 Hana Mucević1,2
Hana Mucević1,2 Jennifer E. McWhirter1†Jillian Macleod3
Jennifer E. McWhirter1†Jillian Macleod3 Hisba Shereefdeen1,2
Hisba Shereefdeen1,2 Melissa MacKay1Leslie Cheng2Melissa Phypers2
Melissa MacKay1Leslie Cheng2Melissa Phypers2 Lauren E. Grant1*†
Lauren E. Grant1*†- 1Department of Population Medicine, University of Guelph, Guelph, ON, Canada
- 2Outbreak Management Division, Centre for Foodborne, Environmental and Zoonotic Infectious Diseases, Public Health Agency of Canada, Guelph, ON, Canada
- 3College of Biological Sciences, University of Guelph, Guelph, ON, Canada
Introduction: Public risk communication is intended to inform and protect the health of individuals during enteric illness outbreaks. However, there is limited practical research that assesses the effectiveness of communication during outbreaks. The aim of this study was to identify best practices in public risk communication during enteric illness outbreak investigations.
Methods: A scoping review of five bibliographic databases and gray literature was conducted to identify studies that described public communication during foodborne, waterborne, or enteric zoonotic outbreaks. Eligibility criteria were applied to citations and then full text by two independent reviewers. Data from included studies was extracted and synthesized into categories. Evidence adequacy and agreement were assessed and used to assign an overall level of confidence for each best practice.
Results: In total, 25 studies were included with most studies occurring in North America and Western Europe. Seven principles, nine practices, and eight platforms were identified. Of these, six principles, four practices, and two platforms received a high confidence rating in their overall effectiveness.
Discussion: Effective risk communication during enteric illness outbreak investigations requires public health authorities to identify, characterize, tailor information to, and meaningfully engage with their target audiences, build relationships and collaborate with media outlets, and maintain and increase credibility to deliver trustworthy risk communication messages.
1 Introduction
Enteric illness is caused by exposure to contaminated food or water, contact with animals, or via person-to-person contact that commonly result in self-limiting gastrointestinal symptoms, such as abdominal pain, nausea, and diarrhea (Public Health Agency of Canada, 2017). However, enteric illness can also cause more severe outcomes, particularly in high-risk groups such as children and older adults, that require medical attention, and in rare instances, can be fatal (Public Health Agency of Canada, 2017). Chronic sequelae, including reactive arthritis, irritable bowel syndrome, ankylosing spondylitis, and others, can also develop following enteric infection (Galanis et al., 2023; Gohari et al., 2022). Enteric illnesses pose a significant annual burden on the health of Canadians. The most recent national burden of illness estimate suggests that 4 million Canadians become sick due to an enteric illness each year, resulting in over 11,000 hospitalizations and 230 deaths (Thomas et al., 2013; Thomas et al., 2014). In Ontario alone, estimated healthcare utilization for enteric illness includes 137,000 primary care visits, 40,000 emergency department visits, and 6,200 hospitalizations based on available evidence (Drudge et al., 2019; Greco et al., 2020). Contamination can occur at different points along the agri-food continuum, including production, processing, transportation, retail, preparation, and consumption. An enteric illness outbreak occurs when multiple people are exposed to and become ill from the same enteric pathogen. This contrasts with isolated, sporadic events arising from lack of personal preventive behaviors (e.g., poor hand hygiene or cross-contamination while preparing a meal consumed by an individual or household).
Management of enteric illness outbreaks requires rapid, coordinated efforts and significant resources. Early, rapid interventions limiting those exposed to a common, contaminated source during an enteric illness outbreak can be highly effective and are integral to controlling disease spread. During an outbreak investigation, clear, frequent information exchange is required between government, industry, and public stakeholders. Effective risk communication informs the public of key outbreak characteristics, such as suspected food sources, and enables the public to engage in recommended, protective behaviors (World Health Organization, 2017; Infanti et al., 2013; Tumpey et al., 2019). Aspects of risk communication that influence public behavior include the source, timing, message content, and communication channels used (Cairns et al., 2013; Andersen and Spitzberg, 2010; Janoske et al., 2012; Vilella-Vila and Costa-Font, 2008). Although risk communication is an integral part of responding to enteric illness outbreaks, there is limited evidence on how to effectively communicate risk to the public during enteric illness outbreaks, specifically, where multiple stakeholders across sectors and at all jurisdictional levels are involved and the potential impact of a slow response is significant. This evidence is needed to inform best practices and identify critical knowledge gaps related to effective communication in these rapidly evolving situations (Frisby et al., 2014).
To address a lack of collated evidence on this topic, we conducted a scoping review to identify and synthesize the extent and nature of the literature on risk communication best practices during enteric illness outbreak investigations (Arksey and O’Malley, 2005). The objectives of this review are to: (1) Identify and synthesize relevant literature for public risk communication best practices during enteric illness outbreaks, and (2) Generate a set of recommendations for best practices for risk communication during enteric illness outbreaks.
2 Methods
2.1 Overview
We conducted a scoping review in accordance with the Joanna Briggs Institute Manual for Evidence Synthesis (Peters et al., 2020) and PRISMA for Scoping Reviews (PRISMA-ScR) guidelines (Tricco et al., 2018) to identify and characterize effective risk communication practices (intervention) during enteric illness outbreaks affecting general populations (population) to ultimately reduce the incidence of outbreak-associated enteric illnesses (outcome). There is no relevant comparator group for this particular synthesis.
2.2 Scoping review protocol
A preliminary search of PROSPERO, PubMed, and Google Scholar was conducted and no published or in-progress systematic or scoping reviews on the topic were identified. The scoping review protocol was developed according to the Joanna Briggs Institute Manual for Evidence Synthesis (Peters et al., 2020) and refined by an interdisciplinary research team with expertise in enteric illness outbreak management, health communication, and review methodology (Supplementary File S1).
2.3 Eligibility criteria
Literature was included if it was primary academic or gray literature describing public risk communication practices during human enteric illness outbreak investigations related to foodborne, waterborne, or enteric zoonotic illnesses and written in English or French. No study design, date, or geographic restrictions were employed. Articles with no full text availability were excluded.
2.4 Information sources
Five bibliographic databases with topics related to risk communication, enteric illnesses, and human infectious disease outbreaks were searched: Ovid MEDLINE, CAB Direct, Web of Science, PsycInfo, and Communication and Mass Media Complete. The search strategy was first developed for Ovid MEDLINE through consultation with a Research Librarian and research team and was then adapted for each database as appropriate (Supplementary Table S1). The initial search of bibliographic databases was carried out on March 13, 2023. A simplified gray literature search strategy was then iteratively developed. Gray literature comprises materials produced outside traditional publishing channels, such as documents written by governments and industry groups (Paez, 2017). Two information sources were queried: Google Scholar and ProQuest Theses and Dissertations (Supplementary Table S2). Following established guidelines (Canadian Agency for Drugs and Technology in Health, 2018), the first 50 results of each search were reviewed to identify relevant citations.
2.5 Selection of sources of evidence
Citations were uploaded into Covidence, an online review management software, and duplicates were removed using the deduplication tool (Covidence, n.d.). Twenty-five citations were initially screened using their titles and abstracts to test agreement between the two reviewers (HM, JM). Once 95% agreement was obtained, the remaining titles and abstracts were independently screened against the eligibility criteria. Next, the full text of selected citations was assessed by the two reviewers using the same eligibility criteria. Any disagreements were resolved through discussion.
2.6 Data extraction
A data extraction tool was initially developed by one reviewer (HM) and was then assessed and modified by the research team prior to full data extraction. Data items included study characteristics (title, authors, year of publication, location, aim), study population, sample size, study design, methods, type of outbreak, type of pathogen, communication framework or model, communication platforms used, communication practices identified, evaluation methods and results, study limitations, and future directions or recommendations. Data was extracted independently by two researchers (HM, JM) in Covidence, and any discrepancies were then identified and resolved through discussion. Data was exported into Excel (Microsoft Corporation, 2018) for synthesis.
2.7 Data synthesis
Data was synthesized according to three categories: communication principles, communication practices, and communication platforms. These categories emerged from the included studies, aligned with the objectives of the review, and validated by enteric illness epidemiologists on the research team. Communication principles are overarching strategies used to potentially broaden message reach. Communication practices describe the types of information that should be included in risk messages to the public. Communication platforms are mechanisms by which risk communication messages can be delivered. The weight of evidence for each category was evaluated according to evidence adequacy and evidence agreement, which were derived from relevant evidence assessment frameworks applicable to qualitative evidence and the review scope. Specifically, the Intergovernmental Panel for Climate Change’s uncertainties guidelines (Mastrandrea et al., 2010) and the Confidence in Evidence from Reviews of Qualitative Research Assessment (Noyes et al., 2018) were used. Evidence adequacy relates to the type and generalizability of studies, where study type refers to the way evidence is collected and evaluated (University of Wisconsin Population Health Institute, 2022) and generalizability refers to how well the evidence represents the finding of interest (Noyes et al., 2018). In addition, the weight of evidence was assessed via the number of relevant studies (Mastrandrea et al., 2010; Glenton et al., 2018). Scores of high, moderate, or low were systematically assigned to type, generalizability, and weight of evidence (Supplementary Table S3). For weight of evidence, numerical cut-offs were chosen based on the data. A final evidence adequacy score was determined by directly summing the scores for type, generalizability, and weight of evidence.
Evidence agreement refers to the level of consensus for effectiveness of each principle, practice, or platform for risk communication during enteric illness outbreaks (Mastrandrea et al., 2010). For each principle, practice, or platform, the proportion of studies with concordant evidence was determined and a score of high (75–100%), moderate (25–74%), or low (0–24%) was assigned.
Overall confidence in the effectiveness of each principle, practice, or platform was assigned a score of high, moderate, or low using a scoring matrix of evidence adequacy and evidence agreement (Supplementary Table S4). In general, the higher the evidence adequacy and agreement, the higher confidence there is in the principle, practice, or platform’s ability to effectively communicate risk during enteric illness outbreaks. No confidence was assigned when evidence adequacy and/or agreement could not be assessed (Mastrandrea et al., 2010).
3 Results
3.1 Selection of sources of evidence
A total of 8,365 citations were initially identified (8,342 citations from bibliographic databases and 23 citations from gray literature). After deduplication, 8,164 citations were screened by title and abstract and 95 citations were screened via full text for eligibility. After screening, 25 studies were included (Figure 1).
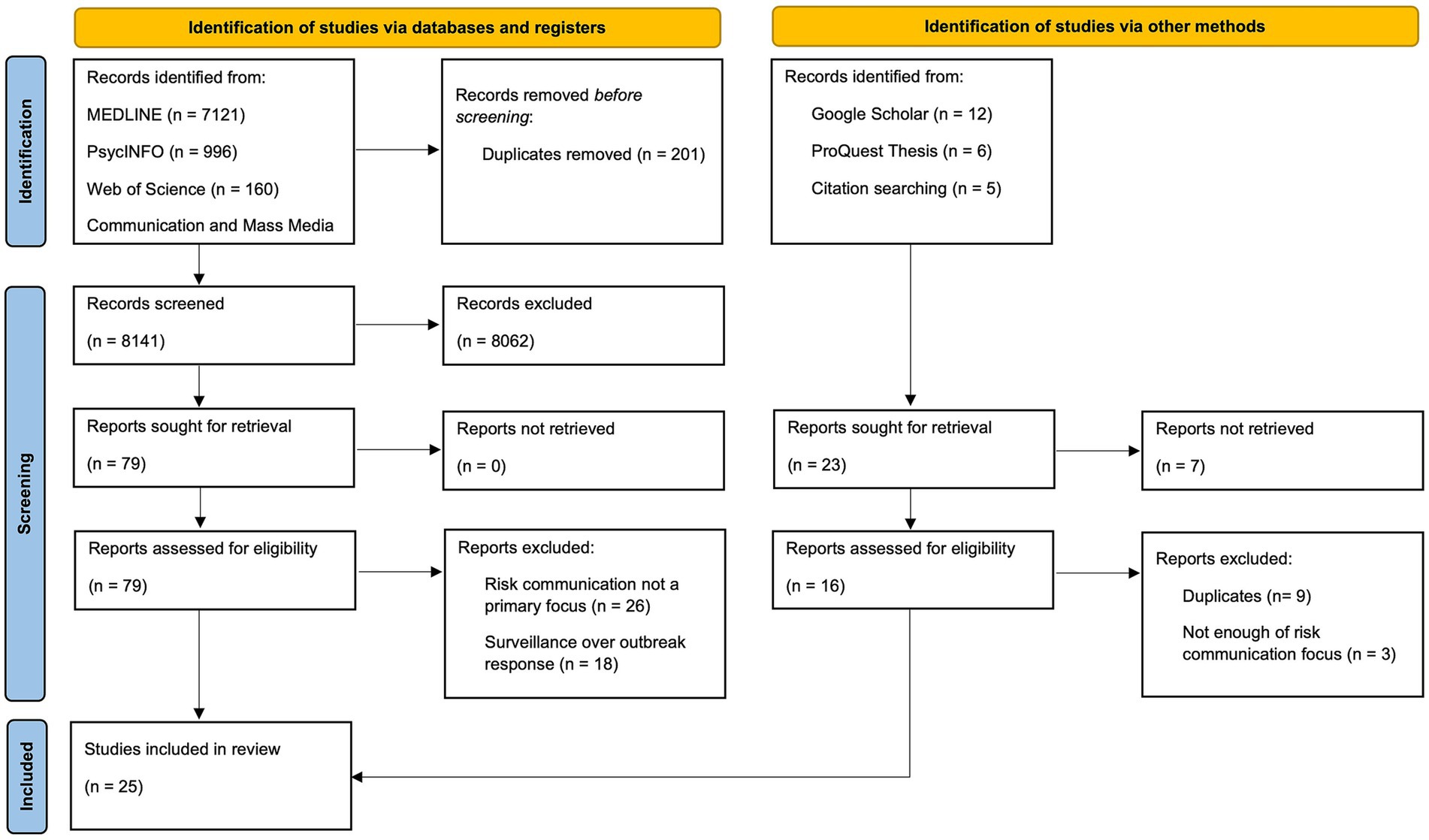
Figure 1. PRISMA flow diagram of identification and assessment of studies from academic databases and gray literature for inclusion in the scoping review.
3.2 Sources of evidence
Study locations were primarily in North America and Western Europe. Most studies were conducted in a single country (n = 22). Almost half of the studies occurred in the United States (n = 14), followed by Germany (n = 5), Canada (n = 2), and the Netherlands (n = 2). Other study locations included Ethiopia, South Africa, Denmark, Sweden, Norway, and Belgium. The most common study design was qualitative (n = 12), followed by mixed methods (n = 6), quantitative (n = 5), and opinion papers (n = 2). Over half of the studies used a communication framework or model to guide their risk communication and evaluation (n = 16). Most studies involved foodborne illness outbreaks (n = 23), although the causative pathogen varied. Outbreaks caused by Escherichia coli (n = 8) and Salmonella (n = 7) were most common followed by Listeria (n = 4), multi-pathogen outbreaks (n = 2), and outbreaks with an unknown etiologic agent (n = 2).
3.3 Narrative synthesis
Seven principles, nine practices, and eight platforms were identified (Tables 1–3). The overall evidence evaluation identified six principles, four practices, and two platforms with a high confidence rating in their overall effectiveness (Table 4). The six high-confidence principles were: (1) maintaining rapid and ongoing risk communication, (2) using consistent messaging, (3) building trust with the public, (4) addressing the social/cultural context of the outbreak, (5) collaborating within and across organizational levels, and (6) establishing and maintaining two-way communication with the public. The four high-confidence practices were: (1) provide preventive measures and other behavioral recommendations to minimize disease risk, (2) communicate the pathogen source, including implicated food item(s) and case location(s), (3) express empathy, and (4) state what is unknown about the outbreak. The two high-confidence platforms were newspaper (print or online) and television. Social media and websites received a moderate rating of confidence.
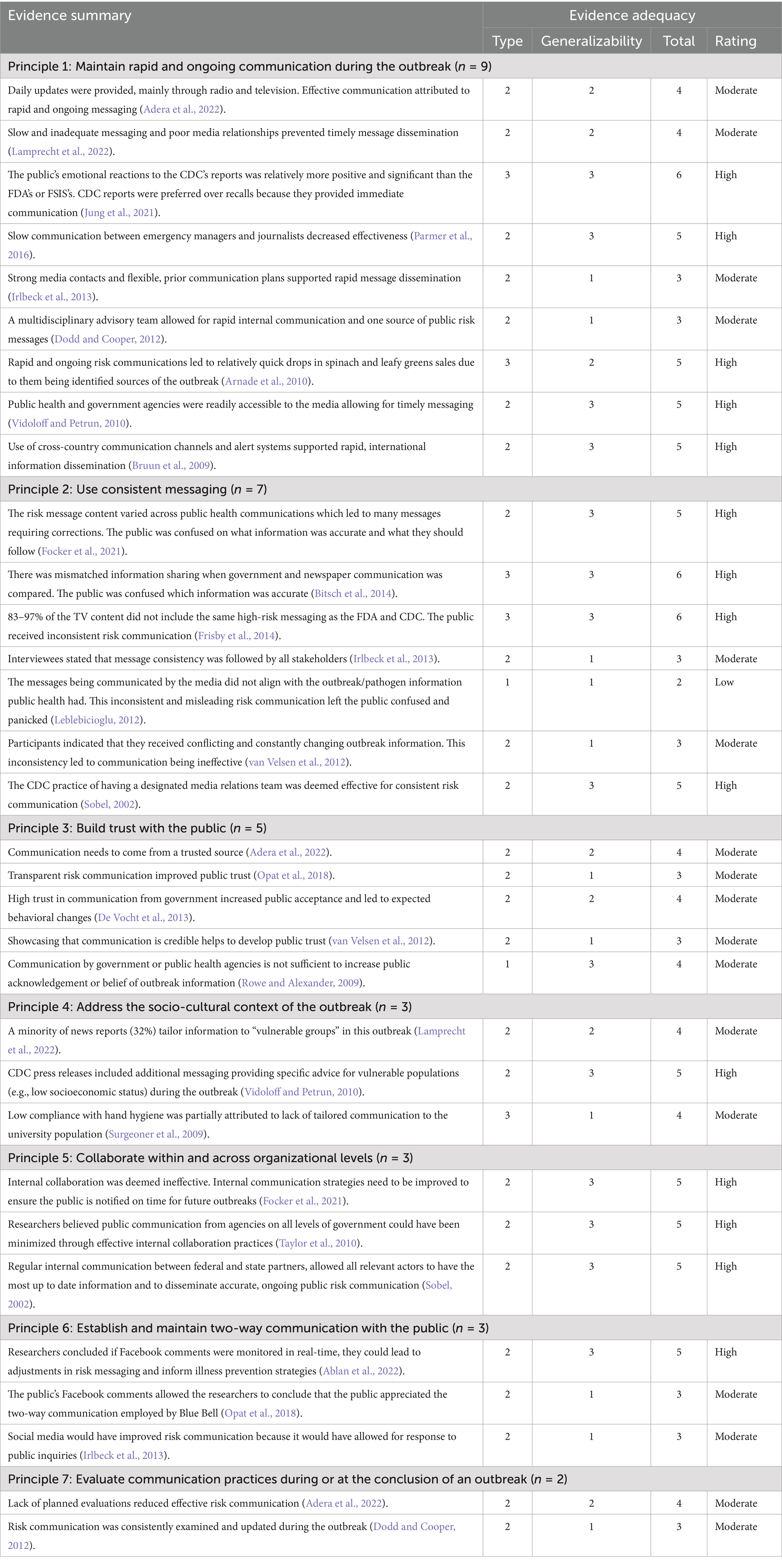
Table 1. Principles for effective risk communication during enteric illness outbreaks (n = 7).
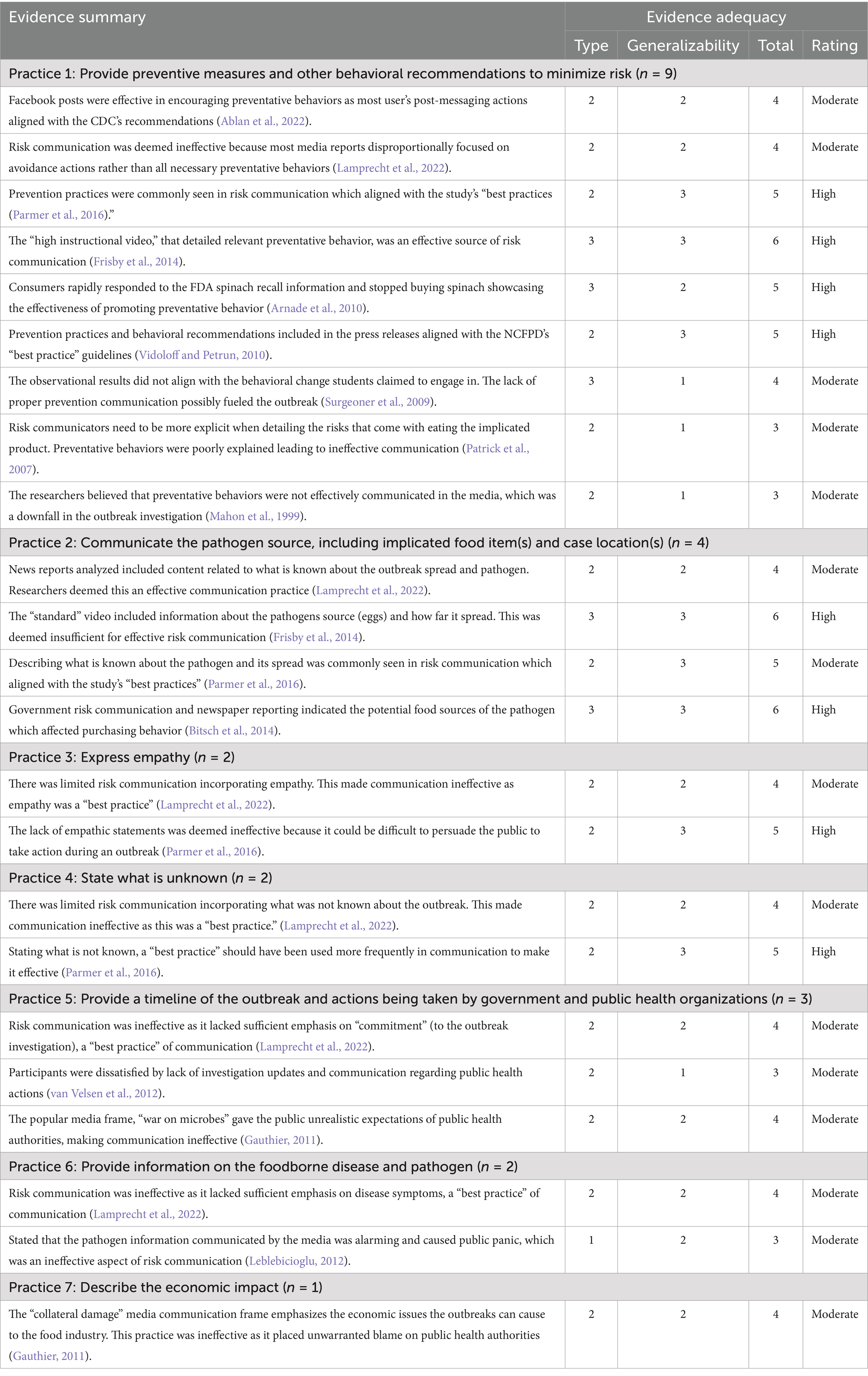
Table 2. Practices for effective risk communication during enteric illness outbreaks (n = 7).
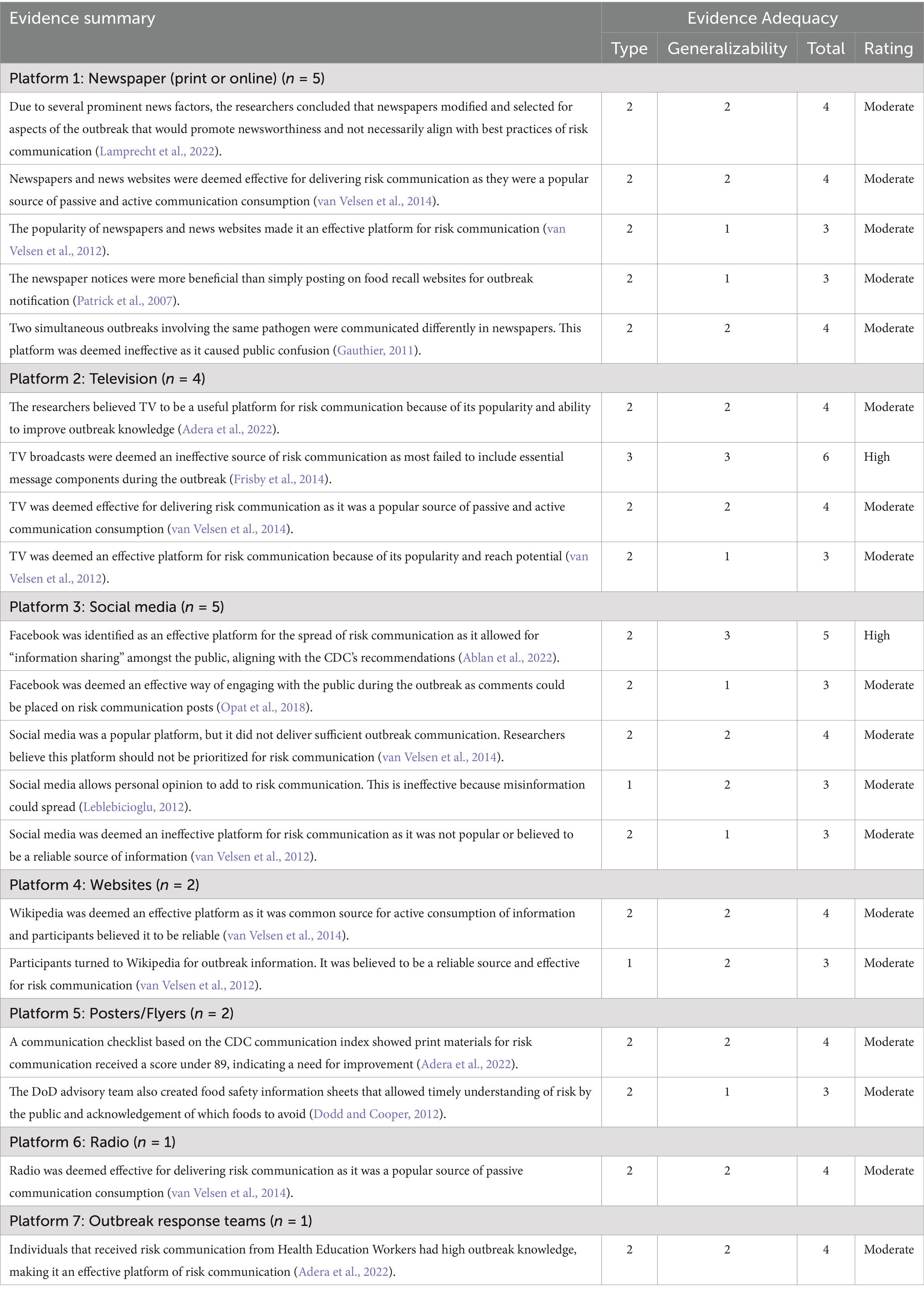
Table 3. Platforms for effective risk communication during enteric illness outbreaks (n = 7).

Table 4. Overall evidence evaluation for identified principles, practices, and platforms for effective risk communication during enteric illness outbreaks.
3.4 Principles (n = 7)
3.4.1 Maintain rapid and ongoing communication during the outbreak
Risk communication messages should be regularly and consistently disseminated for the duration of the outbreak, including when the outbreak has been declared over. If daily updates can be provided, these should be communicated early in the morning. Public health authorities should be guided by a flexible risk communication plan, designed and tested prior to crisis onset. The plan should include building strong relationships with media outlets to facilitate rapid information dissemination to the public via media platforms. National alert systems should be explored for rapid notification of national and international stakeholders, when applicable (Adera et al., 2022; Arnade et al., 2010; Dodd and Cooper, 2012; Irlbeck et al., 2013; Jung et al., 2021; Lamprecht et al., 2022; Parmer et al., 2016).
3.4.2 Use consistent messaging
Messaging should be consistent within and across stakeholders that communicate with the public, particularly public health authorities and media. Messages delivered by public health authorities and media should importantly be similar. Public health authorities should actively collaborate with media outlets, possibly using integrated communication strategies, to ensure consistent messaging. A designated media relations team may be useful in streamlining message creation and delivery (Bitsch et al., 2014; Focker et al., 2021; Frisby et al., 2014; Irlbeck et al., 2013; Leblebicioglu, 2012; Sobel, 2002; van Velsen et al., 2012).
3.4.3 Build trust with the public
Public health authorities should be the first (i.e., most timely) communicator of risk during outbreaks. The public is more likely to view authorities as a trusted source of information when they are first in delivering risk communication messages. Risk communicators must be honest in their messaging and remain accessible to the public. Lying (e.gs. half-truths, omissions), downplaying public health risks, and silence should be avoided. Credibility systems should be established by public health authorities to promote an objective certification system for risk communication messages delivered to the public (Adera et al., 2022; De Vocht et al., 2013; Opat et al., 2018; Rowe and Alexander, 2009; van Velsen et al., 2012).
3.4.4 Address the social/cultural context of the outbreak
Risk communicators must identify specific sub-populations that may be disproportionately affected by the outbreak. Risk communication should be tailored to multiple target socio-demographic audiences according to their communication preferences, which should be determined in a proactive manner. This will likely require the development of multiple message formats and use of multiple platforms to deliver tailored, contextual risk communication messages (Lamprecht et al., 2022; Surgeoner et al., 2009; Vidoloff and Petrun, 2010).
3.4.5 Collaborate within and across organizational levels
Collaboration within national government agencies and across organizational levels with jurisdictional partners at sub-national and local/regional levels is important for creating and delivering risk communication messages. Creation and delivery of risk messages should be coordinated and guided by a framework detailing how national agencies can and will work with jurisdictional partners, while respecting the autonomous nature of many of these organizations. These frameworks can also provide guidance to partners on creating effective risk communication messages if partners choose to create their own communication products. Strong inter-coordination can be achieved through regular, timely calls with all relevant partners to draft and deliver risk communication messages for the duration of the outbreak. Likewise, strong internal coordination can be supported through regular communication and use of internal online platforms to act as a singular source of outbreak information (Focker et al., 2021; Sobel, 2002; Taylor et al., 2010).
3.4.6 Establish and maintain two-way communication with the public
Public health authorities should monitor public reactions and responses to risk communication products, including questions posed by the public, which may indicate opportunities for public health authorities to address misunderstandings or confusion. Public feedback can also highlight opportunities for improving future risk communication products and should be collected and evaluated to support iterative improvement. Real-time monitoring of reactions and responses can be achieved on most online and social media platforms. In addition, public health authorities should interact with the public by directly responding to questions and comments for the duration of the outbreak (Ablan et al., 2022; Irlbeck et al., 2013; Opat et al., 2018).
3.4.7 Evaluate communication practices during and/or at the conclusion of an outbreak
An evaluation plan should be proactively developed by public health authorities to monitor the effectiveness of risk communication products and support iterative improvement, both during an outbreak and for future outbreaks. During an outbreak, the effectiveness of risk communication products should be monitored in real-time and adjustments to communication strategies or products made accordingly. Once an outbreak has concluded, a more thorough evaluation can be conducted to support future improvement of communication practices. The communication strategies and plan should be reviewed for effectiveness in as close to real-time as possible (Adera et al., 2022; Dodd and Cooper, 2012).
3.5 Practices (n = 9)
3.5.1 Provide preventive measures and other behavioral recommendations to minimize risk
The public must be informed of actions they can take to prevent illness during the outbreak, including avoiding the source of the outbreak (if known), and using general safe food handling and hygiene practices. In addition, there may be other behavioral recommendations specific to a particular hazard or sub-population that should be identified with knowledge from industry or other stakeholders and included as part of tailored risk communication products (Ablan et al., 2022; Arnade et al., 2010; Frisby et al., 2014; Lamprecht et al., 2022; Mahon et al., 1999; Parmer et al., 2016; Patrick et al., 2007; Surgeoner et al., 2009; Vidoloff and Petrun, 2010).
3.5.2 Communicate the pathogen source, including implicated food, water, or animal source(s) and case location(s)
The type of outbreak (foodborne, waterborne, or zoonotic) and source(s) should be stated. If the source is unknown, the public should be informed that the source is unknown and that there are several sources being investigated. These sources should be named, if possible. In addition, case locations should be reported and regularly updated as the outbreak evolves (Bitsch et al., 2014; Frisby et al., 2014; Lamprecht et al., 2022; Parmer et al., 2016).
3.5.3 Express empathy
Public health authorities should include empathetic statements in their risk communication to help support the public in staying calm and limiting unnecessary fear regarding the outbreak. Empathetic statements support the emotional processing of information, which tends to occur prior to logical processing of information (Lamprecht et al., 2022; Parmer et al., 2016).
3.5.4 State what is unknown about the outbreak
Details of the outbreak that are still being investigated and are currently unknown should be shared to promote honest and transparent communication. The public should be made aware of how these unknowns may impact their risk of illness (Lamprecht et al., 2022; Parmer et al., 2016).
3.5.5 Provide a timeline of the outbreak and actions being taken by government and public health organizations
Official outbreak investigation details, including a timeline and when the investigation is closed, should be clearly communicated. Actions taken by relevant agencies should also be described, emphasizing the continuous commitment of public health authorities to the investigation (Gauthier, 2011; Lamprecht et al., 2022; van Velsen et al., 2012).
3.5.6 Provide information on the enteric illness and pathogen
Epidemiological information including length of the latent period, length of the incubation period, clinical signs and symptoms, and other descriptive epidemiological information should be presented. Additional high-level details about the pathogen itself can also be provided (Lamprecht et al., 2022; Leblebicioglu, 2012).
3.5.7 Describe the economic impact
If the outbreak is associated with a specific product, industry stakeholders should be consulted by public health authorities regarding planned risk communication products. If substantial economic loss may occur, it is important that risk communication products do not place unnecessary blame on public health authorities (Gauthier, 2011).
3.5.8 Communicate incidence risk and rates
While this practice was identified, no evidence was provided on how to effectively communicate measures of disease burden during an outbreak.
3.5.9 Describe medical interventions that can be safely used to reduce exposure or adverse health outcomes
This practice relates to informing the public of medications and treatments used to reduce or eliminate the pathogen, as well as ongoing treatment development efforts. No evidence was provided for how to effectively communicate this information.
3.6 Platforms (n = 8)
3.6.1 Newspaper (Print or online)
Risk communication can be delivered through physical newspapers or news websites. News sources that are popular amongst the target audience(s) should be prioritized by public health authorities for information sharing. Public health authorities should seek to build and maintain good working relationships with news outlets to promote timely, objective, and prioritized information sharing during outbreaks (Gauthier, 2011; Lamprecht et al., 2022; Patrick et al., 2007; van Velsen et al., 2012, 2014).
3.6.2 Television
Risk communication should be delivered on popular television channels that are frequented by the target audience(s). Television news broadcasts are an important source of outbreak information with a broad reach and should be prioritized during outbreaks (Adera et al., 2022; Frisby et al., 2014; van Velsen et al., 2012, 2014).
3.6.3 Social media
Facebook and X (formerly Twitter) are universally popular social media platforms for risk communication. Risk communication should be disseminated from official public health accounts to establish and ensure credibility. Public health authorities can use social media to monitor the public’s reactions and inquiries related to outbreak risk communication. The effectiveness of risk communication may be affected if public opinion becomes intertwined with risk communication information provided by public health authorities (Ablan et al., 2022; Leblebicioglu, 2012; Opat et al., 2018; van Velsen et al., 2012, 2014).
3.6.4 Websites
Public health authorities should monitor webpages posted by other sources (e.g., other government websites, private industry websites, Wikipedia) to ensure accurate information is being presented to the public. Where possible, incorrect information should be flagged or edited when identified (van Velsen et al., 2012, 2014).
3.6.5 Posters/Flyers
Physical copies of posters or flyers with outbreak information can be posted or distributed within relevant communities during an outbreak. Appropriate use of graphics and design elements may improve awareness and comprehension. Where possible, plain language should be used (Adera et al., 2022; Dodd and Cooper, 2012).
3.6.6 Radio
Radio broadcasts can be important sources of information during an outbreak. If known, radio channels popular with target audience(s) should be prioritized to share information with the public (van Velsen et al., 2014).
3.6.7 Outbreak response teams
Public health authorities may create response teams at the onset of an outbreak to raise awareness in affected communities, particularly via person-to-person communication. These teams should include government, health, media, and social science personnel (Adera et al., 2022).
3.6.8 E-mails
If contact information is available, e-mails can be used to directly communicate with target audiences; however, no evidence was provided regarding how to effectively utilize this platform.
4 Discussion
4.1 Summary of main findings
In this scoping review, we synthesized findings from 25 studies that evaluated the effectiveness of risk communication principles, practices, or platforms during enteric illness outbreak investigations. We identified 7 principles, 9 practices, and 8 platforms for which evidence exists for their effectiveness, and further identified 6, 4, and 2 high-confidence principles, practices, and platforms, respectively. To support their incorporation into risk communication efforts, we provide the following four recommendations in no particular order: (1) build relationships and collaborate with media outlets, (2) identify target audiences and tailor information accordingly, (3) engage with target audiences, and (4) increase and maintain credibility of public health organizations delivering risk communication messages.
4.1.1 Build relationships and collaborate with media outlets
Effective implementation of identified risk communication principles and practices and use of platforms requires collaboration with various entities along communication pathways from the investigating public health organization to target audiences. This includes collaboration within and across the investigating organization, other public health organizations, private industry stakeholders, and media outlets. Media outlets play an important role in disseminating health information, particularly during outbreaks, as they can increase public awareness and shape public opinion (Pinto et al., 2023). In Canada, various demographic groups are engaged with media outlets, with over 80% of adults reading print or digital newspapers each week (Watson, 2024).
During enteric illness outbreaks, it is important to ensure timely communication of the most pertinent outbreak information. Collaboration with media outlets can facilitate enteric illness outbreak communication efforts by increasing message consistency, information dissemination, awareness about ongoing outbreaks, and uptake of protective behavioral recommendations (Maciel-Lima et al., 2015; Hong et al., 2019; Pieri, 2019; Nwakpu et al., 2020; Adera et al., 2022). Conversely, a lack of collaboration in risk communication can impede message uptake and undermine the credibility of information (Food and Agriculture Organization of the United Nations and World Health Organization, 2016; Savoia et al., 2023).
Collaboration with media outlets can be facilitated by guiding protocols and communication plans that promote positive relationships between media outlets and public health organizations. Specifically, promoting collaboration with media outlets requires a strategic approach across three stages: pre-outbreak preparation, active communication during the outbreaks, and post-outbreak follow-up. Prior to the outbreak, positive relationships should be established between media outlets and public health organizations responsible for risk communication (Irlbeck et al., 2013; Centers for Disease Control and Prevention, 2014). Further, designing a streamlined pathway for communication between these two stakeholders can increase understanding of their respective roles and goals during outbreak risk communication and increase the efficacy of collaboration (Lamprecht et al., 2022). During the outbreak, consistent engagement with the media can facilitate rapid dissemination of outbreak information to the public, including advisories that the outbreak has ended. During the outbreak, designated media relations teams should be established to ensure accurate, timely, and consistent dissemination of outbreak information (Sobel, 2002; Dodd and Cooper, 2012). Once the outbreak has concluded, public health authorities should evaluate their performance and collaborative efforts with media outlets to identify opportunities for improving future risk communication (Food and Agriculture Organization of the United Nations and World Health Organization, 2016). Further, feedback from media outlets should be sought to understand how public health organizations can better support collaboration when future enteric illness outbreaks occur (Food and Agriculture Organization of the United Nations and World Health Organization, 2016).
4.1.2 Identify target audiences and tailor information accordingly
The primary goal of risk communication is to provide the public with information needed to make informed health decisions (World Health Organization, 2017). To support this, it is important to identify target audiences and tailor messages to address their concerns and needs, ensuring that the information is culturally relevant and accessible. Studies indicate that certain populations are at greater risk of acquiring enteric illnesses, including pregnant women, young children, older adults, and the immunocompromised (Barkley et al., 2016; Cardemil et al., 2017). Tailoring communication to vulnerable groups during enteric illness outbreaks can increase accessibility, uptake, and acceptance of behavioral recommendations (Kreuter et al., 1999; Benham et al., 2021).
To effectively tailor risk communication, it is important to understand the populations at risk. This involves identifying and characterizing specific sub-populations at risk, assessing their current knowledge and perceptions of risk, and recognizing any barriers to communicating with them (Public Health Ontario, 2016). For instance, when developing risk communication products, particularly during foodborne illness outbreaks, it is important to maintain cultural sensitivity, as food preparation and consumption practices are often deeply rooted in tradition (Food and Agriculture Organization of the United Nations and World Health Organization, 2016). Additionally, platform preferences must be considered to ensure that the most effective communication channels are used to reach those at risk. Audiences use a variety of platforms and channels to acquire information, including social media, websites, and newspapers, with some consulting multiple sources to inform their health decision-making process (Lin et al., 2014; Jardine et al., 2015; Ali et al., 2020). Tailored communication can enhance the adoption of behavioral recommendations (Glanz et al., 2015), highlighting the importance of a customized approach when communicating about enteric illness outbreak investigations.
4.1.3 Engage with target audiences
Engaging with target audiences can contribute to the success of risk communication during enteric illness outbreaks. In general, top-down communication has been used during public health events given the urgency of the situation (Public Health Ontario, 2023). However, adopting a bi-directional communication approach when the situation is less urgent can offer benefits. Promoting two-way communication with the public allows investigating health organizations to understand the needs of those at risk, reduce the impact of ongoing outbreaks, increase public engagement with risk communication products, increase trust in investigating organizations, and promote the uptake of recommended behaviors (Guan et al., 2021; Public Health Ontario, 2023). Social media is an effective platform for disseminating information to a broad audience and promoting bi-directional conversation (Malecki et al., 2021). With over 33 million social media users in Canada, and 1 in 7 using social media networks daily (Dixon, 2024), public health organizations have access to a platform with a broad reach potential. While our scoping review found conflicting evidence regarding the effectiveness of social media for risk communication – some sources questioned its reliability (van Velsen et al., 2012) and cited the potential for spread of misinformation (Leblebicioglu, 2012) – others recognized its value in helping users acquire information about the outbreak and share their own experiences and opinions (Opat et al., 2018; Ablan et al., 2022).
To promote engagement with the public, it is important to consider practices that can enhance the public’s engagement with risk communication products. Generally, risk communication products disseminated by government and public health organizations experience less interaction (Kamiński et al., 2021). However, public health organizations are among the most trusted sources of information during outbreaks (Waddell, 2020), and therefore practices promoting engagement with target audiences should be implemented. For instance, when communicating via social media, aligning risk communication products with best practices such as using a conversational tone and including call to actions may help to increase engagement (MacKay et al., 2022).
4.1.4 Increase and maintain credibility of public health organizations delivering risk communication messages
An individual’s perception of the investigating organization can influence public trust (Food and Agriculture Organization of the United Nations and World Health Organization, 2016). This study identified transparency and timeliness as contributing factors to building trust and credibility. Maintaining transparency, such as addressing uncertainties in an ongoing outbreak and explaining how the investigating agency plans to address them, is important for building credibility, enhancing public understanding, and encouraging uptake of recommended behaviors (Food and Agriculture Organization of the United Nations and World Health Organization, 2016; Plohl and Musil, 2021). Similarly, maintaining timeliness of risk communication, such as addressing when the outbreak has ended, is also important for building and maintaining trust and credibility, and positively influencing risk perception and action (Food and Agriculture Organization of the United Nations and World Health Organization, 2016; Gong et al., 2021; Yi et al., 2024). For instance, enhanced intra-organization coordination and initiating of risk communication by information sources can prevent the spread of misinformation and rumors (Adera et al., 2022).
Other identified practices that can build and maintain trust and credibility include expressing empathy. Empathetic communication should address and validate the emotions of the public (Public Health Ontario, 2016). Using empathy when communicating about enteric illness outbreak investigations can increase trust, promote engagement with risk communication products, and support the uptake of recommended behaviors (Liao et al., 2020; Parmer et al., 2016; MacKay et al., 2022; Savoia et al., 2023).
4.2 Implementation of best practices
To support implementation, active, multifaceted training and education approaches, such as workshops, online training modules, centralized resources, and other educational outreach is recommended to enhance knowledge retention and application by practitioners (MacKay et al., 2024). In addition, incorporating these practices into ongoing public health training programs, such as those for emergency preparedness or food safety, would ensure that practitioners are well-versed in their application. These strategies not only increase the reach of evidence but also motivate practitioners to adopt and integrate these practices effectively into their work environments (McCormack et al., 2013). Tailored approaches that reinforce learning and keep practitioners updated on evolving best practices are likely to be beneficial (McAlpine et al., 2024).
4.3 Relationship to general health and risk communication
These findings align closely with established principles of crisis and risk communication while highlighting unique considerations for enteric illness outbreaks. General risk communication emphasizes timeliness and transparency to build public trust and combat misinformation, which is particularly critical for enteric illnesses due to their acute nature and potential for rapid spread through foodborne pathways (Food and Agriculture Organization of the United Nations and World Health Organization, 2016). Tailored messaging, a cornerstone of effective communication, becomes even more vital for vulnerable populations, such as pregnant individuals or the immunocompromised, who face heightened risks during enteric outbreaks (Barkley et al., 2016; Kreuter et al., 1999). The role of media and multi-channel outreach, commonly leveraged in health crises, requires additional coordination with food safety authorities and industry stakeholders to address consumer concerns effectively (Maciel-Lima et al., 2015; Malecki et al., 2021). Furthermore, enteric illnesses demand an immediate behavioral focus, such as avoiding contaminated foods or practicing safe food preparation, in contrast to longer-term health interventions like vaccination campaigns (Glanz et al., 2015; Food and Agriculture Organization of the United Nations and World Health Organization, 2016). Together, these considerations underscore the importance of tailoring risk communication strategies to the unique characteristics of enteric illness outbreaks.
4.4 Limitations
This scoping review has several limitations. First, while a geographic limiter was not applied in our search strategy, most studies included in the review were from North America and Europe. This may bias our findings to risk communication efforts appropriate to these contexts whilst limiting generalizability to other areas. Second, our review excluded studies that only described risk communication during an enteric illness outbreak and did not provide an evaluation of its effectiveness. This may have excluded or downplayed important principles, practices, or platforms. We attempted to mitigate this by still listing identified practices and platforms with no evidence of effectiveness for completeness. Third, this review may not have captured new and emerging risk communication efforts (e.g., use of TikTok) where peer-reviewed evidence is still forthcoming. We aimed to include other sources of evidence that may have described novel risk communication approaches using a gray literature search.
5 Conclusion
This scoping review synthesized evidence for effective risk communication principles, practices, and platforms that can be implemented during enteric illness outbreaks. These approaches are intended to be general; however, their implementation should be guided by organizational and community needs. Proactive and intentional planning and adoption of evidence-based risk communication approaches is needed to optimize sustainable use and implementation. Ongoing evaluation of these and other emerging approaches is needed to support effective message dissemination and uptake of health protective behaviors during outbreaks. Effective risk communication remains an essential component of responses to enteric illness outbreaks in support of limiting adverse health outcomes and unnecessary healthcare utilization.
Data availability statement
The original contributions presented in the study are included as citations in the article. Further inquiries can be directed to the corresponding author.
Author contributions
HM: Methodology, Investigation, Writing – original draft. JEM: Methodology, Supervision, Writing – review & editing. JM: Investigation, Writing – review & editing. HS: Writing – review & editing. MM: Writing – review & editing, Methodology. LC: Methodology, Writing – review & editing. MP: Funding acquisition, Methodology, Writing – review & editing. LG: Methodology, Writing – review & editing, Conceptualization, Project administration, Supervision.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. Funding was provided by the Public Health Agency of Canada.
Acknowledgments
We thank Jacqueline Kreller-Vanderkooy for their assistance in developing the scoping review protocol.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcomm.2024.1509940/full#supplementary-material
References
Ablan, M., Pomeroy, M., Sood, N. J., and Marshall, K. E. (2022). A Qualitative Content Analysis of Responses to CDC's Foodborne Outbreak Messages on Facebook. Food Prot. Trends 42, 174–185. doi: 10.4315/fpt-21-028.37179820
Adera, N. G., Ketama, B., and Girma, E. (2022). Effectiveness and quality of risk communication process in Ethiopia: The case of risk communication during cholera outbreak in Addis Ababa, Ethiopia. PLoS One 17:e0265203. doi: 10.1371/journal.pone.0265203
Ali, S. H., Foreman, J., Tozan, Y., Capasso, A., Jones, A. M., and DiClemente, R. J. (2020). Trends and predictors of COVID-19 information sources and their relationship with knowledge and beliefs related to the pandemic: Nationwide cross-sectional study. JMIR Public Health Surveill. 6:e21071. doi: 10.2196/21071
Andersen, P. A., and Spitzberg, B. H. (2010). “Myths and maxims of risk and crisis communication” in Handbook of risk and crisis communication. eds. R. L. Heath and H. D. O’Hair (New York: Routledge), 205–226.
Arksey, H., and O’Malley, L. (2005). Scoping studies: towards a methodological framework. Int. J. Soc. Res. Methodol. 8, 19–32. doi: 10.1080/1364557032000119616
Arnade, C., Calvin, L., and Kuchler, F. (2010). Consumers’ Response to the 2006 Foodborne Illness Outbreak Linked to Spinach. Available at: https://www.ers.usda.gov/amber-waves/2010/march/consumers-response-to-the-2006-foodborne-illness-outbreak-linked-to-spinach/ (Accessed March 20, 2023).
Barkley, J., Julian, E., Viveiros, B., Gosciminski, M., and Bandy, U. (2016). Preventing foodborne and enteric illnesses among at-risk populations in the United States and Rhode Island. Rhode Island Med. J. 99, 25–28
Benham, J. L., Atabati, O., Oxoby, R. J., Mourali, M., Shaffer, B., Sheikh, H., et al. (2021). COVID-19 vaccine-related attitudes and beliefs in Canada: National cross-sectional survey and cluster analysis. JMIR Public Health Surveill. 7:e30424. doi: 10.2196/30424
Bitsch, V., Koković, N., and Rombach, M. (2014). Risk communication and market effects during foodborne illnesses: A comparative case study of bacterial outbreaks in the U.S. and in Germany. Int. Food Agribusiness Manage. Rev. 17, 1–18. doi: 10.22004/ag.econ.183451
Bruun, T., Sørensen, G., Forshell, L. P., Jensen, T., Nygard, K., Kapperud, G., et al. (2009). An outbreak of Salmonella Typhimurium infections in Denmark, Norway and Sweden, 2008. Euro surveillance: bulletin Europeen sur les maladies transmissibles. Eur. Commun. Disease Bull. 14:19147. doi: 10.2807/ese.14.10.19147-en
Cairns, G., de Andrade, M., and MacDonald, L. (2013). Reputation, relationships, risk communication, and the role of trust in the prevention and control of communicable disease: a review. J. Health Commun. 18, 1550–1565. doi: 10.1080/10810730.2013.840696
Canadian Agency for Drugs and Technology in Health. (2018). Grey matters; a practical tool for searching health-related grey literature. Available at: https://www.cda-amc.ca/grey-matters-practical-tool-searching-health-related-grey-literature (Accessed May 5, 2023).
Cardemil, C. V., Parashar, U. D., and Hall, A. J. (2017). Norovirus infection in older adults: Epidemiology, risk factors, and opportunities for prevention and control. Infect. Dis. Clin. N. Am. 31, 839–870. doi: 10.1016/j.idc.2017.07.012
Centers for Disease Control and Prevention. (2014). Crisis and emergency risk communication: working with the media. Available at: https://emergency.cdc.gov/cerc/ppt/CERC_Working_with_the_Media.pdf (Accessed June 9, 2023).
Covidence. (n.d.). Data Synthesis and Extraction Tool. https://app.covidence.org/reviews/300370
De Vocht, M., Cauberghe, V., Sas, B., and Uyttendaele, M. (2013). Analyzing consumers' reactions to news coverage of the 2011 Escherichia coli O104:H4 outbreak, using the Extended Parallel Processing Model. J. Food Prot. 76, 473–481. doi: 10.4315/0362-028X.JFP-12-339
Dixon, S.J. (2024). Most popular social networks worldwide as of April 2024, by number of monthly active users. Available at: https://www.statista.com/statistics/272014/global-social-networks-ranked-by-number-of-users/ (Accessed July 13, 2024).
Dodd, C. C., and Cooper, M. J. (2012). Multidisciplinary response to the Escherichia coli O104 outbreak in Europe. Mil. Med. 177, 1406–1410. doi: 10.7205/MILMED-D-12-00097
Drudge, C., Greco, S., Kim, J., and Copes, R. (2019). Estimated annual deaths, hospitalizations, and emergency department and physician office visits from foodborne illness in Ontario. Foodborne Pathogen Distribution 16, 173–179. doi: 10.1089/fpd.2018.2545
Focker, M., van den Borne, B. H. P., Fischer, M., Schuh, E., Mader, A., Andersson, M. G., et al. (2021). Interactions between risk assessors and risk managers during three major food incidents in Europe. J. Food Sci. 86, 3611–3627. doi: 10.1111/1750-3841.15824
Food and Agriculture Organization of the United Nations and World Health Organization. (2016). Risk communication applied to food safety handbook. Available at: https://www.fao.org/3/i5863e/i5863e.pdf (Accessed June 9, 2023).
Frisby, B. N., Veill, S. R., and Sellnow, T. L. (2014). Instructional messages during health-related crises: essential content for self-protection. Health Commun. 29, 347–354. doi: 10.1080/10410236.2012.755604
Galanis, E., Goshtasebi, A., Hung, Y. W., Chan, J., Matsell, D., Chapman, K., et al. (2023). Developing International Classification of Disease code definitions for the study of enteric infection sequelae in Canada. Canada Commun. Disease Report 49, 299–309. doi: 10.14745/ccdr.v49i78a01
Gauthier, E. (2011). Foodborne microbial risks in the press: the framing of listeriosis in Canadian newspapers. Public Understand. Sci. 20, 270–286. doi: 10.1177/0963662510363379
Glanz, J. M., Kraus, C. R., and Daley, M. F. (2015). Addressing parental vaccine concerns: engagement, balance, and timing. PLoS Biol. 13:e1002227. doi: 10.1371/journal.pbio.1002227
Glenton, C., Carlsen, B., Lewin, S., Munthe-Kaas, H., Colvin, C. J., Tunçlap, Ö., et al. (2018). Applying GRADE-CERQual to qualitative evidence synthesis findings—paper 5: how to assess adequacy of data. Implementation Sci. 13:14. doi: 10.1186/s13012-017-0692-7
Gohari, M. R., Taylor, M., MacKinnon, M. C., Panagiotoglou, D., Galanis, E., Kaplan, G. G., et al. (2022). Patterns of enteric infections in a population-wide cohort study of sequelae, British Columbia, Canada. Epidemiol. Infect. 151:e7. doi: 10.1017/S0950268822001911
Gong, N., Jin, X., Liao, J., Li, Y., Zhang, M., Cheng, Y., et al. (2021). Authorized, clear and timely communication of risk to guide public perception and action: lessons of COVID-19 from China. BMC Public Health 21:1545. doi: 10.1186/s12889-021-11103-1
Greco, S. L., Drudge, C., Fernandes, R., Kim, J., and Copes, R. (2020). Estimates of healthcare utilisation and deaths from waterborne pathogen exposure in Ontario, Canada. Epidemiol. Infect. 148:e70. doi: 10.1017/S0950268820000631
Guan, B., Bao, G., Liu, Q., and Raymond, R. G. (2021). Two-way risk communication, public value consensus, and citizens’ policy compliance willingness about COVID-19: Multilevel analysis based on a nudge View. Admin. Soc. 53, 1106–1149. doi: 10.1177/0095399721990332
Hong, Y., Kim, J.-S., and Xiong, L. (2019). Media exposure and individuals’ emergency preparedness behaviours for coping with natural and human-made disasters. J. Environ. Psychol. 63, 82–91. doi: 10.1016/j.jenvp.2019.04.005
Infanti, J., Sixsmith, J., Barry, M. M., Núñez-Córdoba, J., Oroviogoicoechea-Ortega, C., and Guillén-Grima, F. (2013). A literature review on effective risk communication for the prevention and control of communicable diseases in Europe. Stockholm: ECDC.
Irlbeck, E., Jennings, J. F., Meyers, C., Gibson, C., and Chambers, T. (2013). A case study of the crisis communications used in the 2009 Salmonella outbreak in peanut products. J. Appl. Commun. 97, 19–32. doi: 10.4148/1051-0834.1125
Janoske, M., Liu, B., and Sheppard, B. (2012). “Understanding risk communication best practices: a guide for emergency managers and communicators” in Report to Human Factors/Behavioral Sciences Division, Science and Technology Directorate, U.S. Department of Homeland Security (College Park, MD: START).
Jardine, C. G., Boerner, F. U., Boyd, A. D., and Driedger, S. M. (2015). The more the better? A comparison of the information sources used by the public during two infectious disease outbreaks. PLoS One 10:e0140028. doi: 10.1371/journal.pone.0140028
Jung, J., Bir, C., Widmar, N. O., and Sayal, P. (2021). Initial Reports of Foodborne Illness Drive More Public Attention Than Do Food Recall Announcements. J. Food Prot. 84, 1150–1159. doi: 10.4315/JFP-20-383
Kamiński, M., Szymańska, C., and Nowak, J. K. (2021). Whose Tweets on COVID-19 Gain the Most Attention: Celebrities, Political, or Scientific Authorities? Cyberpsychol. Behav. Soc. Netw. 24, 123–128. doi: 10.1089/cyber.2020.0336
Kreuter, M. W., Bull, F. C., Clark, E. M., and Oswald, D. L. (1999). Understanding how people process health information: a comparison of tailored and nontailored weight-loss materials. Health Psychol. 18, 487–494. doi: 10.1037/0278-6133.18.5.487
Lamprecht, C., Guenther, L., and Joubert, M. (2022). ‘Polony panic’: News values and risk messages in news coverage of the South African listeriosis outbreak of 2017–2018. Health Risk Soc. 24, 67–91. doi: 10.1080/13698575.2022.2033177
Leblebicioglu, H. (2012). Enterohemorrhagic Escherichia coli Epidemic: The Sensitive Role of the Media in the Handling of Epidemics. Clin. Infect. Dis. 54, 450–451. doi: 10.1093/cid/cir719
Liao, Q., Yuan, J., Dong, M., Yang, L., Fielding, R., and Lam, W. W. T. (2020). Public engagement and government responsiveness in the communications about COVID-19 during the early epidemic stage in China: Infodemiology study on social media data. J. Med. Internet Res. 22:e18796. doi: 10.2196/18796
Lin, L., Jung, M., McCloud, R. F., and Viswanath, K. (2014). Media use and communication inequalities in a public health emergency: a case study of 2009–2010 pandemic influenza A virus subtype H1N1. Public Health Rep. 129, 49–60. doi: 10.1177/00333549141296S408
Maciel-Lima, S. M., Rasia, J. M., Bagatelli, R. C., Gontarski, G., and Colares, M. J. (2015). The impact that the influenza A (H1N1) pandemic had on news reporting in the state of Paraná, Brazil. Historia Ciencias Saude 22, 273–291. doi: 10.1590/S0104-59702015000100016
MacKay, M., Colangeli, T., Jaworski, J., Ford, C., Papadopoulos, A., McWhirter, J.E., et al. (2022). Social media guidebook for public health. Available at: https://machmb.ca/wp-content/uploads/2022/08/Social-Media-Guidebook-Crisis-Communication-for-Public-Health_English.pdf (Accessed June 9, 2023).
MacKay, M., McAlpine, D., Worte, H., Grant, L. E., Papadopoulos, A., and McWhirter, J. E. (2024). Public health communication professional development opportunities and alignment with core competencies: an environmental scan and content analysis. Offres de perfectionnement professionnel en communication en santé publique et correspondance avec les compétences essentielles: analyse contextuelle et analyse de contenu. Health Promot. Chronic Disease Prevent. Canada 44, 218–228. doi: 10.24095/hpcdp.44.5.03
Mahon, B. E., Slutsker, L., Hutwagner, L., Drenzek, C., Maloney, K., Toomey, K., et al. (1999). Consequences in Georgia of a nationwide outbreak of Salmonella infections: what you don’t know might hurt you. Am. J. Public Health 89, 31–35. doi: 10.2105/AJPH.89.1.31
Malecki, K. M. C., Keating, J. A., and Safdar, N. (2021). Crisis Communication and Public Perception of COVID-19 Risk in the Era of Social Media. Clin. Infect. Dis. 72, 697–702. doi: 10.1093/cid/ciaa758
Mastrandrea, M. D., Field, C. B., Stocker, T. F., Edenhofer, O., Ebi, K. L., Frame, D. J., et al. (2010). Guidance note for lead authors of the IPCC Fifth Assessment Report on consistent treatment of uncertainties. Intergovernmental Panel on Climate Change (IPCC). Available at: http://www.ipcc.ch (Accessed March 15, 2023).
McAlpine, D., MacKay, M., Grant, L. E., Papadopoulos, A., and McWhirter, J. E. (2024). Modernizing public health communication competencies in Canada: A survey of the Canadian public health workforce. Can. J. Public Health 115, 664–679. doi: 10.17269/s41997-024-00890-w
McCormack, L., Sheridan, S., Lewis, M., Boudewyns, V., Melvin, C. L., Kistler, C., et al. (2013). Communication and dissemination strategies to facilitate the use of health-related evidence. Evid. Rep. Technol. Assess. 213, 1–520. doi: 10.23970/ahrqepcerta213
Noyes, J., Booth, A., Lewin, S., Carlsen, B., Glenton, C., Colvin, C. J., et al. (2018). Applying GRADE-CERQual to qualitative evidence synthesis findings–paper 6: how to assess relevance of the data. Implement. Sci. 13:4. doi: 10.1186/s13012-017-0693-6
Nwakpu, E. S., Ezema, V. O., and Ogbodo, J. N. (2020). Nigeria media framing of coronavirus pandemic and audience response. Health Promot. Perspect. 10, 192–199. doi: 10.34172/hpp.2020.32
Opat, K., Magness, H., and Irlbeck, E. (2018). Blue Bell's Facebook Posts and Responses During the 2015 Listeria Crisis: A Case Study. J. Appl. Commun. 102, 1–16. doi: 10.4148/1051-0834.2232
Paez, A. (2017). Grey literature: An important resource in systematic reviews. J. Evid. Based Med. 10, 233–240. doi: 10.1111/jebm.12266
Parmer, J., Baur, C., Eroglu, D., Lubell, K., Prue, C., Reynolds, B., et al. (2016). Emergency risk messaging in mass media news stories: is the public getting the information they need to protect their health? Health Commun. 31, 1215–1222. doi: 10.1080/10410236.2015.1049728
Patrick, M. E., Griffin, P. M., Voetsch, A. C., and Mead, P. S. (2007). Effectiveness of recall notification: community response to a nationwide recall of hot dogs and deli meats. J. Food Prot. 70, 2373–2376. doi: 10.4315/0362-028X-70.10.2373
Peters, M. D. J., Godfrey, C., McInerney, P., Munn, Z., Tricco, A. C., and Khalil, H. (2020). “Chapter 11: Scoping Reviews (2020 version),” in JBI Manual for Evidence Synthesis. eds. E. Aromataris and Z. Munn (JBI). Available from https://synthesismanual.jbi.global.
Pieri, E. (2019). Media framing and the threat of global pandemics: the Ebola Crisis in UK media and policy response. Sociol. Res. Online 24, 73–92. doi: 10.1177/1360780418811966
Pinto, R., Lacerda, J., Silva, L., Araújo, A. C., Fontes, R., Lima, T. S., et al. (2023). Text mining analysis to understand the impact of online news on public health response: case of syphilis epidemic in Brazil. Front. Public Health 11:1248121. doi: 10.3389/fpubh.2023.1248121
Plohl, N., and Musil, B. (2021). Modeling compliance with COVID-19 prevention guidelines: the critical role of trust in science. Psychol. Health Med. 26, 1–12. doi: 10.1080/13548506.2020.1772988
Public Health Agency of Canada. (2017). Canada’s foodborne illness outbreak response protocol (FIORP). Available at: https://www.canada.ca/en/public-health/services/publications/health-risks-safety/canadas-foodborne-illness-outbreak-response-protocol-fiorp-guide-multi-jurisdictional-enteric-outbreak-response.html (Accessed March 1, 2023).
Public Health Ontario. (2016). EOH fundamentals: Risk communication. Available at: https://www.publichealthontario.ca/-/media/documents/f/2016/fundamentals-risk-comm.pdf?la=en (Accessed May 12, 2023).
Public Health Ontario. (2023). Risk communication and trust in public health during the COVID-19 pandemic. Retrieved from https://www.publichealthontario.ca/-/media/Documents/nCoV/main/2023/risk-communication-trust-public-health-covid-19-pandemic.pdf?rev=ba8a54b6d93d4b75acab6de7c38a987e&la=fr (Accessed May 12, 2023).
Rowe, S., and Alexander, N. (2009). Risk communication for the masses: who are we to say? (and what are we to say?). Nutr. Today 44, 260–264. doi: 10.1097/NT.0b013e3181c263a3
Savoia, E., Piltch-Loeb, R., Stanton, E. H., and Koh, H. K. (2023). Learning from COVID-19: government leaders’ perspectives to improve emergency risk communication. Glob. Health 19:86. doi: 10.1186/s12992-023-00993-y
Sobel, J. (2002). Investigation of multistate foodborne disease outbreaks. Public Health Rep. 117, 8–19. doi: 10.1016/S0033-3549(04)50103-6
Surgeoner, B. V., Chapman, B. J., and Powell, D. A. (2009). University students’ hand hygiene practice during a gastrointestinal outbreak in residence: what they say they do and what they actually do. J. Environ. Health 72, 24–28
Taylor, E., Kastner, J., and Renter, D. (2010). Challenges involved in the Salmonella Saintpaul outbreak and lessons learned. J. Public Health Manage. Pract. 16, 221–231. doi: 10.1097/PHH.0b013e3181b3a3e4
Thomas, M. K., and Murray, R.Canadian Burden of Food-borne Illness Estimates Working Group (2014). Estimating the burden of food-borne illness in Canada. Can. Commun. Disease Rep. 40, 299–302. doi: 10.14745/ccdr.v40i14a02
Thomas, M. K., Murray, R., Flockhart, L., Pintar, K., Pollari, F., Fazil, A., et al. (2013). Estimates of the burden of foodborne illness in Canada for 30 specified pathogens and unspecified agents, circa 2006. Foodborne Pathog. Dis. 10, 639–648. doi: 10.1089/fpd.2012.1389
Tricco, A. C., Lillie, E., Zarin, W., O'Brien, K. K., Colquhoun, H., Levac, D., et al. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann. Intern. Med. 169, 467–473. doi: 10.7326/M18-0850
Tumpey, A. J., Daigle, D., and Nowak, G. (2019). “Communicating During an Outbreak or Public Health Investigation” in The CDC Field Epidemiology Manual. eds. S. A. Rasmussen and R. A. Goodman (New York: Oxford Academic).
University of Wisconsin Population Health Institute. (2022). Our methods - evidence rating: guidelines. County Health Rankings & Roadmaps. Retrieved May 20, 2023, from https://www.countyhealthrankings.org/take-action-to-improve-health/what-works-for-health/our-methods
van Velsen, L., Van Gemert-Pijnen, J. E. W. C., Beaujean, D. J. M. A., Wentzel, J., and van Steenbergen, J. E. (2012). Should health organizations use web 2.0 media in times of an infectious disease crisis? An in-depth qualitative study of citizens' information behavior during an EHEC outbreak. J. Media Internet Res. 14:e181. doi: 10.2196/jmir.2123
van Velsen, L., Van Gemert-Pijnen, J. E. W. C., Beaujean, D. J. M. A., Wentzel, J., van Steenbergen, J. E., and Timen, A. (2014). Public knowledge and preventive behavior during a large-scale Salmonella outbreak: results from an online survey in the Netherlands. BMC Public Health 14:100. doi: 10.1186/1471-2458-14-100
Vidoloff, K. G., and Petrun, E. (2010). Communication Successes and Constraints: Analysis of the 2008 Salmonella Saintpaul foodborne illness outbreak. J. Northwest Commun. Assoc. 39, 65–90.
Vilella-Vila, M., and Costa-Font, J. (2008). Press media reporting effects on risk perceptions and attitudes towards genetically modified (GM) food. J. Behav. Exp. Econ. 37, 2095–2106. doi: 10.1016/j.socec.2008.04.006
Waddell, C. (2020). Carleton researchers find Canadians most trust public health officials on COVID-19. Available at: https://newsroom.carleton.ca/2020/carleton-researchers-find-canadians-most-trust-public-health-officials-on-covid-19/#:~:text=Asked%20to%20rank%20a%20series,37%20per%20cent%20of%20respondents (Accessed May 12, 2023).
Watson, A. (2024). Weekly print and digital newspaper reach in Canada from March 2019 to November 2023, by generation. Available at: https://www.statista.com/statistics/261801/newspaper-reach-in-canada-by-age/ (Accessed May 12, 2023).
World Health Organization. (2017). Communicating risk in public health emergencies: a WHO guideline for emergency risk communication (ERC) policy and practice. (Licence No. CC BY-NC-SA 3.0 IGO). Available at: https://apps.who.int/iris/handle/10665/259807 (Accessed March 1, 2023).
Keywords: best practices, risk communication, health communication, enteric illness, foodborne illness, foodborne disease, acute gastrointestinal illness, outbreaks
Citation: Mucević H, McWhirter JE, Macleod J, Shereefdeen H, MacKay M, Cheng L, Phypers M and Grant LE (2025) Best practices in public risk communication during enteric illness outbreak investigations: a scoping review. Front. Commun. 9:1509940. doi: 10.3389/fcomm.2024.1509940
Edited by:
Sean J. Upshaw, The University of Texas at Austin, United StatesReviewed by:
Patrick Merle, Florida State University, United StatesTimothy L. Sellnow, University of Central Florida, United States
Copyright © 2025 Mucević, McWhirter, Macleod, Shereefdeen, MacKay, Cheng, Phypers and Grant. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lauren E. Grant, bGF1Z3JhbnRAdW9ndWVscGguY2E=
†These authors share senior authorship