 Maryam Balke
Maryam Balke René Garbsch
René Garbsch Jessica Cormann1
Jessica Cormann1 Frank C. Mooren
Frank C. Mooren Boris Schmitz
Boris Schmitz- 1Department of Early Neurological Rehabilitation, Cellitinnen Hospital St. Mary Cologne, Cologne, Germany
- 2Department of Rehabilitation Sciences, Faculty of Health, University of Witten/Herdecke, Witten, Germany
- 3DRV Clinic Koenigsfeld, Center for Medical Rehabilitation, Ennepetal, Germany
Background: Post-COVID syndrome (PCS) is a frequent condition with an incidence of 7.8–10.6 per 100 unvaccinated and 3.5–5.3 events per 100 vaccinated persons. Cognitive and motor fatigue are common clinical manifestations, limiting patients’ occupational, educational, and social activities severely.
Objective: This study aimed to develop a diary to keep record of daily changes in energy levels of patients with PCS to adapt their rehabilitation program.
Material and methods: We conducted a prospective observational study at two German rehabilitation centers in a codesign approach with repeated feedback loops. Daily energy changes were analyzed and validated using the Multidimensional Fatigue Inventory-20 (MFI-20).
Results: The final diary revealed that morning and evening energy levels of patients with PCS differed significantly, with 49.6 ± 18.6% and 33.4 ± 19.7%, respectively (p ≤ 0.0001, on admission). Energy levels decreased by ∼5% with active therapy and increased by ∼5% with passive therapy (p < 0.0001). A comparison with MFI-20 at discharge showed good negative correlation (r = −0.5358, p < 0.0001), and patient interviews revealed that most patients (N = 19; 95%) rated the diary as “useful for self-reflection” and “helpful tool to learn the process of pacing.”
Discussion/conclusion: This diary is a valid and user-friendly tool to detect and control the effects of daily therapy during the rehabilitation of patients with PCS. It will facilitate individual planning and adaptation of therapies in PCS and other fatigue groups and may help to implement an effective relation of exercise load to load capacity (pacing) for optimal coping with the disease and an improved handling of daily activities in patients’ lives.
Clinical Trial Registration: Clinicaltrials.gov, identifier (NCT06883500).
Introduction
Since the onset of the COVID-19 pandemic, rehabilitation facilities have been confronted with a large number of patients affected by post-COVID syndrome (PCS). Recently published data based on electronic health records revealed that PCS (or postacute sequelae of SARS-CoV-2 infection/PASC) among unvaccinated persons varies between 7.76 events per 100 persons (omicron era) and 10.64 events per 100 persons (pre-delta era). The cumulative incidence of PCS is lower in vaccinated persons, varying between 3.50 events per 100 persons (omicron era) and 5.34 events (delta era) (1). Per definition, PCS encompasses symptoms that persist for a duration exceeding 12 weeks after the onset of infection with the SARS-CoV-2 virus, beginning either during the infection or in the postinfection phase (2). Chronic cognitive and motor fatigue are common clinical manifestations of PCS, often accompanied by various other deficits such as muscle pain, headache, balance problems, autonomic dysfunction, sleep disturbance, and difficulties in alertness and memory (3–5). While a generally accepted definition of chronic fatigue syndrome does not exist, it can be defined as a subjective state that is beyond tiredness or sleepiness, interferes with activities of daily living and responsibilities, and is intensified by stress of any kind (6). Patients often describe their symptoms of fatigue as a lack of mental energy and muscle strength, with a delayed recovery after physical exertion (7). The situation is even aggravated if post-exertional malaise (PEM) is present, which is characterized by symptoms worsening after inadequate physical or mental activity. In this regard, PCS symptoms may overlap with clinical symptoms of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) (8).
Since patients’ occupational, educational, and social activities can be deteriorated to a comparable extent due to PCS and chronic fatigue as in other chronic diseases, such as multiple sclerosis or cancer (9), leading to a heavy economic burden (10), the need for effective medical rehabilitation is high (11).
As a method of energy self-management, the cognitive behavioral approach of “pacing” has been suggested to achieve symptom reduction and stabilization in ME/CFS (12, 13). Pacing aims to find a level of daily activity at which patients can function, but which does not increase symptom severity (14). The PACE trial highlighted that cognitive behavioral therapy and graded exercise therapy are strategies for efficient pacing (15), yet these results have been controversially discussed (16). A recent meta-analysis on activity pacing interventions for people with chronic fatigue syndrome showed promising results in that interventions were effective at reducing fatigue, psychosocial distress, physical function, and depression (17). However, other authors call for additional RCTs using objectively quantified and digitized pacing over longer durations since the methods of pacing are not standardized (18). In this regard, a retrospective analysis of 86 patients with PCS demonstrated that a stronger adherence to pacing, as measured by the engagement in pacing subscale (EPS), leads to faster recovery and improvement of symptoms (19). Our observations align with current recommendations that both overexertion and underexertion should be avoided in the case of PCS. Therefore, graded exercise therapy, for example, cannot be applied in this context (20).
A diary is a useful tool to reflect and document an individual's health experience daily over a given time (21), so that symptom and behavioral trends become visible with less recall bias than in questionnaires or retrospective interviews alone (22). In the medical field, diaries are a means of clinical evaluation of behavior and efficacy of therapies, e.g., in sleep medicine (23), oncology (24, 25), urinary incontinence (26), Parkinson's disease (27), headache (28), seizure (29), and psychological implications of intensive care (30, 31). Moreover, since the onset of digital applications, it has become easier to track human behavior, to draw conclusions on the validity of existing theories, and to provide big data, as shown successfully with Cure (32) and MyFitnessPal app (33). Recently, a digital application targeting patients with chronic fatigue syndrome has been launched (34). A validated PCS-specific diary—developed in collaboration with patients with PCS—is currently not available for both patients and therapists.
The present study aimed to develop a diary together with affected patients to keep record of patients with PCS' energy levels throughout a structured rehabilitation process. We hypothesized that the diary would be capable of documenting the effects of different therapies on daily energy levels and would help to adapt therapies more specifically to patients’ needs.
Methods
Study design and patients
A prospective multicenter observational cohort study of patients with PCS referred for medical rehabilitation was performed according to STROBE guidelines at Clinic Koenigsfeld Ennepetal, Germany, and Neurological Therapy Center Cologne, Germany, between January 2022 and April 2024. In an initial step, a diary was developed by experts together with patients (codesign; see below). Versions of the diary were provided to patients to investigate usability and sensitivity to daily changes in fatigue/energy levels. Patient interviews were performed to collect feedback. The final version of the diary was validated against the Multidimensional Fatigue Inventory-20 (MFI-20). Patients completed the diary during inpatient (Koenigsfeld) and outpatient (Cologne) medical rehabilitation, both including a combination of physical, cognitive, and respiratory training as well as relaxation and psychotherapy as indicated. Inclusion criteria were a history of at least one COVID-19 infection (positive PCR test at the time of infection) and ongoing or newly expressed performance deficits lasting for at least 3 months prior to recruitment. Performance deficits were documented according to the recent consensus statement, with the cluster of lead symptoms including fatigue/exercise intolerance, shortness of breath, and cognitive dysfunction (35). Patients with coronary artery disease (CAD) after acute myocardial infarction or reperfusion via coronary angioplasty or coronary artery bypass graft, who completed and used the fatigue diary as part of a prospective cohort study, were included as a control group.
Energy diary—phases of development
A codesign approach was used, and the diary was developed over three phases through repeated feedback loops, including interviews with patients with PCS and an expert consensus, consisting of doctors, scientists, and therapists, using the Delphi method.
Phase 1A and 1B: expert consensus and diary development
An expert panel of clinicians, nurses, therapists, and scientists was built to create a specific diary for patients with PCS during rehabilitation, which should be able to detect energy fluctuations throughout the therapy day. In an initial step, existing fatigue diaries for patients’ self-assessment were screened for similarities and applicability in PCS (36–39). The requisition was that the format would be applicable for rehabilitation settings and would be comprehensive enough to reflect intraday changes of fatigue/energy levels correctly. Version 1 of the diary asked for the self-reporting of fatigue at the beginning and at the end of the rehabilitation day, using a visual analog scale from 0 (no fatigue) to 10 (maximum fatigue) (“please indicate your level of fatigue at the beginning and at the end of the day on a scale between 1 and 10”). Emojis ranging from happy to sad, colored from green to red, were used to assess patients' overall condition after each exercise. Participants received a folder containing a diary, user instructions, and legend, comprehensive information about pacing and space for personal notes, and an introduction to the concept by a therapist. The usability assessment of Version 1 involved 27 patients. During weekly visits, clinicians asked about patients' experiences and feedback, which was reported to the panel of experts.
Based on the experiences and feedback on Version 1, an adapted Version 2 of the diary asked for “energy levels” instead of “fatigue” at the beginning of the day, after each therapy session, and at the end of the day, using a visual analog scale from 0 (no energy) to 100 (maximum energy) (“please indicate your level of energy at the beginning of the day, after each therapy session, and at the end of the rehabilitation day on a scale between 0 and 100”; Supplementary Figure 1). The assessment of the usability of Version 2 involved 20 patients.
Phase 2: usability and qualitative content analysis interviews
Feedback on wording and overall usability of the diary Version 2 was collected via standardized interviews with patients. Twenty patients with PCS took part in individual semi-structured problem-centered phone-based interviews (guided by JC), including nine open-ended questions (Supplementary Table 1). Answers were anonymized, transcribed, coded, and categorized using qualitative content analysis in accordance with the established classification system by Mayring (40–42). Interpretation involves deciphering and contextualizing the coded text passages in relation to the research question, elucidating patterns, connections, and meanings. The results were presented to the expert group to decide on necessary modifications and the design of the final version.
Phase 3: validation and clinical applicability
The final version of the fatigue diary was validated in N = 66 patients using the Multidimensional Fatigue Inventory (MFI-20) (43), which provides an aggregate score and three subscales pertaining to general, physical, and mental fatigue (scores range from 0 to 100, with higher values indicating elevated levels of fatigue). The mean self-reported energy levels were correlated with MFI-20 scores quantified on admission and discharge. The effects of different therapy categories on changes in self-reported energy levels were assessed by grouping therapies performed during inpatient rehabilitation (Koenigsfeld, n = 33) into three categories: active therapies, consisting of physical (endurance training, strength training, outdoor activities, etc.) and respiratory therapies (respiratory muscle training), cognitive therapies (cognitive training, education and talks, etc.), and passive therapies (relaxation, massages, hydrojet, etc.).
Statistical analysis
Data were analyzed using SPSS (V.28, IBM, Armonk, USA) and GraphPad Prism (V.10, GraphPad Software, Boston, USA). Constant variables are expressed as mean ± standard deviation (SD) or 95% confidence interval (CI) or median (range) as indicated. The categorical variables are presented as n (%). Energy levels in the morning and evening were averaged across all patients for analysis of daily changes. Energy levels at admission and discharge were defined as the mean of the morning and evening energy levels closest to admission and discharge, within a tolerance of 3 days (in case of missing data). For comparisons of energy levels, only values in which at least 20% of the cohort were involved were used. Effects of different therapy types were analyzed only from center Koenigsfeld for better comparability. Non-normal distribution was tested using skewness and kurtosis. Differences between groups were analyzed using mixed-effects model, unpaired two-sided t-test, or Mann–Whitney U test if indicated. Chi-square test was used for categorical variables. Differences within-group were analyzed using mixed-effects model, paired two-sided t-test, or Wilcoxon test in case of non-normal distribution. Spearman rank correlation analyses were performed to investigate correlations between energy levels and MFI scores. Differences in subgroups [sex and age (divided by median split)] over time were analyzed using two-way repeated-measures ANOVA. Statistical significance was accepted at p < 0.05.
Ethics approval and consent to participate
The study was approved by the respective ethical review committee (Ethik-Kommission Universität Witten/Herdecke; reference number 159/2021 for PCS and 115/2020 for CAD patients) and conformed to the Declaration of Helsinki. Written informed consent was obtained from all participants for study participation.
Results
Phase 1A and 1B: expert consensus and diary development
Figure 1 provides an overview of the diary creation process including final validation. Version 1 of the diary asked patients to indicate intraday changes in fatigue on a visual analog scale from 0 to 10 (0 = no fatigue, 10 = maximum fatigue). Evaluation of results from 27 patients (81.5% women, 18.5% men, mean age F:M = 42 ± 13.0:49 ± 13.0) revealed that the diary was not able to detect changes in patients' fatigue levels over the day (morning vs. evening levels), so that an evaluation of therapy effects would not be possible. Based on patients' feedback and discussion in the expert panel, Version 2 of the diary asked for self-reported changes in “energy levels” instead of “fatigue levels.” This version was sensitive to daily changes in energy levels and also reflected the effects of different therapy sessions (see below, Phase 3: validation and clinical applicability).
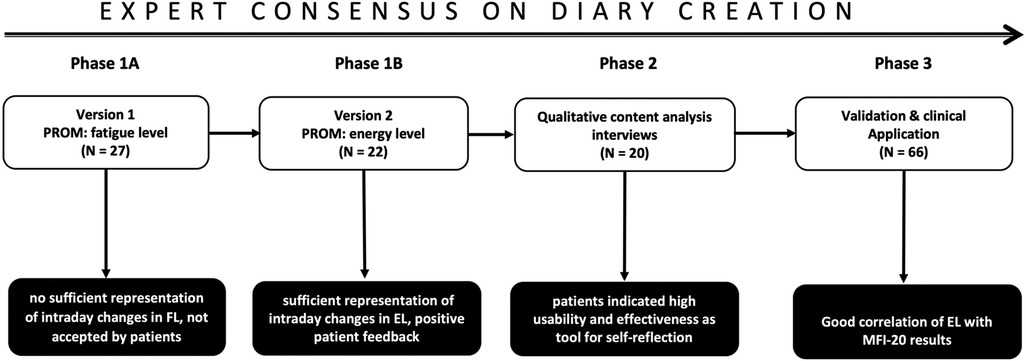
Figure 1. Expert consensus on diary creation, validation, and clinical application. The process of design, validation, and testing of clinical applicability was structured in three phases involving both an expert panel and affected patients. Phase 1 (A/B) Comprised monthly interdisciplinary expert meetings and initial patients’ feedback. Diary Version 1 asked for changes in FL, but daily variations were not reflected, and patients rejected Version 1. Final result: Version 2 reflects intraday changes in energy levels. Phase 2: Qualitative content analysis and usability assessment of Version 2 using structured patient interviews. Final result: sufficient representation of intraday changes in EL, positive patient feedback. Phase 3: Validation and testing of clinical application. Correlation of mean daily energy levels with results of the Multifunctional Fatigue Inventory-20. Investigation of the effects of therapy sessions on energy levels. Result: good correlation with energy level, useful to monitor and control effects of individual therapy sessions. PROM, patient-reported outcome measure; FL, fatigue level; EL, energy level. White box: activity in expert consensus/codesign. Black box: results of expert consensus process.
Phase 2: qualitative content analysis interviews
Twenty patients (70% women, 30% men, mean age F:M 47.6 ± 14.1:45.6 ± 16.0) were interviewed on wording and general usability of the diary (Version 2) using nine open-ended questions (Supplementary Table 1). Overall, patients rated the diary as having appropriate wording and being practical to use. The majority of patients (N = 19, 95%) indicated that formatting and color features were adequate and considered the diary useful as a tool for self-reflection and as a guide and memory aid. Percentual tracking (energy level 0–100) was considered as helpful to assess one's energy levels by 11 patients (55%), while visual tracking with smileys was rated as helpful by 4 patients (20%), and 3 patients (15%) indicated percentual tracking and visual tracking as equally helpful for the subjective assessment of energy levels. In addition, most patients (N = 19; 95%) considered the diary a helpful tool to learn the process of pacing, understand the development of fatigue, and follow therapy effects. Fifty-five percent indicated that a digital diary version (delivered via an app) would be preferable. Analysis of the interviews in the expert consensus process led to the conclusion that no major changes were required. However, one extra page was added to each week for individual notes and comments.
Phase 3: validation and clinical applicability
Version 2 of the fatigue diary with subjective assessment of energy levels was provided to 80 patients with PCS to be filled out during the rehabilitation process. Ultimately, diaries of 66 patients were available for analysis (N = 7 not handed in on discharge, N = 6 premature discharge, N = 1 not usable, incorrectly completed, Figure 1).
Patients' characteristics
Patients with PCS (N = 66; 67% women) involved in the final usability and validation study were referred to rehabilitation with an average age of 51.7 ± 10.3 years and a mean time interval between first infection and start of medical rehabilitation of 453.0 ± 294.7 days (Table 1). Fatigue/exercise intolerance was observed in ∼96% of patients, while cognitive dysfunction (∼76%) and shortness of breath (∼59%) were less common. Detailed examination of fatigue using the MFI-20 questionnaire revealed overall high levels of fatigue (MFI-20 score, 78.0 ± 12.4), with as many as 52% of patients with PCS exceeding the threshold for chronic fatigue syndrome (>70; Table 2). During the acute phase of infection, 97% of patients received ambulant care or acute care at home, while 3% of patients required in-hospital care. Overall, patients reported a high frequency of circulatory system disorders as well as endocrine, nutritional, and metabolic disorders.
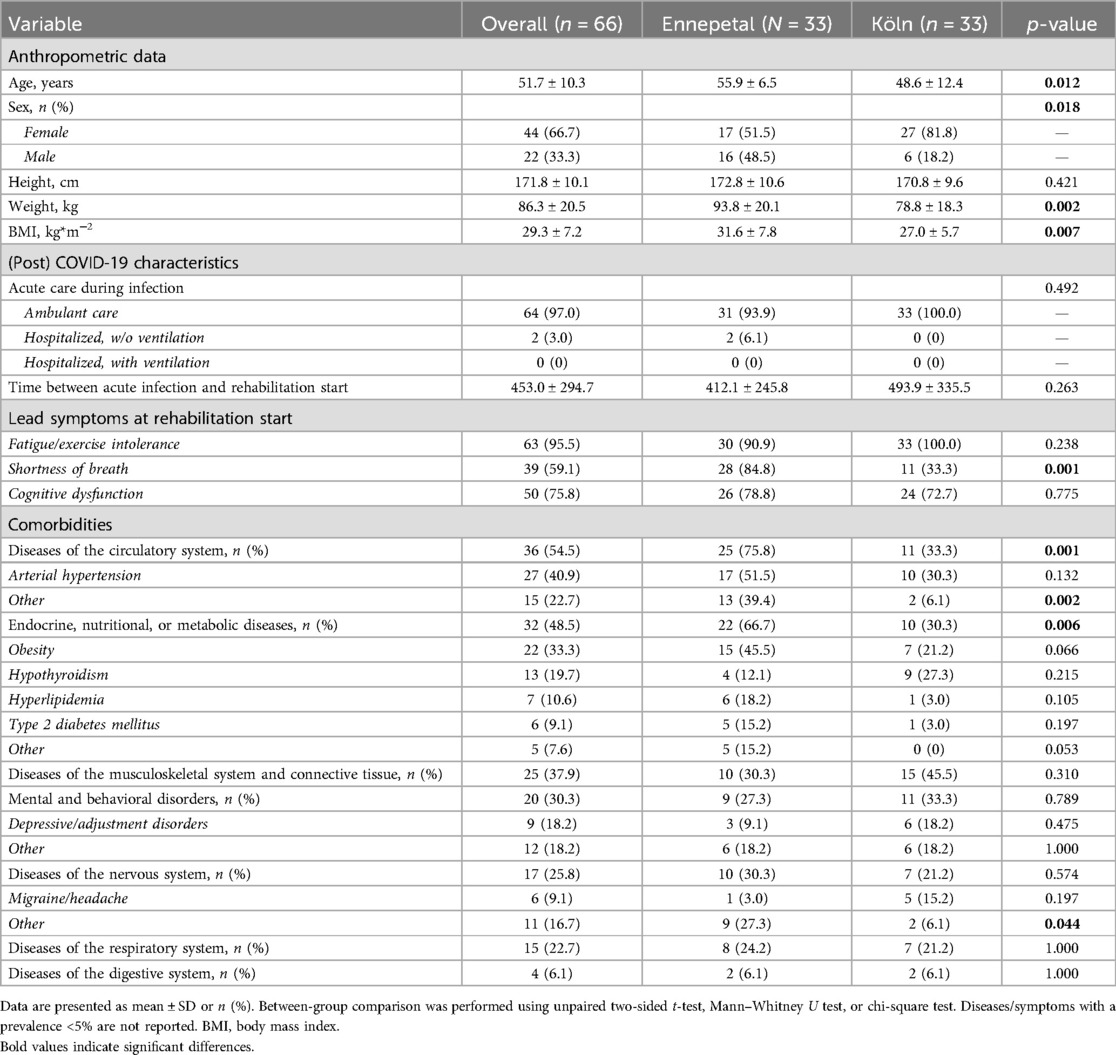
Table 1. Anthropometric and clinical data, medication, and blood parameters.
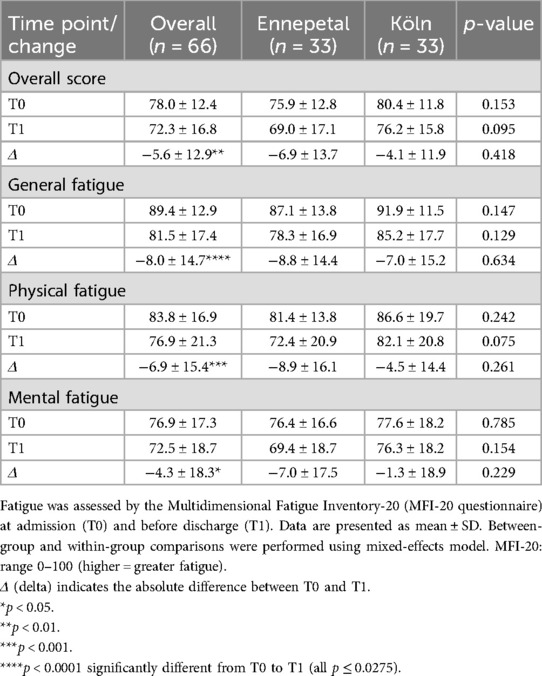
Table 2. Fatigue assessed by Multidimensional Fatigue Inventory-20 (MFI-20).
Diary results—intraday energy level changes
Morning and evening energy levels differed with a significant decrease during the day and a significant increase with overnight recovery (both p ≤ 0.0001; Figures 2A,B). On admission, patients reported a mean energy level of 49.6 ± 18.6% in the morning (max. 100%; min. 15%) and 33.4 ± 19.7% in the evening (max. 80%; min. 20%) using the diary. Over the course of rehabilitation, patients showed small fluctuations in both morning (mean max. 55%; min. 42%) and evening (mean max., 38%; min., 29%) energy levels, but no statistically significant changes were seen from admission to discharge (both p > 0.05). A difference in morning and evening energy levels was seen independently of sex and age (both p < 0.0001) (Figures 2C,D). Of note, male and female patients with PCS indicated significantly different morning energy levels (male, 57.7%; female, 44.5%; p < 0.0001). In addition, on admission, 17.2% of patients with PCS were affected by an energy level of ≤10% in the evening, which improved by the time of discharge, leaving only 9.5% of patients in this state (p = 0.222). Compared to PCS patients, CAD patients (N = 11, 57.1 ± 5.3 years, 55% women) had significantly higher morning (86.8 ± 5.8 vs. 48.2 ± 3.1) and evening (54.9 ± 6.4 vs. 34.1 ± 1.9) energy levels (both p < 0.0001), while the significant daily energy reduction was also seen in CAD patients (Figures 2E,F). During rehabilitation, morning energy levels of CAD patients increased slightly (+7.5, n.s.), while energy levels of PCS patients remained stable. None of the CAD patients reported an energy level of <10% in the evening.
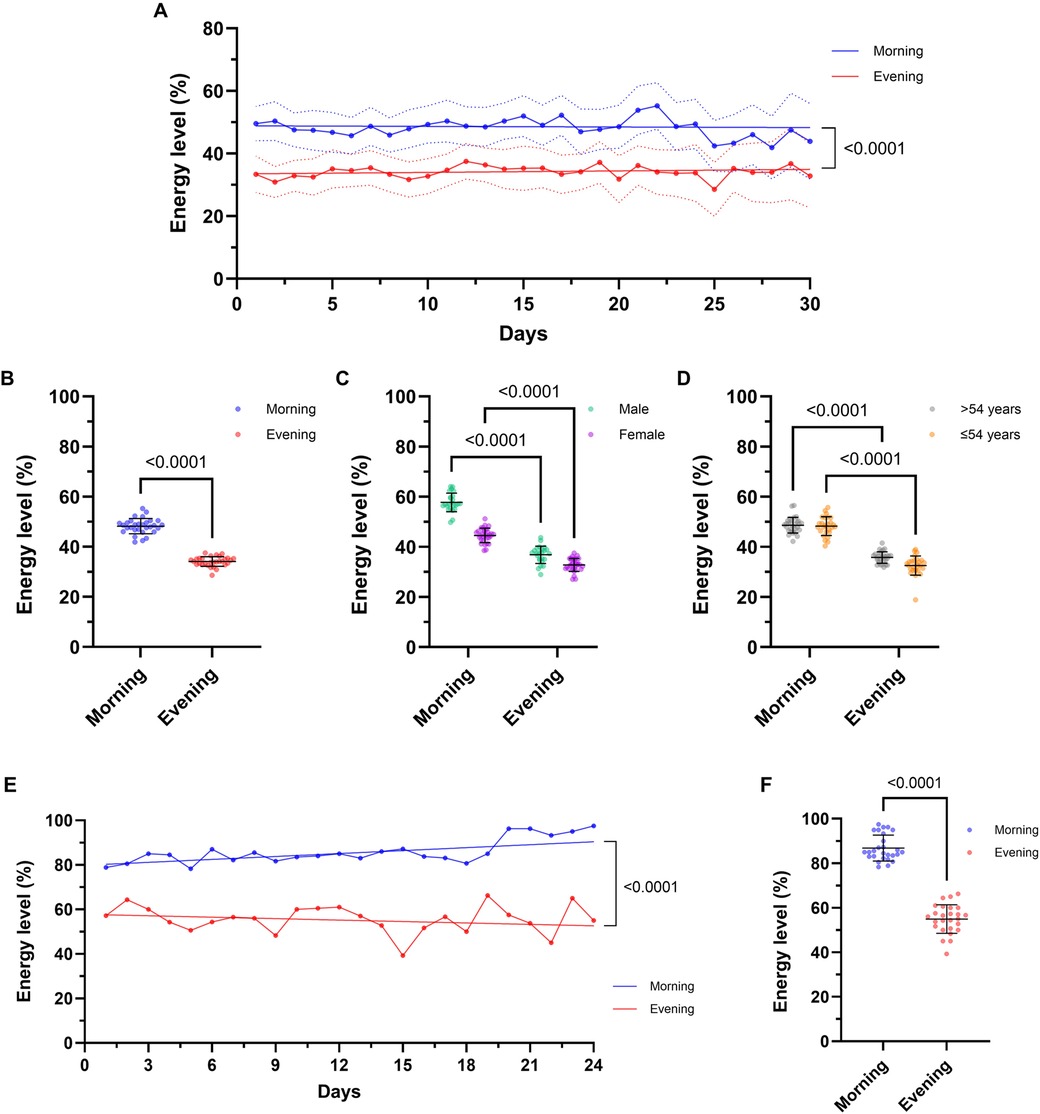
Figure 2. The post-COVID-19 syndrome (PCS) energy diary registers changes in patients’ daily energy levels during rehabilitation. Energy levels of PCS patients (N = 66) are given (A) over the entire rehabilitation process per day (morning vs. evening), (B) in comparison between all morning and evening ratings and separated by (C) sex (female, N = 44; male, N = 22) and (D) median age (>54 years, N = 31; ≤ 54 years, N = 35). Energy levels of patients with coronary artery disease (CAD; N = 11) are given (E) over the entire rehabilitation process per day (morning vs. evening) and (F) in comparison between all morning and evening ratings. Comparison between morning and evening ratings reveals that the fatigue diary documents the loss of energy during the day, as well as energy restoration overnight (p < 0.0001), for both PCS and CAD patients. No differences in morning and evening energy levels were seen from admission to discharge (both p > 0.05). Significant difference in morning and evening ratings was seen, independent of sex and age (all p < 0.0001). Data are presented as the mean of individual data points (with 95% confidence interval) or as mean ± SD. Two-way repeated-measures ANOVA was performed to analyze morning and evening ratings (averaged across all patients) over the entire rehabilitation process as well as for subgroup analyses. Comparison of morning and evening ratings was performed using paired t-test. The trend line was modeled using linear regression slopes.
Analysis of inpatient vs. outpatient rehabilitation revealed significantly different mean morning energy levels (inpatient, 57.6 ± 4.4%; outpatient, 39.9 ± 3.6%; p < 0.0001), while evening energy levels were comparable (inpatient, 33.5 ± 4.2%; outpatient, 34.5 ± 3.3%; p > 0.05). This difference was detected in both, female (inpatient, 54.4 ± 6.6%; outpatient, 38.9 ± 3.2%; p < 0.0001) and male (inpatient, 61.3 ± 4.4%; outpatient, 45.9 ± 8.6%; p > 0.0001) patients, suggesting that inpatient rehabilitation may allow a larger energy gain after daily therapies have been completed (all p ≥ 0.05; Table 2).
Diary validation and effects of therapy on energy levels
General, mental, and physical fatigue was assessed with the validated MFI-20 questionnaire at admission and discharge and correlated to the mean daily energy levels reported in the diary (Figure 3). On admission, the mean daily energy level of patients with PCS showed an inverse correlation with general (r = −0.3591, p = 0.0077) and physical (r = −0.3229, p = 0.0173) but not overall (p = 0.067) and mental fatigue (p = 0.836). At the end of rehabilitation, all subgroups of fatigue correlated significantly with the energy levels assessed via the diary (all r ≤ −0.4018, p ≤ 0.0021; Figures 3E–H). The effects of individual therapy classes (active, passive, cognitive) on energy levels were analyzed in patients from center Koenigsfeld (Figure 4; N = 33) to assess the clinical applicability of the diary. During a mean of 29.9 ± 5.7 days, patients participated in ∼23 therapies per week including ∼11 active and ∼3 passive therapies. Energy levels decreased on average by ∼2% with each cognitive therapy session (total of 488 sessions, p = 0.0057) and by ∼5% with active therapy sessions (1,926 sessions), while passive therapy sessions (337 sessions) regenerated energy levels by ∼5% (both p < 0.0001). Of note, cardiopulmonary exercise testing (CPET) was perceived as a strong energy drain, reducing the energy level by ∼20% (p = 0.0007). The change in energy levels in percent correlated significantly with the rating of therapies using emojis (r = 0.4124, p < 0.0001).
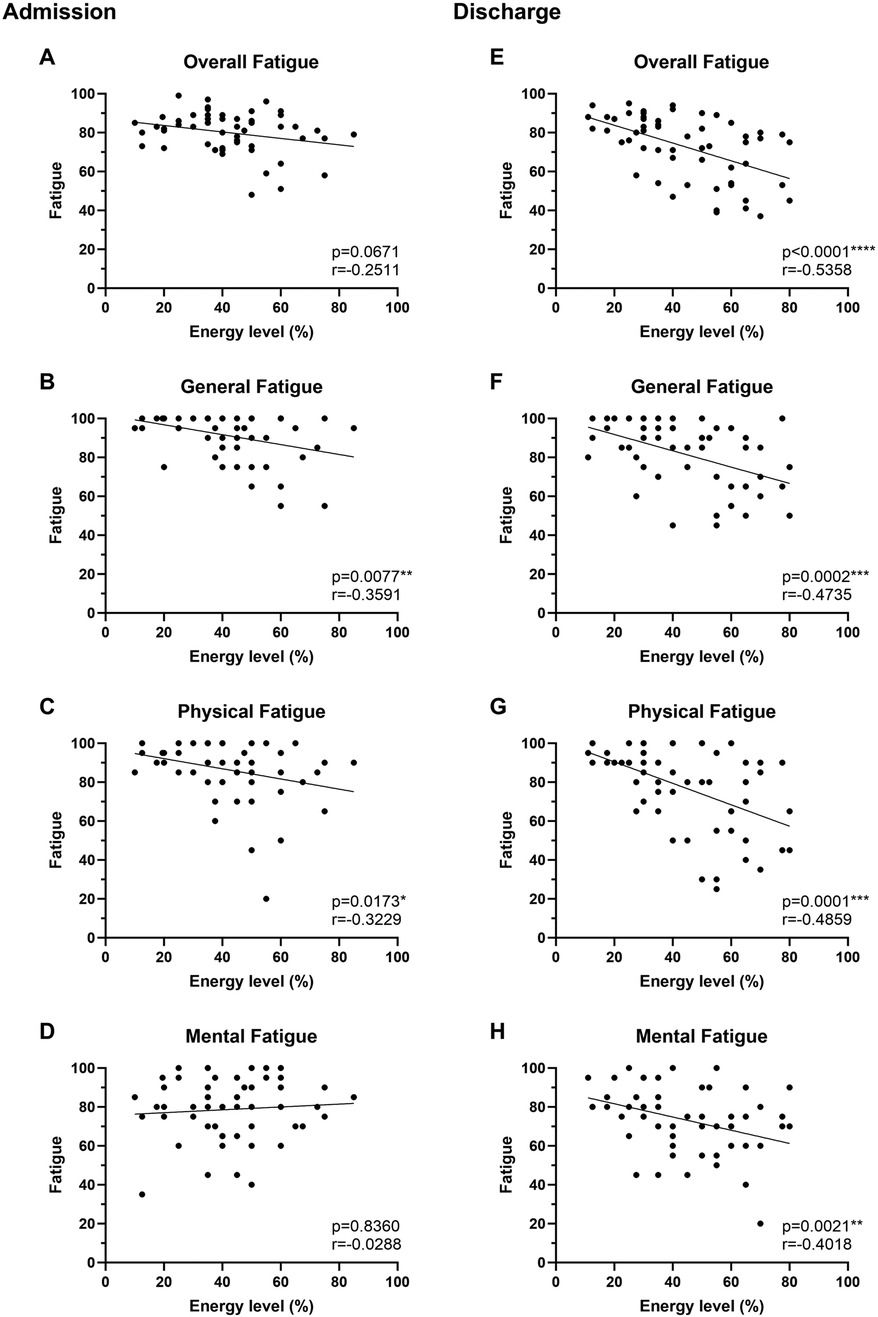
Figure 3. Diary energy levels correlate with Multidimensional Fatigue Inventory-20 (MFI-20) scores. Fatigue of PCS patients was assessed by MFI-20 (score 0–100, higher values = higher fatigue) at admission (A–D) and before discharge (E–H) and compared with mean daily energy levels assessed by the fatigue diary (N = 58). Each data point represents an individual measurement. Correlations were performed using Spearman rank correlation. The trend line indicates linear regression.
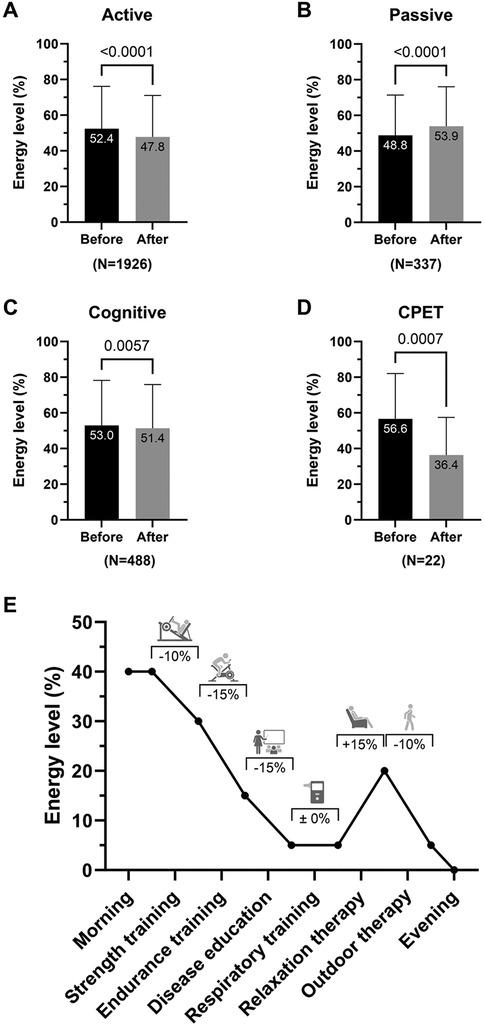
Figure 4. The post-COVID-19 syndrome (PCS) energy diary indicates changes in patients’ energy level subsequent to therapy. (A–D) Energy levels before and after individual patient's therapies (N = 33) were compared by type of therapy. (E) A representative daily progression is depicted with therapies and respective changes in energy level. On average, active therapies reduced energy levels by ∼5% while passive therapies regenerated energy levels to a similar extent. A larger energy drain (∼20%) was seen after cardiopulmonary exercise testing (CPET). In total, PCS patients performed 1,926 active, 337 passive, and 488 cognitive therapies during a mean of 29.9 ± 5.7 rehabilitation days. Active therapies included all physical and respiratory therapies, passive therapies included relaxation therapies, and cognitive therapies included cognitive training, disease education, and talks. CPET was listed separately to analyze the effect of strenuous physical activity on energy levels. Data are presented as mean ± SD and were analyzed using paired t-test.
Discussion
The present study aimed to develop a diary to keep record of patients with PCS' energy levels throughout the rehabilitation process and investigate its usability and validity. Our findings suggest that the resulting diary, developed together with affected patients, was able to detect changes in energy levels throughout the day and that reported energy levels correlated significantly with MFI-20 scores of overall, physical and mental fatigue. The diary was able to reflect the effects of the different therapy classes (active, passive, cognitive) on energy levels. The initial diary version was based on the assessment of fatigue levels. Interestingly, this first version was incapable of detecting changes in fatigue perception during the day. The terms “fatigue” and “low energy” are often used equivalently in the literature but must be distinguished in terms of objective and quantifiable changes in performance called fatigability (44, 45). Since no common definition in the scientific domain has been agreed upon (46), it is necessary to subdivide the term fatigue into pathological and non-pathological, physical vs. mental, neurological vs. non-neurological, and cognitive vs. affective fatigue and overlaps (45). At least in neurological diseases such as multiple sclerosis and Parkinson's disease, perception of fatigue and performance fatigability have been shown to be distinct and potentially independent (47, 48). Our data suggests that within this multidimensional condition of constant fatigue as seen in PCS, subjective changes during rehabilitation may be better described as energy gains and losses as indicated by the patients involved in the diary development. The significantly lower energy level in PCS patients compared with CAD patients (∼40% in morning and ∼20% in evening energy level) further emphasized the need for adjustments of rehabilitation programs according to individual energy levels by personalized training loads and strategies, e.g., pacing. The reported mean daily energy levels correlated well with the results of the Multidimensional Fatigue Inventory indicating an overall association of the constructs. The markedly stronger correlations at discharge compared with admission might indicate an improved understanding of pacing with increased awareness of energy resources. Moreover, it might reflect the time-dependent development of such a skill as for other aspects of mindfulness.
The diary was able to detect energy drains and gains: active therapies such as aerobic or strength exercise reduced energy levels while passive therapies such as relaxation therapy regenerated energy levels. The largest energy drain (∼20%) was seen after exhaustive, cardiopulmonary exercise testing (CPET), and might be sex-specific (49). Using the fatigue diary, it was also possible to follow the overnight restoration of energy levels after active therapies and CPET. The observed difference between types of rehabilitation indicates that energy restoration overnight (i.e., after completing daily therapy) may be more successful in inpatient rehabilitation than in outpatient rehabilitation. While this might be explained by travel burden and regular tasks of daily life, further investigations are warranted.
In current clinical management and monitoring of fatigue of different origin, experts mainly use either self-reported fatigue levels such as the visual analog scale, multidimensional fatigue scales such as the MFI-20 or the Functional Assessment of Chronic Illness Therapy Scale—Fatigue, as well as the European Organization for Research and Treatment of Cancer quality of life questionnaire fatigue subscale (EORTC QLQ-C30), among others (50). However, these assessments are episodic, and questionnaires and scales are not designed to assess patients’ symptom changes in everyday life. Moreover, they do not enable patients and therapists to visualize intraday changes or adjust behavior and therapy frequently and in time. We postulate that a PCS-specific diary could enable rehabilitation teams to adjust patients’ therapies quickly and more effectively to individual needs. We believe that energy-tracking is essential for daily performance management and that our data and the developed diary can help to individualize and optimize PCS rehabilitation. With respect to post-rehabilitation and ambulant use, symptom observation by activity logs, diaries, calendars, and smart devices has been suggested to identify potential risk factors for energy loss (51). A digital version of the PCS diary could help to collect long-term data on the possible course of PCS, to identify risk factors for poor progress, and to assess the need for subsequent interventions (52).
A fine tuning of exercise load and exercise capacity seems to be crucial for a positive outcome of exercise therapy in many chronic diseases, either during pacing for patients with PCS/ME/CFS or other chronic neurological/immunological diseases such as multiple sclerosis, Parkinson's disease, rheumatic disease, and cancer (15). Therefore, a broader need for personalized monitoring of energy levels is necessary. Data from CAD patients suggest some general validity of the energy diary and its practical applicability for other diseases with limitations in exercise performance. As expected, morning and evening energy levels were significantly higher compared with PCS patients. The slightly increasing morning energy levels during rehabilitation might indicate a positive adaptation of fatiguability not seen in PCS patients, while changes in exercise capacity during rehabilitation were comparable for CAD and PCS patients (11).
For a successful clinical application, patients' acceptance is of central importance. In this respect, the interview results suggested that keeping a self-management diary was convenient for patients during rehabilitation and was well accepted. Patients also indicated that reporting their feedback to therapists in detail was of importance to them. These results are in line with reports suggesting that a codesign approach including patients' perspectives is useful in the development of tools and technology assisting patients during rehabilitation (53).
The current study has some limitations. While patients kept detailed track of changes in energy levels during therapy, changes during evenings, weekends, and after discharge were not recorded. Thus, no conclusions on the applicability of the diary in daily life can be drawn. Moreover, data from participants after rehabilitation to evaluate the benefits of energy management based on the energy diary would be useful to investigate the long-term effects of the tool.
To conclude, we provide evidence that a diary based on patients' subjective energy assessment represents a useful and valid tool to detect and control the effects of daily therapy sessions during the rehabilitation of patients with PCS. It may be used to facilitate specific scheduling of therapies during rehabilitation and may help implement pacing. The diary may be a useful therapeutic tool for patients living with fatigue, including patients with ME/CFS, cancer, multiple sclerosis, and other immunologic disorders. However, detailed studies on validity in these patient groups are still necessary.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethik-Kommission der Universität Witten/Herdecke, Alfred-Herrhausen Str. 50,58448 Witten. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MB: Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. RG: Data curation, Formal analysis, Investigation, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. JC: Data curation, Investigation, Project administration, Writing – review & editing. PP: Resources, Software, Supervision, Validation, Writing – review & editing. FM: Resources, Software, Supervision, Writing – review & editing. BS: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Visualization, Writing – review & editing.
Funding
The authors declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fresc.2025.1633466/full#supplementary-material
References
1. Xie Y, Choi T, Al-Aly Z. Postacute sequelae of SARS-CoV-2 infection in the pre-delta, delta, and omicron eras. N Engl J Med. (2024) 391(6):515–25. doi: 10.1056/NEJMoa2403211
2. Koczulla A, Ankermann T, Behrends U, Berlit P, Berner R, Böing S, et al. S1-Leitlinie long-/post-COVID [German S1 guideline long-/post-COVID]. Pneumologie. (2022) 76(12):855–907. doi: 10.1055/a-1946-3230
3. Mooren FC, Böckelmann I, Waranski M, Kotewitsch M, Teschler M, Schäfer H, et al. Autonomic dysregulation in long-term patients suffering from post-COVID-19 syndrome assessed by heart rate variability. Sci Rep. (2023) 13(1):15814. doi: 10.1038/s41598-023-42615-y
4. Ceban F, Ling S, Lui LMW, Lee Y, Gill H, Teopiz KM, et al. Fatigue and cognitive impairment in post-COVID-19 syndrome: a systematic review and meta-analysis. Brain Behav Immun. (2022) 101:93–135. doi: 10.1016/j.bbi.2021.12.020
5. Gutzeit J, Weiß M, Nürnberger C, Lemhöfer C, Appel KS, Pracht E, et al. Definitions and symptoms of the post-COVID syndrome: an updated systematic umbrella review. Eur Arch Psychiatry Clin Neurosci. (2025) 275(1):129–40. doi: 10.1007/s00406-024-01868-y
6. Strahler J, Doerr JM, Ditzen B, Linnemann A, Skoluda N, Nater UM. Physical activity buffers fatigue only under low chronic stress. Stress. (2016) 19(5):535–41. doi: 10.1080/10253890.2016.1192121
7. Rosenthal TC, Majeroni BA, Pretorius R, Malik K. Fatigue: an overview. Am Fam Physician. (2008) 78(10):1173–9.19035066
8. Sanal-Hayes NEM, Mclaughlin M, Hayes LD, Mair JL, Ormerod J, Carless D, et al. A scoping review of ‘pacing’ for management of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): lessons learned for the long COVID pandemic. J Transl Med. (2023) 21(1):720. doi: 10.1186/s12967-023-04587-5
9. Bateman L, Bested AC, Bonilla HF, Chheda BV, Chu L, Curtin JM, et al. Myalgic encephalomyelitis/chronic fatigue syndrome: essentials of diagnosis and management. Mayo Clin Proc. (2021) 96(11):2861–78. doi: 10.1016/j.mayocp.2021.07.004
10. Zhao T, Cox IA, Ahmad H, Campbell JA, Hensher M, Palmer AJ, et al. The economic burden of myalgic encephalomyelitis/chronic fatigue syndrome in Australia. Aust Health Rev. (2023) 47(6):707–15. doi: 10.1071/AH23106
11. Mooren JM, Garbsch R, Schäfer H, Kotewitsch M, Waranski M, Teschler M, et al. Medical rehabilitation of patients with post-COVID-19 syndrome-A comparison of aerobic interval and continuous training. J Clin Med. (2023) 12(21):6739. doi: 10.3390/jcm12216739
12. Twomey R, DeMars J, Franklin K, Culos-Reed SN, Weatherald J, Wrightson JG. Chronic fatigue and postexertional malaise in people living with long COVID: an observational study. Phys Ther. (2022) 102(4):pzac005. doi: 10.1093/ptj/pzac005
13. Friedberg F, Sunnquist M, Nacul L. Rethinking the standard of care for myalgic encephalomyelitis/chronic fatigue syndrome. J Gen Intern Med. (2020) 35(3):906–9. doi: 10.1007/s11606-019-05375-y
14. Nurek M, Rayner C, Freyer A, Taylor S, Järte L, MacDermott N, et al. Recommendations for the recognition, diagnosis, and management of long COVID: a delphi study. Br J Gen Pract. (2021) 71(712):e815–25. doi: 10.3399/bjgp.2021.0265
15. White PD, Goldsmith K, Johnson AL, Chalder T, Sharpe M. Recovery from chronic fatigue syndrome after treatments given in the PACE trial. Psychol Med. (2013) 43(10):2227–35. doi: 10.1017/S0033291713000020
16. Devendorf AR, Jackson CT, Sunnquist M, AJ L. Defining and measuring recovery from myalgic encephalomyelitis and chronic fatigue syndrome: the physician perspective. Disabil Rehabil. (2019) 41(2):158–65. doi: 10.1080/09638288.2017.1383518
17. Casson S, Jones MD, Cassar J, Kwai N, Lloyd AR, Barry BK, et al. The effectiveness of activity pacing interventions for people with chronic fatigue syndrome: a systematic review and meta-analysis. Disabil Rehabil. (2023) 45(23):3788–802. doi: 10.1080/09638288.2022.2135776
18. Antcliff D, Keenan AM, Keeley P, Woby S, McGowan L. Testing a newly developed activity pacing framework for chronic pain/fatigue: a feasibility study. BMJ Open. (2021) 11(12):e045398. doi: 10.1136/bmjopen-2020-045398
19. Ghali A, Lacombe V, Ravaiau C, Delattre E, Ghali M, Urbanski G, et al. The relevance of pacing strategies in managing symptoms of post-COVID-19 syndrome. J Transl Med. (2023) 21(1):375. doi: 10.1186/s12967-023-04229-w
20. Vink M, Vink-Niese F. Is it useful to question the recovery behaviour of patients with ME/CFS or long COVID? Healthcare. (2022) 10(2):392. doi: 10.3390/healthcare10020392
21. Verbrugge LM. Health diaries. Med Care. (1980) 18(1):73–95. doi: 10.1097/00005650-198001000-00006
22. Butz A. Use of health diaries in pediatric research. J Pediatr Health Care. (2004) 18(5):262–3. doi: 10.1016/j.pedhc.2004.06.004
23. Riemann D, Espie CA, Altena E, Arnardottir ES, Baglioni C, Bassetti CLA, et al. The European insomnia guideline: an update on the diagnosis and treatment of insomnia 2023. J Sleep Res. (2023) 32(6):e14035. doi: 10.1111/jsr.14035
24. Koshy B, Avudaiappan SL, Anand AS. Self-care behaviour of patients with breast cancer in the management of side effects of chemotherapy. Cureus. (2023) 15(9):e44586. doi: 10.7759/cureus.44586
25. Oakley C, Johnson J, Ream E. Developing an intervention for cancer patients prescribed oral chemotherapy: a generic patient diary. Eur J Cancer Care (Engl). (2010) 19(s1):21–8. doi: 10.1111/j.1365-2354.2010.01198.x
26. Perrouin-Verbe MA, Drake MJ, Thomas L. The challenges of real-life bladder diary use and interpretation. Eur Urol Focus. (2022) 8(1):11–7. doi: 10.1016/j.euf.2022.01.002
27. Evers LJW, Peeters JM, Bloem BR, Meinders MJ. Need for personalized monitoring of Parkinson’s disease: the perspectives of patients and specialized healthcare providers. Front Neurol. (2023) 14:1150634. doi: 10.3389/fneur.2023.1150634
28. Minen M, George A, Lebowitz N, Katara A, Snyder I. Headache providers’ perspectives of headache diaries in the era of increasing technology use: a qualitative study. Front Neurol. (2023) 14:1270555. doi: 10.3389/fneur.2023.1270555
29. Brinkmann BH, Karoly PJ, Nurse ES, Dumanis SB, Nasseri M, Viana PF, et al. Seizure diaries and forecasting with wearables: epilepsy monitoring outside the clinic. Front Neurol. (2021) 12:690404. doi: 10.3389/fneur.2021.690404
30. Kredentser MS, Blouw M, Marten N, Sareen J, Bienvenu OJ, Ryu J, et al. Preventing posttraumatic stress in ICU survivors: a single-center pilot randomized controlled trial of ICU diaries and psychoeducation. Crit Care Med. (2018) 46(12):1914–22. doi: 10.1097/CCM.0000000000003367
31. Sayde GE, Stefanescu A, Conrad E, Nielsen N, Hammer R. Implementing an intensive care unit (ICU) diary program at a large academic medical center: results from a randomized control trial evaluating psychological morbidity associated with critical illness. Gen Hosp Psychiatry. (2020) 66:96–102. doi: 10.1016/j.genhosppsych.2020.06.017
32. Pierson E, Althoff T, Thomas D, Hillard P, Leskovec J. Daily, weekly, seasonal and menstrual cycles in women’s mood, behaviour and vital signs. Nat Hum Behav. (2021) 5(6):716–25. doi: 10.1038/s41562-020-01046-9
33. Althoff T, Nilforoshan H, Hua J, Leskovec J. Large-scale diet tracking data reveal disparate associations between food environment and diet. Nat Commun. (2022) 13(1):267. doi: 10.1038/s41467-021-27522-y
34. Mäcken J, Wiegand M, Müller M, Krawinkel A, Linnebank M. A mobile app for measuring real time fatigue in patients with multiple sclerosis: introducing the Fimo Health app. Brain Sci. (2021) 11(9):1235. doi: 10.3390/brainsci11091235
35. Soriano JB, Murthy S, Marshall JC, Relan P, Diaz JV. A clinical case definition of post-COVID-19 condition by a delphi consensus. Lancet Infect Dis. (2022) 22(4):e102–7. doi: 10.1016/S1473-3099(21)00703-9
36. Hospices MC. Fatigue diary and weekly planner. Marie Curie Hospices (2024). Available online at: https://www.mariecurie.org.uk/document/fatigue-diary (Accessed July 15, 2025).
37. Support MC. Your fatigue diary. Macmillan Cancer Support (2023). Available online at: https://www.macmillan.org.uk/dfsmedia/1a6f23537f7f4519bb0cf14c45b2a629/19799-10061/mac11664-e09-diary-fatigue-p05-20250207 (Accessed July 15, 2025).
38. Clyde NGG. Fatigue diary. NHS Greater Galscow & Clyde (2023). Available online at: https://www.nhsggc.scot/downloads/fatigue-diary/ (Accessed July 15, 2025).
39. lichterzellen.de. Fatigue-Tagebuch. lichterzellen.de (2024). Available online at: https://www.lichterzellen.de/f%C3%BCr-patienten-1/lies-dich-schlau/fatigue/ (Accessed July 15, 2025).
40. Pohontsch NJ. Qualitative content analysis. Rehabilitation (Stuttg). (2019) 58(6):413–8. doi: 10.1055/a-0801-5465
41. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. (2007) 19(6):349–57. doi: 10.1093/intqhc/mzm042
42. Kitzinger J. Qualitative research. Introducing focus groups. Br Med J. (1995) 311(7000):299–302. doi: 10.1136/bmj.311.7000.299
43. Smets EM, Garssen B, Bonke B, De Haes JC. The multidimensional fatigue inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res. (1995) 39(3):315–25. doi: 10.1016/0022-3999(94)00125-o
44. Stahl SM. The psychopharmacology of energy and fatigue. J Clin Psychiatry. (2002) 63(1):7–8. doi: 10.4088/jcp.v63n0102
45. Solomon NL, Manea V. Quantifying energy and fatigue: classification and assessment of energy and fatigue using subjective, objective, and mixed methods towards health and quality of life. In: Wac K, Wulfovich S, editors. Quantifying Quality of Life: Incorporating Daily Life into Medicine. Cham: Springer International Publishing (2022). p. 79–117. doi: 10.1007/978-3-030-94212-0_4
46. Kluger BM, Krupp LB, Enoka RM. Fatigue and fatigability in neurologic illnesses: proposal for a unified taxonomy. Neurology. (2013) 80(4):409–16. doi: 10.1212/WNL.0b013e31827f07be
47. Lou JS, Kearns G, Benice T, Oken B, Sexton G, Nutt J. Levodopa improves physical fatigue in Parkinson’s disease: a double-blind, placebo-controlled, crossover study. Mov Disord. (2003) 18(10):1108–14. doi: 10.1002/mds.10505
48. Bailey A, Channon S, Beaumont JG. The relationship between subjective fatigue and cognitive fatigue in advanced multiple sclerosis. Mult Scler. (2007) 13(1):73–80. doi: 10.1177/1352458506071162
49. Garbsch R, Schäfer H, Kotewitsch M, Mooren JM, Waranski M, Teschler M, et al. Sex-specific differences of cardiopulmonary fitness and pulmonary function in exercise-based rehabilitation of patients with long-term post-COVID-19 syndrome. BMC Med. (2024) 22(1):446. doi: 10.1186/s12916-024-03658-8
50. Urbano Chamorro I, de la Torre-Montero JC. Cancer-related fatigue and activities of daily living: lessons learned from the COVID-19 pandemic. BMC Palliat Care. (2024) 23(1):110. doi: 10.1186/s12904-024-01437-z
51. Prusinski C, Yan D, Klasova J, McVeigh KH, Shah SZ, Fermo OP, et al. Multidisciplinary management strategies for long COVID: a narrative review. Cureus. (2024) 16(5):e59478. doi: 10.7759/cureus.59478
52. Wu B-Q, Liu D-Y, Shen T-C, Lai Y-R, Yu T-L, Hsu H-L, et al. Effects of hyperbaric oxygen therapy on long COVID: a systematic review. Life (Basel). (2024) 14(4):438. doi: 10.3390/life14040438
53. Schmitz B, Wirtz S, Sestayo-Fernández M, Schäfer H, Douma ER, Alonso Vazquez M, et al. Living lab data of patient needs and expectations for eHealth-based cardiac rehabilitation in Germany and Spain from the TIMELY study: cross-sectional analysis. J Med Internet Res. (2024) 26:e53991. doi: 10.2196/53991
Keywords: post-COVID-19, post-COVID syndrome, chronic fatigue syndrome, diary approach, neurorehabiliation
Citation: Balke M, Garbsch R, Cormann J, Pape P, Mooren FC and Schmitz B (2025) Design and validation of an energy level diary for fatigue management in patients with post-COVID syndrome. Front. Rehabil. Sci. 6:1633466. doi: 10.3389/fresc.2025.1633466
Received: 30 May 2025; Accepted: 30 June 2025;
Published: 21 July 2025.
Edited by:
David Putrino, Icahn School of Medicine at Mount Sinai, United StatesReviewed by:
Alexander Kogel, University Hospital Leipzig, GermanyThomas Urban, Schmalkalden University of Applied Sciences, Germany
Copyright: © 2025 Balke, Garbsch, Cormann, Pape, Mooren and Schmitz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maryam Balke, bWFyeWFtLmJhbGtlQHVuaS13aC5kZQ==
†These authors have contributed equally to this work
‡ORCID:
Maryam Balke
orcid.org/0000-0001-9104-8592