 Anett Balikó1,2
Anett Balikó1,2 Zsolt Szakács3Béla Kajtár4
Zsolt Szakács3Béla Kajtár4 Zsombor Ritter5
Zsombor Ritter5 Attila Gyenesei6
Attila Gyenesei6 Nelli Farkas7László Kereskai4
Nelli Farkas7László Kereskai4 István Vályi-Nagy8
István Vályi-Nagy8 Hussain Alizadeh3*László Pajor4
Hussain Alizadeh3*László Pajor4- 1Tolna County Balassa János Hospital, Szekszárd, ;Hungary
- 2PhD Doctoral School – Interdisciplinary Medical Sciences (D93), Medical School, University of Pécs, Pécs, ;Hungary
- 3First Department of Medicine, Medical School, University of Pécs, Pécs, ;Hungary
- 4Department of Pathology, Medical School, University of Pécs, Pécs, ;Hungary
- 5Department of Medical Imaging, Medical School, University of Pécs, Pécs, ;Hungary
- 6Szentágothai Research Centre, University of Pécs, Pécs, ;Hungary
- 7Institute of Bioanalysis, Medical School, University of Pécs, Pécs, ;Hungary
- 8South-Pest Hospital Centre – National Institute for Infectology and Haematology, Budapest, ;Hungary
Background: The clinical and genetic heterogeneity of diffuse large B-cell lymphoma (DLBCL) presents distinct challenges in predicting response to therapy and overall prognosis. The main objective of this study was to assess the application of the immunohistochemistry- and interphase fluorescence in situ hybridization (FISH)-based molecular markers in the diagnosis of DLBCL and its prognostic value in patients treated with rituximab-based immunochemotherapy.
Methods: This is a multicenter, retrospective study, which analyzed data from 7 Hungarian hematology centers. Eligible patients were adults, had a histologically confirmed diagnosis of DLBCL, were treated with rituximab-based immunochemotherapy in the first line, and had available clinicopathological data including International Prognostic Index (IPI). On the specimens, immunohistochemistry and FISH methods were performed. Germinal center B-cell like (GCB) and non-GCB subtypes were classified by the Hans algorithm. Outcomes included overall survival (OS), event-free survival (EFS), and EFS at 2 years (EFS24). For survival analysis, we used Kaplan-Meier curves with the log-rank test and multivariate Cox regression.
Results: A total of 247 DLBCL cases were included. Cases were positive for MYC, BCL2, BCL6, and MUM1 expression in 52.1%, 66.2%, 72.6%, and 77.8%, respectively. BCL6 translocation, BCL2 gene copy number (GCN) gain, IGH::MYC translocation, MYC GCN gain, IGH::BCL2 translocation, and BCL6 GCN gain were detected in 21.4%, 14.1%, 7.3%, 1.8%, 7.3%, and 0.9%, respectively. At a median follow-up of 52 months, 140 patients (56.7%) had disease progression or relapse. The Kaplan-Meier estimate for EFS24 was 56.2% (CI: 50.4–62.8%). In univariate analysis, only IPI and BCL6 expression were significant predictors of both OS and EFS, whereas MUM1 predicted EFS only. In multivariate analysis, the IPI score was a significant independent negative, whereas MIB-1 and BCL6 protein expressions were significant independent positive predictors of both OS and EFS.
Conclusion: In our study, we found that only IPI, BCL6 protein expression and MIB-1 protein expression are independent predictors of survival outcomes in DLBCL. We did not find any difference in survival by GCB vs. non-GCB subtypes. These findings may improve prognostication in DLBCL and can contribute to designing further research in the area.
1 Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common high-grade non-Hodgkin lymphoma accounting for 30–40% of B-cell non-Hodgkin lymphomas (1). DLBCL has considerable biologic, molecular, and clinical heterogeneity resulting in different responses to therapy (2). DLBCL is a potentially curable disease with an overall 60–70% chance of achieving durable complete remission (CR) with the currently used standard first-line immunochemotherapy. However, 30–40% of patients are either refractory to first-line treatment or experience relapse and eventually will die of disease progression (3). Patients achieving remission lasting for 24 months or more from the end of first-line treatment have favorable prognosis at long term (4–6). The diagnosis and subtyping of DLBCL have come far to date, from morphological assessment of tissue slide to now, where numerous ancillary tests are a prerequisite, including immunophenotyping performed by immunohistochemistry (IHC), cytogenetics, and detailed molecular testing to classify the disease based on cell of origin (COO). With the advent of novel therapeutic options, it is expected that molecular subtyping of DLBCL at diagnosis will allow prognostic stratification of patients into distinct subgroups which could provide preclinical rationale for therapeutic targeting the involved pathways and paving the application of personalized treatment. The original DLBCL molecular classification using DNA microarray-based technology was initially described by Alizadeh et al. (7). This technology allowed the analysis of transcriptional gene expression pattern, and distinguished two major COO subtypes of DLBCL: germinal center B-cell like (GCB) and activated B-cell like (ABC). This resulted in the molecular subtyping of 80–85% of all DLBCL cases. Treated with standard immunochemotherapy, the ABC subgroup had poorer 5-year survival compared to the GCB group (16% vs. 76%, respectively).
Hans (8), Choi (9), and Tally (10) are the most established algorithms that are based on IHC to assess COO with the Hans algorithm being the most commonly used in clinical practice. However, the clinical significance of COO subtyping using IHC remains controversial, and the assessment of COO by gene expression profiling rather than IHC is better associated with the prognosis of DLBCL (11).
Translocations, gene rearrangements, and protein expression patterns including but not limited to BCL6, BCL2, and MYC have been shown to have prognostic implications.
The human proto-oncogene BCL6 was identified from chromosomal breaks at 3q27, is expressed predominantly in germinal center B-cells (12, 13), and functions as a sequence-specific transcriptional repressor (14, 15). Mutation or translocation of BCL6 gene has been implicated in the pathogenesis of certain subtypes of DLBCL (12). BCL6 is frequently affected by chromosomal translocations, occurring more frequently in ABC DLBCL. There is no consensus on the effect of BCL6 translocation on prognosis of DLBCL, especially in the rituximab era, with studies showing either favorable (16, 17), neutral (18, 19), or unfavorable outcomes (20).
The BCL2 protein is a central regulator of the mitochondrial apoptotic pathway and its gene is located on the chromosome arm 18q21 (21). The primary function of BCL2 is to promote cell survival by inhibiting apoptosis (22–24). The BCL2 gene is overexpressed in many cancers including DLBCL and is usually associated with drug resistance (25). In DLBCL, the ratio of BCL2-positive cases is highly variable, ranging from 20% to 80% across studies that used IHC (26, 27). Some studies showed BCL2 protein expression as a marker of poor prognosis in GCB subtype of DLBCL (26, 28), while others reported it to be a marker of poor prognosis in ABC-DLBCL, only (29).
Chromosomal translocations dysregulating MYC (8q24) were reported in 5–15% of GCB DLBCL cases (17), while MYC protein detection in 5–40% of DLBCL cases (30–32). MYC gene translocation was associated with a very poor outcome in DLBCL (33–36). MYC translocation in DLBCL is usually associated with other gene abnormalities, e.g., BCL2 or BCL6 rearrangements (37, 38). Some studies show that about 30% of DLBCL co-express high levels of MYC and BCL2 proteins, which cases are called ‘double expressor’ DLBCL (DEL) (39).
Although substantial knowledge has accumulated about prognostication in DLBCL, a lot of questions have remained unanswered. The main objective of this study was to describe the distribution of and to test the prognostic ability of IHC- and interphase fluorescence in situ hybridization (FISH)-based molecular markers in a Hungarian cohort of newly diagnosed DLBCL patients from the rituximab era.
2 Patients and methods
This multicenter, retrospective study was approved by the Committee of Science and Research Ethics (ETT-TUKEB) under reference number 50268-8/2017.
2.1 Study population and sample assessment
This study is reported according to the STROBE Statement (40).
A total of 342 adult patients diagnosed with DLBCL were assessed. Tissue samples were sent by 7 Hungarian Hematology centers to the central hematopathology lab in the Department of Pathology, Medical School, Clinical Centre, University of Pécs between Jan 2010 and Mar 2017. All samples were reviewed by 2 senior pathologists. The final pathology report was established according to the diagnostic criteria of the 2016 WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (37). Out of the 342, 95 cases were excluded due to incomplete clinicopathological data, so a total of 247 cases were further assessed in the study. All specimens were fixed in 10% neutral formalin and conventional paraffin embedding was performed.
IHC was carried out according to standard protocols using CD10, clone 56C6; CD20, clone L26 (Visionbiosystems Novocastra, UK); MUM1/IRF4, clone MUM1p; BCL2, clone 124; BCL6, clone PG-B6p (Dako, Denmark); MYC, clone Y69 (Abcam, UK); Ki-67, clone B56 (Hisztopatológia Kft., Hungary) specific primary antibodies as well as Envision+ System-HRP (DakoCytomation, Denmark) and Bond Polymer Refine Detection (Leica Biosystems, UK) developing reagents. According to the Hans algorithm, at least 30% reactivity–either membranous or nuclear–is required for a tumor to be considered positive for a particular marker. The tumors were classified as GCB-like when exhibiting CD10+ (BCL6+/-, MUM1+/-) or CD10-, BCL6+, MUM1- phenotype. Non-GCB/ABC like was the subtype in the case of all the other–CD10-, BCL6+, MUM1+ or CD10-, BCL6-, MUM1+–phenotypic variables (8). DEL was defined as combined BCL2 (≥50%) and MYC (≥40%) positivity (37).
FISH was performed using 5 μm paraffin tissue sections for IGH::MYC, IGH::BCL2, BCL6 rearrangement and for MYC, BCL2, BCL6 gene copy number (GCN) gain. For these, Vysis IGH/MYC/CEP8 TC-DF, Vysis LSI IGH/BCL2 DC-DF, and Vysis LSI BCL6 (ABR) DC Break Apart probes (Abbott Molecular Inc., USA) were used. FISH reactions were analyzed in Zeiss Axioplan-MOT II fluorescent microscope and evaluated by means of ‘grid sampling’ and ‘color rationing’ methods (41). We have used double fusion FISH probes to detect IGH::BCL2 and IGH::MYC fusions, since non-IG BCL2 fusions are rare in DLBCL, and the prognostic significance of non-IG MYC fusions is controversial. Cases with non-IG BCL2 or MYC fusions showed signal patterns indicating BCL2 or MYC gain in our series. A tumor was defined positive for rearrangement using IGH/MYC, IGH/BCL2, and BCL6 probes if the fusion or the dissociated FISH signs occurred in at least 50% of the nuclei. The definition of MYC, BCL2, and BCL6 GCN gains included the lack of the polyploidy of the relevant chromosome and/or detection of at least one extra gene copy at least in 50% of the nuclei or identifying ‘double minutes’ and/or ‘beaded lace-like’ signals and/or uncountable (homogeneous staining region or cloudy-like) signals.
2.2 Clinical assessment
Detailed clinical and laboratory data including treatment regimen and clinical outcomes (overall survival, OS; event-free survival, EFS; EFS at 24 months, EFS24) were collected from patients’ records, then, all data were reviewed by a senior hematologist. The clinical stage was evaluated by the modified Ann Arbor and Lugano classifications (42, 43). CR, partial response, progression, refractory disease, and relapse were defined according to the International Working Group response criteria for lymphoma (44). EFS was defined as the time from the end of first line treatment until the earliest occurrence of disease progression or death of any cause. EFS24 was defined as being alive and free of any disease related event 24 months from the end of therapy.
2.3 Statistical analysis
In univariate statistics, Chi2 test was used to analyze the association across clinical variables. Kaplan-Meier curves with a median estimate (with 95% confidence interval, CI) and the log-rank test were used for univariate survival analysis. Multivariate Cox regression analysis was applied to identify independent prognostic factors for the outcomes (OS and EFS). The models were adjusted for gender, international prognostic index (IPI) subgroups, IHC (CD10, BCL6, MUM1, high MIB-1 >90%, MYC, and BCL2) and for FISH findings (BCL6 translocation and BCL2 GCN gain). In general, P <0.05 value was considered statistically significant. Statistical analysis was performed using R statistical software version 4.2.0 (45) and the survminer package v0.4.9 statistical software (46).
3 Results
Table 1 summarizes the clinical characteristics of the 247 patients included. The median age at the time of diagnosis was 65 years (range: 19–91 years), 65.2% of patients were >60 years, 46.6% were male, 42.9% had an elevated serum lactate dehydrogenase and 74.1% had an advanced (stage III/IV) disease. The majority (94.7%) were treated with R-CHOP or similar regimens, the most common salvage therapies were the R-ICE and R-DHAP protocols.
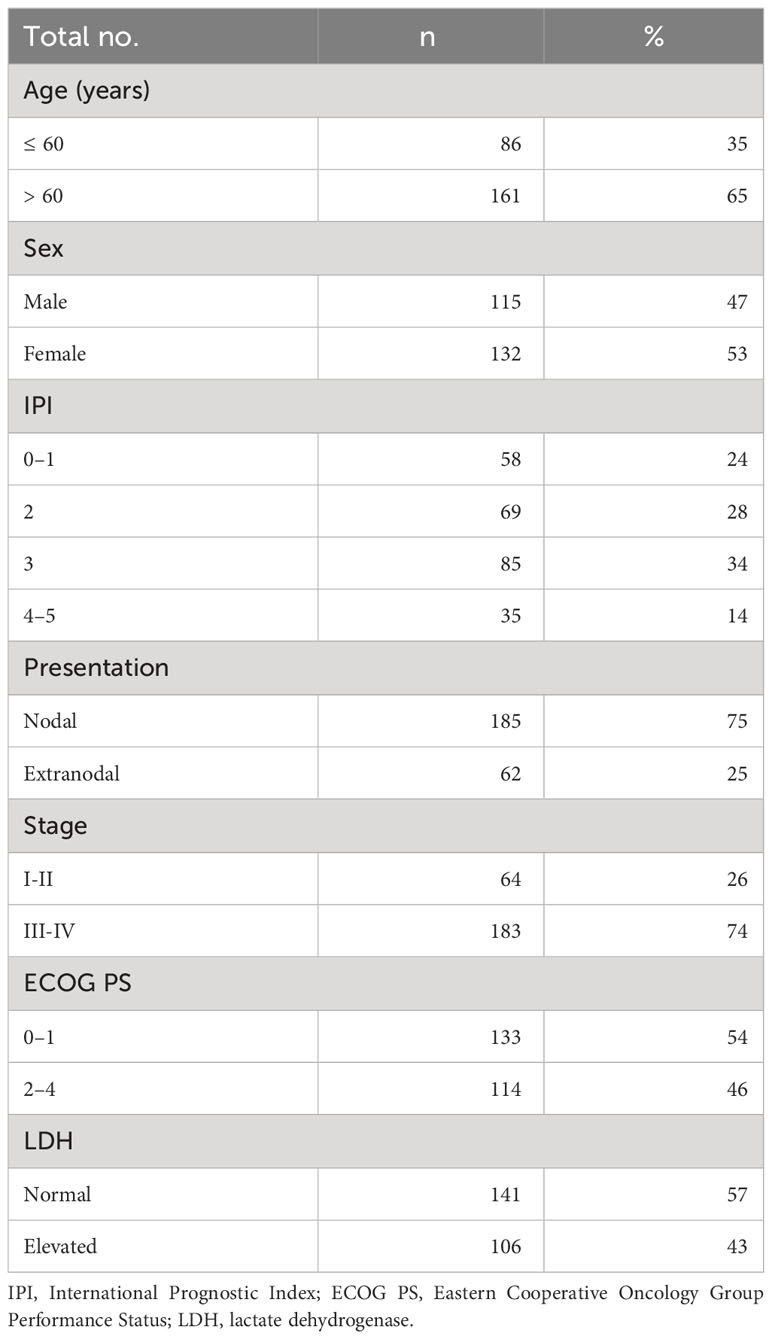
Table 1 Characteristics of patients included.
3.1 IHC and FISH distribution, and their associations
Table 2 summarizes the IHC findings, Table 3 shows FISH distribution by COO subtypes. A total of 234 and 220 patients had available IHC and FISH data, respectively.
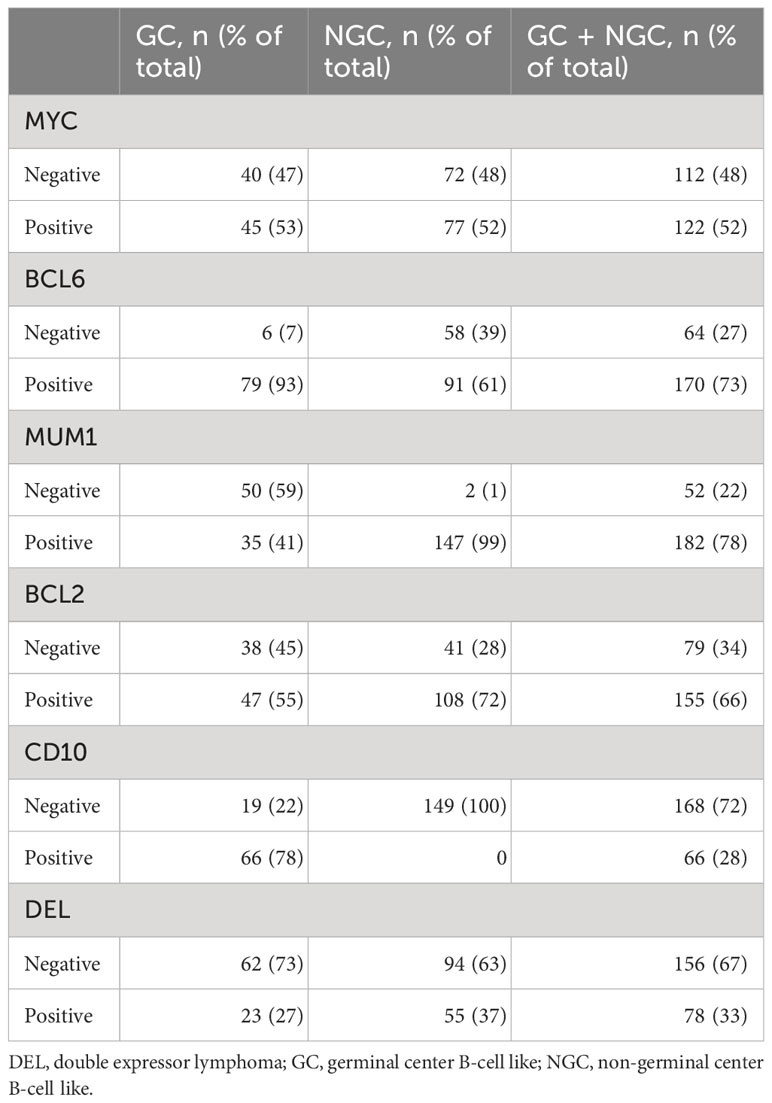
Table 2 Immunohistochemical staining results by cell of origin subtypes.
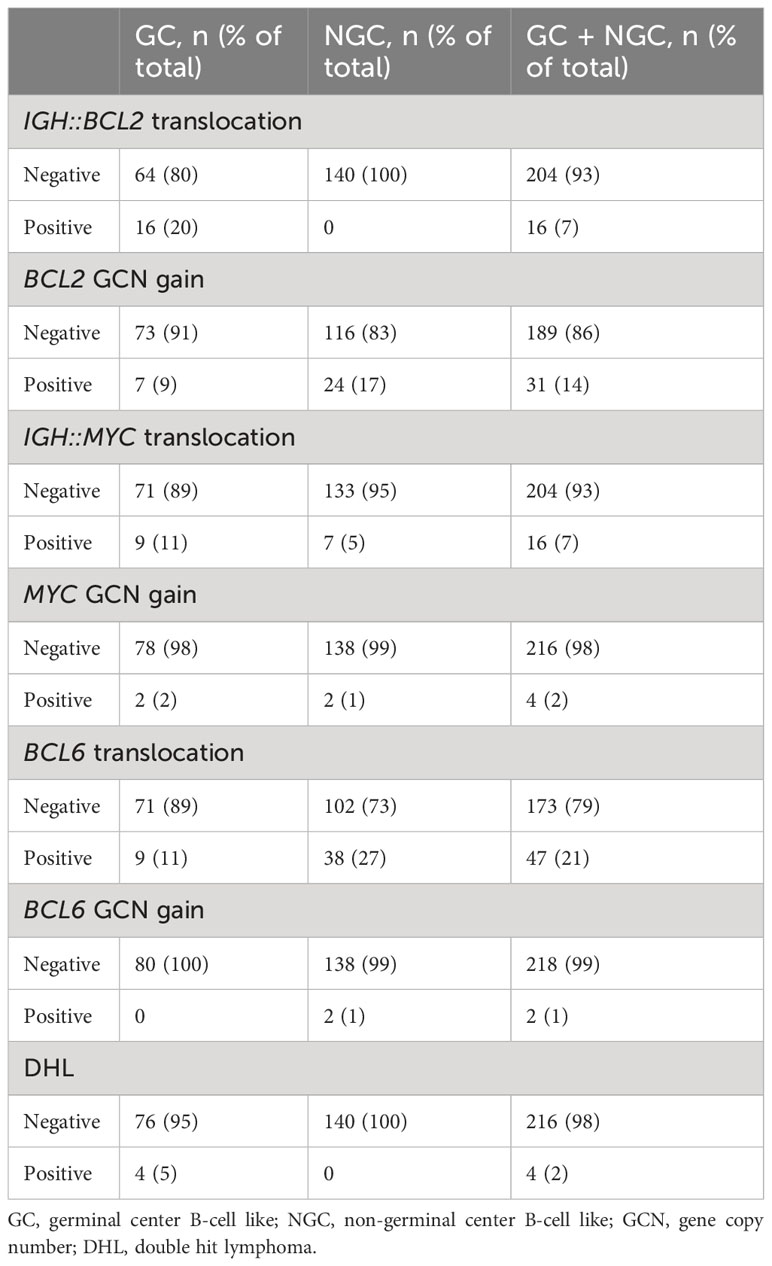
Table 3 Interphase fluorescent in situ hybridization results by cell of origin subtypes.
A positive IHC staining for MYC, BCL2, BCL6, and MUM1 protein was seen in 52.1%, 66.2%, 72.6%, and 77.8%, respectively. DEL (MYC and BCL2 co-expression) accounted for 33.3% and did not occur more frequently in the non-GCB group (p=0.112). High proliferation index (MIB-1 antibody >90%) was detected in 26.2%. BCL6 protein expression was significantly more common among those having high proliferation activity compared to those having low proliferation activity (82.5% vs. 69.6%, respectively, with p=0.047). Based on the Hans algorithm, non-GCB and GCB types accounted for 63.7% (149/234 cases) and 36.3% (85/234 cases), respectively.
With FISH, MYC translocation was detected in 16 cases (7.3%), and all of them were positive for MYC protein expression. No case of MYC translocation was found with negative MYC protein expression. MYC translocation was statistically significantly associated with MYC protein expression (p<0.001) and male gender (p=0.049) but not with COO (p=0.086). There were only 4 cases (1.8%) of MYC GCN gain.
BCL2 translocation was detected in 7.3%, all were in the GCB group (p<0.001). However, there was no significant difference in the prevalence of BCL2 protein expression by the presence of BCL2 translocation (p=0.194). BCL2 translocation seemed independent of gender (p=0.213). BCL2 GCN gain was detected in 14.1% of cases, its presence was not significantly associated with BCL2 protein expression (p=0.068), COO groups (p=0.085), and gender (p=0.303).
BCL6 gene rearrangement was confirmed in 21.4%, and it was significantly associated with COO (9 with GCB and 38 with non-GCB subtype; that is, 4.1% vs. 17.3%, respectively, with a p-value of 0.006). There was no significant association of BCL6 gene rearrangement with BCL6 protein expression (p=0.315) or gender (p=0.693). There were only 2 cases with BCL6 GCN gain.
There were 4 cases (1.8%) of dual MYC and BCL2 translocations (2 cases of DEL, another two had only BCL2 protein overexpression), and all were in the GCB group.
BCL2 gene alterations were more common with DEL compared to non-DEL (p=0.003), whereas the ratio of MYC gene alterations was similar between the groups (p=0.999).
3.2 Survival
At a median follow-up of 52 months (range: 0–131 months), 140 patients (56.7%) had disease progression or relapse. The overall response rate was 78.4% and the CR rate was 47.0%. The Kaplan-Meier estimate for EFS24 was 56.2% (CI: 50.4–62.8%). The 108 patients being not event-free at 24 months had a median OS of 7.1 months (CI: 6.5–8.0 months) after progression.
Table 4 summarizes the Kaplan-Meier survival estimates for all comparisons (234 and 220 patients had available IHC and FISH data, respectively). IPI and BCL6 expression were significant predictors of OS and EFS in univariate analysis (Figures 1, 2, respectively), whereas MUM1 predicted only EFS. BCL6 rearrangement, BCL2 GCN gain, IGH::MYC translocation, and IGH::BCL2 translocation did not have any prognostic impact on survival. Subgroup analysis by COO did not change the findings, nor did we find any difference in OS and EFS by COO subtype (Figure 3). Our results showed no difference in the 5-year survival in low-stage (I-II) and high-stage disease according to the COO. BCL6 rearrangement did not predict OS and EFS in the non-GCB subgroup. DEL phenotype did not predict OS or EFS. We did not find any impact of double protein expression using MYC and BCL2 on the OS in low and high-stage diseases. The rate of double-hit lymphoma in this cohort of patients was 1.8% and the median OS for these group of patients was 33.8 months.
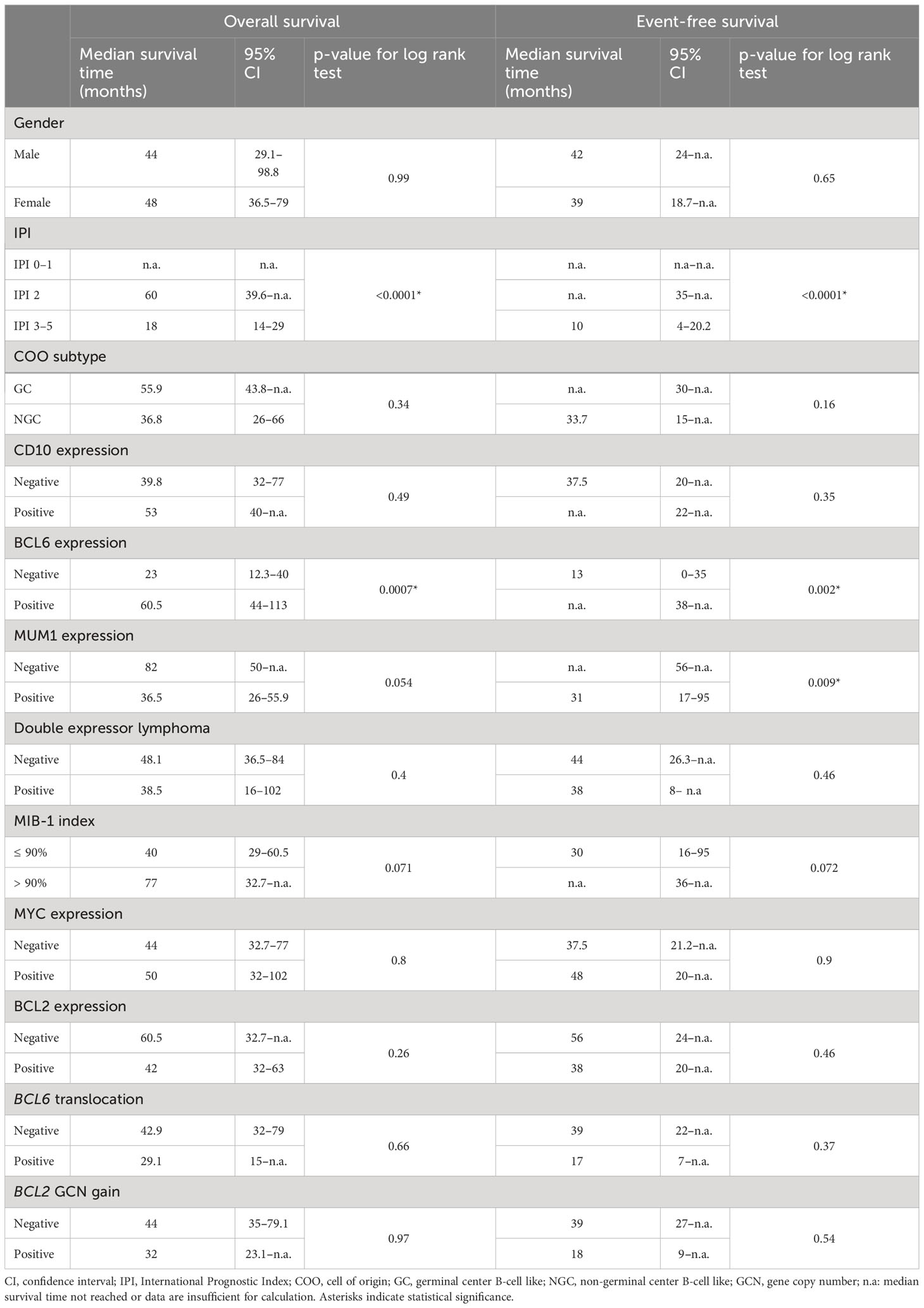
Table 4 Kaplan Meier estimates and log-rank tests for overall survival and event-free survival.
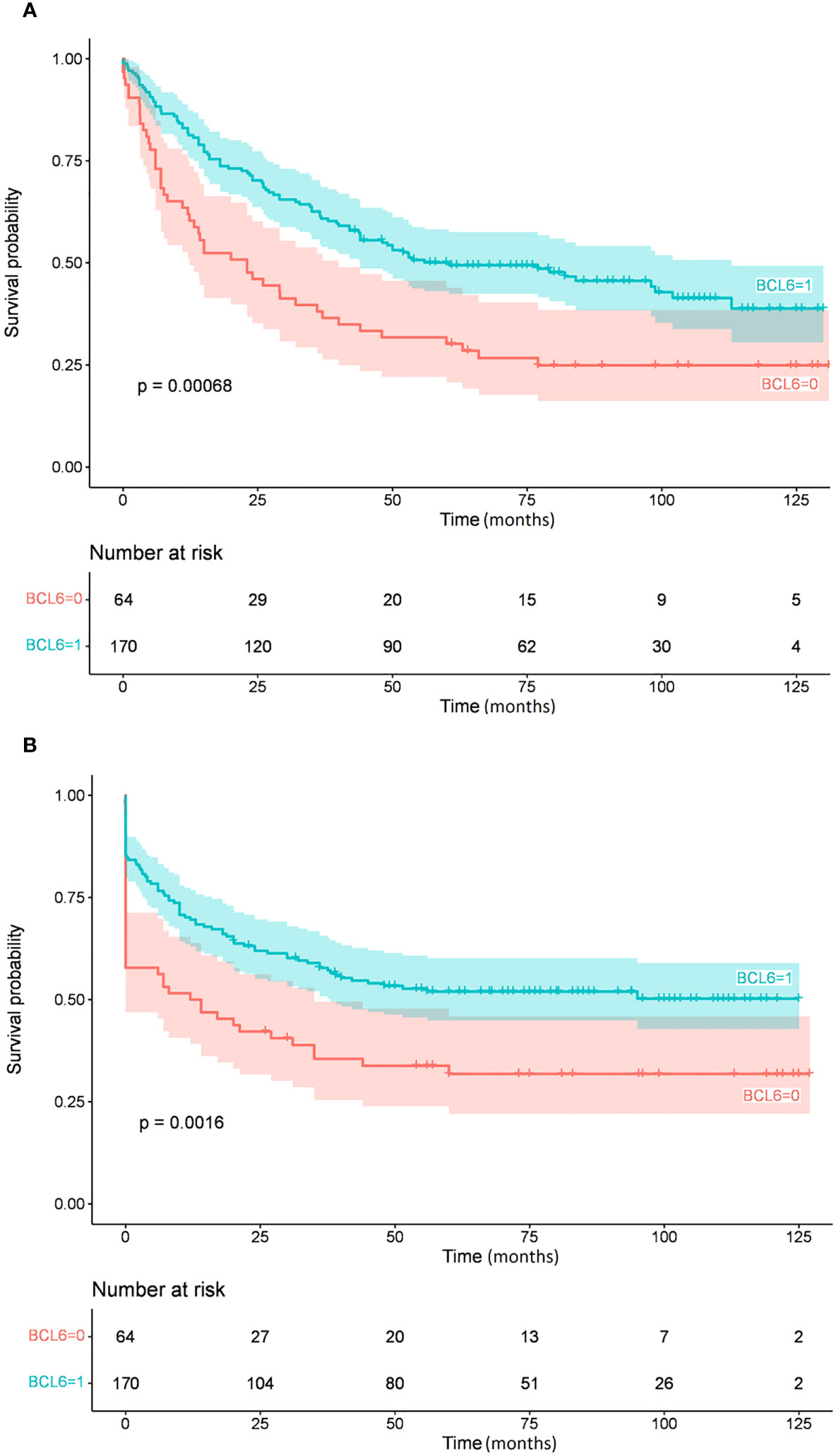
Figure 1 Overall survival (A) and event-free survival (B) by BCL6 protein expression.
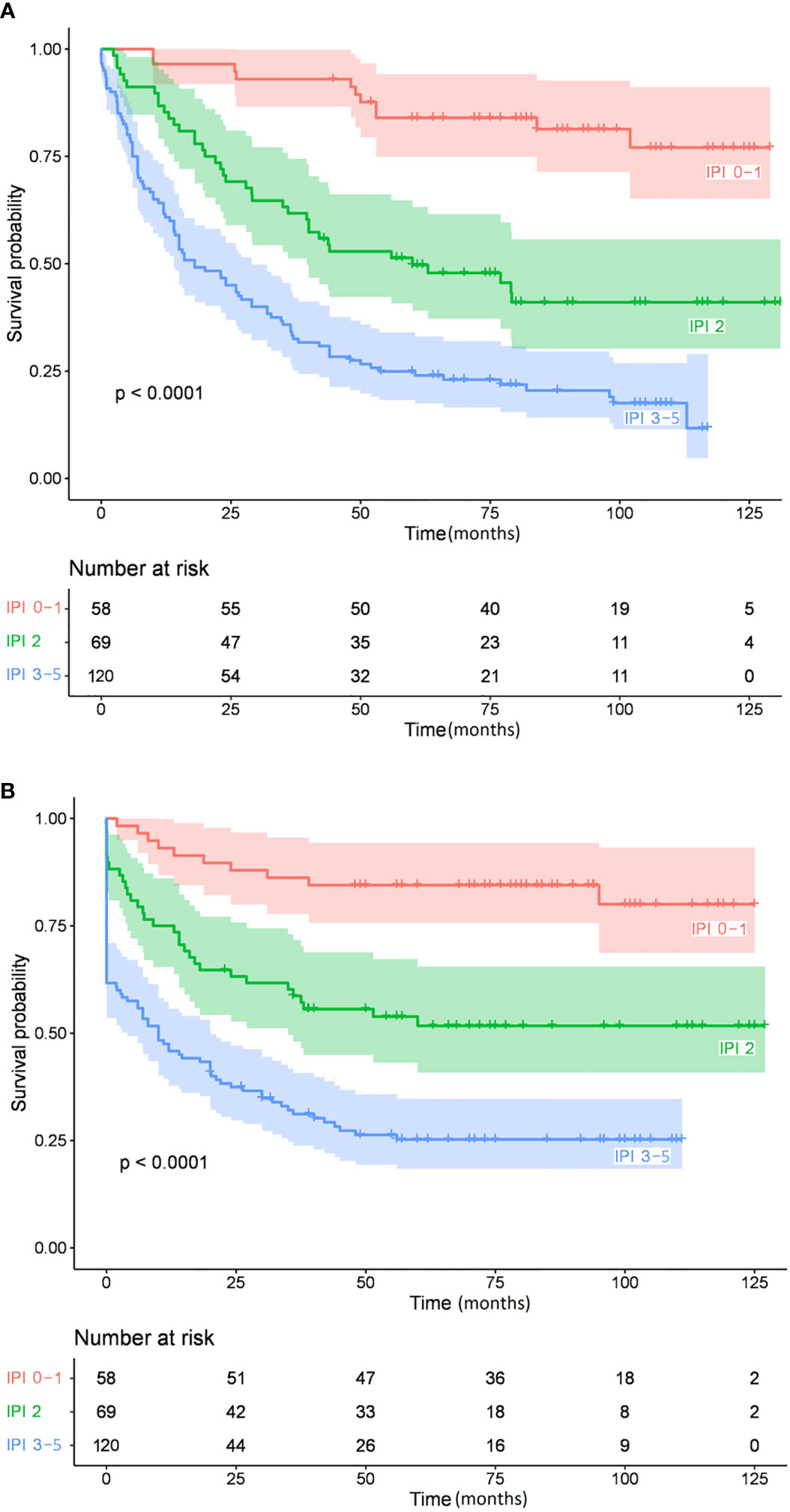
Figure 2 Overall survival (A) and event-free survival (B) by the International Prognostic Index.
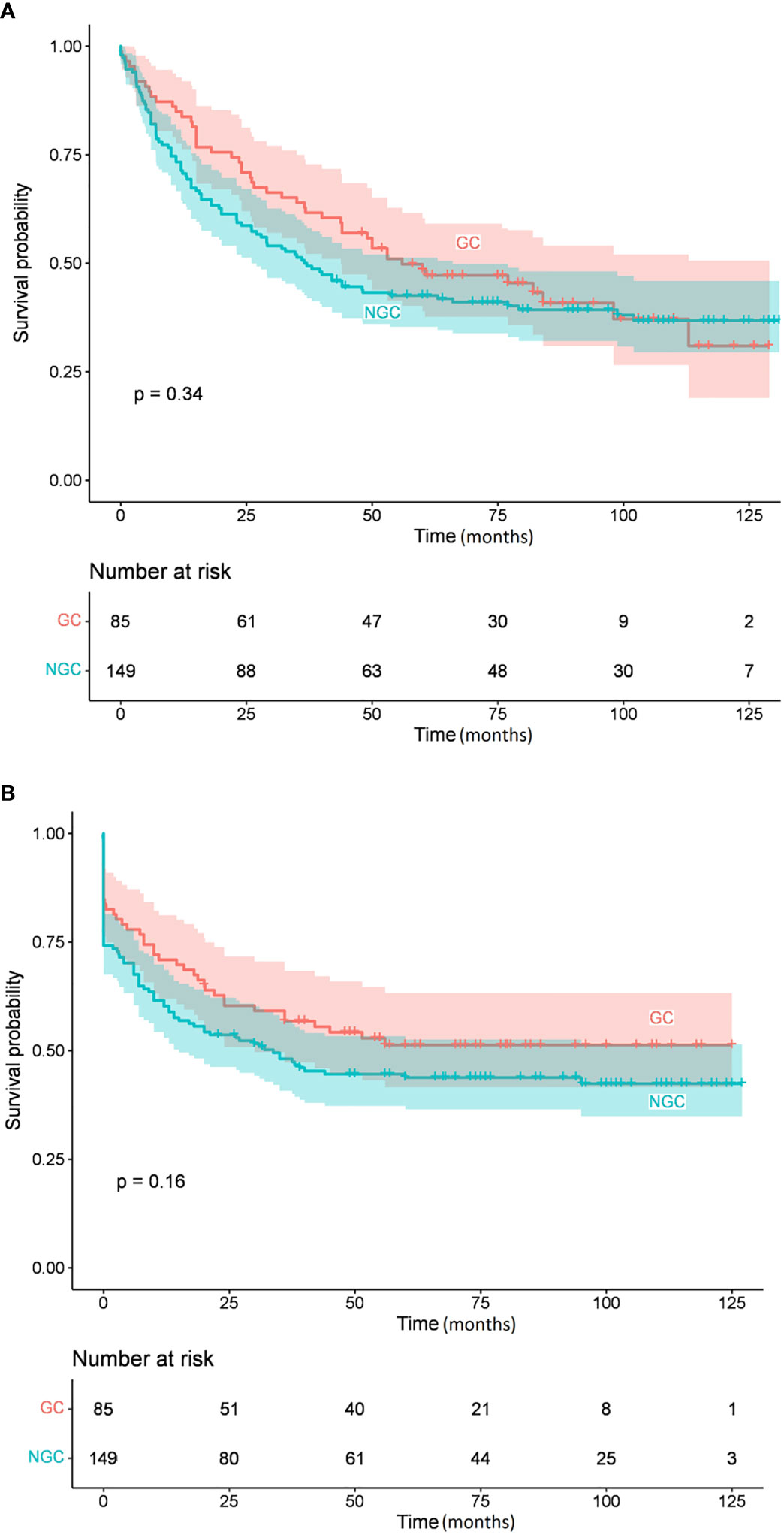
Figure 3 Overall survival (A) and event-free survival (B) by cell of origin subgroups.
Table 5 summarizes the findings of the multivariate analysis of 220 patients. IPI score was a significant independent negative, whereas MIB-1 and BCL6 protein expressions were significant independent positive predictors of both OS and EFS.
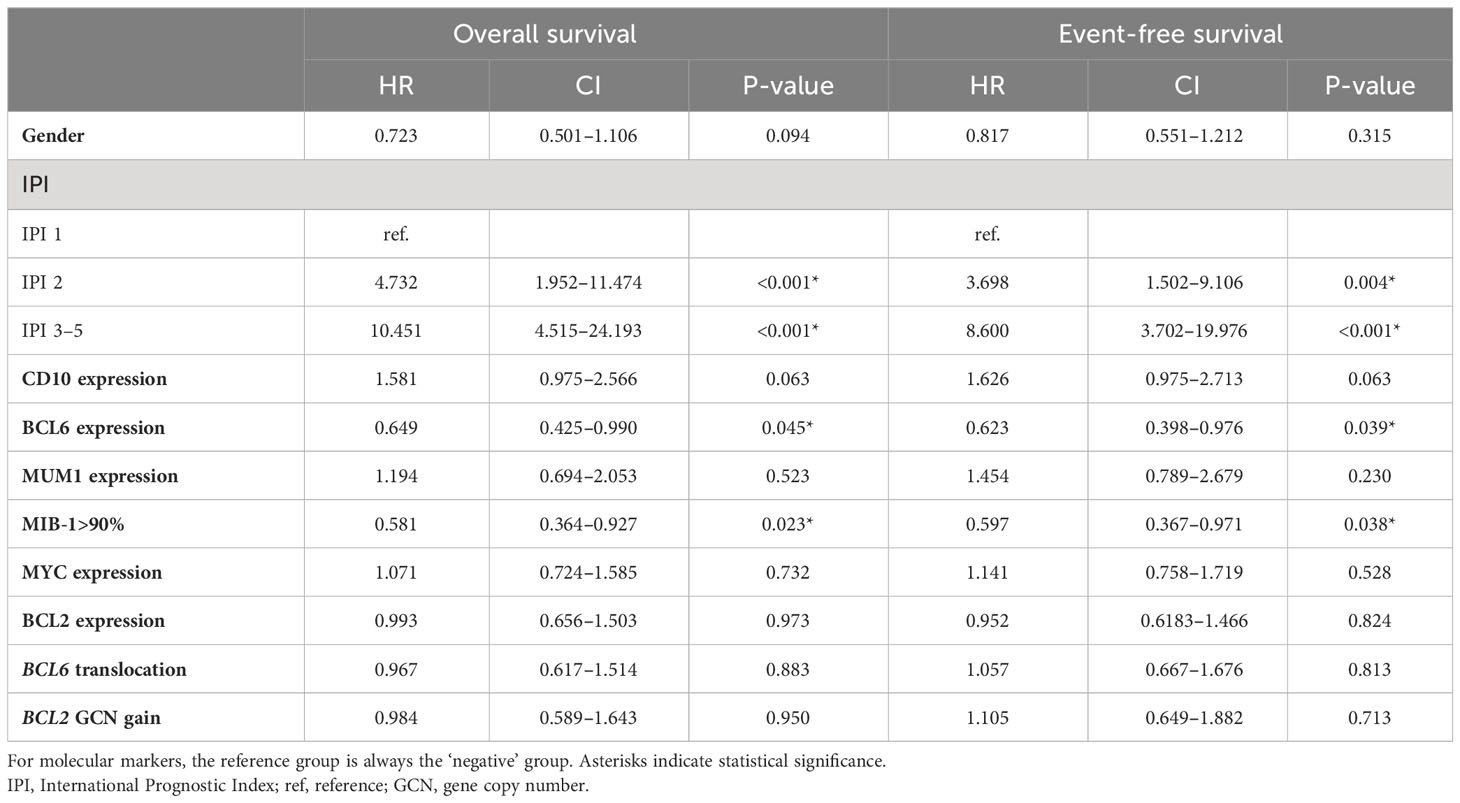
Table 5 Multivariate Cox regression analysis for overall survival and event-free survival.
4 Discussion
The clinical and genetic heterogeneity of DLBCL still presents challenges in predicting response to treatment and prognosis. The 2016 revision of the World Health Organization classification of lymphoid neoplasms made it mandatory to classify the molecular subgroups of DLBCL into GCB and ABC subtypes (37) and this remains unchanged in the WHO 5th edition published in 2023 (38). However, 10–15% of DLBCL cases cannot be categorized into one of the two COO groups and are termed unclassified DLBCL using gene expression studies. In the current study, we used IHC and FISH techniques on samples from DLBCL patients to classify rituximab-treated patients in many ways including by COO. Then, we interpreted survival data in this context.
In our cohort of patients, the COO phenotype failed to predict prognosis, which is surprising knowing that some studies have demonstrated significantly better survival for the GCB group (47, 48). However, the prognostic value of COO remains controversial, and other authors did not report any differences in overall prognosis based on COO, in line with our observations (49–51). Table 6. summarizes the COO distribution and survival data of DLBCL patients according to the immunophenotyping results reported in our study and other published reports. The controversy of the literature may be explained by many factors including but not restricted to the retrospective nature of the studies with a mixed pool of patients receiving various treatment regimens, in addition to a relatively short follow-up period (52).
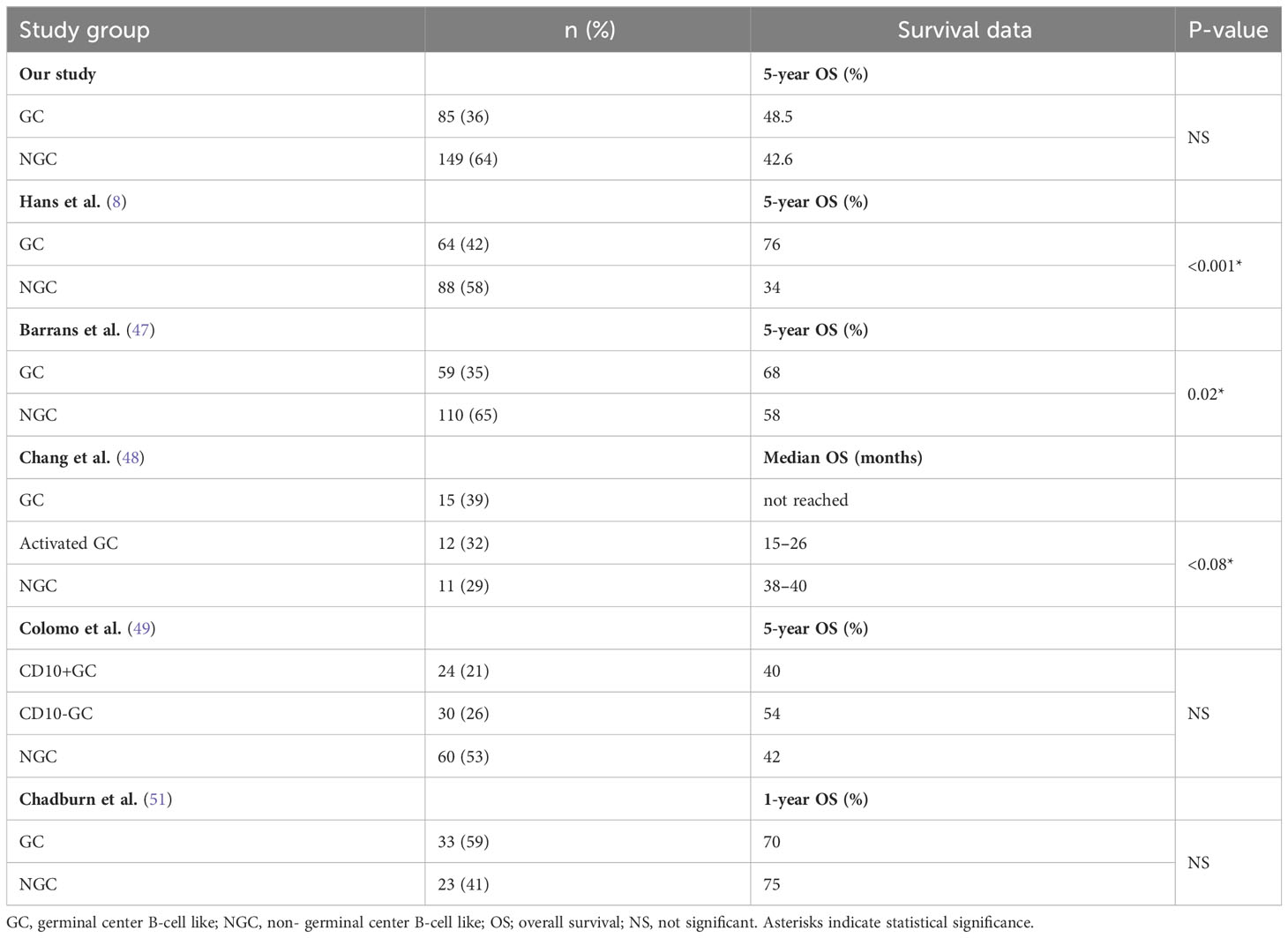
Table 6 Distribution and survival data of DLBCL patients included in different studies according to immunophenotype.
Factors that were independently associated with EFS in the multivariate analysis were IPI, high MIB-1 (>90%), and BCL6 expression. According to our results, BCL6 protein overexpression carries a positive prognostic effect on OS and EFS. BCL6 protein expression is considered as a hallmark of GC origin in DLBCL and it is associated with favorable outcome reported by some studies, consistent with our results (8, 19, 53–56). However, our findings demonstrated no significant association between BCL6 protein expression and BCL6 translocation. In our study, the frequency of BCL6 gene rearrangement was 21.4% and most of the cases were stratified into the non-GCB group according to the Hans algorithm. The association between the BCL6 gene alteration and non-GCB phenotype was confirmed by other studies as well (17, 20, 57, 58). In our study, BCL6 rearrangement had no prognostic impact on OS or EFS. Other studies yielded conflicting results showing that BCL6 rearrangement was associated with a worse outcome (20, 59–63), reporting no significant associations at all (64–67), or implying an association with favorable outcomes (68, 69).
BCL2, MUM1, and MYC protein expressions did not emerge as independent prognostic variables in multivariate analysis. Unlike the high proliferation index (>90%) detected by MIB-1 antibody, which proved to be an independent predictor of good prognosis regarding OS and EFS. We did not find any significant difference in OS and EFS of DEL cases compared to the non-DEL cases.
Our finding suggesting no impact of BCL2 expression on the prognosis of patients with DLBCLis in line with the results of some previous publications (8, 70–73). However, other researchers have observed adverse outcomes with BCL2 protein overexpression (17, 26, 27, 74). In addition, in our study, there was no significant association between BCL2 protein expression and BCL2 gene aberrations.
Finally, even in the rituximab era, there are still significant differences in OS and EFS across the IPI groups.
Our study has several strengths and limitations. The major strength of our work includes the size and coverage of the study population (247 DLBCL cases from 7 Hungarian centers), allowing a detailed and representative survival analysis. The major limitation of our work is the study’s retrospective design, which, as reflected by the number of excluded patients, resulted in lack of a full dataset in some analyses.
5 Conclusion
Successful integration of predictive and prognostic tools in DLBCL trials requires combination of clinical and molecular factors. Our study provides additional support to previously reported publications that DLBCL is characterized by heterogeneous molecular features and clinical outcomes. Based on our findings, only the IPI, BCL6 expression by IHC, and high (>90%) MIB-1 expression and not the other markers analyzed (CD10, BCL2, MUM1, MYC positivity, and gender) are independent predictors of OS and EFS in DLBCL. We did not find any difference in survival by GCB vs. non-GCB subtypes. These findings may improve prognostication in DLBCL and can contribute to designing further research in the area. However, considering the limitations of our study, these findings should be validated in prospective series.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by The Committee of Science and Research Ethics (ETT-TUKEB) under reference number 50268-8/2017. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
HA, IV-N, BA, and LP designed the research; NF and ZS analyzed data; HA, BA, and ZS drafted the manuscript; HA, LP, BA, IV-N, ZR, AG, BK, LK and ZS reviewed and approved the final version of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The research was supported by the NVKP_16-1-2016-0005 project of National Research and Development Office, Hungary as well as the EFOP-3.6.1-16-2016-0004 and the MTA PAB Clinicopathology WG.
Acknowledgments
The authors thank the patients, all primary treating physicians, nursing and laboratory staff members who participated in this multicenter trial for their excellent cooperation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. (2008). WHO classification of tumours of haematopoietic and lymphoid tissues. Lyon, France: IARC.
2. Sujobert P, Salles G, Bachy E. Molecular classification of diffuse large B-cell lymphoma: what is clinically relevant? Hematol Oncol Clin North Am (2016) 30(6):1163–77. doi: 10.1016/j.hoc.2016.07.001
3. Crump M, Neelapu SS, Farooq U, Van Den Neste E, Kuruvilla J, Westin J, et al. Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study. Blood (2017) 130(16):1800–8. doi: 10.1182/blood-2017-03-769620
4. Maurer MJ, Ghesquières H, Jais JP, Witzig TE, Haioun C, Thompson CA, et al. Event-free survival at 24 months is a robust end point for disease-related outcome in diffuse large B-cell lymphoma treated with immunochemotherapy. J Clin Oncol (2014) 32(10):1066–73. doi: 10.1200/JCO.2013.51.5866
5. Jakobsen LH, Bøgsted M, Brown PN, Arboe B, Jørgensen J, Larsen TS, et al. Minimal loss of lifetime for patients with diffuse large B-cell lymphoma in remission and event free 24 months after treatment: A danish population-based study. J Clin Oncol (2017) 35(7):778–84. doi: 10.1200/JCO.2016.70.0765
6. Ritter Z, Papp L, Zámbó K, Tóth Z, Dezső D, Veres DS, et al. Two-year event-free survival prediction in DLBCL patients based on in vivo radiomics and clinical parameters. Front Oncol (2022) 12:820136. doi: 10.3389/fonc.2022.820136
7. Alizadeh AA, Eisen MB, Davis RE, Ma C, Lossos IS, Rosenwald A, et al. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature (2000) 403(6769):503–11. doi: 10.1038/35000501
8. Hans CP, Weisenburger DD, Greiner TC, Gascoyne RD, Delabie J, Ott G, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood (2004) 103(1):275–82. doi: 10.1182/blood-2003-05-1545
9. Choi WW, Weisenburger DD, Greiner TC, Piris MA, Banham AH, Delabie J, et al. A new immunostain algorithm classifies diffuse large B-cell lymphoma into molecular subtypes with high accuracy. Clin Cancer Res (2009) 15(17):5494–502. doi: 10.1158/1078-0432.CCR-09-0113
10. Meyer PN, Fu K, Greiner TC, Smith LM, Delabie J, Gascoyne RD, et al. Immunohistochemical methods for predicting cell of origin and survival in patients with diffuse large B-cell lymphoma treated with rituximab. J Clin Oncol (2011) 29(2):200–7. doi: 10.1200/JCO.2010.30.0368
11. Scott DW, Wright GW, Williams PM, Lih CJ, Walsh W, Jaffe ES, et al. Determining cell-of-origin subtypes of diffuse large B-cell lymphoma using gene expression in forMalin-fixed paraffin-embedded tissue. Blood (2014) 123(8):1214–7. doi: 10.1182/blood-2013-11-536433
12. Ye BH, Lista F, Lo Coco F, Knowles DM, Offit K, Chaganti RS, et al. Alterations of a zinc finger-encoding gene, BCL-6, in diffuse large-cell lymphoma. Science (1993) 262:747–50. doi: 10.1126/science.8235596
13. Cattoretti G, Chang CC, Cechova K, Zhang J, Ye BH, Falini B, et al. BCL-6 protein is expressed in germinal-center B cells. Blood (1995) 86:45–53. doi: 10.1182/blood.V86.1.45.bloodjournal86145
14. Chang CC, Ye BH, Chaganti RS, Dalla-Favera R. BCL-6, a POZ/zinc-finger protein, is a sequence-specific transcriptional repressor. Proc Natl Acad Sci U S A. (1996) 93(14):6947–52. doi: 10.1073/pnas.93.14.6947
15. Cattoretti G, Pasqualucci L, Ballon G, Tam W, Nandula SV, Shen Q, et al. Deregulated BCL6 expression recapitulates the pathogenesis of human diffuse large B cell lymphomas in mice. Cancer Cell (2005) 7(5):445–55. doi: 10.1016/j.ccr.2005.03.037
16. Jerkeman M, Aman P, Cavallin-Stahl E, Torlakovic E, Akerman M, Mitelman F, et al. Prognostic implications of BCL6 rearrangement in uniformly treated patients with diffuse large B-cell lymphoma–a Nordic Lymphoma Group study. Int J Oncol (2002) 20(1):161–5. doi: 10.3892/ijo.20.1.161
17. Kramer MH, Hermans J, Wijburg E, Philippo K, Geelen E, van Krieken JH, et al. Clinical relevance of BCL2, BCL6, and MYC rearrangements in diffuse large B-cell lymphoma. Blood (1998) 92(9):3152–62. doi: 10.1182/blood.V92.9.3152
18. Bastard C, Deweindt C, Kerckaert JP, Lenormand B, Rossi A, Pezzella F, et al. LAZ3 rearrangements in non-Hodgkin's lymphoma: correlation with histology, immunophenotype, karyotype, and clinical outcome in 217 patients. Blood (1994) 83:2423–7. doi: 10.1182/blood.V83.9.2423.2423
19. Winter JN, Weller EA, Horning SJ, Krajewska M, Variakojis D, Habermann TM, et al. Prognostic significance of Bcl-6 protein expression in DLBCL treated with CHOP or R-CHOP: a prospective correlative study. Blood (2006) 107:4207–13. doi: 10.1182/blood-2005-10-4222
20. Barrans SL, O'Connor SJ, Evans PA, Davies FE, Owen RG, Haynes AP, et al. Rearrangement of the BCL6 locus at 3q27 is an independent poor prognostic factor in nodal diffuse large B-cell lymphoma. Br J Haematol (2002) 117(2):322–32. doi: 10.1046/j.1365-2141.2002.03435.x
21. Czabotar PE, Lessene G, Strasser A, Adams JM. Control of apoptosis by the BCL-2 protein family: implications for physiology and therapy. Nat Rev Mol Cell Biol (2014) 15(1):49–63. doi: 10.1038/nrm3722
22. Vaux DL, Cory S, Adams JM. Bcl-2 gene promotes haemopoietic cell survival and cooperates with c-myc to immortalize pre-B cells. Nature (1988) 335(6189):440–2. doi: 10.1038/335440a0
23. Letai AG. Diagnosing and exploiting cancer's addiction to blocks in apoptosis. Nat Rev Canc (2008) 8(2):121–32. doi: 10.1038/nrc2297
24. Tsujimoto Y, Cossman J, Jaffe E, Croce CM. Involvement of the bcl-2 gene in human follicular lymphoma. Science (1985) 228(4706):1440–3. doi: 10.1126/science.3874430
25. Delbridge AR, Grabow S, Strasser A, Vaux DL. Thirty years of BCL-2: translating cell death discoveries into novel cancer therapies. Nat Rev Canc (2016) 16(2):99–109. doi: 10.1038/nrc.2015.17
26. Visco C, Tzankov A, Xu-Monette ZY, MIranda RN, Tai YC, Li Y, et al. Patients with diffuse large B-cell lymphoma of germinal center origin with BCL2 translocations have poor outcome, irrespective of MYC status: a report from an International DLBCL rituximab-CHOP Consortium Program Study. Haematologica (2013) 98(2):255–63. doi: 10.3324/haematol.2012.066209
27. Horn H, Ziepert M, Becher C, Barth TF, Bernd HW, Feller AC, et al. MYC status in concert with BCL2 and BCL6 expression predicts outcome in diffuse large B-cell lymphoma. Blood (2013) 121(12):2253–63. doi: 10.1182/blood-2012-06-435842
28. Iqbal J, Meyer PN, Smith LM, Johnson NA, Vose JM, Greiner TC, et al. BCL2 predicts survival in germinal center B-cell-like diffuse large B-cell lymphoma treated with CHOP-like therapy and rituximab. Clin Cancer Res (2011) 17(24):7785–95. doi: 10.1158/1078-0432.CCR-11-0267
29. Iqbal J, Neppalli VT, Wright G, Dave BJ, Horsman DE, Rosenwald A, et al. BCL2 expression is a prognostic marker for the activated B-cell-like type of diffuse large B-cell lymphoma. J Clin Oncol (2006) 24(6):961–8. doi: 10.1200/JCO.2005.03.4264
30. Chisholm KM, Bangs CD, Bacchi CE, Molina-Kirsch H, Cherry A, Natkunam Y. Expression profiles of MYC protein and MYC gene rearrangement in lymphomas. Am J Surg Pathol (2015) 39(3):294–303. doi: 10.1097/PAS.0000000000000365
31. Karube K, Campo E. MYC alterations in diffuse large B-cell lymphomas. Semin Hematol (2015) 52(2):97–106. doi: 10.1053/j.seminhematol.2015.01.009
32. Meyer N, Penn LZ. Reflecting on 25 years with MYC. Nat Rev Canc (2008) 8(12):976–90. doi: 10.1038/nrc2231
33. Pelengaris S, Khan M, Evan G. c-MYC: more than just a matter of life and death. Nat Rev Canc (2002) 2(10):764–76. doi: 10.1038/nrc904
34. Savage KJ, Johnson NA, Ben-Neriah S, Connors JM, Sehn LH, Farinha P, et al. MYC gene rearrangements are associated with a poor prognosis in diffuse large B-cell lymphoma patients treated with R-CHOP chemotherapy. Blood (2009) 114(17):3533–7. doi: 10.1182/blood-2009-05-220095
35. Barrans S, Crouch S, Smith A, Turner K, Owen R, Patmore R, et al. Rearrangement of MYC is associated with poor prognosis in patients with diffuse large B-cell lymphoma treated in the era of rituximab. J Clin Oncol (2010) 28(20):3360–5. doi: 10.1200/JCO.2009.26.3947
36. Zhang HW, Chen ZW, Li SH, Bai W, Cheng NL, Wang JF. Clinical significance and prognosis of MYC translocation in diffuse large B-cell lymphoma. Hematol Oncol (2011) 29(4):185–9. doi: 10.1002/hon.991
37. Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood (2016) 127(20):2375–90. doi: 10.1182/blood-2016-01-643569
38. Alaggio R, Amador C, Anagnostopoulos I, Attygalle AD, Araujo IBO, Berti E, et al. The 5th edition of the world health organization classification of haematolymphoid tumours: lymphoid neoplasms. Leukemia (2022) 36(7):1720–48. doi: 10.1038/s41375-022-01620-2
39. Johnson NA, Slack GW, Savage KJ, Connors JM, Ben-Neriah S, Rogic S, et al. Concurrent expression of MYC and BCL2 in diffuse large B-cell lymphoma treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone. J Clin Oncol (2012) 30(28):3452–9. doi: 10.1200/JCO.2011.41.0985
40. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. J Clin Epidemiol. (2008) 61(4):344–9. doi: 10.1016/j.jclinepi.2007.11.008
41. Pajor G, Kajtár B, Pajor L, Alpár D. State-of-the-art FISHing: automated analysis of cytogenetic aberrations in interphase nuclei. Cytomet A. (2012) 81(8):649–63. doi: 10.1002/cyto.a.22082
42. Lister TA, Crowther D, Sutcliffe SB, Glatstein E, Canellos GP, Young RC, et al. Report of a committee convened to discuss the evaluation and staging of patients with Hodgkin's disease: Cotswolds meeting. J Clin Oncol (1989) 7(11):1630–6. doi: 10.1200/JCO.1989.7.11.1630
43. Cheson BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, Zucca E, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol (2014) 32(27):3059–68. doi: 10.1200/JCO.2013.54.8800
44. Cheson BD, Pfistner B, Juweid ME, Gascoyne RD, Specht L, Horning SJ, et al. Revised response criteria for Malignant lymphoma. J Clin Oncol (2007) 25(5):579–86. doi: 10.1200/JCO.2006.09.2403
45. R Core Team. (2022). R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing. Available at: https://www.R-project.org [Accessed February 6, 2023].
46. Kassambara. (2021). Computing. Vienna, Austria Available at: https://www.R-project.org/ [Accessed February 6, 2023].
47. Barrans SL, Carter I, Owen RG, Davies FE, Patmore RD, Haynes AP, et al. Germinal center phenotype and bcl-2 expression combined with the International Prognostic Index improves patient risk stratification in diffuse large B-cell lymphoma. Blood (2002) 99(4):1136–43. doi: 10.1182/blood.v99.4.1136
48. Chang CC, McClintock S, Cleveland RP, Trzpuc T, Vesole DH, Logan B, et al. Immunohistochemical expression patterns of germinal center and activation B-cell markers correlate with prognosis in diffuse large B-cell lymphoma. Am J Surg Pathol (2004) 28(4):464–70. doi: 10.1097/00000478-200404000-00005
49. Colomo L, López-Guillermo A, Perales M, Rives S, Martínez A, Bosch F, et al. Clinical impact of the differentiation profile assessed by immunophenotyping in patients with diffuse large B-cell lymphoma. Blood (2003) 101(1):78–84. doi: 10.1182/blood-2002-04-1286
50. Linderoth J, Jerkeman M, Cavallin-Ståhl E, Kvaløy S, Torlakovic E. Nordic Lymphoma Group Study. Immunohistochemical expression of CD23 and CD40 may identify prognostically favorable subgroups of diffuse large B-cell lymphoma: a Nordic Lymphoma Group Study. Clin Cancer Res (2003) 9(2):722–8.
51. Chadburn A, Chiu A, Lee JY, Chen X, Hyjek E, Banham AH, et al. Immunophenotypic analysis of AIDS-related diffuse large B-cell lymphoma and clinical implications in patients from AIDS Malignancies Consortium clinical trials 010 and 034. J Clin Oncol (2009) 27(30):5039–48. doi: 10.1200/JCO.2008.20.5450
52. Dunleavy K, Wilson WH. Role of molecular subtype in predicting outcome of AIDS-related diffuse large B-cell lymphoma. J Clin Oncol (2010) 28(16):e260. doi: 10.1200/JCO.2009.27.7087
53. Takeshita M, Iwashita A, Kurihara K, Ikejiri K, Higashi H, Udoh T, et al. Histologic and immunohistologic findings and prognosis of 40 cases of gastric large B-cell lymphoma. Am J Surg Pathol (2000) 24(12):1641–9. doi: 10.1097/00000478-200012000-00008
54. Lossos IS, Jones CD, Warnke R, Natkunam Y, Kaizer H, Zehnder JL, et al. Expression of a single gene, BCL-6, strongly predicts survival in patients with diffuse large B-cell lymphoma. Blood (2001) 98(4):945–51. doi: 10.1182/blood.v98.4.945
55. Advani P, Ngamphaiboon N, Pukiat S, Chavez J, Deeb G, Elefante A, et al. The expression of bcl-6 in diffuse large B cell lymphoma (DLBCL) is associated with improved progression free survival and overall survival following front-line rituximab-chemotherapy. Blood (2010) 116(21):5073. doi: 10.1182/blood.v116.21.5073.5073
56. Iqbal J, Greiner TC, Patel K, Dave BJ, Smith L, Ji J, et al. Distinctive patterns of BCL6 molecular alterations and their functional consequences in different subgroups of diffuse large B-cell lymphoma. Leukemia (2007) 21(11):2332–43. doi: 10.1038/sj.leu.2404856
57. Copie-Bergman C, Gaulard P, Leroy K, Briere J, Baia M, Jais JP, et al. Immuno-fluorescence in situ hybridization index predicts survival in patients with diffuse large B-cell lymphoma treated with R-CHOP: a GELA study. J Clin Oncol (2009) 27(33):5573–9. doi: 10.1200/JCO.2009.22.7058
58. Shustik J, Han G, Farinha P, Johnson NA, Ben Neriah S, Connors JM, et al. Correlations between BCL6 rearrangement and outcome in patients with diffuse large B-cell lymphoma treated with CHOP or R-CHOP. Haematologica (2010) 95(1):96–101. doi: 10.3324/haematol.2009.007203
59. Gao P, Li Q, Wang Z, Yan F, Lu C, Cao X. [Significance of BCL6, MYC, P53 genes abnorMalities for the prognosis of diffuse large B-cell lymphoma]. Zhonghua Yi Xue Yi Chuan Xue Za Zhi. (2014) 31(5):628–31. doi: 10.3760/cma.j.issn.1003-9406.2014.01.020
60. Akyurek N, Uner A, Benekli M, Barista I. Prognostic significance of MYC, BCL2, and BCL6 rearrangements in patients with diffuse large B-cell lymphoma treated with cyclophosphamide, doxorubicin, vincristine, and prednisone plus rituximab. Cancer (2012) 118(17):4173–83. doi: 10.1002/cncr.27396
61. Akasaka T, Ueda C, Kurata M, Akasaka H, Yamabe H, Uchiyama T, et al. Nonimmunoglobulin (non-Ig)/BCL6 gene fusion in diffuse large B-cell lymphoma results in worse prognosis than Ig/BCL6. Blood (2000) 96(8):2907–9. doi: 10.1182/blood.V96.8.2907
62. Liang X, Wang J, Bai W, Sun R. Expression of CD68, cyclin D1 and rearrangement of bcl-6 gene are adverse prognostic factors in diffuse large B-cell lymphoma. Zhonghua Bing Li Xue Za Zhi. (2015) 44(8):559–64. Chinese.
63. Li S, Wang Z, Lin L, Wu Z, Yu Q, Gao F, et al. BCL6 rearrangement indicates poor prognosis in diffuse large B-cell lymphoma patients: A meta-analysis of cohort studies. J Canc (2019) 10(2):530–8. doi: 10.7150/jca.25732
64. Chen PM, Yang MH, Yu IT, Lin JT, Lin YC, Fan FS, et al. Low incidence of BCL-6 gene alterations for diffuse large B-cell lymphomas in Taiwan Chinese. Cancer (2002) 94(10):2635–44. doi: 10.1002/cncr.10545
65. Pedersen MO, Gang AO, Brown P, Pedersen M, Knudsen H, Nielsen SL, et al. Real world data on young patients with high-risk diffuse large B-cell lymphoma treated with R-CHOP or R-CHOEP - MYC, BCL2 and BCL6 as prognostic biomarkers. PloS One (2017) 12(10):e0186983. doi: 10.1371/journal.pone.0186983
66. Ye Q, Xu-Monette ZY, Tzankov A, Deng L, Wang X, Manyam GC, et al. Prognostic impact of concurrent MYC and BCL6 rearrangements and expression in de novo diffuse large B-cell lymphoma. Oncotarget (2016) 7(3):2401–16. doi: 10.18632/oncotarget.6262
67. Batlle-López A, González de Villambrosía S, Francisco M, Malatxeberria S, Sáez A, Montalban C, et al. Stratifying diffuse large B-cell lymphoma patients treated with chemoimmunotherapy: GCB/non-GCB by immunohistochemistry is still a robust and feasible marker. Oncotarget (2016) 7(14):18036–49. doi: 10.18632/oncotarget.7495
68. Niitsu N, Okamoto M, Nakamura N, Nakamine H, Aoki S, HIrano M, et al. Prognostic impact of chromosomal alteration of 3q27 on nodal B-cell lymphoma: correlation with histology, immunophenotype, karyotype, and clinical outcome in 329 consecutive patients. Leuk Res (2007) 31(9):1191–7. doi: 10.1016/j.leukres.2006.11.004
69. Offit K, Lo Coco F, Louie DC, Parsa NZ, Leung D, Portlock C, et al. Rearrangement of the bcl-6 gene as a prognostic marker in diffuse large-cell lymphoma. N Engl J Med (1994) 331(2):74–80. doi: 10.1056/NEJM199407143310202
70. Tang SC, Visser L, Hepperle B, Hanson J, Poppema S. Clinical significance of bcl-2-MBR gene rearrangement and protein expression in diffuse large-cell non-Hodgkin's lymphoma: an analysis of 83 cases. J Clin Oncol (1994) 12(1):149–54. doi: 10.1200/JCO.1994.12.1.149
71. Hill ME, MacLennan KA, Cunningham DC, Vaughan Hudson B, Burke M, Clarke P, et al. Prognostic significance of BCL-2 expression and bcl-2 major breakpoint region rearrangement in diffuse large cell non-Hodgkin's lymphoma: a British National Lymphoma Investigation Study. Blood (1996) 88(3):1046–51. doi: 10.1182/blood.V88.3.1046.1046
72. Sanchez E, Chacon I, Plaza MM, Munoz E, Cruz MA, Martinez B, et al. Clinical outcome in diffuse large B-cell lymphoma is dependent on the relationship between different cell-cycle regulator proteins. J Clin Oncol (1998) 16(5):1931–9. doi: 10.1200/JCO.1998.16.5.1931
73. Zhang A, Ohshima K, Sato K, Kanda M, Suzumiya J, Shimazaki K, et al. Prognostic clinicopathologic factors, including immunologic expression in diffuse large B-cell lymphomas. Pathol Int (1999) 49(12):1043–52. doi: 10.1046/j.1440-1827.1999.00980.x
Keywords: diffuse large B-cell lymphoma, MYC, BCL6, BCL2, IHC, FISH, prognosis
Citation: Balikó A, Szakács Z, Kajtár B, Ritter Z, Gyenesei A, Farkas N, Kereskai L, Vályi-Nagy I, Alizadeh H and Pajor L (2023) Clinicopathological analysis of diffuse large B-cell lymphoma using molecular biomarkers: a retrospective analysis from 7 Hungarian centers. Front. Oncol. 13:1224733. doi: 10.3389/fonc.2023.1224733
Received: 18 May 2023; Accepted: 21 August 2023;
Published: 08 September 2023.
Edited by:
Robert Ohgami, The University of Utah, United StatesReviewed by:
Joaquim Carreras, Tokai University, JapanSebastian Fernandez-Pol, Stanford University, United States
Copyright © 2023 Balikó, Szakács, Kajtár, Ritter, Gyenesei, Farkas, Kereskai, Vályi-Nagy, Alizadeh and Pajor. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hussain Alizadeh, YWxpemFkZWguaHVzc2FpbkBwdGUuaHU=