefrontal cortex; Δ%, percentage change from pre- to post-ECT. P-values are one-sided. The scatterplots are not controlled for patient age.
3.4.2 Prediction of anterograde memory impairment
In contrast to our second hypothesis, the baseline hippocampal volume did not correlate with the degree of anterograde memory loss in any combination between laterality and either visual or verbal anterograde memory (p > 0.28 in all cases).
3.5 Post-hoc analyses
To explore whether the antidepressant effect of ECT could mediate our results, partial correlation analyses were performed between the baseline volume or the cortical thickness of the individual ROIs and the post-ECT change in HAM-D6. All analyses were controlled for age, and additionally the baseline total brain volume in the case of HC. We found a trending correlation between a better antidepressant effect and a smaller baseline volume of both the left HC (r = 0.470, two-sided p = 0.06) and the right HC (r = 0.466, two-sided p = 0.06). No significant correlations were observed with the cortical ROIs, but a trend was found with the left PCC (r = −0.465, p = 0.052).
To investigate whether floor effects in autobiographical memory performance potentially influenced our results, we examined whether the baseline volume of the right HC (controlled for age and baseline total brain volume) and the cortical thickness of the right PHG and left vlPFC (controlled for age) were correlated with the baseline autobiographical memory performance. A larger baseline right hippocampal volume was found to be correlated with better autobiographical memory performance at baseline (r = 0.559, two-sided p = 0.02). The baseline thickness of the cortical ROIs did not correlate with baseline performance (two-sided p ≥ 0.65 in both cases).
To explore whether the baseline thickness of the rest of the cortex was associated with the degree of autobiographical memory loss, correlation analyses were extended to all remaining regions parcellated by the Desikan–Kiliany atlas. This yielded significant correlations with the following regions: right insula, lateral orbitofrontal cortex, fusiform gyrus, supramarginal gyrus, inferior temporal gyrus, banks of the inferior temporal sulcus, and bilateral middle temporal gyrus (see Supplementary Figure S1).
An independent samples t-test showed no gender differences in the baseline cortical thickness of the left vlPFC or the right PHG (two-sided p ≥ 0.65 in both cases).
4 Discussion
Overall, we found that structures in both hemispheres correlated with the degree of post-ECT memory loss. Specifically, we found, as hypothesized, that a larger baseline thickness of the right PHG and the left vlPFC correlated with less severe autobiographical memory loss. Unexpectedly, we also found that a lower baseline volume of the right HC correlated with less severe autobiographical memory loss. We did not find hippocampal volume to be associated with either visual or verbal anterograde memory impairment.
The ROIs that were correlated with autobiographical memory loss were located in both hemispheres, and we found additional trending correlations in the right hemisphere (mPFC and AG). Furthermore, the post-hoc analyses almost exclusively showed right hemisphere correlations. This is interesting as the supratentorial neural correlates of this memory modality are predominantly found to be left-lateralized in the literature (14, 41). The association between autobiographical memory loss and the right hemisphere in our data could reflect the nature of autobiographical amnesia after ECT, which typically presents as a reversed gradient, i.e., recently established memories are more vulnerable to loss after ECT (4). This predominantly episodic, rather than semantic, memory loss occurring after ECT could explain the importance of the right hemisphere, as this hemisphere appears to be more involved in episodic recall than the left hemisphere, according to lesion studies (42, 43). It could also be a contributing factor that our patients’ autobiographical recall experiences are more emotionally intense due to their depression. This could explain the strong signal from the right hemisphere, as the literature has shown that the right hemisphere is recruited in addition to the left when recalling emotionally intense autobiographical memories (14), and when the memories elicit negative emotions in particular, there is evidence for a right-hemisphere dominance (44).
4.1 Hypothesis 1: prediction of autobiographical memory decline after ECT
Overall, we found partial support of our first hypothesis as the degree of post-ECT autobiographical memory decline was correlated with the baseline cortical thickness of several of the predetermined ROIs.
We found that a larger baseline thickness of the right PHG, driven by entorhinal and perirhinal cortices, and the left vlPFC, driven by the pars orbitalis, appeared to protect against severe autobiographical memory loss. This might reflect that a relatively larger structure constitutes a neural reserve and, therefore, a relative resilience toward developing autobiographical amnesia after ECT, in accordance with the threshold theory (8). The relevance of these memory regions in relation to ECT-induced autobiographical memory loss is corroborated by post-hoc analyses showing that the thickness of only a small part of the cortex, including these regions, is related to the memory loss. The direction of the correlations is in accordance with the literature generally showing associations between a larger relative size of the cerebral regions involved in autobiographical memory and better autobiographical memory function (45–47). In contrast, we also found a smaller baseline volume of the right HC to be correlated with less severe autobiographical memory decline after ECT. Importantly, however, this result cannot formally serve as evidence against the null hypothesis as the direction of the correlation was opposite to what was hypothesized. Accordingly, the following considerations are merely exploratory. The unexpected direction could be explained by a floor effect, i.e., an inferior autobiographical memory recall at baseline could entail that there are fewer memories and details to lose over time, let alone to detect psychometrically. This explanation is supported by the post-hoc analyses showing that a smaller baseline right hippocampal volume, and not cortical thickness, was strongly correlated with inferior autobiographical memory performance at baseline. The antidepressant effect of ECT could potentially also mediate the finding as a smaller hippocampal volume has been found to predict a better antidepressant effect of ECT (19), possibly leading to a more favorable cognitive outcome. Accordingly, a post-hoc analysis of our data indicated a trend toward the antidepressant effect being larger in subjects with a smaller HC, albeit an actual mediation analysis was not performed due to insufficient statistical power. No significant correlations were observed between the antidepressant effect and the cortical ROIs, although a trend was observed with the left PCC. This might reflect that the antidepressant effect did not confound the correlation between regional cortical brain reserve and autobiographical memory loss.
Our results might reflect that the entorhinal and perirhinal cortices are important to the mechanism behind ECT-induced autobiographical amnesia. In accordance with this, the entorhinal and perirhinal cortices have earlier been linked to retrograde and subordinately autobiographical memory function (48, 49). The entorhinal cortex is regarded as a hub in the communication between the HC and the neocortex and has been found to be involved in long-term memory retrieval, supposedly extending beyond hippocampal involvement (49). Furthermore, animal studies have found perirhinal lesions in combination with entorhinal lesions to cause more extensive retrograde amnesia than entorhinal lesions alone (50). Therefore, it seems plausible that a pre-ECT neural reserve in these regions serves protectively against post-ECT amnesia.
The finding that a larger baseline thickness of the left vlPFC correlated with less autobiographical memory loss after ECT may suggest that the vlPFC plays an important role in the mechanism behind ECT-induced autobiographical amnesia. This is plausible as the vlPFC has been found to be essential to the active retrieval of autobiographical memories (51). Furthermore, the fMRI literature has shown that, when recalling autobiographical memories, the vlPFC is increasingly active the more recently established the memory is (52). Similarly, ECT-related autobiographical amnesia appears more pronounced for the most novel memories (temporal gradient) (4), thus substantiating the relevance of the vlPFC. The increased vlPFC activation with more recent autobiographical memory recall is in fact particularly the case with the anterior vlPFC (52), which corresponds to our finding that the pars orbitalis was the driver of the correlation.
4.2 Hypothesis 2: prediction of anterograde memory impairment after ECT
Our results did not support this hypothesis as the baseline hippocampal volume was not associated with the degree of anterograde memory decline after ECT. Our best attempt at explaining this result is the possibility that the hippocampal volume, in fact, might not reliably reflect anterograde memory ability in neurologically intact middle-aged people as the positive correlation from the literature emerges with age-related atrophy and neurological disease (15). Weak or even negative correlations have been observed in younger healthy adults (15). While a recent meta-analysis has provided partial rebuttal for this position, as it substantiates the positive correlation in healthy children and adolescents (53), the variance in anterograde memory performance explained by the hippocampal volume does seem to be considerably lower even in healthy elderly people compared with same-aged patients with mild cognitive impairment or Alzheimer’s dementia (54). Another possible explanation as to why we did not find a correlation between hippocampal volume and anterograde memory impairment could be the suboptimal statistical power associated with the relatively small sample size of this study.
5 Strengths and limitations
The relatively small sample size was the main limitation. Nevertheless, as our findings are coherent with established knowledge about the human memory function and its neuroanatomical foundation and as all of our findings are moderate or strong correlations, we expect to incite other researchers to attempt replicating our results in larger samples. It is also important to note that the results were not false discovery rate (FDR)-corrected since the purpose of the study was exploratory.
The observational design and the lack of a control group introduced a risk of a confounding effect due to varying simultaneous medications and potentially biased ratings. Nonetheless, the observational design does contain a high degree of ecological validity. With regard to the lack of a control group, the observed memory changes may not entirely be attributable to ECT. In the case of autobiographical memory, a degree of memory loss is expected due to the passage of time and to depression. In the case of the anterograde memory tests, improvements due to test–retest effects might have masked an association with hippocampal volume.
To assess autobiographical memory performance, we applied the most frequently used outcome measure in the field, the CAMI-SF. While its validity has been debated, we argue that the instrument has several advantages in the assessment of autobiographical amnesia in this population as the alternatives lack either ecological validity or sensitivity to recent episodic memory loss (6). However, we also argue that the sensitivity of the CAMI-SF could be improved (6) and recognize that the instrument has not undergone formal validation (55–58).
6 Conclusion
We found partial support for our first hypothesis, as a larger baseline cortical thickness of the right PHG and the left vlPFC correlated with less severe autobiographical memory decline after ECT. These early findings may reflect that a neural reserve in these specific brain areas serves as a protective mechanism against the development of autobiographical memory loss after ECT. This raises the question of whether these measurements have potential to be used as predictive biomarkers for the risk of severe autobiographical amnesia following ECT. However, the findings cannot be generalized at present as they would need to be replicated in larger samples.
The future implications of our findings, if replicated, appear promising as the application of a structural MRI scan before treatment commencement could potentially aid clinicians in identifying patients at high risk of developing autobiographical amnesia following treatment. Ultimately, this information would qualify the shared treatment decision-making and possibly inform the adjustment of treatment parameters to limit disproportional amnesic side effects. Finally, the observed neural correlates might enable future theories of the mechanism underlying amnesia following ECT.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethical Committee of the Capital Region of Denmark. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AM: Writing – original draft, Formal Analysis, Funding acquisition, Visualization, Conceptualization, Project administration, Methodology, Writing – review & editing, Investigation. CL: Investigation, Writing – review & editing, Methodology, Funding acquisition, Project administration, Visualization. KG: Methodology, Investigation, Writing – review & editing. KM: Supervision, Methodology, Writing – review & editing. BF: Supervision, Methodology, Writing – review & editing. HL: Writing – review & editing, Methodology. UL: Methodology, Writing – review & editing. PV: Funding acquisition, Supervision, Project administration, Writing – review & editing, Methodology.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. The project was supported with unrestricted grants from the following funds: The Danish Health Authority [4-1613-417/1], Jascha Fonden [2022-0300 and 2024-0098], Helsefonden [18-B-0266 and 22-B-0237], Tømmerhandler Johannes Fogs Fond [2022-0141], Grosserer L. F. Foghts Fond [22.102], and Læge Gerhard Linds Legat [01-10046].
Acknowledgments
We would like to express our gratitude to the patients for their willingness to participate in the study despite their illness.
Conflict of interest
AM and CL report having received an honorarium from Lundbeck. KM reports having received honoraria from Lundbeck, Gedeon Richter and Angelini.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1699102/full#supplementary-material
References
1. Kolar D. Current status of electroconvulsive therapy for mood disorders: a clinical review. Evid Based Ment Health. (2017) 20:12–4. doi: 10.1136/eb-2016-102498, PMID: 28053184
2. Bjørnshauge D, Hjerrild S, and Videbech P. Electroconvulsive therapy practice in the kingdom of Denmark. J ECT. (2019) 35:258–63. doi: 10.1097/YCT.0000000000000586, PMID: 31764449
3. Leiknes KA, Schweder LJV, and Høie B. Contemporary use and practice of electroconvulsive therapy worldwide. Brain Behav. (2012) 2:283–344. doi: 10.1002/brb3.37, PMID: 22741102
4. Fraser LM, O’Carroll RE, and Ebmeier KP. The effect of electroconvulsive therapy on autobiographical memory: a systematic review. J ECT. (2008) 24:10–7. doi: 10.1097/YCT.0b013e3181616c26, PMID: 18379329
5. Semkovska M and McLoughlin DM. Objective cognitive performance associated with electroconvulsive therapy for depression: a systematic review and meta-analysis. Biol Psychiatry. (2010) 68:568–77. doi: 10.1016/j.biopsych.2010.06.009, PMID: 20673880
6. Mathiassen AB, Semkovska M, Lundsgaard CC, Gbyl K, and Videbech P. Autobiographical memory after electroconvulsive therapy: systematic review and meta-analysis. Br J Psychiatry. (2025), 1–11. doi: 10.1192/bjp.2025.2, PMID: 40357797
7. Katzman R, Terry R, DeTeresa R, Brown T, Davies P, Fuld P, et al. Clinical, pathological, and neurochemical changes in dementia: A subgroup with preserved mental status and numerous neocortical plaques. Ann Neurol. (1988) 23:138–44. doi: 10.1002/ana.410230206, PMID: 2897823
8. Satz P. Brain reserve capacity on symptom onset after brain injury: A formulation and review of evidence for threshold theroy. Neuropsychology. (1993) 7:273–95. doi: 10.1037/0894-4105.7.3.273
9. Sumowski JF, Rocca MA, Leavitt VM, Riccitelli G, Deluca J, and Filippi M. Brain reserve and cognitive reserve in multiple sclerosis: What you’ve got and how you use it. Neurology. (2013) 81:604. doi: 10.1212/WNL.0b013e3182a0ef3d, PMID: 23667062
10. Stern Y, Arenaza-Urquijo EM, Bartrés-Faz D, Belleville S, Cantilon M, Chetelat G, et al. Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimer’s Dementia. (2020) 16:1305–11. doi: 10.1016/j.jalz.2018.07.219, PMID: 30222945
11. Walhovd KB, Fjell AM, Dale AM, Fischl B, Quinn BT, Makris N, et al. Regional cortical thickness matters in recall after months more than minutes. Neuroimage. (2006) 31:1343–51. doi: 10.1016/j.neuroimage.2006.01.011, PMID: 16540346
12. Boccia M, Teghil A, and Guariglia C. Looking into recent and remote past: Meta-analytic evidence for cortical re-organization of episodic autobiographical memories. Neurosci Biobehav Rev. (2019) 107:84–95. doi: 10.1016/j.neubiorev.2019.09.003, PMID: 31491472
13. Shepardson S, Dahlgren K, and Hamann S. Neural correlates of autobiographical memory retrieval: An SDM neuroimaging meta-analysis. Cortex. (2023) 166:59–79. doi: 10.1016/j.cortex.2023.05.006, PMID: 37315358
14. Svoboda E, McKinnon MC, and Levine B. The functional neuroanatomy of autobiographical memory: A meta-analysis. Neuropsychologia. (2006) 44:2189–208. doi: 10.1016/j.neuropsychologia.2006.05.023, PMID: 16806314
15. Van Petten C. Relationship between hippocampal volume and memory ability in healthy individuals across the lifespan: Review and meta-analysis. Neuropsychologia. (2004) 42:1394–413. doi: 10.1016/j.neuropsychologia.2004.04.006, PMID: 15193947
16. Jayaweera HK, Hickie IB, Duffy SL, Hermens DF, Mowszowski L, Diamond K, et al. Mild cognitive impairment subtypes in older people with depressive symptoms: relationship with clinical variables and hippocampal change. J Geriatr Psychiatry Neurol. (2015) 28:174–83. doi: 10.1177/0891988715573535, PMID: 25762610
17. Scoville WB and Milner B. Loss of recent memory after bilateral hippocampal lesions. J Neurol Neurosurg Psychiatry. (1957) 20:11–21. doi: 10.1136/jnnp-2015-311092, PMID: 26283686
18. Danieli K, Guyon A, and Bethus I. Episodic Memory formation: A review of complex Hippocampus input pathways. Prog Neuropsychopharmacol Biol Psychiatry. (2023) 126:110757. doi: 10.1016/j.pnpbp.2023.110757, PMID: 37086812
19. Gbyl K, Rostrup E, Raghava JM, Andersen C, Rosenberg R, Larsson HBW, et al. Volume of hippocampal subregions and clinical improvement following electroconvulsive therapy in patients with depression. Prog Neuropsychopharmacol Biol Psychiatry. (2021) 104:110048. doi: 10.1016/j.pnpbp.2020.110048, PMID: 32730916
20. Gbyl K, Rostrup E, Raghava JM, Carlsen JF, Schmidt LS, Lindberg U, et al. Cortical thickness following electroconvulsive therapy in patients with depression: a longitudinal MRI study. Acta Psychiatr Scand. (2019) 140:205–16. doi: 10.1111/acps.13068, PMID: 31265120
21. Gbyl K, Lindberg U, Wiberg Larsson HB, Rostrup E, and Videbech P. Cerebral perfusion is related to antidepressant effect and cognitive side effects of Electroconvulsive Therapy. Brain Stimul. (2022) 15:1486–94. doi: 10.1016/j.brs.2022.10.007, PMID: 36332891
22. Gbyl K, Jørgensen NR, and Videbech P. Serum S100B protein after electroconvulsive therapy in patients with depression. Acta Neuropsychiatr. (2022) 34:269–275. doi: 10.1017/neu.2022.8, PMID: 35249591
23. Gbyl K, Støttrup MM, Mitta Raghava J, Xue Jie S, and Videbech P. Hippocampal volume and memory impairment after electroconvulsive therapy in patients with depression. Acta Psychiatr Scand. (2021) 143:238–52. doi: 10.1111/acps.13259, PMID: 33251575
24. WHO. The ICD-10 classification of mental and behavioral disorders. Geneva: World Health Organization (1993).
25. Sheehan D, Lecrubier Y, Sheehan K, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. (1998) 59:22–33., PMID: 9881538
26. Wechsler D. Wechsler Adult Intelligence Scale San Antonio, TX: The Psychological Corporation, 4th ed. (2008). doi: 10.1037/t15169-000.
27. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. (1960) 23:56–62. doi: 10.1136/jnnp.23.1.56, PMID: 14399272
28. Lecrubier Y and Bech P. The Ham D6 is more homogenous and as sensitive as the Ham D17. Eur Psychiatry. (2007) 22:252–5. doi: 10.1016/j.eurpsy.2007.01.1218, PMID: 17344030
29. McElhiney M, Moody B, and Sackeim H. The Autobiographical Memory Interview - Short Form, Version 3. New York: New York State Psychiatric Institute (2001).
30. Jensen JH, Støttrup MM, Nayberg E, Knorr U, Ullum H, Purdon SE, et al. Optimising screening for cognitive dysfunction in bipolar disorder: Validation and evaluation of objective and subjective tools. J Affect Disord. (2015) 187:10–9. doi: 10.1016/j.jad.2015.07.039, PMID: 26301477
31. Meyers K and Meyers J. Rey complex figure test and recognition trial: professional manual. Odessa: psychol Assess Resour. (1995).
32. Hubley AM. Using the rey-osterrieth and modified taylor complex figures with older adults: A preliminary examination of accuracy score comparability. Arch Clin Neuropsychol. (2010) 25:197–203. doi: 10.1093/arclin/acq003, PMID: 20139110
33. Gagnon M, Awad N, Mertens VB, and Messier C. Comparing the rey and taylor complex figures: A test-retest study in young and older adults. J Clin Exp Neuropsychol. (2003) 25:878–90. doi: 10.1076/jcen.25.6.878.16480, PMID: 13680464
34. Yamashita H and Yasugi M. Comparison of the medical college of Georgia complex figures and the Rey-Osterrieth complex figure tests in a normal sample of Japanese University students. Percept Mot Skills. (2008) 107:45–50. doi: 10.2466/PMS.107.1.45-50, PMID: 18986030
35. Freesurfer image analysis suite version 7.4.1 2017 . Available online at: http://surfer.nmr.mgh.harvard.edu/ (Accessed September 11, 2024).
36. Reuter M, Schmansky NJ, Rosas HD, and Fischl B. Within-subject template estimation for unbiased longitudinal image analysis. Neuroimage. (2012) 61:1402–18. doi: 10.1016/j.neuroimage.2010.07.020, PMID: 20637289
37. Desikan RS, Ségonne F, Fischl B, Quinn BT, Dickerson BC, Blacker D, et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage. (2006) 31:968–80. doi: 10.1016/j.neuroimage.2006.01.021, PMID: 16530430
38. Destrieux C, Fischl B, Dale A, and Halgren E. Automatic parcellation of human cortical gyri and sulci using standard anatomical nomenclature. Neuroimage. (2010) 53:1–15. doi: 10.1002/jhbs.20162, PMID: 20547229
39. Iglesias JE, Augustinack JC, Nguyen K, Player CM, Player A, Wright M, et al. A computational atlas of the hippocampal formation using ex vivo, ultra-high resolution MRI: Application to adaptive segmentation of in vivo MRI. Neuroimage. (2015) 115:117–37. doi: 10.1016/j.neuroimage.2015.04.042, PMID: 25936807
41. Berntsen D, Sciences B, National D, Memories IA, Introduction A, Past U, et al. Understanding autobiographical memory. (2015).
42. Levine B, Black SE, Cabeza R, Sinden M, Mcintosh AR, Toth JP, et al. Episodic memory and the self in a case of isolated retrograde amnesia. Brain. (1998) 121:1951–73. doi: 10.1093/brain/121.10.1951, PMID: 9798749
43. Markowitsch HJ, Calabrese P, Neufeld H, Gehlen W, and Durwen HF. Retrograde amnesia for world knowledge and preserved memory for autobiographic events. A Case Rep Cortex. (1999) 35:243–52. doi: 10.1016/S0010-9452(08)70797-4, PMID: 10369096
44. Buchanan TW, Tranel D, and Adolphs R. Memories for emotional autobiographical events following unilateral damage to medial temporal lobe. Brain. (2006) 129:115–27. doi: 10.1093/brain/awh672, PMID: 16291807
45. Gilboa A, Ramirez J, Köhler S, Westmacott R, Black SE, and Moscovitch M. Retrieval of autobiographical memory in Alzheimer’s disease: Relation to volumes of medial temporal lobe and other structures. Hippocampus. (2005) 15:535–50. doi: 10.1002/hipo.20090, PMID: 15884035
46. Philippi N, Noblet V, Botzung A, Després O, Renard F, Sfikas G, et al. MRI-based volumetry correlates of autobiographical memory in alzheimer’s disease. PloS One. (2012) 7. doi: 10.1371/journal.pone.0046200, PMID: 23071546
47. Palombo DJ, Bacopulos A, Amaral RSC, Olsen RK, Todd RM, Anderson AK, et al. Episodic autobiographical memory is associated with variation in the size of hippocampal subregions. Hippocampus. (2018) 28:69–75. doi: 10.1002/hipo.22818, PMID: 29171926
48. Burwell RD, Bucci DJ, Sanborn MR, and Jutras MJ. Perirhinal and postrhinal contributions to remote memory for context. J Neurosci. (2004) 24:11023–8. doi: 10.1523/JNEUROSCI.3781-04.2004, PMID: 15590918
49. Takehara-Nishiuchi K. Entorhinal cortex and consolidated memory. Neurosci Res. (2014) 84:27–33. doi: 10.1016/j.neures.2014.02.012, PMID: 24642278
50. Squire LR, Clark RE, and Knowlton BJ. Retrograde amnesia. Hippocampus. (2001) 11:50–5. doi: 10.1002/1098-1063(2001)11:1<50::AID-HIPO1019>3.0.CO;2-G
51. Petrides M. The mid-ventrolateral prefrontal cortex and active mnemonic retrieval. Neurobiol Learn Mem. (2002) 78:528–38. doi: 10.1006/nlme.2002.4107, PMID: 12559832
52. Maguire EA, Henson RNA, Mummery CJ, and Frith CD. Activity in prefrontal cortex, not hippocampus, varies parametrically with the increasing remoteness of memories. Neuroreport. (2001) 12:441–4. doi: 10.1097/00001756-200103050-00004, PMID: 11234742
53. Botdorf M, Canada KL, and Riggins T. A meta-analysis of the relation between hippocampal volume and memory ability in typically developing children and adolescents. Hippocampus. (2022) 32:386–400. doi: 10.1002/hipo.23414, PMID: 35301771
54. Sudo FK, De Souza AS, Drummond C, Assuncao N, Teldeschi A, Oliveira N, et al. Inter-method and anatomical correlates of episodic memory tests in the Alzheimer’s Disease spectrum. PloS One. (2019) 14:1–12. doi: 10.1371/journal.pone.0223731, PMID: 31600312
55. Sackeim HA. Autobiographical memory and electroconvulsive therapy: do not throw out the baby. J ECT. (2014) 30:177–86. doi: 10.1097/YCT.0000000000000117, PMID: 24755727
56. Semkovska M and McLoughlin DM. Retrograde autobiographical amnesia after electroconvulsive therapy: on the difficulty of finding the baby and clearing murky bathwater. J ECT. (2014) 30:187–90. doi: 10.1097/YCT.0000000000000122, PMID: 24755723
57. Sackeim HA. Autobiographical memory and electroconvulsive therapy: Final thoughts on the bathwater. J ECT. (2014) 30:189–90. doi: 10.1097/YCT.0000000000000128, PMID: 33311974
Keywords: electroconvulsive therapy, amnesia, prediction, brain reserve, hippocampal volume, cortical thickness
Citation: Mathiassen AB, Lundsgaard CC, Gbyl K, Miskowiak K, Fagerlund B, Larsson HBW, Lindberg U and Videbech P (2025) Brain reserve in memory regions is associated with the preservation of autobiographical memories after electroconvulsive therapy. Front. Psychiatry 16:1699102. doi: 10.3389/fpsyt.2025.1699102
Received: 04 September 2025; Accepted: 22 October 2025;
Published: 10 November 2025.
Edited by:
Samet Kose, University of Health Sciences, TürkiyeReviewed by:
Jeroen Antonius Van Waarde, Rijnstate Hospital, NetherlandsChristopher C. Abbott, University of New Mexico Health Sciences Center, United States
Copyright © 2025 Mathiassen, Lundsgaard, Gbyl, Miskowiak, Fagerlund, Larsson, Lindberg and Videbech. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: André Beyer Mathiassen, YW5kcmUubWF0aGlhc3NlbkByZWdpb25oLmRr