 Elizabeth Hunter
Elizabeth Hunter Kohrine Hazim
Kohrine Hazim Benjamin C. Lok
Benjamin C. Lok Jeanette M. Andrade
Jeanette M. Andrade- 1Department of Food Science and Human Nutrition, University of Florida, Gainesville, FL, United States
- 2Department of Computer & Information Science & Engineering, University of Florida, Gainesville, FL, United States
Introduction: Virtual simulations have been used in various healthcare fields to enhance knowledge and technical skills. Few focus on enhancing personal skills like cultural responsiveness. The purpose of this study was to assess the feasibility of using virtual simulations to enhance cultural responsiveness among nutrition and dietetic undergraduate students.
Methods: Two virtual simulations were developed using Dialogflow and Synthesia software. Both simulations had virtual agents who had chronic kidney disease and another chronic condition and were considered diverse - financial status, age, gender, and race/ethnicity. Content matter experts reviewed the scenarios and potential questions that a student would ask and the responses for accuracy and relevance. Nutrition and dietetic undergraduate students (n = 55) completed a 5-item open-ended survey regarding ease, difficulty, likes, dislikes, improvements of the simulations, and a closed ended question on a 5-point Likert scale towards agreement with cultural responsiveness. NVivo v14 was used to analyze the transcripts from the interaction with the agents and the responses from the survey using conceptual content analysis.
Results: Participants indicated that the two simulations were easy to use. Some difficulties identified were the inability to get a response from the agents. From the transcript analysis, the main themes that participants asked the virtual agents were focused on lifestyle, eating habits, finances, and general medical. Participants (72%) agreed/strongly agreed that their cultural responsiveness improved.
Conclusion: Virtual simulations may be a method to enhance cultural responsiveness. Further research should be conducted to determine if these virtual simulations help students apply cultural responsiveness when working with clients.
1 Introduction
Racial and ethnic diversity within the United States continues to expand, with the largest growth observed among Hispanics/Latinos, Asian Americans, and individuals of mixed ethnicities (Jensen et al., 2020). Beyond this increase in racial and ethnic diversity, the population is also aging; in 2021, 16.8% of the population was over the age of 65 years, compared to 13% in 2010 (Agency for Healthcare Research, 2023). Moreover, there was a decline in household income, especially among Hispanics/Latinos and Asian Americans, with a rising number of Hispanics/Latinos and African Americans living at poverty level (Shrider et al., 2020). Furthermore, health disparities among all age groups still exist for certain ethnic/racial groups, sexes, geographical locations (rural), socioeconomic statuses, and health professionals (Agency for Healthcare Research, 2023). Social and health disparities are contributing to higher rates of non-communicable diseases such as diabetes, cardiovascular disease, obesity, kidney disease, and certain types of cancer (e.g., the breast and colon) (Benavidez et al., 2024) due to many factors, which include poor nutritional quality.
In the healthcare setting, it is essential that practitioners within all fields—physicians, nurses, social workers, dietitians, and others—communicate and provide appropriate treatment to diverse populations. In the dietetic field, to achieve a higher standard of care for diverse populations, the Accreditation Council for Education in Nutrition and Dietetics (ACEND) has required all accredited dietetic programs, undergraduate and graduate, incorporate methods to enhance cultural responsiveness. Cultural responsiveness is the capacity to provide patient-centered care to individuals, despite differences in ethnicity, language, worldview, health beliefs, sexual orientation, religion, and a host of other individual, family, and social variables (Illes et al., 2015). Beaulieu and Jimenez-Gomez (2022) suggested that aspects of cultural competence, knowledge, awareness, and skills be considered for cultural responsiveness. Knowledge is focused on acquiring information about another person’s culture and identifying how it impacts their experiences. Awareness is the ability to discriminate and consider one’s own culture and biases. The skills are the ability to utilize information about a person’s culture to provide tailored care. Overall, a practitioner must not only be cognitively aware of the person’s culture but also respond appropriately (Campinha-Bacote, 2018; Campinha-Bacote, 2011; Campinha-Bacote, 2002; Alexander, 2008).
Based on a cross-sectional study, undergraduate dietetic students (n = 187) indicated they were provided several cultural activities within courses, such as designing menus for racially/ethnically diverse groups, completing case studies on diverse populations, and presenting on nutrition in cultural groups to enhance their cultural responsiveness (Andrade, 2019). Even though exposing dietetic students to these cultural activities may expand their knowledge, attitudes, and beliefs toward culture, limited focus has been on evaluating their cultural responsiveness during a counseling session and the subsequent impact on their clients’ health outcomes. One method may be to expose students to simulated clients (actors) to practice their counseling skills in a safe environment (Stephenson et al., 2015; Horrell and Andrade, 2018; Gibson and Davidson, 2016). Although, for the students to obtain a realistic experience, extensive training needs to take place with these simulated clients (Miller et al., 2011). A study showed that even when students (n = 8) counseled a graduate student who role-played as diverse clients (age, gender, ethnicity, and socioeconomic status) with various diseases (gastritis and liver cirrhosis), results showed students had limited cultural responsiveness (Horrell and Andrade, 2018). A strategy to assess cultural responsiveness during counseling is through a virtual simulation. Virtual simulations have been used in medical education to aid students in enhancing their knowledge, motivation, and skills to solve real-world problems (Gibson and Davidson, 2016; Adams et al., 2010; Zick et al., 2007). Despite its popularity in today’s technological world, virtual simulations are not mainstream, especially for enhancing cultural responsiveness. Thus, the purpose of this study was to assess the feasibility of using virtual simulations to enhance cultural responsiveness among nutrition and dietetic undergraduate students.
2 Methods
2.1 Development of virtual simulations
In a kidney practicum class that the researchers, JMA and KH, facilitate, graduate dietetic students complete six paper-based case studies of culturally diverse adults with varying stages of kidney disease and other co-morbidities to assess their counseling abilities. These case studies were adapted from the National Institutes of Diabetes and Digestive and Kidney Diseases, with incorporation of the researcher’s, JMA, experience working with adults with kidney disease. From these case studies, the researchers chose two to convert to virtual simulations to assess the feasibility of capturing cultural responsiveness as these are generally the first two the students are exposed to in the practicum due to limited comorbidities and complexities and who were considered diverse in ethnicity, gender, socioeconomic status, and dietary habits.
These virtual simulations were designed using the Healthcare Simulation Standards of Best Practice™. These standards were initially designed to improve the training and education of nurses and other healthcare practitioners through traditional education methods (e.g., classroom). However, with the expansion of simulations to train and educate healthcare practitioners, these standards incorporated best practices for these such as consulting with content experts, using realistic scenarios, and piloting and testing these simulations before implementation (Watts et al., 2021). Furthermore, these standards are in place to ensure that these simulations are creating a readiness for clinical practice and improving the quality of patient care and safety. Virtual People Factory (VPF), which uses Google DialogFlow, was the platform used to build these simulations. VPF is an educational tool for health professional students to practice basic interviewing skills (Rossen et al., 2009). VPF uses a web-browser interface through which users interact with virtual agents using a text-based chat mechanism similar to online chat interfaces. The researchers, JMA and EH, designed the virtual agents to respond to potential questions that a student may ask during the counseling session, including broad topics such as social, general medical, and dietary. Based on the questions asked, VPF is programmed to respond based on a priori defined intents for each virtual agent. Specific intents included preparation and cooking of foods, purchasing foods (e.g., shopping at international food stores), traditional spices/foods consumed, availability and access to foods, etc. These potential questions that a student may ask and responses from the virtual agents were reviewed by six content matter experts (three registered dietitian nutritionists, one social worker, and two nurses) who provided additional questions and responses. Thus, a total of 298 potential versions of questions, ranging from 4 to 14 questions per intent, for a total of 32 responses that an agent would provide to the students, were embedded within the simulations (Table 1). Each response had an encoded video of the agent speaking with captions and a transcript chat box. After the DialogFlow intents and responses were loaded into the software, it was exported to Synthesia, an AI video creation platform, to produce the videos. When students asked a question to the agents, if the question triggered an intent, the agents would respond with a recorded video answer. Each intent response had its own video. Closed captioning was present during the videos, and the student was given a transcript of the response in the main chat box (Figures 1, 2). Additionally, each time an intent was triggered, the interview progress bar would grow by one section in one of four specific bar categories, including social, general medical, lifestyle, and dietary habits. As intents were triggered, the student was able to keep track via the discovery box. This box contained short summaries of each previously triggered intent. It is important to note that the student was not required to find all the possible intents when interacting with the agents. The same content matter experts who reviewed the potential questions participated in these simulations to provide feedback on modifications prior to piloting this to students.
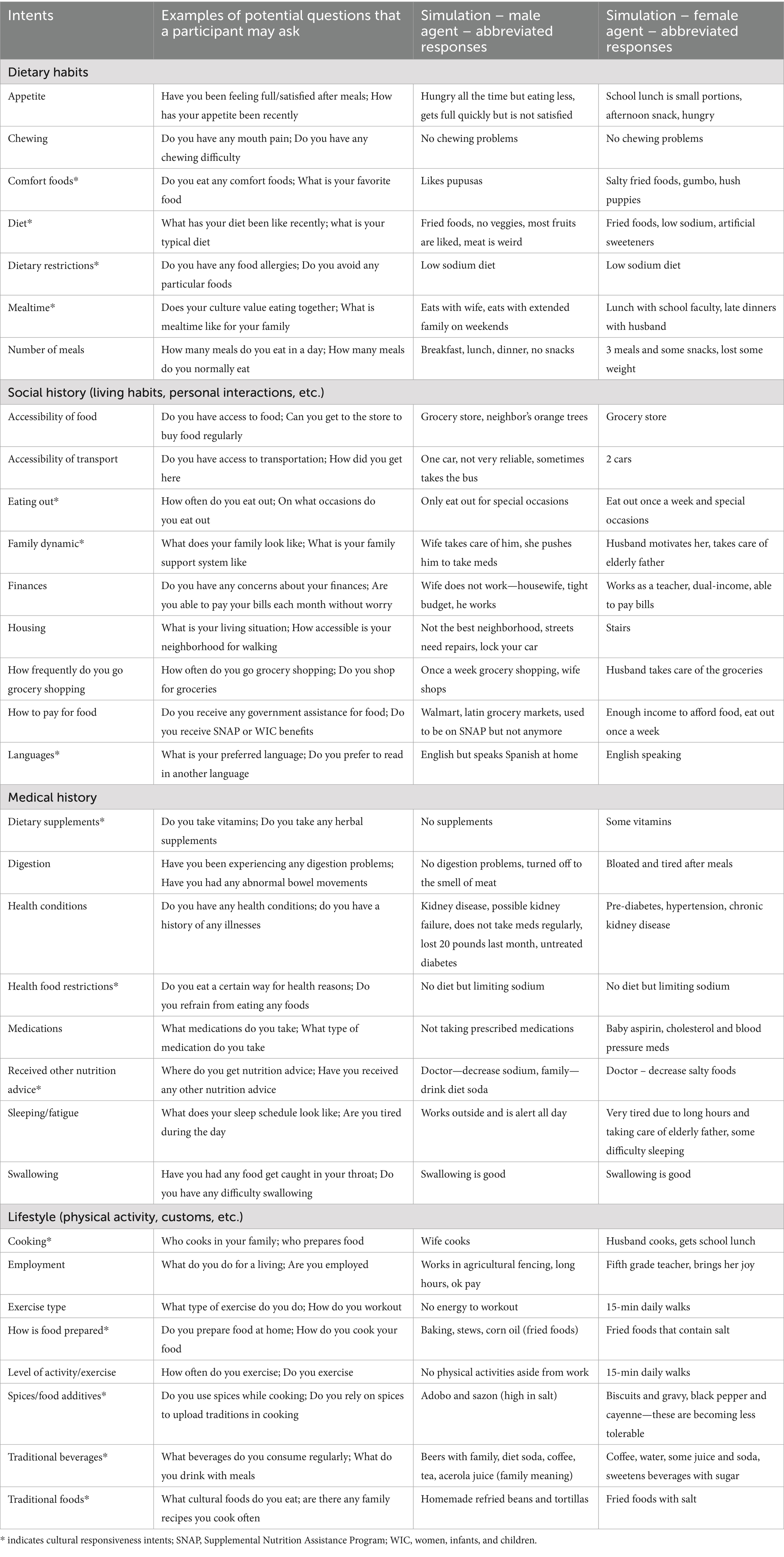
Table 1. Intents, potential questions, and abbreviated responses from simulations.
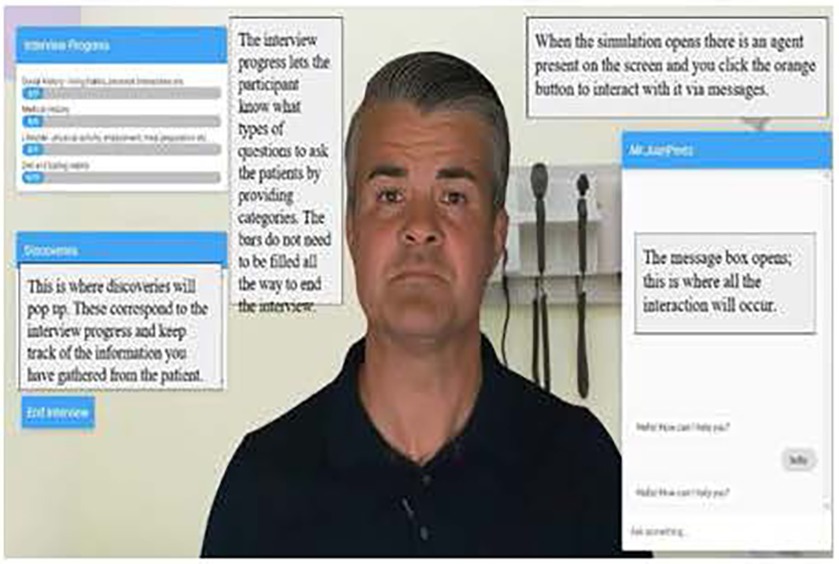
Figure 1. Virtual people factory male agent for the simulation.
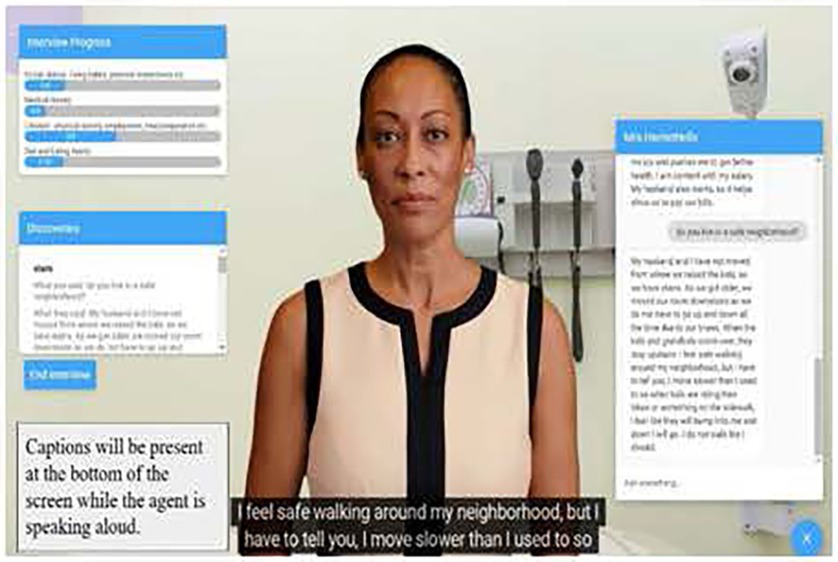
Figure 2. Virtual people factory female agent for the simulation.
2.2 Setting and sample
The feasibility study was conducted in November 2023–February 2024 with upper-level undergraduate nutritional sciences and dietetic students. An email was sent to faculty (n = 4) within the Food Science and Human Nutrition department at the University of Florida who teach either a Medical Nutrition Therapy course or a Nutrition and Metabolism course to recruit students to interact with the virtual simulations. These courses were chosen as they are upper-level divisions in which students, who major in nutritional sciences with sub-classification of pre-medical, pre-dental, pre-physician assistant, or dietetics, either had or were concurrently exposed to a counseling/communication class. For students who expressed interest in participating in the study (n = 90), the researcher, EH, provided participants with a mock medical chart for the virtual agents, instructions on accessing the virtual simulations and completing the surveys. Participants were instructed to type in questions for the virtual agents as if they were counseling a live person based on the medical chart provided to them and to spend at least 20 min on these simulations. Even if the questions they typed were not answered by the virtual agent, they were instructed to continue interacting with the agents. Participants were informed that their questions and the responses from the virtual agents would be downloaded as transcripts for the researchers to analyze. Students completed a survey after interacting with each agent. For each survey, students identified their gender, ethnicity, and whether they were a nutritional sciences or dietetics major, as well as the order in which they completed the virtual simulation, five open-ended questions, and a question based on a 5-point Likert scale. The five open-ended questions were focused on the ease of using the simulations, difficulty of using the simulations, likes about the simulations, dislikes about the simulations, and improvements for the simulations. The 5-point Likert scale question was focused on the participants’ level of agreement (1 = strongly disagree to 5 = strongly agree) if the simulations changed their cultural responsiveness. The study was approved by the UF Institutional Review Board (IRB #202301389), and students consented by agreeing to participate by clicking on the simulation links.
2.3 Statistical analysis
The transcripts from the virtual simulation interactions were downloaded and transcribed word for word into Excel v2307 before being uploaded into NVivo v14. These transcripts were analyzed by two independent coders, JMA and EH, who were trained in this area, using the conceptual content analysis methodology to identify common themes based on frequency (Garrison et al., 2006). In the content analysis method, both qualitative and quantitative techniques can be used to analyze the information to enhance the quality of the phenomena being studied (Bengtsson, 2016; Morgan, 1993; Berg, 2001). The two researchers separately read all transcripts from each interview and developed initial coding schemes. A process of rereading data, redefining existing codes, and developing new codes took place until a final codebook was agreed upon for each data set. Once the themes were established, the researchers identified the frequency. Means were identified for time spent in the simulations, the number of interactions, the number of intentions achieved, and error (i.e., agents that did not respond or responded incorrectly). Furthermore, responses from the open-ended questions about likes, dislikes, ease, and difficulties were analyzed similarly to the transcripts. The Likert scale question was presented as a mean and standard deviation using Excel. A paired t-test was run to determine if there were differences in cultural responsiveness from each virtual simulation.
3 Results
3.1 Participant characteristics
From the initial interest expressed by potential participants, transcripts from the interactions with the virtual agents indicated a total of 63 who completed the female virtual simulation and 58 who completed the male virtual simulation. Participants, on average, spent 27 min with the female virtual agent, interacted with the agent at least 16.9 times, triggered 11 intents, and received 2.9 error messages. For the male agent, participants spent an average of 23 min, interacted with the agent at least 17.9 times, triggered 10 intents, and received 3.0 error messages. A total of 55 participants completed both surveys, in which 64% were nutritional sciences majors, 53% were female participants, 45% were white non-Hispanic, and 89% completed the female agent first (see Table 2 about demographics).
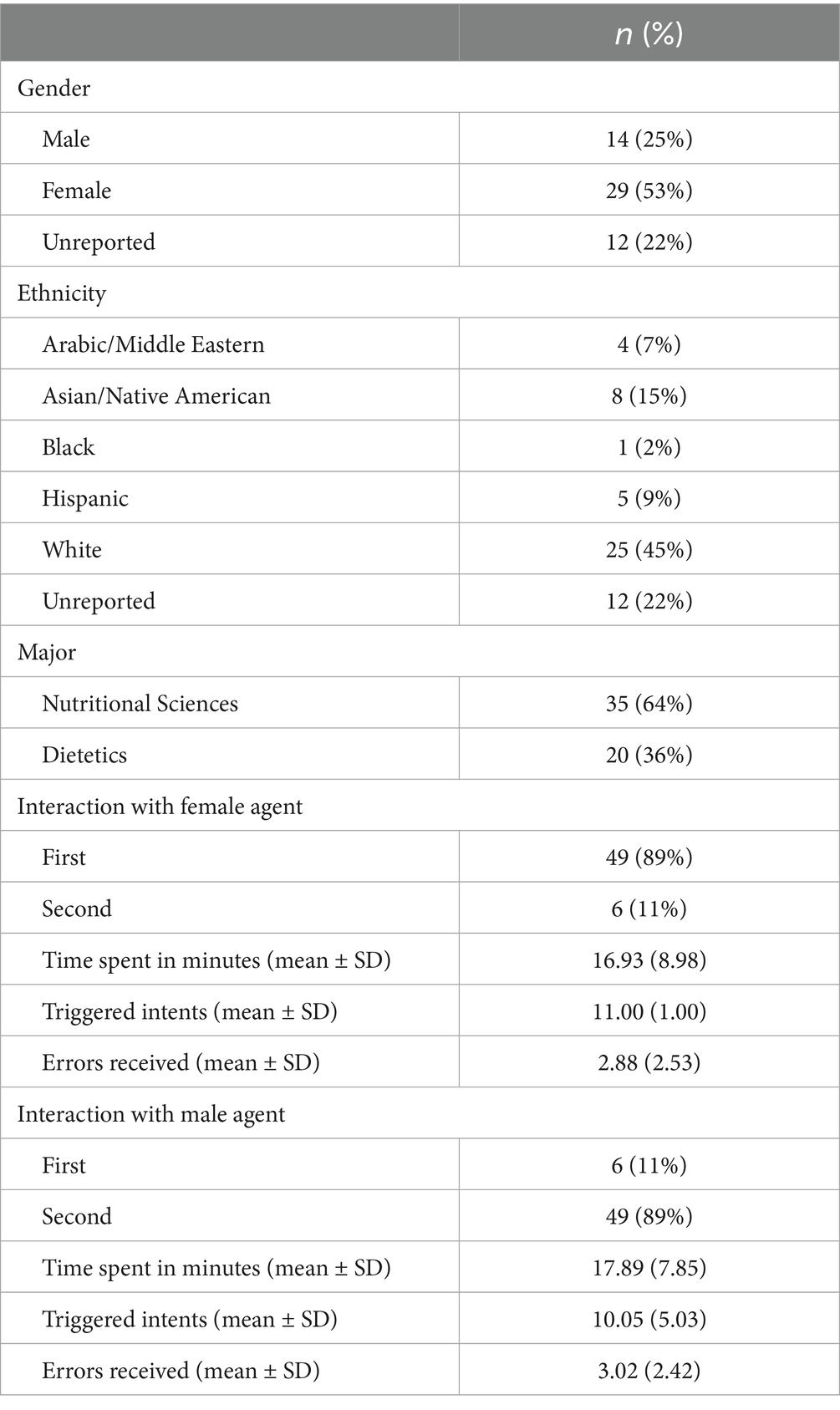
Table 2. Participants’ demographics of those who completed the survey (n = 55).
3.2 Survey results
From the open-ended responses, participants indicated that the simulations were easy to use, and they enjoyed them as they had to think of the questions to ask, as opposed to a paper-based case study or even a role-playing interaction in which the questions need to be approved before interaction. Improvements for these simulations included having the agents respond to more questions and providing more hints on how to ask questions due to error messages or that the agent did not respond. Combining the perceived cultural responsiveness from both surveys, participants (72%) agreed/strongly agreed that their cultural responsiveness improved after interacting with these simulations, with a mean score of 2.9 ± 0.9. The results from a paired t-test indicated a significant difference in scores between the male agent (M = 3.3, SD = 0.9) and the female agent (M = 2.8, SD = 0.9), t(45) = −8.37, p < 0.001 (Table 3).
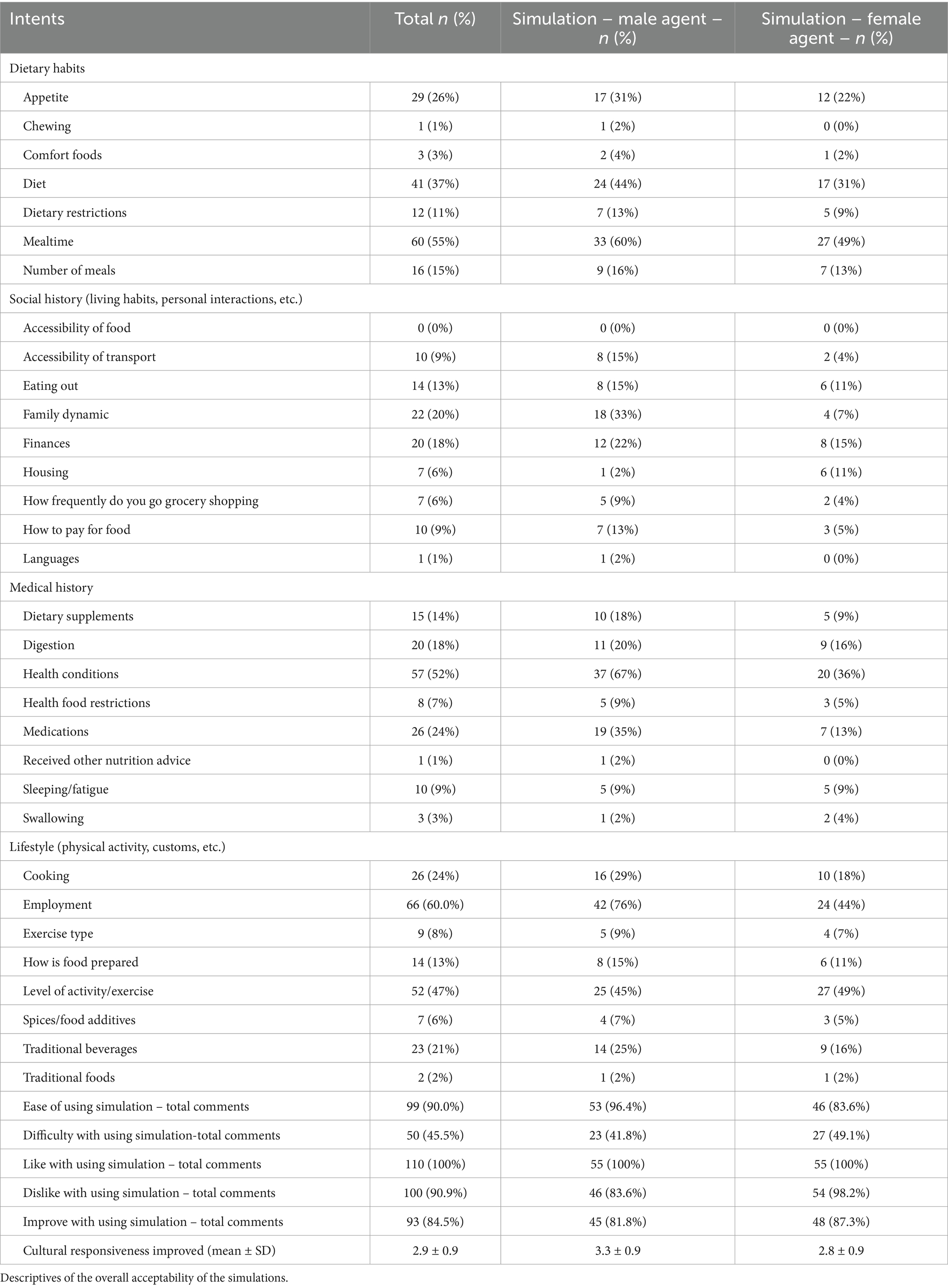
Table 3. Themes and frequency of responses per transcript review (n = 55).
3.3 Virtual simulation transcript results
After reviewing the participants’ transcripts, themes and frequencies were identified. The themes that emerged were lifestyle, finances, dietary/eating habits, and general medical, in which 96.2% of participants asked these. From the 15 intents (46.9% of total intents) in which participants could have asked questions about culture, only 3.8% of questions were focused on traditional foods and beverages consumed and spices and other traditional ingredients used to prepare foods (Table 3).
3.3.1 Lifestyle
The most frequently asked question was focused on the type of job or if the agent was employed (66 times asked; 60%), with the second frequent question was the level of activity and/or exercise type (65 times asked; 55.5%), with finally the family dynamic–social support and living arrangements (36 times asked; 32.7%).
3.3.2 Finances
The most frequently asked question was about income in general (20 questions; 18.2%), and the subsequent frequently asked questions were ability to access healthcare (14 questions; 12.7%), ability to pay for food (10 questions; 9.0%), residence—house, apartment, owner, or renter (7 questions; 6.0%), and frequency of purchasing groceries (7 questions; 6.0%).
3.3.3 Dietary/eating habits
The most frequently asked question was mealtimes (60 questions; 55.0%) and subsequently the most frequently asked were overall diet or dietary restrictions (53 questions; 48.2%), ability to cook, frequency of cooking, and/or preparation of foods (51 questions; 46.4%), appetite (29 questions; 26.0%), and frequency of eating out and/or where they ate out (19 questions; 17.3%). Many questions that focused on cultural/traditional eating habits were from the male virtual agent, in which participants asked about traditional beverages consumed (14 questions, 25%).
3.3.4 General medicine
The most frequently asked questions focused on other medical/health conditions (57 questions; 52.0%), followed by medications/dietary supplements taken (47; 42.3%), issues with digestion (20 questions; 18.0%), sleeping/fatigue, and chewing/swallowing issues (14; 12.7%).
4 Discussion
This study focused on the feasibility of virtual simulations to enhance the cultural responsiveness of nutritional sciences and dietetic students. Participants indicated that their cultural responsiveness improved more with the male agent compared to the female agent, with more cultural questions asked of the male agent than the female agent. Overall, participants thought that the simulations were easy to use, they liked the virtual simulations, and would like to have them in courses. Suggestions for improvement were further instructions about how to word the questions to ensure the virtual agents would respond. The main themes for the questions focused on lifestyle, finances, dietary/eating habits, and general medical.
Participants self-reported that their cultural responsiveness increased after interacting with the simulations, predominantly with the male agent. This was most notably observed in the questions asked of the male virtual agent, who identified as Puerto Rican. As most participants initially asked about the types of foods generally consumed, the virtual agent responded that he consumed rice, beans, and fried meats, which prompted participants to subsequently follow up with traditional beverages consumed. Furthermore, at least in the brief scenario provided to the participants on entering the simulation, it was mentioned that the male agent had a social support system and family meals. Thus, there were more questions asked about family/social support and the mealtime environment compared to the female agent. For the female virtual agent, who identified as African American, the reported food intake was that of traditional American foods, such as chicken and mashed potatoes. Additionally, at least with the brief scenario, there was no mention about social support or other potential cultural activities, which led to less questions asked in these topics. Participants may have been triggered by the nationality of the male virtual agent, whereas the nationality of the female virtual agent was not fully disclosed aside from identifying the ethnicity. Furthermore, in the brief scenario, information was highlighted about family, social support, and background of the male agent compared to the female agent, which may have led to the discrepancies in questions asked. Limited studies have focused on perceptions of cultural responsiveness from pre-allied health students; however, studies that have focused on cultural competence/humility of these students showed similar results when students were exposed to culturally diverse individuals, especially simulated actors who had identified from a specific region (Walkowska et al., 2023; Hawala-Drury and Hill, 2012; Van Kessel et al., 2022).
Several questions focused on non-cultural topics such as the financial aspects of the virtual agents, which included finances in general, paying for food, and housing. Neither of the brief medical scenarios provided to the participants had information about insurance, employment status, or other financially related topics. However, in courses that participants have or are currently enrolled in about communication/counseling, there could be class discussions about social and health disparities, which may have allowed participants to ask these questions. Furthermore, in the counseling class from which participants were recruited, the topics included counseling theories and techniques for counseling individuals, which included types of questions to ask. The questions to ask may cover diet, medical, and social history but have a limited focus on cultural responsiveness. This was like a study conducted in a medical nutrition therapy course in which participants (n = 8) counseled a live actor throughout 16 weeks. They noted that most of their counseling skills improved, except for culture. A few participants who provided further explanation mentioned that they did not think it was relevant to ask cultural questions (Horrell and Andrade, 2018). In a course that has multiple content areas to address, it may be challenging to incorporate culture/cultural responsiveness. However, if students are not exposed to this information during their undergraduate and/or graduate training, the ability for them to enhance and improve their cultural responsiveness while in practice may not occur. It was noted in this study that after a participant asked a question, once the agent responded, limited probing occurred. For example, once the agent responded with the food typically consumed, instead of the participants probing on how the food was prepared or the spices/seasonings used, they may have moved on to another topic. Additionally, no participants asked the agents about their background, such as the environment in which they live, why they consume the foods that they do, etc. As several comments within the dislikes and improvement portion of the survey indicated to provide handouts or resources of the types of questions to ask, if more culture-related topics were mentioned, it may have prompted participants to ask these questions. Additionally, the virtual agents did not provide more information aside from the coded information. Thus, it does not mimic a conversation that may occur in which a client/patient provides further information that contributes to probing. From reviews that have focused on educational methods to enhance cultural competence/humility of pre-allied health students, several studies included within their reviews also showed that students self-reported an increase in these skills after exposure to diverse populations (Walkowska et al., 2023; Van Kessel et al., 2022). However, these methods focused on live actors, shadowing, role-playing, and/or participating within the clinic. Moreover, when the objective is focused on cultural exposure, learners are presented with information to enhance their knowledge and skills toward this topic. For this study, there was no module or other exposure to cultural responsiveness. Integrating modules or training prior to completion of virtual simulations may aid participants in asking questions pertinent to this area. Thus, further exploration needs to be conducted in virtual formats.
To reduce social desirability bias in self-reported instruments (Brenner and DeLamater, 2016), studies suggest validating not only from the instrument itself but also by using other external data sources (Althubaiti, 2016), such as transcript reviews. In this study, 3.8% of questions were related to culture. Even though a total of 72% agreed/strongly agreed that their cultural responsiveness improved with the simulations, upon further focus on each simulation with the mean score, it was predominantly from the male agent. This was in alignment with the questions asked, in which they focused on the spices, foods, and beverages consumed. Therefore, other methods, such as focus groups or additional questions on the open-ended survey, specifically about how or why cultural responsiveness has changed or not, would be necessary.
The improvement areas for these simulations were focused on how to ask questions, as there were errors in which an agent did not respond. Furthermore, depending on the type of question asked, the agent may have responded, but not with the correct information. For example, if a student asked, “how many meals do you eat daily?” Sometimes, the agents responded with the types of foods consumed, rather than the number of meals consumed. This issue may have been related to the coding of these questions and where they were placed as intents. It was identified through the transcripts that participants who asked questions in different ways to obtain information and agents did not respond or responded incorrectly; hence, they stopped participating in the simulations. It is possible that outlining a minimum number of intents would have improved participation despite error messages. Corrective actions that have been completed since the development of these agents have been the use of artificial intelligence systems that are able to detect words and phrases at a higher rate to ensure the information that is provided is accurate. This may allow for the user to interact more effectively with the agent and to spend further time obtaining information until a level of satisfaction is reached. Increased familiarity with the software and repeated uses of the simulation might also reduce the number of error messages received.
Some limitations should be considered when interpreting the results from this study. As the survey was self-reported, selection bias may have occurred (Brenner and DeLamater, 2016). There was an attempt to reduce this bias through review of the transcripts, in which for at least the male agent, there were more questions pertaining to culture than the female agent. For the virtual simulations, some participants ended the simulation once they received multiple error messages when asking questions. As technology has advanced since the conceptualization of this study, utilizing artificial intelligence systems that are compatible with educational systems to allow for more fluid flowing conversations that mimic live sessions would be necessary. Furthermore, aside from an interview, participants did not have to counsel or provide education to the virtual simulation. By including this aspect, it may have allowed participants to expand and explore cultural responsiveness.
In conclusion, students preparing to work in healthcare fields, such as medical, nursing, and dietetics, need to incorporate the appropriate skills and knowledge in working with diverse populations. In the current classroom environment, students may not have opportunities to enhance their cultural responsiveness, thus, providing unique opportunities such as virtual simulations may be a solution. As the use of virtual simulations continues to grow in the medical field, this study adds to the literature, demonstrating that cultural responsiveness can be attained within this environment. Findings illustrated that nutritional science students and dietetic students enjoyed the interactions with the simulations with a few suggestions for improvement. From the student interactions with the agents, they focused on dietary/eating habits, finances, lifestyle, and general medicine, with limited focus on culture, even though they indicated that their cultural responsiveness improved. Further research should explore why cultural responsiveness improved and enhance features of the agents to capture this through interactions with them. As this study showed the feasibility that simulations could enhance cultural responsiveness, future long-term studies should focus on how these improvements translate into practical application.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by UF Institutional Review Board (IRB #202301389). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
EH: Formal analysis, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. KH: Formal analysis, Methodology, Writing – review & editing. BL: Data curation, Software, Writing – review & editing. JA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This project was generously supported by Association of Public and Land-Grant Universities. This research was funded by USDA-NIFA, grant number 2022-67037-36614.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Adams, K. M., Kohlmeier, M., Powell, M., and Zeisel, S. H. (2010). Invited review: nutrition in medicine: nutrition education for medical students and residents. Nutr. Clin. Pract. 25, 471–480. doi: 10.1177/0884533610379606
Agency for Healthcare Research (2023). Available online at: National healthcare quality and disparities report https://www.ahrq.gov/research/findings/nhqrdr/index.html (Accessed November 2, 2024)
Alexander, G. (2008). Cultural competence models in nursing. Crit. Care Nurs. Clin. North Am. 20, 415–421. doi: 10.1016/j.ccell.2008.08.012
Althubaiti, A. (2016). Information bias in health research: definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 9, 211–217. doi: 10.2147/JMDH.S104807
Andrade, J. M. (2019). Determining the associations between dietetic-related activities and undergraduate dietetic students’ general cultural knowledge, attitudes, and beliefs. Nutrients 11:1202. doi: 10.3390/nu11061202
Beaulieu, L., and Jimenez-Gomez, C. (2022). Cultural responsiveness in applied behavior analysis: self-assessment. J. Appl. Behav. Anal. 55, 337–356. doi: 10.1002/jaba.907
Benavidez, G. A., Zahnd, W. E., Hung, P., and Eberth, J. M. (2024). Chronic disease prevalence in the US: sociodemographic and geographic variations by zip code tabulation area. Prev. Chronic Dis. 21:230267. doi: 10.5888/pcd21.230267
Bengtsson, M. (2016). NursingPlus open how to plan and perform a qualitative study using content analysis. NursingPlus Open. 2, 8–14. doi: 10.1016/j.npls.2016.01.001
Berg, B. (2001). Qualitative research methods for the social sciences. Upper Saddle River, NJ: Allyn and Bacon.
Brenner, P. S., and DeLamater, J. (2016). Lies, damned lies, and survey self-reports? Identity as a cause of measurement Bias. Soc. Psychol. Q. 79, 333–354. doi: 10.1177/0190272516628298
Campinha-Bacote, J. (2002). The process of cultural competence in the delivery of healthcare services: a model of care. J. Transcult. Nurs. 13, 181–184. doi: 10.1177/10459602013003003
Campinha-Bacote, J. (2011). Delivering patient-centered care in the midst of a cultural conflict: the role of cultural competence. Online J. Issues Nurs. 16, 1–8. doi: 10.3912/OJIN.Vol16No02Man05
Campinha-Bacote, J. (2018). Cultural competemility: a paradigm shift in the cultural competence versus cultural humility debate-part 1. Online J. Issues Nurs. 24, 1–10. doi: 10.3912/OJIN.Vol24No01PPT20
Garrison, D. R., Cleveland-innes, M., Koole, M., and Kappelman, J. (2006). Revisiting methodological issues in transcript analysis: negotiated coding and reliability. Internet High. Educ. 9, 1–8. doi: 10.1016/j.iheduc.2005.11.001
Gibson, S. J., and Davidson, Z. E. (2016). An observational study investigating the impact of simulated patients in teaching communication skills in preclinical dietetic students. J. Hum. Nutr. Diet. 29, 529–536. doi: 10.1111/jhn.12352
Hawala-Drury, S., and Hill, M. H. (2012). Interdisciplinary: cultural competency and culturally congruent education for millennials in health professions. Nurse Educ. Today 32, 772–778. doi: 10.1016/j.nedt.2012.05.002
Horrell, K., and Andrade, J. (2018). Nutrition and dietetic practice the impact role-playing sessions have on undergraduate dietetic students’ counseling abilities: a qualitative study. J. Hum. Nutr. Diet. 2, 1–8.
Illes, R. A. C., Grace, A. J., Niño, J. R., and Ring, J. M. (2015). Culturally responsive integrated health care: key issues for medical education. Int. J. Psychiatry Med. 50, 92–103. doi: 10.1177/0091217415592368
Jensen, E., Jones, N., Rabe, M., et al. (2020). U.S. population more racially and ethnically diverse than measured. Washington, D.C.: United States Census Bureau.
Miller, C., Lee, M., Rogers, L., and Peck, B. (2011). “Enhancing tertiary healthcare education through 3D MUVE-based simulations” in Teaching through multi-user virtual environments: applying dynamic elements to the modern classroom. eds. G. Vincenti and J. Braman (Hershey, PA: Information Science Reference), 314–365.
Morgan, D. (1993). Qualitative content analysis: a guide to paths not taken. Qual. Health Res. 3, 112–121. doi: 10.1177/104973239300300107
Rossen, B., Lind, S., and Lok, B. (2009). “Human-centered distributed conversational modeling: efficient modeling of robust virtual human conversations” in Intelligent virtual agents. eds. Z. Ruttkay, M. Kipp, A. Nijholt, and H. Vilhjalmsson (Berlin, Germany: Springer Berlin Heidelberg).
Shrider, E. A., Kollar, M., Chen, F., and Semega, J. (2020). Income and poverty in the United States: 2020 current population reports. Washington, D.C: United States Census Bureau.
Stephenson, T., Mayes, L., Combs, E., and Webber, K. (2015). Developing communication skills of undergraduate students through innovative teaching approaches. NACTA J. 59, 313–318. doi: 10.56294/sctconf2024.1214
Van Kessel, G., Fryer, C., Flynn, B., Ferrar, K., Roush, S., and Kessel, V. G. (2022). Effectiveness of training in changing allied health students’ cultural competency skills. Int. J. Allied Health Sci. Pract. 20, 1–16.
Walkowska, A., Przymuszała, P., Marciniak-Stępak, P., Nowosadko, M., and Baum, E. (2023). Enhancing cross-cultural competence of medical and healthcare students with the use of simulated patients—a systematic review. Int. J. Environ. Res. Public Health 20:2505. doi: 10.3390/ijerph20032505
Watts, P. I., McDermott, D. S., Alinier, G., Charnetski, M., Ludlow, J., Horsley, E., et al. (2021). Healthcare simulation standards of best practice TM simulation design. Clin. Simul. Nurs. 58, 14–21. doi: 10.1016/j.ecns.2021.08.009
Keywords: virtual simulations, cultural responsiveness, dietetic students, higher education, feasibility
Citation: Hunter E, Hazim K, Lok BC and Andrade JM (2025) Virtual simulations to address cultural responsiveness of nutrition and dietetic students: a feasibility study. Front. Educ. 10:1629482. doi: 10.3389/feduc.2025.1629482
Edited by:
Paitoon Pimdee, King Mongkut’s Institute of Technology Ladkrabang, ThailandReviewed by:
Didem Keleş, İzmir University of Economics, TürkiyeFiona Mccullough, University of Nottingham, United Kingdom
Copyright © 2025 Hunter, Hazim, Lok and Andrade. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jeanette M. Andrade, amFuZHJhZGUxQHVmbC5lZHU=