 Fatima Ebrahim1†Sarah Malek1†Kris James2Kyle MacDonald2Peter Cadieux2
Fatima Ebrahim1†Sarah Malek1†Kris James2Kyle MacDonald2Peter Cadieux2 Jeremy Burton2
Jeremy Burton2 Iacopo Cioffi1
Iacopo Cioffi1 Celine Lévesque1
Celine Lévesque1 Siew-Ging Gong1*
Siew-Ging Gong1*- 1Faculty of Dentistry, University of Toronto, Toronto, ON, Canada
- 2Departments of Surgery, Microbiology and Immunology, University of Western Ontario, London, ON, Canada
Orthodontic patients are at a significant risk for oral diseases due to increased plaque accumulation and oral bacterial dysbiosis. We aimed to determine the efficacy of the commercially available Lorodent Probiotic Complex at reducing plaque accumulation and Streptococcus mutans bacterial levels in adolescent orthodontic patients. Sixty adolescents undergoing fixed orthodontic treatment for a minimum of 6 months were recruited in a randomized, double-blind, parallel-group, placebo-controlled trial. They received either Lorodent probiotic lozenge (intervention, n = 30) or placebo lozenge (control, n = 30) orally every day for a 28-day administration period. Participants were assessed at four appointments (T1–T4) over a total of 56 days. Compliance and lozenge satisfaction were monitored. Saliva samples and supragingival plaques were collected for evaluation of S. mutans levels. Clinical assessment using a Plaque Index (PI) was used. Compliance with lozenge intake of all participants was over 90%. There was no significant change in the PI and composite PI scores in both placebo and probiotic groups at each time frame (all p > 0.05) or the relative S. mutans DNA levels in the saliva and plaque between the probiotic and placebo groups. The findings of high compliance and satisfaction with the probiotic lozenges combined with the study's rigorous design offer a baseline for subsequent testing of further potential probiotics (of varying formulations, concentrations), especially in adolescents.
Introduction
A major negative effect of having fixed orthodontic appliances is a potential increase in oral diseases such as caries and periodontal diseases [1, 2]. Orthodontic patients can develop gingivitis [3] that may progress to periodontal disease [4]. Indeed, in children, gingivitis is the most commonly occurring periodontal disease [5] and approximately one third of North Americans suffer from either gingivitis or periodontal disease [6].
The formation of a dental biofilm, generally known as dental plaque, is fundamental to the disease processes observed in the oral cavity [7]. Dental plaque comprises an aggregation of bacteria, salivary components and their exopolymer matrix [8]. Substantial epidemiologic evidence has shown that the presence in plaque of aciduric and acidogenic bacteria such as Streptococcus mutans and lactobacilli plays an important role in the formation of caries [9]. Various preventive approaches against dental caries and periodontal diseases have been thoroughly researched (e.g., good oral hygiene practices, use of fluoride, sugar substitutes, remineralizing agents, and antimicrobial chemical rinses); in spite of this, the incidence of gingivitis and caries remains high in orthodontic patients [10]. There remains a need for a simple, adjunctive aid that can be used to reduce plaque accumulation and cariogenic oral pathogens, especially for at-risk patients such as the orthodontic population. Recent evidence suggests that probiotic therapy might be applied to the maintenance of oral health [11–13].
The World Health Organization defines probiotics as “live microorganisms which when administered in adequate amounts confer a health benefit on the host” [14]. The favorable effects of probiotic therapy are mainly achieved through the modulation of existing microbial flora associated with the host, thus attaining a balanced and healthy microbe-host relationship. Classic probiotic strains, such as those that belong to the genus Lactobacillus, have been tested for their ability to confer a probiotic effect in the oral cavity [15–19]. Indeed, probiotics have been used in orthodontics, with conflicting results [20–22]. The Lorodent Probiotic Complex (Integra Medical LLC) is a commercially available probiotic lozenge. It is a blend of six probiotic bacteria with Streptococcus salivarius BLIS K12 and five probiotic strains of the genus Lactobacillus (new nomenclature according to [23]): Lacticaseibacillus paracasei (previously L. paracasei), Lactiplantibacillus plantarum (previously L. plantarum), Ligilactobacillus salivarius (previously L. salivarius) and Limosilactobacillus reuteri (previously L. reuteri), and Lactobacillus acidophilus, being the key ingredients. The aim of the current study was to investigate the effectiveness of the Lorodent Probiotic Complex with a 3 × 105 CFU/lozenge in reducing plaque and salivary/plaque S. mutans levels in adolescent participants undergoing fixed orthodontic appliance therapy. We hypothesized that the Lorodent Probiotic Complex lozenges could improve gingival health and reducing the level of S. mutans in plaque and saliva.
Methods and Materials
Trial Design
This randomized, double-blind, parallel-group, placebo-controlled trial was conducted at the Graduate Orthodontic Clinic at the University of Toronto, Faculty of Dentistry (Supplementary Material - CONSORT Checklist) and subjects were recruited between August 2014 to October 2014. The clinical trial was registered and conducted in compliance with Health Canada (#185428). The study was approved by the Research Ethics Board at the University of Toronto (protocol #30148). The study was registered at the University of Toronto Faculty of Dentistry Center for Clinical Research.
Participants
Patients undergoing orthodontic treatment at the Graduate Orthodontic clinic, University of Toronto, Faculty of Dentistry, were screened by two orthodontic residents (FE and SH) under the supervision of an orthodontist (SGG) for eligibility by combining review of the medical and dental histories with a dental examination.
Eligibility criteria for the study included male and female subjects between 11 and 18 years of age, in healthy medical condition, who were not pregnant, not past or current users of alcohol or tobacco, and who had not used antimicrobial mouth rinses, probiotics, antibiotics or anti-inflammatory drugs within 1 month prior to the study.
Inclusion Criteria
• Fully erupted teeth #16, 21, 23, 36, 41, 43;
• No active caries;
• Mild to moderate plaque accumulation (Plaque Index [24] score of at least 1);
• Mild to moderate crowding;
• Undergoing fixed orthodontic treatment on both arches with edgewise metal orthodontic brackets on at least 20 teeth and 1st molars bonded for at least 6 months and submitted to a standardized orthodontic archwire sequence of 0.016″ NiTi, 0.016″ × 0.022″ NiTi, 0.019″ × 0.025″ NiTi, and 0.019″ × 0.025″ stainless steel.
Exclusion Criteria
• Allergies or sensitivity to milk or milk products, gluten, soy or any other ingredient present in the Lorodent Probiotic Complex;
• Existing dental caries or xerostomia;
• Any systemic condition that could directly affect gingival condition;
• Recent (within the past 45 days) or planned (within the next 90 days) surgery of any kind (major or minor);
• Participated in another clinical trial within 30 days prior to randomization;
• Experienced any nausea, fever, vomiting, bloody diarrhea or severe abdominal pain within the past 30 days;
• Patients with orthodontic bands.
Participants were randomly assigned to two groups, using a randomization protocol (details included in Supplementary Material—Methods and Materials). All participants received professional tooth cleaning at baseline, i.e., just before being enrolled in the clinical trial. The appliance was bonded in all participants using a standard protocol, e.g., standard bonding procedure using 37% phosphoric acid, Transbond™ Plus Self Etching primer (3M Unitek), and Transbond™ light cure adhesive (3M Unitek) (light cured Bis-GMA composite resin). Participants were withdrawn from the study for the following reasons: (1) personal reasons; (2) reports of fever, nausea, vomiting, diarrhea or severe abdominal pain after having used the probiotic; and (3) pregnancy, antibiotic use, or a severe medical condition. The clinical data and samples collected from such subjects were withdrawn from the study analysis.
Interventions
The blueberry flavored Lorodent probiotic and placebo lozenges (Integra Medical Inc.) were chosen for this study because of its commercial availability and prior in vitro testing of its effectiveness against cariogenic bacteria by the company (Integra Medical, Inc.; data not shown). The probiotic complex was formulated to contain active probiotics (S. salivarius K12, and five probiotic strains of the genus Lactobacillus: Lacticaseibacillus paracasei, Lactiplantibacillus plantarum, Lactobacillus acidophilus, Ligilactobacillus salivarius and Limosilactobacillus reuteri) at a total probiotic concentration of ~3 × 105 CFU/lozenge. In addition, both probiotic and placebo contained lactitol, inulin, dicalcium phosphate, blueberry flavor (natural), dextrose, fructose, stearic acid, citric acid, vanilla flavor (natural), and stevia rebaudiosidea (97%) as excipients. Stored in a −80°C freezer until distributed to participants, all subjects were instructed to store the lozenges in their fridge at home for the duration of the trial. All lozenges had expiration dates that exceeded the end of the trial study by a minimum of 6 months.
The lozenges were administered for 28 consecutive days, followed by another 28-day follow-up without lozenge administration, for a total trial length of 56 days (Figure 1). Previous studies on probiotic lozenges have examined their use with an ~1-month period of intervention [25, 26]. An additional time point midway through the 28-day intervention was added to the present study in attempt to gain a better understanding of any progression of changes that may occur. A fourth time point was added 28 days after cessation of lozenge administration to evaluate if any potential changes would persist after discontinuation of lozenge administration. An initial loading dose of two lozenges two times per day (between 7:00–9:00 a.m. and 7:00–9:00 p.m.) for the first 7 days, followed by a maintenance dose of two lozenges once a day (between 7:00 and 9:00 a.m.) for the next 21 days was prescribed. The total administration period was 28 days, in line with other similar studies [25, 26] and previous safety assessments with S. salivarius K12 (1 × 1010 CFU) [27]. Participants of both groups were given standardized oral hygiene instructions and information on how and when to take the lozenges, based on a written script used by both the examiners (FE and SH who were not involved in the orthodontic treatment of the participants and who met to calibrate each other prior to the start of patient contact). Specifically, subjects were instructed to take the lozenges after their tooth brushing and to slowly dissolve the lozenges on their tongue for 5 min without chewing or swallowing and not to brush or rinse their mouth for 1 h following administration of the lozenges. Subjects were also told, based on the written script, to maintain the current standard of care regarding oral hygiene, i.e., to brush two times per day and floss once per day at a minimum. They were also instructed to not brush their teeth before the appointment or upon arrival to the clinic or to use any antimicrobial mouth rinse during the 56-day trial period. Any adverse events at each appointment or immediately after ingestion, e.g., fever or gastrointestinal discomfort including nausea, vomiting, bloody diarrhea or severe abdominal pain, were noted. Changes to their medical history were also noted throughout course of study.
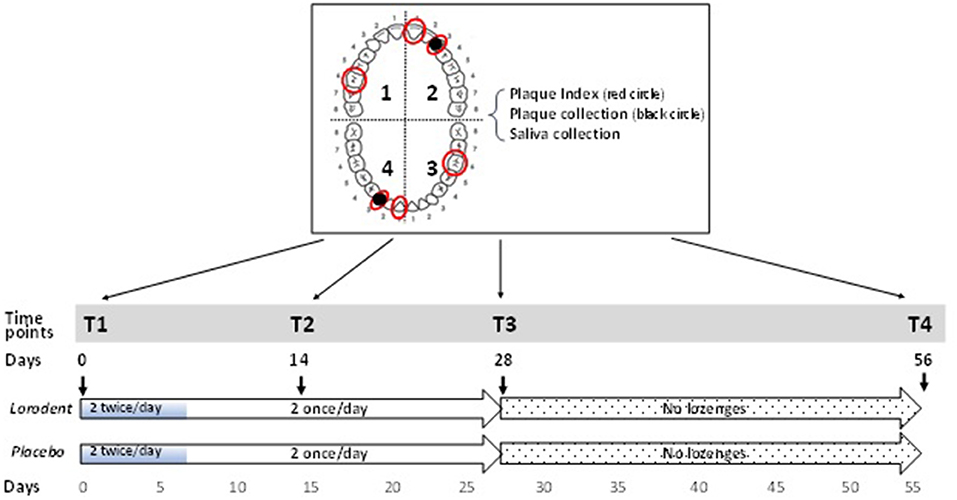
Figure 1. Experimental design and time points of clinical measurements and sample collection. Two lozenges (Lorodent or placebo) were taken twice a day for 7 days (total of 4/day for 7 days = 28 lozenges), followed by 2 lozenges a day for the next 21 days (total of 2/day for 21 days = 42 lozenges); total number of lozenges in trial = 28 + 42. Plaque Index was measured and plaque and saliva samples collected at T1 (0 days), T2 (14 days), T3 (28 days), and T4 (56 days) of the study. The plaque index was measured on teeth # 16, 21, 23, 36, 41, and 43 (red circles) and plaque were collected teeth # 23 and 43 (black circles in tooth arch diagram on top left).
Data and sample collection were taken at the following four time points (Figure 1):
• T1—baseline examination and sample collection at day 0 and initiation of lozenge administration.
• T2—examination and sample collection at day 14.
• T3—examination and sample collection at day 28. Lozenge administration ceased and all remaining lozenges returned to investigators.
• T4—follow up examination and sample collection at day 56.
Sample collection and clinical measurements at T1, T3, and T4 occurred and coincided with the subject's regular orthodontic visits at the Graduate Orthodontic Clinic. One additional appointment (T2), 14 days after the initial data collection, did not coincide with orthodontic visits. Patients were compensated financially in the form of gift cards for their participation in this clinical trial.
Outcome Measures
Clinical Evaluation of Plaque
The Plaque Index (PI) was used to clinically grade the extent and severity of plaque accumulation [24]. PI scores range from 0 (no plaque in gingival area), 1 (a film of plaque), 2 (moderate) to 3 (abundance of soft matter within the gingival pocket and/or on the gingival margin and adjacent tooth surface) (Supplementary Table S1). A modification was made in the study to the Ramfjord teeth to replace the first premolars with the canines, since the canines have one of the highest incidences of white spot lesion formation during orthodontic treatment [28, 29]. Also, by including subjects with extracted first premolars (a common orthodontic treatment plan and found in over a third of the patients treated in the orthodontic clinic), subjects were recruited from a larger pool. Scores of 0–3 (PI) were assigned for the buccal, lingual, mesial and distal surfaces of teeth # 16, 21, 23, 36, 41, and 43 at four time points (T1, T2, T3, and T4) (Figure 1). A total of 24 (6 teeth with 4 surfaces) PI scores each were documented for each subject at each time point. Each participant's overall plaque status at each time point was represented by composite PI (cPI) scores, obtained by adding all 24 PI scores. PI was assessed by two calibrated examiners (FE and SH). Alignment and assessment of examiner scoring were performed at the start of the study (Supplementary Material—Methods and Materials).
S. mutans DNA Quantitation and Real Time Quantitative PCR
Plaque and salivary samples were collected at each time point and analyzed for the levels of S. mutans DNA levels. Well established and validated protocols in DNA extraction and real time qPCR using S. mutans specific primers (details provided in Supplementary Material—Methods and Materials) were used to quantify the levels of S. mutans DNA levels in saliva and plaque.
Measurement of Compliance and Lozenge Satisfaction
At each appointment, subjects were queried as to their ability to follow the oral hygiene, use of mouth rinses, etc. Participants recorded days of lozenge intake on a compliance paper calendar. Compliance was assessed based on the percentage of boxes/lozenges from the total number of lozenges of 70. Monitoring of lozenge safety was conducted through verbal questioning at each appointment. At the conclusion of the study, each participant was asked to complete a 10-item “End of Study Questionnaire”, adapted from a similar questionnaire used by the Xylitol for Adult Caries Trial [30] (Supplementary Table S2). The questions in the questionnaire included their satisfaction with taste of lozenges, success at taking 2 lozenges per day for 28 days, difficulty in taking 2 lozenges per day, difficulty in remembering to take the lozenges every day, whether the study length was too long, whether participants feel the need to prevent white spots, decay or gum disease, whether they lost interest in the study, what they think of the effectiveness of the lozenges, the type of lozenges participants believed they were taking and the likelihood of participants using lozenges if they were shown to be effective at reducing white spots, decay or gum disease.
Statistical Methods
Inter- and intra-rater reliabilities for PI assessments for both FE and SH were computed using weighted kappa statistics and outcomes were interpreted according to Landis and Koch [31]. An independent T-test was used to test age differences between groups. Compliance with lozenge intake was appraised at T2 and T3 using a 2-sided chi-square test. The sex distribution in both groups was tested with a chi-square test.
PI scores were considered scalar values as in previous studies (e.g., [32]). A mixed-effect model was used to test between group and within group differences in PI scores using the study group, the timepoint, and the interaction Group-by-timepoint as fixed factors. Wilcoxon Signed Rank tests were used to test within group changes in microbial DNA (from T1 to T3). Mann-Whitney U-tests were used to test between-group differences the microbial DNA at each time point. Post-hoc comparisons were adjusted using the Bonferroni method. The operator involved in the statistical analysis (IC) was blinded to the allocation of participants to the two groups.
An a priori power analysis was conducted using G*Power (Heinrich-Heine-Universität Düsseldorf, Germany) [33]. As this study was not designed to test sex differences, sex was not considered while computing the sample size. A total sample of 49 participants was required to achieve a power of 0.80 using a medium effect size (d = 0.5) and an alpha of 0.05 (considering two study groups, 4 timepoints, and interactions). The level of significance was set at p < 0.05. SPSS ver. 24 (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Armonk, NY: IBM Corp.) was used for the statistical analyses.
Results
Subject Recruitment Demographics
Out of the 87 subjects screened, 60 met the eligibility criteria and were randomized into two equal groups of 30 each in the probiotic/placebo lozenge groups (Figure 2). A final number of 29 subjects in each in the probiotic/placebo groups was obtained—one participant from the probiotic group withdrew due to antibiotic intake following an accident and a participant from the placebo group was withdrawn due to reports of adverse events (gastrointestinal discomfort and diarrhea) after initiation of study.
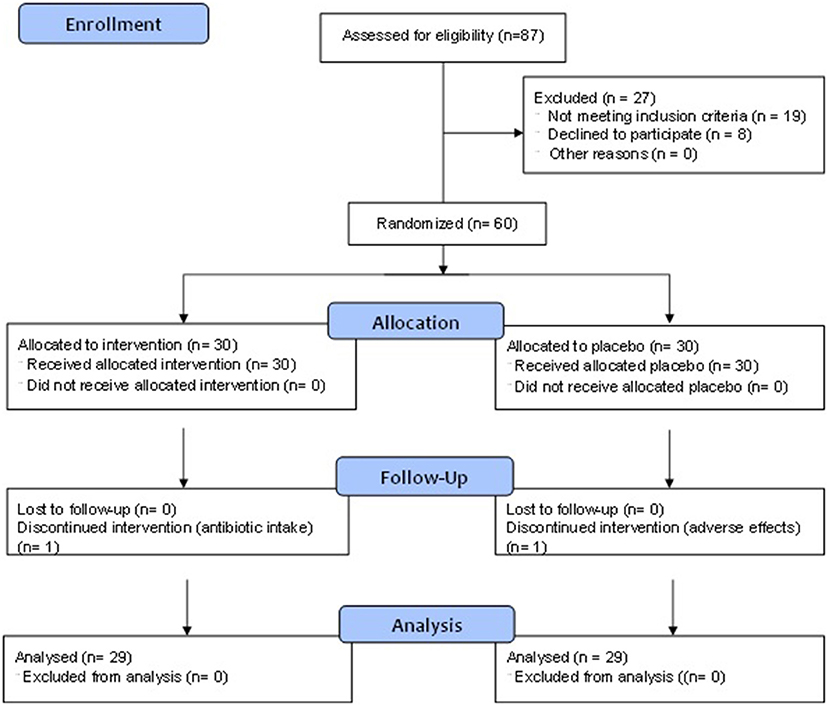
Figure 2. CONSORT flow diagram.
Demographic characteristics did not significantly differ between the two groups. Overall, more females were enrolled in the study compared to males (56.9% females, 43.1% males)—in the probiotic group, 16/29 (55.2%) were males and 13/29 (44.8%) were females compared to 9/29 (31.0%) males, and 20/29 (69.0%) females in the placebo groups. The distribution of male and female participants did not differ significantly across groups [(X2 = 1, N = 58) = 3.445, p = 0.063]. The mean ± SD participants' ages were 15.7 ± 1.7 years; the mean ± SD age in the probiotic group was 15.75 ± 1.67 years compared to 15.64 ± 1.75 years in the placebo group. The groups were similar in age (p = 0.807).
Rater Reliability
Examiner alignment before the study resulted in “substantial” agreement between the examiners for Samples B (intra-oral photos: kappa = 0.72 for PI, p-values for both of < 0.001) and C (live clinical patients: kappa = 0.74 for PI; p-values for both of < 0.001). After the study, the inter-rater agreement improved to “almost perfect” (kappa = 0.82 for PI; p-values for both of < 0.001) when the examiners re-scored Sample B. Intra-rater reliability of the PI scores assigned to Sample B (intraoral photos) showed that both examiners independently had “almost perfect” agreement (PI- examiner 1: kappa = 0.83, examiner 2: kappa = 0.84; p-values < 0.001). The intra-rater reliability was not significantly different between examiners (p < 0.001).
Compliance With Intervention, Patients' Satisfaction, and Adverse Events
Analysis of compliance with lozenge intake at T2 and T3 revealed that all participants reported compliance of over 90%. The mean values between groups were also very similar: At T2 and T3, 89.7% (p = 1.00) and 72.4% (p = 0.56) of subjects in both groups reported a perfect compliance, respectively, with no significant difference between the two groups.
The lozenges were well received by subjects, with 89.6% of participants reportedly very satisfied or satisfied with the lozenge taste and 81% responded they would be fairly likely to use them if they were shown to be effective at reducing white spots, decay or gum disease.
One participant, later identified to be in the placebo group, discontinued use of lozenges 2 weeks after the initial intake of lozenges due to reports of gastrointestinal pain and diarrhea that continued for a couple of days after discontinuation of lozenge administration. The subject was monitored for another 6 weeks, with no recurrence of symptoms. None of the participants in the probiotic group reported any adverse events.
Effects of the Interventions on Plaque Index and Bacterial Levels
PI scores were not different between groups (F = 0.866, p = 0.347) or timepoints (Group-by-timepoint interaction F = 0.629, p = 0.596). No significant improvements in both PI and cPI scores from baseline were seen throughout the intervention period for the probiotic group at any time frame (p > 0.05) (Figure 3, show plots depicting temporal changes of PI in both groups).
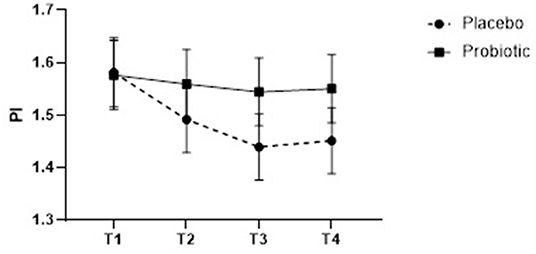
Figure 3. Plaque Index (PI) scores of participants taking control and probiotic lozenges at the 4 time points of the study. Note that the PI scores range from 1 to 4 (Supplementary Table S1) and PI scores shown in both groups ranged between 1.4 and 1.6.
Supragingival plaque and salivary samples were analyzed from 58 (29 probiotic; 29 placebo) and 29 (15 probiotic; 14 placebo) at T1 and T3 for the relative levels of S. mutans DNA. The average DNA yields from the plaque and saliva samples were 1.2 and 5.5 ng/μL, respectively. In general, the relative proportions of S. mutans DNA in the plaque and saliva samples were relatively low and undetectable in 20 plaque and 3 saliva samples (Figure 4). Of the remaining samples with detectable values, no significant differences in the amount of change in the relative proportions of S. mutans were found between the two groups (Table 1). A trend, however, for the S. mutans levels to decrease (p = 0.372), and increase (p = 247), was noticed in the supragingival plaques in the probiotic and placebo groups, respectively.
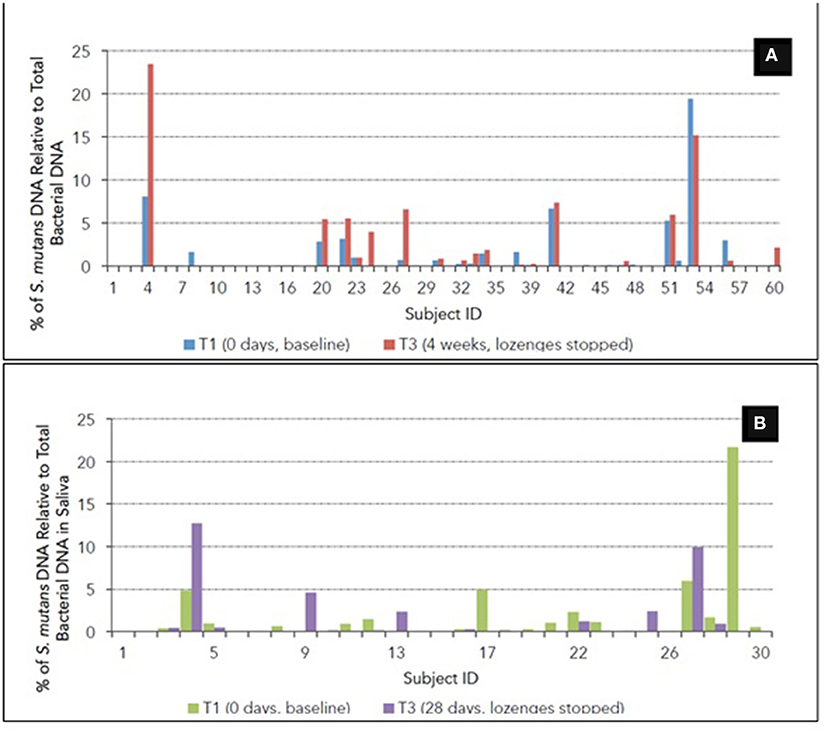
Figure 4. Percentage of S. mutans DNA relative to total bacterial DNA from (A) supragingival plaque and (B) saliva for each participant at T1 and T3. In the majority of samples, S. mutans DNA levels were not detectable.
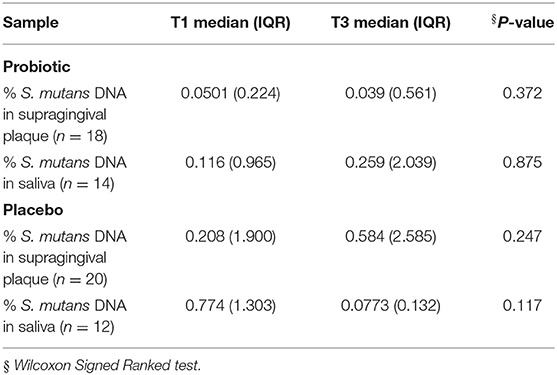
Table 1. Changes in S. mutans DNA in plaque and saliva.
Discussion
This current study joins the many previous studies designed to better understand the efficacy of a probiotic strategy in the improvement of oral health. The vulnerability of orthodontic patients to caries and poor gingival health and the built-in nature of recurrent orthodontic visits over an extended period make them especially suitable as study subjects for a probiotic study. Additionally, any findings generated in this population group are applicable to the understanding of the effectiveness of oral probiotics in improving oral health in all individuals, whether under orthodontic treatment or not.
Our findings of a lack of statistical differences in PI and salivary and plaque S. mutans levels between the probiotic to control groups were corroborated by other studies targeting the orthodontic population. For example, Benic et al. [11] and Kohar et al. [34] found no statistically significant differences in PI measures in orthodontic subjects given Limosilactobacillus reuteri (formerly L. reuteri) and S. salivarius M18 lozenges, respectively. In addition, Gizani et al. [17] did not find a statistical significant difference in salivary MS counts in subjects consuming lozenges containing two strains of Limosilactobacillus reuteri once daily for 17 months. In contrast, a study found that the proportion of streptococci was significantly reduced, compared to the administered probiotic strains containing combinations of Enterococcus and Lactobacillus strains [35]. Also, the authors of a systematic review concluded that, of the 9 included randomized controlled trials, 8 provided evidence that probiotics “improves oral health in patients undergoing fixed orthodontic therapy” [22]. Interestingly, several of these studies used yogurt as a delivery vehicle, suggesting that dairy products might be more effective carrier vehicles for probiotics for oral health, rather than lozenges, a point reinforced by a systematic review and meta-analysis that concluded the effectiveness of dairy products in reducing S. mutans levels [36]. Indeed, bacteria such as Lacticaseibacillus rhamnosus (formerly L. rhamnosus) [37], Lacticaseibacillus rhamnosus with Bifidobacterium animalis subsp. lactis [38], and S. salivarius M18 [1] appeared to be effective in reducing dental caries, especially if milk is used as a delivery vehicle (reviewed in [36]). Because dairy products contain calcium phosphate and casein phosphopeptides, enamel remineralization of the carious tooth can be enhanced [39], especially when these probiotics are supplemented with fluoride, another product known to improve remineralization [40]. Although the Lorodent Probiotic Complex was formulated with the premise that a combination of bacterial strains might have a synergistic effect that together would be effective in combating oral diseases, similar to some probiotics used for gastrointestinal health [41, 42], that expectation of synergistic effect with combined probiotic strains was not achieved in the current study. One potential reason for the lack of any clinically measurable effects of the probiotic complex on plaque accumulation could be due to the fact that the active CFUs/lozenge was ~105 CFUs/lozenge, an amount below the 109 active CFUs/lozenge usually used for probiotic therapy in the gastrointestinal literature [1, 38, 40, 43]. Future studies could be dedicated toward using dairy products to carry the Lorodent Complex, a higher dose of the probiotic complex in addition to the adoption of evaluation of its anti-caries properties, e.g., measurement of the presence of white spot lesions, and changes in microbial composition of the plaque and/or saliva during administration of the probiotic (e.g., by next-generation sequencing).
Although no differences were detected in the PI scores or microbiological measurements of S. mutans in supragingival plaque or saliva in subjects taking the probiotic complex, one finding from the study stood out clearly. That is, the current study showed a strikingly high compliance of 90% with the blueberry-flavored lozenge use, even when it involved the necessity of taking the lozenges twice a day for 7 days. Many past studies of prescribed drug regimens in adolescence showed compliance rates around 50% (reviewed in [44]). The high compliance and acceptability of these lozenges suggest that commercialization marketing of lozenges as a delivery vehicle for anti-caries probiotics or any therapeutic modality will be well received by adolescents, a major target group of anti-caries efforts. Additionally, no adverse events were experienced in the probiotic group in this study, corroborating the safety shown in other preclinical studies of the probiotic species included in the Lorodent lozenge [27], and thereby establishing the safety of the Lorodent Probiotic Complex in humans at the dosage tested.
Dental crowding has been directly associated with plaque accumulation [45]. In this study, only subjects that had been treated orthodontically for longer than 6 months, with the majority of the subjects being treated longer than 9 months, where little or no crowding were observed. The lack of crowding and the regular monitoring of their oral hygiene suggest that factors related to the probiotics might be at play in the outcome of the study. For example, it is also possible that a longer probiotic treatment may be needed to establish the Lorodent probiotic strains in the oral cavity—oral hygiene in adolescent orthodontic patients is usually poor and mechanical debridement around the orthodontic bracket more arduous, resulting in oral biofilms that are thicker, denser and generally more pathogenic. Indeed, previous studies have also shown that S. mutans levels increased about four times in patients undergoing active orthodontic treatment compared to controls [46]. In this regard, perhaps it may help to have complete mouth disinfection with chlorhexidine prior to probiotic usage to increase the ability of the probiotic strains to compete and establish themselves, as had been previously reported [47].
In the current study, we measured the levels of S. mutans DNA in the saliva and plaque in addition to the PI scores, both of which are indicators of oral health. Although plaque accumulation itself is not a risk factor for caries, the dental biofilm is a critical component involved in the development of caries and periodontal diseases, both of which are the leading causes of tooth loss [48]. We observed that there was no significant difference in the PI scores in both probiotic and control groups. The Silness and Löe's Plaque Index, as used in the current study, may suffer from lack of accuracy and reliability for the current study. The index is used in periodontology to assess plaque in marginal gingival areas; in contrast, plaque in orthodontic patients usually accumulates in the direct vicinity of the bracket. Furthermore, the scale may not be precise enough to detect less noticeable changes in plaque levels produced by the probiotic. Although alternative plaque indexing scales exist, e.g., the Orthodontic Plaque Index (OPI) [49], or the use of a digital plaque image analysis (DIPA; using a digital camera, UV flash units and software evaluation) [50], they suffer from lack of validation and/or are expensive and technically demanding. In the microbial analysis, although we used a highly sensitive and specific technique (real-time quantitative PCR), the vast number of samples in the current study necessitated the use of a multiplex DNA extraction kit that, although convenient, tends to result in lower yields of DNA that in turn might have resulted in lack of detection of S. mutans in many of the plaque samples. Finally, it must be noted that this study was based on an a priori sample size calculation for which we considered a medium effect size, and not on data retrieved from other studies or pilot investigations using a similar research design or methods. Computing the sample size using data from previous studies or pilot investigations could have improved the quality of our sample size calculation. Also, our study was not designed and sufficiently powered to test the effect of age and sex on the outcome measures. However, the study groups in the current study had similar age and sex distributions.
Our study illustrated that probiotic therapy in the forms of lozenges at the specific formulation and bacterial count did not influence the plaque accumulation and S. mutans levels in saliva and supragingival plaque over the 2-month period in patients undergoing orthodontic treatment. Our study also showed that probiotic lozenges can be practically implemented in the clinical orthodontic setting, in terms of its acceptability by adolescents. Future probiotic studies should focus on bacterial strains, e.g., that of the S. salivarius M18 [1], with strong initial in vitro evidence to have anti-caries activities, the most effective dosage and frequency of administration for any strains or combination of strains and delivery vehicle. Future probiotic studies could also investigate combination therapy with chlorhexidine or fluoride to increase the probiotic's effectiveness and the possibility of incorporating a pretreatment phase of oral disinfection using chlorhexidine to reduce the oral bacterial load prior to probiotic administration favor probiotic colonization of the oral microbiome.
Conclusions
The results from this randomized, double-blind, parallel-group, placebo-controlled trial suggested that, although the Lorodent Probiotic Complex was not effective at improving the plaque index or the salivary and plaque levels of S. mutans among adolescents undergoing fixed orthodontic appliance therapy, there was high compliance and acceptability of the product. Future studies utilizing probiotics against oral diseases will need to focus on variables such as efficacious and higher dosages of bacterial strains and delivery vehicles, different dosages and frequencies of administration, and possible combinations with chlorhexidine and/or fluoride, and high bacterial enumeration.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by University of Toronto Human Ethics Board. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin. Informed consent was obtained from all individual participants included in the study.
Author Contributions
FE, SM, S-GG, PC, and JB conceived and designed the experiment. FE, SM, KJ, and KM performed the experiment. FE, SM, S-GG, IC, and CL analyzed the data. IC statistical analyses. FE, SM, and S-GG wrote the draft manuscript. All authors reviewed and approved the final manuscript.
Funding
This work was supported with funds from Ontario Centers for Excellence/Natural Sciences and Engineering Research Council (OCE/NSERC): Lead Investigator—Cadieux PA and Burton JP.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors wish to acknowledge the significant contributions of Ms. Natalya Yudina, CEO of Integra Medical, Inc., in providing the Lorodent lozenges and the placebo lozenges for the study.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/froh.2022.884683/full#supplementary-material
References
1. Burton JP, Drummond BK, Chilcott CN, Tagg JR, Thomson WM, Hale JD, et al. Influence of the probiotic Streptococcus salivarius strain M18 on indices of dental health in children: a randomized double-blind, placebo-controlled trial. J Med Microbiol. (2013) 62:875–84. doi: 10.1099/jmm.0.056663-0
2. Pitts NB, Zero DT, Marsh PD, Ekstrand K, Weintraub JA, Ramos-Gomez F, et al. Dental caries. Nat Rev Dis Primers. (2017) 3:17030. doi: 10.1038/nrdp.2017.30
3. Kinane DF. Causation and pathogenesis of periodontal disease. Periodontol (2000). (2001) 25:8–20. doi: 10.1034/j.1600-0757.2001.22250102.x
4. Tatakis DN, Kumar PS. Etiology and pathogenesis of periodontal diseases. Dent Clin North Am. (2005) 49:491–516. doi: 10.1016/j.cden.2005.03.001
5. Ranney R, Debski B, Tew J. Pathogenesis of gingivitis and periodontal disease in children and young adults. Pediatr Dent. (1981) 3:89–100.
6. Wiebe CB, Putnins EE. The periodontal disease classification system of the American Academy of Periodontology–an update. J Can Dent Assoc. (2000) 66:594–7.
7. Marsh PD. Dental plaque as a biofilm: the significance of pH in health and caries. Compend Contin Educ Dent. (2009) 30:76–78, 80, 83–77; quiz 88, 90.
8. Socransky SS, Haffajee AD. Periodontal microbial ecology. Periodontol (2000). (2005) 38:135–87. doi: 10.1111/j.1600-0757.2005.00107.x
9. Loesche WJ. Role of Streptococcus mutans in human dental decay. Microbiol Rev. (1986) 50:353–80. doi: 10.1128/mr.50.4.353-380.1986
10. Migliorati M, Isaia L, Cassaro A, Rivetti A, Silvestrini-Biavati F, Gastaldo L, et al. Efficacy of professional hygiene and prophylaxis on preventing plaque increase in orthodontic patients with multibracket appliances: a systematic review. Eur J Orthod. (2015) 37:297–307. doi: 10.1093/ejo/cju044
11. Benic GZ, Farella M, Morgan XC, Viswam J, Heng NC, Cannon RD, et al. Oral probiotics reduce halitosis in patients wearing orthodontic braces: a randomized, triple-blind, placebo-controlled trial. J Breath Res. (2019) 13:036010. doi: 10.1088/1752-7163/ab1c81
12. Meurman JH, Stamatova I. Probiotics: contributions to oral health. Oral Dis. (2007) 13:443–51. doi: 10.1111/j.1601-0825.2007.01386.x
13. Seminario-Amez M, López-López J, Estrugo-Devesa A, Ayuso-Montero R, Jané-Salas E. Probiotics and oral health: a systematic review. Med Oral Patol Oral Cir Bucal. (2017) 22:e282–8. doi: 10.4317/medoral.21494
14. Hill C, Guarner F, Reid G, Gibson GR, Merenstein DJ, Pot B, et al. Expert consensus document. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol. (2014) 11:506–14. doi: 10.1038/nrgastro.2014.66
15. Agossa K, Dubar M, Lemaire G, Blaizot A, Catteau C, Bocquet E, et al. Effect of Lactobacillus reuteri on gingival inflammation and composition of the oral microbiota in patients undergoing treatment with fixed orthodontic appliances: Study protocol of a randomized control trial. Pathogens. (2022) 11:112. doi: 10.3390/pathogens11020112
16. Bustamante M, Oomah BD, Mosi-Roa Y, Rubilar M, Burgos-Díaz C. Probiotics as an adjunct therapy for the treatment of halitosis, dental caries and periodontitis. Probiotics Antimicrob Proteins. (2020) 12:325–34. doi: 10.1007/s12602-019-9521-4
17. Gizani S, Petsi G, Twetman S, Caroni C, Makou M, Papagianoulis L. Effect of the probiotic bacterium Lactobacillus reuteri on white spot lesion development in orthodontic patients. Eur J Orthod. (2016) 38:85–9. doi: 10.1093/ejo/cjv015
18. Hasslöf P, Hedberg M, Twetman S, Stecksén-Blicks C. Growth inhibition of oral mutans streptococci and candida by commercial probiotic lactobacilli–an in vitro study. BMC Oral Health. (2010) 10:18. doi: 10.1186/1472-6831-10-18
19. Lin CW, Chen YT, Ho HH, Hsieh PS, Kuo YW, Lin JH, et al. Lozenges with probiotic strains enhance oral immune response and health. Oral Dis. (2021) 1–10. doi: 10.1111/odi.13854
20. Alp S, Baka ZM. Effects of probiotics on salivary Streptecoccus mutans and Lactobacillus levels in orthodontic patients. Am J Orthod Dentofacial Orthop. (2018) 154:517–23. doi: 10.1016/j.ajodo.2018.01.010
21. Hadj-Hamou R, Senok AC, Athanasiou AE, Kaklamanos EG. Do probiotics promote oral health during orthodontic treatment with fixed appliances? A systematic review. BMC Oral Health. (2020) 20:126. doi: 10.1186/s12903-020-01109-3
22. Pietri FK, Rossouw PE, Javed F, Michelogiannakis D. Role of probiotics in oral health maintenance among patients undergoing fixed orthodontic therapy: a systematic review of randomized controlled clinical trials. Probiotics Antimicrob Proteins. (2020) 12:1349–59. doi: 10.1007/s12602-020-09683-2
23. Zheng J, Wittouck S, Salvetti E, Franz CMAP, Harris HMB, Mattarelli P, et al. A taxonomic note on the genus Lactobacillus: description of 23 novel genera, emended description of the genus Lactobacillus. Beijerinck (1901) and union of Lactobacillaceae and Leuconostocaceae. Int J Syst Evol Microbiol. (2020) 70:2782–858. doi: 10.1099/ijsem.0.004107
24. Löe H. The gingival index, the plaque index and the retention index systems. J Periodontol. (1967) 38:610–6. doi: 10.1902/jop.1967.38.6.610
25. Vicario M, Santos A, Violant D, Nart J, Giner L. Clinical changes in periodontal subjects with the probiotic Lactobacillus reuteri Prodentis: a preliminary randomized clinical trial. Acta Odontol Scand. (2013) 71:813–9. doi: 10.3109/00016357.2012.734404
26. Vivekananda MR, Vandana KL, Bhat KG. Effect of the probiotic Lactobacilli reuteri (Prodentis) in the management of periodontal disease: a preliminary randomized clinical trial. J Oral Microbiol. (2010) 2. doi: 10.3402/jom.v2i0.5344
27. Burton JP, Cowley S, Simon RR, McKinney J, Wescombe PA, Tagg JR. Evaluation of safety and human tolerance of the oral probiotic Streptococcus salivarius K12: a randomized, placebo-controlled, double-blind study. Food Chem Toxicol. (2011) 49:2356–64. doi: 10.1016/j.fct.2011.06.038
28. Julien KC, Buschang PH, Campbell PM. Prevalence of white spot lesion formation during orthodontic treatment. Angle Orthod. (2013) 83:641–7. doi: 10.2319/071712-584.1
29. Khalaf K. Factors affecting the formation, severity and location of white spot lesions during orthodontic treatment with fixed appliances. J Oral Maxillofac Res. (2014) 5:e4. doi: 10.5037/jomr.2014.5104
30. Bader JD, Vollmer WM, Shugars DA, Gilbert GH, Amaechi BT, Brown JP, et al. Results from the Xylitol for adult caries trial (X-ACT). J Am Dent Assoc. (2013) 144:21–30. doi: 10.14219/jada.archive.2013.0010
31. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. (1977) 33:159–74. doi: 10.2307/2529310
32. De David SC, Mário TG, De Freitas GC, Kantorski KZ, Wikesjö UME, Moreira CHC. Correlation between plaque control and gingival health using short and extended oral hygiene intervals. Clin Oral Investig. (2018) 22:2593–7. doi: 10.1007/s00784-018-2358-5
33. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. (2009) 41:1149–60. doi: 10.3758/BRM.41.4.1149
34. Kohar N, Emmanuel V, Astuti L. Comparison between probiotic lozenges and drinks towards periodontal status improvement of orthodontic patients. Dental J (Majalah Kedokteran Gigi). (2020) 48:126–9. doi: 10.20473/j.djmkg.v48.i3.p126-129
35. Arweiler NB, Auschill TM, Heumann C, Hellwig E, Al-Ahmad A. Influence of probiotics on the salivary microflora oral streptococci and their integration into oral biofilm. Antibiotics. (2020) 9:803. doi: 10.3390/antibiotics9110803
36. Nadelman P, Magno MB, Masterson D, da Cruz AG, Maia LC. Are dairy products containing probiotics beneficial for oral health? A systematic review and meta-analysis. Clin Oral Investig. (2018) 22:2763–85. doi: 10.1007/s00784-018-2682-9
37. Stecksén-Blicks C, Renfors G, Oscarson ND, Bergstrand F, Twetman S. Caries-preventive effectiveness of a fluoride varnish: a randomized controlled trial in adolescents with fixed orthodontic appliances. Caries Res. (2007) 41:455–9. doi: 10.1159/000107932
38. Toiviainen A, Jalasvuori H, Lahti E, Gursoy U, Salminen S, Fontana M, et al. Impact of orally administered lozenges with Lactobacillus rhamnosus GG and Bifidobacterium animalis subsp. lactis BB-12 on the number of salivary mutans streptococci, amount of plaque, gingival inflammation and the oral microbiome in healthy adults. Clin Oral Investig. (2015) 19:77–83. doi: 10.1007/s00784-014-1221-6
39. Bowen WH, Pearson SK. Effect of milk on cariogenesis. Caries Res. (1993) 27:461–6. doi: 10.1159/000261581
40. Stecksén-Blicks C, Sjöström I, Twetman S. Effect of long-term consumption of milk supplemented with probiotic lactobacilli and fluoride on dental caries and general health in preschool children: a cluster-randomized study. Caries Res. (2009) 43:374–81. doi: 10.1159/000235581
41. Famularo G, De Simone C, Matteuzzi D, Pirovano F. Traditional and high potency probiotic preparations for oral bacteriotherapy. BioDrugs. (1999) 12:455–70. doi: 10.2165/00063030-199912060-00005
42. Timmerman HM, Koning CJ, Mulder L, Rombouts FM, Beynen AC. Monostrain, multistrain and multispecies probiotics–A comparison of functionality and efficacy. Int J Food Microbiol. (2004) 96:219–33. doi: 10.1016/j.ijfoodmicro.2004.05.012
43. Petersson LG, Magnusson K, Hakestam U, Baigi A, Twetman S. Reversal of primary root caries lesions after daily intake of milk supplemented with fluoride and probiotic lactobacilli in older adults. Acta Odontol Scand. (2011) 69:321–7. doi: 10.3109/00016357.2011.568962
44. Staples B, Bravender T. Drug compliance in adolescents: assessing and managing modifiable risk factors. Paediatr Drugs. (2002) 4:503–13. doi: 10.2165/00128072-200204080-00003
45. Ashley FP, Usiskin LA, Wilson RF, Wagaiyu E. The relationship between irregularity of the incisor teeth, plaque, and gingivitis: a study in a group of schoolchildren aged 11-14 years. Eur J Orthod. (1998) 20:65–72. doi: 10.1093/ejo/20.1.65
46. Rosenbloom RG, Tinanoff N. Salivary Streptococcus mutans levels in patients before, during, and after orthodontic treatment. Am J Orthod Dentofacial Orthop. (1991) 100:35–7. doi: 10.1016/0889-5406(91)70046-Y
47. Aminabadi NA, Erfanparast L, Ebrahimi A, Oskouei SG. Effect of chlorhexidine pretreatment on the stability of salivary lactobacilli probiotic in six- to twelve-year-old children: a randomized controlled trial. Caries Res. (2011) 45:148–54. doi: 10.1159/000325741
48. Sanz M, Beighton D, Curtis MA, Cury JA, Dige I, Dommisch H, et al. Role of microbial biofilms in the maintenance of oral health and in the development of dental caries and periodontal diseases. Consensus report of group 1 of the Joint EFP/ORCA workshop on the boundaries between caries and periodontal disease. J Clin Periodontol. (2017) 44(Suppl. 18):S5–11. doi: 10.1111/jcpe.12682
49. Beberhold K, Sachse-Kulp A, Schwestka-Polly R, Hornecker E, Ziebolz D. The Orthodontic Plaque Index: an oral hygiene index for patients with multibracket appliances. Orthodontics. (2012) 13:94–9.
Keywords: plaque indices, lozenges, Streptococcus mutans, saliva, supragingival plaque, compliance
Citation: Ebrahim F, Malek S, James K, MacDonald K, Cadieux P, Burton J, Cioffi I, Lévesque C and Gong S-G (2022) Effectiveness of the Lorodent Probiotic Lozenge in Reducing Plaque and Streptococcus mutans Levels in Orthodontic Patients: A Double-Blind Randomized Control Trial. Front. Oral. Health 3:884683. doi: 10.3389/froh.2022.884683
Received: 26 February 2022; Accepted: 28 March 2022;
Published: 27 April 2022.
Edited by:
Mohammed S. Razzaque, Lake Erie College of Osteopathic Medicine, United StatesReviewed by:
Vahid Rakhshan, Institute for Cognitive Science Studies, IranArthur C. Ouwehand, International Flavors and Fragrances, Finland
Copyright © 2022 Ebrahim, Malek, James, MacDonald, Cadieux, Burton, Cioffi, Lévesque and Gong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Siew-Ging Gong, c2cuZ29uZ0BkZW50aXN0cnkudXRvcm9udG8uY2E=
†These authors have contributed equally to this work