 Nikolai Zinke
Nikolai Zinke Anne Ritz1
Anne Ritz1 Nico Bunzeck
Nico Bunzeck- 1University of Lübeck, Lübeck, Germany
- 2Center of Brain, Behavior and Metabolism, University of Lübeck, Lübeck, Germany
Introduction: University students are experiencing more and more stress, which can negatively impact their mental health. Therefore, new ways are needed to address this issue. To this end, we examined the effectiveness of an app-delivered mindfulness-based stress training and a possible interaction with additional group meetings within a university setting.
Methods: A randomized mixed experimental design was used to assess an 8-weeks Mindfulness-Based Intervention (MBI) delivered via podcasts and supplemented by group meetings, either in video calls (VC) or a virtual reality (VR) environment. The intervention aimed to improve mental health, focusing on risk factors stress and loneliness as well as protective factors such as self-compassion and self-efficacy.
Results: Our results indicated partial overall effectiveness of the MBI, with significant reductions in stress experience and loneliness and increases in self-compassion, yet all at the facet level. Exploratory analyses revealed that group meetings enhanced mindfulness, which in turn contributed to stress reduction, but the relationships of VR immersion and stress reduction yielded mixed results.
Discussion: Our findings give novel insights into how the specific positive effects of the MBI might interact with digital group meetings, which could pave the way for further research with optimized intervention settings.
Introduction
Mental health in higher education has become a critical concern, especially since the onset of COVID-19, where lockdowns had a direct impact on the way we socially interact. As a result, stress levels among young adults have surged, leading to increased depression, anxiety, and psychosomatic symptoms (Madigan et al., 2023). Students also face stress from the transition to university and persistent challenges including academic workload, financial concerns, and performance pressure (Hill et al., 2018). Therefore, stress-reducing psychological support programs, as well as their empirical evaluation (Amanvermez et al., 2023; Yusufov et al., 2019), are of great importance especially for student populations. In this context, digital learning expands implying a growing demand for accessible digital mental wellbeing initiatives (Haleem et al., 2022). Indeed, innovative approaches, such as serious games, not only offer novel ways to socially interact, but they also can enhance therapeutic strategies for emotional wellbeing (David et al., 2020). This study aims to bridge the gap between stress-reducing mental health programs and digital social interaction by examining the effectiveness of a digital mindfulness-based intervention delivered via the 7Mind® app. The study focuses on both risk-related and protective mental health outcomes and also investigates whether digital group meetings held via conventional video calls or a virtual reality (VR) environment enhance the effectiveness of the intervention.
Mindfulness, defined by Kabat-Zinn (2003) as “the awareness that emerges through paying attention on purpose, in the present moment, and nonjudgmentally to the unfolding of experience moment by moment” (p. 145), is central to the mindfulness-based stress reduction (MBSR) approach. Developed for patients with physical symptoms (Kabat-Zinn, 1982), such as chronic pain, MBSR is an 8–10-week course with weekly 2-h sessions, combining meditation, physical exercises, and Hatha yoga. Its efficacy is comparable to cognitive-behavioral therapy (CBT) for anxiety reduction (Yusufov et al., 2019) and equivalent to treatments such as escitalopram (Hoge et al., 2023). Moreover, MBSR has also been shown to reduce loneliness (Teoh et al., 2021) and improve confidence in managing it (Besse et al., 2022), which is characterized by dissatisfaction with social relationships. Importantly, loneliness is particularly prevalent among young (and older) adults (Victor and Yang, 2012; Hawkley et al., 2022) and has been linked to physical and psychological risks, including increased mortality and immune dysfunction (Holt-Lunstad et al., 2015).
Apart from positive effects on health-risk outcomes, such as stress, anxiety and depression (Grossman et al., 2004; McConville et al., 2017), MBSR can also impact on health-protective outcomes. For instance, mindfulness-based interventions have been shown to increase self-compassion (Kriakous et al., 2021), which is crucial for mental wellbeing and can be defined as the ability to treat oneself kindly in difficult situations. Resilience, i.e., the capacity to adapt to stress, can also be improved through mindfulness training by promoting emotion regulation and reducing over-identification with stressors, as seen in nursing staff (Lin et al., 2019). Furthermore, MBSR can increase self-efficacy (i.e., the belief in one's ability to influence outcomes), leading to reduced stress and anxiety in various populations, including migraine patients (Wells et al., 2021). Finally, life satisfaction can also be improved by mindfulness practices (Aşik and Albayrak, 2022).
Findings from several systematic reviews and meta-analyses support the effectiveness of MBSR interventions among university students. Dawson et al. (2020) reported small to moderate effect sizes for improvements in stress reduction and psychological wellbeing (e.g., anxiety, depression, overall wellbeing), though questions remain about the suitability of digital delivery formats for student populations. Zuo et al. (2023) confirmed the efficacy of MBSR for addressing anxiety, depression, and stress in university students, but highlighted heterogeneity in delivery formats and a lack of comparative evidence between app-based and traditional approaches. Similarly, Chiodelli et al. (2022) emphasized variability in implementation fidelity and noted that modern technology platforms such as mobile apps and VR remain underutilized. Collectively, these reviews underscore the university context and indicate the growing need for (a) scalable, tech-integrated interventions, (b) rigorous evaluations of app-based MBSR in academic settings, and (c) further investigations of the role of group support mechanisms.
In recent years, app-delivered mindfulness programs have emerged as cost-effective, flexible alternatives to in-person courses. Although they are well-suited to the busy lifestyles of university students, current research only provides preliminary evidence for their effectiveness. For example, Huberty et al. (2019) showed that the “Calm” app reduced stress and increased mindfulness and self-compassion in highly stressed students. Another study showed promising results for online MBSR during COVID-19 (Riley et al., 2022). However, high dropout rates and small sample sizes remain persistent issues. For instance, Alrashdi et al. (2023) conducted a meta-analysis focusing on university students and found notable attrition, often due to a lack of engagement and support mechanisms. Similarly, Linardon (2023) reported weighted meta-analytic attrition rates in app-based mindfulness trials and highlighted the urgent need for improved retention strategies. Moreover, methodological shortcomings such as the lack of control groups and non-randomized designs hinder the interpretability of outcomes. Spijkerman et al. (2016) and Sommers-Spijkerman et al. (2021) emphasize these flaws and stress the need for rigorous randomized controlled trials with clear and comparable conditions.
While app-based courses offer several advantages, they also face challenges due to the lack of social interaction and direct trainer guidance, which may impact adherence and engagement. To enhance engagement and effectiveness, various strategies have been proposed, including the use of digital group meetings and immersive technologies. Winter et al. (2022) reviewed adherence-boosting methods and found that personalized reminders, guided facilitation, and community-based platforms can significantly improve retention rate. Virtual community interventions, as explored by El Morr et al. (2020), and group-facilitated sessions with VR components (Krägeloh et al., 2019), also showed promise for increasing both adherence and psychological benefits, though often in small pilot samples.
Professional guidance has been shown to improve adherence in online interventions (Musiat et al., 2022), which indicates that additional, regular (online) group meetings could facilitate the effectiveness of an app-based MBSR intervention. This could be achieved by promoting social support and collective self-efficacy, which are both key for stress reduction (Cruwys et al., 2020; Yusufov et al., 2019). In practical terms, digital group meetings may be conducted via conventional video call software (as represented in 2D, e.g., on a laptop monitor) or alternatively, within a VR environment (as represented in 3D on VR glasses). The latter offers an innovative way to enhance mindfulness by creating immersive environments and enables the user to explore computer-generated worlds that simulate real-life experiences, potentially enhancing the emotional and sensory impact of mindfulness training (Turner and Casey, 2014). Research also suggests that VR-based mindfulness may be more effective than traditional methods (Ma et al., 2023), or at least promote adherence (Modrego-Alarcón et al., 2021). More generally, VR may promote learning through enhanced motivation and engagement, especially among younger students (Jiang and Fryer, 2024; Lin et al., 2024).
The present study focuses on the 7Mind® course, an eight-week online intervention delivered via 45-minute podcasts (see Methods). While the program was certified as a MBSR prevention program by the Central Prevention Testing Center (ZPP) (course ID: KU-ST-NAKHWV) and followed an 8-week structure and incorporated guided meditations and thematic content, it should be considered an MBSR-inspired rather than a fully standardized MBSR intervention. Therefore, we call it Mindfulness-Based Intervention (MBI). For additional details, see Supplementary material. Initial research, using the same app intervention, has shown promising but mixed results (Karing, 2024). Specifically, it revealed positive effects of the 7Mind®app on several measures, including mindfulness, emotion regulation, and stress over a short, medium and long-term. However, there were no significant differences compared to other conditions (including a face-to-face mindfulness intervention alone, a combination with the app, and an active control condition).
Taken together, mindfulness-based interventions can have positive effects on mental wellbeing but the effectiveness of app-based interventions are less clear. Moreover, social interactions via digital group meetings may further promote motivation and adherence to mindfulness practices. Therefore, we hypothesize (a) that the online MBI using the 7Mind®app will have beneficial effects compared to a control group, specifically by reducing health risks and strengthening health-protective outcomes (H.1); (b) that regular group meetings will enhance the course's effectiveness (H.2); and (c) that integrating VR into group meetings will further boost effectiveness (H.3). Additionally, we pose two exploratory questions. E.1: Does mindfulness mediate the course's effects on health-related outcomes? Mindfulness has been shown to reduce stress and improve mood (Keng et al., 2012; Birnie et al., 2010). E.2: Does VR immersion intensity correlate with intervention effectiveness, as it may increase emotional engagement and adherence (Modrego-Alarcón et al., 2021)? This interventional study was conducted with psychology students from the University of Lübeck, integrated into their curriculum.
This study was not preregistered in a formal registry, but a detailed study protocol, along with ethical approval, the dataset, codebook, and R analysis code, is available on OSF: https://osf.io/zs9xe/files/osfstorage.
Method
Procedure
The study began with a preparation meeting (about 80 Min) including an information brochure and the possibility to ask questions. The investigator (A.R.) explained eligibility criteria, emphasizing voluntary participation and the option to withdraw without giving reasons. After signing consent forms, participants downloaded the 7Mind® app (7Mind®, 2024) and received instructions. Those in group meetings received organizational details, while VR participants were introduced to the Meta Quest 2 headset and Horizon Workrooms software (Meta, 2024). Loaned headsets allowed familiarization with the VR software a week before the course. Pretest data were collected, participants were randomly assigned to conditions, completed the MBI (groups: active control, AC; video call, VC; virtual reality; VR) or waited (passive control group, PC), and then took post-test measures before compensation. At the end of the investigation period, a 45-min follow-up meeting was held.
The MBI course by 7Mind® was based on the principles of mindfulness-based programs (Crane et al., 2017). It included eight 60-min audio modules on stress, mindfulness exercises, and meditation. After each session, participants received a summary handout and were instructed to practice independently. The course required weekly module completion and passing a quiz to advance (7Mind®, 2024). The MBI was accompanied by weekly online meetings in small groups of five to seven participants (i.e., 8 × 60 min) within two intervention conditions: either as 2D video call meetings (using Webex, VC group) or in a virtual 3D meeting room using VR glasses (VR group, see below). The group meetings served to structure and elaborate the 7Mind® podcasts and to facilitate experience-based group exchange. The course instructor (A.R.) was psychologist by training (M.Sc.) and had teaching experiences with university students.
Participants were randomly assigned to one of four conditions. However, minor irregularities in randomization could not be avoided for organizational reasons (see SM1 in Supplementary material for details). The passive control group (PC) only completed pre- and post-test assessments (n = 32). The active control group (AC) completed the MBI (n = 35), but without weekly group meetings. Two additional groups supplemented the MBI with weekly online meetings as described above. Specifically, the video call group met via a 2D video platform (VC, n = 31), while the VR group used Meta Quest 2 VR glasses to meet in a 3D environment on Horizon Workrooms (VR, n = 29), featuring a virtual landscape with avatars around a table (for demonstration see SF1 in Supplementary material). Apart from this, the group meetings were held in the same way in both intervention groups. A flowchart of the study design is shown in Figure 1.
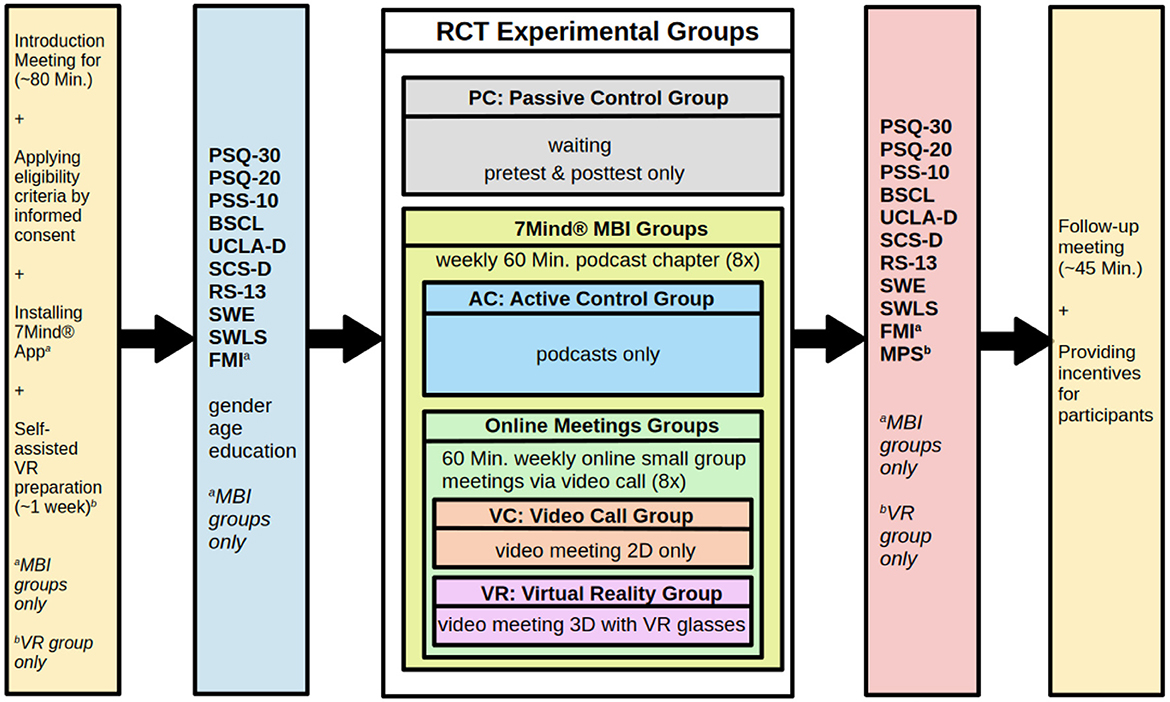
Figure 1. Flowchart of study design. PSQ-30/PSQ-20, perceived stress questionnaire (30 or 20 items version); PSS-10, perceived stress scale; BSCL, brief symptom checklist; UCLA-D, German UCLA loneliness scale; SCS-D, German self-compassion scale; RS-13, resilience; SWE, general self-efficacy scale; SWLS, satisfaction with life scale; FMI, Freiburg mindfulness inventory; MPS, multimodal presence scale; RCT, randomized control trial; PC, passive control; AC, active control; VC, video call; VR, virtual reality.
Participants
Participants were recruited via the Online Recruitment System for Economic Experiments (ORSEE) (Greiner, 2015), and gave written informed consent in accordance with the Declaration of Helsinki before taking part. The study was approved by the local ethics committee (University of Lübeck). All participants confirmed that they were students at the University of Lübeck, of legal age and in good health (i.e., no former or current mental or physical illnesses such as anxiety disorders or cardiovascular problems), consumed alcohol and nicotine only in moderation, had a good sense of balance and were physically healthy, and that they were currently not taking any prescription medication (except birth control pill). A total of 130 participants were recruited via email. Two participants withdrew from the study due to time constraints. One participant was excluded due to missings across all measurements. The final sample with minimal missing data and three dropouts at second measurement point (see Supplementary material) contained a total of 127 students participated (105 female, 21 male, 1 unspecified), with a mean age of 24.06 years (SD = 5.02, range = 18–52). Of these, 72 were psychology students, and 33 had a Bachelor's degree, averaging 4.21 semesters of study (SD = 2.63).
Nineteen subjects demonstrated elevated levels of mental stress, identified by the Brief Symptom Checklist (BSCL, see below) pretest scores (T ≥ 63 indicating high-risk subjects; Franke et al., 2015). However, we did not remove these participants from the final sample, assuming these were acceptable variations within the normal range. In the intervention groups (n = 88), 26 reported prior VR experience, though none owned a headset. Participants chose either €100 or €75 plus five hours of course credits as compensation. Additionally, all subjects had 12 months of free access to the 7Mind® app (7Mind®, 2024); the PC group received access only after the end of their study participation.
Instruments
We report all collected variables, including those not analyzed, in accordance with JARS guidelines (Appelbaum et al., 2018). While not part of the main analyses, additional self-generated variables were assessed to evaluate participants' experiences in the MBI groups (AC/VC/VR) and included open-ended responses (e.g., perceived usefulness or potential barriers of the VR glasses). Free-text responses are summarized in the Supplementary material. The Supplementary material and OSF material provides additional methodological details, sample characteristics, and supplementary analyses. These materials enhance transparency and allow for replication.
All measures contained self-reported Likert scales. Unless otherwise specified, mean values were calculated for all scales. Cronbach's alpha was used to assess internal consistency; for pre- and post-test measurements, separate alpha values were reported.
Perceived stress (PSQ/PSS-10)
Perceived stress was operationalized using several scales (PSQ-30, PSQ-20, and PSS) for two reasons. Firstly, these instruments capture different aspects of the stress experience (experience of external stressors vs. perceived coping resources) and, secondly, the construct validity of these scales is still discussed in light of chronic stress (Schmidt et al., 2020). The original Perceived Stress Questionnaire contains 30 items (Levenstein et al., 1993) and is available in two German-language versions (Fliege et al., 2009): as both the PSQ-30 (αs = 0.94/0.95) and a short version (PSQ-20; αs = 0.92/0.93). The PSQ-20 consists of four subscales: tension (αs = 0.82/0.83), demands (αs = 0.81/0.82), joy (reverse-coded; αs = 0.80/0.82) and worries (αs = 0.84/0.86). Example item: “You have too many things to do.” The 10-item Perceived Stress Scale (PSS-10; Schneider et al., 2020) is an economic alternative to assess perceived stress and based on appraisals of own coping resources (αs = 0.82/0.82). PSS-10 subscales included helplessness (αs = 0.81/0.86) and self-efficacy (reverse-coded; αs = 0.76/0.67). Example item: “In the last month, how often have you been able to control irritations in your life?”
Stress symptoms (BSCL)
The Brief Symptom Checklist (BSCL; Franke, 2017), a 53-item scales, assessed general stress symptoms (αs = 0.96/0.95) with ten subscales: aggressiveness/hostility (αs = 0.71/0.71), anxiety (αs = 0.82/0.72), depression (αs = 0.86/0.83), paranoia (αs = 0.73/0.80), phobia (αs = 0.80/0.80), psychoticism (αs = 0.83/0.67), somatization (αs = 0.78/0.71), insecurity in social contacts (αs = 0.76/0.76), compulsivity (αs = 0.84/0.80), and an unspecified additional scale (αs = 0.70/0.70). Example item: “I feel anxious.” A cut-off value by T ≥ 63 indicates high-risk subjects (Franke et al., 2015).
Loneliness (UCLA-D)
Loneliness was measured using the 20-item German UCLA Loneliness Scale (UCLA-D; Döring and Bortz, 1993), with excellent reliability (αs = 0.92/0.93). Subscales included emotional isolation (αs = 0.86/0.84), feelings of loneliness (αs = 0.82/0.86), and social isolation (αs = 0.76/0.78). Example item: “I have no one I can turn to.”
Self-compassion (SCS-D)
Self-compassion was measured using the 12-item German Self-Compassion Scale (SCS-D; Hupfeld and Ruffieux, 2011), with excellent overall reliability (αs = 0.91/0.90) and six subscales: self-kindness (αs = 0.72/0.69), self-judgment (αs = 0.88/0.86), common humanity (αs = 0.60/0.61), isolation(αs = 0.61/0.67), mindfulness (αs = 0.64/0.62), and over-identification (αs = 0.68/0.68). Example item: “I disapprove of and condemn my own mistakes and weaknesses.”
Resilience (RS-13)
The 13-item RS-13 scale (Leppert et al., 2008) assessed resilience with strong reliability (αs = 0.87/0.87). Example item: “I am determined.”
Self-efficacy (SWE)
Self-efficacy was measured using the General Self-Efficacy Scale (SWE; Schwarzer and Jerusalem, 2003), showing high reliability (αs = 0.87/0.89). Example item: “It is not difficult for me to realize my intentions and goals.”
Life satisfaction (SWLS)
Life satisfaction was assessed using the 5-item Satisfaction with Life Scale (SWLS; Janke and Glöckner-Rist, 2014), with solid reliability (αs = 0.82/0.89). Example item: “I am satisfied with my life.”
Mindfulness (FMI)
Mindfulness was assessed with the 14-item Freiburg Mindfulness Inventory (FMI; Walach et al., 2006; αs = 0.84/0.81) only in the MBI conditions (AC/VC/VR). Example item: “I am open to the experience of the present moment.”
VR immersion (MPS)
The VR immersion was measured with the 15-item Multimodal Presence Scale (MPS; Volkmann et al., 2018) only in the VR condition (α = 0.85), including subscales for physical presence (α = 0.81), self-presence (α = 0.92), and social presence (α = 0.85). Example item: “The virtual environment seemed real to me.”
Data analysis
With respect to BSCL, several outliers were identified based on QQ normality plots. Therefore, we used an alternative operationalization based on a “tendency toward stress” approach (counting items > 0; see Franke, 2017). This adjustment reduced outliers in QQ plots, mitigating severe violations of parametric assumptions and allowing us to avoid removing data points. Missing data were minimal and handled by mean imputation at the item level within each scale, consistent with recommendations for handling small proportions of MCAR data (Tabachnick and Fidell, 2019).
For hypothesis testing, we used Linear Mixed Models (LMM) and Ordinary Least Squares (OLS) regression models, reporting unstandardized regression coefficients (b), standard errors (SE), p-values, and effect sizes (R2 as well as Cohen's d for mean differences). Given only minor deviations from normality, we relied on parametric significance estimates for hypothesis testing. To assess robustness, we also computed bias-corrected and accelerated (BCa) bootstrap confidence intervals (95% CI, 5,000 samples) for (fixed) effects (LMM/OLS). Furthermore, we calculated parametric bootstrap confidence intervals (95% CI, 5,000 samples) for random effects (LMM). We report only the BCa confidence intervals as an additional robustness check, even in cases where these intervals may include zero. Data were analyzed using R, version 4.2.2 (R Core Team, 2022), with lme4 (Bates et al., 2015) for mixed-effects modeling, ggplot2 (Wickham et al., 2016) for visualization, mediation (Tingley et al., 2014) for conducting mediational analyses, pwr (Champely et al., 2020) and simr (Green and MacLeod, 2016) packages for a post-hoc power and sensitivity analyses.
Post-hoc power and sensitivity analysis
A post-hoc sensitivity analysis assessed the model's power to detect the strongest observed interaction effect (PC vs. AC/VC/VR × time on self-compassion: self-kindness) using pwr package. For the obtained effect size of b = 0.10 [f2 = 0.071; representing a small-to-moderate effect size according to Cohen's (1988) guidelines] with df = 126 and α = 0.05, the analysis yielded a power of 1 – β = 0.85, indicating sufficient sensitivity for detecting the hypothesized interaction (see Subscale's Analyses). In addition, to evaluate the sensitivity of the model testing, a simulation-based power analysis was conducted using simr package. Based on the same model (PC vs. AC/VC/VR × time on self-compassion: self-kindness) with 251 observations, the minimum detectable effect size (MDES) was estimated. With 2,000 simulations at α = 0.05, the model achieved 81.05% power (95% CI: [79.26%; 82.75%]) to detect an effect estimate of the interaction term PC vs. AC/VC/VR × time of b = 0.10. Thus, the analysis confirms that the empirical effect was detected with sufficient statistical power.
Results
Preliminary analyses: independence checks and intercorrelations
To test if baseline characteristics (e.g., sociodemographic and pretest scores) were independent of intervention conditions, χ2 tests, ANalyses Of VAriance (ANOVAs), and Ordinary Least Squares (OLS) regressions were conducted. χ2 tests showed independence for gender [χ2(3) = 1.603, p = 0.659], study program [χ2(3) = 0.885, p = 0.829], study degree [χ2(3) = 3.481, p = 0.323], and VR experience [χ2(2) = 4.497, p = 0.106]. ANOVAs showed no significant differences by condition for age [F(3, 123) = 1.261, p = 0.291] and semester [F(3, 121) = 0.157, p = 0.925]. OLS regressions for pretest scores indicated overall minor dependencies for BSCL subscale depression [F(3, 121) = 3.136, p = 0.028], but no systematic differences (all ps ≥ 0.05) for remaining outcomes. Minor trends emerged for loneliness and life satisfaction (0.05 ≥ps < 0.10). High-risk subjects (derived from BSCL: T ≥ 63; Franke et al., 2015), were evenly distributed across conditions [χ2(3) = 2.499, p = 0.518]. Thus, baseline characteristics were considered sufficiently independent of intervention conditions. Additionally, the dependent variables showed the expected pattern of intercorrelations. For details refer to ST1 (Supplementary material).
Analysis procedure
To test our hypotheses, hierarchical Linear Mixed Models (LMM) were conducted with subjects as random intercepts. Model 1 included intercepts only, while Model 2 added time (pretest vs. post-test, coded 0/1), and Model 3 included three orthogonal Helmert contrasts for intervention conditions: (1) PC vs. AC/VC/VR (PC: −3, others: 1); (2) AC vs. VC/VR (AC: −2, others: 1); and (3) VC vs. VR (VC: −1, VR: 1). These unscaled contrasts reflect the stepwise structure of the intervention manipulation. Coefficients are based on raw contrast weights; hypothesis tests remain unaffected by contrast scaling (Cohen et al., 2013). The last saturated Model 4 included the three interaction terms [time × contrast (1), time × contrast (2), and time × contrast (3)] for testing the hypotheses H.1, H.2, and H.3. For model comparison, χ2-Tests were conducted for testing incremental increases in variance explanation.
Overall changes by time
Analyses began with overall scales and proceeded to subscales. The intercept-only model (Model 1) showed substantial within-person variability across measures (ICC range: 0.30–0.82). Main effects by time in Model 2 (pre- vs. post-test) showed reductions in perceived stress [PSS-10: b = −0.17, SE = 0.04, 95% Boot CI = (−0.274; −0.058), Boot SE = 0.06, d = −0.33, p < 0.001] and increases in self-compassion [b = 0.17, SE = 0.04, 95% Boot CI = (0.069; 0.275), Boot SE = 0.05, d = 0.37, p < 0.001], self-efficacy [b = 0.09, SE = 0.03, 95% Boot CI = (0.024; 0.166), Boot SE = 0.04, d = 0.28, p = 0.002], and life satisfaction [b = 0.25, SE = 0.06, 95% Boot CI = (0.107; 0.395), Boot SE = 0.07, d = 0.39, p < 0.001]. Subscale time effects yielded reductions in stress [e.g., helplessness: b = −0.17, SE = 0.05, 95% Boot CI = (−0.301; −0.046), Boot SE = 0.06, d = −0.29, p = 0.001] and loneliness [social isolation: b = −0.10, SE = 0.04, 95% Boot CI = (−0.187; −0.003), Boot SE = 0.05, d = −0.23, p = 0.011] and increases in self-compassion subscales [e.g., self-kindness: b = 0.16, SE = 0.06, 95% Boot CI = (0.016; 0.307), Boot SE = 0.08, d = 0.23, p = 0.011; isolation: b = 0.18, SE = 0.07, 95% Boot CI = (0.014; 0.340), Boot SE = 0.08, d = 0.24, p = 0.007]. Trends were observed for reduction in perceived stress [PSQ-20: b = −0.02, SE = 0.01, 95% Boot CI = (−0.053; 0.011), Boot SE = 0.01, d = −0.15, p = 0.096; demands: b = −0.03, SE = 0.02, 95% Boot CI = (−0.072; 0.010), Boot SE = 0.02, d = −0.17, p = 0.057]. The following models (Model 3) were build up as incremental references for the last models (Model 4) testing the hypotheses at once.
Hypothesis testing
Overall scales' level
In the fourth models, perceived stress (PSS-10) yielded a significant incremental variance explanation [χ2(3) = 7.83, p = 0.050] with a trend for PC vs. AC/VC/VR × time [b = −0.04, SE = 0.02, 95% Boot CI = (−0.102; 0.014), Boot SE = 0.03, p = 0.081], qualified by a non-significant mean difference with lower means at post-test in the MBI conditions compared to PC (ΔM = −0.45, SE = 0.37, d = −0.18, p = 0.223) but a significant decrease within AC (ΔM = −0.31, SE = 0.14, d = −0.16, p = 0.033). Further trends were observed for PC vs. AC/VC/VR × time [loneliness: b = −0.03, SE = 0.02, 95% Boot CI = (−0.074; 0.010), Boot SE = 0.02, p = 0.072, χ2(3) = 3.89, p = 0.274 and self-compassion: b = 0.04, SE = 0.02, 95% Boot CI = (−0.010; 0.098), Boot SE = 0.03, p = 0.069, χ2(3) = 3.78, p = 0.286]. Loneliness decreased significantly in MBI conditions vs. PC (ΔM = −0.88, SE = 0.32, d = −0.44, p = 0.006). Self-compassion at post-test tended to be higher in MBI conditions (AC/VC/VR) than in PC, though not significantly (ΔM = 0.18, SE = 0.45, d = 0.06, p = 0.684). Taken together, these trends and significant effects (especially for loneliness) were in line with H.1. The remaining interaction terms were non-significant (ps ≥ 0.10).
Subscales' level
The stress subscale demands [PSQ-20] had a significant interaction for PC vs. AC/VC/VR × time [b = −0.02, SE = 0.01, 95% Boot CI = (−0.042; 0.004), Boot SE = 0.01, p = 0.047, χ2(3) = 5.66, p = 0.129] with both non-significant lower post-test means in MBI conditions vs. PC (ΔM = −0.05, SE = 0.14, d = −0. 05, p = 0.711) and decreases within the MBI conditions (ΔM = −0.05, SE = 0.10, d = −0.04, p = 0.596). The perceived stress [PSS-10] subscale self-efficacy yielded a significant interaction for PC vs. AC/VC/VR × time [b = −0.06, SE = 0.03, 95% Boot CI = (−0.117; 0.005), Boot SE = 0.03, p = 0.035, χ2(3) = 6.10, p = 0.107] with trends indicating lower post-test means in MBI conditions vs. PC (ΔM = −0.62, SE = 0.36, d = −0.25, p = 0.088) and a decrease within VR condition (ΔM = −0.30, SE = 0.15, d = −0.14, p = 0.051); see Table 1 and Figure 2. AC vs. VC/VR × time was significant for helplessness subscale [PSS-10] [b = 0.09, SE = 0.04, 95% Boot CI = (−0.018; 0.188), Boot SE = 0.05, p = 0.041, χ2(3) = 7.57, p = 0.056], with a non-significant post-test difference, yet favoring AC (ΔM = 0.45, SE = 0.29, d = 0.23, p = 0.119); in addition, a significant decrease within AC condition was observed (ΔM = −0.38, SE = 0.16, d = −0.17, p = 0.022). Social isolation in MBI was significantly lower vs. PC at post-test [b = −0.05, SE = 0.02, 95% Boot CI = (−0.100; 0.007), Boot SE = 0.03, p = 0.031, χ2(3) = 4.84, p = 0.184; ΔM = −1.06, SE = 0.36, d = −0.45, p = 0.004; see Table 2 and Figure 3]. Finally, a significant interaction for PC vs. AC/VC/VR × time was found for the self-kindness subscale of self-compassion with a significant incremental variance explanation [b = 0.11, SE = 0.04, 95% Boot CI = (0.003; 0.215), Boot SE = 0.05, p = 0.003, χ2(3) = 10.08, p = 0.018], but the post-test difference between MBI conditions and PC was not significant (ΔM = 0.71, SE = 0.52, d = 0.20, p = 0.172). However, within the VC condition, there was an increasing trend (ΔM = 0.38, SE = 0.21, d = 0.13, p = 0.079); see Table 3 and Figure 4. Further trends (0.05 ≤ ps < 0.10) were observed for stress symptoms (unspecified subscale), and two self-compassion scales (common humanity and over-identification), see ST2 (Supplementary material).
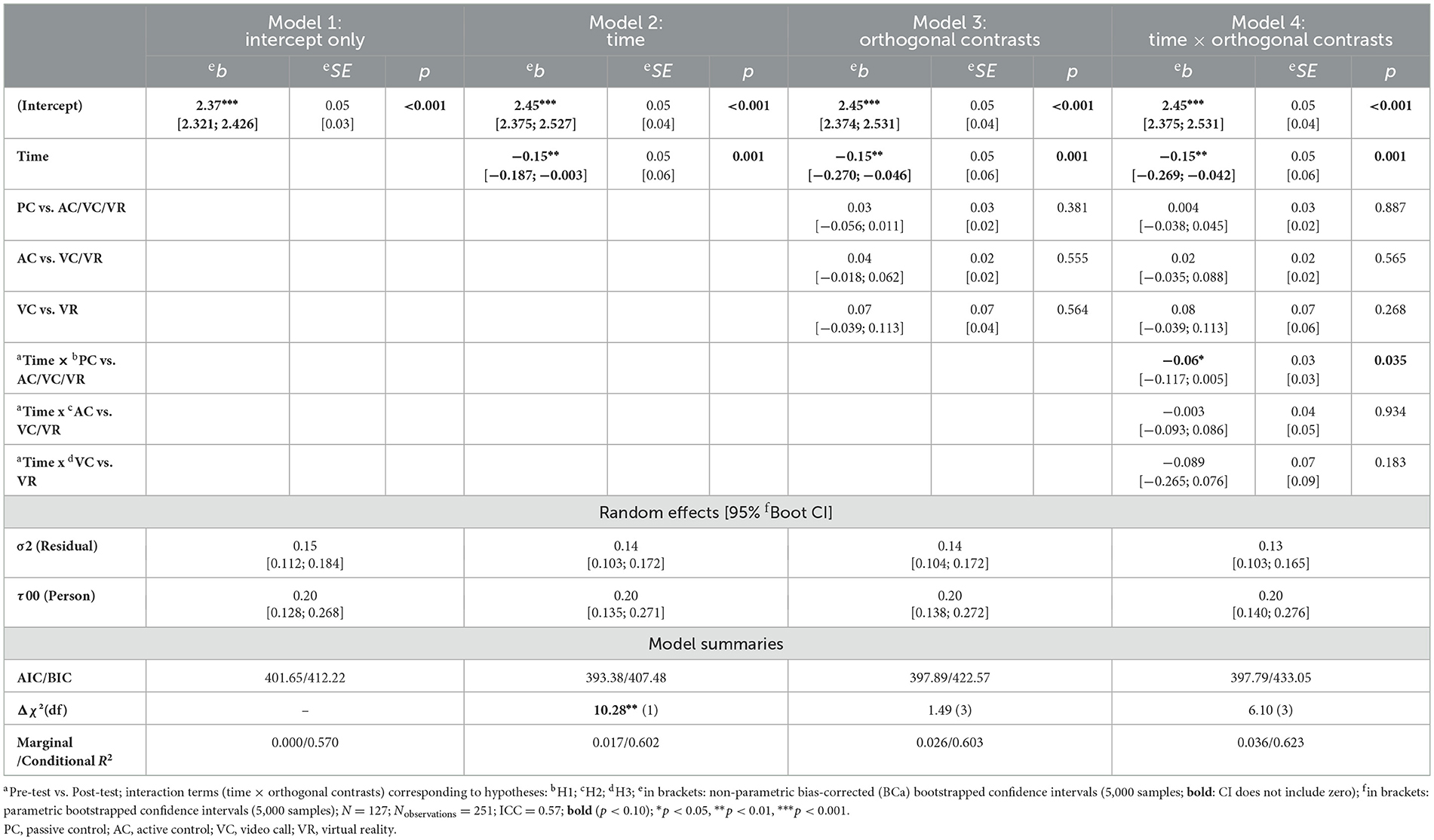
Table 1. Results of hierarchical linear mixed models, dependent variable (DV): stress experience [PSS-10] (subscale: self-efficacy).
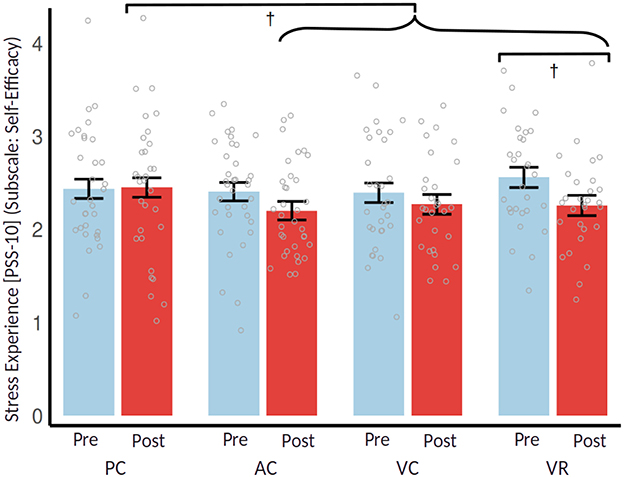
Figure 2. Estimated Means of Stress Experience [PSS-10] (Subscale: Self-Efficacy) with 95% confidence intervals; brackets indicate post-hoc mean differences †p < 0.10. PC, passive control; AC, active control; VC, video call; VR, virtual reality.
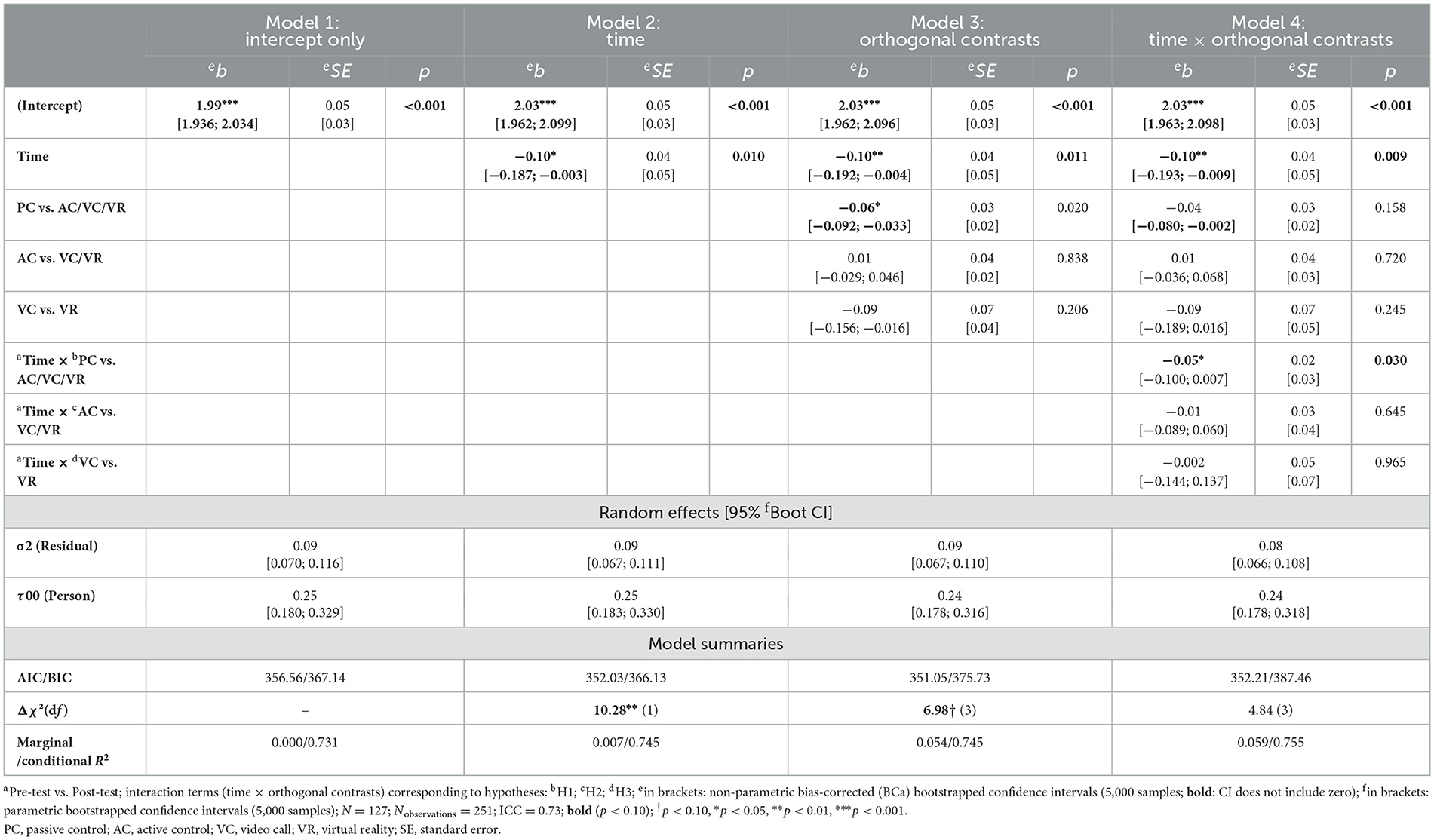
Table 2. Results of hierarchical linear mixed models, DV: loneliness (subscale: social isolation).
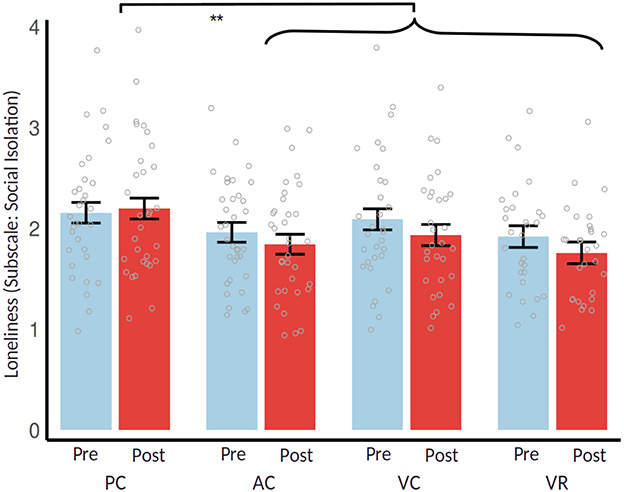
Figure 3. Estimated means of loneliness (Subscale: Social Isolation) with 95% confidence intervals; brackets indicate post-hoc mean differences **p < 0.01. PC, passive control; AC, active control; VC, video call; VR, virtual reality.
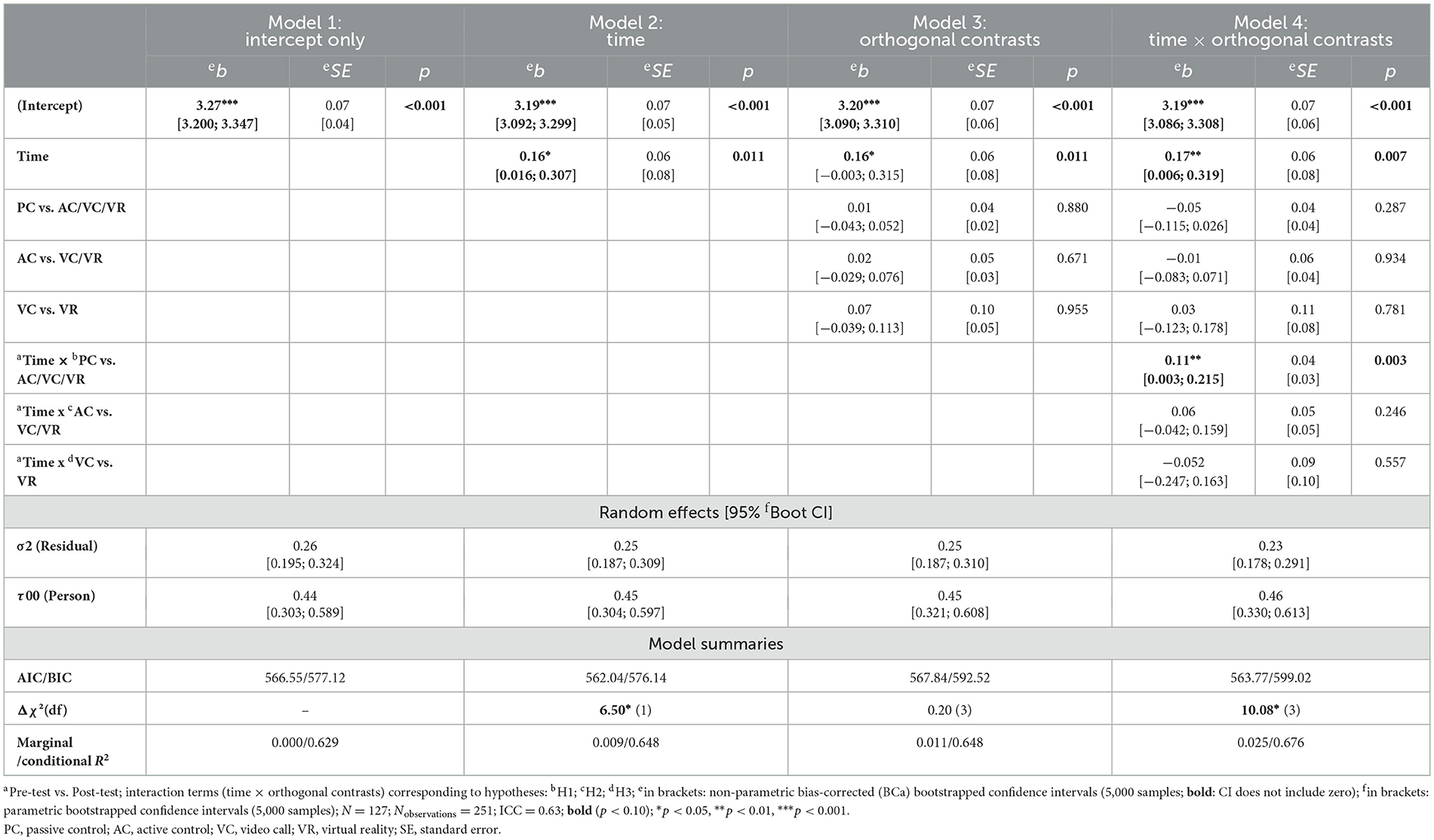
Table 3. Results of hierarchical linear mixed models, DV: self-compassion (subscale: self-kindness).
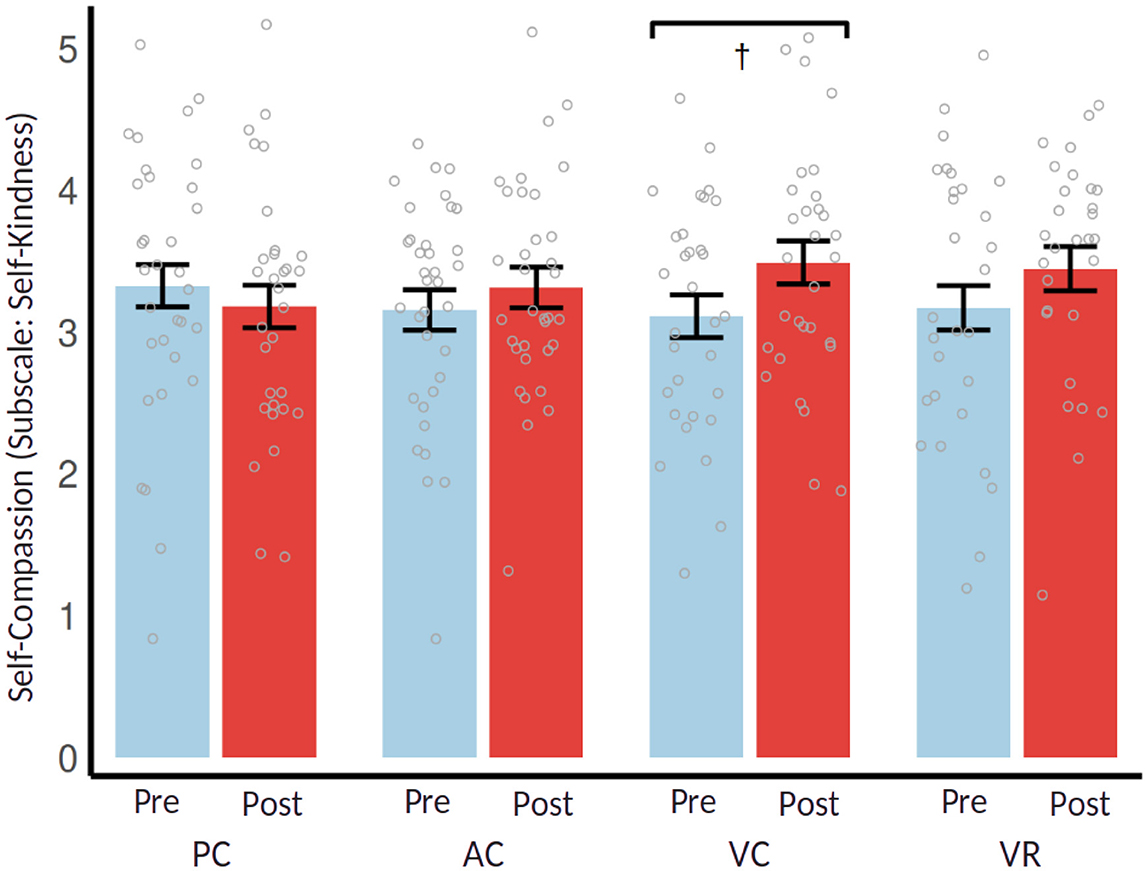
Figure 4. Estimated means of self-compassion (subscale: self-kindness) with 95% confidence intervals; brackets indicate post-hoc mean differences †p < 0.10. PC, passive control; AC, active control; VC, video call; VR, virtual reality.
In summary, hypothesis H.1 (i.e., a beneficial effect of the MBI) was supported (especially for subscales of stress experience, loneliness, and self-compassion, see Tables 1–3), while hypotheses H.2 (i.e., enhancing effects of regular group meetings) and H.3 (i.e., boosting effects of VR group meetings) could be rejected. For analysis details see ST2 (Supplementary material).
Exploratory analyses
Mediation by mindfulness
To explore E.1 (i.e., a mediating effect of mindfulness), only the three intervention groups (AC/VC/VR) were analyzed, omitting PC. First, we tested the direct effect of the orthogonal contrasts on mindfulness following the procedure above. Mindfulness increased significantly across all MBI conditions [b = 0.37, 95% Boot CI = (0.282; 0.449), SE = 0.04, Boot SE = 0.04, d = 1.04, p < 0.001], with a significant AC vs. VC/VR × time interaction [b = 0.05, SE = 0.02, 95% Boot CI = (−0.004; 0.106), Boot SE = 0.03, p = 0.038]. Although no significant post-test difference was observed (ΔM = 0.25, SE = 0.17, d = 0.25, p = 0.130), within-subject mindfulness increased slightly more in VC/VR (ΔM = 0.42, SE = 0.14, d = 0.25, p = 0.003) than in AC (ΔM = 0.27, SE = 0.09, d = 0.24, p = 0.004); see Figure 5. However, no interaction was found for VC vs. VR × time [b = 0.02, SE = 0.04, 95% Boot CI = (−0.101; 0.147), Boot SE = 0.06, p = 0.696].
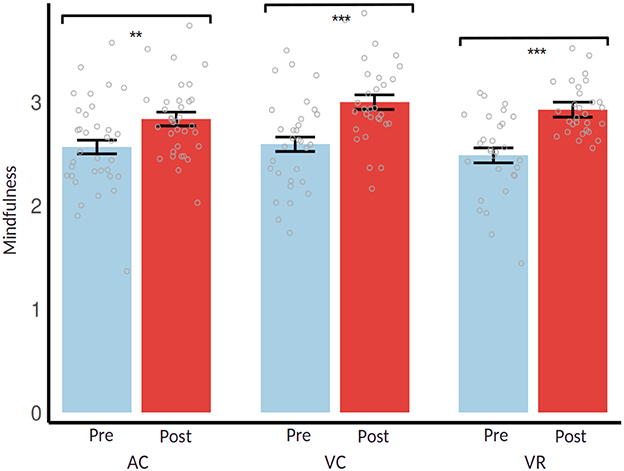
Figure 5. Estimated means of mindfulness with 95% confidence intervals; brackets indicate post-hoc mean differences **p < 0.01, ***p < 0.001. PC, passive control; AC, active control; VC, video call; VR, virtual reality.
To test mindfulness as a mediator (i.e., individual changes in mindfulness through the MBI), we used Baron and Kenny's (1986) approach, checking for direct and indirect effects, with OLS regressions controlling for pre-test scores. Mediation was assessed using the bootstrap method with 10,000 samples (Preacher and Hayes, 2004). Mediation was considered significant if the 95% CI excluded zero.
In Model 1 (R2 = 0.45), VC/VR vs. AC did not yield a significant association with stress experience (PSQ-30) measured at post-test level [b = 0.01, SE = 0.01, 95% Boot CI = (−0.008; 0.025), Boot SE = 0.01, p = 0.308]. Model 2 (R2 = 0.42) showed that (post-test) mindfulness was higher in VC/VR than in AC [b = 0.05, SE = 0.02, 95% Boot CI = (0.014; 0.083), Boot SE = 0.02, p = 0.016]. In Model 3 (R2 = 0.54), (post-test) mindfulness was negatively associated with stress experience [b = −0.19, SE = 0.04, 95% Boot CI = (−0.278; −0.109), Boot SE = 0.04, p < 0.001], significantly improving the model fit [ΔR2 = 0.10, ΔF(1, 87) = 18.82, p < 0.001]; in addition, (post-test) stress experience was higher in VC/VR than in AC [b = 0.02, SE = 0.01, 95% Boot CI = (0.002; 0.033), Boot SE = 0.01, p = 0.031]. However, VC vs. VR conditions did not show any associations neither with stress experience nor with mindfulness (ps ≥ 0.730); see Table 4 for inspecting coefficients.
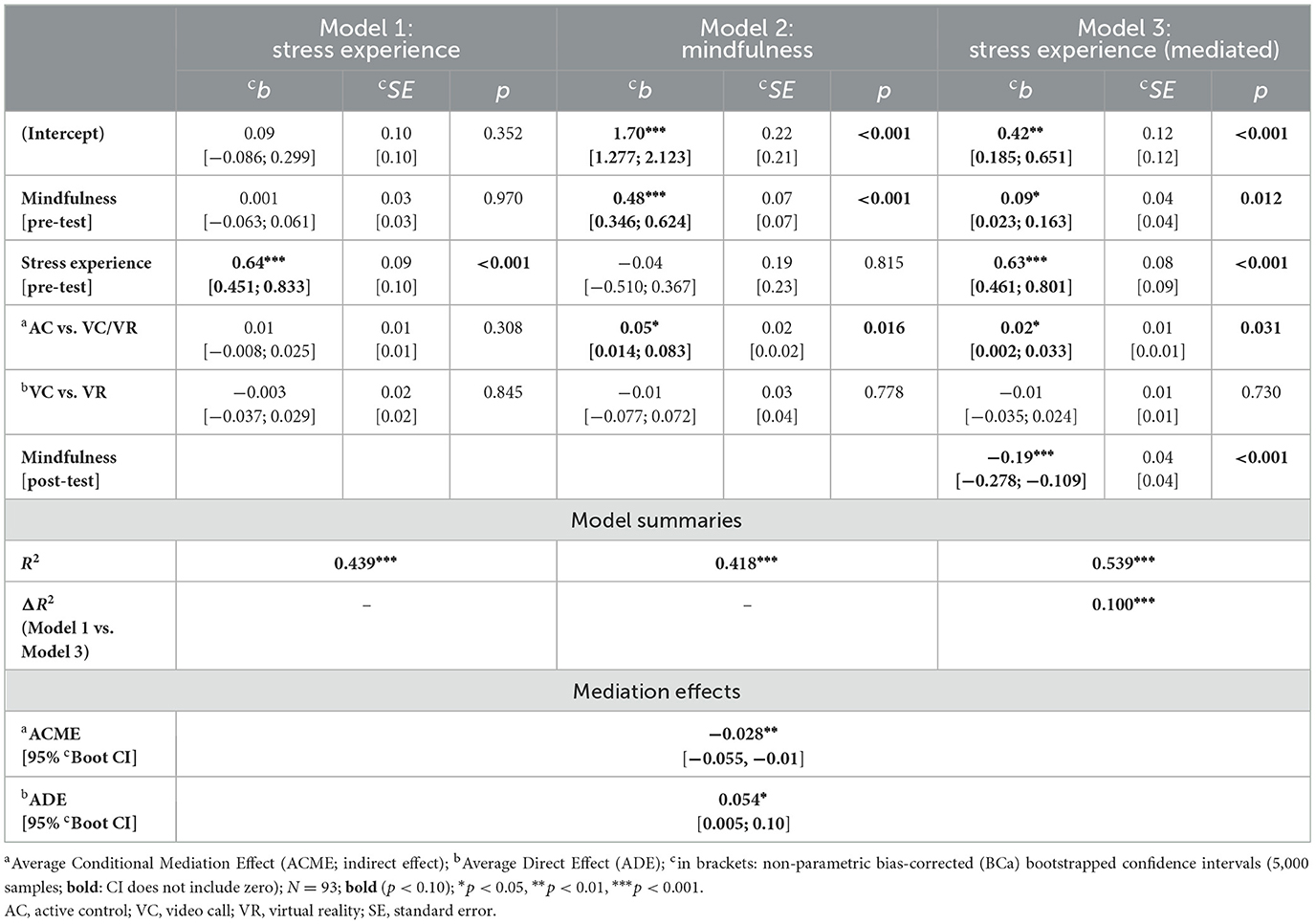
Table 4. Results of OLS regressions—mediation by mindfulness (outcome: stress experience [PSQ-30]) controlled for pre-test levels.
The indirect effect of (post-test) mindfulness (i.e., average causal mediation effects, ACME) on (post-test) stress experience for the path AC vs. VC/VR → mindfulness → stress experiecne was significant [b = −0.03, 95% Boot CI = (−0.055, −0.01), p = 0.012], with a suppressor effect that partially masked the direct effect (i.e., average direct effect, ADE), which became significant in the final model [b = 0.05, 95% Boot CI = (0.007, 0.10), p = 0.027]; see mediational path in Figure 6. However, the ACME for the path including contrast VC vs. VR was not significant [b = 0.004, 95% Boot CI = (−0.027, 0.03), p = 0.81]. Thus, mindfulness mediated but also counteracted the group condition's direct effect on stress. Mediation effects occurred for several remaining outcomes with a similar pattern, yet only regarding the AC vs. VC/VR contrast, especially for the stress scales, self-compassion and self-efficacy, see ST3 (Supplementary material).
![Diagram showing a mediation model with three variables: Orthogonal Contrast (AC vs. VC/VR), Mindfulness, and Stress Experience (PSQ-30). Arrows indicate effects: Orthogonal Contrast to Mindfulness (b = 0.05, SE = 0.02), Mindfulness to Stress Experience (b = -0.19, SE = 0.04), and Orthogonal Contrast directly to Stress Experience (b = 0.01, SE = 0.01). The average conditional mediation effect (ACME) is -0.028 with a confidence interval of [-0.055, -0.01], and the average direct effect (ADE) is 0.054 with a confidence interval of [0.006, 0.10].](https://www.frontiersin.org/files/Articles/1613894/feduc-10-1613894-HTML/image_m/feduc-10-1613894-g006.jpg)
Figure 6. Mediational by mindfulness (outcome: stress experience [PSQ-30]) controlled for pre-test levels. bold (p < 0.10): *p < 0.05, **p < 0.01, ***p < 0.001. AC, active control; VC, video call; VR, virtual reality; PSQ, perceived stress questionnaire; ACME, average causal mediation effects; ADE, average direct effect; CI, confidence interval; SE, standard error.
Relationships between VR immersion and outcomes
To explore E.2 (correlation of VR immersion with intervention effectiveness), the VR group was analyzed separately to examine relationships between VR immersion and outcomes. VR immersion was assessed globally and across three subscales: physical presence, social presence, and self presence. We constructed the models similarly to those of the hypothesis tests, except that we used the mean-centered VR Immersion scales instead of the orthogonal contrasts.
Globally, no significant interactions were found between overall VR immersion and time for any target variables (ps > 0.05). However, analyses of the subscales revealed interactions with time. For perceived stress (PSQ-30) in Model 4 [χ2(3) = 11.69, p = 0.009], Physical presence × time showed a stronger negative correlation post-test [b = −0.11, SE = 0.04, 95% Boot CI = (−0.216; 0.030), Boot SE = 0.07, p = 0.021]. Social presence × time, in contrast, showed a stronger positive correlation post-test [b = 0.12, SE = 0.04, 95% Boot CI = (0.022; 0.222), Boot SE = 0.06, p = 0.002] and no relationship for self presence × time [b = −0.04, SE = 0.02, 95% Boot CI = (−0.115; 0.034), Boot SE = 0.04, p = 0.161]; see Table 5. Simple slopes for stress experience by VR immersion dimensions are shown in Figure 7, with similar patterns for some other outcomes, especially for stress scales, loneliness and self-compassion, see ST4 (Supplementary material).
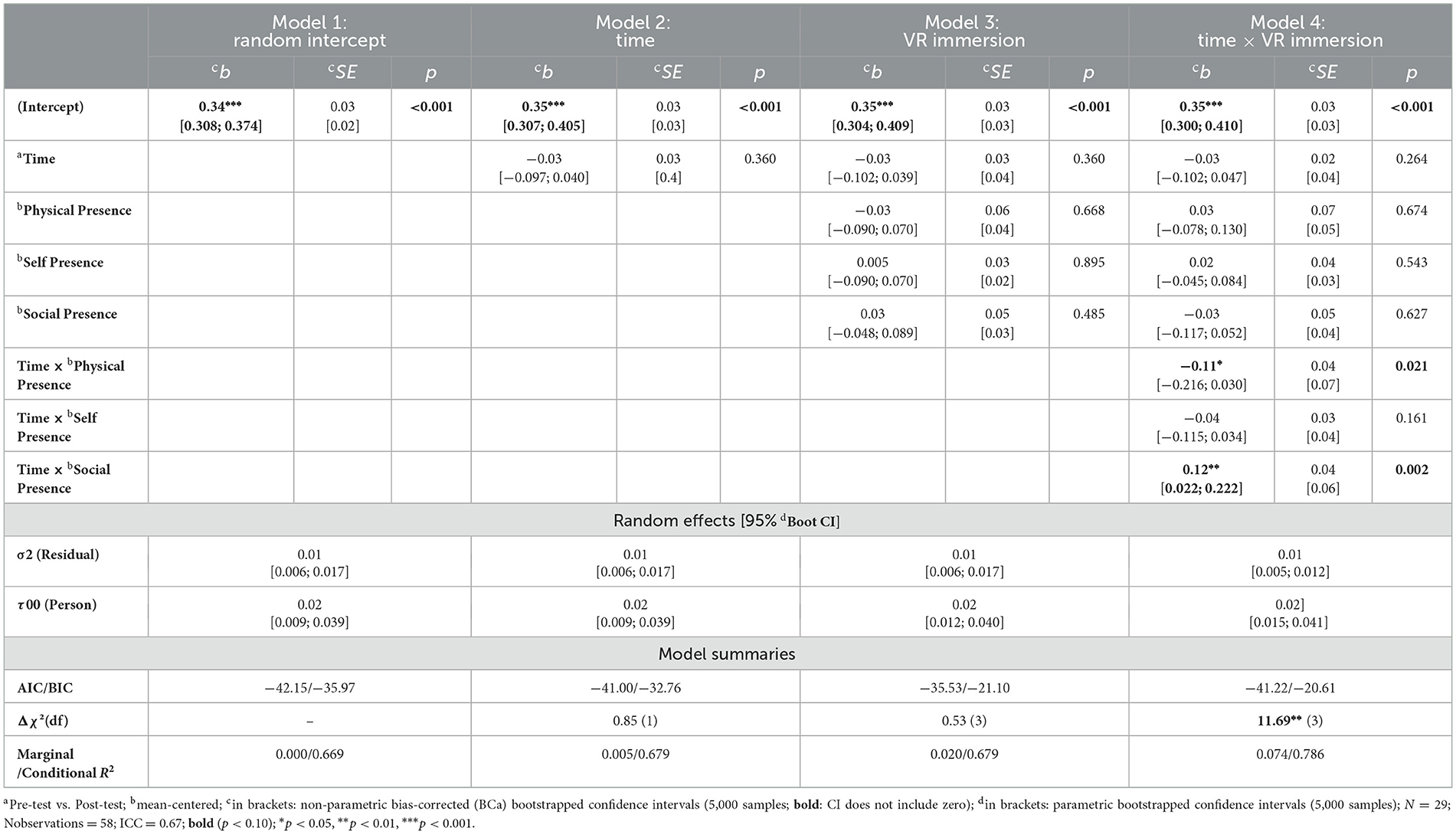
Table 5. LMMs: relationships between VR immersion subdimensions and stress experience [PSQ-30].
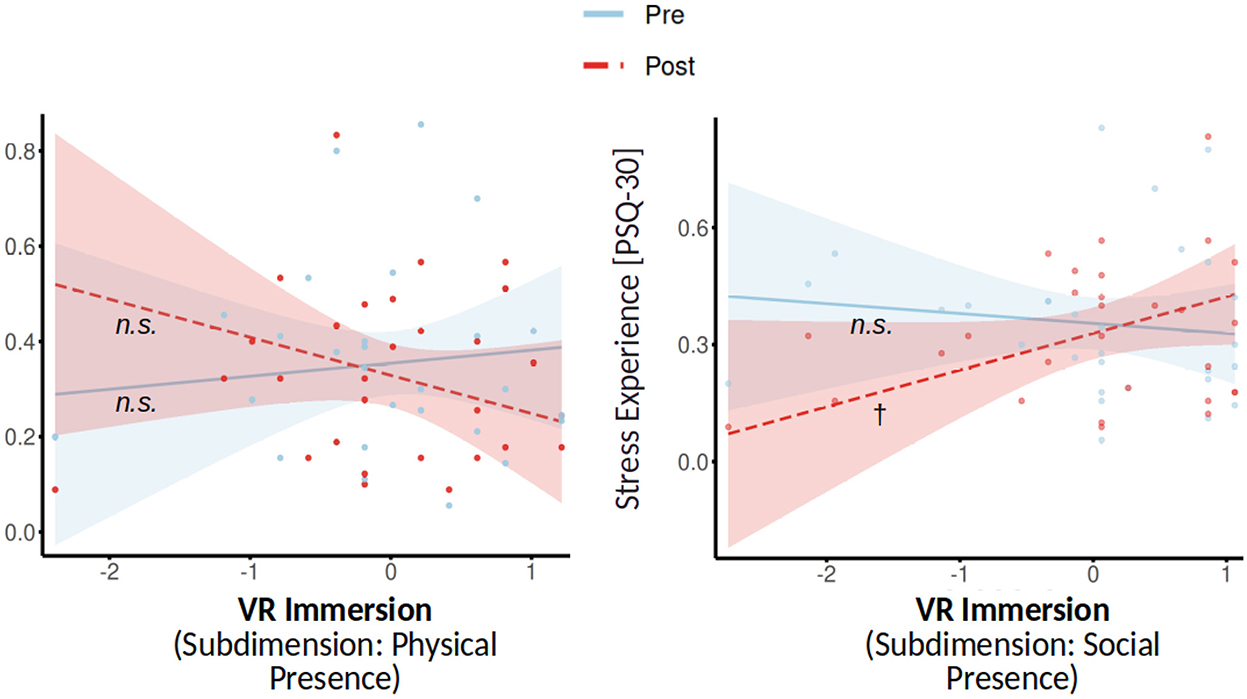
Figure 7. Simple slopes for VR immersion subdimensions × time, dependent variable: Stress Experience [PSQ-30]. n.s. (p ≥ 0.10), †p < 0.10. VR, virtual reality; PSQ, perceived stress questionnaire.
Discussion
The study aimed to evaluate the effectiveness of an app-delivered mindfulness-based stress reduction training in a university setting and to investigate whether additional digital group meetings could be beneficial. The 8-week 7Mind®Mindfulness-Based Intervention (MBI) was implemented using a randomized, controlled design with students being assigned to four intervention conditions: one condition used the MBI only as an active control group (AC), while in two remaining conditions the subjects attended additional weekly guided meetings either via video calls (VC) or in a virtual reality setting (VR). The remaining condition was a passive control group (PC), completing only pre- and post-tests, waiting 8 weeks. To evaluate the effectiveness of the MBI variants, several dependent measures of psychological wellbeing including health-risk (e.g., stress experience) and protective outcomes (e.g., self-compassion) were used. In addition, we explored the mediating effects of mindfulness and whether VR immersion is associated with the outcomes to gain deeper insights.
Effectiveness of MBI Across conditions
The initial hypothesis (H.1) was based on the premise that our MBI would be effective across all intervention groups (AC/VC/VR) when compared to a passive control group (PC). This was confirmed with significant effects on reducing stress and loneliness, yet increasing self-compassion. Our findings align with those of previous studies, which have demonstrated that MBIs can enhance mental and physical wellbeing by mitigating stress (McConville et al., 2017; Grossman et al., 2004). Similarly, the reduction of loneliness can be considered a beneficial outcome in line with previous studies (Besse et al., 2022). Our MBI was found to enhance the tendency to treat oneself with kindness and compassion, which should, in turn, contribute to an improvement in the wellbeing of those who participated in the course. Moreover, the initial findings were corroborated, indicating that app-based mindfulness training can also have beneficial effects.
Subsequent contributions have also demonstrated the stress-reducing impact of an app-delivered mindfulness intervention. While Karing (2024), Huberty et al. (2019), and Riley et al. (2022) demonstrated positive outcomes of app-delivered mindfulness interventions, their designs lacked features such as structured group meetings or immersive technologies. For instance, Schwartz et al. (2023) reviewed randomized controlled trials of mindfulness-based mobile apps and found that these apps improved wellbeing, but the absence of group dynamics and contextual support often limited their impact. Hwang et al. (2022) evaluated a smartphone-based stress reduction app and reported positive effects on stress levels, although the study did not incorporate group support or immersive features that might further enhance user engagement. In contrast, our study integrated weekly online group meetings and a VR environment, aligning more closely with the immersive frameworks discussed by Arpaia et al. (2021). Their narrative review highlights that VR-enhanced mindfulness-based applications may amplify emotional and sensory engagement, though few empirical studies have explored this in student populations. Furthermore, Xu et al. (2022) conducted a mixed-methods review and found that virtual mindfulness interventions positively impacted wellbeing, but most studies lacked rigorous mediation analysis or comparison of delivery formats (e.g., video vs. VR). Our study adds value by addressing these gaps—evaluating mindfulness as a mediator and assessing VR immersion subcomponents.
The role of digital group meetings in MBI
The second hypothesis (H.2) posits that regular online group meetings (VC/VR) will enhance the efficacy of the MBI relative to the active control group (AC). These meetings may also facilitate stress reduction through social interactions and collective self-efficacy (Cruwys et al., 2020; Yusufov et al., 2019). However, no significant additive effects were found for the group meeting conditions (VC/VR) compared to the active control condition (AC). Unexpectedly, the AC showed greater stress reduction than group meetings, yet consistent with some studies showing limited benefits of video-based mindfulness interventions over active control groups (Moulton-Perkins et al., 2022).
In the associated exploratory research question (E.1), we postulated that mindfulness acted as a mediator, given that this represents a central mechanism of the mindfulness-based training. All intervention groups (AC/VC/VR) showed significantly higher mindfulness at post-test (cf. Karing, 2024; Huberty et al., 2019), with group meetings (VC/VR) enhancing mindfulness more than podcast-only (AC), which is in line with prior studies (Visted et al., 2015). This mindfulness increase, often linked to stress reduction (Keng et al., 2012), may reflect a suppressor effect, where group meetings elevated social stress in some subgroups, dampening the actually positive outcomes of the MBI. Indeed, such a pattern was observed in studies of group-based stress reduction trainings, where individual levels of group identification and social support varied (see Imel et al., 2008; McKimmie et al., 2020). Future studies should investigate whether and under what conditions certain subgroups could benefit from (online) group meetings.
Virtual reality: opportunities and challenges
In our last hypothesis (H.3), we proposed that group meetings enhanced with a VR environment would provide additional benefits over those with conventional VC software. Indeed, VR environments could enhance the effects of a mindfulness-based training over traditional approaches (Ma et al., 2023) possibly by intensifying sensory experiences (Turner and Casey, 2014) and strengthening motivation and adherence (Jiang and Fryer, 2024; Modrego-Alarcón et al., 2021). However, we did not observe any direct effects in our study. Free-text comments (SM3 in Supplementary material) noted some VR-related burdens (e.g., discomfort, headache, technical issues), possibly explaining the lack of additional VR effects, similar to challenges noted in earlier work on VR discomfort (Jensen and Konradsen, 2018). However, these rather subjective comments should be interpreted with caution.
The second exploratory research question (E.2) examined the potential association between the intensity of immersion in the VR environment and our outcome variables. Although the global measure of VR immersion demonstrated no correlation with the outcomes, an examination of single sub-dimensions of VR immersion revealed contrasting results. Higher physical presence was linked to reduced stress, whereas higher social presence had the opposite effect, which suggests social immersion could have amplified social stimuli as (social) stressors, counteracting stress reduction. This mechanism is consistent with findings that training in intersubjective skills, compared with a mindfulness-based approach after exposure to psychosocial stressors, reduced the physiological stress response (measured by cortisol) (Engert et al., 2017). Another study (Faucher et al., 2016) suggests that cognitive behavioral therapy is slightly superior to the mindfulness-based approach for treating social anxiety disorder. These mixed findings underscore the need for further VR-aided mindfulness-based training research given the limited number of studies with substantial heterogeneity (Ma et al., 2023).
Strengths, limitations, and future directions
The randomized design, including both active and passive control groups, allowed for a rigorous comparison across intervention conditions. Moreover, implementing the intervention in a real-world university setting offers valuable insight into its ecological validity and practical applicability. However, the small sample size with a high proportion of female psychology students, limits generalizability. Specifically, our results may not fully extend to older populations, individuals with limited technological proficiency, or those with different cultural backgrounds. Methodological aspects, such as minor randomization issues (see SM1 in Supplementary material) and unmonitored compliance (exercise frequency and intensity), may also have impacted the results. Main effects over time, even in the passive control group, raise questions about true intervention effects vs. testing effects or reactivity. Furthermore, the lack of measures assessing subjective satisfaction with the at-home MBI may have introduced an unaccounted confounding variable. Therefore, future studies should increase the frequency of data collection (e.g., via weekly assessments or diary methods) to better capture intra-individual changes and dynamic, process-related situational factors (Pawsey et al., 2021), or physiological assessments (e.g., cortisol levels). The absence of follow-up assessments further limits insights into long-term effects. Future research should also explore variations of group meetings and VR environments, e.g., examining different VRs to clarify how they might enhance or hinder mental health training. While VR offers promising opportunities, its effectiveness may be influenced by individual differences in technology acceptance, susceptibility to motion sickness, and prior experience with immersive environments. Future research should, therefore, explore how these factors affect engagement and outcomes in more diverse populations. Along these lines, the integration of VR and artificial intelligence (AI) in mindfulness-based interventions is a promising research area (Mitsea et al., 2023). As technology advances, future studies should examine how these tools can be adapted for diverse populations and contexts, ensuring accessibility and reducing barriers (Eichel et al., 2021).
Practical implications
Our findings show that app-based mindfulness training, supported by digital group meetings, can be embedded into students' daily lives to strengthen stress management, reduce social isolation, and enhance self-compassion. These benefits translate into greater resilience when facing academic pressures, healthier responses to personal setbacks, and improved social connectedness. Video calls offer a practical and accessible format for regular peer support, while VR environments—when designed for comfort and usability—can provide immersive spaces that foster deeper focus and engagement. Looking ahead, refining VR platforms to minimize technical and physical barriers, and integrating adaptive features such as AI-driven personalization or real-time feedback, could further tailor mindfulness training to individual needs. Universities could harness these technologies to deliver flexible, scalable mental health support that evolves with students' learning contexts and lifestyles.
Conclusion
To conclude, this study supports the potential of app-based mindfulness training for improving psychological wellbeing. The main results align with existing research on efficacy of mindfulness-based interventions and the notion that, under favorable conditions, guided group settings can benefit mental health training. In practical terms, managing social stressors and ensuring psychological safety in group settings may enhance positive group effects. Effective group facilitation, flexible scheduling, and minimizing disruptions could further support mindfulness and stress reduction outcomes. The app-delivered format offers a low-threshold intervention for university students, potentially suitable for public funding. However, further research is needed to optimize design and delivery for broader needs.
Data availability statement
The datasets presented in this study can be found at https://osf.io/zs9xe/files/osfstorage.
Ethics statement
The procedure was approved by the Ethics Committee of the Universität in Lübeck (Aktenzeichen: 2022-418; approved on August 4, 2022; see approval at https://osf.io/zs9xe/files/osfstorage). The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
NZ: Data curation, Formal analysis, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. AR: Conceptualization, Data curation, Investigation, Resources, Validation, Writing – review & editing. NB: Conceptualization, Funding acquisition, Investigation, Project administration, Resources, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by a grant from the foundation “Innovation in der Hochschule” (“HySkiLab”,Gesund(heit) lehren und lernen in hybriden Skills-Labs); see https://stiftung-hochschullehre.de/projekt/hyskilab/. We would like to thank 7Mind® for providing the course at a reduced price for students through the “7Mind® Science Support” cooperation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Gen AI was used in the creation of this manuscript. AI (ChatGPT with model 4o from OpenAI) was used for analyzing free-text comments (see Supplementary material) and helping to write R analysis scripts.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/feduc.2025.1613894/full#supplementary-material
References
7Mind®. (2024). Stress, lass nach! Der 7Mind Stresspräventionskurs | 7mind.de. Available online at: https://www.7mind.de/magazin/stress-stresspraeventionskurs-kurs-achtsamkeit-stresswaeltigung (Accessed September 30, 2024).
Alrashdi, D. H., Chen, K. K., Meyer, C., and Gould, R. L. (2023). A systematic review and meta-analysis of online mindfulness-based interventions for university students: an examination of psychological distress and wellbeing, and attrition rates. J. Technol. Behav. Sci. 9, 211–223. doi: 10.1007/s41347-023-00321-6
Amanvermez, Y., Rahmadiana, M., Karyotaki, E., De Wit, L., Ebert, D. D., Kessler, R. C., et al. (2023). Stress management interventions for college students: a systematic review and meta-analysis. Clin. Psychol. Sci. Pract. 30, 423–444. doi: 10.1111/cpsp.12342
Appelbaum, M., Cooper, H., Kline, R. B., Mayo-Wilson, E., Nezu, A. M., Rao, S. M., et al. (2018). Journal article reporting standards for quantitative research in psychology: the APA Publications and Communications Board task force report. Am. Psychol. 73:3. doi: 10.1037/amp0000191
Arpaia, P., D'Errico, G., De Paolis, L. T., Moccaldi, N., and Nuccetelli, F. (2021). A narrative review of mindfulness-based interventions using virtual reality. Mindfulness 12, 1–16. doi: 10.1007/s12671-021-01783-6
Aşik, E., and Albayrak, S. (2022). The effect of mindfulness levels on the life satisfaction of nursing students. Perspect. Psychiatr. Care 58, 225–231. doi: 10.1111/ppc.12898
Baron, R. M., and Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 51, 1173–1182. doi: 10.1037/0022-3514.51.6.1173
Bates, D., Maechler, M., Bolker, B., Walker, S., Christensen, R. H. B., Singmann, H., et al. (2015). Package ‘lme4.' Convergence 12:2. Available online at: http://dk.archive.ubuntu.com/pub/pub/cran/web/packages/lme4/lme4.pdf
Besse, R., Whitaker, W. K., and Brannon, L. A. (2022). Reducing loneliness: the impact of mindfulness, social cognitions, and coping. Psychol. Rep. 125, 1289–1304. doi: 10.1177/0033294121997779
Birnie, K., Speca, M., and Carlson, L. E. (2010). Exploring self-compassion and empathy in the context of mindfulness-based stress reduction (MBSR). Stress Health 26, 359–371. doi: 10.1002/smi.1305
Champely, S., Ekstrom, C., Dalgaard, P., Gill, J., Weibelzahl, S., Anandkumar, A., et al. (2020). Pwr: Basic Functions for Power Analysis. Available online at: https://CRAN.R-project.org/package=pwr
Chiodelli, R., Mello, L. T. N. D., Jesus, S. N. D., Beneton, E. R., Russel, T., Andretta, I., et al. (2022). Mindfulness-based interventions in undergraduate students: a systematic review. J. Am. Coll. Health 70, 791–800. doi: 10.1080/07448481.2020.1767109
Cohen, J. (1988). Statistical Power Analysis for the Behavioral Sciences (2nd Edn.). New York, NY: Routledge.
Cohen, J., Cohen, P., West, S. G., and Aiken, L. S. (2013). Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences (3rd Edn.). New York, NY: Routledge. doi: 10.4324/9780203774441
Crane, R. S., Brewer, J., Feldman, C., Kabat-Zinn, J., Santorelli, S., Williams, J. M. G., et al. (2017). What defines mindfulness-based programs? The warp and the weft. Psychol. Med. 47, 990–999. doi: 10.1017/S0033291716003317
Cruwys, T., Stewart, B., Buckley, L., Gumley, J., and Scholz, B. (2020). The recovery model in chronic mental health: a community-based investigation of social identity processes. Psychiatry Res. 291:113241. doi: 10.1016/j.psychres.2020.113241
David, O. A., Costescu, C., Cardos, R., and Mogoaşe, C. (2020). How effective are serious games for promoting mental health and health behavioral change in children and adolescents? A systematic review and meta-analysis. Child Youth Care Forum 49, 817–838. doi: 10.1007/s10566-020-09566-1
Dawson, A. F., Brown, W. W., Anderson, J., Datta, B., Donald, J. N., Hong, K., et al. (2020). Mindfulness-based interventions for university students: a systematic review and meta-analysis of randomised controlled trials. Appl. Psychol. Health Wellbeing 12, 384–410. doi: 10.1111/aphw.12188
Döring, N., and Bortz, J. (1993). Psychometrische Einsamkeitsforschung: Deutsche Neukonstruktion der UCLA Loneliness Scale [Psychometric research on loneliness: a new German version of the University of California at Los Angeles (UCLA) Loneliness Scale]. Diagnostica 39, 224–239. doi: 10.1026/0012-1924
Eichel, K., Gawande, R., Acabchuk, R. L., Palitsky, R., Chau, S., Pham, A., et al. (2021). A retrospective systematic review of diversity variables in mindfulness research, 2000–2016. Mindfulness 12, 2573–2592. doi: 10.1007/s12671-021-01715-4
El Morr, C., Ritvo, P., Ahmad, F., Moineddin, R., and Team, M. V. C. (2020). Effectiveness of an 8-week web-based mindfulness virtual community intervention for university students on symptoms of stress, anxiety, and depression: randomized controlled trial. JMIR Mental Health 7:e18595. doi: 10.2196/18595
Engert, V., Kok, B. E., Papassotiriou, I., Chrousos, G. P., and Singer, T. (2017). Specific reduction in cortisol stress reactivity after social but not attention-based mental training. Sci. Adv. 3:e1700495. doi: 10.1126/sciadv.1700495
Faucher, J., Koszycki, D., Bradwejn, J., Merali, Z., and Bielajew, C. (2016). Effects of CBT vs. MBSR treatment on social stress reactions in social anxiety disorder. Mindfulness 7, 514–526. doi: 10.1007/s12671-015-0486-4
Fliege, H., Rose, M., Arck, P., Levenstein, S., and Klapp, B. F. (2009). “PSQ. Perceived Stress Questionnaire [Verfahrensdokumentation, PSQ20-Skalenberechnung, PSQ20-Fragebogen Englisch, Deutsch, Deutsch (letzte 2 Jahre), PSQ30-Skalenberechnung, PSQ30-Fragebogen Englisch, Französisch, Deutsch, Italienisch und Spanisch], ” in Leibniz-Institut für Psychologie (ZPID) (Hrsg.), Open Test Archive. Trier: ZPID.
Franke, G. H., Stenzel, S., Rank, C., Herbold, D., and Küch, D. (2015). “Die Brief Symptom Checklist (BSCL) im Einsatz bei Patientinnen und Patienten der Orthopädischen Rehabilitation,” in Jahrestagung des AK Klinische Psychologie, Berlin. Available online at: https://www.researchgate.net/profile/Gabriele-Franke-2/publication/281833605_Die_Brief_Symptom_Checklist_BSCL_im_Einsatz_bei_Patientinnen_und_Patienten_der_orthopadischen_Rehabilitation/links/55fa5a3508aeba1d9f2fe1af/Die-Brief-Symptom-Checklist-BSCL-im-Einsatz-bei-Patientinnen-und-Patienten-der-orthopaedischen-Rehabilitation.pdf (Accessed September 10, 2025).
Green, P., and MacLeod, C. J. (2016). SIMR: An R package for power analysis of generalized linear mixed models by simulation. Methods Ecol. Evol. 7, 493–498. doi: 10.1111/2041-210X.12504
Greiner, B. (2015). Subject pool recruitment procedures: organizing experiments with ORSEE. J. Econ. Sci. Assoc. 1, 114–125. doi: 10.1007/s40881-015-0004-4
Grossman, P., Niemann, L., Schmidt, S., and Walach, H. (2004). Mindfulness-based stress reduction and health benefits: a meta-analysis. J. Psychosom. Res. 57, 35–43. doi: 10.1016/S0022-3999(03)00573-7
Haleem, A., Javaid, M., Qadri, M. A., and Suman, R. (2022). Understanding the role of digital technologies in education: a review. Sustain. Oper. Comput. 3, 275–285. doi: 10.1016/j.susoc.2022.05.004
Hawkley, L. C., Buecker, S., Kaiser, T., and Luhmann, M. (2022). Loneliness from young adulthood to old age: explaining age differences in loneliness. Int. J. Behav. Dev. 46, 39–49. doi: 10.1177/0165025420971048
Hill, M. R., Goicochea, S., and Merlo, L. J. (2018). In their own words: Stressors facing medical students in the millennial generation. Med. Educ. Online 23:1530558. doi: 10.1080/10872981.2018.1530558
Hoge, E. A., Bui, E., Mete, M., Dutton, M. A., Baker, A. W., Simon, N. M., et al. (2023). Mindfulness-based stress reduction vs escitalopram for the treatment of adults with anxiety disorders: a randomized clinical trial. JAMA Psychiatry 80, 13–21. doi: 10.1001/jamapsychiatry.2022.3679
Holt-Lunstad, J., Smith, T. B., Baker, M., Harris, T., and Stephenson, D. (2015). Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspect. Psychol. Sci. 10, 227–237. doi: 10.1177/1745691614568352
Huberty, J., Green, J., Glissmann, C., Larkey, L., Puzia, M., Lee, C., et al. (2019). Efficacy of the mindfulness meditation mobile app “calm” to reduce stress among college students: randomized controlled trial. JMIR mHealth uHealth 7:e14273. doi: 10.2196/14273
Hupfeld, J., and Ruffieux, N. (2011). Validierung einer deutschen Version der Self-Compassion Scale (SCS-D). Zeitschrift für Klinische Psychologie und Psychotherapie 40, 115–123. doi: 10.1026/1616-3443/a000088
Hwang, H., Kim, S. M., Netterstrøm, B., and Han, D. H. (2022). The efficacy of a smartphone-based app on stress reduction: randomized controlled trial. J. Med. Internet Res. 24:e28703. doi: 10.2196/28703
Imel, Z., Baldwin, S., Bonus, K., and MacCoon, D. (2008). Beyond the individual: group effects in mindfulness-based stress reduction. Psychother. Res. 18, 735–742. doi: 10.1080/10503300802326038
Janke, S., and Glöckner-Rist, A. (2014). “Deutsche Version der Satisfaction with Life Scale (SWLS),” in Zusammenstellung sozialwissenschaftlicher Items und Skalen (ZIS)[German version of the Satisfaction with Life Scale (SWLS). Compilation of social science items and scales]. Mannheim: GESIS–Leibniz-Institut für Sozialwissenschaften.
Jensen, L., and Konradsen, F. (2018). A review of the use of virtual reality head-mounted displays in education and training. Educ. Inform. Technol. 23, 1515–1529. doi: 10.1007/s10639-017-9676-0
Jiang, J., and Fryer, L. K. (2024). The effect of virtual reality learning on students' motivation: a scoping review. J. Comput. Assist. Learn. 40, 360–373. doi: 10.1111/jcal.12885
Kabat-Zinn, J. (1982). An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. Gen. Hosp. Psychiatry 4, 33–47. doi: 10.1016/0163-8343(82)90026-3
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: past, present, and future. Clin. Psychol. Sci. Pract. 10, 144–156. doi: 10.1093/clipsy.bpg016
Karing, C. (2024). Long-term effects of combined mindfulness intervention and app intervention compared to single interventions during the COVID-19 pandemic: a randomized controlled trial. Front. Psychol. 15:1355757. doi: 10.3389/fpsyg.2024.1355757
Keng, S-. L., Smoski, M. J., Robins, C. J., Ekblad, A. G., and Brantley, J. G. (2012). Mechanisms of change in mindfulness-based stress reduction: self-compassion and mindfulness as mediators of intervention outcomes. J. Cogn. Psychother. 26, 270–280. doi: 10.1891/0889-8391.26.3.270
Krägeloh, C. U., Medvedev, O. N., Taylor, T., Wrapson, W., Rix, G., Sumich, A., et al. (2019). A pilot randomized controlled trial for a videoconference-delivered mindfulness-based group intervention in a nonclinical setting. Mindfulness 10, 700–711. doi: 10.1007/s12671-018-1024-y
Kriakous, S. A., Elliott, K. A., Lamers, C., and Owen, R. (2021). The effectiveness of mindfulness-based stress reduction on the psychological functioning of healthcare professionals: a systematic review. Mindfulness 12, 1–28. doi: 10.1007/s12671-020-01500-9
Leppert, K., Koch, B., Brähler, E., and Strauß, B. (2008). Die Resilienzskala (RS) – Überprüfung der Langform RS-25 und einer Kurzform RS-13. Klinische Diagnostik Und Evaluation 1, 226–243. Available online at: https://www.academia.edu/download/44388154/A_406.pdf
Levenstein, S., Prantera, C., Varvo, V., Scribano, M. L., Berto, E., Luzi, C., et al. (1993). Development of the perceived stress questionnaire: a new tool for psychosomatic research. J. Psychosom. Res. 37, 19–32. doi: 10.1016/0022-3999(93)90120-5
Lin, L., He, G., Yan, J., Gu, C., and Xie, J. (2019). The effects of a modified mindfulness-based stress reduction program for nurses: a randomized controlled trial. Workplace Health Safety 67, 111–122. doi: 10.1177/2165079918801633
Lin, X. P., Li, B. B., Yao, Z. N., Yang, Z., and Zhang, M. (2024). The impact of virtual reality on student engagement in the classroom–a critical review of the literature. Front. Psychol. 15:1360574. doi: 10.3389/fpsyg.2024.1360574
Linardon, J. (2023). Rates of attrition and engagement in randomized controlled trials of mindfulness apps: systematic review and meta-analysis. Behav. Res. Ther. 170:104421. doi: 10.1016/j.brat.2023.104421
Ma, J., Zhao, D., Xu, N., and Yang, J. (2023). The effectiveness of immersive virtual reality (VR) based mindfulness training on improvement mental-health in adults: a narrative systematic review. Explore 19, 310–318. doi: 10.1016/j.explore.2022.08.001
Madigan, S., Racine, N., Vaillancourt, T., Korczak, D. J., Hewitt, J. M., Pador, P., et al. (2023). Changes in depression and anxiety among children and adolescents from before to during the COVID-19 pandemic: a systematic review and meta-analysis. JAMA Pediatr. 177, 567–577. doi: 10.1001/jamapediatrics.2023.0846
McConville, J., McAleer, R., and Hahne, A. (2017). Mindfulness training for health profession students—the effect of mindfulness training on psychological wellbeing, learning and clinical performance of health professional students: a systematic review of randomized and non-randomized controlled trials. Explore 13, 26–45. doi: 10.1016/j.explore.2016.10.002
McKimmie, B. M., Butler, T., Chan, E., Rogers, A., and Jimmieson, N. L. (2020). Reducing stress: social support and group identification. Group Process. Intergr. Relat. 23, 241–261. doi: 10.1177/1368430218818733
Meta. (2024). Virtuelle Büros und Meetings in Horizon Workrooms | forwork.meta.com. Available online at: https://forwork.meta.com/de/horizon-workrooms/ (Accessed September 30, 2024).
Mitsea, E., Drigas, A., and Skianis, C. (2023). Digitally assisted mindfulness in training self-regulation skills for sustainable mental health: a systematic review. Behav. Sci. 13:1008. doi: 10.3390/bs13121008
Modrego-Alarcón, M., López-del-Hoyo, Y., García-Campayo, J., Pérez-Aranda, A., Navarro-Gil, M., Beltrán-Ruiz, M., et al. (2021). Efficacy of a mindfulness-based programme with and without virtual reality support to reduce stress in university students: a randomized controlled trial. Behav. Res. Ther. 142:103866. doi: 10.1016/j.brat.2021.103866
Moulton-Perkins, A., Moulton, D., Cavanagh, K., Jozavi, A., and Strauss, C. (2022). Systematic review of mindfulness-based cognitive therapy and mindfulness-based stress reduction via group videoconferencing: feasibility, acceptability, safety, and efficacy. J. Psychother. Integr. 32, 110–130. doi: 10.1037/int0000216
Musiat, P., Johnson, C., Atkinson, M., Wilksch, S., and Wade, T. (2022). Impact of guidance on intervention adherence in computerised interventions for mental health problems: a meta-analysis. Psychol. Med. 52, 229–240. doi: 10.1017/S0033291721004621
Pawsey, F., Wong, J. H. K., Kenttä, G., and Näswall, K. (2021). Daily mindfulness is associated with recovery processes among Coaches—A 4-week diary study. Int. Sport Coach. J. 8, 371–381. doi: 10.1123/iscj.2020-0045
Preacher, K. J., and Hayes, A. F. (2004). SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Meth. Instrum. Comput. 36, 717–731. doi: 10.3758/BF03206553
R Core Team. (2022). R version 4.2.2: A language and environment for statistical computing [Computer software]. Vienna, Austria: R Foundation for Statistical Computing. Available online at: http://www.R-project.org (Accessed September 10, 2025).
Riley, T. D., Roy, S., Parascando, J. A., Wile, K., LaGamma, C., Dong, H., et al. (2022). Mindfulness-based stress reduction live online during the COVID-19 pandemic: a mixed methods feasibility study. J. Integrat. Complement. Med. 28, 497–506. doi: 10.1089/jicm.2021.0415
Schmidt, K., Enge, S., and Miller, R. (2020). Reconsidering the construct validity of self-reported chronic stress: a multidimensional item response theory approach. Psychol. Assess. 32:997. doi: 10.1037/pas0000946
Schneider, E. E., Schönfelder, S., Domke-Wolf, M., and Wessa, M. (2020). Measuring stress in clinical and nonclinical subjects using a German adaptation of the Perceived Stress Scale. Int. J. Clin. Health Psychol. 20, 173–181. doi: 10.1016/j.ijchp.2020.03.004
Schwartz, K., Ganster, F. M., and Tran, U. S. (2023). Mindfulness-based mobile apps and their impact on wellbeing in nonclinical populations: systematic review of randomized controlled trials. J. Med. Internet Res. 25:e44638. doi: 10.2196/44638
Schwarzer, R., and Jerusalem, M. (2003). “SWE. Skala zur Allgemeinen Selbstwirksamkeitserwartung [Verfahrensdokumentation, Autorenbeschreibung und Fragebogen],” in Leibniz-Institut für Psychologie (ZPID) (Hrsg.), Open Test Archive. Trier: ZPID.
Sommers-Spijkerman, M., Austin, J., Bohlmeijer, E., and Pots, W. (2021). New evidence in the booming field of online mindfulness: an updated meta-analysis of randomized controlled trials. JMIR Mental Health 8:e28168. doi: 10.2196/28168
Spijkerman, M. P. J., Pots, W. T. M., and Bohlmeijer, E. (2016). Effectiveness of online mindfulness-based interventions in improving mental health: a review and meta-analysis of randomised controlled trials. Clin. Psychol. Rev. 45, 102–114. doi: 10.1016/j.cpr.2016.03.009
Tabachnick, B. G., and Fidell, L. S. (2019). Using Multivariate Statistics (7th Edn.). London: Pearson.
Teoh, S. L., Letchumanan, V., and Lee, L-. H. (2021). Can mindfulness help to alleviate loneliness? A systematic review and meta-analysis. Front. Psychol. 12:633319. doi: 10.3389/fpsyg.2021.633319
Tingley, D., Yamamoto, T., Hirose, K., Keele, L., and Imai, K. (2014). mediation: R Package for Causal Mediation Analysis. J. Stat. Softw. 59, 1–38. doi: 10.18637/jss.v059.i05
Turner, W. A., and Casey, L. M. (2014). Outcomes associated with virtual reality in psychological interventions: where are we now? Clin. Psychol. Rev. 34, 634–644. doi: 10.1016/j.cpr.2014.10.003
Victor, C. R., and Yang, K. (2012). The prevalence of loneliness among adults: a case study of the United Kingdom. J. Psychol. 146, 85–104. doi: 10.1080/00223980.2011.613875
Visted, E., Vøllestad, J., Nielsen, M. B., and Nielsen, G. H. (2015). The impact of group-based mindfulness training on self-reported mindfulness: a systematic review and meta-analysis. Mindfulness 6, 501–522. doi: 10.1007/s12671-014-0283-5
Volkmann, T., Wessel, D., Jochems, N., and Franke, T. (2018). German translation of the multimodal presence scale. Mensch und Computer. Dresden. 2018, 475–479. doi: 10.18420/muc2018-mci-0428
Walach, H., Buchheld, N., Buttenmüller, V., Kleinknecht, N., and Schmidt, S. (2006). Measuring mindfulness—The Freiburg Mindfulness Inventory (FMI). Pers. Individ. Dif. 40, 1543–1555. doi: 10.1016/j.paid.2005.11.025
Wells, R. E., O'Connell, N., Pierce, C. R., Estave, P., Penzien, D. B., Loder, E., et al. (2021). Effectiveness of mindfulness meditation vs headache education for adults with migraine: a randomized clinical trial. JAMA Intern. Med. 181, 317–328. doi: 10.1001/jamainternmed.2020.7090
Wickham, H., Chang, W., and Wickham, M. H. (2016). Package ‘ggplot2.' Create Elegant Data Visualisations Using the Grammar of Graphics. Version 2 (Vienna: The R Foundation), 1–189.
Winter, N., Russell, L., Ugalde, A., White, V., and Livingston, P. (2022). Engagement strategies to improve adherence and retention in web-based mindfulness programs: systematic review. J. Med. Internet Res. 24:e30026. doi: 10.2196/30026
Xu, J., Jo, H., Noorbhai, L., Patel, A., and Li, A. (2022). Virtual mindfulness interventions to promote wellbeing in adults: a mixed-methods systematic review. J. Affect. Disord. 300, 571–585. doi: 10.1016/j.jad.2022.01.027
Yusufov, M., Nicoloro-SantaBarbara, J., Grey, N. E., Moyer, A., and Lobel, M. (2019). Meta-analytic evaluation of stress reduction interventions for undergraduate and graduate students. Int. J. Stress Manag. 26, 132–145. doi: 10.1037/str0000099
Keywords: mindfulness, stress reduction, virtual reality, group meetings, self-compassion, loneliness
Citation: Zinke N, Ritz A and Bunzeck N (2025) Mindfulness-based interventions and student wellbeing: can digital group meetings enhance app-based training? Front. Educ. 10:1613894. doi: 10.3389/feduc.2025.1613894
Received: 22 April 2025; Accepted: 08 September 2025;
Published: 23 October 2025.
Edited by:
Warhel Asim Mohammed, University of Duhok, IraqReviewed by:
Annalisa Valle, Catholic University of the Sacred Heart, ItalyHerman Hay-ming Lo, Hong Kong Polytechnic University, Hong Kong SAR, China
Nabila Enam, Saint Joseph's University, United States
Copyright © 2025 Zinke, Ritz and Bunzeck. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nikolai Zinke, bmlrb2xhaS56aW5rZUB1bmktbHVlYmVjay5kZQ==; Nico Bunzeck, bmljby5idW56ZWNrQHVuaS1sdWViZWNrLmRl