 Ann M. Partee*
Ann M. Partee* Shubhi Sachdeva
Shubhi Sachdeva Marissa A. Bivona†
Marissa A. Bivona† Kelsey A. Clayback†
Kelsey A. Clayback† Sasha Miller-Marshall†
Sasha Miller-Marshall† Kyra Parker†
Kyra Parker† Pilar Alamos
Pilar Alamos Cloe Frank
Cloe Frank Jason T. Downer
Jason T. Downer Amanda P. Williford
Amanda P. Williford- Center for Advanced Study of Teaching and Learning, University of Virginia, Charlottesville, VA, United States
Early childhood mental health consultation (ECMHC) is a targeted prevention service that aims to build the capacity of early care and education (ECE) professionals and foster supportive environments that promote children’s social–emotional competence and improve mental health and well-being. A key challenge to delivering ECMHC at scale is navigating complex multi-level factors to maximize successful implementation and program benefits at scale. The current study describes the implementation tensions arising during the first year of a pilot ECMHC program conducted in partnership across multiple agencies and a state’s department of education. In the 2021–2022 pilot year, ECMHC was offered as a free service to ECE programs in one large region of Virginia, with the goal of examining feasibility to scale statewide in future years. Consultation was implemented in 45 preschool classrooms across 30 programs. Implementation data were collected using consultation logs and participant surveys, and 20 participants (educators, families, program directors) participated in focus groups. Three implementation tensions are highlighted in this paper: (1) ideal plans versus reality of a new ECMHC roll-out; (2) how to support ECE professionals’ practice as it relates to children’s behavior, without contributing to a deficit view that children need to be “fixed;” and (3) systemic factors in the early childhood field that undermine the implementation and effectiveness of ECMHC. For each tension, we provide context from the larger literature on ECMHC, describe relevant decision points from Virginia’s pilot ECMHC program, and present implementation data to illustrate these tensions in practice. We conclude with reflections on lessons learned that have implications for other ECMHC and SEL intervention scale-up efforts.
1. Introduction
During early childhood, young children have countless experiences with early care and education (ECE) providers and families that contribute to children’s emerging social–emotional development, mental health, and well-being. Early childhood mental health is defined as “the developing capacity of the child from birth to 5 years old to form close and secure adult and peer relationships; experience, manage, and express a full range of emotions; and explore the environment and learn – all in the context of family, community, and culture” (Zero to Three, 2017). Children’s mental health, synonymous with social–emotional competence in early childhood, develops through their relationships with adults (Zeanah and Zeanah, 2019). Indeed, an emphasis on the importance of relationships between children and their adult caregivers is a distinguishing feature of mental health in early childhood from mental health in adolescence or adulthood (Zeanah and Zeanah, 2019). Social–emotional learning (SEL) programs and interventions seek to strengthen children’s abilities to form secure relationships, manage emotions, and engage in their learning environment (McClelland et al., 2017). One type of SEL intervention is early childhood mental health consultation (ECMHC). ECMHC is a targeted prevention service that builds the capacity of ECE professionals to interact with young children in ways that promote their social–emotional competence and improve their mental health and well-being.
Critically, Virginia, along with the entire United States and rest of the world, is facing an unprecedented health, social, and economic crisis with the COVID-19 pandemic. Even before COVID-19, many young children, particularly those from low-income families and communities of color, faced traumatic experiences that have had a significant impact on their social–emotional competence and mental health (National Scientific Council on the Developing Child, 2012; Bartlett and Smith, 2019; Shonkoff et al., 2021). Further amplifying these existing inequities, there are well-documented disparities in the rates of COVID-19 infection, illness, and death among communities of color due to inequities in social determinants of health such as discrimination, crowded housing, and access to health care (Center for Disease Control and Prevention, 2022). Further, low-wage workers are more likely to experience job loss due to the pandemic, resulting in greater economic hardship, food insecurity, and evictions (Center on Budget and Policy Priorities, 2020). Children are impacted even if they do not directly experience these traumatic events. For instance, the pandemic adds stress to families who may be trying to simultaneously parent and work from home. Young children’s daily routines have been upended and many had to adapt to remote learning for an extended period of time, which made it more difficult to form meaningful connections with their ECE providers1 and peers. In this current context, there is a great need for high-quality and effective services that promote young children’s social–emotional competence and mental health.
Early childhood education2 is a key setting in which to situate efforts to enhance children’s social–emotional competence and mental health as well as address and prevent any concerns in these areas from further progressing (Trigg and Keyes, 2019). Children spend a significant amount of time in ECE settings, and there is a long history of ECE programs supporting young children’s social–emotional competence and mental health through relationship building, classroom curricula, and programming (McClelland et al., 2017). For over a decade, the Center on the Social and Emotional Foundations of Early Learning (CSEFEL) has provided resources nationally to ECE programs that support providers’ implementation of the Pyramid Model for Promoting Social–Emotional Competence in Infants and Young Children framework (Hemmeter et al., 2006). However, addressing challenging behaviors in the classroom is still an area of stress for ECE providers (Friedman-Krauss et al., 2014; Clayback and Williford, 2022), and programs resort to exclusionary discipline such as suspensions and expulsions from early childhood programs and at inequitably higher rates for young Black boys (Albritton et al., 2019; Garro et al., 2021). Disproportionate use of exclusionary discipline with Black children is not explained by the level of disruptive behavior (Bradshaw et al., 2010), suggesting that racial bias may play a role (Gregory et al., 2017). Concerns about exclusionary discipline in early childhood and programs’ disproportionate use with Black children led the U.S. Department of Health and Human Services and the U.S. Department of Education to release a policy statement with recommendations for early childhood programs to promote children’s social–emotional competence and mental health and reduce exclusionary discipline (U.S. Department of Health and Human Services and Education, 2014). ECMHC was included as a recommended strategy in this policy statement and is increasingly being provided to early childhood teachers to support young children’s social–emotional competence and mental health.
ECMHC in ECE programs is a prevention-oriented service that aims to build the capacity of ECE providers and families to foster supportive environments that promote children’s social-emotional competence and mental health. Through a collaborative relationship, consultants with early childhood mental health expertise support ECE program staff, teachers, and families to prevent and address concerns related to children’s mental health and behavior (Cohen and Kaufmann, 2005). Some ECMHC programs have an explicit goal to prevent and reduce the practice of suspensions and expulsions from ECE programs (Conners Edge et al., 2021). Consultation activities that are implemented with ECE providers and families vary depending on the specific ECMHC model and whether the consultation is focused on addressing issues at the program- (supports the overall quality and climate of the program), classroom- (supports classroom systems and processes that shape children’s social–emotional development such as warm interactions, positive teacher-child relationships, and consistent routines), or child/family- (supports a child or family’s mental health and/or behavioral needs) level (Hunter et al., 2016). Despite this variation, most ECMHC approaches incorporate common components, such as a referral system, needs assessment, feedback to key stakeholders, and strategy implementation; however, there is still much to be learned about how best to roll out these ECMHC features, particularly when trying to scale up availability of these resources beyond a single classroom or program.
In fall 2020, state legislation3 in Virginia required that a workgroup composed of stakeholders in infant and early childhood mental health study the feasibility of adopting an ECMHC program to prevent suspensions and expulsions of young children attending ECE programs. Based on recommendations made by this workgroup, the Virginia Department of Education (VDOE) funded a university research center and a statewide early childhood service provider to develop, implement, and evaluate a birth-to-five pilot model of ECMHC in 2021–2022. Over the 2021–2022 pilot year, ECMHC services were delivered primarily in one large region of the state, but a key aim of the pilot was to understand and learn from implementation successes and barriers as the state considers a potential expansion of services state-wide. The ECMHC model was designed to serve providers of children birth-to-five in ECE settings, including child care centers, family day homes, Early Head Start and Head Start, and school-based ECE programs. Priority was given to programs that received public funds, but any program was eligible to receive services. Services were delivered to programs at no charge.
The goal of the current paper is to describe Virginia’s pilot ECMHC program during its first year of implementation, with a particular focus on grappling with tensions that arose in the implementation process. We highlight three tensions that illustrate competing needs and values that arose when designing and rolling out this new ECMHC program to serve ECE programs: (1) the tension between ideal and pragmatic roll-out; (2) the tension between supporting teachers’ practice as it relates to an individual child and contributing to a deficit view that children need to be “fixed”; and (3) the tension with addressing systemic factors impacting the ECE field that can undermine the implementation and effectiveness of ECMHC. For each tension, we provide context from the broader literature on ECMHC and describe the decision points that were made for Virginia’s pilot ECMHC program. We present relevant implementation data to illustrate these tensions in practice and then reflect on lessons learned that have implications for other ECMHC scale-up efforts.
2. Conceptual model of implementation
Implementation of ECMHC involves the amount or dosage of consultation that is delivered to ECE professionals, the quality of consultation, the extent to which consultation matches participants’ needs, and participants’ responsiveness to services (Durlak and DuPre, 2008). Implementation frameworks emphasize myriad factors that influence dosage, quality, alignment, and responsiveness. For example, Domitrovich et al. (2008) propose a conceptual framework for understanding implementation fidelity of school-based interventions. The authors define an intervention as a set of features or practices (referred to as core elements) linked to an intended outcome. In this model, effective implementation is bolstered by a “support system,” which may include pre-intervention training and ongoing coaching or consultation. This conceptual framework highlights multi-level factors that may influence implementation: (1) macro-level (e.g., federal, state, and local policies that impact schools; university partnerships; funding; leadership), (2) school-level (e.g., school policies; school and classroom climate; size), and (3) individual-level (e.g., educator professional and psychological characteristics; perception of the intervention). At all three levels of the model, these contextual factors are interdependent and influence quality of implementation and ultimately children’s outcomes.
Though this framework has predominantly been applied to K-12 settings, we use the model to understand implementation of the Virginia ECMHC model in ECE contexts. Early childhood contexts differ in important ways from older grades (Hindman and Bustamante, 2019), and thus the framework by Domitrovich et al. (2008) must be modified to apply. At the macro-level, factors influencing implementation of ECMHC include the broader system of early childhood, which is characterized by a multitude of structural and policy challenges. For example, compared to the K-12 system, the early education system is underfunded, and educators experience low wages (Whitebook et al., 2014), high stress and turnover (Schaack et al., 2020; Doromal et al., 2022), and report lacking adequate professional development (Gomez et al., 2015; Schaack et al., 2022). We refer to the school-level of the model as “program-level,” since many early childhood settings operate outside of a typical school system and include a variety of auspices (e.g., Head Start/Early Head Start, state-funded, private), each of which operates differently. At the program-level, many early childhood programs do not have protected planning time, in contrast to the K-12 system. As a result, ECE providers are forced to engage in professional development activities during other times such as nap time and before or after the school day (Fettig and Artman-Meeker, 2016). Education requirements and training opportunities are also more variable across programs in the ECE system compared to K-12. At the individual level, ECE providers need to be open to adopting new strategies or making shifts to their classroom practice to support children (Domitrovich et al., 2009; Cook et al., 2015; Domitrovich et al., 2019). Providers’ own mental health and beliefs may act as a barrier or facilitator to implementation. For example, teachers report that stress is a major barrier to implementation (McGoey et al., 2014), and teacher burnout is associated with lower implementation fidelity (Domitrovich et al., 2009). In ECE settings, provider mental health may be especially relevant for implementation, given the macro-level factors mentioned above. Understanding how implementation frameworks developed for the K-12 context apply to ECE settings is important when bringing any social–emotional learning program into early learning settings for young children. In the context of ECMHC, beliefs and biases may also influence engagement in consultation if providers attribute behavioral difficulties to the child or family rather than factors that the provider has some control over (Nemer et al., 2019). Racial bias may be particularly salient, given our focus on using ECMHC to reduce exclusionary discipline and specifically eliminate racial disparities in these practices (Davis et al., 2020).
A key challenge to delivering ECMHC at scale is navigating these interdependent multi-level factors to maximize successful implementation and program benefits at scale. The current paper describes implementation of the Virginia ECMHC pilot and raises critical tensions that relate to factors at the macro-, program-, and individual-levels.
3. Implementation of early childhood mental health consultation in Virginia
Team members from a university research center and a statewide early childhood service provider designed a birth-5 ECMHC model, in partnership with the VDOE, that aligned with recommendations from the state’s HJ51 workgroup report. Key components of the model include aligned infant/toddler and preschool services, an open referral system, and multi-tiered services based on identified needs. Though the Virginia ECMHC model is coordinated to ensure similar services are delivered across the entire birth-to-five continuum, this paper focuses explicitly on data stemming from services provided to preschool-aged classrooms and children.
3.1. Early childhood mental health consultation program components and procedures
Figure 1 displays Virginia’s birth-to-five ECMHC model. The first step to implement ECMHC services was to seek referrals for children and teachers who needed support. The Virginia ECMHC team developed flyers, videos, and other recruitment materials which were sent to program leaders, teachers, families, and communities through various channels. Those who were interested in requesting ECMHC services were asked to fill out an online referral form that included questions about the referral/request for services (e.g., name of program, locality, program type); contact information for follow-up (e.g., phone number or email of the person submitting the referral); and the reason for requesting/referring to services. Respondents were able to request consultation at the classroom level or more targeted support around one or a few individual children in a classroom. After a referral was received, teachers were asked to complete a teacher intake survey, and for child-specific referrals, families were asked to complete a family intake survey and family permission form. ECMHC services were not initiated until family permission was obtained. Families and teachers could elect to participate in services but decline that their data collected as part of the pilot be used for research purposes.
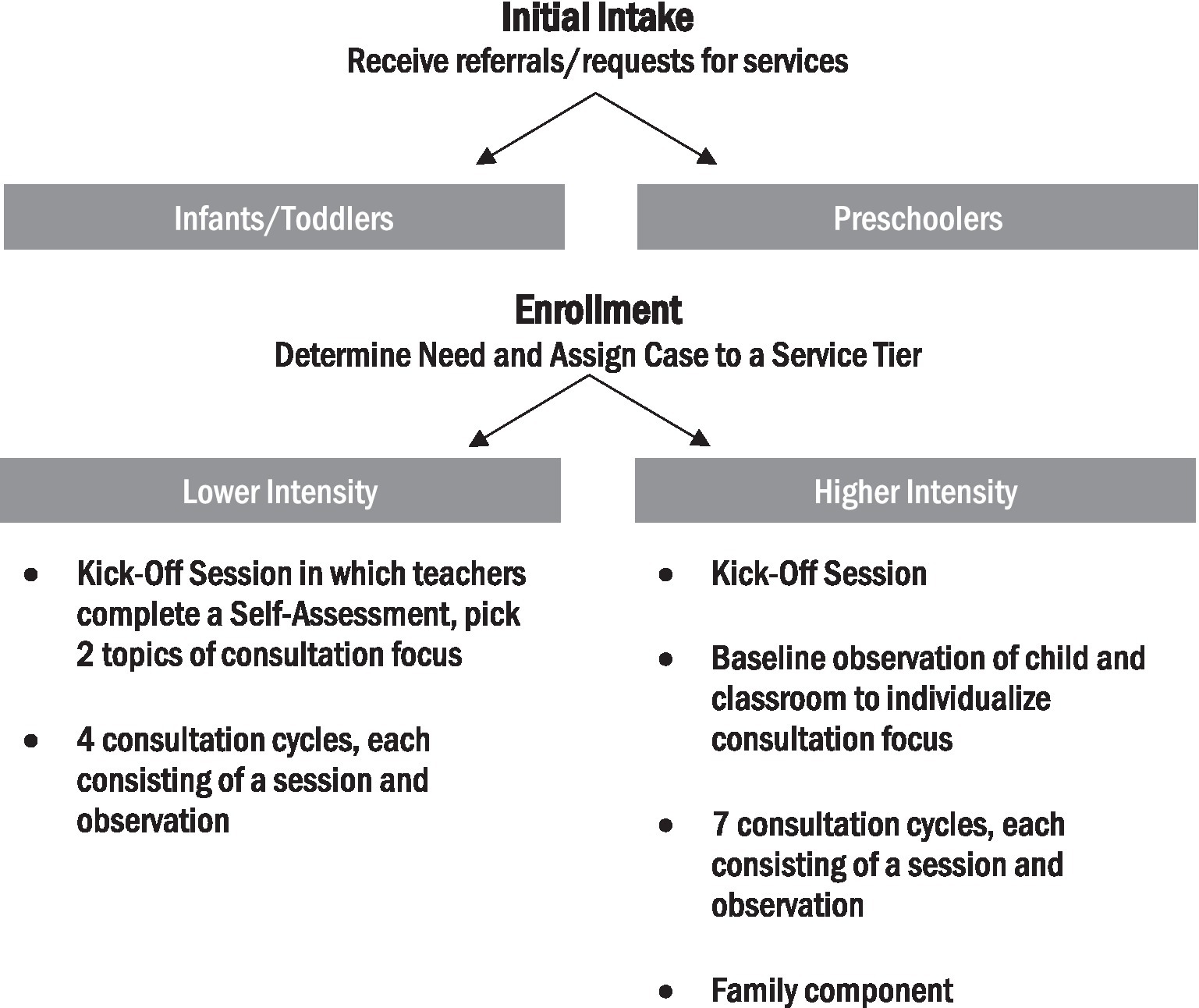
Figure 1. Birth-5 ECMHC model.
The service tier (i.e., higher intensity services versus lower intensity services) was determined based on identified needs. All classroom-wide referrals were assigned to the lower intensity service tier. For child-specific referrals, needs were assessed using two teacher-reported rating scales: the Preschool Expulsion Risk Measure (PERM; Gilliam and Reyes, 2018) and the Child Behavior Rating Scale (CBRS; Bronson et al., 1990). The PERM was the primary measure used to guide assignment to the service tier. In cases where PERM scores indicated substantial teacher frustration or risk of suspension/expulsion, the case was assigned to receive higher intensity services. Cases with low frustration or risk of suspension/expulsion were assigned to receive lower intensity services. The CBRS was used as a secondary measure in cases where the PERM score did not reach the research team’s high or low benchmark score.
The lower intensity tier begins with a kick-off session in which teachers complete a self-assessment to identify two social–emotional teaching topics on which they would like to enhance their practice. Next, teachers engage in consultation cycles around the two selected topics. Consultation cycles involve the creation of an action plan with the consultant, teacher implementation of the action plan (videotaped when possible), and the consultant providing feedback to the teacher after observing their implementation of the action plan. The intended dosage for the lower intensive tier is the kick-off session and four consultation cycles, with each cycle consisting of a session and observation. The higher intensity tier also begins with a kick-off session. After the kick-off session, the consultant conducts a baseline observation of the classroom environment using the Teaching Pyramid Observation Tool-Short Form (TPOT-S) based on the research edition in Hemmeter et al. (2014) and the referred child’s engagement in the classroom using the Individualized Classroom Assessment Scoring System (inCLASS; Downer et al., 2010), to gather key information to inform consultation. Consultation cycles follow the same format as the lower intensity tier, however, in the higher intensity tier, the strategies that are included in the action plan emerge from the consultant’s observation and discussion with the teacher. In the higher intensity tier, consultants also support teacher-family collaboration and facilitate referrals to community services, when needed. The intended dosage for the higher intensity tier is the kick-off session and seven consultation cycles, with each cycle consisting of a session and observation. ECMHC services were offered in-person and virtually; however, in some areas, in-person services were not possible due to the distance between consultants’ location and the program. Two full-time consultants and one part-time consultant were hired and trained by the university research center to serve preschool referrals.
3.2. Theory of change
The ECMHC model implemented with teachers and families of preschool-aged children (defined here as children 36–60 months of age) draws heavily from a previously developed ECMHC model called Learning to Objectively Observe Kids (LOOK). Downer et al. (2018) describes the LOOK model’s theory of change, core components, and initial evidence of its impact on teacher practices and preschool children’s outcomes. Central to LOOK’s theory of change is using guided video review to target ECE providers’ beliefs and classroom practice to enhance children’s social–emotional competence and mental health. Providers are asked to film themselves implementing evidence-based strategies with specific children whom the teacher perceives to display challenging behaviors. Consultants then select short video clips and write prompts that encourage providers to observe the child’s engagement in the classroom and analyze their role in creating a supportive environment for the child. The guided video review is intended to promote teachers’ understanding of the role of the classroom context for children’s ability to effectively engage with ECE providers, peers, and tasks, to move away from a perspective that the child is the problem. Additionally, the guided video review helps providers link their use of strategies to improvements in children’s engagement and behavior, thereby increasing providers’ perceived self-efficacy to successfully respond to instances of challenging behavior. The Virginia ECMHC model incorporated LOOK’s theory of change and use of guided video review to facilitate providers’ implementation of evidence-based strategies and reflection on their practice.
3.3. Data collection and methods
To understand implementation of the Virginia ECMHC pilot, data were collected from consultants, teachers, program directors, and families using qualitative and quantitative methods. Regarding quantitative methods, consultants entered their consultation data into a consultant log. The consultant log collected information on the dosage of meetings between consultants and providers and families, the topics of those meetings, the dosage of observations conducted, the format of meetings and observations, and whether the consultant made referrals to external agencies to supplement consultation. Providers completed surveys at the onset and conclusion of consultation. Before and after consultation, teachers reported on their self-efficacy using a modified self-efficacy scale from Bandura (1997), emotional exhaustion using two items based on Jeon et al. (2018), and knowledge of early childhood social–emotional development and effective teacher practice (practitioner-developed items used in the pilot). Teachers also reported on their use of SEL-related resources in their classroom at the beginning of consultation. Additionally, for child-specific referrals, teachers reported pre- and post-consultation on children’s self-regulation and social skills using the Child Behavior Rating Scale (Bronson et al., 1990), challenging behaviors using the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997), and expulsion risk using the Preschool Expulsion Risk Measure (PERM; Gilliam and Reyes, 2018). At the end of consultation, providers, families, and program directors were asked to respond to items asking about their experiences and satisfaction with the ECMHC pilot. Teacher and child sociodemographic data were collected via teacher and family surveys. Quantitative data that are presented in this paper include: sociodemographic characteristics; dosage of consultation; teacher-reported use of SEL-related resources; and teacher emotional exhaustion due to children’s behaviors pre-consultation (“I am emotionally exhausted by children’s behaviors,” rated on a 5-point scale from Strongly Disagree to Strongly Agree).
To gain a better understanding of the experiences of teachers, families, and program directors who engaged with the ECMHC program, we also employed qualitative research methods to hear the stories and lived experiences of our participants. We did this in two ways. First, we conducted one-on-one interviews with participants who chose not to participate in ECMHC or opted out after consultation began. Second, we held video-cued focus groups (Adair and Kurban, 2019; Tobin, 2019) with participants who had more sustained engagement with ECMHC. Participants were contacted via email or phone and invited to participate in the interview or focus group. A $50 e-gift card was offered to incentivize participation. Six program directors and one provider participated in an interview. Eight focus groups were held with a total of 10 teachers, six parents, and four program directors. Rates of participation were as follows: 7.5% for program director focus group, 10% for family focus group, 15% for teacher focus group, and 35% for interviews. At the beginning of each focus group, participants were shown 3 video clips of children in early childhood classrooms. Each video depicted scenes that would be considered relevant to discussions about children’s mental health, classroom behavioral expectations, and teachers’ projected roles within those contexts. We chose scenes depicting conflict between children, teachers teaching social–emotional skills, and children throwing objects, kicking, and hitting other children, since these were some of the common reasons children were referred for ECMHC services.
Interviews and video-cued focus groups were facilitated virtually over Zoom and were video recorded and transcribed with participants’ permission. The transcripts were first checked for accuracy before they went through several rounds of qualitative analysis. For this analysis, we used an inductive approach (Creswell and Poth, 2016; Miles et al., 2018). In the first round, a faculty member who led and participated in all the qualitative interviews and focus groups read through the transcripts and did open coding (Glaser, 2016) and identified thematic codes. In this round, some of the codes that emerged were communication issues, challenges with modalities of how services were offered (online vs. in-person), and lack of access to available resources for families. The researcher then used axial coding (Scott and Medaugh, 2017) to find interconnected thematic codes. This helped to connect interconnected categories. For instance, “challenges in communication with consultants” was connected to “challenges to uptake of services,” as well as “suggestions to improve services.” Similarly, “lack of adequately trained teachers” and “teachers leaving ECE” was connected to “systemic challenges faced by programs and families.” The data began to show three main interconnected themes: (1) challenges to uptake of ECMHC services, (2) systemic challenges faced by families and programs, and (3) suggestions to improve ECMHC services. Next, this researcher went through the data again and did selective coding (Williams and Moser, 2019) for the three emergent themes. Research team members who participated in the interviews and focus groups then worked together, in collaboration with the faculty member, to identify selective quotes that illustrated the emergent themes.
3.4. Overview of participants and implementation findings
During the 2021–2022 pilot year, the Virginia ECMHC pilot received referrals to provide mental health consultation to teachers in 89 preschool classrooms. These referrals were linked to 106 individual children, 94 teachers, 54 ECE programs, and 27 cities or counties across Virginia. Nearly half of the programs (48%) were child care centers.
Figure 2 displays a flowchart of ECMHC participants from the point of referral to services. Teachers in 51% of the 89 referred classrooms (n = 45) were served by the ECMHC pilot. Classroom attrition between receiving the referral and initiating services was primarily due to program or teacher unresponsiveness or not receiving family permission to provide child-specific services. Table 1 reports data on ECMHC implementation. Of the 89 referred classrooms, 88.8% requested consultation that supported the teacher to address a specific child’s challenging behaviors, while 11.2% of classrooms requested classroom-wide support. Among the 45 classrooms that were served by the ECMHC pilot, 57.8% were assigned to receive the higher intensity services, while 35.6% received lower intensity services. A small number of classrooms did not have a service tier assigned because of incomplete rating scales. All 45 classrooms that were served had teachers who participated in a teacher kick-off meeting. However, only 14 teachers participated in at least one consultation session (M = 2.14 sessions, SD = 0.95, range = 1–4) and 6 teachers received at least one observation (M = 1.67, SD = 1.63, range = 1–5). Reasons for the drop-off in services from the kick-off to consultation sessions were complex, and we were not able to capture through systematic quantitative data collection; however, qualitative data described later in section 4 of this paper offer some insight into the low uptake of services.
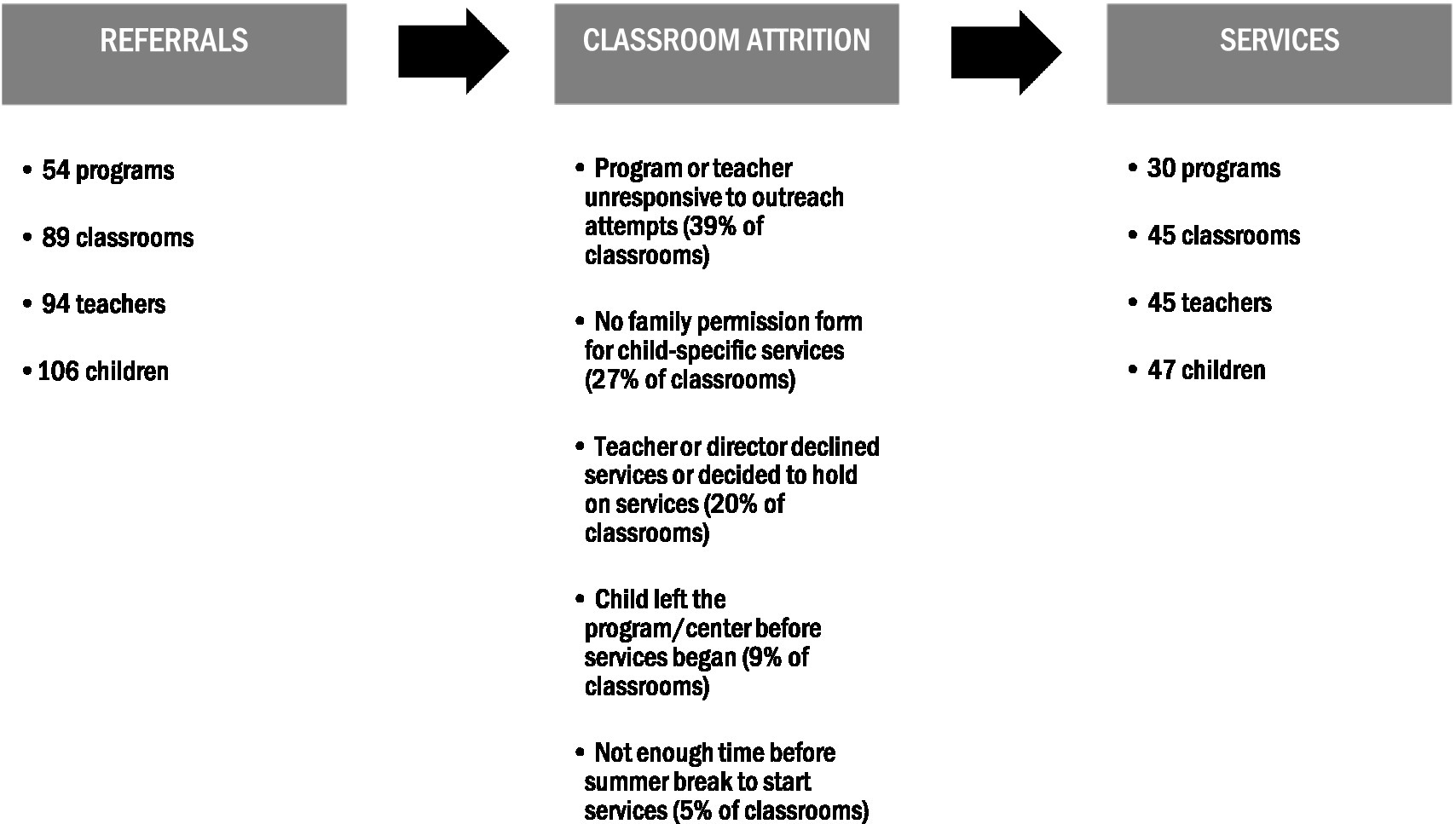
Figure 2. Flowchart from ECMHC referrals to services.
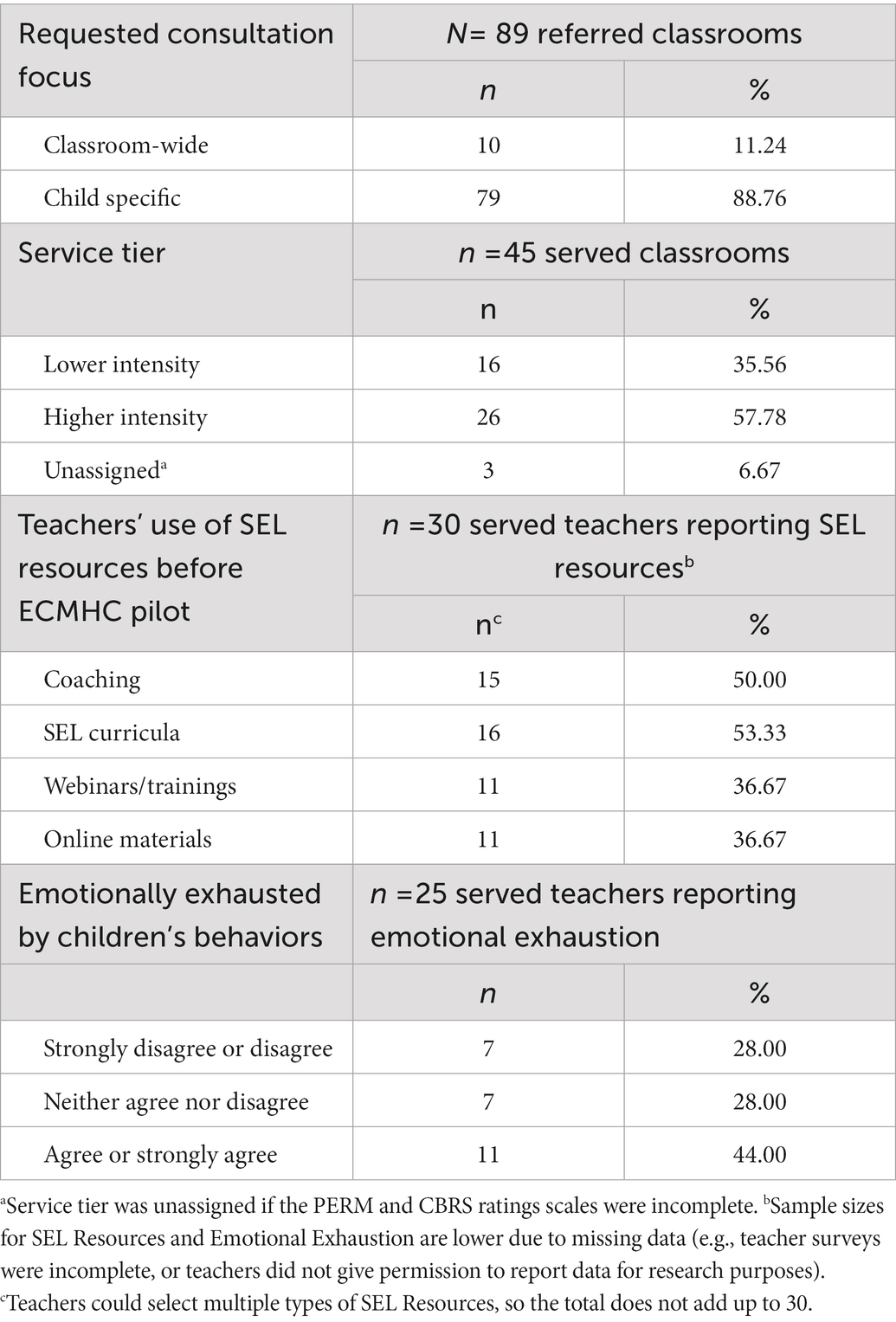
Table 1. ECMHC pilot implementation.
Table 2 reports information about children who were served by the ECMHC pilot. A total of 47 preschool-age children were served by the ECMHC pilot, and demographic data were available for 32 of them (68%). Among these children, 63% were boys (n = 20) and 37% were girls (n = 12). The racial/ethnic composition of children was: 38% Black (n = 12), 47% White (n = 15), 9% Multiracial (n = 3), and 6% Latino (n = 2). Families reported that the majority of children spoke English at home (97%; n = 31) and some spoke Spanish (13%; n = 4). On average, children were 4 years old (M = 4.11, SD = 0.64). A small number of children had an Individualized Education Plan (9%; n = 3). Missing child data are due to not receiving a family intake survey or not having permission to report data for research purposes.
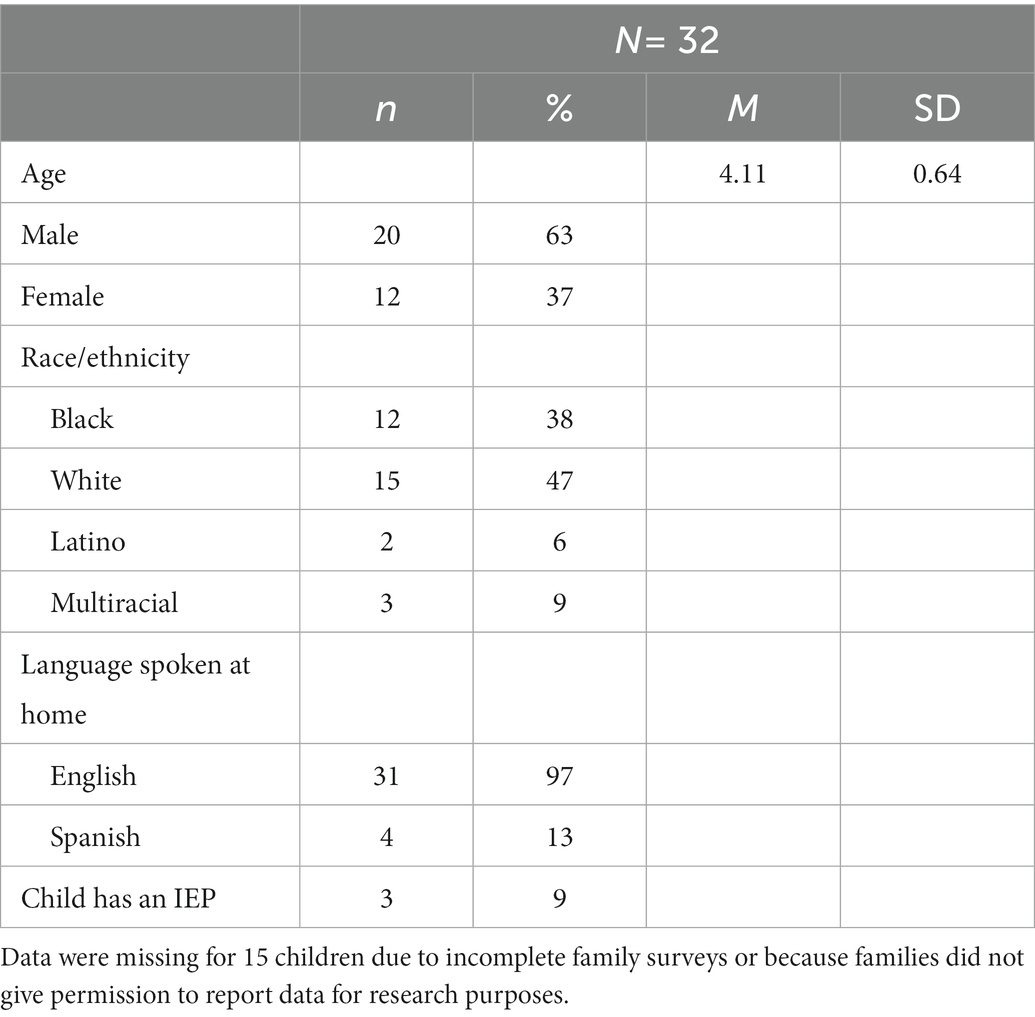
Table 2. Served children’s socio-demographic characteristics.
Table 3 reports information about the educators who were served by the ECMHC pilot. A total of 45 preschool teachers were served by the ECMHC pilot, and sociodemographic data were available for 22 (49%). Of these, all identified as female. The racial/ethnic composition was: 73% White (n = 16), 23% Black (n = 5), and 5% Other race/ethnicity (n = 1). On average, teachers had 16 years of experiences (M = 15.77, SD = 10.06), and 81% had at least a Bachelor’s degree (n = 17). Missing teacher data are due to not receiving a teacher intake survey or not having permission to report data for research purposes.
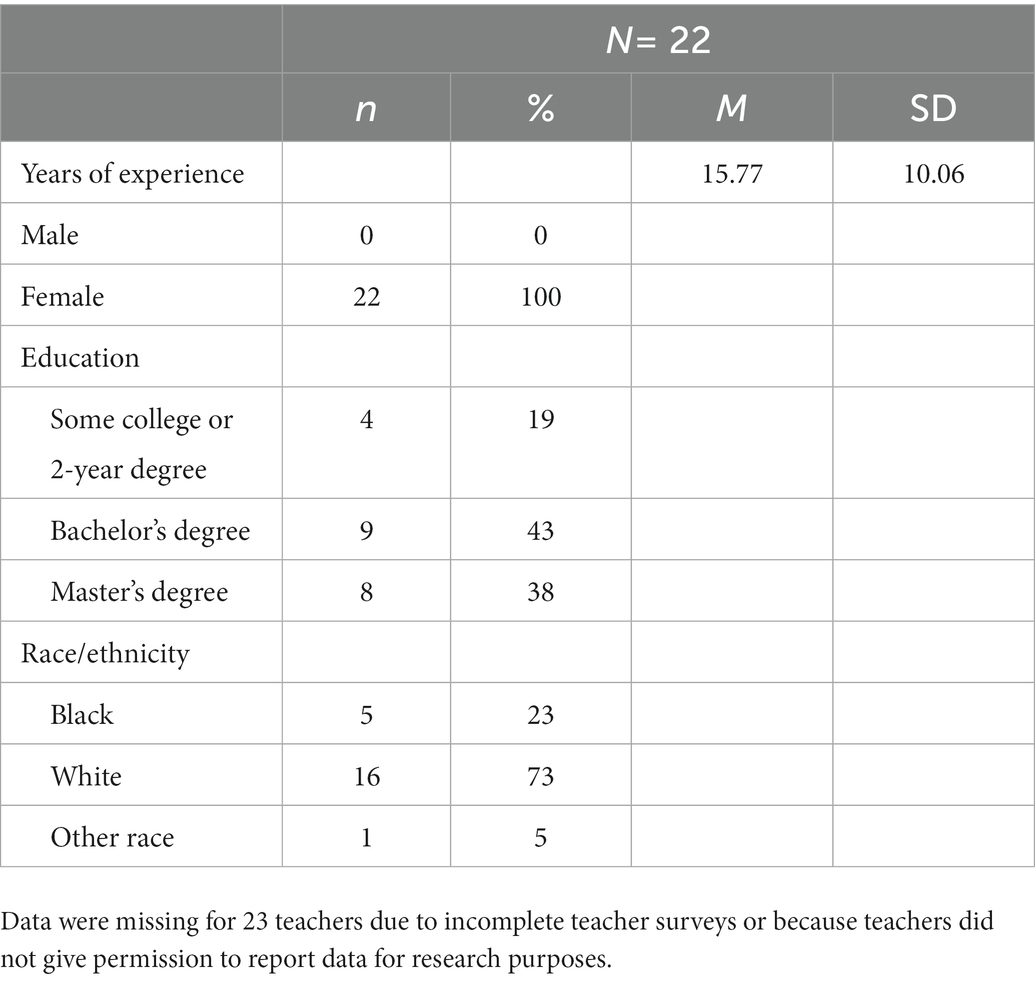
Table 3. Served educators’ socio-demographic characteristics.
4. Tensions that arose in context of the Virginia early childhood mental health consultation pilot’s implementation
The Virginia ECMHC model launched in a single, large community in the state with the goal of closely monitoring implementation to understand how making this new service available to all publicly funded ECE providers would be received, during a time when COVID-19 disruptions continued to place stress on local ECE programs. This emphasis on feasibility and uptake was of particular importance given growing evidence that social–emotional supports in ECE programs are only helpful when implemented consistently and well (Hemmeter et al., 2022).
In seeking to understand the first year of the Virginia ECMHC pilot, from developing the model and delivering services, we identified critical tensions in implementing social–emotional and mental health services in early childhood settings at scale. The tensions we lay out are ones we grappled with throughout the pilot; our goal is not to provide answers, but to discuss these topics and their implications for ECMHC scale-up efforts (and more generally for SEL programming in ECE). Three key tensions are outlined in the following sub-sections: (1) the tension between ideal and pragmatic roll-out; (2) the tension between supporting teachers’ practice as it relates to an individual child and contributing to a deficit view that children need to be “fixed”; and (3) the tension with addressing systemic factors impacting the ECE field that can undermine the implementation and effectiveness of ECMHC. For each tension, we describe relevant literature and present implementation data from the Virginia ECMHC pilot that illustrates how the tension arose in our pilot.
4.1. The tension between ideal and pragmatic roll-out
Tensions related to what is ideal and what is realistic and feasible at scale arose frequently during the implementation of the ECMHC pilot. Our pilot included various stakeholders including educators, families, policymakers, and researchers whom, at times, held different perspectives on what ideal ECMHC implementation looks like. We describe how we grappled with three specific issues around what is ideal versus pragmatic: (1) consultant workforce and qualifications; (2) access to consultation; and (3) systems of support. Decisions related to these tensions were guided by our ongoing partnership with the VDOE and their requests to prioritize consultation for the highest need cases, specifically where a child was at risk of being suspended or expelled.
4.1.1. Consultant workforce and qualifications
In some areas of the United States, finding a candidate who fits the standard job requirements of an IECMH consultant is difficult or almost impossible. The reality is that there are mental health professional deserts, and hiring teams may need to be flexible and discerning when hiring. – Center of Excellence Hiring Guidance.4
The Center of Excellence for Infant and Early Mental Health Consultation recommends the following minimum qualifications for consultants: Master’s degree in social work, psychology, or related field (preferably licensed); at least 2–3 years of experience working as a mental health professional; possess attributes and skills critical to this work (e.g., facilitates consultative stance, culturally sensitive, and empathetic); have specialized knowledge and deep understanding of early childhood development and social, emotional, and relational health. These highly qualified consultants would deliver promotion, prevention, and intervention services to programs, teachers, and children/families, depending on need.
However, these ideal qualifications bump up against reality that the current ECMHC workforce is small and requiring this amount of training is long and costly. At this time, Virginia does not have a large workforce from which to recruit. Further, using licensed mental health professionals as consultants for the full spectrum of services (from promotion and prevention to intervention) takes an already small workforce away from providing other services, such as direct mental health services to children and families. This unintended consequence may contribute to long wait times for those most in need of intensive, targeted support. In addition, given that ECMHC was being provided within classroom and family day home settings, we deemed prior experience within ECE as critical. We addressed this tension by requiring the following key qualifications for consultants: a Bachelor’s degree in psychology, counseling, social work, education, or a related field; a minimum of 2 years of relevant experience, including work in an early childhood environment; and experience with consultation and/or coaching educators. Our qualifications favored certain experiences we deemed critical for consultants who would be working in ECE settings (e.g., experience in early childhood classrooms) and implemented a robust system of initial and ongoing training and support. We did not consider this to be a ‘less than’ approach in relation to Center for Excellence standards, but rather an intentional adaptation that worked for implementing ECMHC in this state and region at this moment in time.
4.1.2. Access to consultation
...I think we stopped utilizing the service because the only thing available to us was virtual…I need someone [an ECMHC consultant] physically to be able to come in and support these teachers. – Joanna5, Program Director.
Another tension between the ideal and the real is related to access to consultation. Ideally, all programs and educators would have access to some type of mental health consultation. Consultants embedded within programs (i.e., internal consultants) may provide better services, since they are able to form strong relationships with educators and families, prior to challenges occurring. Embedded consultants have time to get to know the program climate and culture, including strengths and challenges, and can proactively support teachers, rather than reacting once a child is on the brink of expulsion or a teacher is burnt out. However, as described above, funding and workforce challenges result in difficulty providing highly trained consultants to work intensively in every program. This implementation challenge meant that we needed to allocate resources strategically.
Under realistic conditions of limited resources, we used external consultants (rather than internal consultants) and assigned consultation based on level of need in our ECMHC pilot. External consultants typically are only present in the classroom or program when providing services, compared to internal consultants who already work in a program (Giordano et al., 2020). Though external consultants are commonly used, external consultants may not be fully aware of the existing program, community, and cultural contexts, especially at the beginning of consultation, and this can lead to difficulty establishing trust and strong relationships (Giordano et al., 2020). Scheduling consultation activities, such as meetings and observations, is also more difficult for external consultants, compared to consultants who are internally embedded within a program.
We also experienced tensions related to access to different formats for consultation. For our pilot, ECMHC services were offered both in-person and virtually. We used exclusively virtual consultation in some areas to allow consultants to provide services within a wider geographical range. Though we anticipated that virtual consultation would help us reach more programs, our data showed that the teachers and directors preferred services to be delivered in-person as opposed to virtually. Program directors who chose not to take up the ECMHC services told us that one main reason was because only the virtual option was available to them, which they did not see as beneficial. Program directors and teachers shared that teachers were already spending significant amounts of time on screens and another virtual service would have added to “screen fatigue.” In the focus groups, teachers who had participated in the ECMHC program shared that they would have liked the consultation and observations to be in-person.
4.1.3. Systems of support
I really wish I had mental health services in my school more than just the social worker…who could…step in and get a kid serious services without waiting…There’s so many barriers…my two kids that I had last year…never got the services that they needed. – Sarah, Teacher.
The most effective implementation happens within a system of support (Domitrovich et al., 2008). In the case of early childhood, this system of support also includes coordination across providers of different early childhood services, such as primary care, speech and occupational therapy, mental and behavioral health, and early intervention. Unfortunately, our early childhood system is fragmented, resulting in families navigating separate systems for each necessary support. This theme came up consistently during focus groups with families and teachers who participated in the pilot.
Prior to reaching the level of intensive intervention like ECMHC, systems should ideally be set up to universally promote social and emotional development and prevent challenges in the classroom. These universal supports include access to high quality comprehensive curricula, as well as training and classroom resources to support children’s social and emotional development classroom wide. Fifty percent of teachers who were served by the ECMHC pilot reported having had some prior experience being coached on practices that support children’s social-emotional learning, 53% of teachers reported using a social-emotional curricula, 37% reported accessing webinars and trainings, and 37% reported using online materials (see Table 1). While it is encouraging that half of teachers had received coaching prior to ECMHC, these universal supports for teachers are still not widely implemented in a coordinated and aligned system. The result can be overly relying on targeted and intensive support once challenges occur. Yet, these targeted and specialized interventions are more costly and time intensive and contribute to the next tension—perceptions that a child’s struggles in the classroom represent a deficit in that child and their family, rather than a product of resources available to them in their environment.
4.2. The tension between supporting teachers’ practice as it relates to an individual child and contributing to a deficit view that children need to be “fixed”
Yeah, I think, and the other piece of that, of his behavior you know, mom to a Black boy, and he has behaviors that there are negative associations with, particularly for Black boys. When you hear him being described as, “aggressive,” or you know, “violent,” and stuff like that, when it’s, like, that’s not how he is. The folks who are working with him, and when they talk about him. The lady who works with him now, like, I almost was brought to tears when she first started talking about her experience with Khalil, because she was talking about how smart he is. You know, how he likes to learn. I mean, just, like, all of the strengths that Khalil possesses, where usually what I hear is, he’s hyper, impulsive, you know, those are the things that you first see with Khalil. But after you get to know him, and get to understand him, then you get to see all those things. But the reality is that the world is going to immediately see him as a Black boy who may be acting in a way that’s been labeled as aggressive. Particularly, he has now a diagnosis of ADHD. And where the developmental pediatrician really talked about that from a neurodevelopmental perspective. But even in my line of work, ADHD is not something that... I mean, people kinda laugh at that diagnosis a lot of time. Like, it’s an excuse for why kids behave the way that they do, but when you have a better understanding of it, I mean, you almost are like... People have more of an understanding or sympathy or understanding if he, if he had an autism... diagnosis, than the ADHD. But he has so many of the autism features, but that is not the primary diagnosis that he has. You know, I hate to say that, but I... that’s just kind of the reality. And I, I want to get him into the school system early so that he’s not really known for his behaviors and that they really get a chance to really understand him better because I know how those behaviors are labeled. And they do that for all kids, but the reality is, it is a different experience for little Black boys in particular. Where he can be acting out, and somebody thinks he’s being aggressive and feel threatened by him. And so I’m trying to help him with that because I know what that can lead to later on. – Kacia, Mother.
The excerpt above is taken from a focus group discussion that we had with mothers of children who had been referred for ECMHC services. Kacia is a Black woman who described her experience of raising a Black boy who seemingly had behavioral challenges and was diagnosed to have Attention-Deficit/Hyperactivity Disorder (ADHD). She shared her worries around labels that get attached to children, especially Black boys. For young Black boys, their behaviors are often tagged with negative associations, such as “violent” or “aggressive.” Black parents are aware of teachers’ perceptions of their child’s behavior and the different experiences of Black youth in the classroom. Like many other parents, Kacia became an advocate for her child, an expert, who sees the many strengths of her child and not how the world views her Black child and automatically labels his externalizing behaviors as “aggressive.” It is interesting to note how Kacia described that an autism diagnosis was preferable over a diagnosis of ADHD. Kacia was a social worker and told us that she “knew the system” and even in her “line of work” she had experienced people lacking trust in an ADHD diagnosis.
The goal of the Virginia ECMHC pilot was to support ECE teachers in responding to the social–emotional and mental health needs of the children in their classrooms in the wake of the pandemic. As part of this goal, VDOE was especially interested in reducing and preventing suspensions and expulsions of young children attending ECE programs in Virginia. As a team, we were driven by the belief that behavioral difficulties did not lie with the children but often with the systems around them. Our work was also grounded in the realities of how race plays a role in the way young children and their families are perceived and treated in ECE programs.
In this section, we detail the tension that we experienced as we implemented the ECMHC services and collected and analyzed data. Despite our best intentions to move away from the idea of “fixing children,” and focusing on “fixing contexts,” we felt that we still centered the child, and possibly cast them in deficit ways. This happened in two ways: (1) Centering deficit views of children by seeking child referrals and (2) Referrals reinforcing systemic ways in which BIPOC children are over identified as having behavioral challenges.
4.2.1. Centering deficit views of children by seeking child referrals
ECMHC services were marketed to address teacher mental health concerns, classroom climate, teacher-child interactions, as well as child-specific behavior concerns. The referral form included a question about the reason for requesting services that was deliberately kept open ended, because we did not want to assign labels to the child or teacher. We wanted the family, teacher, or program leader who was requesting the referral to describe behaviors or challenges in their own words, rather than have them check boxes of pre-determined categories. Because consultation did not have to focus on a specific child, the intake form did not require that respondents list an individual child as the intended focus of consultation. However, nearly all classrooms requested support around addressing a specific child’s challenging behavior (see Table 1). Although we deliberately tried to not take a deficit view of the child or their family, as we reflected on our work over the past year, we felt a tension with the mere act of seeking child-specific referrals. Even in the context of an open-ended prompt, the question around the reason for referral provided examples of ways in which a particular child was “behaving” or showing that they had “unmet needs.” We ultimately received descriptors in the referrals such as “hitting others,” “defying authority,” “stealing toys,” “disturbing others during naptime,” and “refusing to follow classroom routines.” As we can see from these examples, these responses described how the child was not fitting well into the context rather than how the context was making it difficult for the child. Further, some teachers that we interviewed—those who utilized the services and those who chose not to—mentioned that they were expecting the ECMHC services to “work with the child directly,” instead of working with teachers and families to enhance the contexts that are possibly not working for the child.
Here we are struggling with the tension of wanting to provide services in cases where specific children were having a difficult time in the classroom and the teacher could use support in re-framing and supporting the child’s behavior while also contending with the possibility that the mere act of seeking referrals to implement a consultation program tends to reinforce deficit-based ideas about children and their families. However, to even begin a consultation process rooted in antiracist practices, where we try to help teachers to see the strengths of a child that they see as a problem or to recognize the funds of knowledge (González et al., 2006) that a family has, the starting point has to be the child and their behavior.
4.2.2. Referrals reinforced systemic ways in which BIPOC children are over identified as having behavioral challenges
A second tension we grappled with related to inadvertently contributing to deficit views of children is over identifying BIPOC children as exhibiting behavioral and mental health challenges. Young BIPOC children often attend early education spaces that are more tightly controlled than spaces White children attend (Adair et al., 2018), and their bodies and behaviors are heavily regulated (Hines-Datiri and Carter Andrews, 2020). BIPOC children’s behaviors are then mislabeled and misinterpreted as problems, issues, or misbehaviors (Gregory et al., 2017). These labels can lead to disparities in the disciplinary experiences of BIPOC and White children (Gregory et al., 2010; Skiba et al., 2011; Losen and Gillespie, 2012; U.S. Department of Education Office for Civil Rights, 2016; Epstein et al., 2017; Boonstra, 2021).
In Virginia’s ECMHC pilot, 41% of children who were referred for services identified as Black and 40% identified as White. Using the American Community Survey 5-year estimates from 2016 to 2020, we calculated an estimate of the racial/ethnic breakdown of children under 17 years for the top five cities and counties from which ECMHC referrals were made. On average, across these localities, the larger population of children was 50% White and 23% Black. As another point of comparison, the statewide sample of preschool children for whom the state had school readiness data was 35% White and 32% Black (Virginia Department of Education and the Center for Advanced Study of Teaching and Learning, University of Virginia, 2022). Comparing our referrals to these estimates, it is likely that Black children were over-identified for ECMHC services; however, we cannot definitively make this conclusion, since we do not have detailed information on race/ethnicity in classrooms served by ECMHC.
Previous studies have suggested that Black families are worried about the stigmas associated with ADHD diagnoses or other behavioral or learning disabilities due to their child being labeled as “crazy” or needing medication to make their child “behave” (Davison and Ford, 2001). Families of BIPOC children are left in limbo, and it is up to the ECE program to accurately accommodate their child and not subject them to the stigmas and stereotypes that come from labels that provide relief to White families as it explains their child’s behavior (Davison and Ford, 2001). When Kacia expressed preferring an autism diagnosis over an ADHD diagnosis for her son, she was falling back on her experience and trying to ensure the best possible outcome for her son. Kacia knows that her son, due to him presenting as Black, would be viewed more negatively with an ADHD diagnosis than an autism diagnosis. She was trying to minimize the damage that these labels do by hoping for a diagnosis that minimizes the deficit view of her child.
These deficit views about BIPOC children get extended to their families too. The parents that we interviewed shared that they were working hard to support their children in school and at home. Like Kacia, we heard stories of parents advocating for their children while they confronted their own challenges concerning workload and income, especially in the aftermath of COVID. However, teachers sometimes expressed deficit views of families, saying that parents were “in denial” about their children’s needs, were not parenting in the right way, or were unable to comprehend their children’s needs. Parents felt they were labeled as uninvolved without consideration for the strides they take to support their children (Devlieghere et al., 2020).
Like families, ECE providers are also working to overcome incredible challenges to ensure the best outcomes for children in their care. What may be perceived by families as a provider pushing a diagnosis on their children might be explained by the provider as efforts to make resources and supports available for the child. Although ECE providers report being both devoted to and rewarded by their work, systemic issues exert real influence on teachers’ stress and well-being which can undermine their responsiveness to children and families. Next, we discuss these systemic issues in the ECE field and how they relate to ECMHC implementation.
4.3. The tension with addressing systemic factors impacting the early care and education field that can undermine the implementation and effectiveness of early childhood mental health consultation
And I, I know, like as an outsider or a professional, and I feel like you, you know the long-term solutions, what needs to happen, but like just with like children and learning, if their basic needs aren’t met, they cannot be there and be present to learn it. I think that’s where teachers were at. They were in crisis. It was fight or flight in that stem of their brain. They were not in a place to learn or work towards a long-term solution. – Tammy, Program Director.
ECMHC focuses on working with adults to better understand and respond to behavior in context, and thus requires the capacity to learn, engage with, and apply new information to make changes in practice. A model of ECMHC that targets the child’s environment (versus a deficit view that sees the child as the point of intervention) requires additional responsibilities and time commitments from adults in the child’s ecosystem. However, the same challenges that might lead a teacher or program to seek out ECMHC (e.g., educator stress, educator lack of self-efficacy, lack of resources, lack of work-time supports, students/families experiencing mental health challenges) may also act as barriers that interfere with access to and engagement with this model of consultation. This tension illustrates the need among ECE teachers for resources and support, but the foundation for receiving them is not always there, analogous to pouring water into a bucket with a hole in the bottom. Patching this hole (i.e., addressing systemic issues in the ECE field at the macro level) is necessary for supports and services like ECMHC, and other SEL programming in ECE settings, to be effective at scale. As previously noted, the dosage of ECMHC that providers received was below the intended dosage of the model. While we expected teachers to participate in 4–7 consultation cycles, depending on the service tier, the average number of sessions was 2.14 (range 1–4) and the average number of observations was 1.67 (range 1–5). We discuss three systemic issues that impact ECE providers’ work and undermined teachers’ engagement with and dosage of ECMHC: (1) turnover, coverage, and workload; (2) provider stress, mental health, and well-being; and (3) compensation for ECE providers. Although these systemic issues were exacerbated by the COVID-19 pandemic, they were already impacting the ECE system; thus, it is important to understand and address these issues well beyond the pandemic when considering implementation of ECMHC and other SEL programs.
4.3.1. Turnover, coverage, and workload
Our teachers, as you know, everywhere with teaching, teachers are like burnt out. They feel like there’s so much on their plate. And when they got down into this, it seemed like a lot more work on a teacher, and they just were not willing to take it on. It seems like a lot of training and things that they had to do and not the support that they were looking for. So that’s why a lot of my teachers were like, “No, I’m not doing that [ECMHC] now.” – Tammy, Program Director.
Focus group and exit interview participants often expressed the sentiment that early childhood educators are at capacity. Turnover and coverage challenges resulted in high workloads and increased stress, which made taking on ECMHC services untenable for teachers in many programs. Teachers and leaders who remained at their programs have dealt with the fallout of high turnover rates during the pandemic (Quinones et al., 2021; Berger et al., 2022). Teachers who remained at their program were caught in a cycle in which turnover and lack of coverage led to a higher workload:
Um, and then, yeah, that was a huge part of it, because you have the teachers who do show up, who were dedicated and loyal to come into work every day, that are working overtime to make up for the lack of teachers that we have. – Liz, Program Director.
Challenges associated with turnover including lack of coverage, overworked staff, inconsistencies in staffing within classrooms, and higher workloads for teachers lead to a lack of time and bandwidth for program staff to complete basic tasks and responsibilities. Early educators already complete many job demands without proper supports, such as paid planning time, adequate staffing, and training (Jeon et al., 2018; Jeon and Wells, 2018; Roberts et al., 2019; Kwon et al., 2022). Within the Virginia ECMHC pilot, programs were experiencing similar challenges that acted as barriers to engagement. Leaders mentioned that they were looking for support without placing additional demands on their teachers, who often need to complete work responsibilities outside of compensated hours. Teachers also declined ECMHC services due to a lack of capacity to engage:
I have no planning time [already]. I do not have time to get another resource [ECMHC services]. – Mandy, Teacher.
Early childhood educators have shown resilience and creativity in their work to support children and families at the same time they have been experiencing high levels of stress, turnover, and financial insecurity (Beltman et al., 2020; Crawford et al., 2021; Eadie et al., 2021; Swigonski et al., 2021). However, the time, resources, and capacity for consistently engaging with consultation (e.g., attending meetings, uploading videos for review, implementing practices and reflecting on them) were not available to all educators and programs. Unfortunately, this likely leads to situations where programs with less resources are in greater need of consultation but have less bandwidth to engage. Additionally, if early educators had more time and resources at their disposal, they may have been more receptive to a model of ECMHC that targets changes to the classroom environment and their practice, rather than a frequently expressed sentiment that many educators wanted someone to pull out or work directly with the child.
4.3.2. Provider stress, mental health, and well-being
So I do know the importance of, um, supporting the teachers, not just with interventions and strategies to help children in the classroom, but dealing with, you know, their own baggage that makes, um, when you come in the classroom and you are already burnt out and tired, then it’s hard to build a relationship with a student that is causing you more stress. And then that in itself causes teachers to make decisions that may not always be the best decision because you are doing it from frustration or because you are tired or you are already stressed and burnt out. – Laura, Program Director.
Larger systems contribute to stress and mental health of adults, shaping the care they provide to children as well as their perceptions of and responses to children’s behavior (Buettner et al., 2016; Jeon et al., 2019; Zinsser et al., 2019). ECE providers experience higher levels of stress, depressive symptoms, and burnout than the general population (Jeon et al., 2018; Jeon and Wells, 2018; Roberts et al., 2019; Kwon et al., 2022). ECE providers also report increased rates of stress, anxiety, anger, frustration, sleeping problems, and physical pain since the start of the pandemic (Berger et al., 2022; Farewell et al., 2022). Program directors, who play a critical role in supporting teacher engagement with ECMHC, including prioritization of consultation, scheduling coverage for consultation meetings and shaping policies and philosophies around interpreting and responding to behavior, also report high levels of stress that interfere with their ability to focus on educators’ well-being and professional development (Kristiansen et al., 2021).
A desired outcome of ECMHC is to enhance teachers’ ability to respond effectively to behaviors they perceive as challenging and to meet young children’s social and emotional needs, which is one of the most commonly reported stressors for early educators (Hoover et al., 2012; Reyes et al., 2021). Nearly half (44%) of teachers served in the Virginia ECMHC pilot reported that they were emotionally exhausted by children’s behaviors (see Table 1). Though the intent is to alleviate a source of stress for educators, ECMHC can add more burden or stress, particularly for educators who might be struggling to manage their own mental health needs. The Virginia ECMHC model worked from a framework of understanding behavior in context, so some educators were learning a new way of understanding and interpreting children’s behavior while unlearning implicit biases and child-focused behavioral attributions. This learning and reflection requires personal work that can bring up difficult emotions at a time when teachers already feel targeted:
I feel like teachers are being targeted a lot right now and they feel like everyone’s telling them how to do their job better- just feeling very criticized about a lot. So I think- if somebody was meeting them where they are and, you know, kind of modeling the, that support- would help them to say like, “Oh, okay. Yeah, that could really help.” They just want to be heard about what’s going on in their classroom. And that’s a tough thing for a teacher. Like those are their four, four walls. That’s the one area in the school they can control, so letting somebody into that is difficult, and especially via video camera. – Tammy, Program Director.
4.3.3. Compensation for early care and education providers
We have staff that’s like, in order for us to come to work, we need you to pay our gas. We need for you to give us the gas money because we just cannot afford it. Uh, so we, coming up with how we are gonna help staff get back and forth to work because gas prices went up. Um, I cannot increase your salary, but I can maybe do a gas voucher. Um, but the ins and outs of doing that is the paperwork for it is just ridiculous. And, when you have over almost 100 staff and maybe 75% of them need assistance with traveling to work, that paperwork is intense. So, it’s like, do we help? – Whitney, Program Director.
In addition to the heightened workload and stress that ECE providers are facing in the aftermath of the pandemic, many providers are struggling financially to meet their own and their family’s basic needs due to disgracefully low compensation. In Virginia, median pay for ECE providers is $10.96 per hour, and 16.4% of providers live below the poverty line, twice the rate of workers in the state overall (McLean et al., 2021). Working during the pandemic, in many cases without health care or benefits such as paid sick leave, has placed additional financial and emotional stress on providers (Markowitz and Bassok, 2022). Low compensation relates to the other two systemic topics previously discussed. Financial insecurity leads to higher stress levels, turnover, and higher workload among remaining teachers.
Despite ECMHC being implemented at the child/family, classroom, or program level, this work cannot be separated from larger systemic forces that impact day-to-day functioning of educators, children, and families. Understanding and addressing systemic issues in the early childhood field (e.g., turnover, workload, stress, mental health, and compensation) will resolve some of the mental health and social–emotional challenges ECMHC targets, while also creating a stronger infrastructure for providing more effective support and implementing SEL interventions when needed. Therefore, we see part of our role as researchers being connected to social justice and advocating for systemic changes that would improve the lives of children, families, and early educators, while also helping us be effective in our role of developing, studying, and understanding supports. Understanding the larger context and the interconnected factors that shape educator, family, and child experiences is essential in approaching ECMHC, and other SEL programming in ECE, from a strengths-based, ecological systems orientation and promoting sustained change at scale.
5. Conclusion
ECMHC is a targeted prevention SEL service intended to build the capacity of ECE professionals to promote children’s social-emotional competence and improve their mental health and well-being. In this paper, we described tensions that illustrate competing needs and values that arose when designing and rolling out Virginia’s pilot ECMHC program during its first year of implementation. We categorized our tensions into three areas: (1) ideal versus pragmatic roll-out; (2) the potential to contribute to a deficit model where children are viewed as needing to be “fixed”; and (3) the systemic factors impacting the ECE field that undermine the implementation and effectiveness of ECMHC. For each tension, we presented a combination of qualitative and quantitative data to illustrate how these tensions played out for the children and providers we intended to serve through ECMHC.
We described these major tensions within the context of implementing a particular social–emotional learning program – ECMHC. However, the tensions arising from the practicality of implementing at scale, programming that may contribute to a deficit model of children who need to be “fixed,” and systemic barriers that prevent or reduce successful uptake are not unique to our ECMHC pilot and are relevant to other SEL services, curricula, and interventions. For example, coaching and consultation are a core component of many SEL interventions and are used to help ensure high quality implementation of the particular SEL program (Pas et al., 2014). However, the cost of coaching and consultation is often prohibitive at scale, especially at the levels of frequency (i.e., weekly or bi-weekly for a full school year) and universality (i.e., to every educator who is engaging in the SEL intervention) delivered in the context of experimental evaluations. In reality, coaching and consultation will not be delivered at this intensity at scale and researchers might consider testing coaching and consultation delivery that could be practically delivered community-wide (e.g., coaching only teachers who are struggling to implement, during initial uptake only, and/or providing more scalable “nudge” supports). Specific to ECMHC programs, the field would benefit from a better understanding of the specific service components, and the dosage of those components, that lead to positive impacts for educators, families, and children, so that limited resources can be allocated most effectively at scale.
In addition, our work highlights the need for SEL interventionists, especially those operating at tier 2 or 3 in a multi-systemic system of support, to be reflective about whether their service may be inadvertently contributing to the idea that children need to be “fixed.” For example, in what ways does pulling a child or group of children out of the classroom for a social skills group communicate to children, their teachers, and their parents that their child needs to be “fixed”? In the context of ECMHC programs specifically, services typically begin with some kind of referral system. Although the referral process is typically not considered to be a program component, we argue that it should be, because systematic investigation of the referral system can lead to helpful insights about how to best create a system that reaches potential participants but does not communicate unintended messages about children in the process. Finally, the systemic barriers our ECE workforce encounters create a system where most any SEL programming may not be able to achieve the intended positive impact. For example, it is near impossible to implement any service, curriculum, or program with good fidelity in partnership with a workforce that does not earn enough money to stay in their profession. Low wages of ECE providers result in constant educator turnover, which makes it very difficult to train and support providers over a longer time span. For example, time and money put into training providers on any SEL program is lost once the teacher has left the profession. Again, in this paper, we do not suggest there is a preferred or correct answer to solve these tensions, but we found that considering these tensions explicitly resulted in modifications that we hope will improve our implementation of ECMHC for children, educators, and families.
This paper also extended an implementation framework that was developed with K-12 school settings in mind to be relevant for the ECE context. We noted unique considerations for implementation within ECE contexts at the individual-, program-, and macro-levels. However, differences at the macro-level are perhaps the most stark when comparing factors that influence implementation of SEL programs in ECE versus K-12 settings. The ECE system is fragmented and underfunded, has chronic workforce instability, and available resources for both children and educators are highly variable. The impacts of these systemic factors are felt everyday by providers and families across the United States. Without policy changes, wide scale implementation of SEL programs is insufficient to support children and families.
We focused on qualitative and survey data where we asked providers to describe their experience of and satisfaction with the ECMHC model to try to center the experiences of the children, providers, and families that we were intending to serve through this pilot. The voices of providers and families who were willing to share their experiences with us, especially through interviews and focus groups, helped us identify the tensions discussed in this paper. Our examination of the ECMHC pilot through these data sources highlight the value of embedding qualitative methodology when examining the scaling of SEL programming.
We recognize several limitations of this work and areas for future directions. First, we piloted the first year of Virginia’s ECMHC model during the world-wide COVID-19 pandemic. As such, some of the tensions described in this paper were almost certainly exacerbated due to the negative repercussions of the pandemic. While we believe that the discussion of the tensions described in this paper will be applicable to the scaling of ECMHC in Virginia and beyond in a post-pandemic context, the fact that our pilot was implemented, and our data collected, during the COVID-19 pandemic limits our ability to compare our findings with prior research and may limit future researchers to compare their findings with our work. Second, the Virginia ECMHC model was designed and implemented birth-to-5, but only preschool data were accessible from this pilot year. In future years, we plan to incorporate data from infant/toddler programs, to better understand implementation of the entire Virginia ECMHC model. Additionally, data from a larger sample of participants will allow us to further examine the implementation tensions outlined in this paper. For example, it would be interesting to explore whether some tensions are more salient for certain ECMHC components versus others (e.g., the service intensity or consultation focus). Third, compared to the overall number of referrals that were received, a small percentage of providers engaged in ECMHC services. We also have much missing quantitative data due to challenges with reaching providers, which limits our understanding of who made a referral but did not progress through services and why. In future years, we will continue to center the voices of providers and families to understand their experiences engaging in the Virginia ECMHC program. Our goal is to continually apply lessons learned to improve our model, work to alleviate systemic barriers faced by providers and families when possible, and develop enhanced supports that will lead to better ECMHC implementation and social–emotional outcomes for young children in Virginia.
Data availability statement
The datasets presented in this article are not readily available because the data are restricted due to confidentiality agreements. Requests to access the datasets should be directed to corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by University of Virginia Institutional Review Board. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author contributions
AP wrote the introduction, implementation of ECMHC in Virginia, and conclusion, edited all other sections of the paper, and led the quantitative data collection and analysis. SS led the qualitative data collection and analysis and the second tension on contributing to deficit views of children. MB led the third tension on systemic issues. KC led the conceptual framework and first tension on ideal versus pragmatic roll-out. SM-M and KP contributed to the second tension on contributing to deficit views of children. PA contributed to analysis of implementation data, and CF contributed to qualitative data collection and identified quotes that best represented themes. AW and JD reviewed, edited, and provided feedback on the manuscript and contributed to the conclusion. All authors contributed to formulating the implementation tensions described in the paper.
Funding
This research was supported by the Virginia Department of Education with funding provided through a federal Governor’s Emergency Education Relief (GEER) Fund. The opinions expressed in this paper are those of the authors and do not represent the views of the funding agencies.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^In this article, we use the terms providers, educators, teachers interchangeably to describe the adults who work as early childhood professionals and provide care and education to young children from birth through preschool in private, faith-based, public, and family day home settings.
2. ^Early childhood education (ECE), early childhood care and education (ECCE), and early childhood education and care (ECEC) are terms that are often used synonymously. In this paper, we define early childhood education (ECE) inclusive of early childhood programs that provide care and education to young children from birth through preschool in private, faith-based, public, and family day home settings.
3. ^House Joint Resolution No. 51 requested that the Virginia Departments of Education, Social Services, and Behavioral Health and Developmental Services convene a workgroup to study and provide recommendations on an ECMHC model and submit a report to the Virginia Governor and General Assembly. The workgroup report is available here .
4. ^ https://www.iecmhc.org/resources/hiring-guidance/
5. ^All names have been changed with permissions from participants to protect their identities.
References
Adair, J. K., Colegrove, K. S., and McManus, M. (2018). Troubling messages: agency and learning in the early school experiences of children of Latinx immigrants. Teach. Coll. Rec. 120, 1–40. doi: 10.1177/0161468118120006
Adair, J. K., and Kurban, F. (2019). Video-cued ethnography in educational settings. Anthropol. Educ. Q. 50, 245–254. doi: 10.1111/aeq.12311
Albritton, K., Mathews, R. E., and Anhalt, K. (2019). Systematic review of early childhood mental health consultation: implications for improving preschool discipline disproportionality. J. Educ. Psychol. Consult. 29, 444–472. doi: 10.1080/10474412.2018.1541413
Bartlett, J. D., and Smith, S. (2019). The role of early care and education in addressing early childhood trauma. Am. J. Community Psychol. 64, 359–372. doi: 10.1002/ajcp.12380
Beltman, S., Dobson, M. R., Mansfield, C. F., and Jay, J. (2020). “The thing that keeps me going”: educator resilience in early learning settings. Int. J. Early Years Educ. 28, 303–318. doi: 10.1080/09669760.2019.1605885
Berger, E., Quinones, G., Barnes, M., and Reupert, A. (2022). Early childhood educators' psychological distress and wellbeing during the COVID-19 pandemic. Early Child. Res. Q. 60, 298–306. doi: 10.1016/j.ecresq.2022.03.005
Boonstra, K. E. (2021). Constructing “behavior problems”: race, disability, and everyday discipline practices in the figured world of kindergarten. Anthropol. Educ. Q. 52, 373–390. doi: 10.1111/aeq.12374
Bradshaw, C. P., Mitchell, M. M., O'brennan, L. M., and Leaf, P. J. (2010). Multilevel exploration of factors contributing to the overrepresentation of black students in office disciplinary referrals. J. Educ. Psychol. 102, 508–520. doi: 10.1037/a0018450
Bronson, M. B., Goodson, B. D., Layzer, J. I., and Love, J. M. (1990). Child behavior rating scale Abt Associates.
Buettner, C. K., Jeon, L., Hur, E., and Garcia, R. E. (2016). Teachers’ social–emotional capacity: factors associated with teachers’ responsiveness and professional commitment. Early Educ. Dev. 27, 1018–1039. doi: 10.1080/10409289.2016.1168227
Center for Disease Control and Prevention. (2022). Risk for COVID-19 infection, hospitalization, and death by race/ethnicity. Available at: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html
Center on Budget and Policy Priorities (2020). Tracking the COVID-19 recession’s effects on food, housing, and employment hardships. Available at: https://www.cbpp.org/sites/default/files/atoms/files/8-13-20pov.pdf
Clayback, K., and Williford, A. P. (2022). Teacher and classroom predictors of preschool teacher stress. Early Educ. Dev. 33, 1347–1363. doi: 10.1080/10409289.2021.1972902
Cohen, E., and Kaufmann, R. (2005). Early childhood mental health consultation. DHHS pub. No. CMHS-SVP0151 Center for Mental Health Services, Substance Abuse and Mental Health Services Administration.
Conners Edge, N. A., Kyzer, A., Abney, A., Freshwater, A., Sutton, M., and Whitman, K. (2021). Evaluation of a statewide initiative to reduce expulsion of young children. Infant Ment. Health J. 42, 124–139. doi: 10.1002/imhj.21894
Cook, C. R., Lyon, A. R., Kubergovic, D., Browning Wright, D., and Zhang, Y. (2015). A supportive beliefs intervention to facilitate the implementation of evidence-based practices within a multi-tiered system of supports. Sch. Ment. Heal. 7, 49–60. doi: 10.1007/s12310-014-9139-3
Crawford, A., Vaughn, K. A., Guttentag, C. L., Varghese, C., Oh, Y., and Zucker, T. A. (2021). "Doing what I can, but I got no magic wand": A snapshot of early childhood educator experiences and efforts to ensure quality during the COVID-19 pandemic. Early Childhood Educ. J. 49, 829–840. doi: 10.1007/s10643-021-01215-z
Creswell, J. W., and Poth, C. N. (2016). Qualitative inquiry and research design: Choosing among five approaches Sage.
Davis, A. E., Perry, D. F., and Rabinovitz, L. (2020). Expulsion prevention: framework for the role of infant and early childhood mental health consultation in addressing implicit biases. Infant Ment. Health J. 41, 327–339. doi: 10.1002/imhj.21847
Davison, J. C., and Ford, D. Y. (2001). Perceptions of attention deficit hyperactivity disorder in one African American community. J. Negro Educ. 70, 264–274. doi: 10.2307/3211279
Devlieghere, J., Li, Y., and Vandenbroeck, M. (2020). Beyond the veil of parents: deconstructing the concept of parental involvement in early childhood education and care. Early Years 42, 587–598. doi: 10.1080/09575146.2020.1840526
Domitrovich, C. E., Bradshaw, C. P., Poduska, J. M., Hoagwood, K., Buckley, J. A., Olin, S., et al. (2008). Maximizing the implementation quality of evidence-based preventive interventions in schools: a conceptual framework. Adv. School Ment. Health Promot. 1, 6–28. doi: 10.1080/1754730x.2008.9715730
Domitrovich, C. E., Gest, S. D., Gill, S., Jones, D., and DeRousie, R. S. (2009). Individual factors associated with professional development training outcomes of the head start REDI program. Early Educ. Dev. 20, 402–430. doi: 10.1080/10409280802680854
Domitrovich, C. E., Li, Y., Mathis, E. T., and Greenberg, M. T. (2019). Individual and organizational factors associated with teacher self-reported implementation of the PATHS curriculum. J. Sch. Psychol. 76, 168–185. doi: 10.1016/j.jsp.2019.07.015
Doromal, J. B., Bassok, D., Bellows, L., and Markowitz, A. J. (2022). Hard-to-staff centers: exploring center-level variation in the persistence of child care teacher turnover. Early Child. Res. Q. 61, 170–178. doi: 10.1016/j.ecresq.2022.07.007
Downer, J. T., Booren, L. M., Lima, O. K., Luckner, A. E., and Pianta, R. C. (2010). The individualized classroom assessment scoring system (inCLASS): preliminary reliability and validity of a system for observing preschoolers’ competence in classroom interactions. Early Child. Res. Q. 25, 1–16. doi: 10.1016/j.ecresq.2009.08.004
Downer, J. T., Williford, A. P., Bulotsky-Shearer, R. J., Vitiello, V. E., Bouza, J., Reilly, S., et al. (2018). Using data-driven, video-based early childhood consultation with teachers to reduce children’s challenging behaviors and improve engagement in preschool classrooms. Sch. Ment. Heal. 10, 226–242. doi: 10.1007/s12310-017-9237-0
Durlak, J. A., and DuPre, E. P. (2008). Implementation matters: a review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am. J. Community Psychol. 41, 327–350. doi: 10.1007/s10464-008-9165-0
Eadie, P., Levickis, P., Murray, L., Page, J., Elek, C., and Church, A. (2021). Early childhood educators' wellbeing during the COVID-19 pandemic. Early Childhood Educ. J. 49, 903–913. doi: 10.1007/s10643-021-01203-3
Epstein, R., Blake, J., and González, T. (2017). Girlhood interrupted: the erasure of black girls’ childhood Georgetown Law Center on Poverty and Inequality doi: 10.2139/ssrn.3000695.
Farewell, C. V., Quinlan, J., Melnick, E., Power, J., and Puma, J. (2022). Job demands and resources experienced by the early childhood workforce serving high-needs populations. Early Childhood Educ. J. 50, 197–206. doi: 10.1007/s10643-020-01143-4
Fettig, A., and Artman-Meeker, K. (2016). Group coaching on pre-school teachers’ implementation of pyramid model strategies. Top. Early Child. Spec. Educ. 36, 147–158. doi: 10.1177/0271121416650049
Friedman-Krauss, A. H., Raver, C. C., Morris, P. A., and Jones, S. M. (2014). The role of classroom-level child behavior problems in predicting preschool teacher stress and classroom emotional climate. Early Educ. Dev. 25, 530–552. doi: 10.1080/10409289.2013.817030
Garro, A., Giordano, K., Gubi, A., and Shortway,. (2021). A consultation approach to target exclusionary discipline of students of color in early childhood education. Contemp. Sch. Psychol. 25, 124–135. doi: 10.1007/s40688-019-00258-9
Gilliam, W. S., and Reyes, C. R. (2018). Teacher decision factors that lead to preschool expulsion: scale development and preliminary validation of the preschool expulsion risk measure. Infants Young Child. 31, 93–108. doi: 10.1097/IYC.0000000000000113
Giordano, K., Eastin, S., Calcagno, B., Wilhelm, S., and Gil, A. (2020). Examining the effects of internal versus external coaching on preschool teachers’ implementation of a framework of evidence-based social-emotional practices. J. Early Child. Teach. Educ. 42, 423–436. doi: 10.1080/10901027.2020.1782545
Gomez, R. E., Kagan, S. L., and Fox, E. A. (2015). Professional development of the early childhood education teaching workforce in the United States: an overview. Prof. Dev. Educ. 41, 169–186. doi: 10.1080/19415257.2014.986820
González, N., Moll, L. C., and Amanti, C. (2006). Funds of knowledge: Theorizing practices in households, communities, and classrooms Routledge doi: 10.4324/9781410613462.
Goodman, R. (1997). The strengths and difficulties questionnaire: a research note. J. Child Psychol. Psychiatry 38, 581–586. doi: 10.1111/j.1469-7610.1997.tb01545.x
Gregory, A., Skiba, R. J., and Mediratta, K. (2017). Eliminating disparities in school discipline: a framework for intervention. Rev. Res. Educ. 41, 253–278. doi: 10.3102/0091732X17690499
Gregory, A., Skiba, R. J., and Noguera, P. A. (2010). The achievement gap and the discipline gap: two sides of the same coin? Educ. Res. 39, 59–68. doi: 10.3102/0013189X09357621
Hemmeter, M. L., Barton, E., Fox, L., Vatland, C., Henry, G., Phan, L., et al. (2022). Program-wide implementation of the pyramid model: supporting fidelity at the program and classroom levels. Early Child. Res. Q. 59, 56–73. doi: 10.1016/j.ecresq.2021.10.003
Hemmeter, M. L., Fox, L., and Snyder, P. (2014). Teaching pyramid observation tool for preschool classrooms : Research edition. Brookes.
Hemmeter, M. L., Ostrosky, M., and Fox, L. (2006). Social and emotional foundations for early learning: a conceptual model for intervention. Sch. Psychol. Rev. 35, 583–601. doi: 10.1080/02796015.2006.12087963
Hindman, A. H., and Bustamante, A. S. (2019). Understanding well-being among teachers in early childhood settings: challenges, supports, and implications for children’s development. J. Appl. Dev. Psychol. 61, 1–3. doi: 10.1016/j.appdev.2019.03.005
Hines-Datiri, D., and Carter Andrews, D. J. (2020). The effects of zero tolerance policies on black girls: using critical race feminism and figured worlds to examine school discipline. Urban Educ. 55, 1419–1440. doi: 10.1177/0042085917690204
Hoover, S. D., Kubicek, L. F., Rosenberg, C. R., Zundel, C., and Rosenberg, S. A. (2012). Influence of behavioral concerns and early childhood expulsions on the development of early childhood mental health consultation in Colorado. Infant Ment. Health J. 33, 246–255. doi: 10.1002/imhj.21334
Hunter, A., Davis, A. E., Perry, D. F., and Jones, W. (2016). The Georgetown manual for school-based early childhood mental health consultation services Georgetown University Center for Child and Human Development https://www.iecmhc.org/documents/FCC_Manual_2020_Proof2.pdf.
Jeon, L., Buettner, C. K., and Grant, A. A. (2018). Early childhood teachers’ psychological well-being: exploring potential predictors of depression, stress, and emotional exhaustion. Early Educ. Dev. 29, 53–69. doi: 10.1080/10409289.2017.1341806
Jeon, H.-J., Kwon, K.-A., Walsh, B., Burnham, M. M., and Choi, Y.-J. (2019). Relations of early childhood education teachers’ depressive symptoms, job-related stress, and professional motivation to beliefs about children and teaching practices. Early Educ. Dev. 30, 131–144. doi: 10.1080/10409289.2018.1539822
Jeon, L., and Wells, M. B. (2018). An organizational-level analysis of early childhood teachers’ job attitudes: workplace satisfaction affects early head start and head start teacher turnover. Child Youth Care Forum 47, 563–581. doi: 10.1007/s10566-018-9444-3
Kristiansen, E., Tholin, K. R., and B, M. (2021). Early childhood Centre directors coping with stress: firefighters and oracles. Int. J. Educ. Manag. 35, 909–921. doi: 10.1108/IJEM-12-2020-0584
Kwon, K.-A., Jeon, S., Castle, S., and Ford, T. G. (2022). Children’s behavioral challenges in head start classrooms: links to teacher well-being and intent to leave. Early Childhood Educ. J. 50, 1221–1232. doi: 10.1007/s10643-021-01253-7
Losen, D. J., and Gillespie, J. (2012). Opportunities suspended: The disparate impact of disciplinary exclusion from school Civil Rights Project/Proyecto Derechos Civiles https://civilrightsproject.ucla.edu/resources/projects/center-for-civil-rights-remedies/school-to-prison-folder/federal-reports/upcoming-ccrr-research/losen-gillespie-opportunity-suspended-2012.pdf.
Markowitz, A. J., and Bassok, D. (2022). Understanding the wellbeing of early educators in the wake of the coronavirus pandemic: lessons from Louisiana. Early Child. Res. Q. 61, 1–14. doi: 10.1016/j.ecresq.2022.05.001
McClelland, M. M., Tominey, S. L., Schmitt, S. A., and Duncan, R. (2017). Social–emotional learning interventions in early childhood. Future Child. 27, 33–47. doi: 10.1353/foc.2017.0002
McGoey, K. E., Rispoli, K. M., Venesky, L. G., Schaffner, K. F., McGuirk, L., and Marshall, S. (2014). A preliminary investigation into teacher perceptions of the barriers to behavior intervention implementation. J. Appl. Sch. Psychol. 30, 375–390. doi: 10.1080/15377903.2014.950441
McLean, C., Austin, L. J. E., Whitebook, M., and Olson, K. L. (2021). Early childhood workforce index–2020. Berkeley: Center for the Study of Child Care Employment, University of California, Berkeley. Available at: https://cscce.berkeley.edu/workforce-index-2020/wp-content/uploads/sites/3/2021/02/Early-Childhood-Workforce-Index-2020.pdf
Miles, M. B., Huberman, A. M., and Saldaña, J. (2018). Qualitative data analysis: A methods sourcebook Sage.
National Scientific Council on the Developing Child (2012). Establishing a level foundation for life: Mental health begins in early childhood: Working paper 6 Center on the Developing Child, Harvard University https://harvardcenter.wpenginepowered.com/wp-content/uploads/2008/05/Establishing-a-Level-Foundation-for-Life-Mental-Health-Begins-in-Early-Childhood.pdf.
Nemer, S. L., Sutherland, K. S., Chow, J. C., and Kunemund, R. L. (2019). A systematic literature review identifying dimensions of teacher attributions for challenging student behavior. Educ. Treat. Child. 42, 557–578. doi: 10.1353/etc.2019.0026
Pas, E., Bradshaw, C., and Cash, A. (2014). “Coaching classroom-based preventive interventions” in Handbook of school mental health. eds. M. Weist, N. Lever, C. Bradshaw, and J. Owens. 2nd ed (Springer), 255–267. doi: 10.1007/978-1-4614-7624-5_19
Quinones, G., Barnes, M., and Berger, E. (2021). Early childhood educators' solidarity and struggles for recognition. Australas. J. Early Childhood 46, 296–308. doi: 10.1177/18369391211050165
Reyes, C. R., Gilliam, W. S., Cicchetti, D., Luthar, S. S., and Burack, J. A. (2021). Addressing challenging behaviors in challenging environments: findings from Ohio's early childhood mental health consultation system. Dev. Psychopathol. 33, 634–646. doi: 10.1017/S0954579420001790
Roberts, A. M., Gallagher, K. C., Daro, A. M., Iruka, I. U., and Sarver, S. L. (2019). Workforce well-being: personal and workplace contributions to early educators' depression across settings. J. Appl. Dev. Psychol. 61, 4–12. doi: 10.1016/j.appdev.2017.09.007
Schaack, D. D., Donovan, C. V., Adejumo, T., and Ortega, M. (2022). To stay or to leave: factors shaping early childhood teachers’ turnover and retention decisions. J. Res. Child. Educ. 36, 327–345. doi: 10.1080/02568543.2021.1955779
Schaack, D. D., Le, V. N., and Stedron, J. (2020). When fulfillment is not enough: early childhood teacher occupational burnout and turnover intentions from a job demands and resources perspective. Early Educ. Dev. 31, 1011–1030. doi: 10.1080/10409289.2020.1791648
Scott, C., and Medaugh, M. (2017). Axial coding. Int. Encycl. Comm. Res. Methods 10:12. doi: 10.1002/9781118901731.iecrm0012
Shonkoff, J. P., Slopen, N., and Williams, D. R. (2021). Early childhood adversity, toxic stress, and the impacts of racism on the foundations of health. Annu. Rev. Public Health 42, 115–134. doi: 10.1146/annurev-publhealth-090419-101940
Skiba, R. J., Horner, R. H., Chung, C. G., Rausch, M. K., May, S. L., and Tobin, T. (2011). Race is not neutral: a national investigation of African American and Latino disproportionality in school discipline. Sch. Psychol. Rev. 40, 85–107. doi: 10.1080/02796015.2011.12087730
Swigonski, N. L., James, B., Wynns, W., and Casavan, K. (2021). Physical, mental, and financial stress impacts of COVID-19 on early childhood educators. Early Childhood Educ. J. 49, 799–806. doi: 10.1007/s10643-021-01223-z
Tobin, J. (2019). The origins of the video-cued multivocal ethnographic method. Anthropol. Educ. Q. 50, 255–269. doi: 10.1111/aeq.12302
Trigg, A. B., and Keyes, A. W. (2019). “Child care and early education as contexts for infant mental health” in Handbook of infant mental health. ed. C. H. Zeanah. 4th ed (Guilford Press), 599–609.
U.S. Department of Education Office for Civil Rights. (2016). 2013–2014 civil rights data collection: A first look. United States: Department of Education Office for Civil Rights. Available at: https://ocrdata.ed.gov/assets/downloads/2013-14-first-look.pdf
U.S. Department of Health and Human Services and Education. (2014). Policy statement on expulsion and suspension policies in early childhood settings Available at: https://www2.ed.gov/policy/gen/guid/school-discipline/policy-statement-ece-expulsions-suspensions.pdf
Virginia Department of Education and the Center for Advanced Study of Teaching and Learning, University of Virginia (2022). VKRP status report for the chairmen of house appropriations and senate finance committees. Report prepared for the Virginia Chairmen of House Appropriations and Senate Finance Committees.
Whitebook, M., Phillips, D., and Howes, C. (2014). Worthy work, STILL unlivable wages: The early childhood workforce 25 years after the National Child Care Staffing Study. Center for the Study of Child Care Employment, University of California, Berkeley, Berkeley. Available at: https://cscce.berkeley.edu/worthy-work-still-unlivable-wages/
Williams, M., and Moser, T. (2019). The art of coding and thematic exploration in qualitative research. Int. Manag. Rev. 15, 45–55.
Zeanah, C. H., and Zeanah, P. D. (2019). “Infant mental health: the clinical science of early experience” in Handbook of infant mental health. ed. C. H. Zeanah. 4th ed (Guilford Press), 5–24.
Zero to Three. (2017). The basics of infant and early childhood mental health: a briefing paper. Available at: https://www.zerotothree.org/wp-content/uploads/2017/08/The-Basics-of-Infant-and-Early-Childhood-Mental-Health_-A-Briefing-Paper.pdf
Keywords: social–emotional learning, implementation, scale–up, early childhood mental health consultation, early childhood education
Citation: Partee AM, Sachdeva S, Bivona MA, Clayback KA, Miller-Marshall S, Parker K, Alamos P, Frank C, Downer JT and Williford AP (2023) Implementation of an early childhood mental health consultation pilot in Virginia: Critical tensions and implications for scale-up. Front. Educ. 8:1070591. doi: 10.3389/feduc.2023.1070591
Edited by:
Celene Domitrovich, Georgetown University, United StatesReviewed by:
Deborah Perry, Georgetown University, United StatesKaryn Hartz, University of Rochester, United States
Copyright © 2023 Partee, Sachdeva, Bivona, Clayback, Miller-Marshall, Parker, Alamos, Frank, Downer and Williford. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ann M. Partee, ✉ YW1wOWFzQHZpcmdpbmlhLmVkdQ==
†These authors have contributed equally to this work