 Shivanand Pawar
Shivanand Pawar Mahesh Chougule
Mahesh Chougule R. M. Channaveer
R. M. Channaveer- 1Department of Social Work JAIN Deemed to be University, Bengaluru, Karnataka, India
- 2Faculty of Social Administration, Thammasat University, Bangkok, Thailand
- 3Department of Social Work, Central University of Karnataka, Kadaganchi, Karnataka, India
Introduction: Enhancing human capital through Social Behavior Change Communication (SBCC) strategy, and social entrepreneurship approach, strategically intends to improve knowledge, skills, and practice at the individual and community level. Grounded in human capital theory, the intervention aimed on building the capabilities of women participants to influence Water, Sanitation, and Hygiene (WASH) outcomes. Community education and stakeholder engagement played a crucial role in strengthening local capabilities and fostering sustainable WASH behaviors. Furthermore, the WASH-based program and stakeholder engagement process have the potential to reduce the risk of infection from waterborne diseases and enhance prevention and control measures within the village community.
Methodology: The study intends to measure the influence of human capital and stakeholder engagement interventions on elevating WASH knowledge, attitude, and practice among women participants. The sample size consists of women participants (N = 110) in the 20–50-year-old age group (Mean = 42.78, SD = 13.98). All the head women participants of the 110 households selected for the study kept village development as a prime focus.
Results: Significant improvement was observed in the outcome status of the knowledge level of women in water, sanitation, and hygiene compared to their baseline status (M = 2.36, SD = 0.631, df = 109, t = 43.792, p < 0.01). A significant increase was observed in the outcome status of the attitude of women toward water, sanitation, and hygiene (M = 16.55, SD = 1.640, df = 109, t =19.755, p < 0.01). In the practice domain of WASH, the women participants showed a significant increase in the outcome status compared to their baseline status (M = 1.29, SD = 0.580, df = 109, t = 17.881, p < 0.01).
Conclusion: Human capital building, social behavior change and communication strategy, stakeholder engagement and social entrepreneurship approach create a conducive environment for sustainable community development.
Introduction
The deaths all over the world due to inadequate water, sanitation, and hygiene (WASH) services have been an alarming phenomenon. The civilians in large numbers are deprived of such basic amenities; the scenario has been similar in the underdeveloped and developed countries across the world (World Health Organization, 2018). Approximately 65% of India's population lives in rural regions, with half of them living below the poverty line (World Bank, 2018). Research from developing nations has consistently shown a strong link between low socio-economic status, poor health, and limited access to healthcare services (Saikia et al., 2019). In Indian states, rural populations, especially females, face a significantly higher risk of mortality compared to their male counterparts (Jana et al., 2022). Maternal mortality rates in the state are a relatively high, contributing to increased death rates within the 15–59 age group (Raza, 2018). Diarrhea, cholera, typhoid, hepatitis-A, and other water-borne diseases have been commonly attributed to open defecation, poor sanitation, and hygiene practices (Bethony et al., 2006; Kanungo et al., 2021). Although India contributes significantly to the global burden of WASH attributable diseases due to its large population, recent improvements in water and sanitation led to relative decline in the WASH-related mortality rates, which may now be lower than those of low and middle-income countries (Pruss-Ustun et al., 2019). It is a major public health concern and crucial as well since human wellbeing is closely linked to cleanliness (Kirithika et al., 2020). Thus, the hygienic practices are a crucial element of public health that both influence and influenced by the economic and social status of women (Jacob and Saggu, 2024).
Sustainable Development Goal (SDG) 6 declares the essence of achieving “clean water and sanitation for all.” Attaining it through raising awareness of disseminating knowledge about water, sanitation, and hygiene (WASH) sets as a precondition. Human capital catalyses this dissemination, as informed individuals within a community can actively contribute to raising awareness about the importance of water and sanitation. The community members whose higher level of knowledge and skills are indicative of higher awareness regarding sanitation and hygiene recognize the value of sustainable practices and advocate for change (Taylor et al., 2015). Human capital and behavior change are positively correlated. The role of capacity-building initiatives, local leadership development, skill development, and participation of people realize positive behavioral changes among the community members (UNICEF and WHO, 2021). The human capital approach not only attempts to address the issues serving as barriers to the implementation of water and sanitation-related program but also contributes to understanding the problem and innovating a solution compatible with the cultural context of the community and the needs of the local community (Caruso et al., 2018). Thus, there is a need to identify an expanded effective service delivery model to achieve the ambitious sanitation and hygiene target set by the SDG (Amebelu et al., 2021). Therefore, understanding the barriers to latrine use, implementing behavioral change strategies, and designing informed interventions are key steps toward increasing latrine use effectively (Talat et al., 2023). In this direction, the effective implementation of the Government of India's Jal Jeevan Mission (JJM) and Swachh Bharat Mission (SBM), the countrywide national campaigns empower rural Gram Panchayats (GPs) to pursue their local efforts in delivering effective water and sanitation services. In addition to addressing the technical aspects of the water and sanitation sector, it is crucial to comprehend the broader governance context to ensure sustainable water and sanitation delivery, especially in rural areas, by reinforcing and enhancing their efficiency (Kanyagui et al., 2024).
India has swiftly advanced in eradicating open defecation nationwide, substantially enhancing water, sanitation, and hygiene conditions because of the JJM and SBM. UNICEF collaborates with the Indian government on critical initiatives such as the SBM, JJM, and WASH in Schools, including preschools known as Anganawadis (childcare centers). The Swachh Bharat Abhiyan (SBA), especially in urban areas, has notably improved the availability of resources for sanitation, hygiene, and access to safe drinking water. According to the WHO-UNICEF Report, essential access to secure water increased from 94.7% to 96.3% between 2000 and 2017. Moreover, basic sanitation facilities increased from 49.3% to 72%, and since 2012, roughly 80% of the urban population has had access to essential hygiene services (WHO-UNICEF, 2022). Despite the SBA having led to better access to WASH services, sanitation issues continue to be a challenge in India (World Health Organization, 2023). To achieve better outcomes, there is still a need for increased hygiene and personal cleanliness education, even though government entities can contribute to the necessary infrastructure improvements in developing nations (Jenkins et al., 2014). By reinforcing standards for cleanliness, personal hygiene, and water usage, it is possible to address numerous communicable diseases effectively (Banerjee et al., 2014). The World Health Organization has been aiding critical stakeholders in India with support for research, capacity building, and promoting the best practices, including enhancing drinking water quality. Understanding the local context plays significant role in effectively mitigating the below-average level of water and sanitation practices in the communities. The UNICEF provides backing for the development and execution of district-wide water, sanitation, and hygiene interventions, along with incorporating behavior modification into state and national regulations (Muniyapillai et al., 2022). Human capital, stakeholder engagement process, community participation, agency collaboration and behavior change contribute to Sustainable community development of rural communities through achieving SDG-3, that demands a healthy life and wellbeing, SDG 6.1 advocates fair access to drinking water, while SDG 6.2 seeks to eliminate open defecation and improve sanitation and hygiene services.
Human development and stakeholder engagement construed to be significant in achieving sustainable development outcomes in development work, particularly within the water, sanitation, and hygiene (WASH) sector (Amebelu et al., 2021; Bisung and Elliott, 2016). However, there is a significant gap in empirical research that integrates these theoretical frameworks to empower women, particularly in rural areas where social and infrastructural barriers are more pronounced. While community-based WASH programs are increasingly recognized for their participation potential, the specific roles and challenges faced by women who are often the primary users and managers of household water and sanitation are rarely the central focus (Grant et al., 2019). Most existing studies overlook the gender dynamics that influence WASH outcomes in small villages. Furthermore, research adopting a gender-centric approach remains scarce and fragmented (Sommer et al., 2020).
The present study seeks to fill in this critical gap by foregrounding women's empowerment as a core component of effective WASH interventions. It argues that empowering women through leadership roles, participatory planning, and capacity building not only improve WASH conditions but also significantly contributes to the sustainable development of rural areas. This dimension aligns with the sustainable Development Goals (SDGs), particularly SDG 5 (Gender equality) and SDG 6 (Clean water and sanitation), underscoring the interlinkages between gender empowerment and broader development outcomes (UN Women, 2018). The uniqueness of this study lies in its effort to demonstrate the practical application of integrated theoretical frameworks, specifically human capital theory and stakeholder engagement models. It showcases how women, as agents of change, can influence WASH (Water, Sanitation, and Hygiene) conditions in villages. Through empirical evidence, the study illustrates how supportive environments and institutional backing can promote women-led WASH innovations, ultimately fostering resilient and equitable community development.
Study objective
The current study aims to explore how human capital and stakeholder engagement interventions can enhance WASH-related knowledge, attitudes, and practices among women in the village, thereby promoting sustainable community development.
Review of literature
Yogananth and Bhatnagar (2018) note the alarming conditions surrounding water, sanitation, and hygiene (WASH). Despite having household toilets, 54% of individuals still practice open defecation. This is attributed to several factors, including limited access to water, a preference for open defecation, personal and cultural beliefs, family influences, and a lack of awareness about the health benefits of using bathrooms. Coffey et al. (2014) further substantiate that in five northern Indian states, 40% of households with a functioning toilet have at least one member who defecates in the open. Additionally, more than half of the individuals in households with a government-provided toilet continue to practice open defecation. Routray et al. (2017b) indicate that open defecation is a widespread practice in rural areas, where around 70% of India's population resides, but it is also seen in urban regions. A study by Lee (2017) highlights a critical situation in certain regions of India, where surface water is scarce, rainfall is minimal, and droughts occur frequently. As a result, women and girls often have to walk 3–5 km each day to collect water for their families. Additionally, due to unsanitary conditions, women are more vulnerable to health issues and may face risks of violence when engaging in open defecation.
Dickin et al. (2021) observe that men reported higher levels of empowerment (63%) in water, sanitation, and hygiene compared to women (26%). This highlights a significant gender gap in WASH-related empowerment. Additionally, it suggests that measuring women's empowerment can help identify their specific challenges and develop more effective solutions. By concentrating on the needs of women, policymakers can create more inclusive and impactful WASH programs. Kayser et al. (2021) observe that 0.33%, which is four in every 1,000 women in rural India, reported experiencing non-marital sexual violence in the past year. Ochieng and Onyango (2019) probed that stakeholder analysis had a statistically significant impact (p = 0.05) on the performance of water and sanitation projects. These findings suggest that involving key individuals in water and sanitation initiatives is essential for successful implementation. Similarly, Gero and Willetts (2020) recommended adopting more systematic interventions to enhance water, sanitation, and hygiene efforts. These interventions aim to improve collaboration among local governments and stakeholders, ensuring greater efficiency and more equitable development outcomes. Sommer et al. (2015) opine that engaged and informed community members are more likely to participate actively. Human capital can facilitate community dialogues, discussions, and decision-making processes to create a sense of ownership and sustainability. Bartram and Cairncross (2010) emphasize that individuals with leadership skills can advocate for WASH policies, mobilize resources, and influence decision-makers to prioritize water and sanitation issues. It involves creating a supportive environment for WASH initiatives. UNICEF (2012a,b) rightly views that human capital can be involved in the monitoring and evaluation of WASH interventions, ensuring that programs are effective and sustainable. It requires the ability to collect, analyze, and interpret data related to WASH indicators. Taylor et al. (2015) postulate that human capital can initiate and engage in educational and awareness programs to inform the community about the importance of water, sanitation and hygiene. It includes conducting workshops, seminars, and training sessions. World Health Organization (2004) categorically presents that strengthening the human capital within the community through capacity-building programs enhances the community's ability to understand and implement effective water, sanitation, and hygiene practices.
There are empirical studies that have attempted to prove the community interventions in the area of WASH. Brouwer et al. (2024) state that the community coverage intervention on water, sanitation, and hygiene had the most effect on intervention effectiveness. Community coverage of intervention produces a pervading effect on the factors external to the interventions. The study found that the interventions' effectiveness decreased by decreased levels of existing conditions of WASH or higher baseline disease burden. Quattrochi et al. (2025) observe that the outcome of community intervention revealed that handwashing was observed in the houses of villages. Access ensured in terms of improved facilities for water and sanitation, quality of water available at water points and in households. Hygiene knowledge and practices changed perceptions of WASH governance, reduced school absenteeism in schools, and significantly influenced the physical development of children. Morse et al. (2020) examined before and after trial with a control in rural areas, assessed the relative effectiveness of a multi-faceted hygiene intervention on diarrhoeal disease reduction in the under-five age group. Self-reported outcomes showed there was reduction in diarrhoeal disease with improved hand washing with soap at key moments. Trivedy and Khatun (2025) affirm that the empowered women potential to control their menstrual hygiene better than the domestic water, sanitation and hygiene situation in the households and communities. It suggests that the individual factors better controllable than the community factors that are external to the individual. This creates an immediate call for action to enhance WASH conditions in the communities. Dery et al. (2020) emphasize the importance of creating opportunities for women to assume leadership roles in WASH (Water, Sanitation, and Hygiene) planning and implementation, which benefits the entire community. The study indicates that women in leadership positions within the WASH sector are viewed as authoritative figures and help incorporate women's voices into policy discussions. However, it also highlights that women remain underrepresented among top decision-makers in the WASH committees, and their contributions are often overlooked during meetings. Thus, Water, Sanitation, and Hygiene (WASH) interventions are widely recognized as a crucial role for development of public health and achieving sustainable development goals in rural areas. Within this sphere, the roles and responsibilities of human capital development and stakeholders' engagement are the core facilitating factors for sustainable outcomes. Nevertheless, their integration into women centered empowerment strategies in rural WASH initiatives remains underexplored especially in remote rural areas such as Vaijapur in Karnataka, India.
Human capital theory its integration in WASH, as advocated by Becker (1993), posits that investment in education, skills, and health improves individual productivity and social wellbeing. In the WASH sector, human capital investment manifests through training community members, particularly women, in hygiene practice, water management, and infrastructure maintenance. Further Bisung and Elliott (2016) add that enhancing human capital in WASH contributes to better knowledge dissemination, behaviors change, and community resilience. Women, often the primary water collectors and household sanitation managers, are uniquely positioned to influence community-led outcomes when empowered through education and leadership roles (Sommer et al., 2020).
Stakeholder engagement in Water, Sanitation, and Hygiene (WASH) is a crucial pillar of community-driven development. Arnstein's (1969) ladder of participation provides foundational framework, emphasizing that inclusive decision-making enhances project legitimacy and sustainability. In the WASH context, the stakeholders are from wider areas from government agencies and NGOs to local village councils, Self Help Groups of women, and households. Effective engagement aligns community needs and priorities with institutional goals, and assure contemporary relevance (Mason et al., 2013). According to the Commissioners of the Lancet Commission on Water, Sanitation, Hygiene, and Health (2021), WASH should be recognized not only as a health intervention but also as a catalyst for education, gender equality, and economic productivity. The commissioners' report calls for systematic and cross-sectional investments that empower local leaders, especially women, to lead WASH planning, implementation, and effective governance.
The reviewed studies clearly show the interrelationship between human capital, behavior change, stakeholder engagement and community empowerment, which collectively contribute to sustainable community development, subsequently influencing the achievement of the SDGs in the rural communities. WASH interventions that integrate human capital development and inclusive stakeholders' engagement, particularly those centered on women's empowerment, can catalyze transformative community development. In rural areas such as Vaijapur village, where institutional capacities may be limited, it is essential to develop local knowledge, build trust, and foster community leadership, particularly among women leaders. This approach can help bridge gaps in formal service delivery and, in turn, ensure sustainable development in the future.
Methodology
Ethical consideration
The authors complied all procedures contributing to this work abide by with the ethical standards of the relevant national and institutional committee on human experimentation and with the Helsinki Decleration of 1975, as revised in 2013. The study was approved by the Ethical Committee for the Advanced Studies and Research School of Social and Behavioral Sciences, Central University of Karnataka letter No. CUK/SSBS/CASR/2021-4.
Research design
The current research utilized an AB design, a single-subject methodology consisting of pre (baseline) and post (outcome) phases, to evaluate the impact of a human capital intervention on three behavioral domains: knowledge, attitudes, and practices among female participants in the village. According to Rubin and Babbie (2010), the AB design is the simplest form of single-case evaluation, comprising one baseline phase (A) and one intervention phase (B). Repp and Brusca (1983) highlight the effectiveness of using a single-subject AB design in interventions, noting that it can yield valuable results. Therefore, the AB design is popular among practitioners and researchers, as it includes just one baseline and one outcome phase, minimizing conflicts with service delivery priorities. These assumptions and conditions were met in the present study, justifying the use of the AB design (Table 1).

Table 1. One group pretest-posttest design or A-B design.
Independent variable: Socio-demographic variables, Human capital intervention, Stakeholder engagement.
Dependent variable: Knowledge, attitude, and practice domains of WASH.
Study area
Kalaburagi district is one of the most underdeveloped areas in the Kalyana Karnataka Region, characterized by significant regional disparities within the state of Karnataka, India (see Figure 1) (Manzoor and Channaveer, 2023). Vaijapur village, situated within this district, is considered one of the most disadvantaged villages. The village has a total population of 889 individuals living in 140 households, of which 30 households had migrated and were permanently closed during the data collection period. The female population constitutes 49% of the total, with an overall literacy rate of 60% and a female literacy rate of just 24.6%.
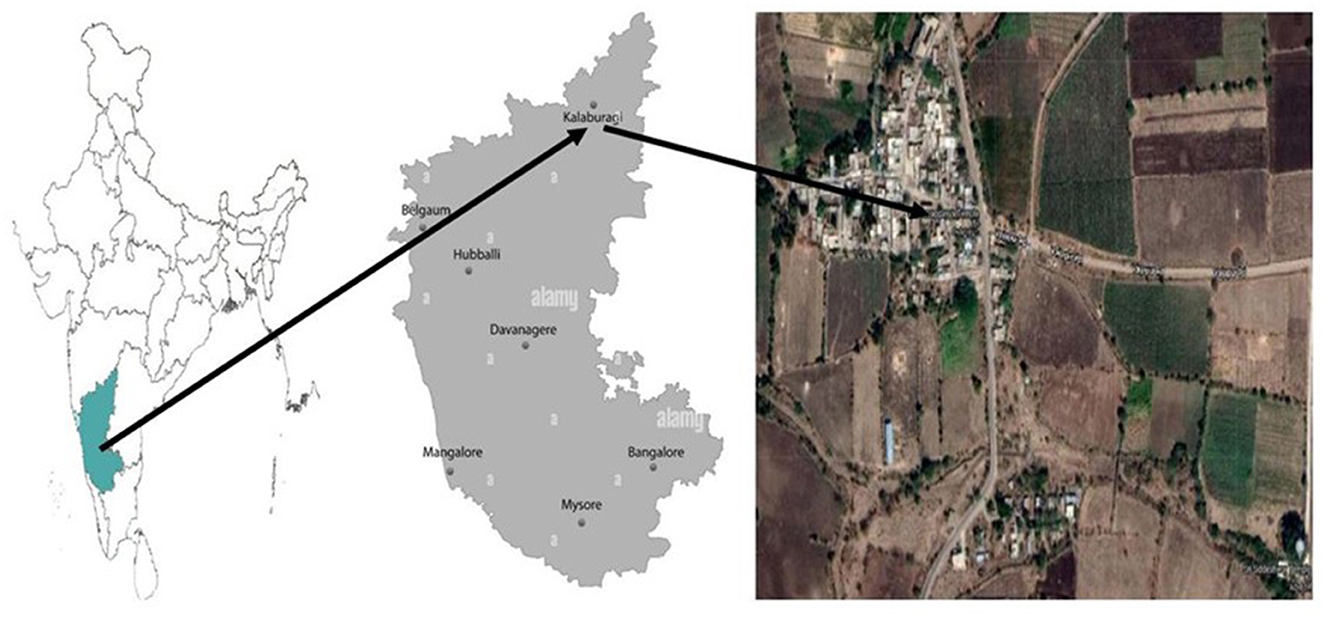
Figure 1. Map of India with Karnataka, Kalaburagi and Vaijapur village images. Source: http://office.incometaxindia, https://www.google.com/maps/place/Vaijapur585213.
Vaijapur village struggles with low per capita income, limited agricultural yields per hectare, and low life expectancy. It is located in an arid agro-climatic zone, where agriculture serves as the backbone of both household and village economies. The major crops cultivated in the village include Tur Dal, Jowar, Sunflower, Groundnut, Bajra, Maize, and Wheat. Many households also rear livestock, particularly goats, cows and buffalo. While agriculture is the primary source of livelihood, additional income is generated through dairy farming, tailoring, and the production of roti and papad (food items) as entrepreneurial activities.
The village is equipped with tanks, bore wells, and open wells that provide sources of irrigation and drinking water.
Sample framework and data collection
The village consisted of 110 households, and the head female members of these households formed the target group for the human capital and stakeholder engagement intervention of the study. Women participants were selected with consideration for cultural and behavioral aspects, as WASH (Water, Sanitation, and Hygiene) is closely connected to women, and gender plays a significant role in social behavior change communication within rural communities.
After establishing rapport with the women's groups and other stakeholders in the village, the researcher developed a community engagement plan to encourage women's participation in WASH initiatives, either individually or in groups. The women were informed about the WASH intervention program, and the stakeholders in the village supported the involvement of women. An open call for participation was made to all women from the 110 households, resulting in the consent of 110 women to take part in the WASH program.
This study ensured representation from women across various social strata, thereby considering factors such as age and socioeconomic conditions to create a diverse sample for the study. The study used a significance level of 0.05, a test power of more than 0.80, and an effect size of ~1 to determine the required sample size. The final sample of 110 is considered a large sample for this study.
Inclusion criteria
The study included women who were recognized as the heads of their households in Vaijapur village. Eligible respondents lived permanently in the village and were actively involved in managing water, sanitation, and hygiene practices (WASH). Only those women who provided consent and demonstrated a willingness to participate were included in the study.
Exclusion criteria
Female household heads who were unavailable during the data collection period due to migration, relocation, or prolonged absence were excluded from the study. Additionally, participants who declined to provide informed consent or were not permanent residents were also excluded.
Data collection tool
The Knowledge, Attitude, and Practice (KAP) tool for Water, Sanitation, and Hygiene (WASH) was designed and developed by Berhe et al. (2020) and was specifically adapted for women participants in the village. This standardized tool assesses three dimensions: knowledge, attitude, and practice, which help evaluate the community's WASH status. The assessment utilized a comprehensive WASH questionnaire consisting of 30 statements. Since English was not the primary language of the respondents, the questionnaire was translated into Kannada, the local language. Two experts validated this Kannada version of the instrument. Participants provided their responses using a five-point Likert scale for knowledge and attitude statements, ranging from “strongly agree” to “strongly disagree,” while practice-related questions were answered with “yes” or “no.” In this context, “strongly disagree” indicated a low level of knowledge and attitude, and “strongly agree” signified a high level. Similarly, a “yes” response indicated good practices, whereas “no” indicated inadequate practices.
Additionally, a socio-economic status tool was developed to profile the women participants in the village.
Statistical analysis
In the present study, descriptive statistics, a paired-sample t-test, and Cohen's d tests were utilized. The paired t-test is commonly employed in social work intervention research to compare participant assessments collected before and after the intervention, allowing for an evaluation of its effectiveness (Rubin and Babbie, 2014). This study ensured that the requirements for conducting the paired t-test were met, including the use of continuous data, independent observations, normal distribution of the data, and the absence of outliers. Moreover, Cohen's d analysis was employed to evaluate the effect size before and after the human capital and stakeholder engagement intervention. Outliers were excluded during the paired-sample t-test.
Human capital and stakeholder engagement intervention
The present study focuses on intervention, where subjects are part of manipulated conditions. Direct exposure and experiential learning involve human participants. Therefore, ethical compliance and clearance were obtained from the Committee for Advanced Studies in Research (CASR) at the Central University of Karnataka. To ensure confidentiality for both the subjects and the data, consent was obtained from the participants and the Gram Panchayat, a local self-government institution, to conduct community interventions at the village level.
The human capital intervention consisted of training sessions for women participants in the village, based on modules developed by WHO and UNICEF regarding WASH (Water, Sanitation, and Hygiene). The researcher, along with resource persons from the district Swachh Bharat Mission, conducted these training programs in two different locations within the village to promote the social inclusion of women by ensuring that all households were enumerated.
Special attention was given to maintain cultural inclusivity throughout the intervention period. Community intervention sessions were held at various locations for the convenience of participants, creating a barrier-free environment for their active and equitable participation. Baseline data was collected in January 2021. The intervention was carried out through oral, visual, demonstration, interaction, and engagement-oriented methods, consisting of 16 sessions totaling 34 h over 16 days in February 2021.
Following this, community mobilization and WASH-related services were addressed. This was succeeded by 15 participatory and focused sessions, which lasted for 60 h, aimed at designing the social entrepreneurship model integration and creating an action plan for implementing, monitoring, and completing toilet construction through a series of community meetings, stakeholder engagement, and participatory interaction. Outcome data was collected after a 90-day gap, in May 2021.
The intervention has addressed the following subjects:
(a) Concept of knowledge: Raise awareness of water, sanitation, and hygiene.
(b) Concept of attitude: Access and utilization of quality water, sanitation, and health promotion,
(c) Concept of practice: Practices related to water, sanitation, and hygiene.
Community intervention sessions and stakeholder engagement process
Community education offers an opportunity to engage village stakeholders in fostering desired changes in people's thinking, behavior, and actions. Intervention sessions were conducted through this stakeholder engagement process, focusing on key themes related to water, sanitation, and hygiene (WASH). Tailored sessions were specifically designed for women participants in the village, incorporating knowledge on WASH and employing a community-based pedagogy approach. These sessions included presentations, open discussions, and metacognitive and reflective activities aimed at enhancing participants' cognitive and practical understanding.
The metacognitive elements introduced during the training allowed participants to develop a better grasp of the content and observe changes in their thinking, which in turn improved their performance. Following the training, village meetings, focus groups, and reflective sessions provided women participants with a platform to share their experiences regarding the implementation of WASH programs. This process of community and stakeholder engagement empowered women to adopt sustainable WASH practices.
Synergy of human capital and stakeholder engagement intervention
Following the initial intervention and prior to the collection of phase-two data, 60 women participants expressed an interest in constructing individual household latrines (IHHL). Subsequently, the researcher initiated a household mobilization task, holding a series of stakeholder meetings with these 60 women, along with Mrs. Sonata Sagar, the Gram Panchayat president (head of local self-government), and two elected Gram Panchayat members—Mrs. Sarubai Jamadar and Mr. Siddesh Kanni.
In collaboration with the Gram Panchayat members, the researcher collected the necessary documents from all 60 households to submit to the Zila Panchayat (district office) to seek approval for constructing toilets under the Swachh Bharat Mission (the Indian government's sanitation campaign). The women participants were motivated by the financial incentives of Rs. 12,000 for general category households and Rs. 15,000 for socio-economically disadvantaged households under the Swachh Bharat Mission.
The 60 women participants pledged to support the Swachh Bharat Mission in their village and subsequently constructed toilets in their households. Additionally, a social entrepreneurship model was integrated to facilitate the implementation of WASH (Water, Sanitation, and Hygiene) programs, based on a WASH action plan designed by local leaders in consultation with the women participants.
The researcher highlighted that rural households often struggle to build toilets due to a lack of financial support. To address this issue, a cost-effective and practical strategy was developed to implement the WASH program across 60 households. Typically, beneficiaries experience long delays in receiving incentives for toilet construction. In response, local leaders stepped in to fund the initial construction of toilets, which helped in coordinating and sourcing the necessary materials. This approach of bulk procurement lowered costs related to materials, transportation, and overall construction for the investors. The potential for profit motivated the investors to complete the construction in one go. Women participants took the lead in monitoring the construction work in their households. As a result, the collaboration of resources—encompassing money, materials, labor, expertise, and agency linkages—created a synergy that enabled the women to successfully complete the construction of 60 toilets in the village.
Results
Table 2 presents the socio-demographic information of the respondents from the community, which consists of a total of 110 households. The respondents demonstrated a harmonious relationship with one another. Among the women participants, the majority (n = 47), representing 42.8%, fell within the age range of 20–39 years. This was followed by 32.7% (n = 36) in the 40–49 age group, and 24.5% (n = 27) of women who were 50 years of age or older.
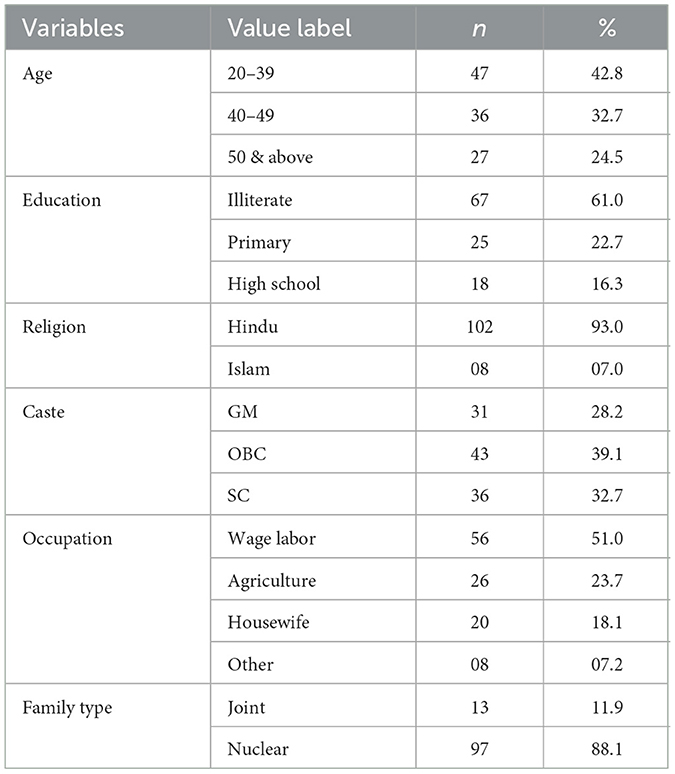
Table 2. Socio-demographic details of the respondents.
The table also details the educational background of the women. It shows that 39.1% (n = 43) have completed education up to the primary and Pre-University Certificate (PUC) levels, while a majority, 61% (n = 67), are illiterate. In terms of religious affiliation, a significant majority, 93% (n = 102), identified as Hindu, while 7% (n = 8) were Islamic.
Regarding caste distribution, 39.1% (n = 43) of the women belong to the Other Backward Class (OBC), 32.7% (n = 36) belong to the Scheduled Caste (SC), and 28.2% (n = 31) belong to the general category. When it comes to occupation, ~51% (n = 56) of respondents rely on wage labor, 23.7% (n = 26) are engaged in agriculture, 18.1% (n = 20) are homemakers, and 7.2% (n = 8) are involved in other activities such as tailoring and stitching.
In terms of family structure, 88.1% (n = 97) of the women live in nuclear families, while only 11.9% (n = 13) reside in joint families.
A paired-sample t-test was conducted to assess whether there was a statistically significant difference in the knowledge levels of female participants between their pre-test and post-test scores (see Table 3). No outliers were identified beyond 1.5 box-lengths from the edges of the box in the boxplot analysis. The findings revealed a statistically significant increase in knowledge scores from the pre-test (M = 2.30, SD = 0.53) to the post-test (M = 5.00, SD = 0.00). Specifically, the mean score increased by 2.70, with a 95% confidence interval of [−2.81, −2.58], t(88) = −47.91, (p < 0.001), and an effect size (d = 0.53). These results indicate a fairly good effect of the intervention.

Table 3. Results of paired samples t-test and descriptive statistics for the WASH knowledge level of women participants by the intervention.
A paired-sample t-test was conducted to determine whether there was a statistically significant mean difference in the attitude of women participants toward access, quality, and water from pre-test to post-test scores (see Table 4). No outliers were detected that were more than 1.5 box-lengths from the edge of the box in a boxplot. There was a statistically significant increase in the attitude toward access, quality, and water scores from the pre-test (M = 18.20, SD = 2.92) to the post-test (M = 23.72, SD = 0.62). A statistically significant mean increase of 5.52, 95% CI [−6.10, 4.93], t(88) = −18.75, p < 0.001, d = 2.77 was observed. The result presents a very high effect size of the intervention.

Table 4. Results of paired samples t-test and descriptive statistics for the attitude of women participants toward access, quality, and water by the intervention.
A paired-sample t-test was conducted to determine whether there was a statistically significant mean difference in the attitude of women participants toward sanitation and health promotion from pre-test to post-test scores (see Table 5). No outliers were detected that were more than 1.5 box-lengths from the edge of the box in a boxplot. There was a statistically significant increase in the attitude toward sanitation and health promotion scores from the pre-test (M = 16.66, SD = 1.08) to the post-test (M = 24.04, SD = 1.09). A statistically significant mean increase of 7.38, 95% CI [−7.57, 7.20], t(88) = −79.81, p < 0.001, d =0.87 was observed. The result explains a good effect size of the intervention.

Table 5. Results of paired samples t-test and descriptive statistics for the attitude of women participants toward sanitation and health promotion by the intervention.
A paired-sample t-test was used to determine whether there was a statistically significant mean difference in the attitude of women participants toward latrine access and utilization from pre-test to post-test scores (see Table 6). No outliers were detected that were more than 1.5 box-lengths from the edge of the box in a boxplot. There was a statistically significant increase in the attitude toward latrine access and utilization scores from the pre-test (M = 15.21, SD = 1.44) to the post-test (M = 21.17, SD = 1.35). A statistically significant mean increase of 5.96, 95% CI [−6.32, −5.60], t(88) = −32.69, p < 0.001, d = 1.72 was found. The result shows a very high effect size of the intervention.

Table 6. Results of paired samples t-test and descriptive statistics for the attitude of women participants toward latrine access and utilization by the intervention.
A paired-sample t-test was used to determine whether there was a statistically significant mean difference in the assessing practices related to water, sanitation, and hygiene among women participants (age group of 20–50 years) from pre-test to post-test scores (see Table 7). No outliers were detected that were more than 1.5 box-lengths from the edge of the box in a boxplot. There was a statistically significant increase in the assessing practices related to water, sanitation, and hygiene among women participants (age group of 20–50 years) scores from the pre-test (M = 1.24, SD =0.45) to the post-test (M = 3.22, SD = 1.13). A statistically significant mean increase of 1.98, 95% CI [−2.24, −1.74], t(88) = −15.74, p < 0.001, d = 1.19 was observed. The result shows a very high effect size of the intervention.

Table 7. Results of paired samples t-test and descriptive statistics for assessing practices related to water, sanitation, and hygiene among women participants (age group of 20–50 years) by the intervention.
Discussion
The study aims to measure how human capital and stakeholder engagement interventions impact the improvement of WASH (Water, Sanitation, and Hygiene) knowledge, attitudes, and practices among women participants. The results indicate a statistically significant increase in WASH knowledge, attitudes, and practices among these women. The intervention activities have positively influenced the participants' behavior, thinking, and belief systems regarding WASH practices. The findings of the study align with a study conducted by Berhe et al. (2020) in rural northern Ethiopia, where a similarly positive impact on WASH knowledge was observed. A significant increase with moderate effect size found in the knowledge domain of the women participants (mean difference = 2.70, 95% CI [−2.81, −2.58], t(88) = −47.91, p < 0.001, d = 0.53). The result of the present study aligns with the study of Melariri et al. (2024) who found significant improvements in South African early childhood development practitioners' knowledge post-structured education program (p < 0.001, 95% CI: 0.58–1.11). In the present study, attitude domain scores of women participants increased with high effect size after the intervention (mean difference = 5.52, 95% CI [−6.10, 4.93], t(88) = −18.75, p < 0.001, d = 2.77), which indicates a dramatic shift toward improved perspectives of the participants regarding access, quality, and utilization of water resources. Similarly, it is evident from the study of Melariri et al. (2024) who also observed attitudinal changes with an increase in mean scores from 18.20 (SD = 2.92) to 23.72 (SD = 0.62), evidencing a large effect size (d = 2.77). The results of Madhu et al. (2024) are consistent with those of the present study. They found improved attitudes toward hygiene and sanitation, as well as hygiene behavior, among the adolescent girls achieved through education interventions carried out in rural India. Analogously, a trial conducted by Sangalang et al. (2022) within the Philippines indicated improved hygiene behavior and good attitudes following intensified health literacy campaigns. Most importantly, this study identified an improved WASH practice in females between 20 and 50 years of age. The mean of practice score improved from 1.24 (SD = 0.45) to 3.22 (SD = 1.13). The results align with the present study, which shows a mean increase of 1.98 (95% CI [−2.24, −1.74], t(88) = −15.74, p < 0.001), resulting in a large effect size (d = 1.19). Evidence for this finding was provided by a quasi-experimental study conducted in Palghar tribal districts of India, which indicated a decrease in diarrheal infections as observed hygiene practice improvements during the post-WASH intervention (Simsek et al., 2024).
At the end, the outcome of the present community intervention study shows a remarkable change in terms of 60 new toilets with handwashing facilities constructed in the households of women participants. The remaining 50 women shown positive frame of mind to construct toilets, but were delayed due to socioeconomic issues like financial problems, lack of decision-making and lack of space in their households. This finding aligns with the study by Shekhar and Dwivedi (2024), which states that open defecation continues to be a common and unavoidable practice among women from lower castes. The female participants reportedly mentioned their economic condition and lack of space as the key reasons for their hesitation in constructing toilets. Routray et al. (2017a) state that in rural Odisha, even women with economic and decision-making power could not construct toilets due to land issues. According to a study by Kanyagui and Viswanathan (2022), the socioeconomic conditions of the women's families were the main influential factors for water and sanitation services.
Thus, the uniqueness of the present study can be observed in the WASH program with a human capital intervention approach, an adopted social and behavioral change communication strategy and an employed stakeholder engagement process. Therefore, the study occupies a significant place in the academic literature. The result and outcome of the present study contribute a notable knowledge base of intersectionality of interdisciplinary knowledge systems particularly in the social work literature and social science literature in general.
Theoretical implications
The theoretical paradigm of the present study is coached in the human capital approach, which focuses on enhance knowledge, attitude, and practice through training sessions. The intervention employed Social Behavior Change Communication (SBCC) strategies incorporating individual and group interactions, rallies, and community engagement activities specifically tailored for women participants. These methods were constructed to foster cognitive, emotional, and behavioral shifts connected to water, sanitation, and hygiene (WASH) practice. Likewise, the social entrepreneurship approach was included to promote sustainable action by implementing a locally practical, community-driven example for toilet construction. By the combination of these theories, the study offers a holistic model for promoting women-led WASH ideas and advancing sustainable community development.
Practical implications
The WASH intervention reflected creative and innovative community transformation potentials, and sustainable outcomes through a community cantered, women led approach. One of the most significant practical outcomes was the activation of broader stakeholder support, including local governance bodies and resource institutions, which extended beyond the initial scope of the intervention. The mobilization of women as primary change makers effectively challenged rooted gender norms, and facilitated inclusive community participation in sanitation initiatives. By fostering an environment where women could take ownership of WASH-related decision-making and implementation, the intervention created a replicable model for similar rural contexts. The use of Social Behavior Change Communication (SBCC) strategies enabled participants to internalize critical health and hygiene messages, while the human capital development approach enhances their capacity to convert knowledge into practical action. Moreover, integrating a social entrepreneurship component allowed community members to identify cost effective, scalable solutions for infrastructure development such as toilet construction that aligned with local needs and resources. Cooperatively, these attempts aided to a sustainable community development model embedded in empowerment, participation, and joint responsibility. The intervention features the value of linking capacity building with participatory governance and locally applicable economic strategies to improve public health and gender equity goals in resource constrained settings.
Sustainable community development models
Studies are reviewed to bring to the fore different models of sustainable community development adopted in the context of WASH program. Mafuta et al. (2020) assert the importance of conflict resolution model in the implementation of the WASH program, which brings to surface many conflicts of various types from the people of the village. The conflicts that thus emerge need to be addressed through community participation for effective implementation of the program. Annan-Aggrey et al. (2022) emphasize the essence of mobilizing the communities of practice model to initiate collaboration with external agencies, shared interest, interaction, and knowledge sharing among people to improve practice for SDGs. Yu et al. (2019) adopted the Train the Trainers approach for the community health workers of Haiti. The training the trainers with a small group could impact the effectiveness of WASH knowledge. The result demonstrated the essence of the training model for effective implementation of the WASH program. Smith et al. (2019) evolved a community-based social marketing approach with social psychology and behavior change theories to select behaviors, identify barriers and benefits, develop strategies, pilot and broad-scale implementation and evaluation of the water- related program. Fu and Ma (2020) throw a new light on the perspective of Self-Governance and Public Participation. Sustainability designed at the national level needs to be translated at the local level to achieve the desired ends. It examines how self-organization, voluntary groups, and the public participation of community members have successfully institutionalized a governing system for the sustainable development of communities. Dreibelbis et al. (2013) employed the Integrated Behavioral Model for Water, Sanitation, and Hygiene. Promotion and provision of low-cost technologies that enable improved water, sanitation, and hygiene (WASH) practices are seen as viable solutions for reducing high rates of morbidity and mortality due to enteric illnesses in low-income countries. Koseoglu et al. (2021) emphasize the importance of the Life Cycle Cost Assessment (LCCA) methodology, which advances investment, acquisition, ownership, maintenance and disposal of the sanitation facility. Investment and interventions that stimulate demand and enhance the capacity of a community are the most cost-effective options for ensuring the sustainability of sanitation facilities in a school. Afzal et al. (2023) postulate that the behavior change interventions are fundamental to achieve sustainability in communities through the identification of new and strengthening the existing positive practices. It is considered central to the quest for sustainable future and solves multidimensional community problems, which require large scale shift in human behavior with regard to their health, social, physical activities and long held habits.
Thus, several theoretical models, explanatory frameworks, and decision-making models have emerged which attempt to guide behavior change interventions related to WASH. The critical viewpoint of an integrated model of human capital, stakeholder engagement, social behavior change and communication and social entrepreneurship adopted in the current study is unique in itself and also an addition to the literature on sustainable community development models discussed in the implementation of the WASH programs.
Challenges faced and sustainability
Building a community rapport was not an easy task for the researcher because the researcher was an outsider to the community. To gain a good rapport with the community, the researcher stayed in the village for 3 months and actively participated in the community and family functions of the village. Working exclusively with the women members of the village was another uphill task to maintain good rapport and communication. Gender bias and prejudices commonly held by the villagers make women encounter challenges and pose barriers to open communication and interactions. Continuous stay in the village provided an opportunity for consistent engagement with the community members. Individual household visits and meetings with the stakeholders of the village created a conducive environment for barrier-free communication, relationships, and interactions. Later, the community members and stakeholders framed a favorable attitude and conduct toward the researcher. Social capital and cultural capital approaches are rightly initiated and integrated as a preliminary process for community intervention. Human capital and stakeholder engagement intervention generated a positive, collaborative and constructive frame of mind among the women members of the village, contributing to a sustainable community change through women's empowerment. Community living of a social change agent makes a lot of difference in understanding the village, mobilizing the village and guiding the village toward a desired change in order to achieve sustainable village development.
Impact of human capital and stakeholder engagement intervention
The study impact is quite glaring and significant as well
• Consequent to human capital and stakeholder engagement intervention, there was a sudden spurt in community consciousness, community mobilization, and community action toward WASH.
• During the intervention period of the study, 60 new Individual Household Latrines (IHHL) were constructed.
• Installation of a handwashing facility at the village school and improving hygiene education and practices among students.
• Active participation of the local key stakeholders like Anganwadi (pre-school center) teacher, Gram Panchayat (local self-government) president and members, who collectively committed to construction of toilets and ensure effective implementation of the WASH initiatives in the village.
• The village achieved significant progress toward becoming open defecation-free (ODF), fostering a sustainable and healthier living environment
• Community engagement model, driven by Social Behavior Change Communication (SBCC), stakeholders' participation, and a social entrepreneurship approach, empowered women to lead the sanitation movement and become change makers. And played a catalyst role in moving toward sustainable community development through the WASH initiatives.
• The initiative demonstrated a direct contribution and realization of Sustainable Development Goal 3 (Good Health and Wellbeing) and goal 6 (Clean Water and Sanitation) establishing clear linkage between local action and global development frameworks.
Limitations of the study
Although the present study presents expected desired changes due to WASH intervention in the village, the results present some limitations. The findings and large effect size of the results though show a glaring change but are limited to the context and culture of the communities. The background of the study village (Vaijapur) that located remotely and has a poor socio-economic and educational background with closed network and open interactions among the villagers, paved the way for the effectiveness of the intervention. The sample covered mostly women of the village. The women in a remote village have less mobility, their engagement is limited to household and agriculture activities, but they possess trust and bond-based interactions. Such a context provides an advantage for external intervention with gender-sensitive approaches. Since the study is village-focused, it does not have representativeness and randomness in the selection of the sample from other communities to facilitate generalizations of the results. The experimental design with an experimental and control group is free from biases, which the present study lacks. However, the study confirms that a similar impact of WASH interventions can be expected, provided a similar community context is ascertained.
Conclusion
The human capital and stakeholder engagement intervention of the study integrates the concept and theory of human capital into social work practice through a community education model. Converting human capital and stakeholder engagement, a theoretical framework into an application framework and practice model is the right appropriation that is necessary in the social work discipline. Merging human capital intervention with social behavior change and communication strategy, integrating it through the stakeholder engagement and the social entrepreneurship approach contribute a multidisciplinary knowledge framework inherently potential to advocate for sustainable community development. Such a framework intends to bring the desired and sustainable change in the social, behavioral and cultural domains of the village. The study also advocates the essence of WHO and UNICEF training modules rightly adopted into the implementation process of the WASH programs in rural India. Adopting single-subject design, the study witnessed by-product results that indicate a path of realizing Sustainable Development Goal 3, ensuring a healthy life and promoting wellbeing, and Sustainable Development Goal 6, confirming the availability of sustainable water and sanitation management for rural communities. The study highlights that the social, economic, health, and educational barriers for women, who have less income, low life expectancy, and less literacy level, could be overcome due to a decisive impact of the capacity-building, stakeholder engagement process and hand-holding support extended to them. These are indicative of a potential nullifying effect to negative conditions in the communities. Subsequently, the human capital could generate human assets that could produce and facilitate a positive change in the villages. It is therefore inferred that the gender plays a decisive role in the participatory development process of the village. Thus, the present study sets a new practice paradigm of empower women to empower villages or communities.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Department of Social Work, Central University of Karnataka India. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
SP: Conceptualization, Data curation, Investigation, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing. MC: Conceptualization, Formal analysis, Funding acquisition, Investigation, Project administration, Resources, Writing – original draft, Writing – review & editing. RC: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frsus.2025.1562033/full#supplementary-material
References
Afzal, A., Jabeen, T., and Javed, M. (2023). Behavior change interventions regarding WASH and its impacts on sustainable community development: a study of district Gujrat, Pakistan. J. Hum. Behav. Soc. Environ. 33, 1160–1177. doi: 10.1080/10911359.2022.2131023
Amebelu, A., Ban, R., Bhagwan, J., Chilengi, R., Chandler, C., Colford, J. M., et al. (2021). The Lancet Commission on water, sanitation and hygiene, and health. Lancet 398, 1469–1470. doi: 10.1016/S0140-6736(21)02005-5
Annan-Aggrey, E., Arku, G., Atuoye, K., and Kyeremeh, E. (2022). Mobilizing ‘communities of practice' for local development and accleration of the Sustainable Development Goals. Local Econ. 37, 219–229. doi: 10.1177/02690942221101532
Arnstein, S. R. (1969). A ladder of citizen participation. J. Am. Inst. Plann. 35, 216–224. doi: 10.1080/01944366908977225
Banerjee, T., Shukla, B. N., Filgona, J., Anupurba, S., and Sen, M. R. (2014). Trends of typhoid fever seropositivity over ten years in north India. Indian J. Med. Res. 140, 310–313.
Bartram, J., and Cairncross, S. (2010). Hygiene, sanitation, and water: forgotten foundations of health. PLoS Med. 7, 01–09. doi: 10.1371/journal.pmed.1000367
Becker, G. S. (1993). Human Capital: A Theoretical and Empirical Analysis, with Special Reference to Education (3rd ed.). Chicago, IL: University of Chicago Press. doi: 10.7208/chicago/9780226041223.001.0001
Berhe, A. A., Aregay, A. D., Abreha, A. A., Aregay, A. B., Gebretsadik, A. W., Negash, D. Z., et al. (2020). Knowledge, attitude, and practices on water, sanitation, and hygiene among rural residents in Tigray Region, Northern Ethiopia. J. Environ. Public Health 2020, 1–9. doi: 10.1155/2020/5460168
Bethony, J., Brooker, S., Albonico, M., Geiger, S. M., Loukas, A., Diemert, D., et al. (2006). Soil-transmitted helminth infections: ascariasis, trichuriasis, and hookworm. Lancet 367, 1521–1532. doi: 10.1016/S0140-6736(06)68653-4
Bisung, E., and Elliott, S. J. (2016). Toward a social capital-based framework for understanding the water-health nexus. Soc. Sci. Med. 148, 243–250. doi: 10.1016/j.socscimed.2014.01.042
Brouwer, A. F., Zahid, M. H., Eisenberg, M. C., Arnold, B. F., Ashraf, S., Benjamin-Chung, J., et al. (2024). Understanding the effectiveness of water, sanitation, and hygiene interventions: a counterfactual simulation approach to generalizing the outcomes of intervention trials. Environ. Health Perspect. 132:127003. doi: 10.1289/EHP15200
Caruso, B. A., Clasen, T., Yount, K. M., and Cooper, H. L. (2018). Assessing women's negative sanitation experiences and concerns: the development of a novel sanitation insecurity measure. Int. J. Environ. Res. Public Health 14:755. doi: 10.3390/ijerph14070755
Coffey, D., Gupta, A., Hathi, P., Khurana, N., Srivastav, N., Vyas, S., et al. (2014). Open defecation: evidence from a new survey in rural north India. Econ. Polit. Weekly 49, 43–55.
Commissioners of the Lancet Commission on Water Sanitation, Hygiene, and Health. (2021). The Lancet Commission on water, sanitation and hygiene, and health. Lancet 398, 1469–1470.
Dery, F., Bisung, E., Dickin, S., and Dyer, M. (2020). Understanding empowerment in water, sanitation and hygiene (WASH): a scoping review. J. Water Sanit. Hyg. Dev. 10, 5–15. doi: 10.2166/washdev.2019.077
Dickin, S., Bisung, E., Nansi, J., and Charles, K. (2021). Empowerment in water, sanitation and hygiene index. World Dev. 137, 1–12. doi: 10.1016/j.worlddev.2020.105158
Dreibelbis, R., Winch, P. J., Leontsini, E., Hulland, K. R. S., Ram, P. K., Unicomb, L., et al. (2013). The Integrated Behavioural Model for Water, Sanitation, and Hygiene: a systematic review of behavioural models and a framework for designing and evaluating behaviour change interventions in infrastructure-restricted settings. BMC Public Health 13, 2–13. doi: 10.1186/1471-2458-13-1015
Fu, Y., and Ma, W. (2020). Sustainable urban community development: a case study from the perspective of self-governance and public participation. Sustainability 12:617. doi: 10.3390/su12020617
Gero, A., and Willetts, J. (2020). Securing a conducive environment for WASH markets. Waterlines 39, 44–60. doi: 10.3362/1756-3488.18-00026
Grant, M., Willetts, J., Huggett, C., and Willets, R. (2019). Gender equality and goal achievement in WASH: an integrated approach. Dev. Prac. 29, 582–596. Available online at: https://waterpartnership.org.au/wp-content/uploads/2016/08/Gender-Goal6-Critical-Connection.pdf
Jacob, M., and Saggu, J. K. (2024). “Menstrual hygienic disparity in India: an inter-state analysis using NFHS-5 indicators,” in Indian Families: Contemporary Family Structures and Dynamics, eds. V. Chandra, and S. Blair (Leeds: Emerald Publishing Limited), 77–95. doi: 10.1108/S1530-353520240000026005
Jana, S., Fu, S. H., Gelband, H., Brown, P., and Jha, P. (2022). Spatio-temporal modelling of malaria mortality in India from 2004 to 2013 from the Million Death Study. Malaria J. 21, 1–10. doi: 10.1186/s12936-022-04112-x
Jenkins, M. W., Freeman, M. C., and Routray, P. (2014). Measuring the safety of excreta disposal behaviour in India with the new safe san index: reliability, validity, and utility. Int. J. Environ. Res. Public Health 11, 8319–8346. doi: 10.3390/ijerph110808319
Kanungo, S., Chatterjee, P., Saha, J., Pan, T., Chakrabarty, N. D., and Dutta, S. (2021). Water, sanitation, and hygiene practices in urban slums of Eastern India. J. Infect. Dis. 2, 573–583. doi: 10.1093/infdis/jiab354
Kanyagui, M. K., Rajendrakumar, S., and Viswanathan, P. K. (2024). Institutional arrangements for improving water and sanitation services in the rural villages of India: a systems thinking approach. World Water Policy 10, 480–510. doi: 10.1002/wwp2.12172
Kanyagui, M. K., and Viswanathan, P. K. (2022). Water and sanitation services in India and Ghana: an assessment of implications for rural health and related SDGs. Water Policy 24, 1073–1094. doi: 10.2166/wp.2022.079
Kayser, G. L., Chokhandre, P., Rao, N., Singh, A., McDougal, L., and Raj, A. (2021). Household sanitation access and risk for non-marital sexual violence among a nationally representative sample of women in India, 2015-16. SSM Popul. Health 13:100738. doi: 10.1016/j.ssmph.2021.100738
Kirithika, S., Kumar, L. M., Kumar, M. K., Keerthana, E., and Lohalavanya, R. (2020). Smart public toilets using IoE. 2020 Int. Confer. Emerg. Trends Inf. Technol. Eng. 1, 1–5. doi: 10.1109/ic-ETITE47903.2020.429
Koseoglu, N. M., Ellis, R., and Biswas, D. (2021). Scenario-based life-cycle cost assessment to support sustainable investment in rural communal sanitation facilities: application to a school-based sanitation facility. J. Water Sanitation Hygiene Dev. 11:771. doi: 10.2166/washdev.2021.230
Lee, Y. J. (2017). Informing women and improving sanitation: evidence from rural India. J. Rural Stud. 55, 203–215. doi: 10.1016/j.jrurstud.2017.07.012
Madhu, M., Ravindra, B. N., Surabhi, K. S., Raghunath, D. K., Shobha, M., and Rajesh, V. (2024). Evaluation of a menstrual hygiene education program for adolescent girls in Rural India. Nurs. Women's Health 28, 446–456. doi: 10.1016/j.nwh.2024.08.002
Mafuta, W., Zuwarimwe, J., Kamuzhanje, J., and Mwale, M. (2020). Sustainable conflict resolution through community based water, sanitation and hygiene (WASH) planning in fragile and conflict situations: the case of Somalia. J. Asian Afr. Stud. 56, 352–363. doi: 10.1177/0021909620928104
Manzoor, R., and Channaveer, R. M. (2023). Impact of capacity building intervention on knowledge about disability among village rehabilitation workers in Kalaburagi, Karnataka India. J. Hum. Behav. Soc. Environ. 33, 1036–1050. doi: 10.1080/10911359.2023.2262003
Mason, N., Matoso, M., and Smith, W. (2013). “A post-2015 global goal for water: sufficient, safe, affordable and sustainable water for all,” in ODI Working Paper. London: Overseas Development Institute (ODI).
Melariri, P. E., Teare, J., Oyedele, O., Eastwood, K., and ten Ham-Baloyi, W. (2024). Impact of an educational intervention on water, sanitation and hygiene knowledge, attitudes, and practices in early childhood development centres in low-socio-economic areas in the Nelson Mandela Bay, South Africa. PLoS ONE 19:e0303077. doi: 10.1371/journal.pone.0303077
Morse, T., Tilley, E., Chidziwisano, K., Malolo, R., and Musaya, J. (2020). Health outcomes of an integrated behaviour-centred water, sanitation, hygiene and food safety intervention-a randomised before and after trial. Int. J. Environ. Res. Public Health. 17:2648. doi: 10.3390/ijerph17082648
Muniyapillai, T., Kulothungan, K., Vignesh, N. J., Dharmaraj, R. B., George, N., Kulothungan Sr., K., et al. (2022). Water, sanitation, and hygiene (WASH) practices among households in Perambalur District: a cross-sectional study. Cureus 14, 1–8. doi: 10.7759/cureus.30115
Ochieng, H., and Onyango, J. (2019). Influence of stakeholder analysis on the performance of water and sanitation projects in Homabay County. Kenya 1, 48–47.
Pruss-Ustun, A., Wolf, J., Bartram, J., Clasen, T., Cumming, O., Freeman, M. C., et al. (2019). Burden of disease from inadequate water, sanitation, and hygiene for selected adverse health outcomes: an updated analysis with a focus on low-and middle-income countries. Int. J. Hygiene Environ. Health 222, 765–777. doi: 10.1016/j.ijheh.2019.05.004
Quattrochi, J. P., Croke, K., Dohou, C., Ghib, L. S., Lokaya, Y., Coville, A., et al. (2025). Effects of a community-driven water, sanitation, and hygiene intervention on diarrhea, child growth, and local institutions: a cluster-randomized controlled trial in rural Democratic Republic of Congo. PLoS Med. 22:e1004524. doi: 10.1371/journal.pmed.1004524
Raza, F. (2018). Hidden Failures and a Malnourished South: Health and Nutrition in Chhattisgarh. Available online at: https://www.orfonline.org/search?q=hidden-failures
Repp, A. C., and Brusca, R. M. (1983). Single-subject research: basic designs for research in special education. Except. Educ. Q. 4, 27–39. doi: 10.1177/074193258300400306
Routray, P., Torondel, B., Clasen, T., and Schmidt, W. P. (2017a). Women's role in sanitation decision making in rural coastal Odisha, India. PLoS ONE 12:e0178042. doi: 10.1371/journal.pone.0178042
Routray, P., Torondel, B., Jenkins, M. W., Clasen, T., and Schmidt, W. P. (2017b). Processes and challenges of community mobilisation for latrine promotion under Nirmal Bharat Abhiyan in rural Odisha, India. BMC Public Health 17, 1–15. doi: 10.1186/s12889-017-4382-9
Rubin, A., and Babbie, E. (2010). Research Methods for Social Work, 7th Edn. Belmont, CA: Wadsworth Publishing Co Inc.
Saikia, N., Bora, J. K., and Luy, M. (2019). Socioeconomic disparity in adult mortality in India: estimations using the orphanhood method. Genus 75, 1–14. doi: 10.1186/s41118-019-0054-1
Sangalang, S. O., Lemence, A. L. G., Ottong, Z. J., Valencia, J. C., Olaguera, M., Canja, R. J. F., et al. (2022). School water, sanitation, and hygiene (WaSH) intervention to improve malnutrition, dehydration, health literacy, and handwashing: a cluster-randomised controlled trial in Metro Manila, Philippines. BMC Public Health 22:2034. doi: 10.1186/s12889-022-14398-w
Shekhar, S., and Dwivedi, A. (2024). Gendered disparities in water and sanitation through an intersectional lens: emphasising women's perspectives. Space Cult. India 11, 20–39. doi: 10.20896/saci.v11i4.1410
Simsek, S., Ocek, Z. A., Turk, M., and Unver, A. (2024). Assessment of water, sanitation, and hygiene among women living in precarious households in a Turkish urban area. BMC Women's Health 24:18. doi: 10.1186/s12905-023-02861-8
Smith, L. K. M., Lynes, J. K., and Wolfe, S. E. (2019). Community-based social marketing—creating lasting, sustainable, environmental change: case study of a household stormwater management program in the region of Waterloo, Ontario. Soc. Market. Q. 25, 308–326. doi: 10.1177/1524500419883288
Sommer, M., Ferron, S., Cavill, S., and House, S. (2015). Violence, gender, and WASH: spurring action on a complex, under-documented and sensitive issue. Environ. Urbaniz. 27, 105–116. doi: 10.1177/0956247814564528
Sommer, M., Ferron, S., Cavill, S., and House, S. (2020). Violence, gender and WASH: spurring action on a complex, under-documented and sensitive topic. Environ. Urbaniz. 27, 105–116.
Talat, U., Ravenscroft, L., and Vlaev, I. (2023). Development of a behaviour change intervention to promote sanitation and latrine use in rural India. BMC Public Health 23, 1–12. doi: 10.1186/s12889-023-17061-0
Taylor, D. L., Kahawita, T. M., Cairncross, S., and Ensink, J. H. (2015). The impact of water, sanitation and hygiene interventions to control cholera: a systematic review. PLoS ONE 10:e0135676. doi: 10.1371/journal.pone.0135676
Trivedy, A., and Khatun, M. (2025). Women's empowerment and water, sanitation, and hygiene in India: exploring the present situation and correlation using geostatistical techniques. SN Soc. Sci. 5:37. doi: 10.1007/s43545-025-01073-1
UN Women (2018). Turning Promises into Action: Gender Equality in the 2030 Agenda for Sustainable Development. United Nations Entity for Gender Equality and the Empowerment of Women. Available online at: https://www.unwomen.org/en/digital-library/publications/2018/2/gender-equality-in-the-2030-agenda-for-sustainable-development-2018
UNICEF (2012a). Raising Even More Clean Hands. Advancing Health, Learning, and Equity Through WASH in Schools. New York, NY: UNICEFPress.
UNICEF (2012b). Towards Better Programming: A Water Handbook. United Nations Children's Fund. New York, NY: UNICEFPress.
UNICEF and WHO. (2021). The Measurement and Monitoring of Water Supply, Sanitation and Hygiene (WASH) Affordability. UNICEF and World Health Organization.
WHO-UNICEF (2022). Estimates of Progress in Household Drinking Water, Sanitation, and Hygiene. Geneva: WHO; New York, NY: UNICEF.
World Health Organization (2004). Water, Sanitation and Hygiene Links to Health: Facts and Figures. Geneva: WHO Press.
World Health Organization (2018). Health Gains from the Swachh Bharat Initiative. Geneva: WHO Press.
World Health Organization (2023). Monitoring Health for the Sustainable Development Goals (SDGs). Geneva: WHO Press.
Yogananth, N., and Bhatnagar, T. (2018). Prevalence of open defecation among households with toilets and associated factors in rural south India: an analytical cross-sectional study. Trans. R. Soc. Trop. Med. Hygiene 112, 349–360. doi: 10.1093/trstmh/try064
Yu, X., Pendseb, A., Slifkoc, S., Inmana, A. G., Konga, P., and Knetteld, B. A. (2019). Healthy people, healthy community: evaluation of a train-the-trainers programme for community health workers on water, sanitation and hygiene in rural Haiti. Health Educ. J. 78, 931–945. doi: 10.1177/0017896919853850
Keywords: human capital intervention, sustainable community development, wash, sustainable development goals, women empowerment
Citation: Pawar S, Chougule M and Channaveer RM (2025) Human capital and stakeholder engagement intervention: a women empowerment pathway to achieve sustainable community development in water, sanitation, and hygiene at Vaijapur Village of Karnataka, India. Front. Sustain. 6:1562033. doi: 10.3389/frsus.2025.1562033
Received: 16 January 2025; Accepted: 03 June 2025;
Published: 01 July 2025.
Edited by:
Girish V. G., Catholic University of Korea, Republic of KoreaReviewed by:
Ann Suwaree Ashton, National Institute of Development Administration, ThailandThi Yen Do, Nanhua University, Taiwan
Copyright © 2025 Pawar, Chougule and Channaveer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mahesh Chougule, ZHJtYWhlc2hAdHUuYWMudGg=