 Loredana Urso1†
Loredana Urso1† Grazia Vernaci1,2†
Grazia Vernaci1,2† Jessica Carlet2
Jessica Carlet2 Marcello Lo Mele3
Marcello Lo Mele3 Matteo Fassan4
Matteo Fassan4 Elisabetta Zulato5Giovanni Faggioni2Alice Menichetti2
Elisabetta Zulato5Giovanni Faggioni2Alice Menichetti2 Elisabetta Di Liso2Gaia Griguolo1,2Cristina Falci2Pierfranco Conte1,2Stefano Indraccolo1,5Valentina Guarneri1,2
Elisabetta Di Liso2Gaia Griguolo1,2Cristina Falci2Pierfranco Conte1,2Stefano Indraccolo1,5Valentina Guarneri1,2 Maria Vittoria Dieci1,2*
Maria Vittoria Dieci1,2*- 1Department of Surgery, Oncology and Gastroenterology—DiSCOG, University of Padova, Padova, Italy
- 2Medical Oncology 2, Istituto Oncologico Veneto IOV-IRCCS, Padova, Italy
- 3Department of Pathology, Azienda Ospedaliera Universitaria, Padova, Italy
- 4Department of Medicine-DIMED, Surgical Pathology and Cytopathology Unit, University of Padua, Padova, Italy
- 5Immunology and Molecular Oncology Unit, Istituto Oncologico Veneto IOV-IRCCS, Padova, Italy
Endocrine therapy represents the cornerstone of treatment in hormone receptor-positive (HR+), HER2-negative metastatic breast cancer (mBC). The natural course of this disease is marked by endocrine resistance, mainly due to Estrogen Receptor 1 (ESR1) acquired mutations. The aim of this study is to evaluate the concordance between ESR1 status in metastatic tumor specimens and matched circulating tumor DNA (ctDNA). Forty-three patients with HR+, HER2-negative mBC underwent both a metastatic tumor biopsy and a liquid biopsy at the time of disease progression. DNA extracted from formalin fixed paraffin embedded (FFPE) tumor specimens and ctDNA from matched plasma were analyzed by droplet digital (dd)PCR for the main ESR1 mutations (Y537S, Y537C, Y537N, D538G, E380Q). We observed a total mutation rate of 21%. We found six mutations on tissue biopsy: Y537S (1), D538G (2), Y537N (1), E380Q (2). Three patients with no mutations in tumor tissue had mutations detected in ctDNA. The total concordance rate between ESR1 status on tumor tissue and plasma was 91%. Our results confirm the potential role of liquid biopsy as a non-invasive alternative to tissue biopsy for ESR1 mutation assessment in mBC patients.
Introduction
Hormone receptor-positive (HR+) breast cancer (BC) accounts for about one third of all BC (1). Endocrine manipulation is the mainstay of treatment of HR+/human epidermal growth factor 2- negative (HER2-) BC, and the traditional armamentarium includes aromatase inhibitors (AI), selective estrogen receptor modulators (SERMs, as tamoxifen), selective estrogen receptor degraders (SERDs, as fulvestrant).
However, in the metastatic setting, development of resistance invariably occurs, and about 15–20% of patients show de novo resistance (2–4). Several mechanisms have been linked to endocrine resistance, including mutation in Estrogen Receptor 1 (ESR1) gene. This gene, located on chromosome 6, encodes for ERα, a member of the nuclear hormone receptors superfamily (5). In response to estrogens, ER interacts with specific estrogen response elements (EREs) on DNA and promotes cell proliferation. Moreover, ER harbors numerous bi-directional cross-talks with membrane tyrosine kinase receptors such as epidermal growth factor (EGFR), HER2, insulin-like growth factor (IGFR), that play an important role in breast cancer cells’ growth and survival (6–9).
ESR1 mutations mostly occur in specific hotspots located in the ligand-binding domain of the receptor and result in estrogen-independent function of ER (10). The most common ESR1 mutations are Y537S/N/C and D538G (11).
ESR1 mutations are rare in primary BC and become more frequent in the metastatic setting, with a total rate of about 30% (12, 13). These mutations are relatively rare in patients treated with tamoxifen only and typically develop after previous exposure to aromatase inhibitors, as a result of the selective pressure of endocrine deprivation therapies (12–18).
Mutant cells are resistant to AI in vitro, while high doses of tamoxifen and fulvestrant inhibit signaling of mutant ER (14, 19). In the combined analysis of the SoFEA and EFECT trials, ESR1 mutations have been shown to be associated with worse progression-free survival (PFS) and overall survival (OS) in patients treated with exemestane versus fulvestrant, with an objective response rate of 9.5 versus 0.0% on respectively fulvestrant and exemestane (17, 20). These findings confirm that ESR1 mutated patients still derive clinical benefit from endocrine therapy with fulvestrant. In this context, preclinical data have shown the effectiveness of new potent oral SERDs (21–24).
Whether detection of ESR1 mutation could impact on treatment decision is still under investigation (NCT03079011).
Circulating tumor DNA (ctDNA) is a cell-free DNA released by tumor cells in the blood (25). ctDNA can be detected in the plasma of patients with cancer, and its analysis may represent a non-invasive tool for detecting and monitoring key gene mutations.
Although different studies showed the potential of Next Generation sequencing (NGS) or Droplet Digital PCR (ddPCR) analyses in identifying ESR1 mutations in ctDNA from HR+ metastatic breast cancer (mBC), few reports compared the sensitivity of the detection in tissue specimens compared to matched plasma samples (26–30).
We conducted a prospective study in a cohort of HR+/HER2- mBC patients to assess the concordance of ESR1 mutation evaluated on matched tumor tissue samples from a metastatic lesion and ctDNA from plasma.
Materials and Methods
Patients
The study population was represented by a prospective cohort of 43 HR+/HER2- (defined as ER or PgR expression ≥10% and HER2 immunohistochemical 0–1+ or 2+ with no amplification at fluorescence in situ hybridization) mBC patients (Age ≥ 18 years) who underwent a biopsy of a metastatic lesion at our Institution, as part of the routine diagnostic-therapeutic management, prior to the start of a new line of systemic treatment. Patients were enrolled from July 2018 to August 2020.
Patients were registered in a prospective database reporting demographics, clinical-pathological features, type of treatment for early (eBC) and advanced BC (aBC), results for ESR1 mutation, and follow-up data.
Treatment for metastatic disease was administered in accordance to national guidelines.
The study (SPIDER) was approved by the Ethic Committee of Istituto Oncologico Veneto (Cod. CESC IOV 2018/26, February 26, 2018). Informed consent was obtained from all subjects.
Samples Preparation and Analysis
DNA Extraction From Formalin-Fixed Paraffin-Embedded Tissue Biopsy
We collected 43 FFPE tumor biopsies, reviewed by a pathologist (MF) for tumor tissue quality and quantity. Genomic DNA (gDNA) was extracted from five FFPE sections containing at least 30% of tumor cells using QIAmp® DNA Micro Kit (Qiagen) following the manufacturer’s instructions. DNA was quantified by Nanodrop One (Thermo Scientific®). Twenty ng of total gDNA was used for the detection of ESR1 mutations.
Plasma Sample Collection and DNA Extraction
Liquid biopsy was performed at the same time point of tissue collection, simultaneously with the routine blood exams, with no additional venipuncture. Twenty ml of blood samples was collected in two Helix ctDNA Stabilization tubes (Diatech Pharmacogenetics SRL) and processed within 24 h. Plasma was separated by centrifugation at 2,000 × g for 10 min at 4°C. Next, to further purify plasma from corpuscular cells, the supernatant was centrifuged at 20,000 × g for 10 min at 4°C. Plasma was stored at −80°C until analysis. ctDNA was extracted from 2 ml of plasma using the Maxwell® RSC ccfDNA Plasma Kit (Promega, Madison, Wisconsin, USA), and quantified using Qubit dsDNA HS Assay Kit (Life Technologies, USA). 7.5 µl of ctDNA was used for the detection of ESR1 mutations.
Detection of ESR1 Mutations by ddPCR
ESR1 mutations were analyzed by ddPCR on the QX200 ddPCR system (Bio-Rad Laboratories) following the manufacturer’s instructions. We assessed the following hotspots in 43 tissue specimens: Y537S, Y537C, Y537N, D538G, E380Q. These hotspots were selected based on their frequency among ESR1 mutations in published studies (11) and in the COSMIC dataset (v92). ddPCR probes were purchased from Bio-Rad. To set-up the method, each assay was tested using pSEPT plasmid bearing the indicated mutations. All samples had adequate proportion of tumor cells. All the mutations detected in tumor tissue biopsy were checked in matched ctDNA. As Y537C/N was barely detected in our tissue sample cohort (0.0 and 2.3%, respectively), all plasma samples were analyzed for the three main hotspots: Y537S, D538G, E380Q. Each sample of tumor tissue DNA was run in duplicate; each sample of cfDNA was run in triplicate.
We defined a positive mutation in tissue DNA with a threshold of 1% allele frequency to avoid technical biases from fixation process (31); for ctDNA we used a cutoff of three mutant-positive droplets per well, following the manufacturer guidelines. Allele frequency for each mutation was determined considering fractional abundance of mutated droplets above the total.
Sample Size and Statistical Analysis
Statistical analyses were conducted using IBM SPSS (Version 20) Software. The association between categorical variables was evaluated using the χ2 test.
We evaluated the concordance between ESR1 mutation analysis on matched tissue DNA and ctDNA samples. We considered three concordance measures: i) the rate of ctDNA mutated samples over the total of tumor tissue mutated samples (ctDNA confirmation rate), ii) the rate of concordant mutated matched pairs over the total of pairs showing at least one mutated sample (ctDNA, tumor tissue, or both; concordance mutation rate), and iii) the rate of concordant mutated or concordant wild-type matched pairs over the total of 43 analyzed pairs (total concordance rate).
PFS was calculated as the time interval from the date of liquid biopsy to disease progression or death, whichever was first. OS was calculated from the date of liquid biopsy to death. Patients without an event were censored at the date of last follow-up.
Survival curves were estimated using the Kaplan–Meier model and we used the log-rank test to study differences between groups. For all the performed tests, significance was inferred for a value p <0.05.
Results
Patients’ Characteristics
From July 2018 to August 2020 we enrolled 43 patients.
Clinicopathologic characteristics at the time of first breast cancer diagnosis are reported in Table 1. Seventeen patients had a stage IV de novo disease at the time of first diagnosis. All patients had HR+/HER2- tumor phenotype as defined by the protocol on at least one tumor biopsy (either primary tumor or relapse). Among those patients who experienced a disease relapse after a prior diagnosis of primary breast cancer, all but three had a concordant HR-positive and HER2-negative tumor phenotype on both primary tumor and relapse biopsy. Three patients with HER2-positive (n = 2) and triple negative (n = 1) primary breast cancer had a subsequent relapse biopsy showing HR-positive and HER2-negative tumor phenotype. For one patient with HR+/HER2− phenotype on relapse biopsy, receptor status of the primary tumor was not available (Supplementary Tables 2 if 3). Median age at first breast cancer diagnosis was 50 years (range 42–62). Most patients had a tumor of ductal histology (n = 37, 86%) and histologic grade 3 (n = 24, 56%). Treatments for early breast cancer are listed in Table 1.
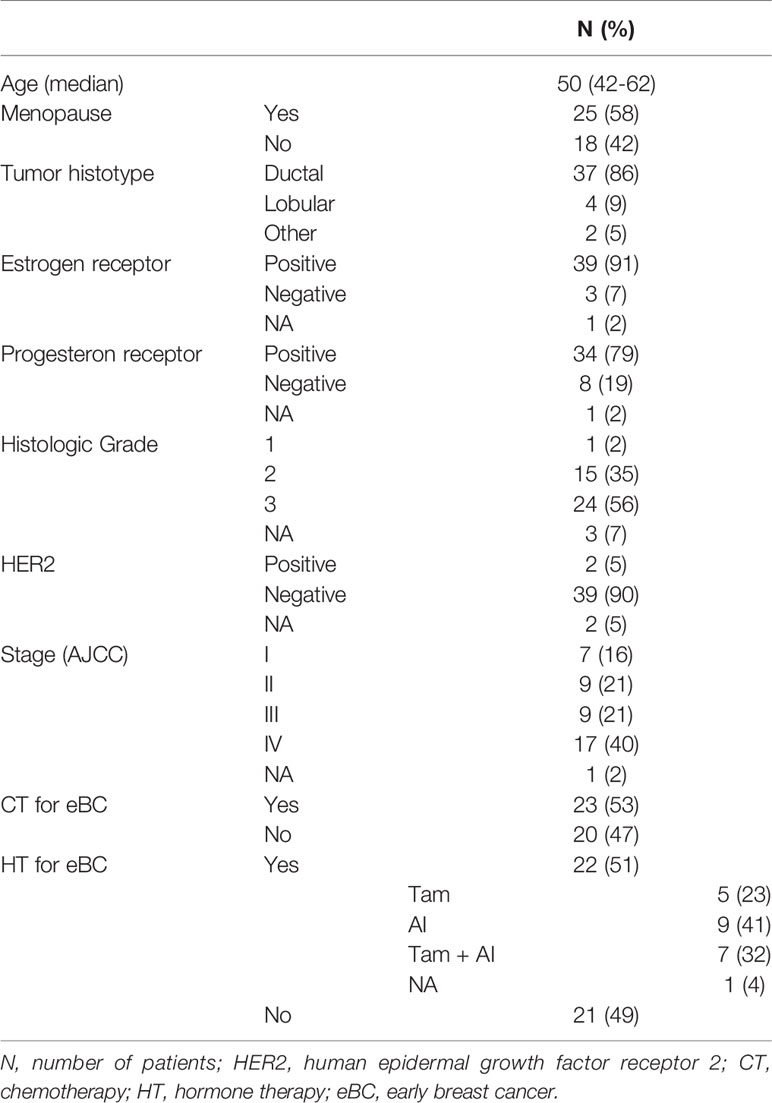
Table 1 Clinical-pathological characteristics at diagnosis and treatment for eBC.
Patients’ characteristics at the time of enrollment in this study are reported in Table 2. The majority of patients presented with visceral metastases (n = 29, 67%), and half of the patients had more than three metastatic sites involved (n = 22, 51%) (Supplementary Table 4). Twenty-eight patients (65%) had not received any prior systemic therapy for advanced disease at the time of enrolment; 26 patients had been previously exposed to AIs for the treatment of early and/or advanced disease (60%).
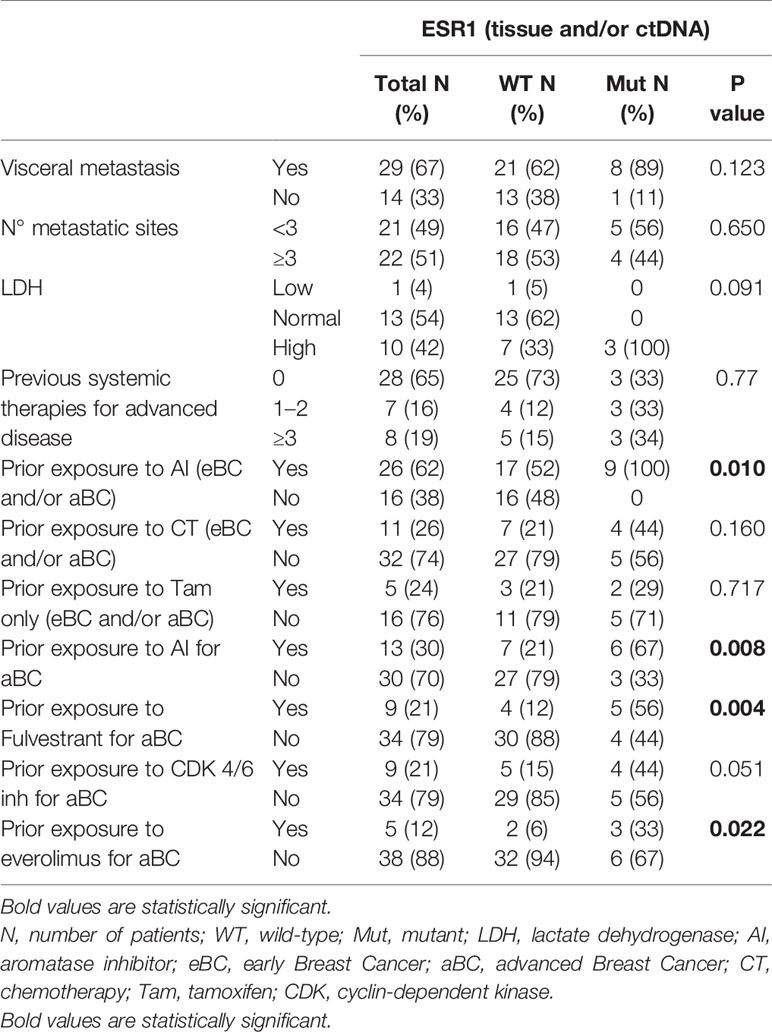
Table 2 Patients’ characteristics according to ESR1 status.
Concordance of ESR1 Mutation on Tumor Tissue Biopsies and ctDNA
We identified the following ESR1 mutations in six of 43 patients (14%) on DNA extracted from tumor biopsies: Y537S (one subject), Y537N (one subject) E380Q (two subjects), D538G (two subjects). Four of the six mutations were confirmed on ctDNA (ctDNA confirmation rate: 67%) (Supplementary Figure 1). The low concentration of cfDNA in the two discordant cases, with less than 700 total droplets detected in the plasma, probably reduced the sensitivity of the test.
In order to verify that identified mutations were acquired de novo, we tested four out of six matched primary tumors, and no mutations were found (data not shown).
The most frequent ESR1 mutations (Y537S, D538G, and E380Q) were assessed on all ctDNA samples. For three WT tissue samples, the analysis of matched plasma revealed the D538G mutation in ctDNA, one of these ctDNA samples showed two concomitant hotspot mutations (D538G and Y537S). Two of these three patients with ESR1 mutation detected on ctDNA and not on tumor tissue had a high disease burden, with more than three metastatic sites and visceral involvement.
Figure 1 shows the results of ddPCR for the discordant cases between tissue and plasma samples.
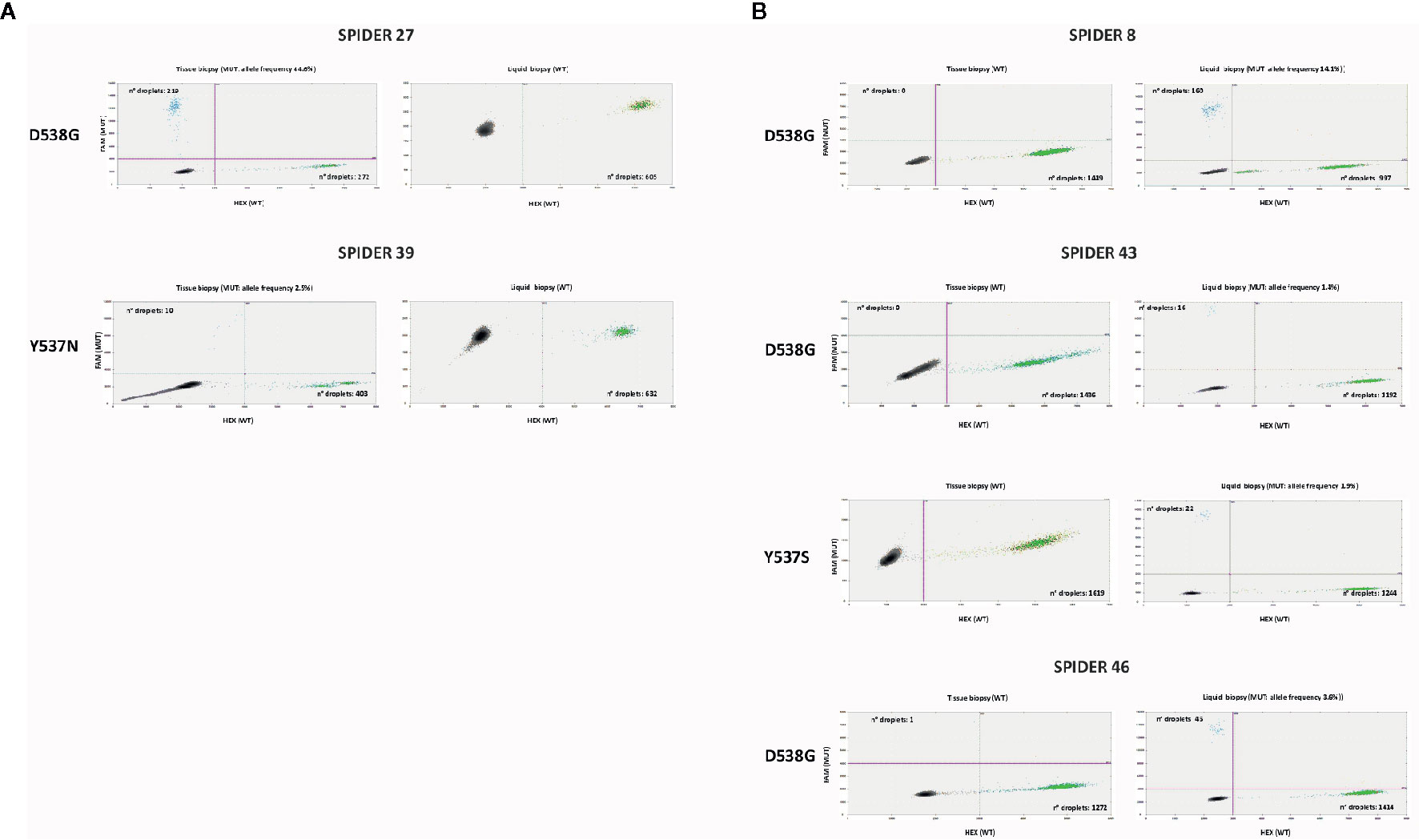
Figure 1 Discordant cases in ddPCR between tissue and liquid biopsy: ddPCR plots show the number of positive droplets for the indicated hotspot mutations (FAM+: blue dots), and the number of wt droplets (HEX+: green dots). Double positive droplets (FAM+/HEX+) were excluded from the analysis. (A) Samples mutated in tissue biopsy and WT in liquid biopsy. (B) Samples WT in tissue biopsy and mutated in liquid biopsy.
Our total ESR1 mutation rate, considering cases showing a mutation on tumor tissue and/or ctDNA over the total, was 21% (9/43).
The concordance rate for mutation was 44% (four cases with ESR1 mutation on matched tissue and ctDNA over nine cases with a mutation detected on tissue and/or ctDNA samples). The total concordance rate (considering the Y537S, D538G and E380Q) between tumor tissue and plasma was 91% (39 concordant mutated or concordant wild-type matched pairs over 43 total pairs analyzed, Figure 2 and Supplementary Table 1).
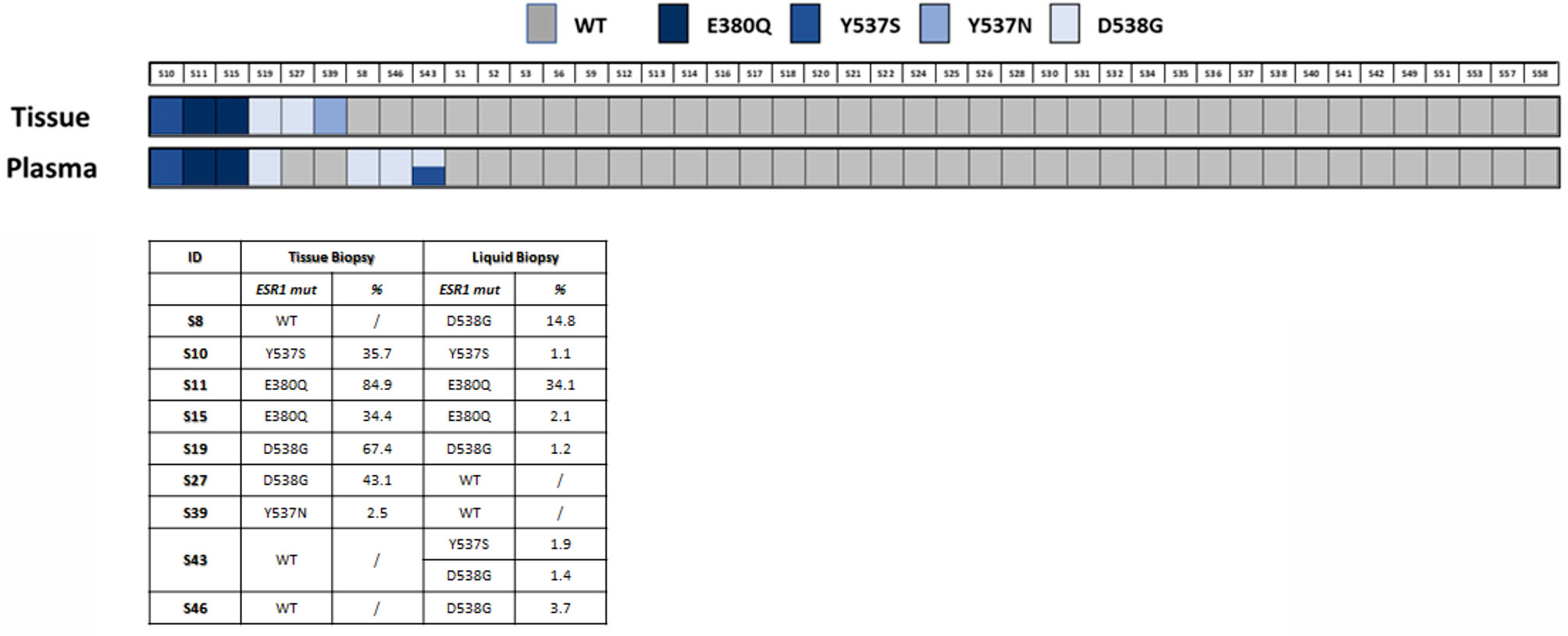
Figure 2 ESR1 mutation in tissue and plasma samples. The lower panel shows the specific ESR1 mutations found and their representation in samples as percentage (%) of mutated allele.
Association of ESR1 Mutations With Patients’ Characteristics and Previous Therapies
Table 2 shows the association of ESR1 mutation status with clinicopathological characteristics at study entry.
We found a statistically significant association between prior exposure to AI (considering both the early and the advanced setting and the advanced setting alone) and the presence of ESR1 mutation (p = 0.010 and p = 0.008 respectively). Prior exposure to fulvestrant and everolimus for aBC was also associated with higher rate of ESR1 mutation (p = 0.004 and p = 0.022 respectively). However, when we performed logistic regression multivariable analysis, none of these factors remained statistically significant after adjusting for the other variables (prior exposure to chemotherapy, aromatase inhibitors, tamoxifen, fulvestrant, CDK4/6 inhibitors, everolimus) (data not shown). The majority of the patients (n = 35, 81%) had received two or less previous treatment for BC, with no differences in terms of ESR1 mutational status. Features related with disease burden were not associated with presence of ESR1 mutation. Notably, we found a numerically higher rate of ESR1 mutation in the case of visceral disease (eight out nine mutated patients, p = 0.123). LDH value as assessed at the time of liquid biopsy was available for 24 patients. All of the three patients with ESR1 mutation had high LDH, although this association was not statistically significant (p = 0.091).
Survival Analysis
Median follow-up was 14.5 months (95%CI 12.0–17.0 months).
As shown in Figure 3, there was no significant difference in PFS between ESR1 wild-type and ESR1-mutated patients: median PFS was 13.6 months (95%CI 9.6–17.5 months) in ESR1 wild type population versus 6.4 months (95%CI 0.00–15.6 months) in ESR1 mutant patients (log-rank p = 0.283, HR 1.62, 95%CI 0.7–4.0, p = 0.288).
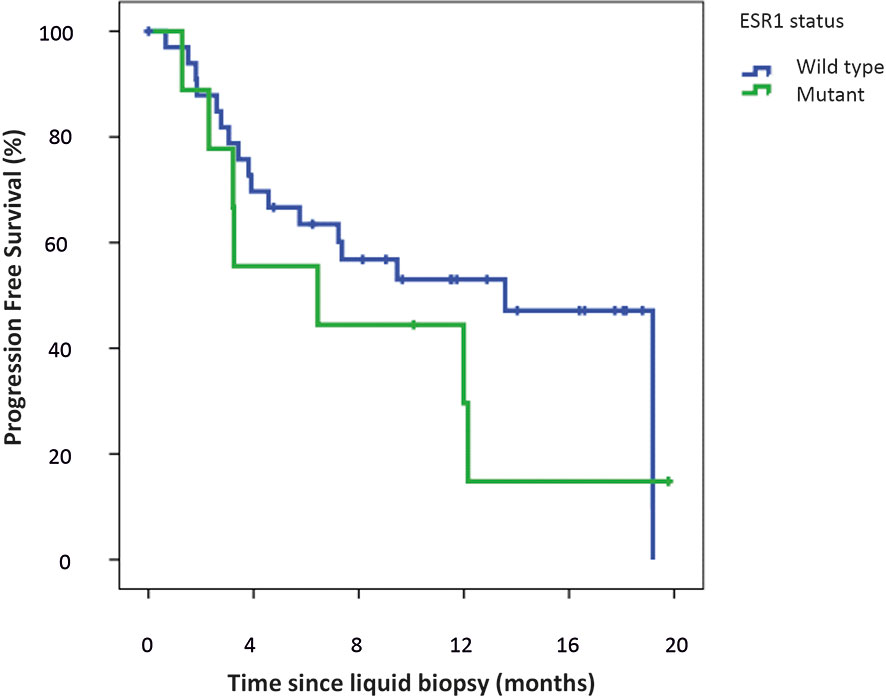
Figure 3 Kaplan–Meier progression-free survival analysis according to ESR1 status.
Discussion
During the natural history of HR+/HER2-negative mBC, the onset of endocrine resistance is the rule, and a deep understanding of underlying mechanisms remains an unmet medical need.
Analysis of tumor tissue allows obtaining crucial predictive and prognostic information to guide clinicians, although, due to its static nature, a tumor biopsy is not able to capture intra-tumor heterogeneity and temporal evolution under exposure to specific treatments. Furthermore, multiple-biopsy testing could affect patients’ quality of life (QoL). In this perspective, liquid biopsy offers a charming tool to overcome these limitations.
In our work, we prospectively examined ESR1 status in the tissue of 43 patients with HR+/HER2- mBC and in matched plasma samples. Overall, our total mutation rate was 21%, consistent with main literature data (12, 14, 15, 26, 29).
In this study, the total concordance rate between ESR1 status on tumor tissue DNA and ctDNA was 91%. Among the five discordant cases described in our cohort, two out of six mutations detected in tumor tissue DNA were undetectable in ctDNA. A possible reason may be represented by the low concentration of cfDNA in these two patients. The other three discordant cases showed a mutation on ctDNA but not on matched tumor tissue DNA. This finding suggests that ctDNA might be able to represent the heterogeneity of mBC, particularly in the case of patients with multi-metastatic disease.
Available literature reports an overall concordance rate for ESR1 mutation between matched tissue and plasma samples ranging from 47 to 100%, although the majority of the data come from small series (Table 3) (15, 29, 30, 32, 36).
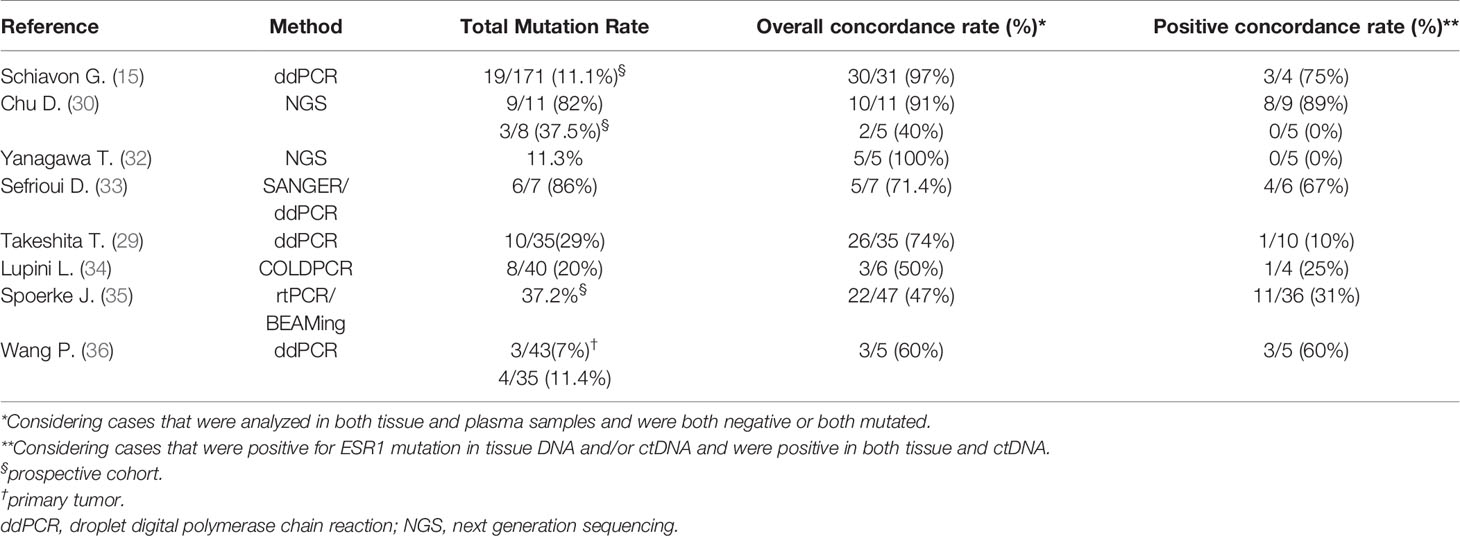
Table 3 Studies investigating concordance of ESR1 mutation between tissue and plasma.
Altogether, our results are consistent with previous studies which evaluated ESR1 mutation by ddPCR and showed a rate of concordance of 74 to 97% (15, 29).
Across available data, concordance rates appear to be lower when the ESR1 mutation status on ctDNA is compared with sequencing results obtained from archival tumor tissue samples rather than recent tumor biopsies, as performed in our study.
All patients with a detectable ESR1 mutation (in either tissue DNA or ctDNA) had a previous exposure to AI (p = 0.010), confirming the role of the selective pressure of hormonal-deprivation therapy in endocrine resistance development (17, 35). With regard to other therapies for advanced disease, a statistically significant association between ESR1 mutation and fulvestrant (p = 0.004) and everolimus (p = 0.022) was evident. It must be taken into account that all these patients received AI either previously (in case of fulvestrant) or concomitantly (in case of everolimus). Thus, the exposure to such therapies is a surrogate of prior treatment with aromatase inhibitor.
In a recent meta-analysis, the presence of ESR1 mutation was associated with worse PFS and OS in a population of patients with HR+/HER2-negative mBC (37).
In our population, the presence of ESR1 mutation did not impact on either PFS or OS, although this finding could be biased by the small sample size with limited follow-up. Moreover, the limited sample size did not allow conducting a survival analysis stratified by line of treatment.
Although this study has limitations, such as the small sample size, the mono-institutional enrollment, and ESR1 status assessment in a single laboratory, our results showed high concordance rate between tumor tissue and ctDNA (91%), providing evidence of reliability and feasibility of liquid biopsy to analyze ESR1 mutation in breast cancer patients. Moreover, the presence of ESR1 mutation in ctDNA of three patients lacking ESR1 mutations in the tissue suggests that liquid biopsy may capture the heterogeneous genetic landscape of metastatic tumors.
In conclusion, our data confirm the potential role of liquid biopsy as a valid and preferable non-invasive alternative to tissue biopsy for ESR1 mutation assessment in mBC patients. Moreover, it can also allow longitudinal tracking of ESR1 mutations during the disease course at multiple timepoints without exposing patients to the risks related to invasive procedures. Clinical utility of this approach to guide treatment choices is currently under investigation.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by IOV Ethics Committee (Cod. CESC IOV 2018/26, February 26, 2018). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MVD conceived and designed the study. LU, JC, MLM, MF, and EZ performed molecular and pathology analyses. GV, GF, AM, EL, GG, CF, PC, VG, and MVD followed the patients. GV and LU acquired, analyzed, and interpretated data and drafted the work. MVD, VG, PC, and SI revised the work critically and approved the final version. All authors agree to be personally accountable for the content of the work. All authors contributed to the article and approved the submitted version.
Funding
This research was supported by grant from Italian Ministry of Health (GR-2016-02361279 to MVD).
Conflict of Interest
MVD reports personal fees for consultancy/advisory role from: Eli Lilly, Novartis, Celgene, Genomic Health, outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank Dr. Barbara Belletti, Division of Molecular Oncology, Centro di Riferimento Oncologico di Aviano (CRO), IRCCS, National Cancer Institute, 33081 Aviano, Italy and Dr. Ben Ho Park, M.D., Ph.D., Adjunct Professor of Oncology, Breast Cancer Program, The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, for providing us with the pSEPT plasmid bearing ESR1 mutations. The QX200 ddPCR system (Bio-Rad Laboratories) was obtained through a grant provided by the University of Padova, Italy (2015).
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.625636/full#supplementary-material
References
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin (2015) 65(2):87–108. doi: 10.3322/caac.21262
2. Rugo HS, Rumble RB, Macrae E, Barton DL, Connolly HK, Dickler MN, et al. Endocrine Therapy for Hormone Receptor-Positive Metastatic Breast Cancer: American Society of Clinical Oncology Guideline. J Clin Oncol (2016) 34(25):3069–103. doi: 10.1200/JCO.2016.67.1487
3. Maass H, Jonat W, Stolzenbach G, Trams G. The problem of nonresponding estrogen receptor-positive patients with advanced breast cancer. Cancer (1980) 46(12 Suppl):2835–7. doi: 10.1002/1097-0142(19801215)46:12+<2835::AID-CNCR2820461420>3.0.CO;2-M
4. Jeselsohn R, Buchwalter G, De Angelis C, Brown M, Schiff R. ESR1 mutations-a mechanism for acquired endocrine resistance in breast cancer. Nat Rev Clin Oncol (2015) 12(10):573–83. doi: 10.1038/nrclinonc.2015.117
5. Le Goff P, Montano MM, Schodin DJ, Katzenellenbogen BS. Phosphorylation of the human estrogen receptor. Identification of hormone-regulated sites and examination of their influence on transcriptional activity. J Biol Chem (1994) 269(6):4458–66. doi: 10.1016/S0021-9258(17)41801-1
6. Klinge CM. Estrogen receptor interaction with estrogen response elements. Nucleic Acids Res (2001) 29(14):2905–19. doi: 10.1093/nar/29.14.2905
7. Schiff R, Massarweh S, Shou J, Osborne CK. Breast cancer endocrine resistance: how growth factor signaling and estrogen receptor coregulators modulate response. Clin Cancer Res (2003) 9(1 Pt 2):447S–54S.
8. Nicholson RI, McClelland RA, Robertson JF, Gee JM. Involvement of steroid hormone and growth factor cross-talk in endocrine response in breast cancer. Endocr Relat Cancer (1999) 6(3):373–87. doi: 10.1677/erc.0.0060373
9. Ali S, Coombes RC. Endocrine-responsive breast cancer and strategies for combating resistance. Nat Rev Cancer (2002) 2(2):101–12. doi: 10.1038/nrc721
10. Feil R, Wagner J, Metzger D, Chambon P. Regulation of Cre recombinase activity by mutated estrogen receptor ligand-binding domains. Biochem Biophys Res Commun (1997) 237(3):752–7. doi: 10.1006/bbrc.1997.7124
11. Segal CV, Dowsett M. Estrogen Receptor Mutations in Breast Cancer—New Focus on an Old Target. Clin Cancer Res (2014) 2014:20. doi: 10.1158/1078-0432.CCR-14-0067
12. Robinson DR, Wu YM, Vats P, Su F, Lonigro RJ, Cao X, et al. Activating ESR1 mutations in hormone-resistant metastatic breast cancer. Nat Genet (2013) 45(12):1446–51. doi: 10.1038/ng.2823
13. Toy W, Shen Y, Won H, Green B, Sakr RA, Will M, et al. ESR1 ligand- binding domain mutations in hormone-resistant breast cancer. Nat Genet (2013) 45(12):1439–45. doi: 10.1038/ng.2822
14. Jeselsohn R, Yelensky R, Buchwalter G, Frampton G, Meric-Bernstam F, Gonzalez-Angulo AM, et al. Emergence of constitutively active estrogen receptor-alpha mutations in pretreated advanced estrogen receptor-positive breast cancer. Clin Cancer Res (2014) 20(7):1757–67. doi: 10.1158/1078-0432.CCR-13-2332
15. Schiavon G, Hrebien S, Garcia-Murillas I, Cutts RJ, Pearson A, Tarazona N, et al. Analysis of ESR1 mutation in circulating tumor DNA demonstrates evolution during therapy for metastatic breast cancer. Sci Transl Med (2015) 7(313):313ra182. doi: 10.1126/scitranslmed.aac7551
16. Reinert T, Saad ED, Barrios CH, Bines J. Clinical Implications of ESR1 Mutations in Hormone Receptor-Positive Advanced Breast Cancer. Front Oncol (2017) 7:26. doi: 10.3389/fonc.2017.00026
17. Fribbens C, O’Leary B, Kilburn L, Hrebien S, Garcia-Murillas I, Beaney M, et al. Plasma ESR1 Mutations and the Treatment of Estrogen Receptor-Positive Advanced Breast Cancer. J Clin Oncol (2016) 34(25):2961–8. doi: 10.1200/JCO.2016.67.3061
18. Razavi P, Chang MT, Xu G, Bandlamudi C, Ross DS, Vasan N, et al. The Genomic Landscape of Endocrine-Resistant Advanced Breast Cancers. Cancer Cell (2018) 34(3):427–38.e6. doi: 10.1016/j.ccell.2018.08.008
19. Merenbakh-Lamin K, Ben-Baruch N, Yeheskel A, Dvir A, Soussan-Gutman L, Jeselsohn R, et al. D538G mutation in estrogen receptor-α: A novel mechanism for R.; Brown, M.; Miller, V.A.; Sarid, D.; et al. D538G mutation in estrogen receptor-α: A novel mechanism for acquired endocrine resistance in breast cancer. Cancer Res (2013) 73:6856–64. doi: 10.1158/0008-5472.CAN-13-1197
20. Turner NC, Swift C, Kilburn L, Fribbens C, Beaney M, Garcia-Murillas I, et al. ESR1 Mutations and Overall Survival on Fulvestrant versus Exemestane in Advanced Hormone Receptor–Positive Breast Cancer: A Combined Analysis of the Phase III SoFEA and EFECT Trials. Clin Cancer Res (2020) 26)(19):5172–7. doi: 10.1158/1078-0432.CCR-20-0224
21. Weir HM, Bradbury RH, Lawson M, Rabow AA, Buttar D, Callis RJ, et al. AZD9496: An Oral Estrogen Receptor Inhibitor That Blocks the Growth of ER-Positive and ESR1-Mutant Breast Tumors in Preclinical Models. Cancer Res (2016) 76(11):3307–18. doi: 10.1158/0008-5472.CAN-15-2357
22. Joseph JD, Darimont B, Zhou W, Arrazate A, Young A, Ingalla E, et al. The selective estrogen receptor downregulator GDC-0810 is efficacious in diverse models of ER+ breast cancer. Elife (2016) 5:10.7554/eLife.15828. doi: 10.7554/eLife.44851
23. Bihani T, Patel HK, Arlt H, Tao N, Jiang H, Brown JL, et al. Elacestrant (RAD1901), a Selective Estrogen Receptor Degrader (SERD), Has Antitumor Activity in Multiple ER(+) Breast Cancer Patient-derived Xenograft Models. Clin Cancer Res (2017) 23(16):4793–804. doi: 10.1158/1078-0432.CCR-16-2561
24. Garner F, Shomali M, Paquin D, Lyttle CR, Hattersley G. RAD1901: a novel, orally bioavailable selective estrogen receptor degrader that demonstrates antitumor activity in breast cancer xenograft models. Anticancer Drugs (2015) 26(9):948–56. doi: 10.1097/CAD.0000000000000271
25. De Rubis G, Rajeev Krishnan S, Bebawy M. Liquid Biopsies in Cancer Diagnosis, Monitoring, and Prognosis. Trends Pharmacol Sci (2019) 40(3):172–86. doi: 10.1016/j.tips.2019.01.006
26. Guttery DS, Page K, Hills A, Woodley L, Marchese SD, Rghebi B, et al. Noninvasive detection of activating estrogen receptor 1 (ESR1) mutations in estrogen receptor-positive metastatic breast cancer. Clin Chem (2015) 61(7):974–82. doi: 10.1373/clinchem.2015.238717
27. Chandarlapaty S, Chen D, He W, Sung P, Samoila A, You D, et al. Prevalence of ESR1 Mutations in Cell-Free DNA and Outcomes in Metastatic Breast Cancer: A Secondary Analysis of the BOLERO-2 Clinical Trial. JAMA Oncol (2016) 2(10):1310–5. doi: 10.1001/jamaoncol.2016.1279
28. Jeannot E, Darrigues L, Michel M, Stern MH, Pierga JY, Rampanou A, et al. A single droplet digital PCR for ESR1 activating mutations detection in plasma. Oncogene (2020) 39(14):2987–95. doi: 10.1038/s41388-020-1174-y
29. Takeshita T, Yamamoto Y, Yamamoto-Ibusuki M, Tomiguchi M, Sueta A, Murakami K, et al. Comparison of ESR1 Mutations in Tumor Tissue and Matched Plasma Samples from Metastatic Breast Cancer Patients. Transl Oncol (2017) 10(5):766–71. doi: 10.1016/j.tranon.2017.07.004
30. Chu D, Paoletti C, Gersch C, VanDenBerg DA, Zabransky DJ, Cochran RL, et al. ESR1 Mutations in Circulating Plasma Tumor DNA from Metastatic Breast Cancer Patients. Clin Cancer Res (2016) 22(4):993–9. doi: 10.1158/1078-0432.CCR-15-0943
31. Prentice LM, Miller RR, Knaggs J, Mazloomian A, Aguirre Hernandez R, Franchini P, et al. Formalin fixation increases deamination mutation signature but should not lead to false positive mutations in clinical practice. PloS One (2018) 13(4):e0196434. doi: 10.1371/journal.pone.0196434
32. Yanagawa T, Kagara N, Miyake T, Tanei T, Naoi Y, Shimoda M, et al. Detection of ESR1 mutations in plasma and tumors from metastatic breast cancer patients using next-generation sequencing. Breast Cancer Res Treat (2017) 163(2):231–40. doi: 10.1007/s10549-017-4190-z
33. Sefrioui D, Perdrix A, Sarafan-Vasseur N, Dolfus C, Dujon A, Picquenot JM, et al. Short report: Monitoring ESR1 mutations by circulating tumor DNA in aromatase inhibitor resistant metastatic breast cancer. Int J Cancer (2015) 137(10):2513–9. doi: 10.1002/ijc.29612
34. Lupini L, Moretti A, Bassi C, Schirone A, Pedriali M, Querzoli P, et al. High-sensitivity assay for monitoring ESR1 mutations in circulating cell-free DNA of breast cancer patients receiving endocrine therapy. Sci Rep (2018) 8(1):4371–018-22312-x. doi: 10.1038/s41598-018-22312-x
35. Spoerke JM, Gendreau S, Walter K, Qiu J, Wilson TR, Savage H, et al. Heterogeneity and clinical significance of ESR1 mutations in ER-positive metastatic breast cancer patients receiving fulvestrant. Nat Commun (2016) 7:11579. doi: 10.1038/ncomms11579
36. Wang P, Bahreini A, Gyanchandani R, Lucas PC, Hartmaier RJ, Watters RJ, et al. Sensitive Detection of Mono- and Polyclonal ESR1 Mutations in Primary Tumors, Metastatic Lesions, and Cell-Free DNA of Breast Cancer Patients. Clin Cancer Res (2016) 22(5):1130–7. doi: 10.1158/1078-0432.CCR-15-1534
Keywords: Estrogen Receptor 1 (ESR1), metastatic breast cancer, endocrine therapy, ctDNA, liquid biopsy
Citation: Urso L, Vernaci G, Carlet J, Lo Mele M, Fassan M, Zulato E, Faggioni G, Menichetti A, Di Liso E, Griguolo G, Falci C, Conte P, Indraccolo S, Guarneri V and Dieci MV (2021) ESR1 Gene Mutation in Hormone Receptor-Positive HER2-Negative Metastatic Breast Cancer Patients: Concordance Between Tumor Tissue and Circulating Tumor DNA Analysis. Front. Oncol. 11:625636. doi: 10.3389/fonc.2021.625636
Received: 03 November 2020; Accepted: 29 January 2021;
Published: 11 March 2021.
Edited by:
Attila A. Seyhan, Brown University, United StatesReviewed by:
John Martens, Erasmus Medical Center, NetherlandsMaria Munoz Caffarel, Biodonostia Health Research Institute (IIS Biodonostia), Spain
Copyright © 2021 Urso, Vernaci, Carlet, Lo Mele, Fassan, Zulato, Faggioni, Menichetti, Di Liso, Griguolo, Falci, Conte, Indraccolo, Guarneri and Dieci. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Vittoria Dieci, bWFyaWF2aXR0b3JpYS5kaWVjaUB1bmlwZC5pdA==
†These authors share first authorship