 Joaquim Barreto
Joaquim Barreto Alessandra M. Campos-Staffico
Alessandra M. Campos-Staffico Wilson Nadruz3
Wilson Nadruz3 Thiago Quinaglia
Thiago Quinaglia Andrei C. Sposito
Andrei C. Sposito- 1Laboratory of Atherosclerosis and Vascular Biology, University of Campinas (Unicamp), Campinas, Sao Paulo, Brazil
- 2Department of Clinical Pharmacy, College of Pharmacy, University of Michigan, Ann Arbor, MI, United States
- 3Cardiology Division, Clinics Hospital, Unicamp, Campinas, Sao Paulo, Brazil
- 4Massachussets General Hospital, Harvard University, Boston, MA, United States
Sodium glucose cotransporter 2 inhibitors (SGLT2) have been increasingly pursued as a promising target for addressing residual cardiovascular risk. Prior trials demonstrated that SGLT2i not only promotes glucose-lowering, but also improves endothelial dysfunction, adiposity, fluid overload, and insulin sensitivity thus contributing to hemodynamic changes implicated in its cardiorenal benefits. The mechanisms in the effect of SGLT2i on blood pressure and their potential role in preventing cardiovascular events are hereby revised.
Introduction
Cardiovascular disease remains the leading cause of death and disability in individuals with type 2 diabetes (T2D) (1). For a long time, achieving optimal glycemic control has been the primary goal of diabetes care due to robust evidence associating glucotoxicity with the progression of both micro- and macrovascular complications (2). However, recent findings have revealed that even with stricter glycemic control, the cardiovascular risk in T2D does not parallel that of healthy individuals (3, 4). The persistence of this risk, despite all the therapeutic interventions, is referred to as the residual cardiovascular risk. This is attributed to the complex, multi-faceted pathophysiology of T2D, which includes not only glucotoxicity but also other risk factors such as hypertension, adiposity, impaired cardiac energy metabolism, dyslipidemia, and kidney failure (5).
As a consequence, the development of new therapeutic targets that address these detrimental pathways alongside glucose-lowering has emerged as an encouraging approach to mitigate residual cardiovascular risk (6). This review provides a comprehensive exploration of the novel mechanistic insights that highlight the significant role of sodium-glucose cotransporter-2 inhibitors (SGLT2i) in attenuating residual cardiovascular risk in T2D. Specifically, we shed light on their blood pressure lowering effect, thereby positioning SGLT2i as reliable therapeutic agents in mitigating cardiovascular complications associated with T2D.
Hypertension
Hypertension is highly prevalent among individuals with T2D, significantly increasing the risk of cardiovascular disease on top of an already heavy burden (7, 8). Considering that both conditions overlap risk factors and pathophysiological pathways, it is estimated that half of individuals with hypertension have insulin resistance, and up to 85% of individuals with T2D also have hypertension (9). Experimental studies have shown that high blood pressure upregulates pathways related to insulin resistance, while T2D triggers the overactivation of the renin-angiotensin-aldosterone system and sympathetic tone, resulting in elevated blood pressure (7, 10). The interplay between T2D and hypertension synergically worsens cardiovascular risk (11, 12). Accordingly, individuals with both conditions have a twofold increase in cardiovascular mortality compared to those with only T2D or hypertension, and this effect linearly grows as blood pressure rise (13, 14). Promisingly, SGLT2i have demonstrated the ability to lower blood pressure whilst optimizing glycemic control (Figure 1).
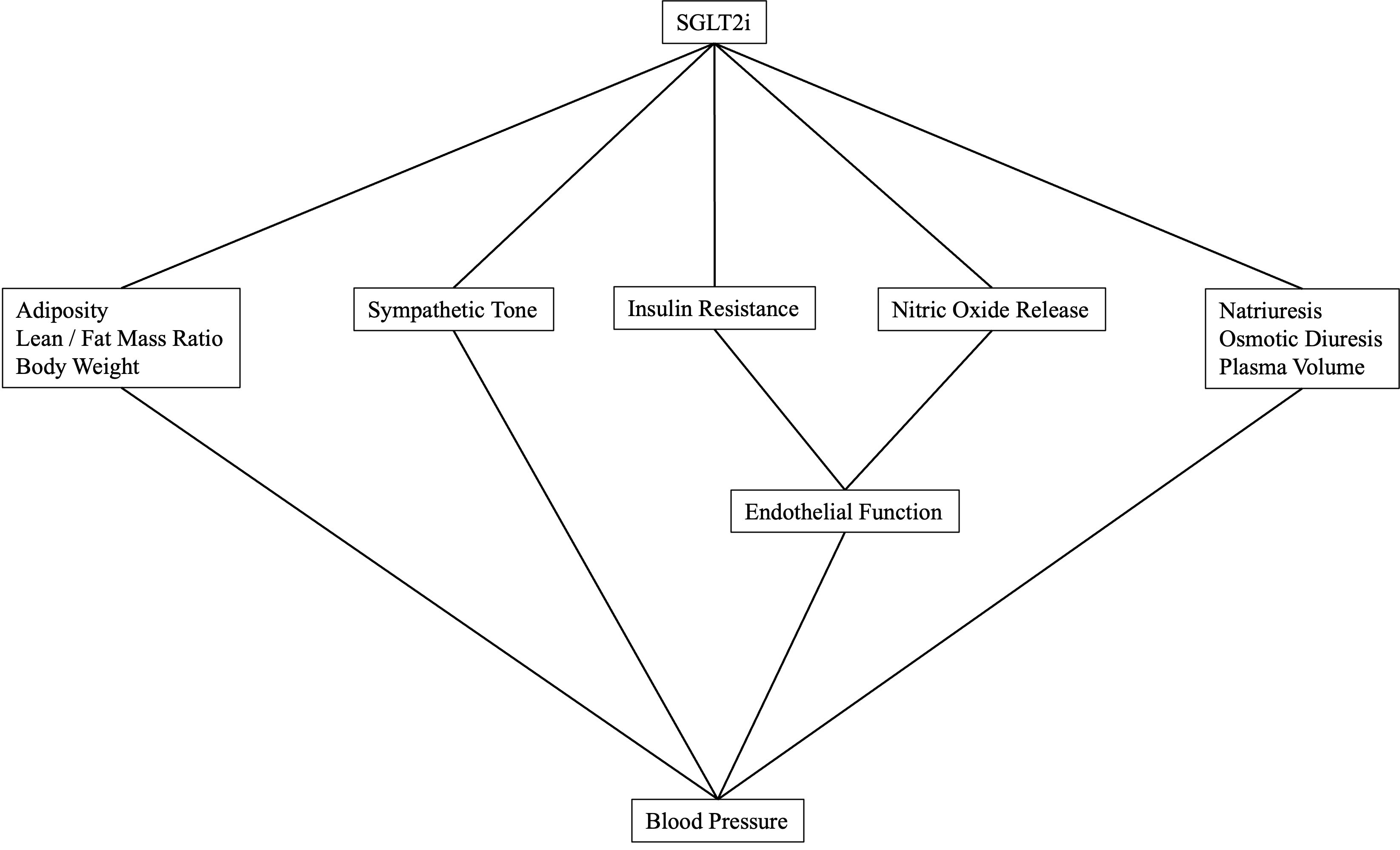
Figure 1 Mechanisms involved in blood pressure reduction by SGLT2i.
In comparison to placebo, SGLT2i reduces 24-hour systolic and diastolic blood pressures by an average of 4 mmHg and 2 mmHg, respectively. This reduction remains consistent regardless of baseline blood pressure or changes in weight (15, 16). Given that a 10 mmHg drop in systolic blood pressure is estimated to decrease incident cardiovascular events by 12%, the impact of SGLT2i on blood pressure could significantly reduce morbidity (17, 18). Furthermore, despite evidence supporting stricter blood pressure targets for individuals at higher cardiovascular risk is beneficial for preventing adverse events, real-world data shows that less than a third of individuals with T2D meet these targets (19–21). SGLT2i could enhance the effects of concomitant antihypertensive drugs, thus improving compliance with blood pressure goals and reducing the incidence of adverse outcomes (20, 22).
Osmotic diuresis
Until recently, blood pressure reduction through SGLT2i was attributed solely to osmotic diuresis. To investigate this further, Heerspink et al. (23) conducted a study on well-controlled individuals with T2D and examined the effect of 12 weeks of dapagliflozin treatment on radiolabeled-estimated plasma volume (23). The results showed that dapagliflozin led to a 7% decrease in plasma volume and a 10 mmHg reduction in 24-hour systolic blood pressure compared to the placebo group (23). While these early hemodynamic changes may be influenced by this mechanism, compensatory renal responses occurred due to plasma volume changes, ultimately restoring homeostasis (24).
In a related study, Scholtes et al. (24) explored the effects of dapagliflozin treatment on individuals with T2D on standardized sodium intake regimens. They found that dapagliflozin upregulated multiple water-conservation compensatory pathways, including vasopressin-mediated water retention, hyperactivation of the renin-angiotensin-aldosterone system, and a sharp decrease in fractional urea excretion (24–26). Consequently, renal adaptative responses play a significant role in mitigating the impact of volume contraction on SGLT2i-induced hemodynamic changes, suggesting the involvement of other concurrent pathways.
Sympathetic tone
Adrenergic overdrive plays a pivotal role in the pathogenesis of hypertension and the progression of end-organ damage (27). In individuals with hypertension, the presence of T2D intensifies the hyperactivation of sympathetic tone, leading not only to elevated blood pressure but also an increased risk of left ventricle hypertrophy, myocardial infarction, heart failure, stroke and mortality (28–31). A study by Hamaoka et al. (32) demonstrated that a 12-week treatment with dapagliflozin in patients with heart failure resulted in a decrease in muscle sympathetic nerve activity and resting heart failure whilst reducing blood pressure. Similarly, Balcıoğlu et al. (33) found that a 24-week treatment with dapagliflozin improved heart rate variability and prevented ventricular premature beats, whereas SGLT2i therapy also prevented vaso-vagal syncope in the SCAN study (34).
These findings suggest that SGLT2i modulation of the autonomic nervous system may contribute to blood pressure reduction and potentially attenuate residual cardiovascular risk. However, further investigation is necessary to gain a comprehensive understanding of the underlying mechanisms of these drugs.
Insulin resistance and endothelial dysfunction
Insulin resistance and endothelial dysfunction, which are key contributors to cardiovascular risk, are associated with increased blood pressure that could be prevented through the use of SGLT2i (35). Insulin plays a pivotal role in regulating blood pressure through two pathways: (i) the phosphatidylinositol 3-kinase (PI3K)/protein kinase-B (Akt)/nitric oxide (NO) pathway, which promotes vasodilatation and, ultimately, decrease blood pressure; and (ii) the mitogen-activated protein kinase (MAPK)/endothelin-1 (ET-1) pathway, which causes vasoconstriction and elevates blood pressure (36). In the presence of insulin resistance, the activity of the MAPK/ET-1 pathway dominates over that of the PI3K/Akt/NO pathway, leading to vasoconstriction with elevated blood pressure prevailing (36). Furthermore, insulin resistance has also been associated with hyperactivated sympathetic tone, activation of the renin-angiotensin aldosterone system, and increased salt-sensitivity; all of which are implicated in hypertension (12, 37–40).
Previous studies have demonstrated that SGLT2i therapy improves endothelial function and insulin sensitivity (41). For instance, in the ADDENDA trial, an open-label prospective randomized clinical trial that enrolled 98 individuals with T2D and carotid atherosclerotic disease, the efficacy of dapagliflozin treatment was examined over a 12-week period. The results demonstrated significant improvements in vasomotor function and increased plasma nitrite levels (42). This study adds to existing evidence that SGLT2i possess multiple beneficial effects. They have been shown to reduce oxidative stress, modulate adhesion molecules, and exhibit anti-inflammatory and anti-apoptotic properties. These collective effects ultimately contribute to the restoration of endothelial function (43–45).
SGLT2i also improve insulin sensitivity. A study by Merovci et al. (46) showed that 14 days of dapagliflozin therapy led to significant improvements in insulin-stimulated glucose disposal in individuals with T2D, suggesting increased muscle insulin sensitivity (46). Glycosuria was partially compensated by an increase in endogenous glucose synthesis following increased glucagon levels (46). Accordingly, Rodriguez et al. found that 12-week treatment with dapagliflozin improved insulin sensitivity, as assessed by serial measurements of plasma insulin and glucose levels adjusted for urinary glucose excretion, in a group of 24 adults with pre-diabetes undergoing oral glucose tolerant test (47). Although the mechanisms involved in SGLT2i abrogation of insulin resistance remains under debate, prior experiments suggest that SGLT2i prevention of glucotoxicity-induced oxidative stress of beta-cells may partially answer for this effect (48).
A recent meta-analysis with 55 clinical trials and over 36 thousand patients demonstrated that all SGLT2i consistently reduce serum uric acid (SUC) levels, compared to placebo, and this may contribute to insulin resistance and endothelial dysfunction reversion (49). In this regard, prior experiments showed that induction of hyperuricemia in T2D mice not only abrogate nitric oxide release and increased blood pressure, but also inhibited the expression vascular adhesion cell molecule in vitro (50). Furthermore, data from clinical studies support hyperuricemia as an independent risk factor not only for cardiovascular events, but also for rapid decline in kidney function of T2D individuals (51). Together, SGLT2i effect on SUC may hence contribute to the reduction of blood pressure and assist in overall cardiovascular risk reduction (52).
Weight loss
SGLT2i therapy promotes weight loss, which also helps reducing residual cardiovascular risk. Currently, eight out of ten individuals with T2D are affected by excess weight (53). Addressing these conditions not only improves blood pressure and glycemic control, but also provides significant benefits in terms of peripheral neuropathy symptoms, exercise tolerance and overall quality of life (54–56). Studies have shown that a decrease of 1 unit in body mass index leads to a 5 mmHg reduction in systolic blood pressure, and a 10% reduction in body weight results in a 1% decrease in glycated hemoglobin (55, 57). Previous research has also demonstrated that a majority of hypertension cases are attributed to excess adiposity, and that reducing adiposity may lead in some cases to the remission of hypertension (58). While the complex relationship between obesity and hypertension is beyond the scope of this article (59), we will focus on the evidence implicating SGLT2i-induced weight loss on blood pressure changes.
In a recent meta-analysis of 18 randomized controlled trials enrolling over 1,430 participants, SGLT2i therapy was associated with an average weight reduction of 2.73 kg (60). Participants who were concomitantly on a regular exercise regimen and had preserved kidney function were twice as likely to experience a weight loss greater than 3% of their baseline weight, and these reductions were independently correlated to systolic blood pressure drops (61–63). Further studies conducted by our group demonstrated that weight loss primarily stems from fat mass loss. This finding is supported by the evidence of an increase in the lean-to-total mass ratio in individuals with T2D treated with dapagliflozin compared to those treated with glibenclamide alongside metformine in the ADDENDA trial (64). Other trials have also shown that the majority of total body mass change consists of water and fat mass loss, with minimal impact on lean mass loss (65–68).
The effect of SGLT2i on glycosuria is involved in adiposity reduction. In this matter, Rajeev et al. found that dapagliflozin increase daily urinary glucose excretion by up to 40g, which in turn translates in an incremental daily energy expenditure of 300kcal (69). The expected weight loss for such caloric deficit is of 10kg per year, which is higher than the observed change in body weight. Such discrepancy is partially explained by the activation of compensatory mechanisms that increase endogenous synthesis of glucose and appetite. In fact, earlier studies showed that dapagliflozin glucose-lowering effect is partially attenuated by a concomitant increase in glucagon and glucose synthesis of 32% and 17%, respectively, that may attenuate caloric deficit attenuating weight loss (46).
Seminal hypothesis-generating experimental studies have also been conducted. For example, Xu et al. showed that empagliflozin reduces inflammation in adipose tissue, increases energy expenditure and heat production, and promotes the expression of uncoupled protein 1 in brown fat tissue (70). Moreover, empagliflozin enhanced the beta oxidation of fatty acids through the upregulation of MAPK pathways, reduced liver steatosis, and increased adiponectin levels in ApoE-/- mice (71). These effects may be abrogated by compensatory increased appetite. In fact, Devenny et al. (72) showed that dapagliflozin induces a 30% increased caloric intake in T2D mice with ad libidum access to food, thus resulting in a 3-fold lower body weight loss compared to animals with restricted access to diet (72). Beyond those mechanisms, the prevention of mitochondrial dysfunction and the modulation of adiponectin levels may be potential mechanisms underlying the impact of SGLT2i on adiposity, although those hypothesis warrants further verification (73, 74).
There has been a growing body of evidence from both clinical and experimental settings supporting the role of SGLT2i as a promising target for tackling overweight and obesity thus contributing to improved blood pressure control. So far, it has become clear that SGLT2i not only reduces body weight, but also shifts body composition toward a decrease in body fat percentage, promoting less atherogenic and hypertensive phenotypes, hence abrogating residual cardiovascular risk (65, 75).
Genetic variants
The influence of gene polymorphisms on SGLT2i has been scarcely explored. For example, UDP-glucuronosyltransferase 1-9 (UGT1A9) enzyme answers for dapagliflozin glucuronidation to its inactive metabolite, dapagliflozin-3-O-glucuronide (D3OG). Prior studies demonstrated that UGT1A9 gene polymorphisms modulate UGT1A9 enzyme activity, and this may have repercussions on dapagliflozin pharmacodynamics, thus affecting its influence on several pathways implicated in blood pressure control (76–78). Furthermore, Solini et al. (79) demonstrated that dapagliflozin prompts putative epigenetic modulation of miR30e-5p and miR199a-3p, that in turn abrogate renal resistive index and may therefore contribute to a favorable hemodynamic profile potentially contributing to cardiovascular prevention (79).
Other in vitro experiments also support a role for canagliflozin in modulating sirtuin 3 gene expression in proximal tubular epithelial cells promoting both renoprotective as a potential driver of blood pressure lowering (80). Likewise, Zhao et al. showed that epigenetic modulation of transient receptor potential channel 3 prevented high-salt diet-induced hypertension in rats, and this effect was at least partially explained by parallel activation of TRPC3/NCX1 pathway modulating intracellular calcium handling (81). From this data, it is possible that individuals with salt‐sensitive hypertension, which is tightly regulated by gene polymorphisms, such as HSD11B2 and CYP3A5, involved in salt-sensitive hypertension, may experience greater blood pressure changes compared to non-salt-sensitive (82).
Cardiorenal benefits
Prior trials provided solid evidence of cardiorenal benefits from SGLT2i treatment in high-risk T2D individuals. In the DECLARE TIMI 58 study dapagliflozin yielded a 17% (HR 0.87, 95%CI: 0.73 – 0.95; p= 0.005) relative risk reduction in the composite outcome of CV death or hospitalization for heart failure in 17,160 patients followed for 4.2 years, when compared to placebo (83). Likewise, in the CANVAS trial, canagliflozin reduced the relative risk of MACE by 14%, (HR 0.86; 95% CI: 0.75 – 0.97, p < 0.001), and that of renal outcomes including 40% reduction in glomerular filtration rate, renal replacement therapy and renal death, by over 40% (HR 0.60, 95% CI: 0.47-0.77). In line with these results, empagliflozin reduced the incidence of the composite outcome of CV death, myocardial infarction, and stroke by 14% (HR 0.86, 95% CI 0.74-0.99; p= 0.04), and that of hospitalization for heart failure by 35% (HR 0.65, 95% CI 0.50 – 0.85; p= 0.002) (84).
Renal benefits from SGLT2i in T2D subjects have been also explored in further trials. In this regard, the CREDENCE study was stopped early at 2.6 years after demonstrating a 30% lower relative risk of a doubling of the creatinine level or death from renal causes in the canagliflozin compared to the placebo group (85). Later findings unequivocally showed that SGLT2i display renoprotective effects regardless of T2D status reducing the relative risk of composite renal outcomes by over 39% (HR 0.61; 95% CI, 0.51 - 0.72; P<0.001) and 28% (HR 0.72; 95% CI 0.64 to 0.82; P<0.001) in the DAPA-CKD and EMPA-KIDNEY trial, respectively (86, 87). Current data thus support a class effect favoring both cardiac and renal events prevention hance playing an imperative role in attenuating the residual risk of T2D (88).
Concluding remarks
Residual cardiovascular risk in individuals with T2D remains an unresolved matter that needs to be adequately addressed. Hypertension affects a significant majority (eight in ten) of individuals with T2D, amplifying the risk of adverse outcomes. However, the utilization of SGLT2i therapy has shown remarkable potential in attenuating this risk and current evidence supports that a part of this benefit is mediated by the influence of SGLT2i on hypertension through mechanisms that were revised in this article. To effectively combat the adverse consequences of residual cardiovascular risk in individuals with T2D, it is imperative to address the knowledge gaps hereby highlighted and implement targeted interventions.
Author contributions
Idea & Conceptualization: JB, AC-S, TQ. Supervision: AC-S. Original Draft Preparation: JB. Critical review & Editing: JB, AC-S, WN, TQ, AS. All authors contributed to the article and approved the submitted version.
Funding
AS is supported by a Research Career Awards grant from the Brazilian National Research Council (CNPq) (grant number 301465/2017-7). AC-S is funded by the Michigan Institute for Clinical & Health Research (U074551), and the National Heart, Lung, and Blood Institute of the NIH (1F32HL162231-01A1).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Bommer C, Sagalova V, Heesemann E, Manne-Goehler J, Atun R, Bärnighausen T, et al. Global economic burden of diabetes in adults: projections from 2015 to 2030. Diabetes Care (2018) 41(5):963–70. doi: 10.2337/dc17-1962
2. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet (1998) 352(9131):837–53. doi: 10.1016/S0140-6736(98)07019-6
3. Dhindsa DS, Sandesara PB, Shapiro MD, Wong ND. The evolving understanding and approach to residual cardiovascular risk management. Front Cardiovasc Med (2020) 7:88. doi: 10.3389/fcvm.2020.00088
4. Lieb W, Enserro DM, Larson MG, Vasan RS. Residual cardiovascular risk in individuals on lipid-lowering treatment: quantifying absolute and relative risk in the community. Open Heart (2018) 5(1):e000722. doi: 10.1136/openhrt-2017-000722
5. Eckel RH, Bornfeldt KE, Goldberg IJ. Cardiovascular disease in diabetes, beyond glucose. Cell Metab (2021) 33(8):1519–45. doi: 10.1016/j.cmet.2021.07.001
6. Kluger AY, Tecson KM, Lee AY, Lerma EV, Rangaswami J, Lepor NE, et al. Class effects of SGLT2 inhibitors on cardiorenal outcomes. Cardiovasc Diabetol (2019) 18(1):99. doi: 10.1186/s12933-019-0903-4
7. Oparil S, Acelajado MC, Bakris GL, Berlowitz DR, Cífková R, Dominiczak AF, et al. Hypertension. Nat Rev Dis Primers (2018) 4:18014. doi: 10.1038/nrdp.2018.14
8. Charoensri S, Kritmetapak K, Tangpattanasiri T, Pongchaiyakul C. The impact of new-onset diabetes mellitus and hypertension on all-cause mortality in an apparently healthy population: A ten-year follow-up study. J Diabetes Res (2021) 2021:3964013. doi: 10.1155/2021/3964013
9. Tsimihodimos V, Gonzalez-Villalpando C, Meigs JB, Ferrannini E. Hypertension and diabetes mellitus: coprediction and time trajectories. Hypertension (2018) 71(3):422–8. doi: 10.1161/HYPERTENSIONAHA.117.10546
10. Sung KC, Lim S, Rosenson RS. Hyperinsulinemia and homeostasis model assessment of insulin resistance as predictors of hypertension: a 5-year follow-up study of Korean sample. Am J Hypertens (2011) 24(9):1041–5. doi: 10.1038/ajh.2011.89
11. Emdin CA, Rahimi K, Neal B, Callender T, Perkovic V, Patel A. Blood pressure lowering in type 2 diabetes: a systematic review and meta-analysis. JAMA (2015) 313(6):603–15. doi: 10.1001/jama.2014.18574
12. Huggett RJ, Scott EM, Gilbey SG, Stoker JB, Mackintosh AF, Mary DA. Impact of type 2 diabetes mellitus on sympathetic neural mechanisms in hypertension. Circulation (2003) 108(25):3097–101. doi: 10.1161/01.CIR.0000103123.66264.FE
13. Hu G, Sarti C, Jousilahti P, Peltonen M, Qiao Q, Antikainen R, et al. The impact of history of hypertension and type 2 diabetes at baseline on the incidence of stroke and stroke mortality. Stroke (2005) 36(12):2538–43. doi: 10.1161/01.STR.0000190894.30964.75
14. Hu G, Jousilahti P, Tuomilehto J. Joint effects of history of hypertension at baseline and type 2 diabetes at baseline and during follow-up on the risk of coronary heart disease. Eur Heart J (2007) 28(24):3059–66. doi: 10.1093/eurheartj/ehm501
15. Baker WL, Buckley LF, Kelly MS, Bucheit JD, Parod ED, Brown R, et al. Effects of sodium-glucose cotransporter 2 inhibitors on 24-hour ambulatory blood pressure: A systematic review and meta-analysis. J Am Heart Assoc (2017) 6(5). doi: 10.1161/JAHA.117.005686
16. Baker WL, Smyth LR, Riche DM, Bourret EM, Chamberlin KW, White WB. Effects of sodium-glucose co-transporter 2 inhibitors on blood pressure: a systematic review and meta-analysis. J Am Soc Hypertens (2014) 8(4):262–75 e9. doi: 10.1016/j.jash.2014.01.007
17. Chen G, McAlister FA, Walker RL, Hemmelgarn BR, Campbell NR. Cardiovascular outcomes in framingham participants with diabetes: the importance of blood pressure. Hypertension (2011) 57(5):891–7. doi: 10.1161/HYPERTENSIONAHA.110.162446
18. Adler AI, Stratton IM, Neil HA, Yudkin JS, Matthews DR, Cull CA, et al. Association of systolic blood pressure with macrovascular and microvascular complications of type 2 diabetes (UKPDS 36): prospective observational study. BMJ (2000) 321(7258):412–9. doi: 10.1136/bmj.321.7258.412
19. Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Back M, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J (2021) 42(34):3227–337. doi: 10.1093/eurheartj/ehab484
20. Ali MK, Bullard KM, Saaddine JB, Cowie CC, Imperatore G, Gregg EW. Achievement of goals in U.S. diabetes care, 1999-2010. N Engl J Med (2013) 368(17):1613–24. doi: 10.1056/NEJMsa1213829
21. Barreto J, Luchiari B, Wolf VLW, Bonilha I, Bovi TG, Assato BS, et al. Compliance with cardiovascular prevention guidelines in type 2 diabetes individuals in a middle-income region: A cross-sectional analysis. Diagnostics (Basel) (2022) 12(4). doi: 10.3390/diagnostics12040814
22. Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, Delgado V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J (2020) 41(2):255–323. doi: 10.1093/eurheartj/ehz486
23. Lambers Heerspink HJ, de Zeeuw D, Wie L, Leslie B, List J. Dapagliflozin a glucose-regulating drug with diuretic properties in subjects with type 2 diabetes. Diabetes Obes Metab (2013) 15(9):853–62. doi: 10.1111/dom.12127
24. Scholtes RA, Muskiet MHA, van Baar MJB, Wie L, Leslie B, List J. The adaptive renal response for volume homeostasis during 2 weeks of dapagliflozin treatment in people with type 2 diabetes and preserved renal function on a sodium-controlled diet. Kidney Int Rep (2022) 7(5):1084–92. doi: 10.1016/j.ekir.2022.02.023
25. Masuda T, Muto S, Fukuda K, Watanabe M, Ohara K, Koepsell H, et al. Osmotic diuresis by SGLT2 inhibition stimulates vasopressin-induced water reabsorption to maintain body fluid volume. Physiol Rep (2020) 8(2):e14360. doi: 10.14814/phy2.14360
26. Scholtes RA, Muskiet MHA, van Baar MJB, Hesp AC, Greasley PJ, Karlsson C, et al. Natriuretic effect of two weeks of dapagliflozin treatment in patients with type 2 diabetes and preserved kidney function during standardized sodium intake: results of the DAPASALT trial. Diabetes Care (2021) 44(2):440–7. doi: 10.2337/dc20-2604
27. Grassi G, Mark A, Esler M. The sympathetic nervous system alterations in human hypertension. Circ Res (2015) 116(6):976–90. doi: 10.1161/CIRCRESAHA.116.303604
28. Qiu S, Cai X, Sun Z, Li L, Zuegel M, Steinacker JM, et al. Heart rate recovery and risk of cardiovascular events and all-cause mortality: A meta-analysis of prospective cohort studies. J Am Heart Assoc (2017) 6(5). doi: 10.1161/JAHA.117.005505
29. Burns J, Sivananthan MU, Ball SG, Mackintosh AF, Mary DA, Greenwood JP. Relationship between central sympathetic drive and magnetic resonance imaging-determined left ventricular mass in essential hypertension. Circulation (2007) 115(15):1999–2005. doi: 10.1161/CIRCULATIONAHA.106.668863
30. Silva LRB, Gentil P, Seguro CS, de Oliveira GT, Silva MS, Zamuner AR, et al. High fasting glycemia predicts impairment of cardiac autonomic control in adults with type 2 diabetes: A case-control study. Front Endocrinol (Lausanne) (2021) 12:760292. doi: 10.3389/fendo.2021.760292
31. Strand AH, Gudmundsdottir H, Os I, Smith G, Westheim AS, Bjornerheim R, et al. Arterial plasma noradrenaline predicts left ventricular mass independently of blood pressure and body build in men who develop hypertension over 20 years. J Hypertens (2006) 24(5):905–13. doi: 10.1097/01.hjh.0000222761.07477.7b
32. Hamaoka T, Murai H, Hirai T, Sugimoto H, Mukai Y, Inoue O, et al. Different responses of muscle sympathetic nerve activity to dapagliflozin between patients with type 2 diabetes with and without heart failure. J Am Heart Assoc (2021) 10(22):e022637. doi: 10.1161/JAHA.121.022637
33. Balcioglu AS, Celik E, Sahin M, Gocer K, Aksu E, Aykan AC. Dapagliflozin improves cardiac autonomic function measures in type 2 diabetic patients with cardiac autonomic neuropathy. Anatol J Cardiol (2022) 26(11):832–40. doi: 10.5152/AnatolJCardiol.2022.1934
34. Sardu C, Massimo Massetti M, Rambaldi P, Gatta G, Cappabianca S, Sasso FC, et al. SGLT2-inhibitors reduce the cardiac autonomic neuropathy dysfunction and vaso-vagal syncope recurrence in patients with type 2 diabetes mellitus: the SCAN study. Metabolism (2022) 137:155243. doi: 10.1016/j.metabol.2022.155243
35. Versari D, Daghini E, Virdis A, Ghiadoni L, Taddei S. Endothelial dysfunction as a target for prevention of cardiovascular disease. Diabetes Care (2009) 32 Suppl 2(Suppl 2):S314–21. doi: 10.2337/dc09-S330
36. Cusi K, Maezono K, Osman A, Pendergrass M, Patti ME, Pratipanawatr T, et al. Insulin resistance differentially affects the PI 3-kinase- and MAP kinase-mediated signaling in human muscle. J Clin Invest (2000) 105(3):311–20. doi: 10.1172/JCI7535
37. Ando K, Fujita T. Pathophysiology of salt sensitivity hypertension. Ann Med (2012) 44 Suppl 1:S119–26. doi: 10.3109/07853890.2012.671538
38. Balafa O, Kalaitzidis RG. Salt sensitivity and hypertension. J Hum Hypertens (2021) 35(3):184–92. doi: 10.1038/s41371-020-00407-1
39. Yatabe MS, Yatabe J, Yoneda M, Watanabe T, Otsuki M, Felder RA, et al. Salt sensitivity is associated with insulin resistance, sympathetic overactivity, and decreased suppression of circulating renin activity in lean patients with essential hypertension. Am J Clin Nutr (2010) 92(1):77–82. doi: 10.3945/ajcn.2009.29028
40. Murabayashi M, Daimon M, Murakami H, Fujita T, Sato E, Tanabe J, et al. Association between higher urinary normetanephrine and insulin resistance in a Japanese population. PloS One (2020) 15(2):e0228787. doi: 10.1371/journal.pone.0228787
41. Xiao L, Nie X, Cheng Y, Wang N. Sodium-glucose cotransporter-2 inhibitors in vascular biology: cellular and molecular mechanisms. Cardiovasc Drugs Ther (2021) 35(6):1253–67. doi: 10.1007/s10557-021-07216-9
42. Sposito AC, Breder I, Soares AAS, Kimura-Medorima ST, Munhoz DB, Cintra RMR, et al. Dapagliflozin effect on endothelial dysfunction in diabetic patients with atherosclerotic disease: a randomized active-controlled trial. Cardiovasc Diabetol (2021) 20(1):74. doi: 10.1186/s12933-021-01264-z
43. Gaspari T, Spizzo I, Liu H, Hu Y, Simpson RW, Widdop RE, et al. Dapagliflozin attenuates human vascular endothelial cell activation and induces vasorelaxation: A potential mechanism for inhibition of atherogenesis. Diabetes Vasc Dis Res (2018) 15(1):64–73. doi: 10.1177/1479164117733626
44. Alshnbari AS, Millar SA, O'Sullivan SE, Idris I. Effect of sodium-glucose cotransporter-2 inhibitors on endothelial function: A systematic review of preclinical studies. Diabetes Ther (2020) 11(9):1947–63. doi: 10.1007/s13300-020-00885-z
45. Soares RN, Ramirez-Perez FI, Cabral-Amador FJ, Morales-Quinones M, Foote CA, Ghiarone T, et al. SGLT2 inhibition attenuates arterial dysfunction and decreases vascular F-actin content and expression of proteins associated with oxidative stress in aged mice. Geroscience (2022) 44(3):1657–75. doi: 10.1007/s11357-022-00563-x
46. Merovci A, Solis-Herrera C, Daniele G, Eldor R, Fiorentino TV, Tripathy D, et al. Dapagliflozin improves muscle insulin sensitivity but enhances endogenous glucose production. J Clin Invest (2014) 124(2):509–14. doi: 10.1172/JCI70704
47. Ramirez-Rodriguez AM, Gonzalez-Ortiz M, Martinez-Abundis E. Effect of dapagliflozin on insulin secretion and insulin sensitivity in patients with prediabetes. Exp Clin Endocrinol Diabetes (2020) 128(8):506–11. doi: 10.1055/a-0664-7583
48. Shyr ZA, Yan Z, Ustione A, Egan EM, Remedi MS. SGLT2 inhibitors therapy protects glucotoxicity-induced beta-cell failure in a mouse model of human KATP-induced diabetes through mitigation of oxidative and ER stress. PloS One (2022) 17(2):e0258054. doi: 10.1371/journal.pone.0258054
49. Akbari A, Rafiee M, Sathyapalan T, Sahebkar A. Impacts of sodium/glucose cotransporter-2 inhibitors on circulating uric acid concentrations: A systematic review and meta-analysis. J Diabetes Res (2022) 2022:7520632. doi: 10.1155/2022/7520632
50. Khosla UM, Zharikov S, Finch JL, Nakagawa T, Roncal C, Mu W, et al. Hyperuricemia induces endothelial dysfunction. Kidney Int (2005) 67(5):1739–42. doi: 10.1111/j.1523-1755.2005.00273.x
51. Bartakova V, Kuricova K, Pacal L, Nova Z, Dvorakova V, Svrckova M, et al. Hyperuricemia contributes to the faster progression of diabetic kidney disease in type 2 diabetes mellitus. J Diabetes Complications (2016) 30(7):1300–7. doi: 10.1016/j.jdiacomp.2016.06.002
52. Spatola L, Ferraro PM, Gambaro G, Badalamenti S, Dauriz M. Metabolic syndrome and uric acid nephrolithiasis: insulin resistance in focus. Metabolism (2018) 83:225–33. doi: 10.1016/j.metabol.2018.02.008
53. Chong B, Jayabaskaran J, Kong G, Chan YH, Chin YH, Goh R, et al. Trends and predictions of malnutrition and obesity in 204 countries and territories: an analysis of the Global Burden of Disease Study 2019. EClinicalMedicine (2023) 57:101850. doi: 10.1016/j.eclinm.2023.101850
54. Bluher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol (2019) 15(5):288–98. doi: 10.1038/s41574-019-0176-8
55. Bramante CT, Lee CJ, Gudzune KA. Treatment of obesity in patients with diabetes. Diabetes Spectr (2017) 30(4):237–43. doi: 10.2337/ds17-0030
56. Gibbs BB, Brancati FL, Chen H, Coday M, Jakicic JM, Lewis CE, et al. Effect of improved fitness beyond weight loss on cardiovascular risk factors in individuals with type 2 diabetes in the Look AHEAD study. Eur J Prev Cardiol (2014) 21(5):608–17. doi: 10.1177/2047487312462823
57. Gummesson A, Nyman E, Knutsson M, Karpefors M. Effect of weight reduction on glycated haemoglobin in weight loss trials in patients with type 2 diabetes. Diabetes Obes Metab (2017) 19(9):1295–305. doi: 10.1111/dom.12971
58. Guimaraes JMN, Griep RH, Fonseca MJM, Duncan BB, Schmidt MI, Mill JG, et al. Four-year adiposity change and remission of hypertension: an observational evaluation from the Longitudinal Study of Adult Health (ELSA-Brasil). J Hum Hypertens (2020) 34(1):68–75. doi: 10.1038/s41371-019-0289-5
59. Hall JE, do Carmo JM, da Silva AA, Wang Z, Hall ME. Obesity-induced hypertension: interaction of neurohumoral and renal mechanisms. Circ Res (2015) 116(6):991–1006. doi: 10.1161/CIRCRESAHA.116.305697
60. Pan R, Zhang Y, Wang R, Xu Y, Ji H, Zhao Y. Effect of SGLT-2 inhibitors on body composition in patients with type 2 diabetes mellitus: A meta-analysis of randomized controlled trials. PloS One (2022) 17(12):e0279889. doi: 10.1371/journal.pone.0279889
61. Cai X, Yang W, Gao X, Chen Y, Zhou L, Zhang S, et al. The association between the dosage of SGLT2 inhibitor and weight reduction in type 2 diabetes patients: A meta-analysis. Obes (Silver Spring) (2018) 26(1):70–80. doi: 10.1002/oby.22066
62. Huh Y, Kim YS. Predictors for successful weight reduction during treatment with Dapagliflozin among patients with type 2 diabetes mellitus in primary care. BMC Prim Care (2022) 23(1):134. doi: 10.1186/s12875-022-01748-1
63. Hu M, Cai X, Yang W, Zhang S, Nie L, Ji L. Effect of hemoglobin A1c reduction or weight reduction on blood pressure in glucagon-like peptide-1 receptor agonist and sodium-glucose cotransporter-2 inhibitor treatment in type 2 diabetes mellitus: A meta-analysis. J Am Heart Assoc (2020) 9(7):e015323. doi: 10.1161/JAHA.119.015323
64. Wolf VLW, Breder I, de Carvalho LSF, Soares AAS, Cintra RM, Barreto J, et al. Dapagliflozin increases the lean-to total mass ratio in type 2 diabetes mellitus. Nutr Diabetes (2021) 11(1):17. doi: 10.1038/s41387-021-00160-5
65. Zeng YH, Liu SC, Lee CC, Sun FJ, Liu JJ. Effect of empagliflozin versus linagliptin on body composition in Asian patients with type 2 diabetes treated with premixed insulin. Sci Rep (2022) 12(1):17065. doi: 10.1038/s41598-022-21486-9
66. Strojek K, Yoon KH, Hruba V, Sugg J, Langkilde AM, Parikh S. Dapagliflozin added to glimepiride in patients with type 2 diabetes mellitus sustains glycemic control and weight loss over 48 weeks: a randomized, double-blind, parallel-group, placebo-controlled trial. Diabetes Ther (2014) 5(1):267–83. doi: 10.1007/s13300-014-0072-0
67. Kovacs CS, Seshiah V, Swallow R, Sugg J, Langkilde AM, Parikh S, et al. Empagliflozin improves glycaemic and weight control as add-on therapy to pioglitazone or pioglitazone plus metformin in patients with type 2 diabetes: a 24-week, randomized, placebo-controlled trial. Diabetes Obes Metab (2014) 16(2):147–58. doi: 10.1111/dom.12188
68. Bolinder J, Ljunggren O, Johansson L, Jones R, Rattunde H, Woerle HJ, et al. Dapagliflozin maintains glycaemic control while reducing weight and body fat mass over 2 years in patients with type 2 diabetes mellitus inadequately controlled on metformin. Diabetes Obes Metab (2014) 16(2):159–69. doi: 10.1111/dom.12189
69. Ricci F, Fedorowski A, Radico F, Wilding J, Langkilde AM, Sjostrom CD, et al. Cardiovascular morbidity and mortality related to orthostatic hypotension: a meta-analysis of prospective observational studies. Eur Heart J (2015) 36(25):1609–17. doi: 10.1093/eurheartj/ehv093
70. Xu L, Nagata N, Nagashimada M, Zhuge F, Ni Y, Chen G, et al. SGLT2 inhibition by empagliflozin promotes fat utilization and browning and attenuates inflammation and insulin resistance by polarizing M2 macrophages in diet-induced obese mice. EBioMedicine (2017) 20:137–49. doi: 10.1016/j.ebiom.2017.05.028
71. Han JH, Oh TJ, Lee G, Maeng HJ, Lee DH, Kim KM, et al. The beneficial effects of empagliflozin, an SGLT2 inhibitor, on atherosclerosis in ApoE (-/-) mice fed a western diet. Diabetologia (2017) 60(2):364–76. doi: 10.1007/s00125-016-4158-2
72. Devenny JJ, Godonis HE, Harvey SJ, Rooney S, Cullen MJ, Pelleymounter MA. Weight loss induced by chronic dapagliflozin treatment is attenuated by compensatory hyperphagia in diet-induced obese (DIO) rats. Obes (Silver Spring) (2012) 20(8):1645–52. doi: 10.1038/oby.2012.59
73. Kralova E, Marusakova M, Hadova K, Krenek P, Klimas J. Dapagliflozin elevates plasma high-density lipoprotein levels and influences visceral fat gene expression in streptozotocin-induced diabetes mellitus. J Pharm Pharmacol (2021) 73(6):778–84. doi: 10.1093/jpp/rgab005
74. Belosludtsev KN, Starinets VS, Belosludtsev MN, Mikheeva IB, Dubinin MV, Belosludtseva NV. Chronic treatment with dapagliflozin protects against mitochondrial dysfunction in the liver of C57BL/6NCrl mice with high-fat diet/streptozotocin-induced diabetes mellitus. Mitochondrion (2021) 59:246–54. doi: 10.1016/j.mito.2021.06.008
75. Li R, Tian Z, Wang Y, Rooney S, Cullen MJ, Pelleymounter MA, et al. The association of body fat percentage with hypertension in a Chinese rural population: the Henan rural cohort study. Front Public Health (2020) 8:70. doi: 10.3389/fpubh.2020.00070
76. Naagaard MD, Chang R, Nagard M, Tang W, Boulton DW. Common UGT1A9 polymorphisms do not have a clinically meaningful impact on the apparent oral clearance of dapagliflozin in type 2 diabetes mellitus. Br J Clin Pharmacol (2022) 88(4):1942–6. doi: 10.1111/bcp.15117
77. DeFronzo RA, Hompesch M, Kasichayanula S, Liu X, Hong Y, Pfister M, et al. Characterization of renal glucose reabsorption in response to dapagliflozin in healthy subjects and subjects with type 2 diabetes. Diabetes Care (2013) 36(10):3169–76. doi: 10.2337/dc13-0387
78. Kasichayanula S, Chang M, Hasegawa M, Liu X, Yamahira N, LaCreta FP, et al. Pharmacokinetics and pharmacodynamics of dapagliflozin, a novel selective inhibitor of sodium-glucose co-transporter type 2, in Japanese subjects without and with type 2 diabetes mellitus. Diabetes Obes Metab (2011) 13(4):357–65. doi: 10.1111/j.1463-1326.2011.01359.x
79. Solini A, Seghieri M, Giannini L, Biancalana E, Parolini F, Rossi C, et al. The effects of dapagliflozin on systemic and renal vascular function display an epigenetic signature. J Clin Endocrinol Metab (2019) 104(10):4253–63. doi: 10.1210/jc.2019-00706
80. Wang Z, Zhai J, Zhang T, He L, Ma S, Zuo Q, et al. Canagliflozin ameliorates epithelial-mesenchymal transition in high-salt diet-induced hypertensive renal injury through restoration of sirtuin 3 expression and the reduction of oxidative stress. Biochem Biophys Res Commun (2023) 653:53–61. doi: 10.1016/j.bbrc.2023.01.084
81. Zhao Y, Li L, Lu Z, Hu Y, Zhang H, Sun F, et al. Sodium-glucose cotransporter 2 inhibitor canagliflozin antagonizes salt-sensitive hypertension through modifying transient receptor potential channels 3 mediated vascular calcium handling. J Am Heart Assoc (2022) 11(15):e025328. doi: 10.1161/JAHA.121.025328
82. Sanada H, Jones JE, Jose PA. Genetics of salt-sensitive hypertension. Curr Hypertens Rep (2011) 13(1):55–66. doi: 10.1007/s11906-010-0167-6
83. Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med (2019) 380(4):347–57. doi: 10.1056/NEJMoa1812389
84. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med (2015) 373(22):2117–28. doi: 10.1056/NEJMoa1504720
85. Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med (2019) 380(24):2295–306. doi: 10.1056/NEJMoa1811744
86. The E-KCG, Herrington WG, Staplin N, Wanner C, Green JB, Hauske SJ, et al. Empagliflozin in patients with chronic kidney disease. N Engl J Med (2023) 388(2):117–27. doi: 10.1056/NEJMoa2204233
87. Heerspink HJL, Stefánsson BV, Correa-Rotter R, Chertow GM, Greene T, Hou FF, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med (2020) 383(15):1436–46. doi: 10.1056/NEJMoa2024816
88. Nuffield Department of Population Health Renal Studies G, Consortium SiM-AC-RT. Impact of diabetes on the effects of sodium glucose co-transporter-2 inhibitors on kidney outcomes: collaborative meta-analysis of large placebo-controlled trials. Lancet (2022) 400(10365):1788–801. doi: 10.1016/S0140-6736(22)02074-8
Keywords: dapagliflozin, empagliflozin, cardiovascular risk, SGLT2i, residual risk
Citation: Barreto J, Campos-Staffico AM, Nadruz W, Quinaglia T and Sposito AC (2023) The role of SGLT2i in attenuating residual cardiovascular risk through blood pressure-lowering: mechanistic insights and perspectives. Front. Clin. Diabetes Healthc. 4:1243530. doi: 10.3389/fcdhc.2023.1243530
Received: 20 June 2023; Accepted: 11 September 2023;
Published: 26 September 2023.
Edited by:
Marco Dauriz, Bolzano Central Hospital, ItalyReviewed by:
Yu Tao, University of North Texas Health Science Center, United StatesCopyright © 2023 Barreto, Campos-Staffico, Nadruz, Quinaglia and Sposito. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joaquim Barreto, am9hcXVpbWJhcnJldG9hbnR1bmVzQGdtYWlsLmNvbQ==