 Abedelmalek Kalefh Tabnjh
Abedelmalek Kalefh Tabnjh Sara Alizadehgharib3
Sara Alizadehgharib3 Peter Lingström
Peter Lingström- 1Department of Cariology, Institute of Odontology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 2Department of Applied Dental Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid, Jordan
- 3Department of Oral Microbiology and Immunology, Institute of Odontology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
Introduction: Smoking and the use of electronic cigarettes (e-cigs) are common practices that have significant consequences for oral health. Although the negative impact of traditional tobacco products on oral tissues is widely known, the emergence of e-cigs poses a new obstacle. This review summarises existing data on the influence of e-cigs on oral health, with a specific emphasis on dental caries and pro-inflammatory agents.
Methods: A comprehensive search was conducted via PubMed, Web of Science, Embase, and Scopus to identify relevant studies published until September 2024. The structured search strategy uncovered 42 articles that were read in full text. The included articles consisted of clinical trials, observational studies, and laboratory investigations that examined the impact of e-cig aerosol on oral bacteria and pro-inflammatory markers and its potential to contribute to dental caries.
Results: The findings indicate that e-cig users may have a higher prevalence of dental caries compared with non-smokers. Most studies focusing on bacteria showed that vaping may inhibit normal flora, giving cariogenic bacteria a chance to grow more. This finding indicates a notable oral health risk associated with vaping. Meta-analyses suggest no effect of using e-cigs on the levels of TNF-α, IL-1β, IL-6, and IL-8 in saliva, even if it may affect their levels in GCF. However, in GCF, only one study reported TNF-α and IL-1β, and only two studies reported IL-6 and IL-8. Nevertheless, the effects of e-cigs on dental caries require further investigation since the data do not provide a clear picture.
Discussion: This review emphasises the necessity for ongoing research to clarify the mechanisms that cause these consequences and to guide public health policies aimed at reducing the harm caused by e-cigarettes.
Systematic Review Registration: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024537910, PROSPERO (CRD42024537910).
1 Introduction
Smoking is an epidemic habit that leads to behavioural, psychological, and physical dependence, similar to the use of other drugs such as alcohol, cocaine, and heroin (1). According to the Pan American Health Organization (PAHO) indicators for 2019, the tobacco epidemic claims the lives of over 8 million people annually, with more than 7 million deaths resulting directly from tobacco use and over 1.2 million from nonsmokers exposed to second-hand smoke (1). All forms of smoking have several well-documented negative impacts on the oral cavity (2), including dental caries, periodontal disorders, poor wound healing, and precancerous lesions that increase risk of oral carcinoma (3).
As an alternative to conventional tobacco products, tobacco-free electronic cigarettes (Electronic Nicotine Delivery Systems, ENDS), commonly referred to as e-cigarettes or vape pens, have gained popularity in recent years (4). The National Cancer Institute lists the components of an electronic cigarette as follows: a battery, a tank for holding liquid, a resistor for heating the liquid, a wick for absorbing liquid, and a nozzle used to inhale the produced aerosol. Among the components that may be included in the liquid within the storage tank are flavour additives (e.g., menthol, blueberry, and cinnamon), chemical additives (e.g., propylene and polyethylene glycol), and nicotine (1). Typically, organic cotton, used to absorb the liquid, is wrapped around a resistor—a high-temperature resistive wire alloy made of FeCrAl such as kanthal™. The battery provides the energy to heat the resistor, which creates the aerosol (5). A sensor detects airflow when the user inhales from the device, triggering the heating of the liquid in the cartridge, which leads to its evaporation. The vapor delivers nicotine to the user. Some of the nicotine can escape into the surrounding air when exhaled. The vapor temperature ranges between 40°C and 65°C. Manufacturers claim that a cartridge can provide ten to 250 puffs, equivalent to five to 30 cigarettes, depending on the brand (5).
There is growing concern about the potential effects of e-cigarettes on oral and dental health as their popularity has significantly increased in recent years (6). That is, there seems to be a connection between vaping and periodontal health (7). Studies on periodontal health have found that e-cigarette users, compared to non-tobacco users, exhibit higher levels of plaque index, clinical attachment loss, probing depth, and marginal bone loss (8). Additionally, a laboratory-based control study has demonstrated that oral fluids, such as gingival crevicular fluid (GCF) and unstimulated whole saliva, from nicotine users, express higher levels of immunoinflammatory biomarkers, including receptor activator of NF-kappa B ligand, interleukin (IL)-1β, and tumour necrosis factor-alpha (TNF-α) (8).
Research on the effects of vaping on dental caries remains limited. Following inhalation, some constituents of the vaping aerosol adhere to the soft and hard tissues of the oral cavity (9). Vaping generates a viscous aerosol that not only promotes biofilm formation and microbial adhesion but also alters the normal oral flora by inhibiting beneficial gram-positive bacteria and encouraging the growth of harmful gram-negative bacteria. The depletion of gram-positive bacteria in the oral cavity may contribute to caries development by facilitating the adhesion of S. mutans to the enamel (10).
Various e-liquids exhibit physical and chemical characteristics similar to sugary food (11). As sucrose is the main ingredient in many flavours, it can significantly increase both biofilm growth and enamel demineralization, findings confirmed by in vitro investigation (7). A major concern is that sucrose and other sugars are often not listed on product labels, potentially leading to consumer misunderstandings about the safety, risks, and contents of both unheated or heated e-cigarette liquids (12). Additionally, the glycerol and propylene glycol found in e-cigarettes promote water absorption, which may lead to xerostomia or dry mouth, further increasing the risk of dental caries (13).
In conclusion, many studies suggest that electronic cigarette use negatively affects oral health, including an increased risk of dental caries due to changes in normal flora, promotion of cariogenic bacteria, biofilm adhesion, sugar production, and xerostomia (7, 14–17). These findings highlight the need for further research to clarify the relationship between vaping and dental caries. This systematic review explores the effects of vaping on oral health, particularly on dental caries and proinflammatory markers.
2 Materials and methods
2.1 Study registration and format
The review methodology followed to PRISMA principles (18) and was registered in PROSPERO (CRD42024537910) (19).
2.2 Population, exposure, comparison and outcomes (PECOs)
The following PECOs guided the formulation of the research question: P (population)—human cells or oral bacteria exposed to e-cigs or smokers who use e-cigs; E (exposure)—smoking electronic cigarettes or the vapour produced by them; C (comparison)—smokers (CS) and non-smokers (NS); and Os (outcomes)—both clinically evaluated and user-reported changes in proinflammatory markers and variables associated with dental caries caused by e-cigs.
2.3 Inclusion and exclusion criteria
The following inclusion criteria were used: observational and interventional studies on e-cigs and its effects on dental caries or proinflammatory markers; studies including any age or sex; laboratory studies considering oral bacteria or human oral cells; and studies written in English, without time limits.
The following exclusion criteria were used: all review studies and meta-analyses; case reports or case series studies; studies with unclear information; papers not focusing on dental caries or proinflammatory markers; comment articles; and posters or conference abstracts.
To prevent unit-of-analysis mistakes in cases where some of the studies included data from paired or repeated observations of participants, The Cochrane Handbook for Systematic Reviews of Interventions (Section 9.3.3) was consulted (20).
2.4 Search strategies
For every database, a specific search plan was created, considering variations in syntax rules and restricted vocabulary (AT). The search strategy used for each database is provided in the Supplementary Material.
2.5 Electronic search
One author (AT) conducted the electronic search across four databases: PubMed, Embase, Web of Science, and Scopus. The search was performed in April 2024 and updated in September 2024. Endnote 21® software was used to check all references for duplicates and study selection. This resulted in more relevant records, which were manually searched using the reference lists of the listed studies.
2.6 Study selection
After removing duplicates, two authors (AT and SA) independently screened the references by title and abstract using the Systematic Review Accelerator website (https://pubmed.ncbi.nlm.nih.gov/32004673/) (21). In case of a disagreement, confirmation was obtained after consulting with a third author (PL). Cohen's Kappa value was used to determine the agreement between the two screeners.
2.7 Data extraction
The extracted data summarised the studies into three major categories: studies focusing on caries-related variables (Table 1), studies focusing on cariogenic bacteria (Table 2), and studies focusing on proinflammatory markers (Table 3). Table 1 lists the variables: age, study type, records type (clinical or surveys), the country of the study, groups included in the study, sample size, study parameters, and outcomes. Table 2 lists the variables: country, study design and type, study groups, study aims, and conclusion. Table 3 lists the variables: age, sex, study design, inclusion criteria for the ES group, the study groups, sample size, the aim of the study, the study parameters, and the conclusion.
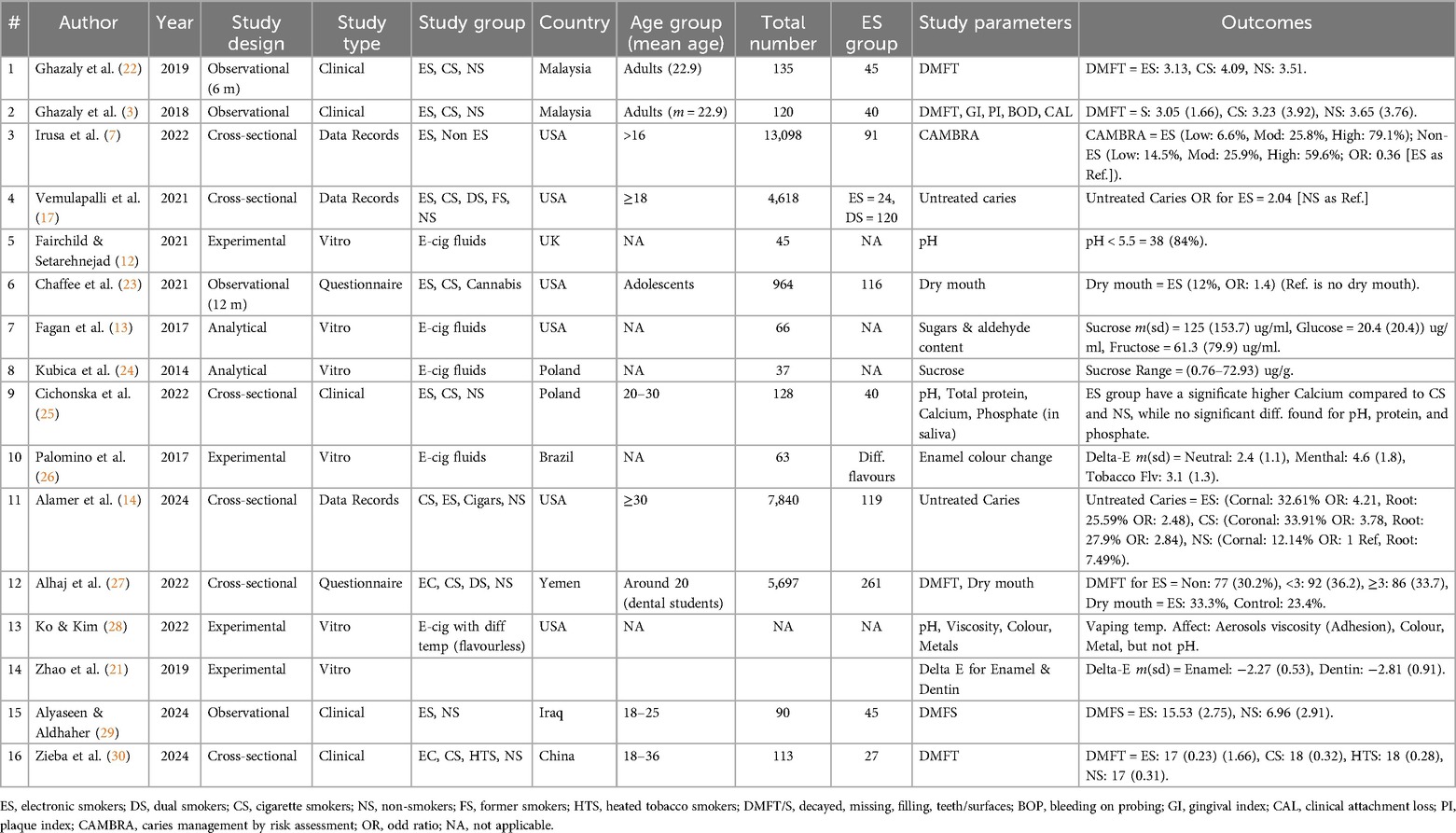
Table 1. Studies on vaping and dental caries-related variables from PubMed, Embase, Web of Science, and Scopus, up to September 2024, N = 16.
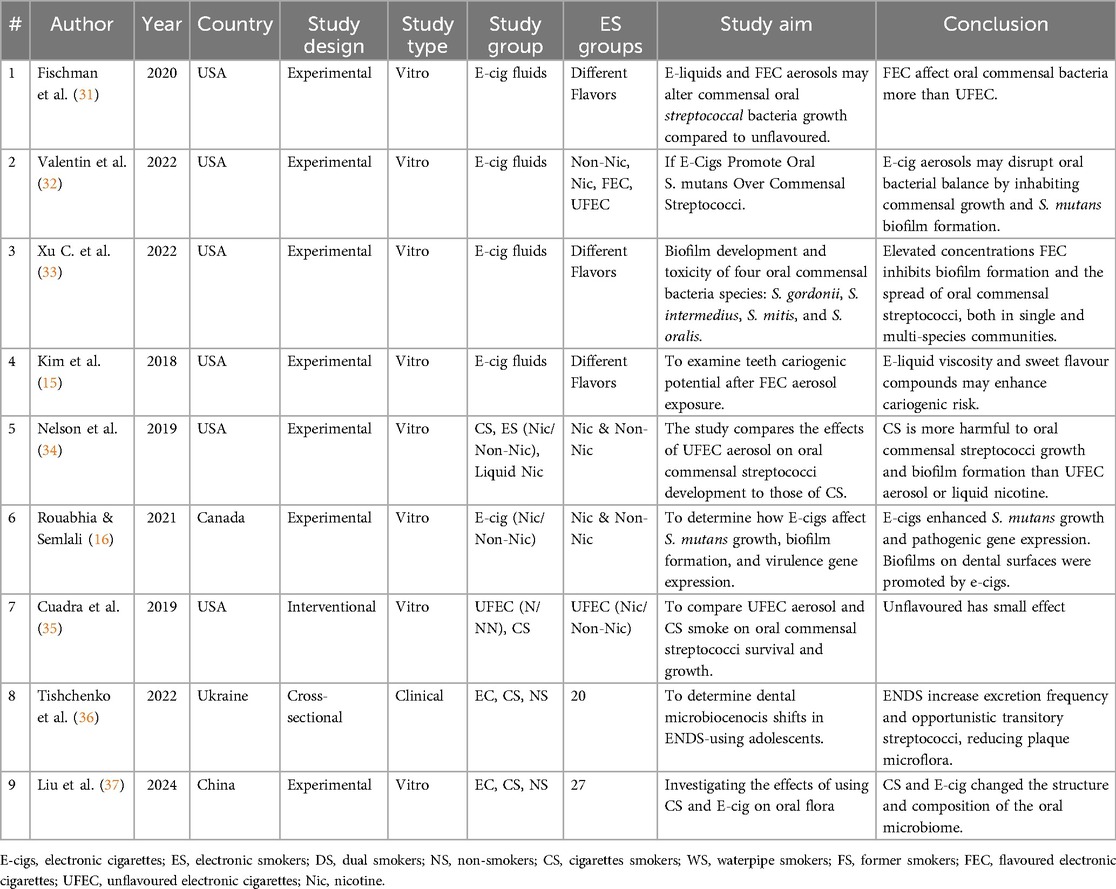
Table 2. Studies on vaping and bacteria from PubMed, Embase, Web of Science, and Scopus, up to September 2024, N = 9.
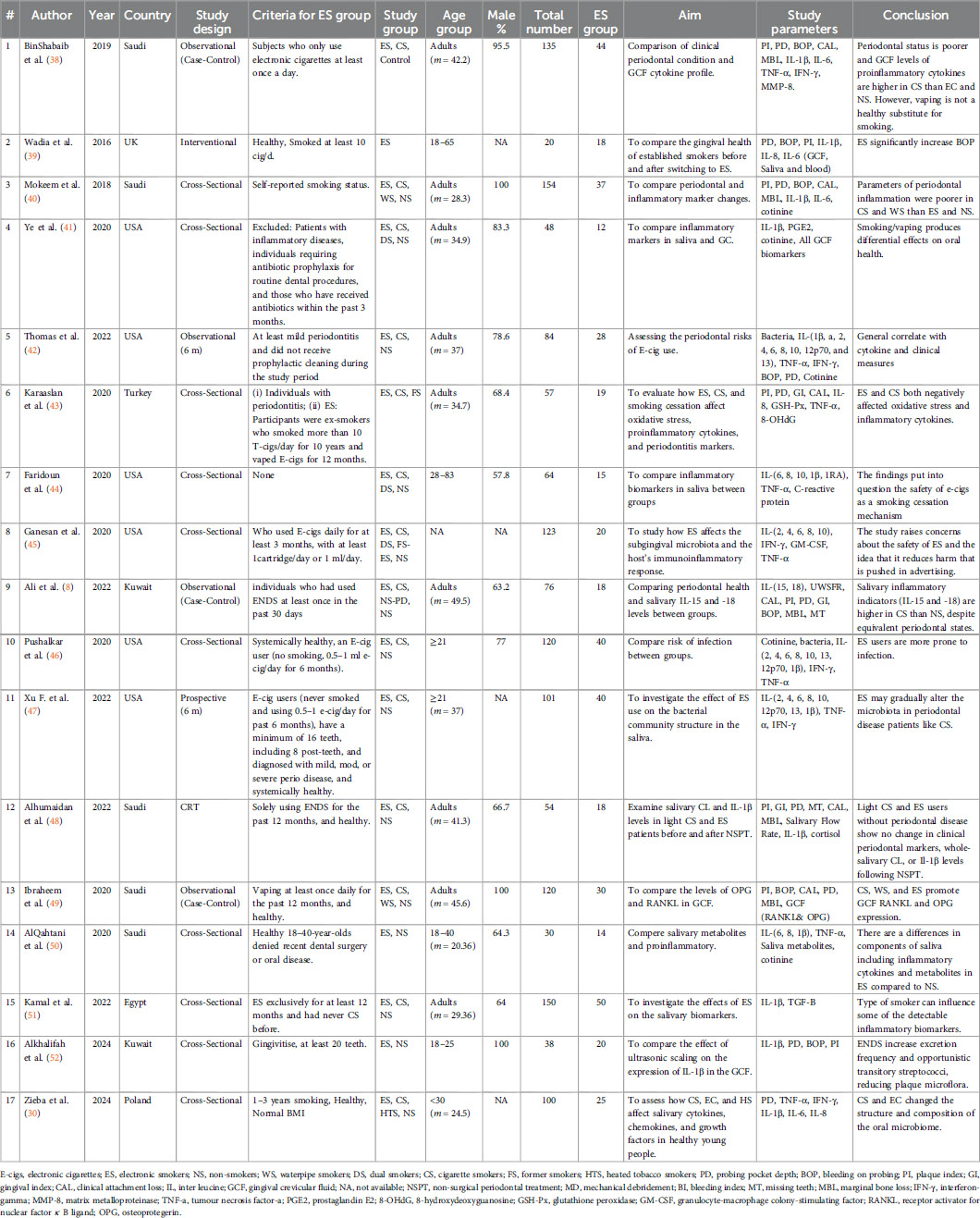
Table 3. Studies on vaping and proinflammatory markers from PubMed, Embase, Web of Science, and Scopus, up to September 2024, N = 17.
When the data were reported just as graphs, the WebPlotDigitizer tool was used (53). Moreover, data reported in forms other than means and SD (e.g., median, IQR, standard error, or confidence intervals) were converted to mean and SD.
2.8 Risk of bias
The quality of cross-sectional and cohort studies was assessed using the JBI Critical appraisal tool (54). The Risk of Bias Approach for Laboratory Studies (55) was used for articles with an exclusive ex vivo or in vitro design. Two reviewers (AT and SA) conducted the assessments, and discussion resolved the differences in evaluations (Figure 1).
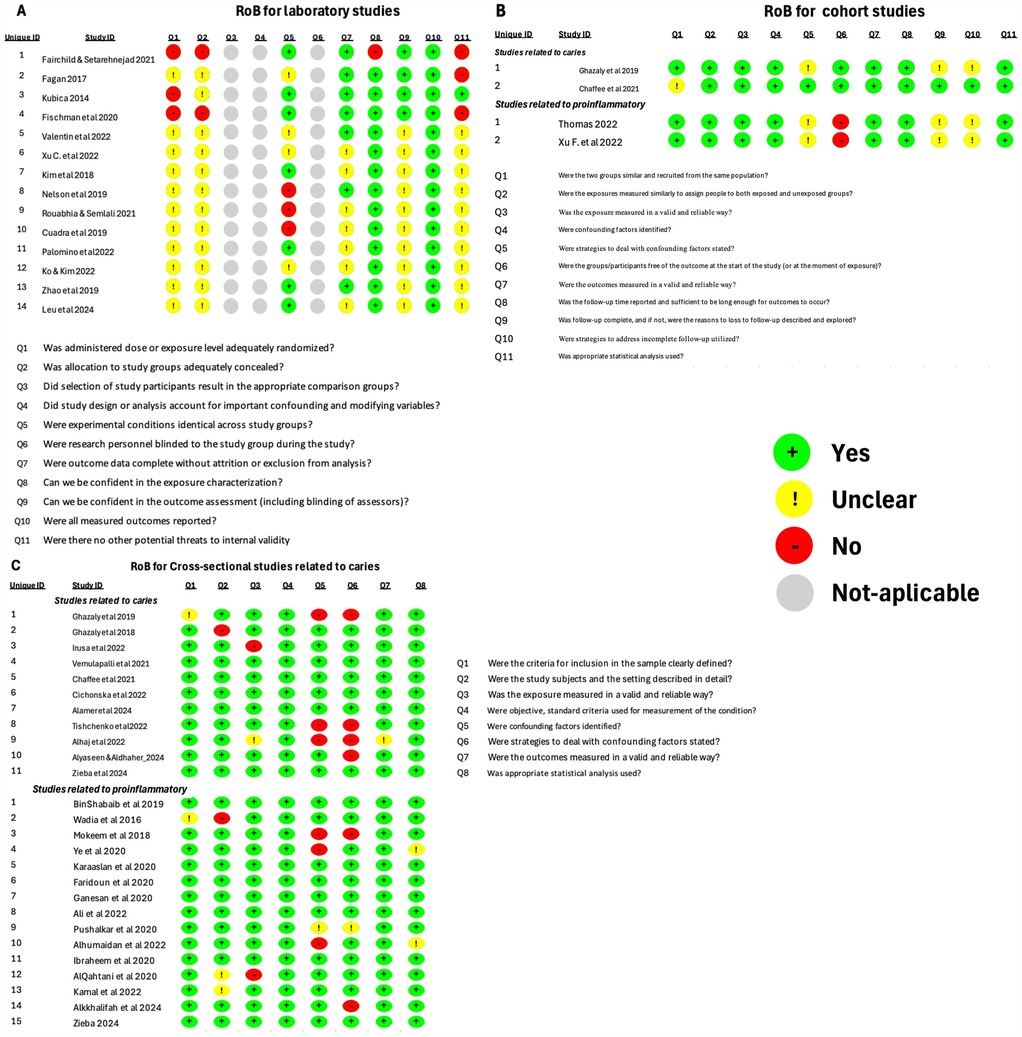
Figure 1. Risk of bias (RoB) analysis. (A) RoB for laboratory studies. (B) RoB for cohort studies. (C) RoB for cross-sectional studies.
2.9 Data synthesis
Meta-analyses were carried out when at least three studies compared and reported the same data. Cohen's D effect size and 95% CIs were the main impact measures (56).
Analyses were done with SPSS 29.0.1.0. The random-effects model estimate of variance was adopted since considerable heterogeneity was expected between studies, and wider confidence intervals help deal with the influence of size uncertainty. The I2 statistics show the percentage of study variation caused by heterogeneity rather than chance. Heterogeneity was evaluated as low (<40%), moderate (40%–60%), substantial (61%–90%), and considerable (91%–100%) (20). To examine heterogeneity, we compared study variables such as participant, intervention, and result similarities as described in the inclusion criteria. Subgroup analysis was performed to explore the influence of study characteristics such as proinflammatory markers in different media (GCF and saliva).
3 Results
3.1 Search
A total of 192 papers were retrieved for studies related to vaping and dental caries. With a manual search, nine more articles were discovered. After duplicates (n = 60) were removed, 141 articles were checked for title and abstract. The Cohen's Kappa value was 0.747 and the two authors' percentage of agreement was 90.8%. Finally, 46 articles were obtained in full-text, and 21 of these articles were eliminated after reading the full text because they did not meet the inclusion criteria. At the end, N = 25 (Figure 2). All of the studies reviewed were published between 2014 and 2024.
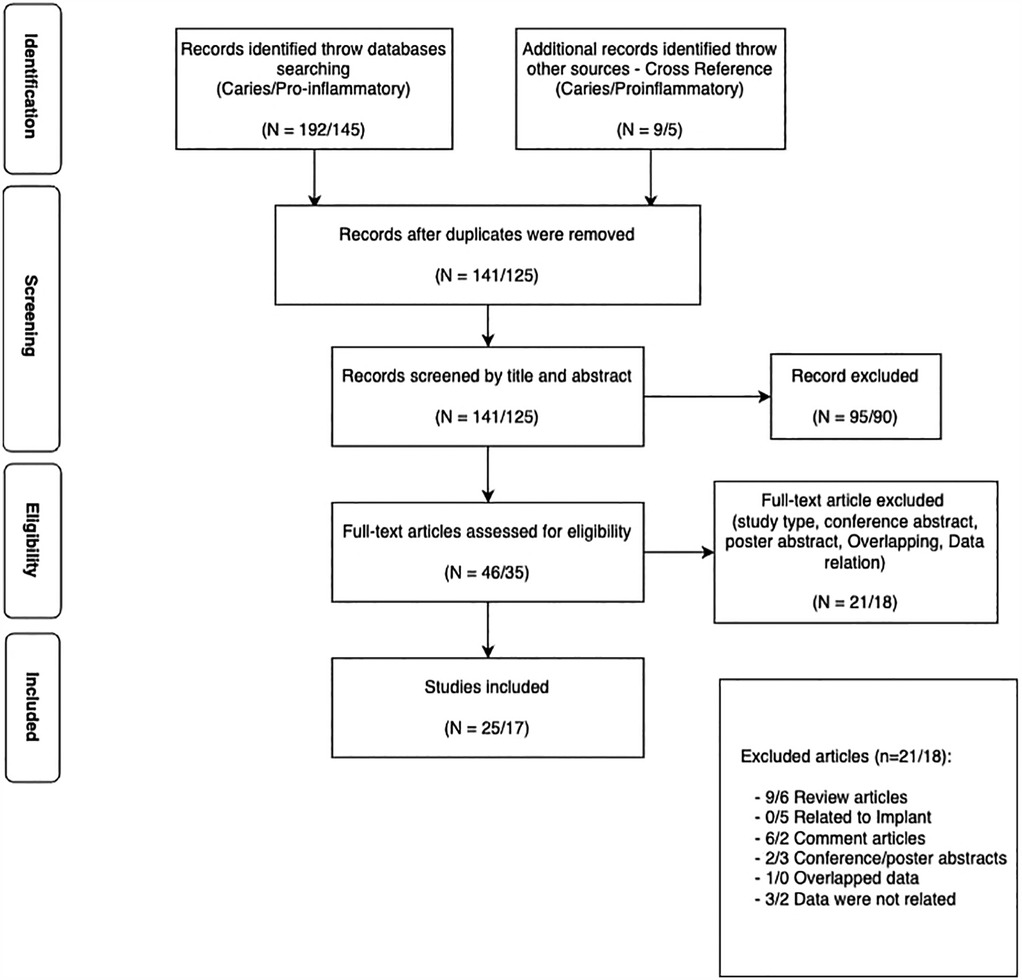
Figure 2. Flow diagram of the selection process of the studies included in the systematic review.
A total of 145 articles about vaping and proinflammatory-related studies were retrieved. Five additional articles were identified through cross-referencing. Following the removal of duplicates (n = 25), a total of 125 papers were screened based on their titles and abstracts. The inter-rater agreement between the two screeners was 96.6%, reflected by a Cohen's Kappa score of 0.909. A total of 35 papers were acquired in full-text format, and 18 of these were excluded following full-text reading due to non-compliance with the inclusion criteria. At the end, N = 17 (Figure 1). All included studies were published between 2018 and 2024. Every effort was made to acquire original data from the authors as required.
3.2 Data synthesis
Of the 25 studies focusing on caries, 14 studies were of laboratory design, nine were cross-sectional design, and two were cohort design. Sixteen studies focused on caries-related variables such as decayed, missing, and filled teeth (DMFT) index, sugar concentrations, dry mouth, untreated caries, pH, caries risk assessment, metal concentrations, and colour change. Five studies were based on questionnaires or data records, six were in vitro studies, and five were clinical studies (Table 1). The remaining nine studies focused on the effects of ENDS on cariogenic bacteria (Table 2). The main variables in those studies were bacterial growth, hardness loss, adhesion, and biofilm. Streptococcus species were the common types within all those articles.
Most of the 17 studies focusing on inflammation were cross-sectional (just two were cohort studies), comparing vaping groups with other groups such as tobacco smokers and non-smokers, and just three studies included the water-pipe smokers as a group. Of these, 12 studies measured the outcome in the saliva, four used GCF, and one, a pilot study, used saliva, GCF, and serum simultaneously (Table 3). The following were the most common proinflammatory markers and other measured parameters: volume, IL-1β, IL-6, IL-8, IFN-γ, TNF-α, UWSFR, and GCF volume. Other inflammatory markers included MMP-8, MMP-9, PGE2, TGF-β, OPG, GM-CSF, GsH-Px, 8-OHdG-IL, 8-OHdG-a, 8-OHdG-1RA, 8-OHdG-2, 8-OHdG-4, 8-OHdG-10, 8-OHdG-12p70, 8-OHdG-13, 8-OHdG-15, and 8-OHdG-18, and cotinine).
Most Laboratory and cohort studies showed an overall risk of bias that is probably moderate (12, 13, 15, 16, 21–24, 26, 28, 31–35, 37, 42, 47). On the other hand, all cross-sectional studies showed a “probably low” risk of bias (3, 7, 8, 14, 17, 22, 23, 25, 29, 30, 36, 38–41, 43–46, 48–52), with the exception of one study, which showed a “probably moderate” risk of bias (27).
3.3 Results of included studies
3.3.1 Vaping and dental caries
Studies done regarding caries showed that users of ENDS (Electronic Nicotine Delivery Systems) may be at a higher risk for dental caries (7) and tend to have more untreated caries scores than non-smokers (14, 17). The results also indicate that users of ENDS experience dry mouth more frequently than non-smokers (23, 27). Studies that focused on ENDS's effects on bacteria revealed that ENDS inhibit normal flora without affecting S. mutans at concentrations of 5% or more, and this inhibition allows S. mutans to proliferate, increasing the risk of dental caries. However, ENDS with lower concentrations have minimal or no effect on oral Streptococcus species in the mouth (15, 16, 31–36).
3.3.2 Vaping and proinflammatory factors
The results indicate a complex relationship between conventional smoking (CS), electronic smoking (ES), and proinflammatory factors. Compared to electronic cigarette smokers (ES) and non-smokers (NS), cigarette smokers (CS) generally exhibit worse periodontal conditions and higher levels of proinflammatory cytokines in GCF (39, 41). Both CS and ES have comparable detrimental effects on oxidative stress markers and inflammatory cytokines, and they are linked to increased expression of inflammatory biomarkers such as RANKL, OPG, IL-15, and IL-18 (8). The notion that ES is a safer smoking cessation aid is challenged by findings that people who use ES devices may also be more susceptible to infections and experience alterations in their oral microbiome, which could lead to oral imbalance (45, 46, 51, 52). However, when it comes to salivary proinflammatory markers such as IL-1β, IL-6, IL-8, and TNF-α, most studies reported no significant difference between users of ES devices and non-smokers (8, 40–42, 46, 51). These findings raise serious concerns about the safety of e-cigs and question the common harm reduction narrative associated with them, as the findings suggest that e-cigs negatively affect oral health in general and inflammatory responses in particular.
3.4 Meta-analysis
Meta-analyses were conducted for DMFT/DMFS (Decayed, Missing, Filled Teeth/Surfaces) scores and the most common proinflammatory markers, provided that at least three studies reported on each marker. The selected markers were IL-1β, IL-6, IL-8, and TNF-α. Cohen's d effect size was used to test the data. The meta-analyses also considered different media, including GCF and saliva, as subgroups.
3.4.1 DMFT
A meta-analysis was conducted on three studies (22, 29, 30) that reported DMFT/DMFS (Figure 3A). A high heterogeneity was found between studies (T2 = 3.19, I2 = 0.98). Two studies reported DMFT (22, 30) and the other one reported DMFS (29).
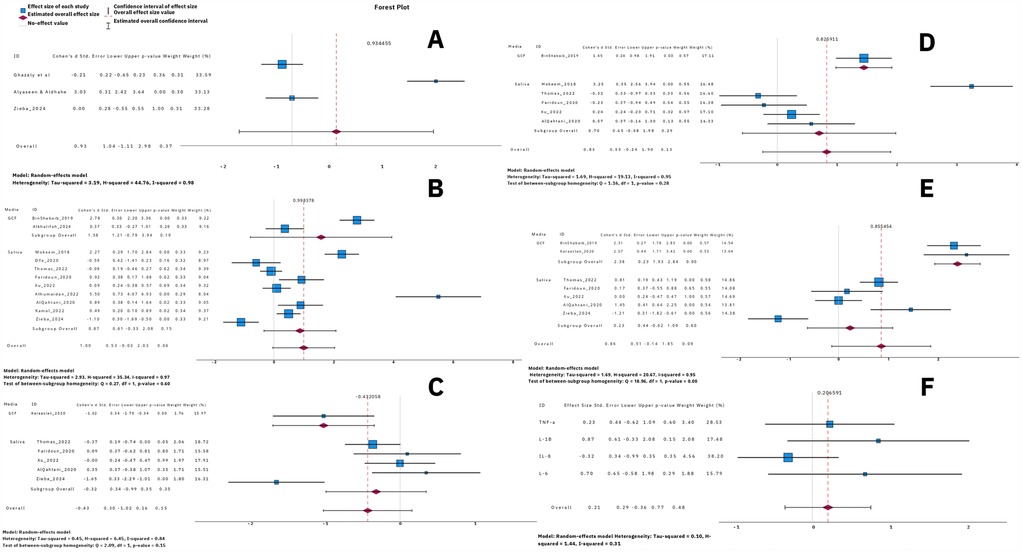
Figure 3. Forest plots for caries and proinflammatory markers. (A) DMFT, (B) IL-1β, (C) IL-8, (D) IL-6, (E) TNF-a, and (F) all salivary proinflammatory markers—IL-1β, IL-6, IL-8, and TNF-α.
3.4.2 IL-1β
A meta-analysis was conducted on eleven studies (30, 38, 40–42, 44, 47, 48, 50–52) that reported IL-1β (Figure 3B). A high heterogeneity was found between studies (T2 = 2.93, I2 = 0.97). Two studies reported IL-1β in GCF and nine in saliva. The heterogeneity between saliva studies was high (T2 = 3.25, I2 = 0.97).
3.4.3 IL-8
A meta-analysis was conducted on six studies (30, 42–44, 47, 50) that reported IL-8 (Figure 3C). A moderate heterogeneity was found between studies (T2 = 0.45, I2 = 0.84). One study reported IL-8 in GCF and five in saliva. The heterogeneity between saliva studies was moderate (T2 = 0.49, I2 = 0.86).
3.4.4 IL-6
A meta-analysis was conducted on six studies (38, 40, 42, 44, 47, 50) that reported IL-6 (Figure 3D). A high heterogeneity was found between studies (T2 = 1.69, I2 = 0.95). One study reported IL-6 in GCF and five in saliva. The heterogeneity between saliva studies was high (T2 = 2.03, I2 = 0.95).
3.4.5 TNF-α
A meta-analysis was conducted on seven studies (30, 38, 42–44, 47, 50) that reported TNF-α (Figure 3E). A high heterogeneity was found between studies (T2 = 1.96, I2 = 0.95). Two studies reported TNF-α in GCF and five in saliva. The heterogeneity between saliva studies was high (T2 = 0.86, I2 = 0.91).
3.4.6 For all markers
A meta-analysis was conducted on all the proinflammatory markers (IL-1β, IL-6, IL-8, and TNF-α) in saliva using the effect size from the meta-analysis for each marker (Figure 3F). Low heterogeneity was found between the markers (T2 = 0.1, I2 = 0.31). The results suggest that vaping does not affect the level of these markers in saliva.
4 Discussion
This systematic review explores the effect of vaping on oral health in general, with a particular focus on dental caries and proinflammatory markers. The findings indicate that the effect of ENDS on dental caries and proinflammatory markers remains unclear and therefore requires further investigation. Most studies included in the meta-analysis had the same risk of bias and shared similar designs, so there was no need for sensitivity analysis.
The review identified various studies that examined multiple criteria related to dental caries. The impact of vaping on the increased risk of dental caries is a concerning trend. Some studies have demonstrated that users of ENDS exhibit a greater prevalence of dental caries compared to non-smokers (29). Furthermore, users ENDS reported a higher prevalence of untreated caries and xerostomia, potentially elevating the risk of dental caries (14, 17, 23, 27). Numerous studies have suggested that vaping alters the composition of the oral microbiota (15, 16, 31–33, 36, 37). These studies indicate that vaping may disrupt the normal flora, facilitating the growth of cariogenic bacteria such as S. mutans, which may replace healthy flora. The change in microbial composition and increased biofilm adherence and sugar production create an environment conducive to tooth demineralization and the development of dental caries. Furthermore, the findings indicate that the concentration of vaping liquid and flavours may influence the degree of caries risk (31, 33, 35). Higher concentrations appear to cause greater alterations in the normal flora. However, the evidence remains ambiguous, and further research is needed to better understand how vaping increases the risk of dental caries and to establish causative links.
Some studies suggest that vaping is associated with changes in some proinflammatory markers (41–46), but some studies report conflicting findings (38–40, 44, 47, 48, 51). A meta-analysis of common markers reported in this study (IL-1β, IL-6, IL-8, and TNF-α) found no significant association between vaping and these markers in saliva. However, potential connections were observed in GCF. After reviewing the outlier studies, we found that most of the heterogeneity stemmed from studies with small standard deviations, which had a significant effect size despite means similar to other studies.
The implications of these findings are significant for global health and the dental practice. As vaping continues to gain popularity, dental professionals should be aware of its potential oral health consequences. This study suggests that while ENDS may be less harmful in certain respects compared to conventional smoking, ENDS are not a completely safe alternative as they may be associated with negative oral health effects. Consequently, comprehensive education on the potential risks of vaping is crucial, particularly for young people and teenagers.
4.1 Limitations
Despite the significance of the findings of this study, several limitations must be considered. The heterogeneity in study design, participants, and methodologies complicates drawing definitive conclusions. Furthermore, several studies failed to adequately account for confounding factors, which compromises the validity of the results. Moreover, the reliance on self-reported data in several studies raises concerns about accuracy.
Future research should use a longitudinal design to focus on the long-term impacts of ENDS on oral health. Investigating how vaping impacts normal flora and inflammatory responses will elucidate the pathways contributing to dental caries. Furthermore, future studies should explore the effects of various vaping devices, temperatures, and flavours, as these elements may significantly influence oral health. In addition, research should aim to standardise methods and include larger, more diverse populations to improve generalizability.
5 Conclusion
The conclusions from this study highlight the possible adverse effects of ENDS on oral health, particularly concerning proinflammatory indicators and dental caries. The findings suggest that vaping may increase the risk of dental caries due to alterations in the normal oral flora and the growth of cariogenic bacteria. Although the meta-analyses indicated no significant impact of vaping on major salivary proinflammatory markers, they suggested a potential effect on salivary markers in the GCF. However, research on GCF remains limited. The existing literature is inconsistent and limited, indicating the need for further studies to better understand these associations and inform public health strategies aimed at reducing the risks associated with vaping.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
AT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. SA: Conceptualization, Data curation, Investigation, Methodology, Supervision, Writing – review & editing. GC: Methodology, Supervision, Writing – review & editing. PL: Conceptualization, Investigation, Project administration, Resources, Supervision, Validation, Writing – review & editing, Methodology.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/froh.2025.1569806/full#supplementary-material
References
1. Costa MB, Brito EN, Renovato SR, Rodrigues RV. Relationship Between E-Cigarette Use and Oral Health: An Integrative Literature Review. Paraná: Seven Publicações Ltda (2023).
2. Ford PJ, Rich AM. Tobacco use and oral health. Addiction. (2021) 116(12):3531–40. doi: 10.1111/add.15513
3. Ghazali AF, Ismail AF, Faisal GG, Halil MH, Daud A. Oral health of smokers and e-cigarette users: a case-control study. J Int Dent Med Res. (2018) 11(2):428–32.
4. Saad MS. The impact of E-cigarettes on oral and dental health: narrative review. Saudi J Med Pharm Sci. (2023) 9(12):863–7. doi: 10.36348/sjmps.2023.v09i12.014
5. Knorst MM, Benedetto IG, Hoffmeister MC, Gazzana MB. The electronic cigarette: the new cigarette of the 21st century? J Bras Pneumol. (2014) 40(5):564–72. doi: 10.1590/S1806-37132014000500013
6. Grana RA, Popova L, Ling PM. A longitudinal analysis of electronic cigarette use and smoking cessation. JAMA Intern Med. (2014) 174(5):812–3. doi: 10.1001/jamainternmed.2014.187
7. Irusa KF, Finkelman M, Magnuson B, Donovan T, Eisen SE. A comparison of the caries risk between patients who use vapes or electronic cigarettes and those who do not: a cross-sectional study. J Am Dent Assoc. (2022) 153(12):1179–83. doi: 10.1016/j.adaj.2022.09.013
8. Ali D, Kuyunov I, Baskaradoss JK, Mikami T. Comparison of periodontal status and salivary IL-15 and -18 levels in cigarette-smokers and individuals using electronic nicotine delivery systems. BMC Oral Health. (2022) 22(1):655. doi: 10.1186/s12903-022-02700-6
9. Ruddick JA. Toxicology, metabolism, and biochemistry of 1, 2-propanediol. Toxicol Appl Pharmacol. (1972) 21(1):102–11. doi: 10.1016/0041-008X(72)90032-4
10. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. (2009) 151(4):W-65–94. doi: 10.7326/0003-4819-151-4-200908180-00136
11. Bakerywala A, Agarwal A, Shaikh H. Effects of E-cigarettes (vaping) on the oral microbiome–a narrative review. Oral Maxillofac Pathol J. (2024) 15(1):81–6.
12. Fairchild R, Setarehnejad A. Erosive potential of commonly available vapes: a cause for concern? Br Dent J. (2021) 231(8):487–91. doi: 10.1038/s41415-021-3563-1
13. Fagan P, Pokhrel P, Herzog TA, Moolchan ET, Cassel KD, Franke AA, et al. Sugar and aldehyde content in flavored electronic cigarette liquids. Nicotine Tob Res. (2018) 20(8):985–92. doi: 10.1093/ntr/ntx234
14. Alamer NI, Alsaleh A, Alkhaldi S. Tobacco products and oral conditions among US adults: NHANES 2017–2020. J Public Health Dent. (2024) 84(2):206–12. doi: 10.1111/jphd.12615
15. Kim SA, Smith S, Beauchamp C, Song Y, Chiang M, Giuseppetti A, et al. Cariogenic potential of sweet flavors in electronic-cigarette liquids. PLoS One. (2018) 13(9):e0203717. doi: 10.1371/journal.pone.0203717
16. Rouabhia M, Semlali A. Electronic cigarette vapor increases Streptococcus mutans growth, adhesion, biofilm formation, and expression of the biofilm-associated genes. Oral Dis. (2021) 27(3):639–47. doi: 10.1111/odi.13564
17. Vemulapalli A, Mandapati SR, Kotha A, Aryal S. Association between vaping and untreated caries: a cross-sectional study of national health and nutrition examination survey 2017-2018 data. J Am Dent Assoc. (2021) 152(9):720–9. doi: 10.1016/j.adaj.2021.04.014
18. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
19. Muka T, Glisic M, Milic J, Verhoog S, Bohlius J, Bramer W, et al. A 24-step guide on how to design, conduct, and successfully publish a systematic review and meta-analysis in medical research. Eur J Epidemiol. (2020) 35(1):49–60. doi: 10.1007/s10654-019-00576-5
20. Higgins JPT, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. Br Med J. (2011) 343:d5928. doi: 10.1136/bmj.d5928
21. Zhao X, Zanetti F, Wang L, Pan J, Majeed S, Malmstrom H, et al. Effects of different discoloration challenges and whitening treatments on dental hard tissues and composite resin restorations. J Dent. (2019) 89:103182. doi: 10.1016/j.jdent.2019.103182
22. Ghazali AF, Ismail AF, Daud A. Caries experience among cigarette and E-cigarette users: a 6-month prospective study. J Pharm Sci Res. (2019) 11(7):2566–9.
23. Chaffee BW, Couch ET, Vora MV, Holliday RS. Oral and periodontal implications of tobacco and nicotine products. Periodontol 2000. (2021) 87(1):241–53. doi: 10.1111/prd.12395
24. Kubica P, Wasik A, Kot-Wasik A, Namieśnik J. An evaluation of sucrose as a possible contaminant in e-liquids for electronic cigarettes by hydrophilic interaction liquid chromatography-tandem mass spectrometry. Anal Bioanal Chem. (2014) 406(13):3013–8. doi: 10.1007/s00216-014-7690-2
25. Cichońska D, Kusiak A, Kochańska B, Ochocińska J, Świetlik D. Influence of electronic cigarettes on selected physicochemical properties of saliva. Int J Environ Res Public Health. (2022) 19(6):3314. doi: 10.3390/ijerph19063314
26. Pintado-Palomino K, de Almeida CVVB, Oliveira-Santos C, Pires-de-Souza FP, Tirapelli C. The effect of electronic cigarettes on dental enamel color. J Esthet Restor Dent. (2019) 31(2):160–5. doi: 10.1111/jerd.12436
27. Alhajj MN, Al-Maweri SA, Folayan MO, Halboub E, Khader Y, Omar R, et al. Oral health practices and self-reported adverse effects of E-cigarette use among dental students in 11 countries: an online survey. BMC Oral Health. (2022) 22(1):18. doi: 10.1186/s12903-022-02053-0
28. Ko TJ, Kim SA. Effect of heating on physicochemical property of aerosols during vaping. Int J Environ Res Public Health. (2022) 19(3):1892. doi: 10.3390/ijerph19031892
29. Alyaseen HA, Aldhaher ZA. The effect of new trend electronic cigarettes on dental caries in relation to glucosyltransferase B and secretory immunoglobulin A (a case-control study). Cell Biochem Biophys. (2024) 82(3):2865–71. doi: 10.1007/s12013-024-01401-x
30. Zięba S, Maciejczyk M, Antonowicz B, Porydzaj A, Szuta M, Lo Giudice G, et al. Comparison of smoking traditional, heat not burn and electronic cigarettes on salivary cytokine, chemokine and growth factor profile in healthy young adults-pilot study. Front Physiol. (2024) 15:1404944. doi: 10.3389/fphys.2024.1404944
31. Fischman JS, Sista S, Lee D, Cuadra GA, Palazzolo DL. Flavorless vs. flavored electronic cigarette-generated aerosol and E-liquid on the growth of common oral commensal streptococci. Front Physiol. (2020) 11:585416. doi: 10.3389/fphys.2020.585416
32. Catala-Valentin A, Bernard JN, Caldwell M, Maxson J, Moore SD, Andl CD. E-Cigarette aerosol exposure favors the growth and colonization of oral Streptococcus mutans compared to commensal streptococci. Microbiol Spectr. (2022) 10(2):e0242121. doi: 10.1128/spectrum.02421-21
33. Xu CP, Palazzolo DL, Cuadra GA. Mechanistic effects of E-liquids on biofilm formation and growth of oral commensal streptococcal communities: effect of flavoring agents. Dent J. (2022) 10(5):85. doi: 10.3390/dj10050085
34. Nelson JM, Cuadra GA, Palazzolo DL. A comparison of flavorless electronic cigarette-generated aerosol and conventional cigarette smoke on the planktonic growth of common oral commensal streptococci. Int J Environ Res Public Health. (2019) 16(24):5004. doi: 10.3390/ijerph16245004
35. Cuadra GA, Smith MT, Nelson JM, Loh EK, Palazzolo DL. A comparison of flavorless electronic cigarette-generated aerosol and conventional cigarette smoke on the survival and growth of common oral commensal streptococci. Int J Environ Res Public Health. (2019) 16(10):1669. doi: 10.3390/ijerph16101669
36. Tishchenko OV, Kryvenko LS, Gargina VV. Influence of smoking heating up tobacco products and e-cigarettes on the microbiota of dental plaque. Pol Merkur Lekarski. (2022) 50(295):16–20.35278292
37. Liu J, Yue Q, Zhang S, Xu J, Jiang X, Su Q, et al. A pilot study on oral microbiome in electronic cigarettes consumers versus traditional cigarettes smokers. Folia Microbiol. (2024) 70:147–58. doi: 10.1007/s12223-024-01185-w
38. BinShabaib M, ALHarthi SS, Akram Z, Khan J, Rahman I, Romanos GE, et al. Clinical periodontal status and gingival crevicular fluid cytokine profile among cigarette-smokers, electronic-cigarette users and never-smokers. Arch Oral Biol. (2019) 102:212–7. doi: 10.1016/j.archoralbio.2019.05.001
39. Wadia R, Booth V, Yap HF, Moyes DL. A pilot study of the gingival response when smokers switch from smoking to vaping. Br Dent J. (2016) 221(11):722–6. doi: 10.1038/sj.bdj.2016.914
40. Mokeem SA, Alasqah MN, Michelogiannakis D, Al-Kheraif AA, Romanos GE, Javed F, et al. Clinical and radiographic periodontal status and whole salivary cotinine, IL-1β and IL-6 levels in cigarette- and waterpipe-smokers and E-cig users. Environ Toxicol Pharmacol. (2018) 61:38–43. doi: 10.1016/j.etap.2018.05.016
41. Ye D, Gajendra S, Lawyer G, Jadeja N, Pishey D, Pathagunti S, et al. Inflammatory biomarkers and growth factors in saliva and gingival crevicular fluid of e-cigarette users, cigarette smokers, and dual smokers: a pilot study. J Periodontol. (2020) 91(10):1274–83. doi: 10.1002/JPER.19-0457
42. Thomas SC, Xu F, Pushalkar S, Lin Z, Thakor N, Vardhan M, et al. Electronic cigarette use promotes a unique periodontal microbiome. mBio. (2022) 13(1):e0007522. doi: 10.1128/mbio.00075-22
43. Karaaslan F, Dikilitaş A, Yiğit U. The effects of vaping electronic cigarettes on periodontitis. Aust Dent J. (2020) 65(2):143–9. doi: 10.1111/adj.12747
44. Faridoun A, Sultan AS, Jabra-Rizk MA, Weikel D, Varlotta S, Meiller TF. Salivary biomarker profiles in E-cigarette users and conventional smokers: a cross-sectional study. Oral Dis. (2021) 27(2):277–9. doi: 10.1111/odi.13533
45. Ganesan SM, Dabdoub SM, Nagaraja HN, Scott ML, Pamulapati S, Berman ML, et al. Adverse effects of electronic cigarettes on the disease-naive oral microbiome. Sci Adv. (2020) 6(22):eaaz0108. doi: 10.1126/sciadv.aaz0108
46. Pushalkar S, Paul B, Li Q, Yang J, Vasconcelos R, Makwana S, et al. Electronic cigarette aerosol modulates the oral microbiome and increases risk of infection. iScience. (2020) 23(3):100884. doi: 10.1016/j.isci.2020.100884
47. Xu F, Pushalkar S, Lin Z, Thomas SC, Persaud JK, Sierra MA, et al. Electronic cigarette use enriches periodontal pathogens. Mol Oral Microbiol. (2022) 37(2):63–76. doi: 10.1111/omi.12361
48. Alhumaidan AA, Al-Aali KA, Vohra F, Javed F, Abduljabbar T. Comparison of whole salivary cortisol and interleukin 1-beta levels in light cigarette-smokers and users of electronic nicotine delivery systems before and after non-surgical periodontal therapy. Int J Environ Res Public Health. (2022) 19(18):11290. doi: 10.3390/ijerph191811290
49. Ibraheem WI, Fageeh HI, Preethanath RS, Alzahrani FA, Al-Zawawi AS, Divakar DD, et al. Comparison of RANKL and osteoprotegerin levels in the gingival crevicular fluid of young cigarette- and waterpipe-smokers and individuals using electronic nicotine delivery systems. Arch Oral Biol. (2020) 115:104714. doi: 10.1016/j.archoralbio.2020.104714
50. Alqahtani S, Cooper B, Spears CA, Wright C, Shannahan J. Electronic nicotine delivery system-induced alterations in oral health via saliva assessment. Exp Biol Med. (2020) 245(15):1319–25. doi: 10.1177/1535370220941258
51. Kamal NM, Shams NS. The impact of tobacco smoking and electronic cigarette vaping on salivary biomarkers. A comparative study. Saudi Dental Journal. (2022) 34(5):404–9. doi: 10.1016/j.sdentj.2022.05.003
52. Alkhalifah AB, Alfuraih NT, Joseph B, Baskaradoss JK. Effect of scaling on levels of interleukin 1-beta and clinical periodontal parameters among e-cigarette users and non-smokers: a prospective study. Tob Induc Dis. (2024) 22. doi: 10.18332/tid/189552
54. Tufanaru C, Munn Z, Aromataris E, Campbell J, Hopp L. JBI Manual for Evidence Synthesis. Adelaide: Joanna Briggs Institute (2020).
55. Rooney AA, Boyles AL, Wolfe MS, Bucher JR, Thayer KA. Systematic review and evidence integration for literature-based environmental health science assessments. Environ Health Perspect. (2014) 122(7):711–8. doi: 10.1289/ehp.1307972
Keywords: dental caries, e-cigarettes, electronic smoking, proinflammatory markers, vaping
Citation: Tabnjh AK, Alizadehgharib S, Campus G and Lingström P (2025) The effects of electronic smoking on dental caries and proinflammatory markers: a systematic review and meta-analysis. Front. Oral Health 6:1569806. doi: 10.3389/froh.2025.1569806
Received: 1 February 2025; Accepted: 31 March 2025;
Published: 11 April 2025.
Edited by:
Shariq Najeeb, Evidentia Dental Outcomes Research, CanadaReviewed by:
Marta Mazur, Sapienza University of Rome, ItalyLiudmyla Kryvenko, Kharkiv National Medical University, Ukraine
Copyright: © 2025 Tabnjh, Alizadehgharib, Campus and Lingström. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abedelmalek Kalefh Tabnjh, YWJlZGVsbWFsZWsua2FsZWZoLnRhYm5qaEBndS5zZQ==