 Abel Nnamdi Chukwuemeka1,2,3
Abel Nnamdi Chukwuemeka1,2,3 Richard Oveh1,4
Richard Oveh1,4 Anita Dabar1,2Omorinola Afolabi1,5Saheed Ademola Ibraheem1,6
Anita Dabar1,2Omorinola Afolabi1,5Saheed Ademola Ibraheem1,6 Folahanmi Tomiwa Akinsolu1,7
Folahanmi Tomiwa Akinsolu1,7 Abideen Olurotimi Salako1,7
Abideen Olurotimi Salako1,7 Omolola Titilayo Alade1,8Foluso Owotade1,9George Uchenna Eleje1,10
Omolola Titilayo Alade1,8Foluso Owotade1,9George Uchenna Eleje1,10 Oliver Ezechi1,7Joanne Lusher1,11
Oliver Ezechi1,7Joanne Lusher1,11 Moréniké Oluwátóyìn Foláyan1,12*
Moréniké Oluwátóyìn Foláyan1,12*
- 1Oral Health Initiative, Nigerian Institute of Medical Research, Yaba, Lagos, Nigeria
- 2Department of Public Health, Lead City University, Ibadan, Oyo, Nigeria
- 3Department of Planning, Research, Monitoring and Evaluation, Lagos State Health Management Agency, Alausa, Lagos, Nigeria
- 4Department of Information and Communication Technology, University of Delta, Agbor, Delta, Nigeria
- 5Department of Social Development, Moshood Abiola Polytechnic, Abeokuta, Ogun, Nigeria
- 6Scientific and Industrial Research Department, National Research Institute for Chemical Technology, Zaria, Kaduna, Nigeria
- 7Department of Clinical Sciences, Nigerian Institute of Medical Research, Yaba, Lagos, Nigeria
- 8Department of Community and Preventive Dentistry, Obafemi Awolowo University, Ile-Ife, Osun, Nigeria
- 9Department of Oral Medicine, Obafemi Awolowo University, Ile-Ife, Osun, Nigeria
- 10Effective Care Research Unit, Department of Obstetrics and Gynaecology, Nnamdi Azikiwe University, Awka, Nigeria
- 11Provost’s Group, Regent’s University London, London, United Kingdom
- 12Department of Child Dental Health, Obafemi Awolowo University, Ile-Ife, Osun, Nigeria
Background: This scoping review aimed to map school-based oral health interventions for adolescents in Nigeria and to identify gaps that can be addressed to promote optimal oral health in the population.
Methods: This scoping review is registered with the Open Science Framework (OSF) Registries (https://doi.org/10.17605/OSF.IO/CMRV4). An electronic search of PubMed, Scopus, Web of Science, African Journals Online, and Google Scholar for papers focused on oral health interventions implemented in schools in Nigeria, involving adolescents, and published in English between January 2000 and July 2024 was retrieved. Information extracted included study characteristics (author, year, study design), study population characteristics, type of interventions, focus, and key findings.
Results: The search yielded 392 results, with five studies meeting the eligibility criteria. All studies focused on oral health education, and education was delivered verbally. Four studies assessed the effect of education on oral hygiene practices, three assessed the effect on the consumption of refined carbohydrates, two measured dental service utilization as an outcome, and one assessed smoking cessation. One study showed that peer- and teacher-led models demonstrated comparable effectiveness, making them viable in resource-limited settings.
Conclusion: This scoping review found that school-based oral health interventions effectively improved oral hygiene among adolescent populations in Nigeria, though the few studies skewed to southern Nigeria make it difficult to generalize findings to Nigeria.
Review registration: OSF, https://doi.org/10.17605/OSF.IO/CMRV4.
Introduction
Adolescents are one of the most important demographic groups in terms of oral health due to their susceptibility to various oral health issues influenced by biological, social, and environmental factors (1). Poor oral health is associated with multiple complications, including pain and discomfort, tooth loss, reduced oral functioning, deformity, school absence, and mortality from oral cancer (2). Oral health issues among adolescents have a long-term impact on general health and well-being. The adverse impact of oral health on general health includes reduced quality of life and risk of diabetes and coronary artery disease (3, 4). Predispositions to poor oral health among adolescents include poor dietary habits, eating disorders, use of alcohol and drugs, teen pregnancy, and various other social and psychological determinants of health (5).
Furthermore, oral diseases are a major public health concern for adolescents in Africa. For example, in 2019, nearly one-third (31.0%) of adolescents across the African continent had untreated caries in permanent teeth (6). In the same period, the prevalence of untreated caries in permanent teeth among 10–19-year-old adolescents in the World Health Organization African Region was 29.8%, and the prevalence of periodontal diseases was 1.7% (6).
The incidence of oral diseases among adolescents in West Africa has also been increasing over the past 30 years, with Nigeria having the highest prevalence of oral diseases (7). Worldwide, about half of all adolescents require dental healthcare, and 34% have unmet dental healthcare needs (8). These indices reflect unmet dental needs among adolescents in West Africa and Nigeria, a global problem. In Nigeria, 15%–58% of adolescents over the age of 15 years present with periodontal disease, which significantly affects the quality of life (9). The pooled caries prevalence among adolescents is 23%, and the adjusted prevalence ratio of having caries increased by 18% for every additional age year (10, 11). In addition, only 8.7% of adolescents reported brushing their teeth twice daily, 16.1% used dental floss daily, 1.1% used dental services in the previous 12 months, and 36.1% consumed refined carbohydrates between meals less than once daily (11). Furthermore, poor oral health status among adolescents is linked to poor mental and sexual health (12). The establishment of health insurance initiatives has not significantly reduced the prevalence of oral disease or access to oral health among adolescents, thus indicating that further upstream policy changes may be required (13).
Moreover, preventive oral health education programs (education on oral hygiene practices, dietary guidance, awareness of oral health risks, encouraging regular dental visits and behavioral interventions addressing habits like smoking, nail-biting, or using teeth as tools, which can harm oral health) and community-based initiatives can promote good oral health (14, 15). Oral health interventions among children in primary schools using skills-based education and improving access to oral health services reduce the burden of oral disease (16). In Nigeria, a four-year oral health intervention among children in primary schools using education increased the uptake of fluoride-containing toothpaste, tooth brushing frequency, and sugar-containing snacks consumption (17). Educational interventions can significantly improve students’ knowledge, attitude, and behavior compared to those receiving usual care (18).
Oral health interventions can enhance access to dental care, strengthen oral health systems, and reduce oral health disparities among populations. It can enhance access to dental care among adolescents (19). Policy reforms, fluoridation programs, national health policies, and initiatives to regulate sugary snack marketing and tobacco control policies can also foster optimal oral health (20). School-based oral health education programs represent one of the most widely used interventions that can provide adolescents with knowledge and skills to maintain good oral hygiene practices, including oral hygiene practices, good dietary habits, and tobacco avoidance (21). These programs often incorporate interactive activities, peer education, and collaboration with dental professionals to engage adolescents effectively (22, 23).
School-based oral health interventions have emerged as a promising strategy for addressing adolescents’ oral health needs in Africa, where access to dental care remains limited (17). School-based programs can potentially improve oral health self-care practices among children and, if well-designed and implemented, can improve the oral health outcomes of adolescents in Nigeria (24). This underscores the need for a comprehensive review of the existing evidence on school-based oral health interventions for adolescents in Nigeria.
This scoping review aimed to systematically map and analyze the characteristics of the interventions, components of oral health interventions, variations in how educations are conducted, and to identify the gaps in adolescent-targeted school-based oral health interventions in Nigeria.
Methods
This scoping review process utilized three frameworks: Arksey and O'Malley Framework, Population Concept Context (PCC) Framework, and PRISMA-ScR guidelines (25, 26). It was registered with Open Science Framework (OSF) Registries (https://doi.org/10.17605/OSF.IO/CMRV4). The Arksey and O'Malley framework consists of five main steps: formulating the research questions, identifying relevant studies, selecting the studies, organizing the data, and compiling, summarizing, and presenting the findings. The target population for this scoping review were adolescents in Nigeria. The review assessed the various types of oral health interventions implemented among the individual, the strategies adopted and the implementation processes. The geographical context for the implementation of these interventions was considered in the assessment.
Research question
To guide the development of the questions in this scoping review, we used the following PCC (Population, Concept, and Context) strategy: Population: adolescents in Nigeria; Concept: oral health interventions; Context: school. The research questions of the scoping review were: What school-based oral health interventions are available for adolescents in Nigeria? What gaps have been identified to address this population's need for optimal oral health?.
The review's objectives were: (1) to outline the characteristics of school-based oral health interventions targeting adolescents in Nigeria. (2) To examine the specific components of these interventions targeting adolescents in Nigerian schools. (3) To investigate the differences in school-based oral health interventions for adolescents across Nigeria. (4) To identify gaps in implementing these interventions among Nigerian adolescents.
Identification of relevant studies
A search strategy was developed to identify relevant studies. The search was conducted in PubMed, Scopus, Web of Science, African Journal Online, and Google Scholar using the prespecified search terms. Search terms were identified within titles, abstracts, or keywords. Mapping terms to subject headings (i.e., MeSH terms) was used within applicable databases to increase the efficiency and precision of the search. The search strategies included phrases like “school-based oral health interventions,” “adolescents,” and “Nigeria.” The search strategies used for each database are detailed in Supplementary Appendix 1.
Eligibility criteria
Studies included in the scoping review focused on oral health interventions implemented in schools in Nigeria that included adolescents 10–19 years old (+2 years). Only complete studies were conducted between January 2000 and July 2024, a critical period that marked the beginning of global and national commitments to improve adolescent health under the Millennium Development Goals and the Sustainable Development Goals. This timeframe allows for studies to be included during these critical policy and programmatic evolution phases. Studies with data that could be independently reported for adolescents within the age range of the study were included in this review. Reviews, editorials, and opinion pieces not addressing study objectives were excluded.
Study selection process
Articles identified through the search strategy were first organized in EndNote. The records were then imported into Rayyan, where duplicates were removed. Three independent reviewers (AC, RO, and AD) carefully screened the titles and abstracts to identify studies that met the inclusion criteria.
Two reviewers (AC and MOF) retrieved full-text articles for studies deemed potentially relevant. Institutional library resources, online databases, and journal websites were accessed to obtain the full texts. When articles were not immediately accessible, reviewers contacted corresponding authors via email to request copies, searched alternative repositories and conducted citation tracking and cross-referencing to locate alternate sources. Articles that remained inaccessible were documented, and their unavailability was acknowledged as a limitation of the review. Throughout the process, any discrepancies in eligibility assessment were resolved through discussions and consensus among the reviewers, ensuring methodological rigor and consistency.
Inter-rater reliability
To ensure the reliability of the screening process, inter-rater agreement among reviewers was assessed using Cohen's Kappa statistic for both the title and abstract screening and the full-text screening phases. The average Kappa value was 0.98. For full-text screening, two reviewers independently screened the full-text articles. The inclusion and exclusion criteria were again applied to determine eligibility. The Cohen's Kappa coefficient for the full-text screening was 0.93, with a 98.7% agreement. The high Kappa values signify substantial to almost perfect agreement (27).
Data charting
Investigators developed a standardized data extraction form for data from included studies. Key information extracted included study characteristics (author details, year of publication, study design), population characteristics, intervention details, outcomes measured, and key findings related to school-based oral health interventions among adolescents in Nigeria.
Collating, summarizing, and reporting results
Characteristics (evidence source data and population characteristics) and data relating to the review objectives (intervention characteristics, types of Intervention, key outcomes of interventions, and intervention implementation gaps) were collated and presented in a table, and a narrative summary was provided.
In addition, a qualitative analysis of the was findings of the studies was conducted using inductive coding to identify key themes and concepts that capture the main ideas emanating from the study findings and identify gaps or areas needing further research. The coding was developed through an iterative process of reviewing the key study outcomes for patterns and meanings, identifying patterns and relationships between codes, and developing coherent themes that reflect the key findings. The developed themes were shared with team members to validate interpretations. The findings was used to compliment the outcomes of the analysis conducted using ChatGPI 3.5.
Results
The initial search yielded 392 records, as shown in Figure 1. Once these records were compiled, 50 duplicate records were removed before screening, leaving 342 records for further review. In the title and abstract screening stage, 260 records were excluded for the following reasons: the studies were not on oral health (n = 93), the population were not adolescents (n = 82), and not conducted in Nigeria (n = 85). A total of 82 studies were sought for retrieval, of which four could not be retrieved. In the full-text screening phase, 73 studies were excluded, with three reasons being that the studies were not focused on a school-based intervention (n = 42), no interventions were reported (n = 29), and the age of study participants was outside the age range for the current study (n = 2). Overall, five (28–32) studies were included in the review.
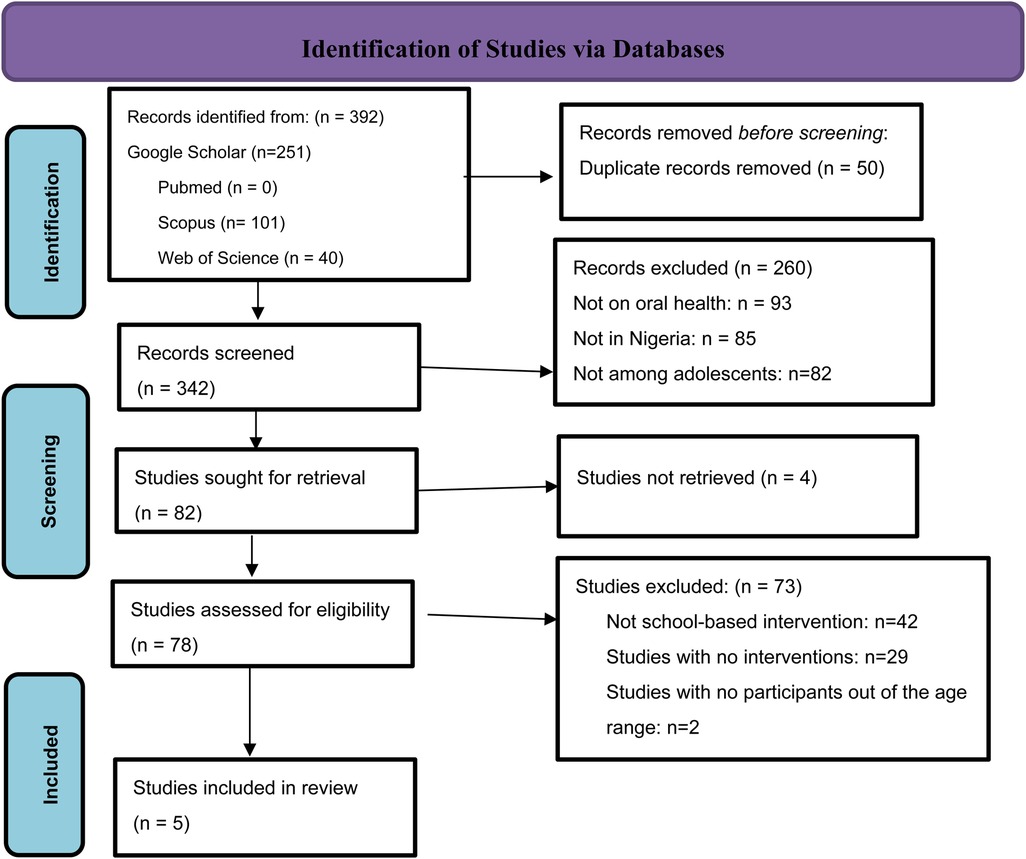
Figure 1. Literature included in the scoping review based on PRISMA 2020 protocol (28).
Population characteristics
Table 1 shows that the studies were published between 2013 and 2023. The distribution of these studies shows a consistent effort to address oral health issues among adolescents over ten years, with interventions taking place in two of the six geopolitical zones in Nigeria: South-East and South-West geopolitical zones of Nigeria. The study population characteristics varied but primarily targeted adolescents aged between 8 and 21. Three studies were conducted in the South-West region (29, 31, 32), and two were conducted in the South-East (28, 30). The total sample for the included studies was 4073 (1,904 males and 2,169 females), with sample sizes ranging significantly from 1,200 (29) to 1,800 students (31). The included studies recruited participants from primary schools (28, 29, 32) and secondary schools (30, 32).
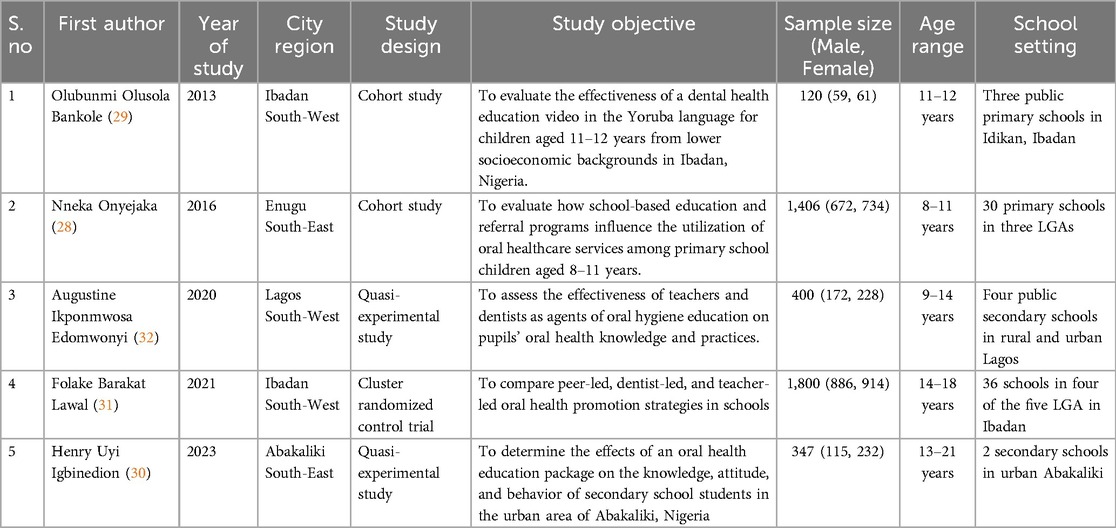
Table 1. Characteristics of the studies included in the scoping review.
Study designs
The studies employed a range of research designs, with one study using clustered randomized controlled trials (31), two adopting quasi-experimental designs (30, 32), and two using a cohort design (28, 29). The randomized controlled trial compared dentist-led, teacher-led, and peer-led education (31). One quasi-experimental study compared teacher-led intervention schools and dentist-led Intervention (32).
Types and tools used for oral health interventions
Table 2 shows that all studies focused on oral health education as the primary Intervention, though the delivery methods varied. All studies conducted verbal education. In addition, one study also used video as an intervention tool (29).
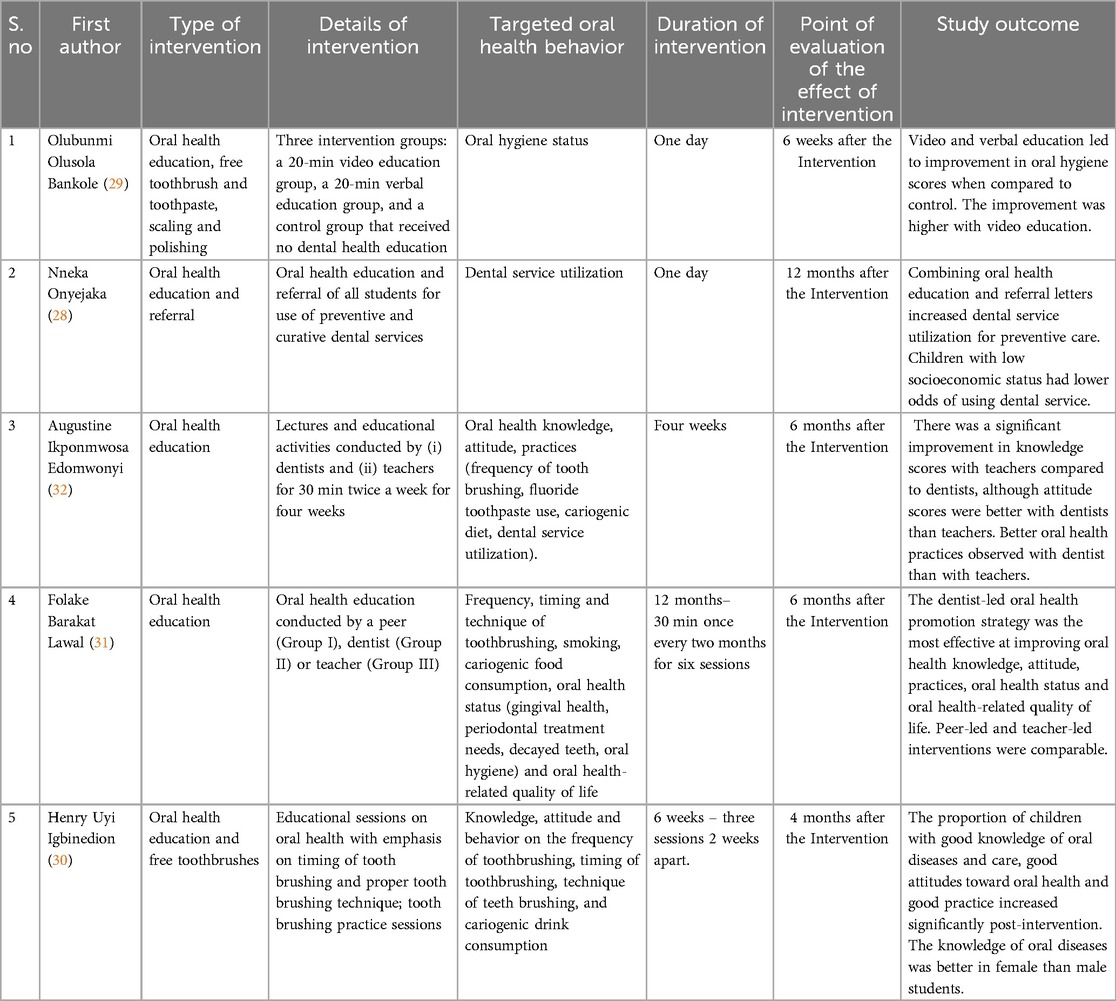
Table 2. Details on the oral health interventions conducted by the studies included in the scoping review.
People trained to provide interventions were dentists (31, 32), teachers (31, 32), and peers (31). One of the studies compared the effect of peer-led, teacher-led, and dentist-led education on tooth brushing and dental service utilization (31). One study combined education with a referral program to encourage dental service utilization (28).
Duration of oral health interventions
The duration of interventions in the included studies ranged from short programs lasting one day (28, 29) to longer interventions that spanned twelve months (31). The post-intervention assessment was conducted for one month (30) to twelve months (28) after Intervention.
Outcomes measured
The primary outcomes measured across the studies included oral health knowledge, behavior change (tooth brushing frequency, timing and techniques, fluoridated toothpaste use, and refined carbohydrates frequency), and dental service utilization. Four of the studies assessed oral hygiene practices, with a specific focus on the frequency (29–32), timing (30), brushing techniques (29, 30–32), use of fluoride toothpaste (32), and consumption of refined carbohydrates (30–32). In addition, two studies measured dental service utilization as an outcome, aiming to assess whether education alone could influence adolescents to seek preventive care (28, 32) and one assessed smoking (31).
Measures of study outcomes include the use of knowledge (30, 31), attitude (30, 31), behavior/practice (30, 31) scores, oral hygiene status (29, 31), gingival health (31), caries experience (31), periodontal treatment needs (31) and oral health quality of life (31). Number of students who visited dental clinics following referrals was calculated (28). Gender disparities in response to the interventions were also examined, focusing on how male and female students reacted differently to the same educational content (30).
Key findings
All five studies reported a positive impact on adolescents’ oral health knowledge and behavior. Four key themes that emerge on the effectiveness of oral health interventions and the factors influencing their outcomes highlighted differences in strategy effectiveness, socioeconomic disparities, gender-related outcomes, and long-term retention of oral health practices.
First, regarding educational modality effectiveness, one study showed that video education yields stronger outcomes in improving oral hygiene scores than verbal methods (29). Another study showed that although dentist-led strategies out-performed teacher-led ones in changing attitudes and practices, teacher-led approaches were effective for knowledge retention (32). Both teacher- and peer-led methods demonstrated substantial improvements and had comparable outcomes, making them viable alternatives in settings with limited access to dental professionals (31).
Second, one study showed that combining knowledge and action (pairing education with referral letters enhances) improved preventive dental care utilization. However, children with lower socioeconomic status face barriers in utilizing dental services despite Intervention. This underscores the need for targeted interventions (28).
Third, one study showed that knowledge, attitude, and practice shifts could result from oral health interventions, as there were improvements in understanding the causes of gum disease and tooth decay and shifts in attitudes toward preventive dental visits (30). However, knowledge gains were higher in teacher-led interventions, while dentist-led strategies were more effective in changing attitudes and practices (32). Gender differences were also observed, with female students showing greater improvements in knowledge and behaviors compared to males (31).
Finally, one study assessed the comparative effectiveness of peer and teacher-led models of oral health education interventions and found that peer-led and teacher-led interventions were comparable, suggesting that both education models can be equally effective when properly structured (31).
Discussion
This study is the first to conduct a comprehensive assessment of the effect and impact of interventions on the oral health of adolescents in Nigeria. First, a limited number of intervention studies are available in the literature, which are restricted to just two of the six geopolitical zones in Nigeria and mainly educational interventions. Second, although the interventions addressed oral hygiene practices, use of fluoride toothpaste, refined sugar consumption and dental service utilization, the effect of the interventions were only reported for oral hygiene practices and use of fluoride toothpaste: none reported on the impact of the interventions on refined sugar consumption. Third, video-based and dentist-led interventions may be more effective in achieving impact.
One of the strengths of this study was the strong focus on behavior change, with interventions generally proving successful at improving key oral health behaviors such as tooth brushing frequency. Including measurable outcomes related to behavior and knowledge provided concrete evidence of the interventions’ effectiveness.
A limitation of the study was the variation in study design, sample size, and intervention duration, making it challenging to compare results across studies. Studies that employed short-term interventions may not adequately capture the long-term sustainability of behavior change or the retention of oral health knowledge over time. In addition, the inability to retrieve four of the 82 screened studies may have resulted in the inadvertent exclusion of publications in the final review. Despite these limitations, the current study contributes to new knowledge on the study matter in Nigeria.
The findings from this scoping review of school-based oral health interventions among adolescents in Nigeria broadly align with several trends observed in global and regional studies on adolescent oral health education (33). For instance, studies conducted in Brazil and India, which share socioeconomic and healthcare challenges like Nigeria, have demonstrated that school-based oral health education can improve oral hygiene practices (34, 35). Much like in Nigeria, studies have shown that multimedia tools (videos, songs, and visual aids) have proven effective in engaging young people and fostering sustained behavior change (36). This indicated that using interactive and engaging methods led to better oral health outcomes than traditional didactic education methods (37).
Oral health education can change oral health behavior by following a pathway that integrates both psychological and social factors, as explained by models like the Cognitive Social Health Information Processing (C-SHIP) model (38) and the Capability, Opportunity, and Motivation (COM-B) model (39). According to the C-SHIP model, oral health education helps individuals perceive, encode, and integrate new information into their beliefs about oral health. Once individuals have formed a knowledge base, it influences their motivation to act. In the COM-B model, capability (knowledge) and motivation interact to drive behavioral change. Thus, when people understand the consequences of poor oral health—such as tooth decay or gum disease—they become more motivated to adopt preventive practices like brushing twice a day, using fluoride toothpaste, or seeking dental services for check-ups.
Education alone is not enough; individuals need opportunities to act on their new knowledge. According to the COM-B model, opportunity refers to social and environmental factors. Education and practical opportunities—like accessible dental services, referrals, and affordable care—can bridge the gap between knowledge and action. For example, pairing oral health education with referral letters (as observed in the findings) (28) increased dental service utilization. This suggests that creating accessible pathways to care can drive behavior changes.
As individuals adopt new oral health behaviors (such as increased brushing frequency), these actions reinforce their motivation to maintain good habits. Over time, consistent behaviors improve oral health outcomes, which feeds back into increasing their capability and motivation to continue these practices. This dynamic process ensures that once behaviors are adopted, they can be sustained in the long term. Peer-led and teacher-led interventions can be particularly effective in creating social motivation for behavior change. These models allow for disseminating oral health knowledge in a culturally acceptable and familiar context, enhancing the social opportunity for adopting new behaviors. The findings show that both models can be as effective as dentist-led strategies in knowledge retention, emphasizing the role of social networks in reinforcing healthy behaviors.
The findings on gender differences in how oral health education influences behavior are consistent with another study conducted in Japan that found that women have more positive attitudes towards dental visits, higher oral health literacy, and better oral health behaviors than men (40). This finding raises important questions about how health interventions are designed and whether they adequately account for how boys and girls might engage with health education. In addition, this raise concerns that current oral health interventions, if not tailored to address these gender-specific needs, could be less effective for one gender compared to the other. The finding suggests that interventions should consider gender-specific motivations and barriers when designing oral health education programs to maximize effectiveness.
In addition, the findings on disparities in dental service use among lower socioeconomic groups indicate the need for targeted education and opportunity creation. The finding mirrors observations from studies in countries such as South Africa, where structural barriers, such as financial constraints, affect adolescents’ health-seeking behaviors (41). These findings suggest that while school-based education is necessary, it may not be sufficient without addressing broader socioeconomic determinants of health. Tailoring interventions to consider socioeconomic barriers—such as subsidizing care or increasing community outreach—ensures that disadvantaged populations have both the knowledge and the opportunity to access preventive services, closing the gap in health outcomes.
Interventions integrating multimedia tools, such as videos and interactive content, showed better engagement and outcomes. Multimedia tools have a greater impact on oral health for school children due to their ability to engage, simplify complex information, and enhance retention (42). These tools use visual, auditory, and interactive elements to capture attention and facilitate learning (43). They also support personalized and self-paced learning, with content adaptable to different levels and cultural contexts (44). The current study findings align with the broader literature on health education, which emphasizes using culturally relevant materials to enhance knowledge retention (45). The use of culturally appropriate education materials that are appropriate for adolescent education is more likely to change oral health behavior by increasing capability (knowledge and skills) within school-based created opportunities (social and environmental factors), and enhancing motivation (emotional and psychological readiness) to engage in preventive practices. The process is dynamic, as changes in behavior further reinforce capability, motivation, and access, creating a sustained cycle of improvement in oral health outcomes. This of culturally appropriate education materials not only makes the content more relatable but also increases participants’ motivation to engage with the learning material.
Table 3 is a summary of the findings from the study. It outlines strategies for improving school-based oral health through diverse behavioral change models. The table also includes our thoughts on the possible implications of the study findings for the future. Multimedia education uses culturally relevant tools to enhance short-term knowledge retention, while guided tooth brushing programs with rewards foster consistent habits. Peer-led education leverages relatability to moderately improve outcomes, complementing teacher-led education, which achieves sustained behavior changes through curriculum integration. Dentist-led education proves most effective but resource-intensive, whereas referral programs boost dental service use, albeit with socio-economic barriers. Gender-specific tailoring addresses learning differences, showing greater benefits for female students. Collectively, these strategies emphasize resource-sensitive, tailored interventions to optimize oral health outcomes in schools. Our postulations on the implications of the study findings for future interventions need to be explored by further studies.
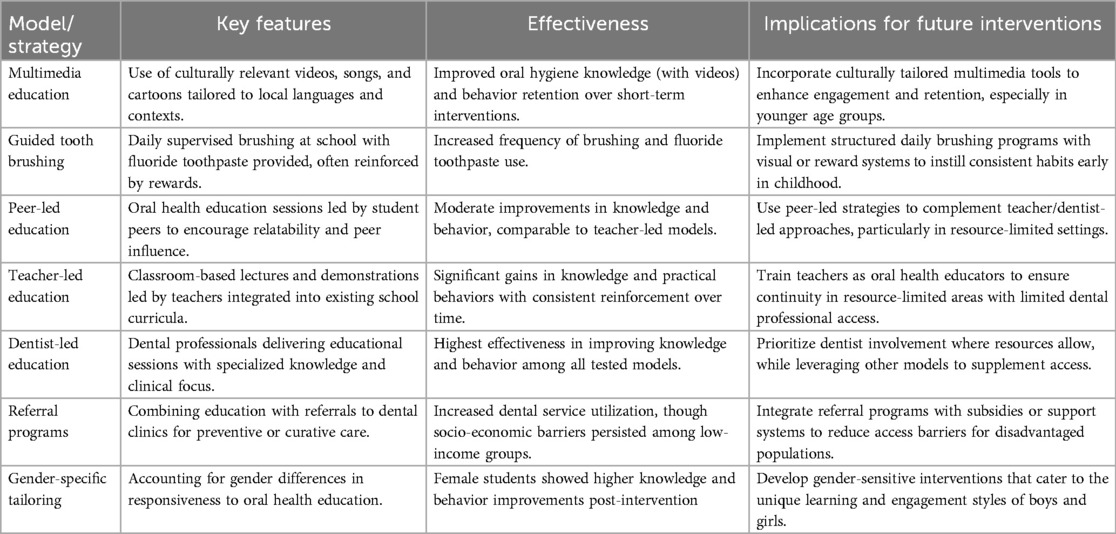
Table 3. Summary of behavioral change models and strategies in school-based oral health interventions.
A key observation in the reviewed studies is the geographic concentration. Most of the research has been conducted in Nigeria's South-East and South-West regions, specifically in cities like Enugu, badan, and Lagos. While these urban centers provide a valuable setting for studying school-based interventions, they do not reflect the diversity of the Nigerian population, particularly the largely rural and semi-urban areas that face even greater healthcare access challenges. In addition, the absence of studies from the northern and middle-belt regions leaves a gap in understanding how different socio-cultural dynamics may influence the effectiveness of oral health programs in these areas. The limited number of dental schools in the northern and middle-belt regions with few epidemiologists and public oral health specialists may have contributed to this observation. The ongoing efforts to strengthen the presence of dental schools in Northern Nigeria may result in changes in context specific knowledge generation in the near future.
Conclusions
The current scoping review highlighted that school-based oral health interventions in Nigeria are focused on oral health education, with most of the studies aimed at improving oral hygiene practices. Oral health education was conducted through verbal communication and complemented with technology in a few cases. Peers, teachers and dentists were also assessed as oral health educators for school-based oral health interventions. However, the studies on school-based oral health interventions in Nigeria are few and skewed to southern Nigeria. Since the cultural and economic differences between northern and southern Nigeria can significantly influence the effectiveness of oral health interventions, there is the need to study Intervention in northern Nigeria.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
AC: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Writing – original draft, Writing – review & editing. RO: Data curation, Validation, Writing – review & editing. AD: Data curation, Validation, Writing – review & editing. OA: Data curation, Validation, Writing – review & editing. SI: Data curation, Validation, Writing – review & editing. FA: Data curation, Project administration, Supervision, Writing – review & editing. AS: Validation, Writing – review & editing. OA: Validation, Writing – review & editing. FO: Validation, Writing – review & editing. GE: Validation, Writing – review & editing. OE: Funding acquisition, Project administration, Supervision, Validation, Writing – review & editing. JL: Validation, Writing – review & editing. MF: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Grant Number: 5NM-ADJGT-22–0082 from the Nigerian Institute for Medical Research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript to inductively analysis the content of the table 1 and 2.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/froh.2025.1577753/full#supplementary-material
References
1. Silk H, Kwok A. Addressing adolescent oral health: a review. Am Acad Pediatr. (2017) 38(2):61–8. doi: 10.1542/pir.2016-0134
2. Pavlovic M, Matijevic D, Vukovic B, Mileusnic I, Gajic M, Jevremovic A. Influence of tooth loss and unmet treatment needs on the social aspects of quality of life and self-esteem in adolescents. J Pharm Pharmacol. (2019) 7:22–31. doi: 10.17265/2328-2150/2019.01.003
3. Takefuji Y. Oral health and diabetes updates. Br Dent J. (2024) 236:582–3. doi: 10.1038/s41415-024-7363-2
4. Dietrich T, Webb I, Stenhouse L, Pattni A, Ready D, Wanyonyi K, et al. Evidence summary: the relationship between oral and cardiovascular disease. Br Dent J. (2017) 222:381–5. doi: 10.1038/SJ.BDJ.2017.224
5. America's Pediatric Dentists. Adolescent oral health care (2025). Available online at: https://www.aapd.org/research/oral-health-policies--recommendations/adolescent-oral-health-care/ (Accessed July 23, 2025).
6. Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 Results. Seattle, United States: Institute for Health Metrics and Evaluation (IHME) (2020). Available online at: https://ghdx.healthdata.org/gbd-2019 (Accessed August 25, 2024).
7. Shomuyiwa DO, Bridge G. Oral health of adolescents in West Africa: prioritizing its social determinants. Glob Health Res Policy. (2023) 8(1):28. doi: 10.1186/s41256-023-00313-2
8. Ghafari M, Bahadivand-Chegini S, Nadi T, Doosti-Irani A. The global prevalence of dental healthcare needs and unmet dental needs among adolescents: a systematic review and meta-analysis. Epidemiol Health. (2019) 41:e2019046. doi: 10.4178/epih.e2019046
9. Akpata ES. Oral health in Nigeria. Int Dent J. (2004) 54(6 Suppl 1):361–6. doi: 10.1111/j.1875-595x.2004.tb00012.x
10. Afolabi AO, Ehizele AO, Nnawuihe UC, Nwaokorie FO, Nwaozuru U, Owotade F, et al. Dental caries prevalence, preventive behaviour and related factors among adolescents in Nigeria: a 10-year systematic review and meta-analysis. BMC Oral Health. (2025) 25(1):1138. doi: 10.1186/s12903-025-06504-2
11. Folayan MO, El Tantawi M, Chukwumah NM, Alade M;, Oginni O, Mapayi B, et al. Individual and familial factors associated with caries and gingivitis among adolescents resident in a semi-urban community in South-Western Nigeria. BMC Oral Health. (2021) 21(1):166. doi: 10.1186/s12903-021-01527-x
12. Folayan MO, Adeniyi AA, Oziegbe EO, Fatusi AO, Harrison A. Integrated oral, mental and sexual health management for adolescents: a call for professional collaboration. Int J Adolesc Med Health. (2016) 30(3):20160060. doi: 10.1515/ijamh-2016-0060
13. Odipo E, Jarhyan P, Nzinga J, Prabhakaran D, Aryal A, Clarke-Deelder E, et al. The path to universal health coverage in five African and Asian countries: examining the association between insurance status and health-care use. Lancet Glob Health. (2024) 12(1):e123–33. doi: 10.1016/S2214-109X(23)00510-7
14. Kanoute A, Faye D, Bourgeois D. Current status of oral health research in Africa: an overview. Int Dent J. (2012) 62(6):301–7. doi: 10.1111/j.1875-595X.2012.00123x
15. Adeniyi AA, Sofola OO, Kalliecharan RV. An appraisal of the oral healthcare system in Nigeria. Int Dent J. (2012) 62(6):292–300. doi: 10.1111/j.1875-595X.2012.00122.x
16. Akera P, Kennedy SE, Lingam R, Obwolo MJ, Schutte AE, Richmond R. Effectiveness of primary school-based interventions in improving oral health of children in low- and middle-income countries: a systematic review and meta-analysis. BMC Oral Health. (2022) 22(1):264. doi: 10.1186/s12903-022-02291-2
17. Esan A, Folayan MO, Egbetade GO, Oyedele TA. Effect of a school-based oral health education programme on use of recommended oral self-care for reducing the risk of caries by children in Nigeria. Int J Paediatr Dent. (2015) 25(4):282–90. doi: 10.1111/ipd.12143
18. CDC. Health and economic benefits of oral health interventions (2024). Available online at: https://www.cdc.gov/nccdphp/priorities/oral-disease.html (Accessed March 26, 2024).
19. CDC. About cavities (tooth decay) (2024). Available online at: https://www.cdc.gov/oral-health/about/cavities-tooth-decay.html (Accessed July 23, 2025).
20. Nakre PD, Harikiran AG. Effectiveness of oral health education programs: a systematic review. J Int Soc Prev Community Dent. (2013) 3(2):103–15. doi: 10.4103/2231-0762.127810
21. Molete M, M; Malele-Kolisa Y, Thekiso M, Lang AY, Kong A, George A. The role of community health workers in promoting oral health at school settings: a scoping review. J Public Health Dent. (2024) 84(2):175–86. doi: 10.1111/jphd.12612
22. Elsadek YE, Edwebi S, Turner A, Vinall-Collier K, Csikar J, Pavitt S. A systematic review of school-based student peer-led oral health interventions to promote the oral health of school children. BMC Oral Health. (2023) 23:742. doi: 10.1186/s12903-023-03482-1
23. World Health Organization. Africa burdened with largest global increase of oral diseases (2023). Available online at: https://www.afro.who.int/news/africa-burdened-largest-global-increase-oral-diseases (Accessed March 26, 2024).
24. Ogwo CE. Effectiveness of school-based oral health programme in the reduction of dental diseases in Nigeria (2017). Available online at: https://www.bibalex.org/baifa/en/resources/document/476501 (Accessed March 26, 2024).
25. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8(1):19–32. doi: 10.1080/1364557032000119616
26. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:71. lashma@12345$doi: 10.1136/bmj.n71
27. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. (1977) 33(1):159–74. doi: 10.2307/2529310
28. Onyejaka NK, Folayan MO, Folaranmi N. Effect of referral for dental service on dental-service utilization by primary school children aged 8 to 11 years in Enugu, Nigeria. Braz J Oral Sci. (2017) 15:151–7. doi: 10.20396/BJOS.V15I2.8648767
29. Bankole OO. Effects of information dissemination using video of indigenous language on 11-12 years children’s dental health. Ethiop J Health Sci. (2013) 23(3):201–8. doi: 10.4314/ejhs.v23i3.2
30. Igbinedion HU, Akaji EA, Chukwuneke FN, Ezeoke UE, Igbinedion EB. Oral health knowledge attitude and behaviour among secondary school children: a quasi-experimental study. Nig J Dent Res. (2023) 8(1):20–9. doi: 10.4314/njdr.v8i1.5
31. Lawal FB. Comparison of peer-led, dentist-led and teacher-led school-based oral health promotion strategies among adolescents in Ibadan, Nigeria (2022). Available online at: https://pgsdspace.ictp.it/xmlui/handle/123456789/1494?show=full (Accessed August 26, 2024).
32. Edomwonyi AI, Adeniyi AA, Adedigba MA, Oyapero A. Use of teachers as agents of oral health education: intervention study among public secondary school pupils in Lagos. J Family Med Prim Care. (2020) 9:2806–13. doi: 10.4103/jfmpc.jfmpc_1269_19
33. Gargano L, Mason MK, Northridge ME. Advancing oral health equity through school-based oral health programs: an ecological model and review. Front Public Health. (2019) 7:359. doi: 10.3389/FPUBH.2019.00359
34. Gauba A, Bal I, Jain AK, Mittal HC. School based oral health promotional intervention: effect on knowledge, practices and clinical oral health related parameters. Contemp Clin Dent. (2013) 4:493–9. doi: 10.4103/0976-237X.123056
35. Tomazoni F, Vettore MV, Baker SR, Ardenghi TM. Can a school-based intervention improve the oral health-related quality of life of Brazilian children? JDR Clin Trans Res. (2019) 4:229–38. doi: 10.1177/2380084418816984
36. Abdulrahaman M, Faruk N, Oloyede A, Surajudeen-Bakinde N, Olawoyin L, Mejabi O, et al. Multimedia tools in the teaching and learning processes: a systematic review. Heliyon. (2020) 6:e05312. doi: 10.1016/j.heliyon.2020.e05312
37. Mehta V, Mathur A, Chaurasia H, Obulareddy VT, ; D'Amico C, Fiorillo L. A brief review on engaging and interactive learning for children: exploring the potential of metaverse-based oral health promotion. Int J Dent. (2024) 2024:6679356. doi: 10.1155/2024/6679356
38. Miller SM, Diefenbach MA. The cognitive-social health information-processing (C-SHIP) model: a theoretical framework for research in behavioral oncology. In: Krantz DS, Baum A, editors. Technology and Methods in Behavioral Medicine. Mahwah, NJ: Lawrence Erlbaum Associates Publishers (1998). p. 219–44.
39. Willmott TJ, Pang B, Rundle-Thiele S. Capability, opportunity, and motivation: an across contexts empirical examination of the COM-B model. BMC Public Health. (2021) 21:1014. doi: 10.1186/s12889-021-11019-w
40. Bhadauria US, Priya H, Purohit B, Singh A. Effectiveness of school oral health programs in children and adolescents: an umbrella review. Evid Based Dent. (2024) 25(4):211. doi: 10.1038/s41432-024-01013-7
41. Omotoso KO, Adesina J, Adewole OG, Gbadegesin TF. Factors influencing healthcare-seeking behaviour of South African adolescents. J Public Health. (2022) 30:2427–39. doi: 10.1007/s10389-021-01572-4
42. Sharma S, Mohanty V, Balappanavar AY, Chahar P, Rijhwani K. Role of digital media in promoting oral health: a systematic review. Cureus. (2022) 14(9):e28893. doi: 10.7759/cureus.28893
43. Wu S. Application of multimedia technology to innovative vocational education on learning satisfaction in China. PLoS One. (2024) 19(2):e0298861. doi: 10.1371/journal.pone.0298861
44. Major L, Francis GA, Tsapali M. The effectiveness of technology-supported personalised learning in low- and middle-income countries: a meta-analysis. Br J Educ Technol. (2021) 52(5):1935–64. doi: 10.1111/bjet.13116
Keywords: dental health, tooth brushing frequency, fluoridated toothpaste, cariogenic diet, dental service utilization, young people, youth, telehealth
Citation: Chukwuemeka AN, Oveh R, Dabar A, Afolabi O, Ibraheem SA, Akinsolu FT, Salako AO, Alade OT, Owotade F, Eleje GU, Ezechi O, Lusher J and Foláyan MO (2025) A scoping review of school-based oral health interventions among adolescents in Nigeria. Front. Oral Health 6:1577753. doi: 10.3389/froh.2025.1577753
Received: 16 February 2025; Accepted: 10 July 2025;
Published: 29 July 2025.
Edited by:
Tina Poklepović Peričić, University of Split, CroatiaReviewed by:
Harsh Priya, All India Institute of Medical Sciences, IndiaNatalie Gordon, University of the Western Cape, South Africa
Copyright: © 2025 Chukwuemeka, Oveh, Dabar, Afolabi, Ibraheem, Akinsolu, Salako, Alade, Owotade, Eleje, Ezechi, Lusher and Foláyan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Moréniké Oluwátóyìn Foláyan, dG95aW51a3BvbmdAeWFob28uY28udWs=