 Shiqiang Su1
Shiqiang Su1 Chao Sun
Chao Sun- 1Department of Urology, Shijiazhuang People’s Hospital, Shijiazhuang, China
- 2Institute of Medicine and Health, Hebei Medical University, Shijiazhuang, China
Background: Serum gamma-glutamyltransferase (GGT) has been reported to be correlated with survival in a variety of malignancies. However, its effect on patients with bladder cancer (BC) treated by radical cystectomy has never been evaluated.
Patients and Methods: We retrospectively evaluated 263 patients who underwent radical surgery in our center. Baseline features, hematologic variables, and follow-up data were obtained. The endpoints included overall survival (OS), cancer-specific survival (CSS), and disease-free survival (DFS). The relationship between GGT and survival were evaluated.
Results: The median follow-up period for all patients was 34.7 (22.9-45.9) months. At the last follow-up, 67 patients died, 51 patients died of cancer, 92 patients experienced disease recurrence. Patients with an elevated serum GGT had a higher rate of pT3-T4 tumors. Patients with a higher preoperative serum GGT had a lower rate of OS, CSS and DFS (P < 0.001 for all). Multivariate analysis identified that preoperative serum GGT was independent predictor of OS (HR: 3.027, 95% CI: 1.716-5.338; P < 0.001), CSS (HR: 2.115, 95% CI: 1.093-4.090; P = 0.026), DFS (HR: 2.584, 95% CI: 1.569-4.255; P < 0.001). Age, diabetes history, pathologic T stage, and lymph node status also were independent predictors of prognosis for BC patients.
Conclusions: Our results indicated that preoperative serum GGT was an independent prognosis predictor for survival of BC patients after radical cystectomy, and can be included in the prognostic models.
Introduction
Bladder cancer (BC) is the second most common malignance of the urinary system. In 2020, there were estimated 81,400 new cases and 17,980 deaths of bladder cancer in the United States (1). Though most of newly diagnosed bladder cancers are presented with non-muscle-invasive disease, nearly 25% of them are muscle invasive BC. For non-muscle-invasive BC, though treating by transurethral tumor exsection, patients often experienced disease recurrence and progression. The rate of disease recurrence for non-muscle-invasive BC in 5 years ranges from 50% to 70%, and the 5-year progression rate ranges from 10% to 30% (2). For muscle invasive BC, after radical surgery and lymph node dissection, these patients have a poor long-term prognosis, with about a 50% for 5-year survival rate (3). Despite the significant progress in systematic therapy, the high rate of mortality for muscle invasive BC hasn’t changed. Since the common clinical staging system performed poor, more prognosis predictors are required to effectively classify BC patients for optimal treatment.
Due to the clinical convenience, several circulating biomarkers have been reported in bladder cancer prognosis, including lactate dehydrogenase (4), hemoglobin, white blood cell count, De Ritis ratio, albumin-globulin ratio, and so on (5). As a membrane bounding enzyme, serum gamma-glutamyltransferase (GGT) has been found to exert key value in glutathione metabolism and is crucial for cellular protection against various oxidants. The pathological state of oxidative stress, which can be observed in the various tumor microenvironment, has been found to result in an elevation in glutathione and GGT levels (6, 7). In addition, GGT is considered to play a potentially vital role in tumor development, disease progression, and anti-cancer drug resistance (7–10). Moreover, GGT has been found as an important prognostic biomarker in various cancer entities, including breast cancer (11), hepatocellular carcinoma (12), ovarian cancer (13), prostate cancer (14), renal cell carcinoma (15), and esophageal squamous cell carcinoma (16). However, to our knowledge, no study has looked at the role of GGT in bladder cancer prognosis. Hence, we conducted this study to assess the prognostic value of preoperative serum GGT in BC patients undergoing radical surgery.
Materials and Methods
Patient Selection
We retrospectively screened the medical records of bladder cancer in our hospital. Between January 2011 and December 2016, there were 315 cases with BC treated by open or laparoscopic radical cystectomy. Patients having the evidence of distant metastasis, undergoing neoadjuvant chemotherapy, having preoperative infection and liver diseases, accompanying other malignances were excluded. Lastly, after excluding 3 patients lacking key data, 268 patients were included for data analyzing (Figure 1). The study was approved by the institutional review board before it was carried out.
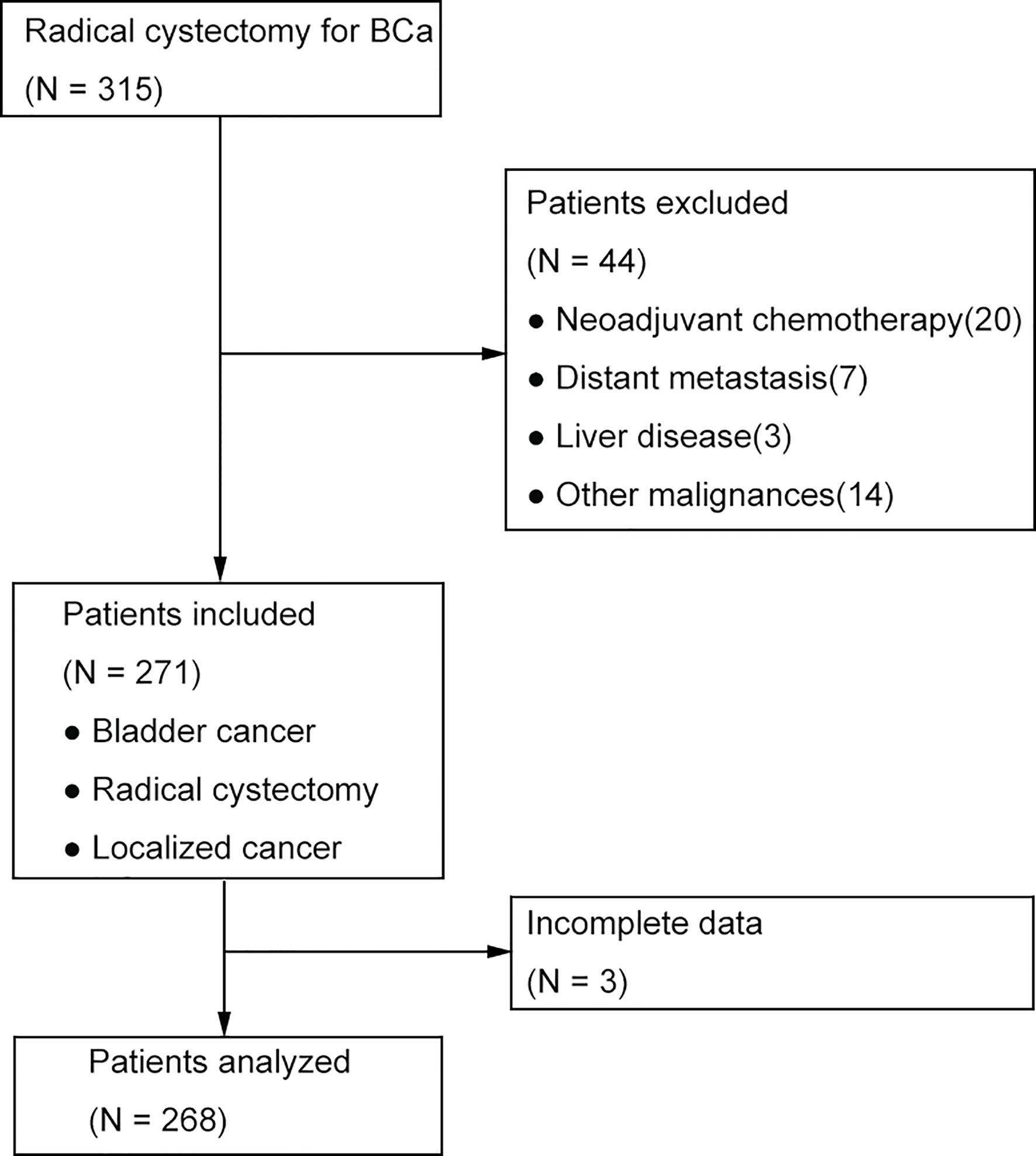
Figure 1 The flow chart for patient selection.
Variables
These variables were extracted from medical records in our hospital. Preoperative variables consisted of demographics and hematological variables, including gender, age, body mass index, ASA score, history of smoking, history of common chronic diseases, serum hemoglobin, number of white blood cell, platelet to lymphocyte ratio (PLR), neutrophil to lymphocyte ratio (NLR), lymphocyte to monocyte ratio (LMR), serum albumin and GGT. The levels of hematological variables were examined by the most recent blood sample examinations conducted within 2 weeks prior to surgery. GGT was detected by IFCC method. After the reaction, the absorption peak was detected at 405nm to calculate the serum concentration of GGT. Postoperative variables consisted of surgical and pathological variables, including surgical approach and procedure, pT stage, status of lymph node, surgical margin, postoperative chemotherapy. The cut-off values of hemoglobin, white blood cell, PLR, NLR, LMR, albumin were decided according to our previous study (4). The best cut-off point of preoperative GGT was estimated through receiver operating characteristic (ROC) curve analysis, which was used as a classification variable to divide the whole cohort into two groups.
Postoperative Management
Patient follow-up embraced regular clinical examinations and laboratory tests, imaging methods included chest radiography, abdominal/pelvic ultrasound, CT or MRI. Follow-up evaluations were conducted every three months for the first two years, semiannually for the next two years, and annually thereafter. Postoperative chemotherapy was administered for some patients when needed and accepted.
Statistical Analysis
The primary outcome was overall survival (OS), the secondary outcomes included cancer-specific survival (CSS) and disease-free survival (DFS).
The normality of continuous variables (age and BMI) was checked by the Kolmogorov-Smirnov test. Due to the non-normal distribution, they were described as median and interquartile range. According to the cut-off value of GGT, all patients were divided into two groups. The associations between preoperative GGT and demographics, hematological, surgical, pathological variables were studied. For continuous variables, the Wilcoxon rank-sum test was applied. For classified variables, the Pearson X 2 or Fisher exact test was applied. The Kaplan-Meier method was applied to calculate patients’ clinical endpoints, and the differences between two groups were compared using the log-rank test. The univariate and multivariate Cox proportion analysis was performed to determine the effect of regular variables and preoperative GGT on OS, CSS and DFS. Hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated by cox proportional analysis. Statistical analyses were conducted using SPSS 14.0 (Chicago, Illinois, USA). A two-sided P < 0.05 was deemed as statistically significant.
Results
Patient Characteristics
The baseline features of included patients were presented in Table 1. The median age at the time of operation was 63 (54-69) years. Of all patients, 41 (15.3%) were female, 227 (84.7%) were male. Seventy-eight (29.1%), forty-one (15.3%), and thirty-seven (13.8%) patients were respectively accompanied with hypertension, diabetes, and cardiac disease. Open and laparoscopic surgeries were performed in 104 (38.8%) and 164 (61.2%) patients, and 13 (4.9%) underwent neobladder, 206 (76.9%) underwent ileal conduit, 49 (18.3%) underwent continent cutaneous. Seventy-eight (29.1%) patients presented with pathological T3-T4 tumors, 40 (14.9%) patients presented with positive lymph node, 7 (2.6%) patients presented with positive surgical margin. Further postoperative chemotherapy was administered in 47 (17.5%) patients.
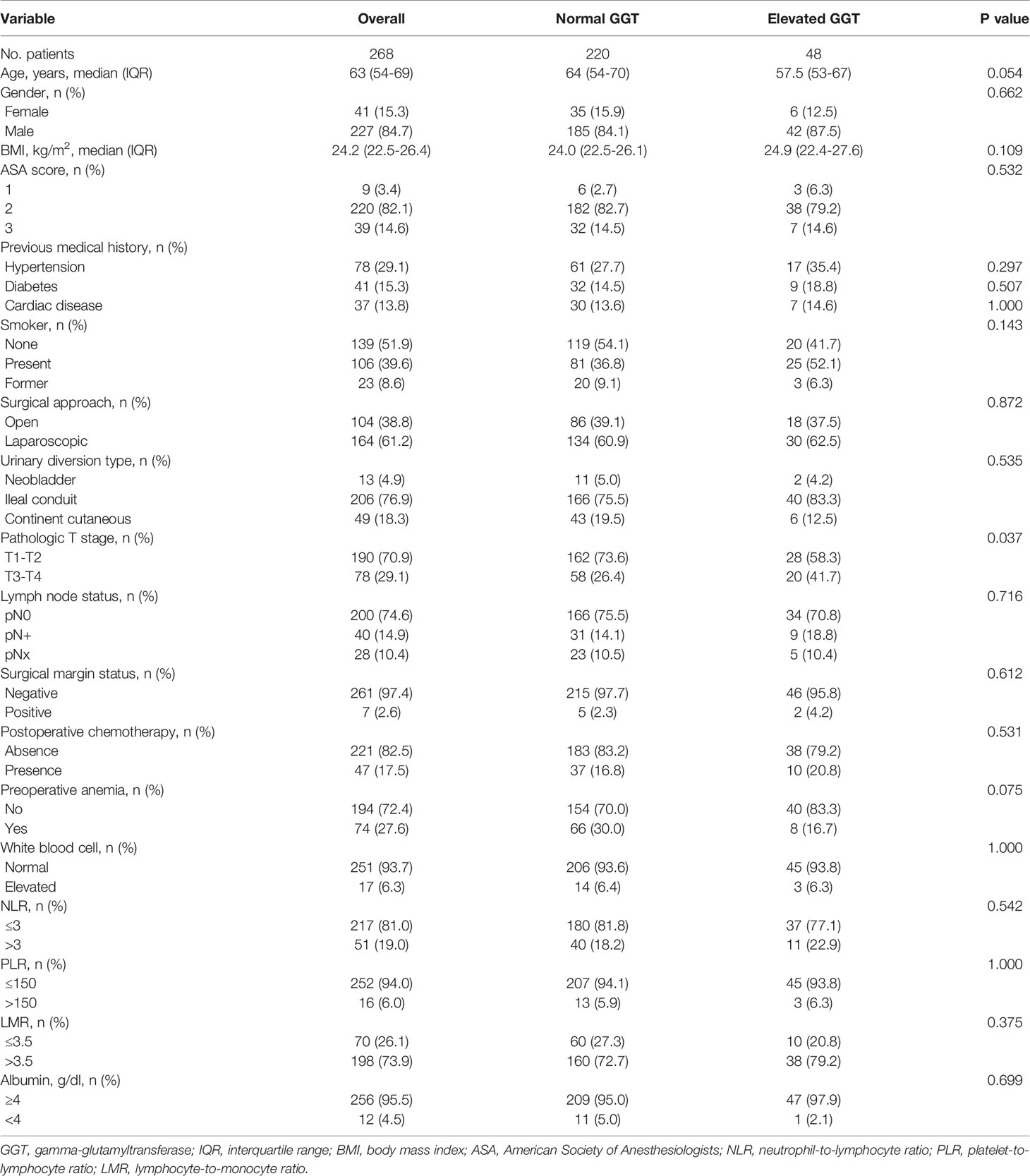
Table 1 Baseline characteristics of patients undergoing radical cystectomy for bladder cancer.
The median follow-up period for all subjects was 34.7 (22.9-45.9) months. At the last follow-up, 67 patients died, 51 patients died of cancer, 92 patients experienced disease recurrence. The three-year OS, CSS, DFS was respectively 74.5%, 78.8%, 66.8%. The five-year OS, CSS, DFS was respectively 61.6%, 67.9%, 51.3%.
Preoperative Serum GGT and Clinicopathological Parameters
The optimal cut-off point of preoperative GGT was 40 U/L. Forty-eight patients had an elevated level of serum GGT, a normal level of serum GGT was presented in 220 patients. Between the two groups, we only found that patients with an elevated serum GGT had a higher rate of pT3-T4 tumors (41.7% vs. 26.4%, P = 0.037). However, the other variables including demographics, hematological, surgical, pathological variables were similar between the two groups (P > 0.05 for all).
Preoperative Serum GGT With Survival
The Kaplan-Meier curves were presented in Figure 2. According to the results, patients with a higher preoperative serum GGT had a lower rate of OS, CSS and DFS (P < 0.001 for all).
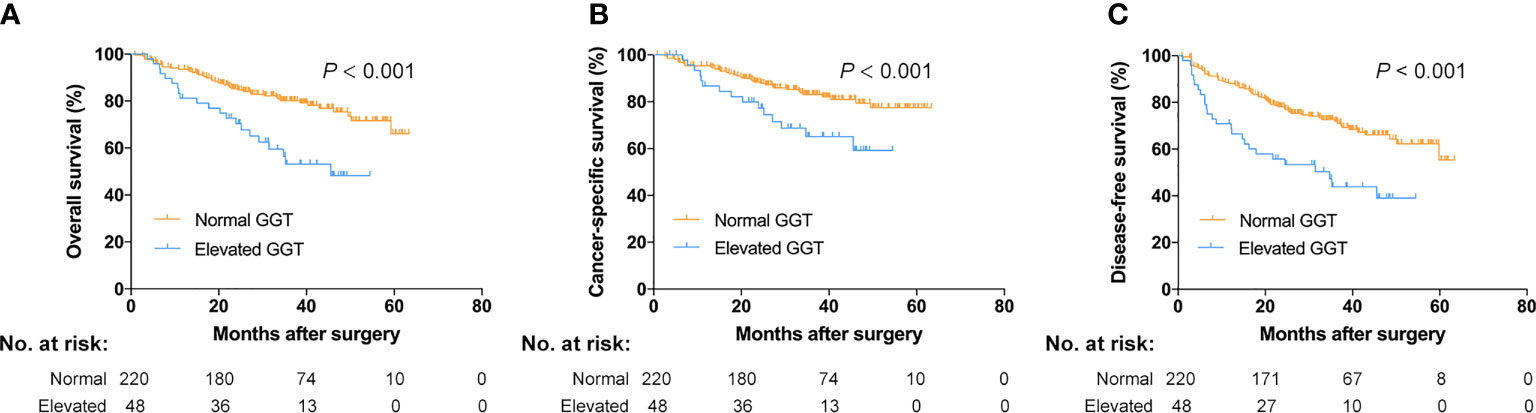
Figure 2 Survival curves for normal and elevated GGT groups. (A) Overall survival; (B) cancer-specific survival; (C) disease-free survival.
Older age (P = 0.001), diabetes history (P = 0.017), continent cutaneous urinary diversion (P = 0.044), higher pT stage (P < 0.001), positive lymph node (P < 0.001), postoperative chemotherapy (P = 0.014), higher level of NLR (P = 0.007), elevated level of preoperative serum GGT (P = 0.001) were correlated to lower rate of OS. Multivariate analysis identified that age (HR: 1.053, 95% CI: 1.022-1.085; P = 0.001), diabetes history (HR: 1.884, 95% CI: 1.024-3.466; P = 0.042), pathologic T stage (HR: 3.140, 95% CI: 1.772-5.564; P < 0.001), positive lymph node (HR: 1.946, 95% CI: 1.020-3.715; P = 0.043), preoperative serum GGT (HR: 3.027, 95% CI: 1.716-5.338; P < 0.001) were independent predictors of OS (Table 2).
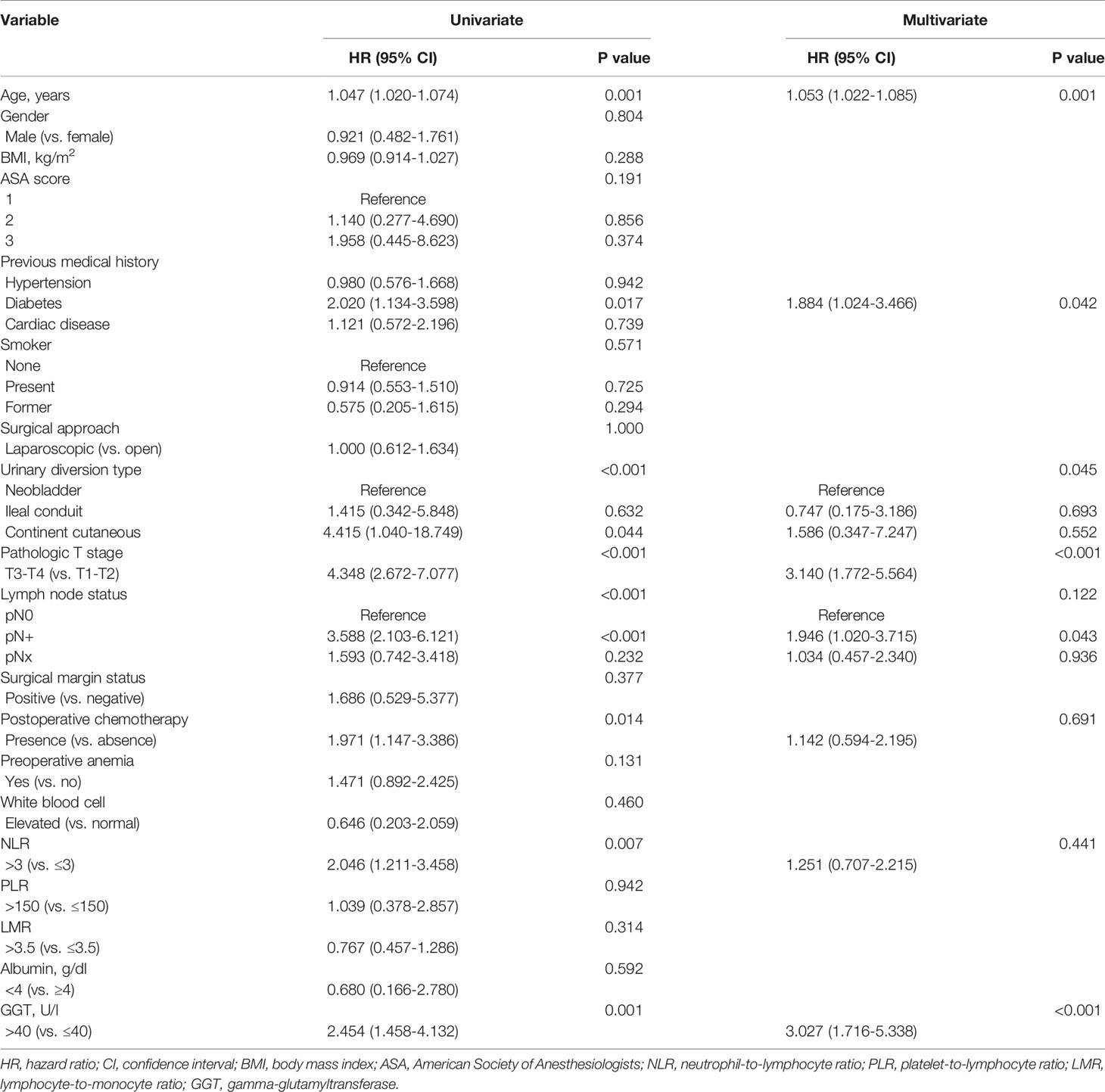
Table 2 Univariate and multivariate analysis for variables predicting overall survival.
The results showed that diabetes history (P = 0.025), higher pT stage (P < 0.001), positive lymph node (P < 0.001), postoperative chemotherapy (P = 0.002), higher level of NLR (P = 0.011), elevated level of preoperative serum GGT (P = 0.012) were correlated to lower rate of CSS. Multivariate analysis identified that diabetes history (HR: 2.250, 95% CI: 1.126-4.496; P = 0.022), pathologic T stage (HR: 3.030, 95% CI: 1.574-5.834; P = 0.001), positive lymph node (HR: 2.555, 95% CI: 1.243-5.254; P = 0.011), preoperative serum GGT (HR: 2.115, 95% CI: 1.093-4.090; P = 0.026) were independent predictors of CSS (Table 3).
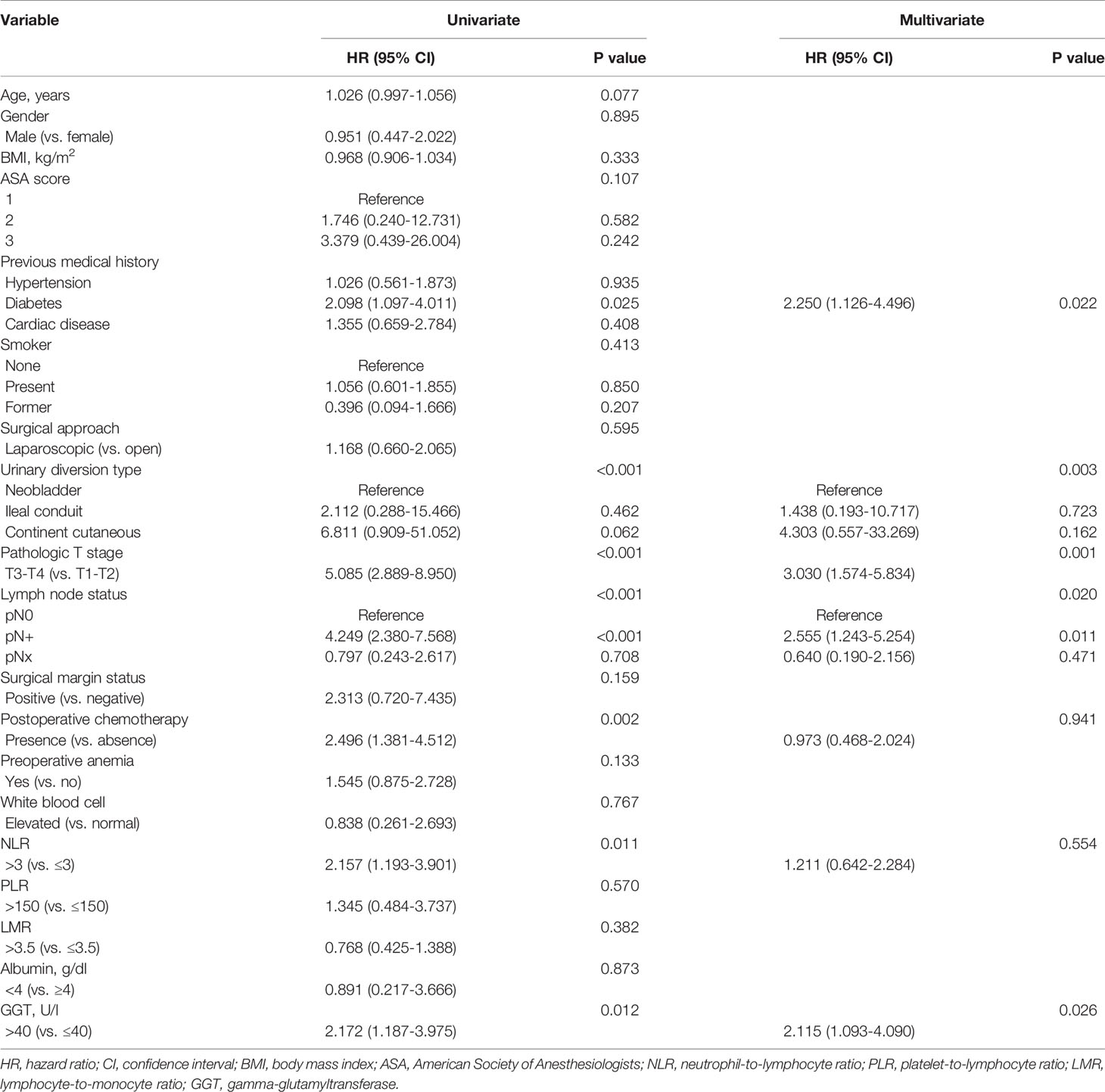
Table 3 Univariate and multivariate analysis for variables predicting cancer-specific survival.
The results showed that older age (P = 0.007), higher pT stage (P < 0.001), positive lymph node (P < 0.001), positive surgical margin (P = 0.043), postoperative chemotherapy (P < 0.001), elevated level of preoperative serum GGT (P < 0.001) were associated with lower rate of DFS. Multivariate analysis identified that age (HR: 1.041, 95% CI: 1.016-1.066; P = 0.001), pathologic T stage (HR: 2.591, 95% CI: 1.580-4.250; P < 0.001), positive lymph node (HR: 1.954, 95% CI: 1.104-3.460; P = 0.022), preoperative serum GGT (HR: 2.584, 95% CI: 1.569-4.255; P < 0.001) were independent predictors of DFS (Table 4).
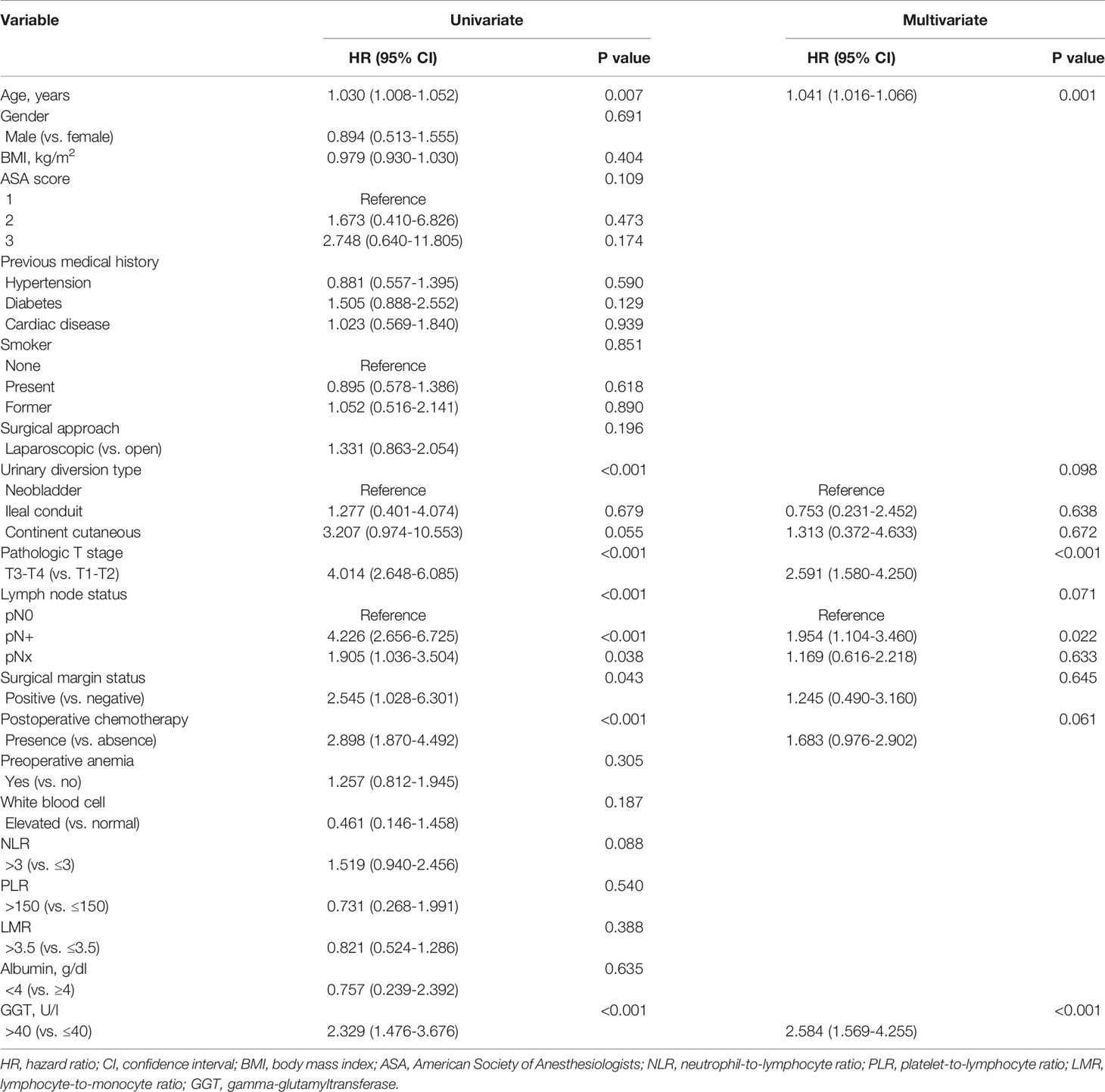
Table 4 Univariate and multivariate analysis for variables predicting progression-free survival.
Discussion
Despite the significant progress in systematic therapy, the long-term survival hasn’t changed significantly for BC patients, especially cases with muscle-invasive disease. At present, biomarkers with prognostic significance in bladder cancer include cell cycle regulating proteins, cell adhesion molecules, oncogenes, tumor related antigens, etc (17). Nevertheless, in order to better understand the mechanism of disease occurrence and progression, more dependable prognosis predictors are still needed. A lot of researches have explored the prognostic value of serum GGT in various cancer patients. However, to our knowledge, no study has looked at the role of GGT in bladder cancer prognosis. Hence, we conducted this study to assess the prognostic value of preoperative serum GGT in BC patients undergoing radical surgery.
In patients with urological cancers, Takemura et al. (14) have assessed the prognostic value of serum GGT on mCRPC patients treated with enzalutamide and its correlation with treatment response. They found that an increase in serum GGT was significantly and independently associated with a shorter overall survival. An elevation in GGT was also correlated to a poorer PSA response, the largest PSA change, and a shorter PSA progression-free survival. Luo et al. (15) have assessed the prognostic value of preoperative serum GGT in the subgroup renal cell patients with tumor thrombus. They found that preoperative elevation of GGT was correlated to poor CSS and recurrence-free survival, and the preoperative GGT level can be an important prognosis predictor for patient with localized renal cell carcinoma and tumor thrombus.
To our best knowledge, we initially examined the prognostic significance of preoperative serum GGT in BC patients. We found that patients with an increased serum GGT had a higher rate of pT3-T4 tumors (41.7% vs. 26.4%, P = 0.037). Since high pathological T stage tumors experienced unfavorable oncological outcomes (4), an increase in GGT level may associated with an inferior prognosis in BC patients. All subjects were classified into two groups based on the cut-off point of preoperative GGT at 40 U/L, the Kaplan-Meier curves were performed and verified that patients belonging to high serum GGT group had a lower rate of OS, CSS and DFS (P < 0.001 for all). Moreover, including other demographics, hematological, surgical and pathological variables, cox regression analyses have found that preoperative serum GGT was an independent predictor for OS (HR: 3.027, 95% CI: 1.716-5.338; P < 0.001), CSS (HR: 2.115, 95% CI: 1.093-4.090; P = 0.026), and DFS (HR: 2.584, 95% CI: 1.569-4.255; P < 0.001) in BC patients undergoing radical cystectomy. Circulating serum GGT is clinically easy to detect and can be applied as a viewer of cancer burden and a meaningful marker in clinical treatment of BC patients.
As a membrane-bound enzyme, GGT plays an important role in maintaining the production of intracellular GSH, an important antioxidant that protects cells from reactive oxygen compounds and free radicals. GGT also plays an important role in supplying amino acids to cells and promoting cell proliferation both physiologically and by limiting cysteine concentrations (7). There is growing evidence that GGT is deregulated in tumor cells and can represent cancer progression and aggressiveness (18). It was proposed that the increase of GGT may contribute to the formation of tumor microenvironment and protect cancer cells from oxidative stress or cytotoxic drugs (19). Nevertheless, GGT can also promote oxidative effects in certain situations. Persistent oxidative stress leads to genomic instability and following imbalance of cell proliferation and apoptosis, which is involved in carcinogenesis and progression (9). Hence, GGT can be used as an indicator of tumor aggressiveness by presenting the degree of oxidative stress. Additionally, it has been reported that GGT can be induced by a variety of inflammatory factors, including tumor necrosis factor and interferon (20, 21). Therefore, we hypothesized that GGT was associated with tumor-associated inflammatory responses and may serve as an inflammatory biomarker to predict the prognosis of cancer patients. Nevertheless, the exact mechanism of increased GGT level in the process of tumor formation was not clearly clarified.
In our study, we also found that age, diabetes history, pathologic T stage, and positive lymph status were independent predictors of prognosis for BC patients undergoing radical cystectomy. Although the difference was significant for the variable age, the predictive effect (HR: 1.053, 95% CI: 1.022-1.085) was minor. The recent publication has reported the similar result (HR: 1.03, 95% CI: 1.01-1.05) (22). In 2018, Peng et al. (23) have performed an updated meta-analysis to examine the relationship between metabolic syndrome and susceptibility and prognosis of bladder cancer. The pooled results indicated that diabetes history significantly increased the risk of bladder cancer and was associated with poor survival. More recently, a Chinese cohort has explored the prognostic value of CD155 in patients with localized muscle-invasive BC. In multivariate analysis, they also identified that T stage and positive lymph node independently predicted relapse-free survival and overall survival. They have further verified that T stage and lymph node status were independent predictors associated with inferior overall survival with data from TCGA database (24). The serum GGT reminded to be an independent predictor in our study after adjusting for these common prognostic factors.
The limitations can’t be ignored. First, this was a single-institutional retrospective study with limited patients, the potential selection bias can’t be controlled. Second, because of the retrospective design, some data may miss and be collected inaccurately, which may affect the results. Third, the median follow-up period for all patients was 34.7 months, which may be insufficient, especially for patients at low risk. Fourth, the cut-off value of serum GGT has not been determined. Through ROC curve analysis, the cut-off point of preoperative GGT was 40 U/L in our study. The best cut-off value of serum GGT reminds to be explored. Thus, prospective external validation from well-designed independent multi-institution cohorts with sufficient follow-up time will verify the universality of our results.
Conclusions
Despite the above limitations, the present study initially investigated the prognostic value of preoperative GGT in BC patients. Our results indicated that preoperative serum GGT was an independent prognosis predictor for survival of BC patients after radical surgery, and can be included in the prognostic models.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Ethics Statement
The studies involving human participants were reviewed and approved by The Ethics Committe of Shijiazhuang People’s Hospital. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
Conception and design: SS and CS. Data collection or management: SS, LL, YN, and HG. Data analysis: SS, YH, SG, and SP. Manuscript writing/editing: SS and CS. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by a grant from science and technology research and development guidance project of Shijiazhuang in 2020 (No. 201460663).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2020. CA: Cancer J Clin (2020) 70(1):7–30. doi: 10.3322/caac.21590
2. Kamat AM, Hahn NM, Efstathiou JA, Lerner SP, Malmström PU, Choi W, et al. Bladder Cancer. Lancet (2016) 388(10061):2796–810. doi: 10.1016/S0140-6736(16)30512-8
3. Su S, Gu L, Ma X, Li H, Wang B, Shi T, et al. Comparison of Laparoscopic and Robot-assisted Radical Cystectomy for Bladder Cancer: Perioperative and Oncologic Outcomes. Clin Genitourin Cancer (2019) 17(5):e1048-e53. doi: 10.1016/j.clgc.2019.06.007
4. Su S, Liu L, Sun C, Yang L, Nie Y, Chen Y, et al. Prognostic Significance of Serum Lactate Dehydrogenase in Patients Undergoing Radical Cystectomy for Bladder Cancer. Urol Oncol (2020) 38(11):852.e1–9. doi: 10.1016/j.urolonc.2020.05.031
5. Mori K, Miura N, Mostafaei H, Quhal F, Motlagh RS, Lysenko I, et al. Prognostic Value of Preoperative Hematologic Biomarkers in Urothelial Carcinoma of the Bladder Treated With Radical Cystectomy: A Systematic Review and Meta-Analysis. Int J Clin Oncol (2020) 25(8):1459–74. doi: 10.1007/s10147-020-01690-1
6. Whitfield JB. Gamma Glutamyl Transferase. Crit Rev Clin Lab Sci (2001) 38(4):263–355. doi: 10.1080/20014091084227
7. Hanigan MH, Gallagher BC, Townsend DM, Gabarra V. Gamma-Glutamyl Transpeptidase Accelerates Tumor Growth and Increases the Resistance of Tumors to Cisplatin In Vivo. Carcinogenesis (1999) 20(4):553–9. doi: 10.1093/carcin/20.4.553
8. Van Hemelrijck M, Jassem W, Walldius G, Fentiman IS, Hammar N, Lambe M, et al. Gamma-Glutamyltransferase and Risk of Cancer in a Cohort of 545,460 Persons - the Swedish AMORIS Study. Eur J Cancer (2011) 47(13):2033–41. doi: 10.1016/j.ejca.2011.03.010
9. Corti A, Franzini M, Paolicchi A, Pompella A. Gamma-Glutamyltransferase of Cancer Cells At the Crossroads of Tumor Progression, Drug Resistance and Drug Targeting. Anticancer Res (2010) 30(4):1169–81.
10. Pompella A, Corti A, Paolicchi A, Giommarelli C, Zunino F. Gamma-Glutamyltransferase, Redox Regulation and Cancer Drug Resistance. Curr Opin Pharmacol (2007) 7(4):360–6. doi: 10.1016/j.coph.2007.04.004
11. Staudigl C, Concin N, Grimm C, Pfeiler G, Nehoda R, Singer CF, et al. Prognostic Relevance of Pretherapeutic Gamma-Glutamyltransferase in Patients With Primary Metastatic Breast Cancer. PloS One (2015) 10(4):e0125317. doi: 10.1371/journal.pone.0125317
12. Xu XS, Wan Y, Song SD, Chen W, Miao RC, Zhou YY, et al. Model Based on γ-Glutamyltransferase and Alkaline Phosphatase for Hepatocellular Carcinoma Prognosis. World J Gastroenterol (2014) 20(31):10944–52. doi: 10.3748/wjg.v20.i31.10944
13. Grimm C, Hofstetter G, Aust S, Mutz-Dehbalaie I, Bruch M, Heinze G, et al. Association of Gamma-Glutamyltransferase With Severity of Disease At Diagnosis and Prognosis of Ovarian Cancer. Br J Cancer (2013) 109(3):610–4. doi: 10.1038/bjc.2013.323
14. Takemura K, Ito M, Nakanishi Y, Kataoka M, Sakamoto K, Suzuki H, et al. Serum γ-Glutamyltransferase as a Prognostic Biomarker in Metastatic Castration-Resistant Prostate Cancer Treated With Enzalutamide. Anticancer Res (2019) 39(10):5773–80. doi: 10.21873/anticanres.13780
15. Luo C, Xu B, Fan Y, Yu W, Zhang Q, Jin J. Preoperative Gamma-Glutamyltransferase is Associated With Cancer-Specific Survival and Recurrence-Free Survival of Nonmetastatic Renal Cell Carcinoma With Venous Tumor Thrombus. BioMed Res Int (2017) 2017:3142926. doi: 10.1155/2017/3142926
16. Yang F, Zhang S, Yang H, Luo K, Wen J, Hu Y, et al. Prognostic Significance of Gamma-Glutamyltransferase in Patients With Resectable Esophageal Squamous Cell Carcinoma. Dis Esophagus (2015) 28(5):496–504. doi: 10.1111/dote.12227
17. Ku JH, Kim WJ, Lerner SP, Chun F, Kluth LA. Diagnostic and Prognostic Markers in Bladder Cancer. Dis Markers (2016) 2016:2425091. doi: 10.1155/2016/2425091
18. Strasak AM, Goebel G, Concin H, Pfeiffer RM, Brant LJ, Nagel G, et al. Prospective Study of the Association of Serum Gamma-Glutamyltransferase With Cervical Intraepithelial Neoplasia III and Invasive Cervical Cancer. Cancer Res (2010) 70(9):3586–93. doi: 10.1158/0008-5472.CAN-09-3197
19. Franzini M, Corti A, Lorenzini E, Paolicchi A, Pompella A, De Cesare M, et al. Modulation of Cell Growth and Cisplatin Sensitivity by Membrane Gamma-Glutamyltransferase in Melanoma Cells. Eur J Cancer (2006) 42(15):2623–30. doi: 10.1016/j.ejca.2006.04.016
20. Bouman L, Sancéau J, Rouillard D, Bauvois B. gamma-Glutamyl Transpeptidase Expression in Ewing’s Sarcoma Cells: Up-Regulation by Interferons. Biochem J (2002) 364(Pt 3):719–24. doi: 10.1042/bj20011854
21. Daubeuf S, Accaoui MJ, Pettersen I, Huseby NE, Visvikis A, Galteau MM. Differential Regulation of Gamma-Glutamyltransferase mRNAs in Four Human Tumour Cell Lines. Biochim Biophys Acta (2001) 1568(1):67–73. doi: 10.1016/S0304-4165(01)00201-X
22. Lai C, Wu Z, Shi J, Li K, Zhu J, Chen Z, et al. Autophagy-Related Long Noncoding RNAs can Predict Prognosis in Patients With Bladder Cancer. Aging (Albany NY) (2020) 12(21):21582–96. doi: 10.18632/aging.103947
23. Peng XF, Meng XY, Wei C, Xing ZH, Huang JB, Fang ZF, et al. The Association Between Metabolic Syndrome and Bladder Cancer Susceptibility and Prognosis: An Updated Comprehensive Evidence Synthesis of 95 Observational Studies Involving 97,795,299 Subjects. Cancer Manag Res (2018) 10:6263–74. doi: 10.2147/CMAR.S181178
Keywords: bladder cancer, radical cystectomy, gamma-glutamyltransferase, prognosis, biomarkers
Citation: Su S, Liu L, Sun C, Nie Y, Guo H, Hu Y, Guo S and Pang S (2021) Preoperative Serum Gamma-Glutamyltransferase as a Prognostic Biomarker in Patients Undergoing Radical Cystectomy for Bladder Cancer. Front. Oncol. 11:648904. doi: 10.3389/fonc.2021.648904
Received: 02 January 2021; Accepted: 08 April 2021;
Published: 07 May 2021.
Edited by:
Matteo Ferro, European Institute of Oncology (IEO), ItalyReviewed by:
Daniela Terracciano, University of Naples Federico II, ItalyFelice Crocetto, Federico II University Hospital, Italy
Copyright © 2021 Su, Liu, Sun, Nie, Guo, Hu, Guo and Pang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chao Sun, c3VuY2hhb3BwdEAxNjMuY29t