 Katrine Lyngvær Fredriksen
Katrine Lyngvær Fredriksen Alexander G. Page
Alexander G. Page Celina Lindhardt
Celina Lindhardt Sobh Chahboun
Sobh Chahboun- 1Institute for Pedagogy, Queen Maud University College, Trondheim, Norway
- 2Mental Healthcare for Children and Adolescents’ Services, Kristiansund, Norway
- 3Department of Social Work, Norwegian University of Science and Technology, Trondheim, Norway
- 4Åsveien School, Trondheim, Norway
Gender plays a critical role in the recognition, diagnosis, and support of children with Autism Spectrum Disorder (ASD). This qualitative study explores the perspectives of special education professionals, who are involved in both diagnosing and following up children with Autism, on how ASD manifests in girls and the diagnostic challenges that arise. Although boys are more frequently diagnosed—and often at younger ages—emerging research and clinical experience suggest that girls may exhibit more nuanced and socially adaptive traits that fall outside traditional diagnostic expectations. Girls with ASD often use compensatory behaviors such as social mimicry, masking of difficulties, and scripting in social situations to conform to neurotypical norms. This study is based on semi structured interviews with three special educators from the Child and Adolescent Psychiatric Services. While these strategies can temporarily obscure core challenges in communication and social reciprocity, they frequently contribute to delayed identification and are associated with long-term psychological consequences, including fatigue, anxiety, and depression. Participants noted that girls are typically referred for evaluation later in adolescence, often in connection with internalizing symptoms such as eating disorders or mood-related concerns, rather than overt behavioral issues. Findings highlight the limitations of diagnostic frameworks that are largely based on male-typical presentations of ASD and emphasize the need for gender-informed assessment practices. This study underscores the importance of developing diagnostic tools and support strategies that account for the diverse ways ASD may present in girls, thereby enhancing early identification, reducing misdiagnosis, and promoting more equitable support within education and mental health services.
Introduction
Extensive research demonstrates that significantly more boys are diagnosed with Autism Spectrum Disorder (ASD) compared to girls (Whiteley et al., 2010; Halladay et al., 2015; Wood-Downie et al., 2021). Although studies vary regarding ASD presentation across ethnic groups and ages, the commonly cited figure is four boys diagnosed for every girl (Fombonne, 2009). Moreover, symptom occurrence differs according to gender. Most importantly, girls often exhibit fewer social challenges and demonstrate relatively better communication skills compared to boys (Stave, 2022). Their more subtle social difficulties can allow girls to adapt more effectively to various environments, such as classrooms. While girls may be better at adapting to their challenges, this does not mean that they do not experience them. Limited research in this area suggests that girls experience similar impairments in adaptive functioning as boys (McQuaid et al., 2021). Furthermore, the need to adapt socially can lead to self-criticism and feelings of not fitting in, increasing risks for anxiety and depression (Stave, 2022). Ironically, their ability to compensate means that girls remain less likely to be diagnosed with ASD than boys (Rutherford et al., 2016). When they are diagnosed, the same factors tend to delay the diagnostic process, meaning that they experience these difficulties for longer periods before identification (McDonnell et al., 2021). Girls with higher cognitive functioning are especially vulnerable to remaining undiagnosed (Hutson and Hutson, 2023). Lastly, when professionals overlook girls, these children often develop additional difficulties, making timely expertise, suitable assessment methods, and proper follow-up critical.
Taken as a whole, this suggests that the stereotypical characteristics typically recognized as ASD hallmarks might predominantly represent a male-specific presentation of autism. Researchers thus question whether existing diagnostic criteria sufficiently reflect symptom expressions in girls (Mathisen, 2016). Such findings further underscore the limitations of a diagnostic approach grounded primarily in the medical model. This views ASD primarily as a disorder characterized by deficits that need to be diagnosed and treated. In this study, the authors critique how current diagnostic frameworks—like DSM-5 and ICD-11—are still largely based on male-typical symptom presentations and pathologize autistic traits (Lonergan, 2021). This model often fails to account for the subtler, masked behaviors more common in girls, leading to underdiagnosis and misdiagnosis (Dwyer, 2022).
A neurodiversity perspective, by contrast, sees ASD not as a deficit but as a natural variation in human neurodevelopment. The study highlights how adopting this view can help reframe compensatory behaviors (e.g., masking and social mimicry) not as deceptive but as adaptive responses to non-inclusive environments (Dwyer, 2022). This lens encourages support tailored to individual needs and promotes earlier, more accurate recognition, especially in girls whose autistic traits deviate from traditional norms (Dwyer, 2022). Adopting this lens may also promote earlier and more accurate identification of girls, whose profiles often fall outside stereotypical symptom patterns.
This study is based on semi structured interviews with three special educators from the Child and Adolescent Psychiatric Services. These participants are involved both in the diagnosis of ASD, and also in the subsequent work with diagnosed children. The purpose of this study is to explore how gender differences affect the recognition, diagnosis, and support of children and adolescents with ASD within Norway’s mental healthcare services. Specifically, it aims to understand the challenges in identifying ASD in girls, focusing on the role of compensatory behaviors and the limitations of current diagnostic tools from the perspective of special education professionals. While there is a growing scholarship within autism and gender-diversity (e.g., Warrier et al., 2020), this paper discusses the binary boy/girl dimension, as this was the framework within which the participants operated. Within this framework, the findings from the participants suggest a lack of knowledge of the gender-dependent presentations of autism, and the difficulties this creates for girls on the spectrum.
A glossary of key terms is provided at the end of the article.
Autism: diagnostic frameworks and gender sensitivity
Diagnostic manuals serve as foundational tools for assessing and identifying ASD in clinical settings. The two most widely used frameworks, the DSM and the ICD, are periodically revised to incorporate emerging scientific knowledge. Norway is transitioning to the ICD-11, which replaces the ICD-10 category of “pervasive developmental disorders” with the more integrated term “autism spectrum disorder.” This aligns with the DSM-5’s spectrum-based approach and represents a conceptual shift toward recognizing the broad variability in autistic presentations (American Psychiatric Association, 2013 Livingston et al., 2019).
Both the ICD-11 and DSM-5 define ASD by persistent deficits in social interaction and communication, alongside restricted and repetitive behaviors. These criteria allow for variation in age of onset, symptom severity, and functional impact. Notably, the ICD-11 provides expanded guidance on how these traits may manifest differently depending on developmental and contextual factors, including gender. For example, it acknowledges the use of compensatory behavior strategies such as imitation, and camouflaging—to manage social situations. These behaviors are more frequently observed in girls and may obscure core difficulties, thereby delaying diagnosis or leading to misdiagnosis (Hull et al., 2017; Bargiela et al., 2016 Hull et al., 2020).
By introducing classifications related to intellectual and language functioning, the ICD-11 also facilitates more individualized assessment and support planning. These improvements aim to increase diagnostic precision and inclusivity, particularly for underrepresented groups (World Health Organization, 2018, 2023). However, despite these updates, critics argue that both the DSM and ICD frameworks still reflect a large medical model of autism, emphasizing deficits over diversity (Dwyer, 2022). This may limit recognition of autistic traits in individuals whose experiences fall outside stereotypical (often male-normed) patterns—what some researchers describe as the “female autism phenotype” (Lai and Szatmari, 2020). This includes, for instance, restricted interests that are more socially acceptable (e.g., animals or fictional characters), or subtler social difficulties masked by high verbal skills.
While both manuals mark progress toward greater inclusiveness, aimed at improving diagnostic recognition, particularly in underdiagnosed groups such as girls, their real-world application remains shaped by clinician training, societal norms, and diagnostic tools that may not fully capture the complexity of autistic experiences across genders. Future research must examine how these frameworks are interpreted in practice and whether they successfully address the biases that contribute to gender-based disparities in ASD diagnosis.
Gender disparities—camouflaging, compensatory behavior, and emotional cost
Gender disparities in ASD diagnoses are widely recognized. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) cites a commonly reported male-to-female prevalence ratio of 4:1. However, a meta-analysis by Loomes et al. (2017) suggests the true ratio may be closer to 3:1, indicating that girls may be underdiagnosed. Notably, prevalence ratios tend to narrow with age—studies have shown a ratio of 5.5:1 in children that decreases to 2.3:1 in adolescence (Rutherford et al., 2016), and even further in adulthood (Bargiela et al., 2016). The fact that disparities decrease with age suggests that autism is more evenly distributed than diagnosis trends suggest, but that that many autistic girls are identified late. A reasonable inference might be that autism occurs evenly, but that many females are missed altogether.
This disparity is partly due to differences in symptom presentation. Girls often show fewer externalizing behaviors and may present with subtler or less stereotypical ASD traits than boys. For instance, while boys may be referred for assessment due to overt behavioral issues, girls are frequently referred later for internalizing symptoms such as anxiety, depression, or eating disorders (Bargiela et al., 2016).
A key factor contributing to delayed recognition is the use of compensatory strategies—often referred to as camouflaging—by autistic girls (Hull et al., 2016 Fombonne, 2020 Burns and Tierney, 2023). These behaviors include mimicking peers’ social behaviors and rehearsing social scripts to appear neurotypical (Hull et al., 2017 Lai et al., 2015). This can involve strategies such as suppressing stimming, imitating neurotypical interactions, hiding emotions, consciously altering eye contact, tone, posture, and turn-taking. Although effective in hiding difficulties, these strategies can lead to chronic stress, burnout, depression and identity confusion (Cage et al., 2018). However, some individuals report temporary benefits of camouflaging, such as reduced bullying or increased acceptance in professional or social settings (Tierney et al., 2016). Simultaneously, there are ethical concerns about expecting people with ASD to conform to neurotypical norms. From a neurodiversity perspective, these behaviors reflect responses to non-inclusive environments rather than deficits (Fombonne, 2020 Dwyer, 2022). Camouflaging may bring short-term acceptance but often leads to internalized stigma.
Balancing these short-term benefits with the long-term psychological toll underscores the need for interventions that reduce reliance on compensatory strategies. Camouflaging behaviors evolve with the individual’s age and changing social demands, which might contribute to underdiagnosis of females (Hull et al., 2019). Despite growing interest in this phenomenon, the literature remains emergent and contested. For example, while Hull et al. (2017) highlight the prevalence and psychological toll of camouflaging, others, like Fombonne (2020), urge caution about overgeneralizing these findings, emphasizing the need for more empirical rigor in this area.
Many existing diagnostic tools were standardized primarily on male samples and may be less sensitive to how ASD manifests in girls. For example, girls may score lower on repetitive behavior domains in instruments like the ADOS or SRS—not because they lack these traits, but because their expressions differ (Navarro-Pardo et al., 2021). However, not all studies support this gender bias hypothesis. Kaat et al. (2021), for instance, found no significant gender differences in scores on standardized measures such as the ADOS, ADI-R, or SRS across multiple sites. This points to a need for further investigation into whether and how diagnostic tools may be overlooking certain profiles, particularly in girls who do not match conventional expectations of autism.
The term “female phenotype” of ASD is increasingly used to describe this divergent symptom presentation, often marked by internalized distress, compensatory behaviors, and social mimicry (Hull et al., 2019). However, it is not a formally recognized subtype, and its conceptualization varies across studies (Cruz et al., 2024). Greater clarity and consensus are needed to operationalize this construction in both research and practice.
Method
This study investigates how gender differences influence diagnostic practices, symptom recognition, and challenges associated with ASD within Norway’s mental healthcare services, focusing specifically on identifying and supporting girls with ASD.
This question is framed by the study’s emphasis on gender disparities in symptom presentation, diagnostic processes, and access to interventions, alongside the challenges posed by compensatory behaviors and the limitations of current diagnostic tools. While this study primarily discusses gender in binary terms (girls and boys), we recognize that gender is a spectrum and that neurodivergent individuals may also identify as nonbinary, transgender, or gender diverse.
Semi-structured interviews were conducted with professionals working in child and adolescent psychiatry (see Appendix 1).
Participants
In selecting participants, it was essential for this study to identify special educators with expertise and experience in working with children and adolescents with ASD.
All three participants were employed as special educators at different units within the same regional BUP (Child and Adolescent Psychiatric Services) in Norway, although the specific branch will not be related for confidentiality reasons.
Table 1 summarizes the profiles of the three participants in the study.
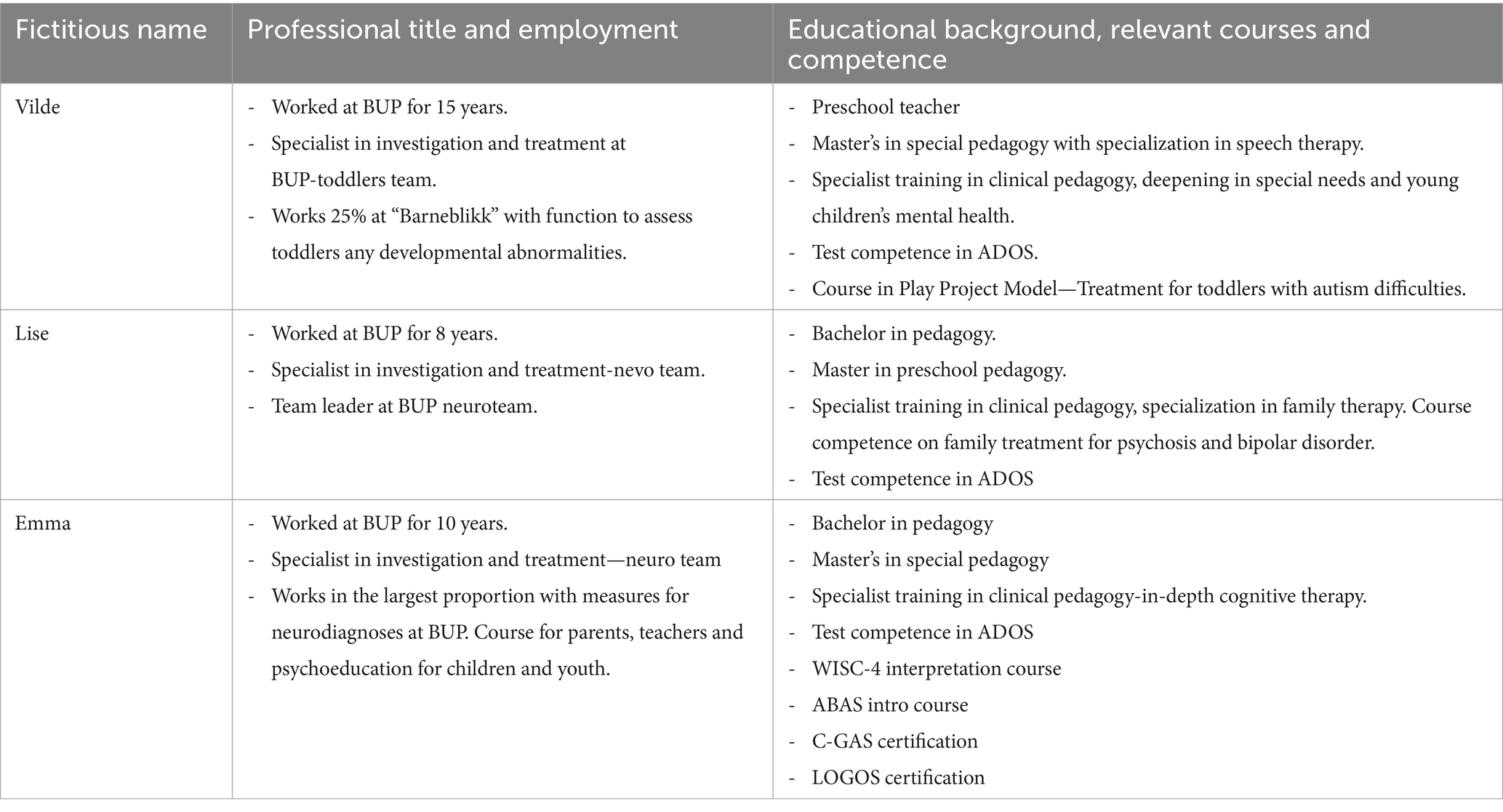
Table 1. Participants in the study.
Recruitment process
The recruitment process aimed to involve 4–5 special education professionals working in child and adolescent psychiatry (BUP), with extensive experience in assessing and supporting children and youth with autism. These participants were selected for their ability to address the study’s research questions through interviews. Several knowledgeable candidates with significant expertise in ASD were contacted, but not all agreed to participate. Ultimately, three suitable participants, all special education professionals in BUP, were included in the study.
It was chosen to focus on special educators as participants for several reasons. It was desirable for the researcher and the study to have an educational perspective, rather than a health perspective, as this is perceived as most relevant to the special education profession and it is considered to be more relevant to those who work closely with children and young people with ASD in an educational context, which is the main target group of this study. Special educators also often work more closely in everyday life with children and young people with ASD and also often follow these children over a longer period of time and can provide a good picture of their everyday functioning and how to further support these children well (Thagaard, 2018).
In contrast, the final sample shows three participants, all from the same institutional context, which may seem like a limited selection of participants. The findings will therefore not necessarily apply to everyone who works closely with children and young people with ASD but are related to these individuals. It may seem like a narrow picture of the experiences of children and young people with autism. On the other hand, these opinions may also apply to other people and are about generalizability. In other words, when the results of an interview survey are considered reliable, the question remains whether the results can be transferred to other interviewees, contexts and situations. Employees in this intuition also encounter a far larger number of people in their daily work than, for example, someone who works directly in a kindergarten or school system and can say something about the symptom expression of a far larger number within this target group.
Interview guide
To obtain useful research data from the participants, it has been important to plan an interview guide that ensures that information is asked that sheds light on the study’s theme and answers the research questions. The main structure consists of the questions that represent central themes in the survey. To answer the research question and central themes in the study, the idea behind preparing the interview guide has been that the first questions should contain opening questions that felt easy to answer to create a safe atmosphere in the interview situation. The questions are then formed in such a way that an investigation process takes place, so that the findings would describe an investigation process from start to end. Therefore, questions related to referral experience start and then move on to thoughts and experience with the use of diagnostic tools. Then, questions are asked about experiences with children and young people’s symptom expressions in relation to gender. Furthermore, questions are asked about measures and their experience of how to better support girls with ASD. By placing questions in this order, the questions act as a funnel from when children are referred to the hospital until they are discharged, and the study can shed light on all steps and experiences related to the assessment process for children and young people with ASD.
Ethical considerations
The research project has been approved by the Norwegian Center for Research Data, Additionally, confidentiality has been taken into consideration (Kvale and Brinkmann, 2015, p. 106). The participants’ right to privacy is protected through anonymization in the form of fictitious names and necessary steps to ensure that the people are not identified or recognized through the data material. The data from this study is not publicly available due to ethical considerations. To protect participant confidentiality and adhere to guidelines approved by the Norwegian Centre for Research Data, interview transcripts and audio recordings cannot be shared.
Implementation of the study and data analysis
The study in its entirety was conducted by the first author as her thesis for her master’s degree in special education, and she is the one who both conducted and transcribed the interviews, as well as coded the data.
The study employed qualitative thematic analysis to examine interview data. Audio recordings were transcribed into written text, with care taken to capture participants’ statements while acknowledging the loss of non-verbal cues.
Before beginning the analysis, the first step involved transcribing the recorded interviews into written text. As Kvale and Brinkmann (2015) note, transcription is an interpretive act in itself, where oral statements are abstracted and important elements such as tone, body language, facial expressions, and emotional nuance are inevitably lost. To ensure accuracy and preserve meaning as faithfully as possible, the recordings were played at a slower speed and listened to multiple times during the transcription process. The analysis then focused on organizing and structuring the data, with an emphasis on reducing the volume of material to better identify content relevant to the research question. This process also involved assessing whether the data collected directly addressed the study’s aims or revealed unexpected but thematically significant insights (Tjora, 2018). Key statements were highlighted, while less central content was marked with color codes—allowing for differentiation without discarding potentially valuable material.
In the analysis work, the focus was on creating order, structure and reducing the amount of data, so that it would be easier to find data material that was relevant to shed light on the study. The work was first done to reduce the amount of data and then relevant content was organized and categorized according to different themes. In this work, the researcher used an inductive coding framework, meaning that the codes were developed along the way. In developing the codes and categories, it was the researcher’s subjective role that shaped the categories. Thematic analysis was conducted by systematically coding the data, highlighting significant insights, and organizing them into themes relevant to the research objectives. A hermeneutic approach guided the interpretation, focusing on the participants’ subjective experiences. Key themes were constructed and a structured and comprehensive analysis was conducted. Key themes included the following: referral differences, diagnostic tools, gender-specific symptom expressions, and support strategies for girls with ASD.
Results and discussion
The present study highlights how referral patterns disproportionately favor earlier identification of boys, who display more stereotypical and externalized symptoms, while girls are often overlooked due to subtler presentations and compensatory behaviors such as social imitation. The analysis of interviews revealed several key themes related to gender disparities in the assessment and diagnosis of ASD. These include differences in referral patterns between boys and girls, concerns about the suitability of current diagnostic tools, variations in symptom presentation, particularly the use of compensatory behaviors among girls—and the long-term impact of delayed diagnosis. The discussion below explores each of these themes in detail, drawing connections to existing research and highlighting implications for clinical and educational practice.
Referral differences
Findings from the study show that all special educators employed in BUP agree that there are more boys who are referred with suspicion of ASD to BUP, but also that boys are referred with suspicion of difficulties seen in connection with ASD at a much earlier time than girls. The participants also describe that girls who are referred to BUP with suspicion of ASD are often referred later, often in their teens, and often with a problem other than ASD, including anxiety, depression or eating disorders.
These findings are in line with previous research, which indicates significant gender differences in both referral and diagnosis patterns, with boys typically referred to and diagnosed at younger ages than girls. Similarly, the male-to-female diagnostic ratio is highest in early childhood (5.5:1) and narrows during adolescence (2.3:1), suggesting that many girls remain undiagnosed until later stages of development (Rutherford et al., 2016; Maenner et al., 2023). It can be shown here that the participants’ experience can be seen in the context of studies that were carried out internationally a few years ago, and that it can still show similar tendencies in Norway several years later in terms of number and age when looking at gender and ASD. Why the girls are not referred to and caught as early as the boys can be seen in the context of several possible reasons. Various hypotheses about the reason for this were also something that appeared in the data material for this study. The analysis of the data points out that one of these may be that girls and boys have different ways of playing and staying close to their peers.
Emma: "I believe that the reason for this lies in fundamental differences between boys' and girls' form of play, especially at kindergarten age. Boys stand out if they do not participate in the group, while girls are good at imitating others and also playing alongside without this being seen as deviant."
The descriptions given explain fundamental differences between boys’ and girls’ forms of play. Boys’ lack of participation in play with peers can be understood as an important factor in why it is relevant to assume that the boy may have difficulties regarding ASD. But when the girl can imitate and play alongside, this is not necessarily seen as deviant. Bühler (2020) argues that girls and boys with ASD experience play differently. Girls with ASD like to stay close to others or as part of a group of friends, but without participating on the same terms as the others. Dean et al. (2017) support the same understanding and describe that girls with ASD often show during recess and in arenas designed for playing with peers by staying close to peers, which means that their social difficulties seem less visible, while the boys isolate themselves to a greater extent and show more limited interests and repetitive behavior. In that way, it becomes easier to detect the social difficulties of boys with ASD, which also leads to a greater likelihood of referral to a specialist (Dean et al., 2017). It is therefore not sufficient that adults observe apparent friendship with other children because they spend time with them. If one is to assess children’s play, it is not enough to observe outdoor play and think that girls are included in friendships because they are surrounded by other children. As a professional, knowledge of girls with ASD in play and friendships is important to assess the quality of these relationships.
Overall, the findings from the study suggest that special educators at BUP experience a noticeable gender difference in the referral flow and diagnosis of ASD, where boys are referred at an earlier age than girls, and show more “typical” characteristics as the diagnosis suggests. The findings also show that the girls who are referred, especially the adolescents, present with additional problems such as anxiety, depression or eating disorders, which is in line with earlier research (Bargiela et al., 2016; Cage et al., 2018). The reason for the different referral style may be that boys show more serious difficulties that the support system believes need investigation, while girls may go unnoticed for a long time, before their difficulties are perceived as alarming enough to seek help and support from BUP.
Diagnostic tools for ASD
At BUP, various diagnostic tools are employed uniformly for all genders and across the autism spectrum. However, findings indicate professional concerns about the suitability and sensitivity of these tools for capturing ASD presentations among girls effectively.
Emma: "No, I don't think the diagnostic tools are good enough for both genders. They need a review if we are going to capture girls in a better way".
These statements highlight concerns that current diagnostic tools do not adequately capture ASD presentations in girls. Research also indicates that boys are four times more likely to be diagnosed with ASD than girls, raising concerns about potential underdiagnosis of girls in clinical settings. Improved understanding of how gender influences diagnosis is critical for enhancing early identification and intervention for girls with ASD (Duvekot et al., 2017).
Emma: "In order for the diagnostic tools to be more adapted to girls, I believe that you should not ask for special interests, but rather if there is something they are particularly concerned about. Rigidity often appears in them in a different way than in boys. They do not act out so easily, but become quiet, withdrawn and withdrawn. We may have to look for these as diagnostic features, not just think that girls are more modest than boys".
This statement suggests that the participants find it easier to identify boys due to stereotypical ASD characteristics, and that as a professional you must spend more time getting to know the patient, to understand their interests, and reasons for why they have the behavior and the difficulties they have. The participant also highlights the aspect of special interest. A characteristic of individuals with ASD is that they often have special interests, something that has not quite been able to be recognized to the same extent in girls. By shifting the focus from a special interest to what someone is particularly interested in or concerned about, one can better understand and meet the individual. Bühler (2020) also describes a way of understanding girls with ASD special interests. He describes that her interests can often be seen as an interest in animals, figures or celebrities, and are thus not so different from the interests of neurotypical girls. With a closer look, one can often see that the special interest is pronounced when looking at the scope and intensity of this interest. In this way, one can gain a better understanding that their symptom picture can be seen in connection with a possible ASD, and that gender can give a different expression in the child’s picture of difficulties than the stereotypical understanding of ASD.
Differences in symptom presentation between genders
The participants involved in this study generally agree that girls initially appear to possess better social interaction skills compared to boys.
Lise: "I think there is a significant difference between girls and boys with autism. Girls are generally better at social skills and communication. And they are often more mature than the boys are. So it is not right that we should rank them, or score them, equally. So there is quite a big difference in symptoms".
Research by Kaland (2019) supports this observation, showing that girls and women with ASD often appear more motivated to learn social norms and nuances, which can superficially make them seem more socially adept than they truly are. Many participants describe particularly notable gender differences in social awareness and communication.
Lise: "I think it's easier for girls to learn body language. And that they understand that you have to use eye contact, maybe must use some gestures. So yes, maybe girls have less stereotypical behavior, and body language, and things that one associates with autism".
The statement describes that girls can be experienced as showing better skills in social competence when it comes to basic stereotypical difficulties seen within ASD, such as difficulties with body language, eye contact and use of gestures. In contrast, the participant chooses to use words such as “learning” to use these skills within social interaction, instead of describing it as something that comes more naturally to girls than to boys with ASD.
Lise: "Yes. It does not come naturally to them; it is part of the diagnosis. But they have such an awareness of how one should be in order to be "neurotypical", and many would like to be like others. And then they are good at observing how others react in interaction, how they use their bodies, and it is not certain that it is conscious, it is unconscious. And then the others imitate. Learn how to react and use facial expressions and learn to recognize others' facial expressions. Because it is difficult with autism. Yes. And general body language like that, I think. That makes it even more difficult to catch these girls."
This emphasizes that autistic girls, like children generally, learn social skills through imitation rather than possessing them naturally, complicating diagnostic efforts.
Interestingly, the participant Emma provides a slightly different perspective on social challenges between genders.
Emma: "The social difficulty becomes very evident in both genders in the teenage years, but perhaps it is most prominent here in girls. Girls are often more verbal in their communication, so pressure also arises in relation to misunderstandings and being misunderstood often here. Boys often get into trouble because of the immaturity that comes with it, which means that they tend to lag behind in play longer than their peers. They are also often controlling in play because they need predictability and control, so they also get into conflicts more easily than their peers."
These observations suggest that girls experience increasingly pronounced social difficulties in adolescence. This aligns with Bühler (2020), who notes that social difficulties in girls become more apparent with age, particularly regarding friendship formation and maintenance (Kirkovski et al., 2013). This indicates that girls with ASD may show the greatest difficulties in forming and maintaining appropriate peer friendships, and that these difficulties become evident from teenage years. During adolescence, social interaction and relationships can be more complex for girls than for boys, which in turn can explain the greater socialization difficulties girls with ASD have compared to the boys. Also, disagreements seen in neurotypical children show that boys show a direct open confrontation, compared to girls who react in more indirect ways (Bowie, 2007; Noakes and Rinaldi, 2006). As Emma describes, she learns that the boys with ASD are controlling in play, and more easily end up in conflict than their peers (Nicholas et al., 2011). Boys with ASD who exhibit higher levels of conflict-seeking and acting-out behavior can be perceived as having a presentation of symptoms that attracts attention to a greater degree. At the same time, the superiority of the girls’ social skills decline relatively during adolescence, as they encounter more complex social settings which make compensatory strategies more difficult.
Compensatory behavior
As has been intimated, compensatory behaviors are a significant factor explaining delayed or missed ASD diagnoses, particularly in girls. Masking behaviors, involving social imitation, create the illusion of effective social functioning despite underlying challenges.
Lise: "There are clearly more girls who mask symptoms. They have better social awareness, generally speaking. And they might be better aware that they don't want to stand out, right. They want to be like the others in their group of friends. They will not struggle with anything. The girls are better at masking, quite simply. You see that in many situations. Both at the office, at school, at home, at handball training, at dancing."
Lise’s statement can be interpreted as that there are more girls who master behavior that can be described as social imitation or compensatory behavior. Because as Lise describes, it can be reflected that with increased social awareness, the chances of hiding or limiting one’s neurodivergent expressions also increase. Studies also refer to similar findings where Hull et al. (2017) describe that masking or social imitation is about maintaining a facade that does not show any obvious difficulties or to limit the visibility of one’s neurodivergent expressions. Several of the participants agree on the experience that girls master a behavior that can be seen in the context of compensatory behavior or masking as they describe it.
Emma: "Girls are probably far better at masking their symptoms than boys. This is another contributing factor to why they are discovered late. Girls are better at imitating others and thus they acquire both approximately adequate body language and eye contact. They generally mature faster than boys, and the maturational deviation may therefore not be so visible. They are also more interested in role-play and acquire a form of social competence through studying others in role-play"
Vilde: "Girls observe much more and try to imitate. Trying to do the same as they see others doing, then to be as "normal" as possible. I guess I have the impression that girls are more concerned with being more "normal" than boys. They don't want to stand out."
In analyzing the participant’s statements, she refers to the use of imitation for girls with ASD and uses terms such as “normal” up to several times. This raises issues as to how normality is constructed by society. Grue (2016), for instance, writes about normative prejudices, the concept that people with disabilities are inferior and in need of being “fixed” to conform with what is considered normal. In this way, girls’ experience of deviating from what is seen as typical, both in terms of neuronormativity and in terms of gender norms, lead to these girls with ASD not being able to be their authentic selves. In that case, society places high expectations on these girls that they must fit in with the community of the “average,” and these long-term compensatory attempts result in further psychological difficulties. With this interpretation in mind, it may be relevant to reflect on questions such as: Is it an ideal to be ordinary? Is it a goal that we should all be like each other? Can the ideal of equality prevent diversity? What about lifting inequality and diversity? (Morken, 2012, p.46). Because with an understanding that diversity and inequality are common, perhaps these girls have not experienced a society that requires learned behavior and compensation. With a focus on positive diversity, girls can be their authentic selves, and that this can prevent further additional difficulties triggered by compensation.
Furthermore, it is shown that findings from the data material from all participants involved show that they have the same experience when it comes to compensatory behavior as differences in symptom presentation between genders. Such findings lead to a reflection on whether it would be useful for clinicians to specifically as questions aimed at uncovering masking behaviors when girls are referred to BUP.
Lise: "Mhm, yes. I think that would have been very useful actually, because then you catch more of the girls who are struggling, but we just don't see it. Then there is a tendency to be expressed if you have masked for too long, that you get a kind of autistic "melt down".
What the participant is describing here is that compensatory behaviors are stressful to maintain, and that if they are maintained for too long, these stresses can mount until they lead to a crisis. This is an example that it is not necessarily an advantage for girls to show better social skills or master a behavior that makes them apparently hide their social difficulties, which is in line with the arguments of Bargiela et al. (2016).
Additional difficulties and functioning
Several descriptions from the participants indicate that girls and boys have different additional difficulties. Other descriptions from the participants are about the functioning of girls and boys with ASD in different parts of the developmental age.
Lise: "We often see autistic meltdowns in girls, who then go from functioning fairly stably, mastering most things in life to having a really big loss of function, going down really hard and appearing very autistic. And then everyone around becomes very worried, because what is happening here, it can't be autism, because suddenly it has become like that. Then you become very confused and do not fully understand what is happening. It is also because the girls have become very stressed, in the face of life in general. They are more vulnerable to stress aren't they. And have a greater tendency to develop additional difficulties. Due to the fact that they may mask or feel a little stress and that they are not good at social things, but would like to be".
The findings from the data material are interpreted as what appears as a result of the girls having used compensatory behavior over many years, masking their symptoms. Suddenly these teenage girls can be seen with a major decline in function, and those who have apparently functioned relatively well for many years are seen as adolescent girls with major and complex difficulties. Hull et al. (2017) refer to these additional difficulties and the results compensatory behavior can have. Compensatory behavior can be associated with high levels of stress, low self-esteem, and several girls with ASD also report extensive depression and anxiety as the compensation is experienced as exhausting. Several girls with ASD also report a need to withdraw after long-term compensation, which can be seen in connection with the participant’s information about sudden and major functional decline.
Descriptions from Vilde also refer to different views on the appearance of symptoms and functional decline seen in girls. Vilde has previously described experiences of boys being referred to at an early stage compared to girls who are usually referred to in their teens. Interpretations from her previous descriptions indicate that boys are referred earlier due to social and behavioral difficulties.
Vilde: "It's a bit like, it's like we were in place. Those boys may have more behavioral difficulties, while girls have more internalized difficulties, perhaps. Anxiety, depression, staying at home in bed. Perhaps to a greater extent than boys".
Findings from the analysis show that the boys who show a greater degree of disruptive behavior are often referred to BUP earlier, while girls tend to go unnoticed through childhood, and use compensatory behavior to cope with everyday situations. When compensatory behavior is experienced by the girls over a long period of time, this can lead to internalizing difficulties, such as anxiety and depression which lead to referral, but then the decline in functioning can already be so great that girls experience school refusal and severe “meltdowns.”
Descriptions that Vilde gives can be confirmed through theory which assumes that girls with ASD show to have internalizing difficulties, such as anxiety and depression, but not externalizing difficulties such as impulse difficulties and behavioral problems (Bargiela et al., 2016). When girls then do not show tendencies to behave in ways that are perceived as disruptive at school, it is also less likely that they will be referred to for their internalizing difficulties, which can overshadow an underlying ASD diagnosis (Bargiela et al., 2016). These findings created reflections for us as researchers on whether there are possibilities that girls do not show as severe a pressure of symptoms in what we know as standardized symptoms for ASD, but that girls can still show a greater decline in function over time. This resulted in follow-up questions to Vilde.
Interviewer: "So even though girls may not show as many symptom expressions, in the end they become more absent from school and perhaps have a greater decline in function then, actually? Even if the symptoms seem to be fewer?”
Vilde: "Yes. I think that girls, both consciously and unconsciously, try to mask or hide their difficulties to a far greater extent than boys".
Findings from the data material can show that girls can often be referred or also apparently show the greatest difficulties regarding its additional difficulties that can make it difficult for clinicians to identify an underlying ASD. Findings from the participant “Vilde” indicate that both masking and additional difficulties can make it more demanding for clinicians to identify girls with ASD, but also to be confident of the correct diagnosis. Examples are further described of typical girls with ASD who have gone for a long time with other diagnoses first, before the underlying difficulty behind the additional difficulties is seen. Additional difficulties seen in girls with ASD are described by the participants Vilde and Lise.
Vilde: “Anxiety, depression, PTSD, eating disorder. But then perhaps we actually think that the diagnosis of autism is the most fundamental difficulty. Which has caused the other difficulties".
Vilde’s statements related to how the diagnosis of ASD can lead to comorbid disorders resulted in follow-up questions regarding how ASD in girls can trigger difficulties such as, for example, PTSD. Vilde then goes on to describe that girls with ASD may have a greater likelihood of ending up in situations that make them vulnerable to sexual abuse. This is through the fact that they have difficulty interpreting other people’s body language, and with the possibility that they imitate someone else’s sexual intention, without realizing it themselves. The study by Bargiela et al. (2016) investigates the incidence of sexual abuse among girls with ASD and describes an incidence of over 60%. Causal relationships are also described in this survey along the same lines as the participant says, with difficulty interpreting the intentions of others, and unconscious imitation of a man’s flirtatious behavior. These findings lead to reflections and interpretations to the extent that if girls with difficulties regarding ASD receive early intervention and psychoeducation for the disorder, then their difficulties can be guided, and girls can be made aware of what social difficulties can entail in relation to others and it is explained that they can be extremely vulnerable to abuse. It should be pointed out that the blame for sexual abuse never lies with the abused, but knowledge and information about future incidents can be preventive.
Additional findings from the analysis refer to statements from Lise who also highlight various additional difficulties girls with ASD can have, and how long-term difficulties relating to ASD can affect comorbid disorders and major functional difficulties.
Lise: "It's mostly anxiety, depression, I think, that comes to my mind first. But also more serious things, such as symptoms of psychosis for example. It is not unusual for us to see girls with autism".
Several examples from the participants describe neurotypical girls with major functional decline, and who often show several additional difficulties of a serious degree. The study from Hull et al. (2017) shows that behavior that is used to mask one’s neurodivergent expressions is used to better fit into society and due to a social expectation from the population that individuals with ASD must change in order to be accepted by others. The study further shows that the compensatory behavior used can lead to great exhaustion, anxiety, depression, the need to seek isolation and result in confusion of one’s own identity. Descriptions from these studies can be seen in connection with findings made in this study, and further show that it is also reported here that girls with ASD show a larger complex picture of difficulties with anxiety, depression, a need for isolation, but also confusion of their own identity which can possibly be linked to psychotic symptoms.
Lise: "We have many examples here at BUP. A typical fourteen-fifteen-year-old girl, who has a sudden functional impairment, experiences a lot of anxiety, depression, self-harm, suicidal thoughts, maybe some attempt, right? Being admitted to the inpatient unit, coming in here, so the first thing we see are the symptoms. And then we map out the worst in a way. Is there psychosis here, is it trauma perhaps, is it clinical depression. Is it severe anxiety. What has happened here? There is also an underlying Asperger's, autism diagnosis. Often".
Both findings from data collection for the participants and previously described theory can point to complex difficulties and are interpreted to mean that the assessment process for girls with ASD can be more extensive and time-consuming than for boys with ASD. These interpretations can also be seen in connection with findings explained in the theory section, which show that girls are often diagnosed later than boys, but also that the investigation process itself is more time-consuming than what is seen in boys with ASD.
Overall, the findings demonstrate significant gender differences in ASD symptom presentations. Girls initially appear socially competent due to compensatory behaviors but experience significant functional decline and severe secondary difficulties as they age. Boys, in contrast, are typically diagnosed earlier due to more overt externalizing symptoms.
Better support for girls with ASD
In considering how to better support girls with ASD, the participants expressed agreement that more understanding and knowledge about girls with ASD is still needed.
Vilde: “It has been shown recently that girls have a different expression, and it is good that it is coming out more in terms of desire. There are quite a few girls who have come forward, or ladies. Which describes how they have been growing up. Then you describe many of the things we have talked about, that they have struggled somewhat to understand themselves. So that you could have avoided many things, many difficulties, if you had known at a much earlier stage what was wrong with them.”
Lise: “I think more knowledge about what it means to have autism for girls. There must be a basis there – Because there are many. This essentially applies to all neurodiagnoses. But especially autism. What does it mean for girls to have autism? And be aware of the symptoms, catch them early so that we don’t see this skewed development.”
The statements highlight the importance of understanding what ASD means within a gender perspective. With increased knowledge and insight, girls can be identified earlier and receive help when they need it. A deeper understanding of the female ASD profile is essential. Without this, girls risk being misdiagnosed or not diagnosed at all, and may miss interventions that could improve their quality of life (Kirkovski et al., 2013). Participants point out that current diagnostic tools are not equally suited across genders, and this may contribute to girls not being identified properly.
Lise: “Things have to be renewed, and we know more about autism symptoms in girls now. But it doesn’t show up in mapping and the test situations that we still use.”
Participants suggest that even though knowledge has improved, the tools used in assessments are outdated, often favoring males. This makes clinicians rely more on observation and professional judgement. The longer diagnostic process for girls indicates a need to improve gender-relevant tools and assessment routines. Late referrals also highlight the importance of increased awareness of how ASD presents in girls (Rutherford et al., 2016).
Lise: “There is a lot missing in the understanding of girls with autism, I think. There is also so little to be gained from research, and it becomes a bit like that, a few drops here and there. But it’s not really something very concrete to use.”
Participants express concern about the lack of research on girls with ASD. This is supported by Duvekot et al. (2017), who argue that research has mainly included boys, which may have shaped our current understanding and criteria in a way that is biased.
Emma: “More research needs to be done on girls and ASD. It is also important that girls and women with ASD get a voice in the research because they are the ones who know the difficulties and the problems best.”
There is a need to listen more to girls and women with ASD and include their voices in research. They can describe how their difficulties are experienced, helping us understand how ASD is expressed across genders. With girls being underrepresented in research, earlier help may be missed. Timely identification of ASD can reduce emotional, behavioral and social difficulties, and improve quality of life through access to appropriate support. It may also promote acceptance and better identity understanding (Bargiela et al., 2016).
Vilde: “There also needs to be more knowledge in the first line. To recognize the basic difficulties, so that they are actually referred here before they develop additional difficulties”.
The analysis also shows the importance of understanding ASD in frontline services. With increased awareness, it becomes easier to detect signs early and refer for further assessment. As girls are often overlooked or misunderstood as shy, withdrawn or rude (Bargiela et al., 2016), greater awareness in schools would make it easier to recognize potential ASD and provide the right support.
Vilde has worked in specialist health services her whole career. She shares an example of a girl she followed over time:
“I think she was seventeen when she was diagnosed with ASD. She herself thinks that if it had been a trained eye that had seen her in first grade, it would have been obvious that she had autism. She also says that she had great difficulties when she went to kindergarten, which was not discovered. In that sense, it could have been picked up already in kindergarten. And she said that the mother tried and tried and tried to get someone to see what was difficult. She has had many rounds at BUP, and received other diagnoses first. Then she was almost an adult before she got the correct diagnosis. She ended up going to long-term therapy. Then she became so confident in herself that she could go out and tell about it. Now she has a family and children. She struggles a little to understand her children, but she manages a lot! She had a child early. The mother thinks it’s about her not fully understanding what was going on. Before she was kind of in the middle of it. But it has gone well. She also has a higher education!”
The further supports that importance of understanding the female ASD profile. Girls may be misdiagnosed with other conditions and go through long assessments. With a correct diagnosis, they can receive targeted support, gain self-understanding, and schools and parents can be better informed. Chahboun et al. (2021) describe how a diagnosis can shape both self-image and how others view the person. It can provide access to help but may also lead to exclusion. How ASD is presented in society strongly influences how individuals are treated. With more insight and less stigma, ASD can be seen as part of human diversity. Then autistic individuals can be themselves—without the pressure to mask or fit in.
Findings related to better support for girls with ASD point to the need for more research and understanding of how ASD presents in girls. By listening to girls’ and women’s voices, we can improve diagnostic tools and make the assessment process more inclusive. This will help ensure earlier support and reduce long, unnecessary assessment processes and secondary difficulties.
Conclusions, limitations and future directions
This study investigates the experiences and competence of special education teachers in assessing girls with ASD. The study demonstrated gender disparities in recognition, diagnosis, and support persist in Norway’s mental health services. The findings reveal significant gender differences in ASD symptom expression. Girls with ASD often present subtler symptom profiles, use compensatory behaviors, and experience delayed referrals, leading to later diagnoses and greater risk of secondary psychological conditions. Boys are more likely to be referred and diagnosed earlier due to disruptive behaviors, while girls are often overlooked until adolescence, when secondary issues such as anxiety, depression, or eating disorders arise. Girls’ subtler symptoms and compensatory behaviors like masking, contribute to delayed diagnoses, as current diagnostic tools are insufficiently adapted to identify girls with ASD. These challenges highlight the need for improved diagnostic approaches, greater awareness among educators and clinicians, and the inclusion of girls’ voices in research to better understand their experiences. Early intervention can reduce psychological difficulties and improve quality of life.
The study emphasizes viewing ASD through the framework of diversity and advocates for increased knowledge and competence across education and healthcare to support children and youth inclusively and effectively. The focus on normativity impacts girls twice, as they also fall greater victim to the expectations around gender norms. The findings stress the need for gender-sensitive diagnostic tools, improved understanding of girls’ ASD phenotype, and earlier intervention. Incorporating girls’ and women’s voices in research can foster more inclusive diagnostics, reduce stigma, and enhance outcomes across ASD.
One topic that emerged over and over again, both as a reason for why girls remained under-diagnosed, and which became a significant source for their negative mental health outcomes, was their compensatory behavior. At the same time, the participants suggested that a set of questions designed to uncover such behavior would be helpful for them in their work. Future research would do well to investigate how such behaviors can be “unmasked,” so that the girls can be correctly diagnosed at an earlier date. This would be complicated by suggestions in prior research that such strategies evolve over time. This would call for longitudinal research examining how girls’ compensatory behaviors manifest at different ages and affect diagnosis, mental health, and educational outcomes. Furthermore, future research should focus on developing gender-sensitive screening practices, including diagnostic tools and guidelines that reflect diverse ASD profiles. This should not be limited to the gender binary, but take a gender-diverse perspective. Involving autistic individuals in the development of these tools will help ensure their relevance and inclusivity.
Author contributions
KF: Writing – original draft, Writing – review & editing. AP: Writing – review & editing. CL: Writing – review & editing. SC: Writing – review & editing, Supervision.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/journals/education/articles/10.3389/feduc.2025.1552943/abstract#supplementary-material
References
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders. 5th Edn. Washington, DC: American Psychiatric Association.
Bargiela, S., Steward, R., and Mandy, W. (2016). The experiences of late-diagnosed women with autism spectrum conditions: an investigation of the female autism phenotype. J. Autism Dev. Disord. 46, 3281–3294. doi: 10.1007/s10803-016-2872-8
Bowie, B. H. (2007). Relational aggression, gender, and the developmental process. J. Child Adolesc. Psychiatr. Nurs. 20, 107–115. doi: 10.1111/j.1744-6171.2007.00092.x
Bühler, M. (2020). Flickor med autism och ADHD: En guidebok för föräldrar och professionella. Lund, Sweden: Studentlitteratur.
Burns, J., and Tierney, S. (2023). “Beyond the mask: the role of camouflaging in managing an autistic identity for girls and women” in Principles of gender-specific medicine. ed. M. Legato (Amsterdam: Elsevier), 805–819.
Cage, E., Di Monaco, J., and Newell, V. (2018). Experiences of autism acceptance and mental health in autistic adults. J. Autism Dev. Disord. 48, 473–484. doi: 10.1007/s10803-017-3342-7
Chahboun, S., Stenseng, F., and Page, A. (2021). The changing faces of autism: the fluctuating international diagnostic criteria and the resulting inclusion and exclusion – a Norwegian perspective. Front. Psych. 12. doi: 10.3389/fpsyt.2022.787893
Cruz, S., Zubizarreta, S. C. P., Costa, A. D., Araújo, R., Martinho, J., Tubío-Fungueiriño, M., et al. (2024). Is there a bias towards males in the diagnosis of autism? A systematic review and meta-analysis. Neuropsychol. Rev. 35, 153–176. doi: 10.1007/s11065-023-09630-2
Dean, M., Harwood, R., and Kasari, C. (2017). The art of camouflage: gender differences in the social behaviors of girls and boys with autism spectrum disorder. Autism 21, 678–689. doi: 10.1177/1362361316671845
Duvekot, J., van der Ende, J., Verhulst, F. C., Slappendel, G., van Daalen, E., Maras, A., et al. (2017). Factors influencing the probability of a diagnosis of autism spectrum disorder in girls versus boys. Autism 21, 678–689. doi: 10.1177/1362361316672178
Dwyer, P. (2022). The neurodiversity approach(es): what are they and what do they mean for researchers? Hum. Dev. 66, 73–92. doi: 10.1159/000523723
Fombonne, E. (2009). Epidemiology of pervasive developmental disorders. Pediatr. Res. 65, 591–598. doi: 10.1203/PDR.0b013e31819e7203
Halladay, A. K., Bishop, S., Constantino, J. N., Daniels, A. M., Koenig, K., Palmer, K., et al. (2015). Sex and gender differences in autism spectrum disorder: summarizing evidence gaps and identifying emerging areas of priority. Mol. Autism. 6:36. doi: 10.1186/s13229-015-0019-y
Hull, L., Lai, M. C., Baron-Cohen, S., Allison, C., Smith, P., Petrides, K. V., et al. (2020). Gender differences in self-reported camouflaging in autistic and non-autistic adults. Autism 24, 352–363. doi: 10.1177/1362361319864804
Hull, L., Mandy, W., and Petrides, K. V. (2016). Behavioural and cognitive sex/gender differences in autism spectrum condition and typically developing males and females. Autism 21, 706–727. doi: 10.1177/1362361316669087
Hull, L., Petrides, K. V., Allison, C., Smith, P., Baron-Cohen, S., Lai, M.-C., et al. (2017). "Putting on my best normal": social camouflaging in adults with autism spectrum conditions. J. Autism Dev. Disord. 47, 2519–2534. doi: 10.1007/s10803-017-3166-5
Hull, L., Petrides, K. V., and Mandy, W. (2019). Understanding camouflaging as a response to autism-related stigma: a social identity theory approach. J. Autism Dev. Disord. 49, 892–902. doi: 10.1007/s10803-018-3741-6
Hutson, P., and Hutson, J. (2023). Autism in females: understanding the overlooked diagnoses, unique challenges, and recommendations. J. Clin. Med. Images 3. doi: 10.1007/978-1-0716-0882-4_61
Kaat, A. J., Shui, A. M., Ghods, S. S., Farmer, C. A., Esler, A. N., Thurm, A., et al. (2021). Sex differences in scores on standardized measures of autism symptoms: a multisite integrative data analysis. J. Child Psychol. Psychiatry 62, 97–106. doi: 10.1111/jcpp.13242
Kaland, N. (2019). Autisme og kjønn: Kognitive forskjeller mellom jenter/kvinner og gutter/menn med ASD. Psykologi i Kommunen, 1, 39–50. Available online at: https://www.researchgate.net/publication/333323804
Kirkovski, M., Enticott, P. G., and Fitzgerald, P. B. (2013). A review of the role of female gender in autism spectrum disorders. J. Autism Dev. Disord. 43, 2584–2603. doi: 10.1007/s10803-013-1811-1
Kvale, S., and Brinkmann, S. (2015). Det kvalitative forskningsintervju. 3rd Edn. Oslo, Norway: Gyldendal.
Lai, M. C., and Szatmari, P. (2020). Sex and gender impacts on the behavioural presentation and recognition of autism. Curr Opin Psychiatry. 33, 117–123. doi: 10.1097/YCO.0000000000000575
Lai, M. C., Lombardo, M. V., Auyeung, B., Chakrabarti, B., and Baron-Cohen, S. (2015). Sex/gender differences and autism: setting the scene for future research. J Am Acad Child Adolesc Psychiatry. 54, 11–24.
Livingston, L. A., Shah, P., and Happé, F. (2019). Compensatory strategies below the surface in autism: a qualitative study. Lancet Psychiatry 6, 766–777. doi: 10.1016/S2215-0366(19)30224-X
Lonergan, R. M. (2021). Gender balance in the validation of diagnostic tools for autism: a systematic review. Eur. Psychiatry 64:S599. doi: 10.1192/j.eurpsy.2021.1598
Loomes, R., Hull, L., and Mandy, W. P. L. (2017). What is the male-to-female ratio in autism Spectrum disorder? A systematic review and meta-analysis. J. Am. Acad. Child Adolesc. Psychiatry 56, 466–474. doi: 10.1016/j.jaac.2017.03.013
Maenner, M. J., Shaw, K. A., Bakian, A. V., Bilder, D. A., Durkin, M. S., and Esler, A., … Cogswell, M. E. (2023). Prevalence and characteristics of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2020. MMWR Surveill. Summ. 72, 1–14. Available at: https://www.cdc.gov/mmwr/volumes/72/ss/ss7202a1.htm?s_cid=ss7202a1_w.
Mathisen, J. R. (2016). Jenter har flest autisme-symptomer. Kilden Kjønnsforskning. Available online at: https://kjonnsforskning.no/nb/2016/11/jenter-har-flest-autisme-symptomer (Accessed December 1, 2024).
McDonnell, C. G., DeLucia, E. A., Hayden, E. P., Penner, M., Curcin, K., Anagnostou, E., et al. (2021). Sex differences in age of diagnosis and first concern among children with autism spectrum disorder. J. Clin. Child Adolesc. Psychol. 50, 645–655. doi: 10.1080/15374416.2020.1766183
McQuaid, G. A., Pelphrey, K. A., Bookheimer, S. Y., Dapretto, M., Webb, S. J., Bernier, R. A., et al. (2021). The gap between IQ and adaptive functioning in autism spectrum disorder: disentangling diagnostic and sex differences. Autism 25, 1565–1579. doi: 10.1177/1362361321994013
Morken, I. (2012). Normalitet og avvik: Spesialpedagogiske utfordringer – En innføring. 2nd Edn. Oslo, Norway: Cappelen Damm Akademisk.
Navarro-Pardo, E., López-Ramón, M. F., Alonso-Esteban, Y., and Alcantud-Marín, F. (2021). Diagnostic tools for autism spectrum disorders by gender: analysis of current status and future lines. Children 8:262. doi: 10.3390/children8040262
Nicholas, S., Moravcik, G. M., and Tetenbaum, S. P. (2011). Autisme hos jenter: Det foreldre og fagfolk bør vite om oppvekst og pubertet. Oslo, Norway: SPISS Forlag.
Noakes, M. A., and Rinaldi, C. M. (2006). Age and gender differences in peer conflict. J. Youth Adolesc. 35, 881–891. doi: 10.1007/s10964-006-9088-8
Rutherford, M., McKenzie, K., Johnson, T., Catchpole, C., O'Hare, A., McClure, I., et al. (2016). Gender ratio in a clinical population sample, age of diagnosis and duration of assessment in children and adults with autism spectrum disorder. Autism 20, 628–634. doi: 10.1177/1362361315606187
Stave, T. K. (2022). Vi må bli bedre til å tolke symptomer på autisme og ADHD hos jenter. Kilden Kjønnsforskning. Available online at: https://kjonnsforskning.no/nb/2022/02/vi-ma-bli-bedre-til-tolke-symptomer-pa-autisme-og-adhd-hos-jenter (Accessed December 1, 2024).
Thagaard, T. (2018). Systematikk og innlevelse: En innføring i kvalitative metoder. 5th Edn. Bergen, Norway: Fagbokforlaget.
Tierney, S., Burns, J., and Kilbey, E. (2016). Looking behind the mask: social coping strategies of girls on the autistic spectrum. Res. Autism Spectr. Disord. 23, 73–83. doi: 10.1016/j.rasd.2015.11.013
Warrier, V., Greenberg, D. M., Weir, E., Buckingham, C., Smith, P., Lai, M. C., et al. (2020). Elevated rates of autism, other neurodevelopmental and psychiatric diagnoses, gender-diverse individuals. Nat. Commun. 11, 1–12.
Whiteley, P., Todd, L., Carr, K., and Shattock, P. (2010). Gender ratios in autism, asperger syndrome and autism spectrum disorder. Autism Insights 2, 17–24. doi: 10.4137/AUI.S4085
Wood-Downie, H., Wong, B., Kovshoff, H., Mandy, W., Hull, L., and Hadwin, J. A. (2021). Sex/gender differences in camouflaging in children and adolescents with autism. J. Autism Dev. Disord. 51, 1353–1364. doi: 10.1007/s10803-020-04615-z
World Health Organization. (2018). ICD-11: the 11th revision of the international classification of diseases. Available online at: https://icd.who.int/browse11/l-m/en (Accessed December 1, 2024).
World Health Organization. (2023). ICD-10: Den internasjonale statistiske klassifikasjonen av sykdommer og beslektede helseproblemer. Available online at: https://finnkode.ehelse.no (Accessed December 1, 2024).
Glossary
BUP (Child and Adolescent Psychiatry Services) - A public mental health service in Norway that provides assessment and treatment for children and adolescents with mental health difficulties (Norwegian: Barne-og ungdomspsykiatrisk poliklinikk).
Barneblikk - A Norwegian interdisciplinary initiative focusing on early identification and support for children in families where parents struggle with mental health or substance abuse. The goal is to ensure children are seen, heard, and supported.
Treatment Neuro-Nevo Team - A multidisciplinary clinical team that provides specialized treatment and follow-up for children and adolescents with complex neurodevelopmental or neurological conditions, typically within BUP or related services.
Neuroteam - A specialized interdisciplinary team focused on the assessment and support of individuals with neurodevelopmental disorders, such as ASD, ADHD, or intellectual disabilities.
ADOS (Autism Diagnostic Observation Schedule) - A standardized diagnostic tool used to assess social interaction, communication, and play in individuals suspected of having ASD. It is often used as part of a comprehensive diagnostic process.
WISC-IV (Wechsler Intelligence Scale for Children – Fourth Edition) - A widely used intelligence test designed to measure cognitive ability in children aged 6 to 16. It assesses verbal comprehension, perceptual reasoning, working memory, and processing speed.
ABAS (Adaptive Behavior Assessment System) - An assessment tool that evaluates adaptive functioning in individuals by measuring skills in areas such as communication, daily living, and social interaction. It is often used in the diagnosis of developmental or intellectual disabilities.
Keywords: autism spectrum disorder (ASD), gender differences, diagnostic practices, female autism phenotype, compensatory behavior, mental health services, Norway, special education
Citation: Fredriksen KL, Page AG, Lindhardt C and Chahboun S (2025) Unmasking autism: gender differences in diagnostic practices and challenges in Norway’s mental healthcare services for children and youth. Front. Educ. 10:1552943. doi: 10.3389/feduc.2025.1552943
Edited by:
Wing Chee So, The Chinese University of Hong Kong, ChinaReviewed by:
Friederike Charlotte Hechler, University of Potsdam, GermanyCaroline Mårland, University of Gothenburg, Sweden
Copyright © 2025 Fredriksen, Page, Lindhardt and Chahboun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sobh Chahboun, c2NoQGRtbWgubm8=