 Cécile Mione1†
Cécile Mione1† Mélanie Casile2,3,4†Juliette Moreau1Jessica Miroir1
Mélanie Casile2,3,4†Juliette Moreau1Jessica Miroir1 Ioana Molnar2,3,4
Ioana Molnar2,3,4 Emmanuel Chautard1,2
Emmanuel Chautard1,2 Maureen Bernadach3,4,5
Maureen Bernadach3,4,5 Myriam Kossai2,6Nicolas Saroul7F. Martin1Nathalie Pham-Dang8Michel Lapeyre1†
Myriam Kossai2,6Nicolas Saroul7F. Martin1Nathalie Pham-Dang8Michel Lapeyre1† Julian Biau1,2*†
Julian Biau1,2*†- 1Department of Radiation Therapy, Centre Jean Perrin, Clermont-Ferrand, France
- 2INSERM U1240 IMoST, University of Clermont Auvergne, Clermont-Ferrand, France
- 3UMR 501, Clinical Investigation Centre, Clermont-Ferrand, France
- 4Department of Clinical Research, Clinical Search and Innovation, Centre Jean Perrin, Clermont-Ferrand, France
- 5Medical Oncology Department, Jean Perrin Center, Clermont-Ferrand, France
- 6Department of Pathology and Molecular Pathology, Centre Jean Perrin, Clermont-Ferrand, France
- 7Department of Otolaryngology-Head and Neck Surgery, Clermont-Ferrand University Hospital, Clermont-Ferrand, France
- 8Department of Maxillo-Facial Surgery, Clermont-Ferrand University Hospital, Clermont-Ferrand, France
Background: Presently, there are few published reports on postoperative radiation therapy for oropharyngeal and oral cavity cancers treated with IMRT/VMAT technique. This study aimed to assess the oncological outcomes of this population treated with postoperative VMAT in our institution, with a focus on loco-regional patterns of failure.
Material and methods: Between 2011 and 2019, 167 patients were included (40% of oropharyngeal cancers, and 60% of oral cavity cancers). The median age was 60 years. There was 64.2% of stage IV cancers. All patients had both T and N surgery. 34% had a R1 margin, 42% had perineural invasion. 72% had a positive neck dissection and 42% extranodal extension (ENE). All patients were treated with VMAT with simultaneous integrated boost with three dose levels: 66Gy in case of R1 margin and/or ENE, 59.4-60Gy on the tumor bed, and 54Gy on the prophylactic areas. Concomittant cisplatin was administrated concomitantly when feasible in case of R1 and/or ENE.
Results: The 1- and 2-year loco-regional control rates were 88.6% and 85.6% respectively. Higher tumor stage (T3/T4), the presence of PNI, and time from surgery >45 days were significant predictive factors of worse loco-regional control in multivariate analysis (p=0.02, p=0.04, and p=0.02). There were 17 local recurrences: 11 (64%) were considered as infield, 4 (24%) as marginal, and 2 (12%) as outfield. There were 9 regional recurrences only, 8 (89%) were considered as infield, and 1 (11%) as outfield. The 1- and 2-year disease-free survival (DFS) rates were 78.9% and 71.8% respectively. The 1- and 2-year overall survival (OS) rates were 88.6% and 80% respectively. Higher tumor stage (T3/T4) and the presence of ENE were the two prognostic factors significantly associated with worse DFS and OS in multivariate analysis.
Conclusion: Our outcomes for postoperative VMAT for oral cavity and oropharyngeal cancers are encouraging, with high rates of loco-regional control. However, the management of ENE still seems challenging.
Introduction
Surgery is one of the cornerstone treatments for oropharyngeal and oral cavity cancers (1). Adjuvant postoperative radiation therapy is recommended for patients with adverse features, including advanced disease and inadequate margins. The addition of concomitant chemotherapy is recommended, particularly for patients who have ‘high risk’ pathological features including extranodal extension (ENE) and/or a positive surgical margin (1, 2).
Intensity Modulated Radiation Therapy (IMRT) or Volumetric Modulated Arctherapy (VMAT) is today the recommended radiation technique for the treatment of head and neck cancers (3). IMRT/VMAT for head and neck cancers is a complex technique both for target volume delineation and treatment planning (4, 5). The delineation of the target volumes is an essential step conditioning the results of the treatment, particularly in terms of loco-regional control (6–9). Presently, there are few published reports on postoperative radiation therapy for oropharyngeal and oral cavity cancers treated with IMRT/VMAT technique. This study aimed to assess the oncological outcomes of operated patients with oropharyngeal and oral cavity squamous cell carcinomas (SCC), treated with postoperative VMAT in our institution, with a focus on loco-regional patterns of failure.
Materials and methods
Patients
The database maintained by the Department of Radiation Oncology at our institution was used to identify patients treated with postoperative VMAT for oropharyngeal or oral cavity SCC from May 2011 to December 2019. Patients with distant metastases or concomitant malignancies at the time of diagnosis, histology other than SCC, R2 margins, and/or a previously irradiated cancer of the head and neck were excluded.
One hundred and sixty-seven patients were retrospectively reviewed. Patient characteristics are described in Table 1.
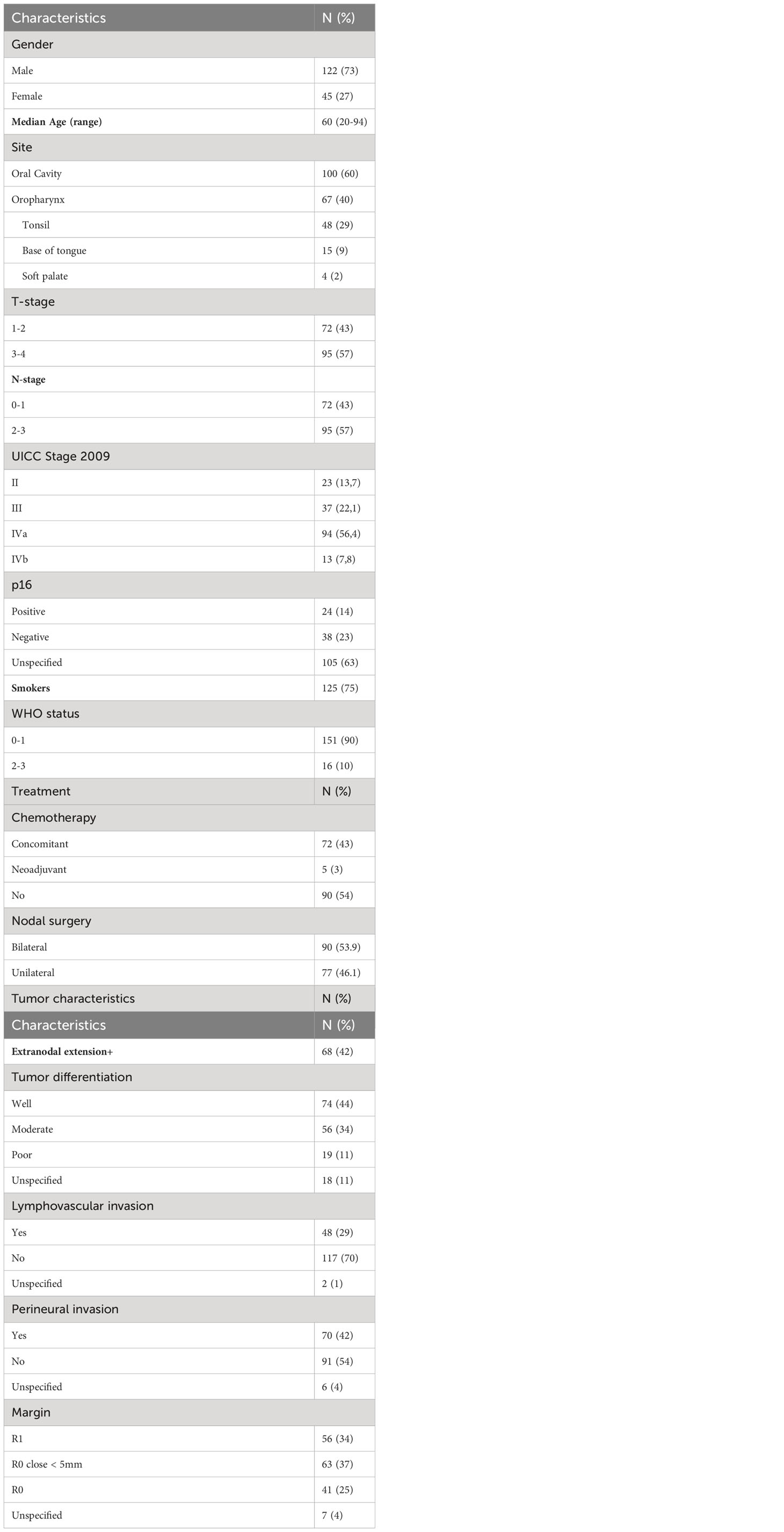
Table 1 Patient and disease characteristics.
The initial location of the tumors was the oropharynx in 40% of cases (n=67) and the oral cavity in 60% (n=100) of cases. The median age of the patients was 60 years (20 - 94 years). One hundred and twenty-five patients were smokers (75%). The WHO performance status was assessed as 0 for 78 patients (46,7%), 1 for 73 patients (43,7%), 2 for 15 patients (8,9%), and 3 for 1 patient (0,7%). The TNM stages (UICC 2009) were as follows: there were 23 stage II (13.7%), 37 stage III (22.1%), 94 stage IVa (56.4%), and 13 stage IVb (7.8%).
Treatment
The overall treatment strategies were individualized for each patient following recommendation by a multidisciplinary tumor board.
Surgery
All patients included underwent surgery on the primary tumor accompanied by lymph node dissection (unilateral for 46.1% and bilateral for 53.9%). The operative technique depended on the location and initial extension of the disease. Sixty-seven patients (40%) had a free flap inserted during surgical reconstruction.
Anatomic pathology
Fifty-six patients (34%) had a positive R1 margin, and sixty-three (37%) had a close margin (<5mm). Seventy patients (42%) had peri-neural invasion (PNI), and 48 (29%) had lympho-vascular invasion. One hundred and twenty one patients (72%) had positive neck dissections, and 68 patients (42%) had ENE (Table 1).
Radiotherapy
Patients underwent radiotherapy in case of advanced tumors (T3-T4), close or positive margins, lymph node involvement with or without ENE, the presence of lymphatic-vascular space invasion, and/or PNI (10, 11). The median interval from surgery to initiation of radiotherapy was 46 days (24 - 100). All patients were irradiated with VMAT (Rapidarc®, Varian Medical Systems, Palo Alto, CA, USA) with simultaneous integrated boost (SIB). A planning CT-scan, supine, in the treatment position, was performed, with 2.5-mm-thick slices, and a personalized thermoformed mask with 5 attachment points. Preoperative imaging was merged with the planning CT scan to guide the contouring of this surgically reshaped area. Target volumes and organs at risk were delineated according to the different expert recommendations (12–17). Three clinical target volumes (CTV) were typically defined. CTV1 (59.4 to 60 Gy) was defined as the preoperative tumor bed with a margin (1 to 2 cm), and manually adjusted according to anatomical barriers. CTV2 (54 Gy) was defined as subclinical tumor sites at risk, according to the risk of tumor involvement (14–16), and as prophylactic nodal irradiation, following guidelines (12, 13, 15). CTV3 (66 Gy) was occasionally identified, in cases of ENE and/or positive margin. Planning target volumes (PTV) related to positioning errors and movements were obtained by adding a 4 mm margin around the CTVs. Treatment was delivered in 30-33 fractions.
The treatment planning system was Eclipse® (Varian Medical Systems). Treatment plans followed the recommendations of the International Commission of Radiation Units report n°83 (18). The treatment was delivered using a Clinac IX® or Novalis TX® (Varian Medical Systems) linear accelerators delivering 6-MV photons, with daily position control by KV/KV beams or CBCT.
Chemotherapy
Seventy-two patients (43%) underwent concomitant chemotherapy. The main indications were R1 positive margins and/or ENE among patients under 70 years of age and in the absence of contraindications (10, 11, 19). Concomitant chemotherapy protocols included either three-weekly high dose Cisplatin, or weekly Cisplatin (Table 1). Five patients (3%) received neoadjuvant chemotherapy with Taxotere-Cisplatin-5Fluoro-Uracile.
Follow-up
Weekly evaluations were performed by the radiation oncologist for all patients during radiation treatment. The first post-treatment follow-up was at 3 months after radiation completion. Then, every 3 months for the first and the second year, alternating surgeon and radiation oncologist, and at least twice a year for up to 5 years, and thereafter yearly. A follow-up imaging was performed at 3 months and then annually.
Recurrences
Local and regional recurrences were confirmed via radiologic imaging (i.e. progression in subsequent images or high SUV on PET imaging) or via pathology specimens (i.e. from surgical biopsy). Diagnostic contrast-enhanced CT and/or PET/CT or MRI documenting the initial evidence of local recurrence were investigated. Radiologically evident recurrence volumes were manually segmented and reviewed by four experienced radiation oncologists (CM, JMO, JMI and JB). The corresponding original planning CTs were identified and the original plans were restored. Recurrence CT was co-registered with initial planning CT using a deformable image registration (Aria with MIRS application, version 2.1, Varian Medical Systems) (20, 21). The recurrence volume was transferred to the initial planning CT and was subsequently deformed according to the deformable co-registration. A clinical validation was carried out by the radiation oncologists. The most likely point of origin of the recurrence was defined clinically by the radiation oncologists, based on their knowledge of anatomy and cancer spread pathways according to Due et al. (22, 23). If the point of origin of the recurrence was outside the initial target volume, recurrence was considered to be “outfield”; if the point of origin of the recurrence was inside the initial target volume, recurrence was considered to be “infield”; and if the point of origin of the recurrence was on the boundary of the initial target volume, recurrence was considered to be “marginal”.
Statistical analysis
Groups defined by initial tumor localization were compared using Fisher’s exact test and the Wilcoxon-Mann-Whitney test. The Kaplan-Meier method was used to calculate survival curves. The last day of radiation therapy was used as time zero. Comparisons between survival curves were made using the log-rank test. Median follow-up was estimated using the reverse Kaplan-Meier method. Factors associated with survival were analyzed using univariate Cox regression models followed by penalized multivariate models, obtained by including all variables with a p-value <.05 in the univariate analysis and model selection with the LASSO method. All analyses were performed using R statistical software version 4.1.0 (R-Project, GNU GPL). P-values under 0.05 were considered significant.
The factors associated with survival analyzed were: gender (male/female), tobacco use (never/current or stopped), WHO stage (0/1-3), tumor status (T1-T2/T3-T4), number of pathological lymph nodes (≥3/<3), tumor differentiation (good/moderate, poor), lymphovascular invasion, PNI, ENE, margin status (R0/close, R1), radiotherapy-treatment time and surgery-radiotherapy time.
Results
Local, regional and loco-regional control
The median follow-up was 33 months. During follow-up, 26 patients (16%) developed loco-regional recurrences: 12 local, 9 regional, and 5 both local and regional (Table 2).
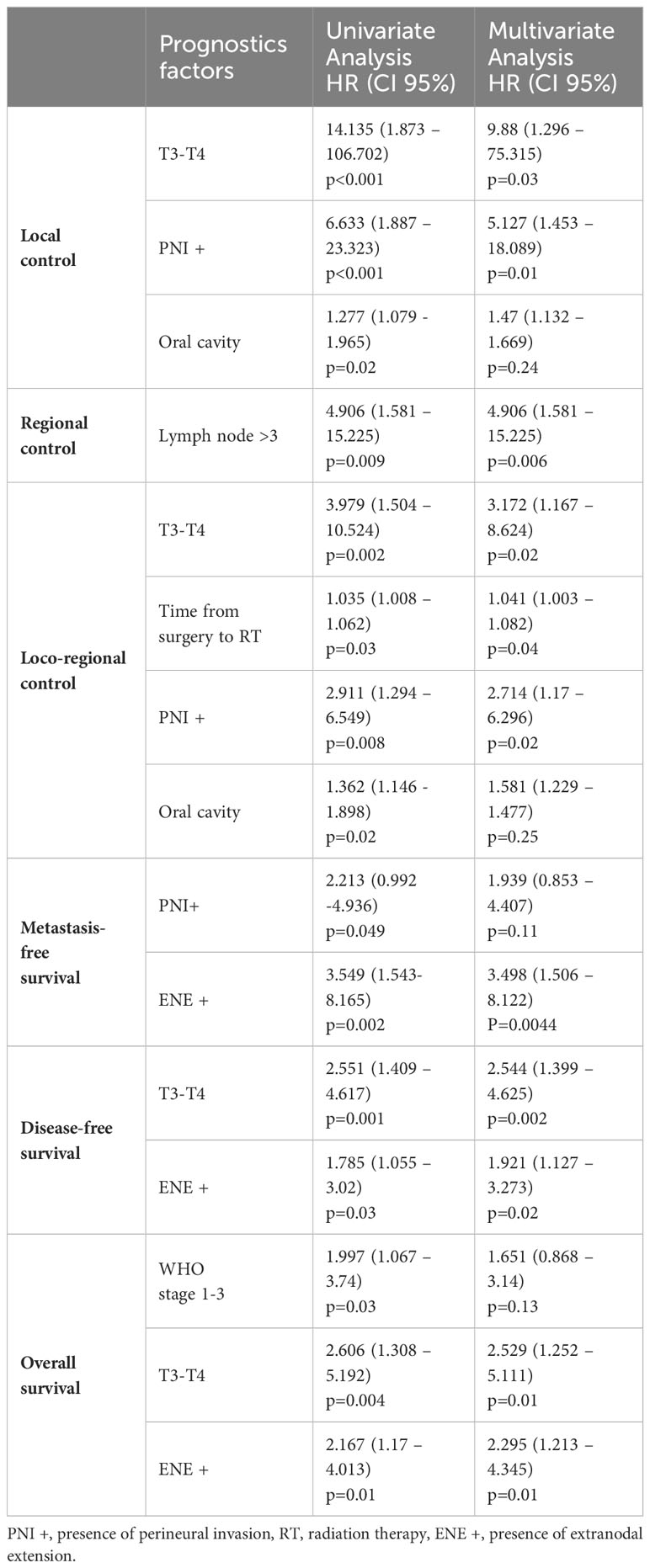
Table 2 Prognostic and predictive factors.
The 1 and 2-year local control rates were 93% and 90% respectively for the overall population. For oral cavity cancers, the 2-year local control rate was 85.1% vs 96.7% for oropharyngeal cancers (p=0.031). Higher tumor stages (T1-2 vs T3-4; p< 0.001) and presence of PNI (p<0.001) were predictive factors for poorer local control in univariate and multivariate analysis (p=0.03 and p=0.01 respectively) (Table 3).
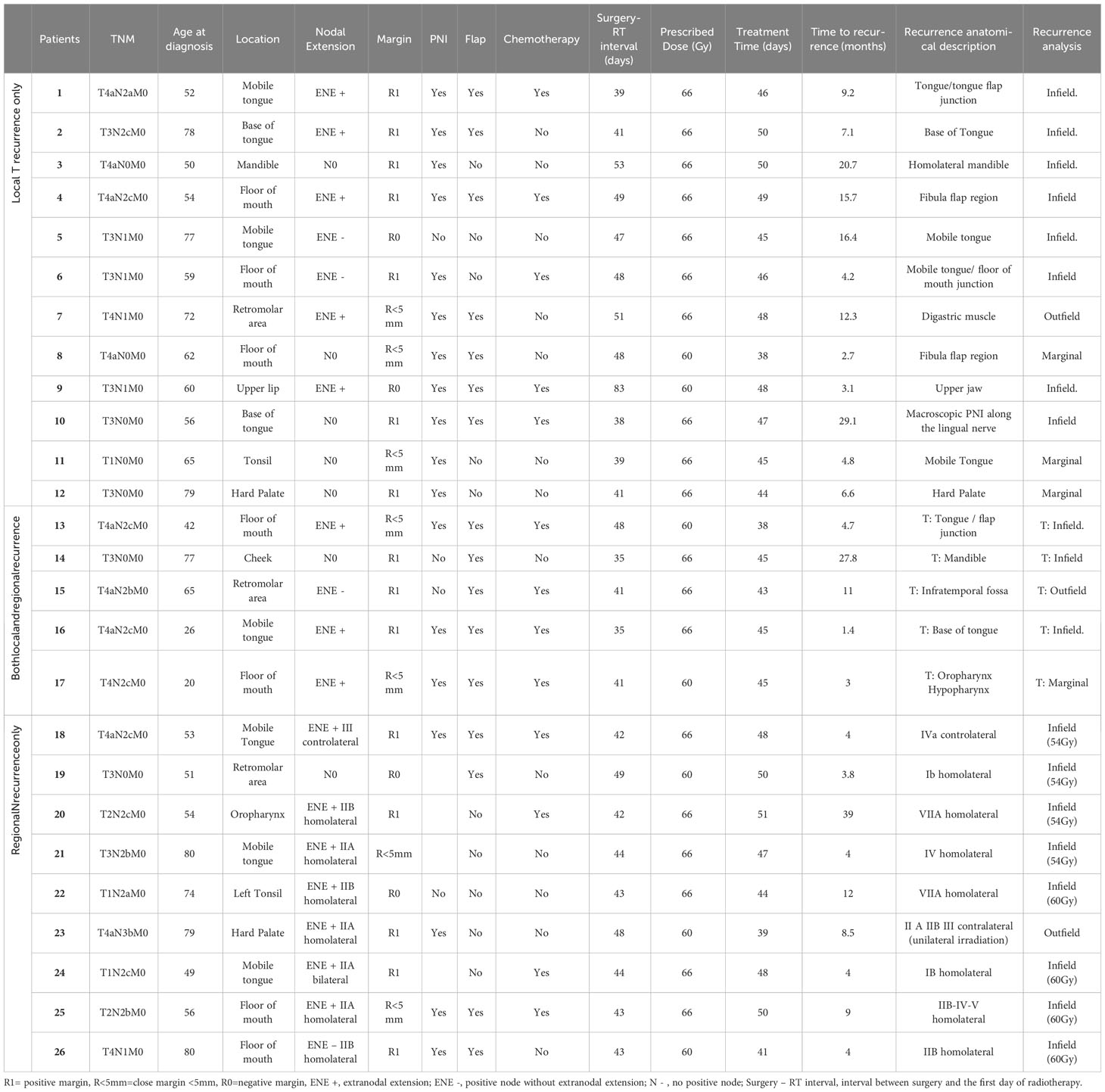
Table 3 Initial characteristics and analysis of the patients who developed a local and/or regional recurrence.
The 1 and 2-year regional control rates were 93.1%. A number of lymph node over 3 was the only predictive factor for a poorer regional control in univariate and multivariate analysis (p=0.009 and p=0.006 respectively) (Table 3).
The 1- and 2-year loco-regional control rates were 88.6% and 85.6% respectively (Figure 1), with 85.3% and 80.1% among oral cavity cancer and 93.6% and 93.6% among oropharynx cancer (p=0.022). Higher tumor stages (T1-2 vs T3-4; p=0.002), presence of PNI (p=0.008) and time from surgery to initiation of VMAT (p=0.03) were predictive factors for poorer loco-regional control in univariate and multivariate analysis respectively (p=0.02, p=0.04, and p=0.02 respectively; Table 3; Figure 1).
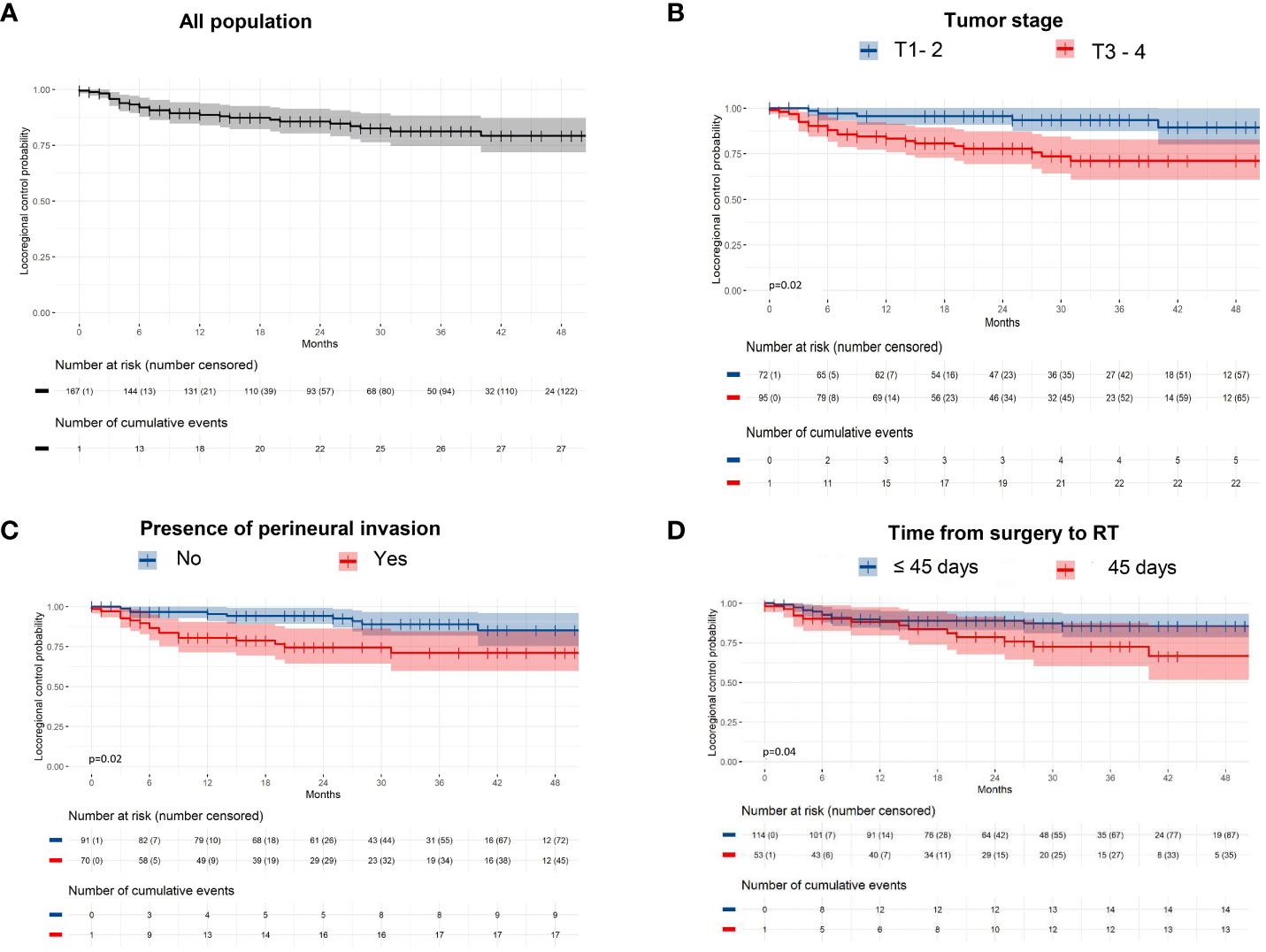
Figure 1 Loco-regional control among (A) the entire population, and (B) according to tumor staging, (C) the presence of perineural invasion, and (D) Time from surgery to radiotherapy.
Local and regional patterns of recurrence
Seventeen patients (10%) developed a local recurrence and 13 patients (8%) a regional recurrence, of whom 5 patients had both a local and regional recurrence. The initial characteristics and patterns of recurrence are described in Table 2.
Concerning the 17 local recurrences, 11 (64%) were considered as infield, 4 (24%) as marginal, and 2 (12%) as outfield. Concerning the 9 regional recurrences only, 8 (89%) were considered as infield, and 1 (11%) as outfield.
Metastasis
During follow-up, there were 26 metastatic events (15.6%) with a 2-year metastasis-free survival probability of 84.5% (Figure 2). Ten patients treated for an oropharyngeal cancer (2-year probability of metastasis-free survival = 85.9%) and 16 patients treated for an oral cavity tumor (2-year probability of metastasis-free survival = 83.3%) developed secondary localizations (bone, lung, cutaneous and liver) with no difference according to the initial tumor location (p=0.74). In univariate analysis, PNI and ENE were associated with poorer metastasis free survival (p=0.049, p=0.002). In multivariate analysis, only ENE remained significant (p=0.004; Table 3; Figure 2).
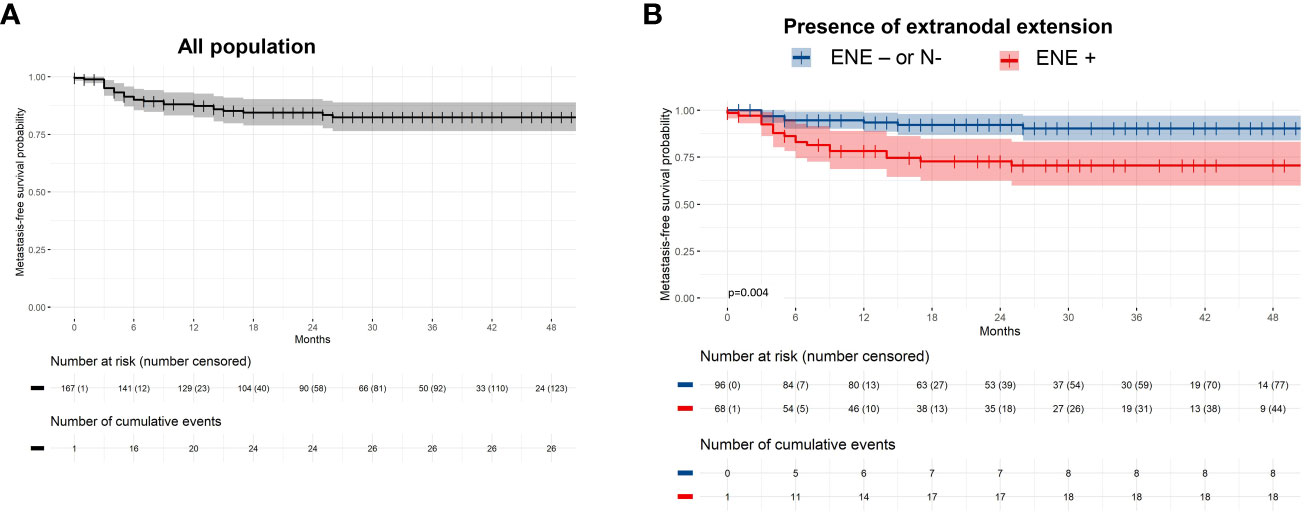
Figure 2 Metastasis-free survival among (A) the entire population, and (B) according to the presence of extranodal extension.
Survival
The 1- and 2-year disease-free survival (DFS) rates were 78.9% and 71.8% respectively (Figure 3). Higher tumor stages (T1-2 vs T3-4; p= 0.001) and presence of ENE (p=0.03) were unfavorable prognostic factors for DFS in univariate and multivariate analysis (p=0.002 and p=0.02 respectively; Table 3; Figure 3).
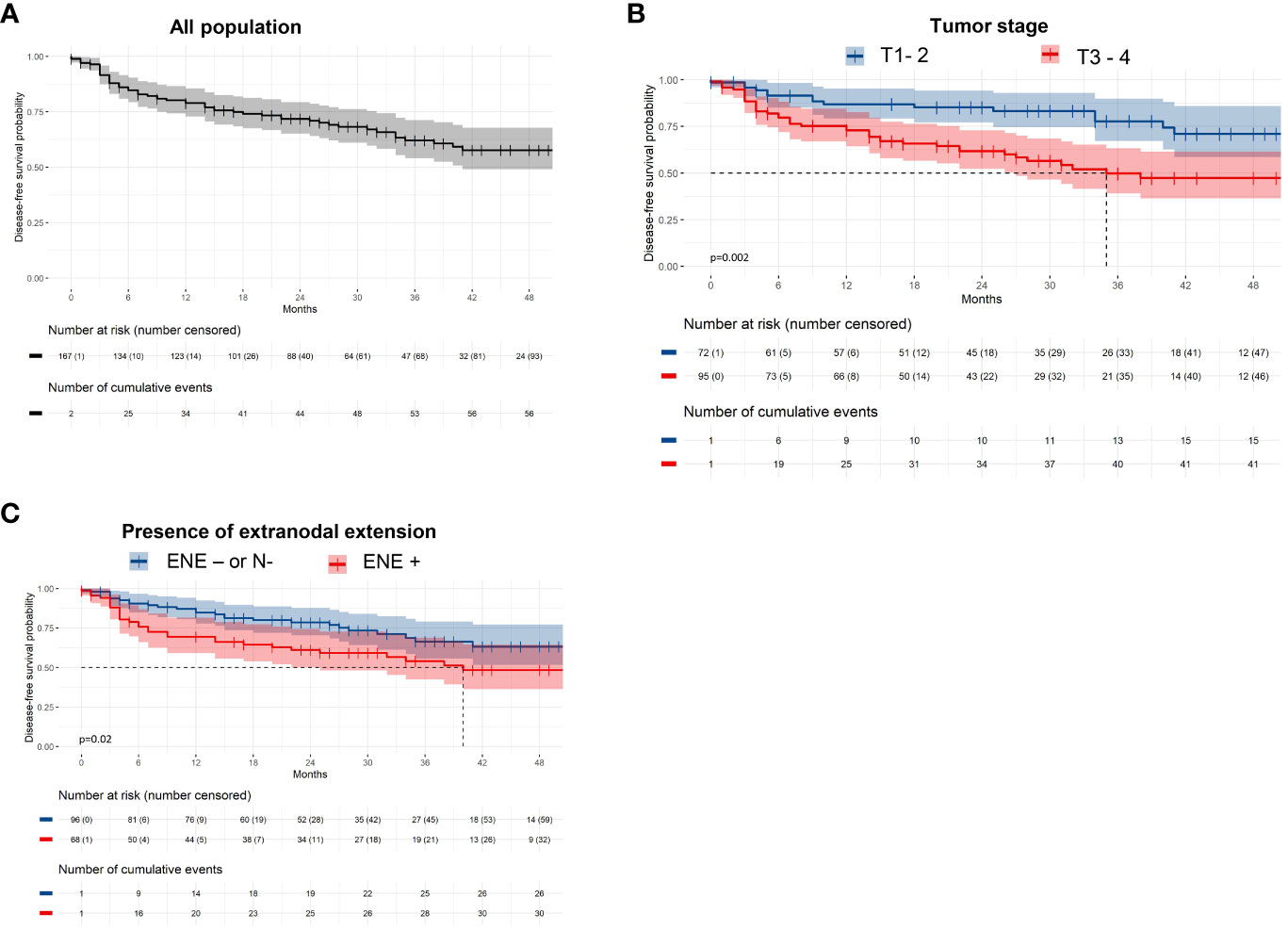
Figure 3 Disease-free survival among (A) the entire population, and (B) according to tumor staging, and (C) the presence of extranodal extension.
Forty-two patients (25%) died during follow-up. The 1- and 2-year overall survival (OS) rates were 88.6% and 80% respectively (Figure 4). In univariate analysis, WHO stage ≥1 (p = 0.03), presence of ENE (p = 0.01) and T3-T4 tumors (p=0.004) were unfavorable prognostic factors for OS. In multivariate analysis, the presence of ENE and T3-T4 tumors were independent unfavorable prognostic factors for OS (p=0.01 and p=0.01 respectively; Table 3; Figure 4).
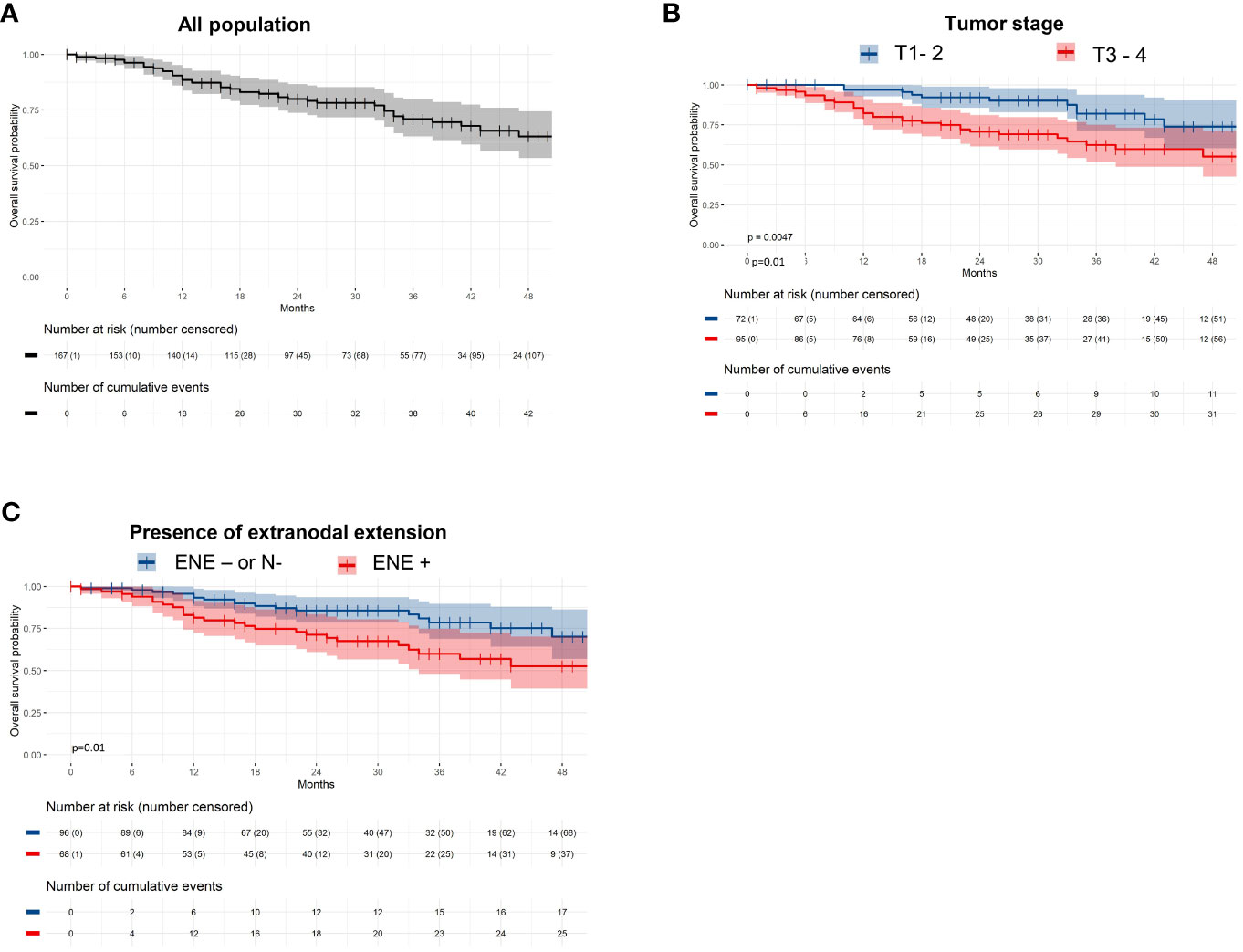
Figure 4 Overall survival among (A) the entire population, and (B) according to tumor staging, and (C) the presence of extranodal extension.
Discussion
IMRT/VMAT has been increasingly used over the last two decades for the treatment of head and neck cancers, and is today the gold standard technique in radiation therapy for these cancers. However, the data regarding the outcomes associated with IMRT/VMAT in the post-operative setting for oral cavity and oropharyngeal cancers is very limited (24–31). Thus our series, despite its relatively small number of patients (n=167), is one of the largest reported to date. The outcomes reported in our series are in line with those reported in the literature (25, 26, 29, 31–34) (Table 4). We found that postoperative VMAT reached high rates of local and loco-regional control. We found that the presence of ENE, despite present-day radiochemotherapy techniques, remains a major issue.
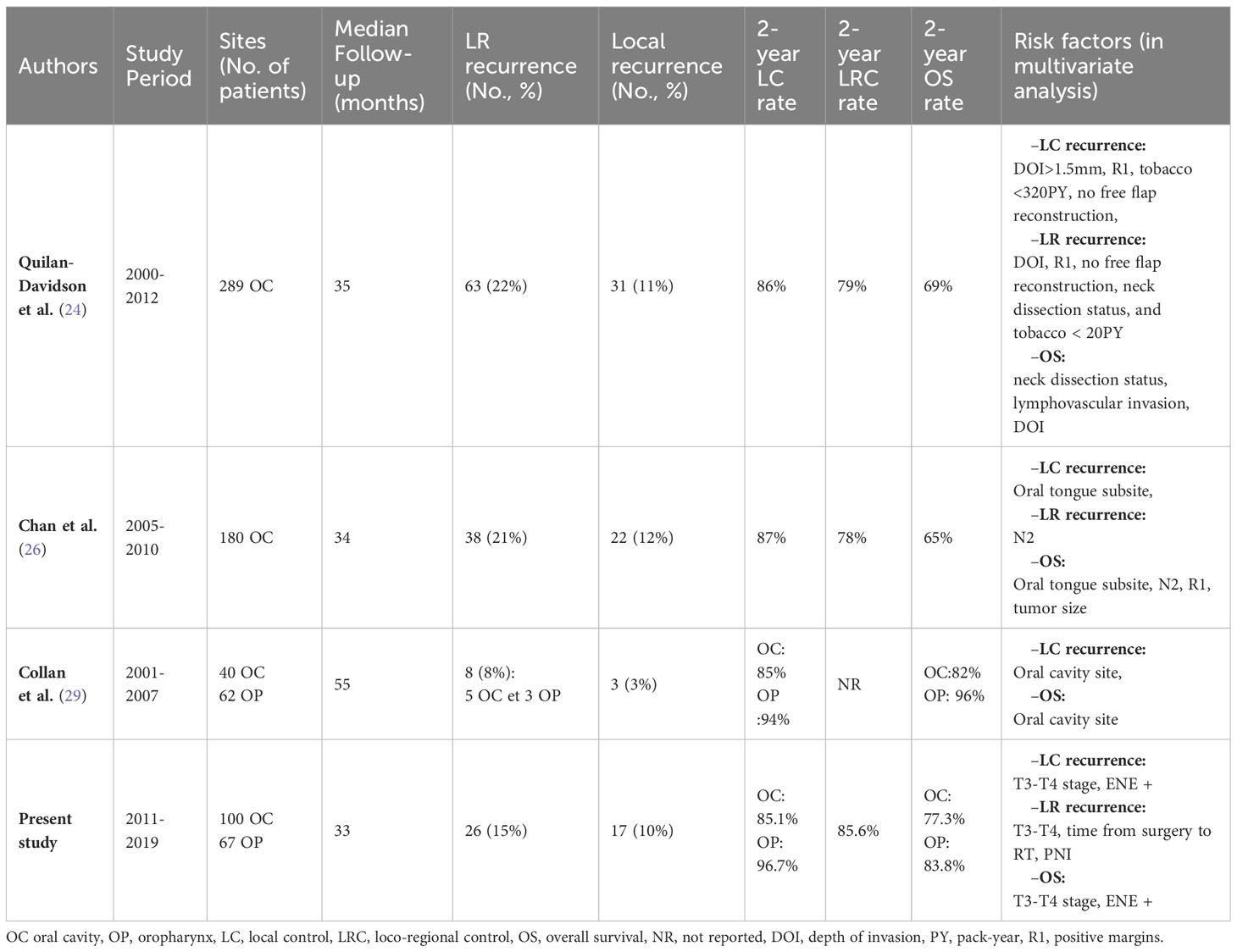
Table 4 Outcomes in previous reports concerning post-operative IMRT in oral cavity and oropharynx SCC.
There are a few limitations to our study that need to be highlighted. Potential biases, inherent in any retrospective analysis, could have affected the results of this study. Because of the retrospective nature of the study, certain data missing in the medical files could not be assessed for all patients. For example, the depth of invasion for oral cavity cancers was often missing, not allowing to use the latest UICC classification. The same issue was faced regarding HPV status, which was not available for all patients, particularly those treated the earliest in the cohort. We also found that the collection of all toxicities were not robust enough to allow good quality interpretation of the data, so we only focused on the oncological outcomes. This series was also single-center. However, all patients were treated in the same institution with surgery and post-operative radiotherapy in fairly homogeneous manner for both dose prescription and delineation.
Concerning local recurrences, during follow-up only 17 patients (10%) developed a local recurrence with actuarial 1 and 2-year local control rates of 93% and 90% respectively. The vast majority of these local recurrences were found to be infield. Higher tumor stages and presence of PNI were the only predictive factors in multivariate analysis for poorer local control. R1 margins were not found to be predictive factors for local control. This is in line with various recent reports that have also found that R1 margins were no longer a factor of poorer local control since the emergence of radiochemotherapy (24, 27, 29, 35). It seems that the negative impact of R1 margins has been fully negated by using higher radiotherapy doses (usually 66Gy) and radiochemotherapy. However, this does not seem to be the case for ENE. Indeed, in our series, the presence of ENE was found to be a prognostic factor for poorer DFS, metastasis-free survival, and OS. A recent series of 439 patients with head and neck SCC (all localizations) treated with postoperative radiotherapy also reported the negative prognostic value of ENE despite the use of radiochemotherapy (35). This finding highlights the need to find new strategies for patients with ENE treated with postoperative radiochemotherapy, as in the ongoing NIVOPOSTOP trial testing the addition of Nivolumab to standard cisplatin-based chemo-radiation (NCT03576417).
We also found that oral cavity cancers generally had poorer outcomes than oropharyngeal cancers, with 2-year LC rates of 85.1% vs 96.7% (p=0.031), and 2-year OS rates of 77.3% vs 83.8% (non-significant, probably due to a lack of statistical power). This is in line with previously reported series (25, 29, 36).
Regarding chemotherapy, 72 patients (43%) were treated with radiotherapy combined with chemotherapy. The local control and OS rates for these high-risk patients were similar to those for patients with a lower risk of recurrence, treated without concomitant chemotherapy. It is possible that without concomitant chemotherapy the outcome among high-risk patients would have been worse (29). The total number of failures in this series is however too small to enable any robust calculations between subgroups.
Conclusion
Our outcomes for postoperative VMAT for oral cavity and oropharyngeal cancers are very encouraging, with high rates of loco-regional control (85.6% at 2 years). However, the management of ENE still seems challenging, as these events were identified as highly unfavorable prognostic factors.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study was approved by CECIC Rhône-Alpes-Auvergne. All patients were informed and were free to oppose their participation in this study. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because All patients were informed and were free to oppose their participation in this study.
Author contributions
JB: Conceptualization, Methodology, Supervision, Writing – original draft, Writing – review & editing. CM: Conceptualization, Investigation, Methodology, Writing – original draft. MC: Conceptualization, Methodology, Writing – review & editing. JMo: Data curation, Methodology, Writing – review & editing. JMi: Data curation, Methodology, Writing – review & editing. IM: Conceptualization, Formal Analysis, Methodology, Writing – review & editing. EC: Conceptualization, Formal Analysis, Methodology, Writing – review & editing. MB: Investigation, Methodology, Writing – review & editing. MK: Investigation, Methodology, Writing – review & editing. NS: Investigation, Methodology, Writing – review & editing. NP-D: Investigation, Methodology, Writing – review & editing. FM: Investigation, Methodology, Writing – review & editing. ML: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
CTV, clinical target volume; DFS, disease-free survival; ENE, extranodal extension; IMRT, intensity modulated radiation therapy; OS, overall survival; PNI, peri-neural invasion; PTV, planning target volume; SCC, squamous cell carcinoma; SIB, simultaneous integrated boost; VMAT, volumetric modulated Arctherapy.
References
1. Schmults CD, Blitzblau R, Aasi SZ, Alam M, Andersen JS, Baumann BC, et al. NCCN guidelines® Insights: squamous cell skin cancer, version 1.2022: featured updates to the NCCN guidelines. J Natl Compr Cancer Network (2021) 19:1382–94. doi: 10.6004/jnccn.2021.0059
2. Koyfman SA, Ismaila N, Crook D, D’Cruz A, Rodriguez CP, Sher DJ, et al. Management of the neck in squamous cell carcinoma of the oral cavity and oropharynx: ASCO clinical practice guideline. J Clin Oncol (2019) 37:1753–74. doi: 10.1200/JCO.18.01921
3. Toledano I, Graff P, Serre A, Boisselier P, Bensadoun R-J, Ortholan C, et al. Intensity-modulated radiotherapy in head and neck cancer: results of the prospective study GORTEC 2004–03. Radiother Oncol (2012) 103:57–62. doi: 10.1016/j.radonc.2011.12.010
4. Eisbruch A, Marsh LH, Dawson LA, Bradford CR, Teknos TN, Chepeha DB, et al. Recurrences near base of skull after IMRT for head-and-neck cancer: implications for target delineation in high neck and for parotid gland sparing. Int J Radiat Oncol Biol Phys (2004) 59:28–42. doi: 10.1016/j.ijrobp.2003.10.032
5. Chen AM, Farwell DG, Luu Q, Chen LM, Vijayakumar S, Purdy JA. Marginal misses after postoperative intensity-modulated radiotherapy for head and neck cancer. Int J Radiat Oncol Biol Phys (2011) 80:1423–9. doi: 10.1016/j.ijrobp.2010.04.011
6. Lee N, Xia P, Fischbein NJ, Akazawa P, Akazawa C, Quivey JM. Intensity-modulated radiation therapy for head-and-neck cancer: The UCSF experience focusing on target volume delineation. Int J Radiat Oncol Biol Phys (2003) 57:49–60. doi: 10.1016/S0360-3016(03)00405-X
7. Peters LJ, O’Sullivan B, Giralt J, Fitzgerald TJ, Trotti A, Bernier J, et al. Critical impact of radiotherapy protocol compliance and quality in the treatment of advanced head and neck cancer: results from TROG 02.02. JCO (2010) 28:2996–3001. doi: 10.1200/JCO.2009.27.4498
8. Bekelman JE, Wolden S, Lee N. Head-and-neck target delineation among radiation oncology residents after a teaching intervention: A prospective, blinded pilot study. Int J Radiat Oncol Biol Phys (2009) 73:416–23. doi: 10.1016/j.ijrobp.2008.04.028
9. Hong TS, Tomé WA, Harari PM. Heterogeneity in head and neck IMRT target design and clinical practice. Radiother Oncol (2012) 103:92–8. doi: 10.1016/j.radonc.2012.02.010
10. Bernier J, Domenge C, Ozsahin M, Matuszewska K, Lefèbvre J-L, Greiner RH, et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med (2004) 350:1945–52. doi: 10.1056/NEJMoa032641
11. Bernier J, Cooper JS, Pajak TF, Van Glabbeke M, Bourhis J, Forastiere A, et al. Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (# 22931) and RTOG (# 9501). Head Neck: J Sci Specialties Head Neck (2005) 27:843–50. doi: 10.1002/hed.20279
12. Grégoire V, Ang K, Budach W, Grau C, Hamoir M, Langendijk JA, et al. Delineation of the neck node levels for head and neck tumors: a 2013 update. DAHANCA, EORTC, HKNPCSG, NCIC CTG, NCRI, RTOG, TROG consensus guidelines. Radiother Oncol (2014) 110:172–81. doi: 10.1016/j.radonc.2013.10.010
13. Lapeyre M, Miroir J, Biau J. Delineation of the lymph nodes for head neck cancers. Cancer Radiotherapie: J la Societe Francaise Radiotherapie Oncologique (2014) 18:572–6. doi: 10.1016/j.canrad.2014.06.013
14. Lapeyre M, Henrot P, Alfonsi M, Bardet E, Bensadoun RJ, Dolivet G, et al. Propositions for the selection and the delineation of peritumoral microscopic disease volumes in oral cavity and oropharyngeal cancers (lymph nodes excluded). Cancer Radiotherapie: J la Societe Francaise Radiotherapie Oncologique (2005) 9:261–70. doi: 10.1016/j.canrad.2005.03.005
15. Lapeyre M, Loos G, Biau J. Delineation for oral cavity and oropharyngeal cancers. Cancer Radiotherapie: J la Societe Francaise Radiotherapie Oncologique (2013) 17:493–7. doi: 10.1016/j.canrad.2013.05.007
16. Lapeyre M, Biau J, Racadot S, Moreira JF, Berger L, Peiffert D. Radiotherapy for oral cavity cancers. Cancer Radiother (2016) 20 Suppl:S116–125. doi: 10.1016/j.canrad.2016.07.002
17. Brouwer CL, Steenbakkers RJ, Bourhis J, Budach W, Grau C, Grégoire V, et al. CT-based delineation of organs at risk in the head and neck region: DAHANCA, EORTC, GORTEC, HKNPCSG, NCIC CTG, NCRI, NRG Oncology and TROG consensus guidelines. Radiother Oncol (2015) 117:83–90. doi: 10.1016/j.radonc.2015.07.041
18. Grégoire V, Mackie TR. State of the art on dose prescription, reporting and recording in Intensity-Modulated Radiation Therapy (ICRU report No. 83). Cancer/Radiothérapie (2011) 15:555–9. doi: 10.1016/j.canrad.2011.04.003
19. Cooper JS, Pajak TF, Forastiere AA, Jacobs J, Campbell BH, Saxman SB, et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med (2004) 350:1937–44. doi: 10.1056/NEJMoa032646
20. Mohamed AS, Rosenthal DI, Awan MJ, Garden AS, Kocak-Uzel E, Belal AM, et al. Methodology for analysis and reporting patterns of failure in the Era of IMRT: head and neck cancer applications. Radiat Oncol (2016) 11:95. doi: 10.1186/s13014-016-0678-7
21. Mohamed AS, Awan M, Kocak E, Beadle BM, Kantor ME, Gunn GB, et al. Methods for analysis and reporting the patterns of Locoregional failure in the era of IMRT for head and neck cancer: deformable image registration–based quality assurance workflow. Int J Radiat Oncol Biol Phys (2014) 90:S569–70. doi: 10.1016/j.ijrobp.2014.05.1719
22. Due AK, Korreman S, Bentzen SM, Tomé W, Bender E, Aznar M, et al. Methodologies for localizing loco-regional hypopharyngeal carcinoma recurrences in relation to FDG-PET positive and clinical radiation therapy target volumes. Acta Oncol (2010) 49:984–90. doi: 10.3109/0284186X.2010.498833
23. Due AK, Vogelius IR, Aznar MC, Bentzen SM, Berthelsen AK, Korreman SS, et al. Methods for estimating the site of origin of locoregional recurrence in head and neck squamous cell carcinoma. Strahlenther Onkol (2012) 188:671–6. doi: 10.1007/s00066-012-0127-y
24. Quinlan-Davidson SR, Mohamed ASR, Myers JN, Gunn GB, Johnson FM, Skinner H, et al. Outcomes of oral cavity cancer patients treated with surgery followed by postoperative intensity modulated radiation therapy. Oral Oncol (2017) 72:90–7. doi: 10.1016/j.oraloncology.2017.07.002
25. Daly ME, Le Q-T, Kozak MM, Maxim PG, Murphy JD, Hsu A, et al. Intensity-modulated radiotherapy for oral cavity squamous cell carcinoma: patterns of failure and predictors of local control. Int J Radiat Oncol Biol Phys (2011) 80:1412–22. doi: 10.1016/j.ijrobp.2010.04.031
26. Chan AK, Huang SH, Le LW, Yu E, Dawson LA, Kim JJ, et al. Postoperative intensity-modulated radiotherapy following surgery for oral cavity squamous cell carcinoma: patterns of failure. Oral Oncol (2013) 49:255–60. doi: 10.1016/j.oraloncology.2012.09.006
27. Cho Y, Yoon HI, Lee IJ, Kim JW, Lee CG, Choi EC, et al. Patterns of local recurrence after curative resection and reconstruction for oropharyngeal and oral cancers: Implications for postoperative radiotherapy target volumes. Head Neck (2019) 41:3916–23. doi: 10.1002/hed.25928
28. Ooishi M, Motegi A, Kawashima M, Arahira S, Zenda S, Nakamura N, et al. Patterns of failure after postoperative intensity-modulated radiotherapy for locally advanced and recurrent head and neck cancer. Japanese J Clin Oncol (2016) 46:919–27. doi: 10.1093/jjco/hyw095
29. Collan J, Lundberg M, Vaalavirta L, Bäck L, Kajanti M, Mäkitie A, et al. Patterns of relapse following surgery and postoperative intensity modulated radiotherapy for oral and oropharyngeal cancer. Acta Oncol (2011) 50:1119–25. doi: 10.3109/0284186X.2010.549839
30. Chao KSC, Ozyigit G, Tran BN, Cengiz M, Dempsey JF, Low DA. Patterns of failure in patients receiving definitive and postoperative IMRT for head-and-neck cancer. Int J Radiat Oncol Biol Phys (2003) 55:312–21. doi: 10.1016/S0360-3016(02)03940-8
31. Wang Z-H, Yan C, Zhang Z-Y, Zhang C-P, Hu H-S, Tu W-Y, et al. Outcomes and xerostomia after postoperative radiotherapy for oral and oropharyngeal carcinoma. Head Neck (2014) 36:1467–73. doi: 10.1002/hed.23488
32. Yao M, Chang K, Funk GF, Lu H, Tan H, Wacha J, et al. The failure patterns of oral cavity squamous cell carcinoma after intensity-modulated radiotherapy—the University of Iowa experience. Int J Radiat Oncol Biol Phys (2007) 67:1332–41. doi: 10.1016/j.ijrobp.2006.11.030
33. Geretschläger A, Bojaxhiu B, Crowe S, Arnold A, Manser P, Hallermann W, et al. Outcome and patterns of failure after postoperative intensity modulated radiotherapy for locally advanced or high-risk oral cavity squamous cell carcinoma. Radiat Oncol (2012) 7:175. doi: 10.1186/1748-717X-7-175
34. Hoffmann M, Saleh-Ebrahimi L, Zwicker F, Haering P, Schwahofer A, Debus J, et al. Long term results of postoperative Intensity-Modulated Radiation Therapy (IMRT) in the treatment of Squamous Cell Carcinoma (SCC) located in the oropharynx or oral cavity. Radiat Oncol (2015) 10:251. doi: 10.1186/s13014-015-0561-y
35. Gau M, Fonseca A, Ozsahin M, Fayette J, Poupart M, Roux P-E, et al. Prognostic impact of extranodal extension in resected head and neck squamous cell carcinomas in the era of postoperative chemoradiation: A retrospective monocentric study. Oral Oncol (2021) 123:105605. doi: 10.1016/j.oraloncology.2021.105605
Keywords: head and neck cancer, radiotherapy, post-operative, VMAT, recurrences
Citation: Mione C, Casile M, Moreau J, Miroir J, Molnar I, Chautard E, Bernadach M, Kossai M, Saroul N, Martin F, Pham-Dang N, Lapeyre M and Biau J (2023) Outcomes among oropharyngeal and oral cavity cancer patients treated with postoperative volumetric modulated arctherapy. Front. Oncol. 13:1272856. doi: 10.3389/fonc.2023.1272856
Received: 04 August 2023; Accepted: 12 October 2023;
Published: 31 October 2023.
Edited by:
Guopei Zhu, Shanghai Jiao Tong University, ChinaCopyright © 2023 Mione, Casile, Moreau, Miroir, Molnar, Chautard, Bernadach, Kossai, Saroul, Martin, Pham-Dang, Lapeyre and Biau. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julian Biau, anVsaWFuLmJpYXVAY2xlcm1vbnQudW5pY2FuY2VyLmZy
†These authors have contributed equally to this work