 Haoxiang Wu
Haoxiang Wu- Fudan University Shanghai Cancer Center, Shanghai, China
Undifferentiated carcinoma with osteoclast-like giant cells of the pancreas (UCOGCP) is a rare pancreatic tumor that accounts for less than 1% of all pancreatic malignancies. The characteristic pathological manifestation of UCOGCP is the presence of osteoclast-like giant cells (OGCs) distributed among pleomorphic undifferentiated tumor cells. UCOGCP can occur either alone or in association with other types of pancreatic tumors. At present, there is no unified consensus or guideline for the diagnosis and treatment of UCOGCP, and most of the literature are individual case reports. With the accumulation in the number of clinical cases and the development of precision medicine technology, the understanding of UCOGCP is also deepening. Researchers have begun to recognize that UCOGCP is a pancreatic tumor with distinctive clinical and molecular characteristics. In this review, we focus on the latest research status and future exploration directions in the diagnosis, treatment, and prognosis of UCOGCP.
Introduction
Pancreatic ductal adenocarcinoma (PDAC) is a malignancy associated with an overall 5-year survival rate of approximately 10% (1). There are several variants of PDAC based on histopathological characteristics. Among these variants, UCOGCP is a rare entity with unique clinical and pathological features. Tumors containing osteoclast-like giant cells occurring outside the bone are relatively rare. They are gradually being discovered in various parts of the body such as the pancreas, kidney, breast, and thyroid gland, with the pancreas being the most common site of occurrence. The primary pathologic characteristic is the presence of osteoclast-like giant cells within the tumor tissue which are morphologically similar to giant cell tumors of bone. UCOGCP is a rare non-endocrine malignant tumor of the pancreas and is easily confused with other types of pancreatic malignant tumors. The first description of this tumor was proposed by Sommers and Meissner in 1954 (2). Juan Rosai later notified that this tumor simulated giant cell tumors of bone in 1968 (3). According to the 4th edition of the WHO classification, undifferentiated carcinoma of pancreas (UCP) is divided into four types: anaplastic type, sarcomatoid type, carcinosarcoma, and undifferentiated carcinoma with osteoclast-like giant cell (4). UCP accounts for 2–7% of pancreatic malignant tumors (5, 6), while UCOGCP accounts for less than 1% of pancreatic malignant tumors (6–8). The 2019 WHO classification classified UCOGCP and UCP as independent subtypes of pancreatic ductal adenocarcinoma (9). More details about the 2019 WHO classification can be seen in Figure 1. Refined classification of pancreatic adenocarcinoma is important because the clinical course and outcome of each subtype differ significantly. PDAC and pancreatic neuroendocrine tumor (PNET) both have generally accepted management guidelines, but UCP does not. There are relatively few existing research articles on UCOGCP, most of which are retrospective case reports. So far, only slightly more than 100 global reports have been retrieved. The individual cases of UCOGCP published over the past five years are summarized in Table 1. Little is currently known about UCOGCP. The histogenesis and biology of this type of tumor has not yet been fully unraveled. This article aims to introduce the latest status and future prospects of diagnosis and treatment of UCOGCP.
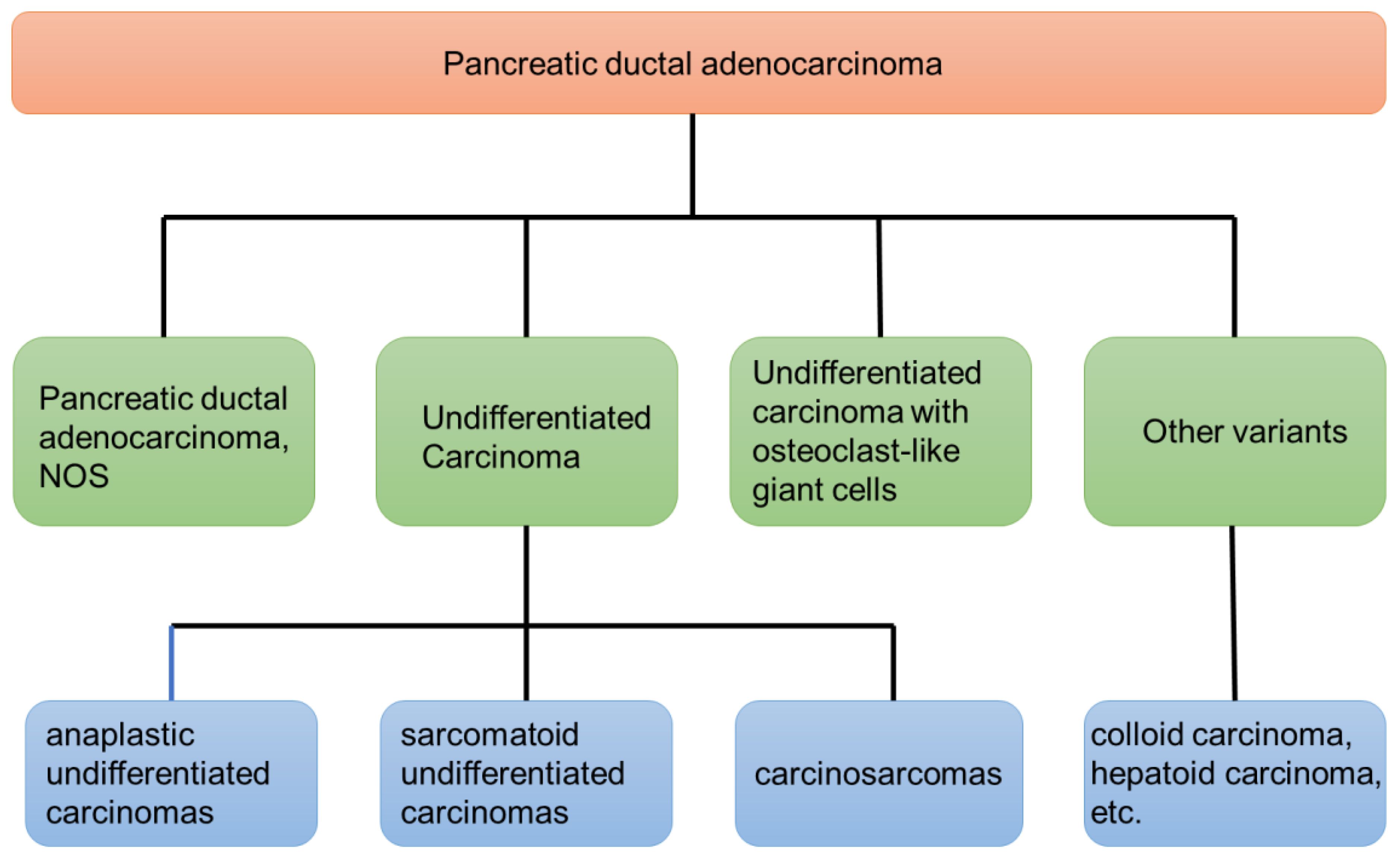
Figure 1 The latest WHO’s classification of pancreatic ductal adenocarcinoma (2019).
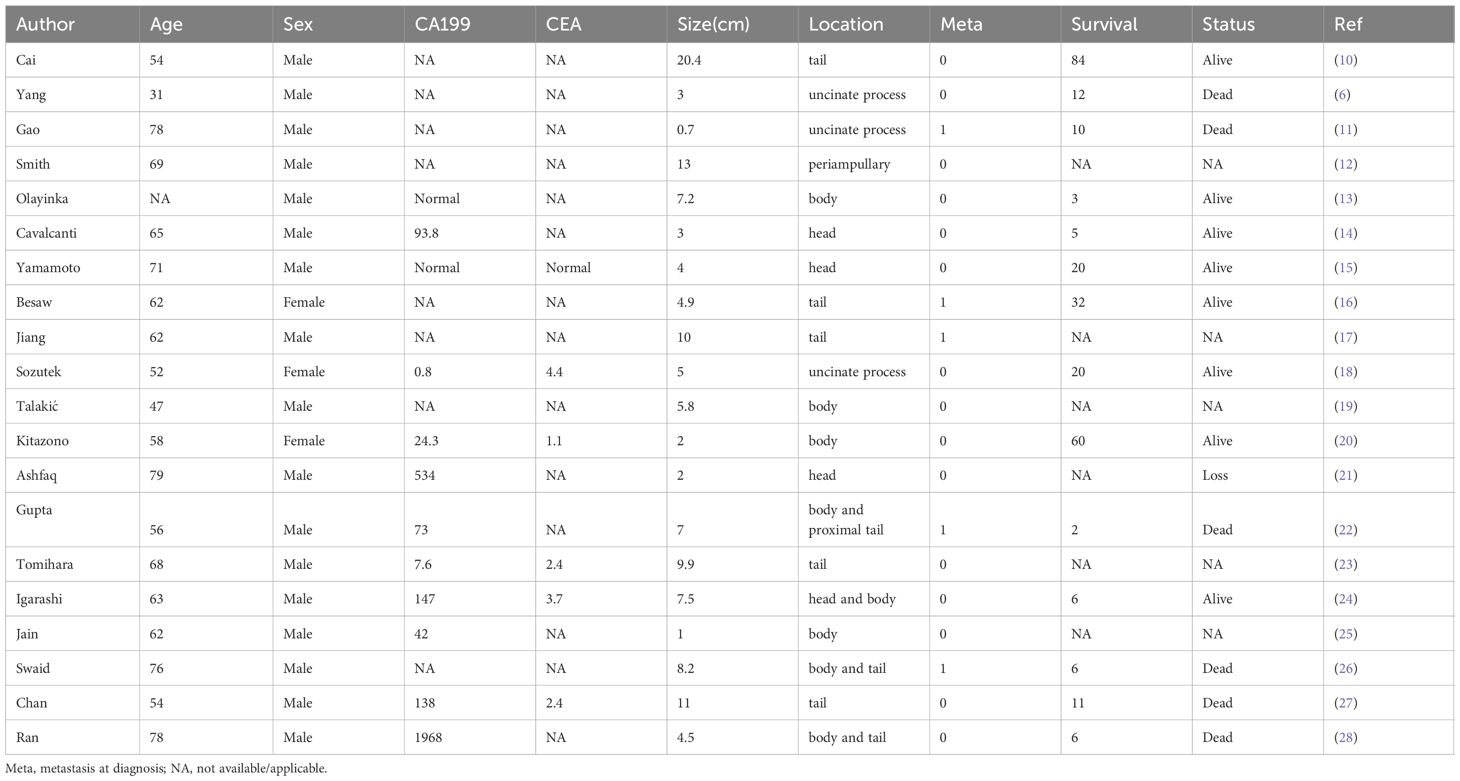
Table 1 Individual case reports on UCOGCP over the past five years.
Diagnosis
Clinical characteristics
UCOGCP has a wide age range of onset and is more commonly observed in middle-aged and elderly people (29). Most studies believe that there is no significant gender difference in the incidence of UCOGCP (5, 30), although some studies showed that it is slightly more common in women (14, 31, 32). In terms of clinical symptoms and signs, UCOGCP is similar to PDAC. Non-specific clinical presentations include abdominal pain, abdominal mass, jaundice, weight loss, etc. Among them, abdominal pain or abdominal discomfort is the most common (29). Some patients do not even have any clinical symptoms. Specific clinical symptoms are related to the location of the tumor and its size. In terms of tumor serological characteristics, tumor markers such as carcinoembryonic antigen (CEA) and CA19–9 are either not significantly elevated or fall within the normal reference range (33). Elevated CA19–9 levels in some UCOGCP patients may be associated with the presence of ductal adenocarcinoma components within the tumor. Some reports indicate an increase in neuron-specific enolase (NSE) levels in certain UCOGCP patients (30).
Imaging characteristics
In clinical practice, the diagnosis of UCOGCP mainly relies on histopathological examination of preoperative biopsies or postoperative specimen and there are no specific imaging findings. Preoperative abdominal ultrasound, contrast-enhanced CT, MRI and other imaging examinations can clearly delineate the size and location of the tumor, which complement each other and contribute to the clear diagnosis of malignant tumors. According to existing reports, UCOGCP mostly presents as cystic-based or mixed cystic-solid mass with delayed enhancement (13, 31, 34), and some cases are purely solid or purely cystic. The masses are frequently accompanied by necrosis and hemorrhage (35). The borders are mostly clear, and the surrounding invasion is not obvious. UCOGCP can occur in any part of the pancreas. Most tumors are located in the head of the pancreas (8, 34).Tumors located in the pancreatic head and neck can result in dilation of the pancreatic duct. It is noteworthy that tumor volume of UCOGCP is usually larger (8), with 80% larger than 5cm and 50% larger than 10cm (33). Analysis of the reasons may be related to the following aspects: (1) Tumors grow quickly; (2) Many tumors are located in the body and tail of the pancreas, with relatively low malignancy and late onset of clinical symptoms; (3) Tumor volume is often accompanied by bleeding which often leads to an increase in tumor size. Endoscopic ultrasound (EUS) is a great tool for the diagnosis of UCOGCP. In EUS examination, PDAC is uniformly hypoechoic, while UCOGCP has uneven echo (36). EUS-guided fine needle aspiration (FNA) and fine needle biopsy (FNB) are able to acquire tumor tissue and further help perform immunohistochemical analysis, which is the only method to diagnose UCOGCP before surgery (8). However, preoperative FNA will increase the incidence of postoperative complications and requires careful selection. Meanwhile EUS-guided FNA can sometimes give the wrong diagnosis. In Muraki’s study, of the 15 UCOGCP patients who underwent preoperative lesion biopsy, only 4 accurate diagnoses were achieved (32). PET-CT can provide useful information about the metabolic status of tumors and the presence of distant metastasis (37). The newer endoscopic ultrasound-guided fine-needle biopsy (EUS-FNB) combined with next-generation sequencing technology also facilitates related diagnosis (38, 39).
Pathological characteristics
UCOGCP is an aggressive non-endocrine tumor of pancreas with no glandular differentiation. Histopathological and immunohistochemical classification remains the gold standard for the diagnosis of UCOGCP. Microscopically, its cellular components are mainly composed of neoplastic mononuclear cells and numerous distinctive multinucleated giant cells. These giant cells resemble the giant cells of the bone which is why they are also called osteoclast-like giant cells. The multinucleated OGCs are considered non-neoplastic because they do not share the molecular aberrations of the neoplastic pleiomorphic mononuclear cells. It is often accompanied by massive hemorrhage and necrosis, which may affect the results of pathological diagnosis. OGCs usually have densely eosinophilic cytoplasm and multiple relatively uniform and bland nuclei clustering in the central aspect of the cell (32). Immunohistochemically, OGCs express CD68, does not express cytokeratin AE1/AE3, and has a very low Ki-67 proliferation index (14, 40). Pleomorphic tumor cells are positive for Vimentin, usually express markers of epithelial differentiation (cytokeratin, EMA), may have mutated p53 immuno-profile, and have a high Ki-67 proliferation index (41, 42). Most cases exhibit prominent intraductal/intracystic growth (32). The histogenesis of UCOGCP is still controversial. From the immunohistochemistry results, monocytes showed characteristics of epithelial origin, and OGCs showed characteristics of mesenchymal origin. Most current studies believe that it is of epithelial origin (7, 8). Most UCOGCP are accompanied by KRAS gene mutations, which also supports the origin of ductal epithelial cells (43, 44). There are also reports of lesions originating during epithelial-to-mesenchymal transition (EMT) (45). Through machine learning of gene expression patterns between UCOGCP samples and PDAC samples, it was found that OGCs originate from stem cell-like mesenchymal epithelial cells (SMEC) (46). UCOGCP can be accompanied by other epithelial tumors, PDAC is the most common, and 75% of cases can be accompanied by PDAC at the same time (8, 32). It can also be accompanied by mucinous cystic neoplasm (MCN), intraductal papillary mucinous neoplasm (IPMN) or malignant stromal tumors (15, 31, 47, 48). Table 2 shows literature reports on UCOGCP with mixed components. If no other distinct epithelial tumor components can be found, it’s called pure UCOGCP. Through analysis of the immunohistochemical expression of three well-known EMT markers, EMT activation was found more frequent in anaplastic carcinomas than in UCOGCP (58).
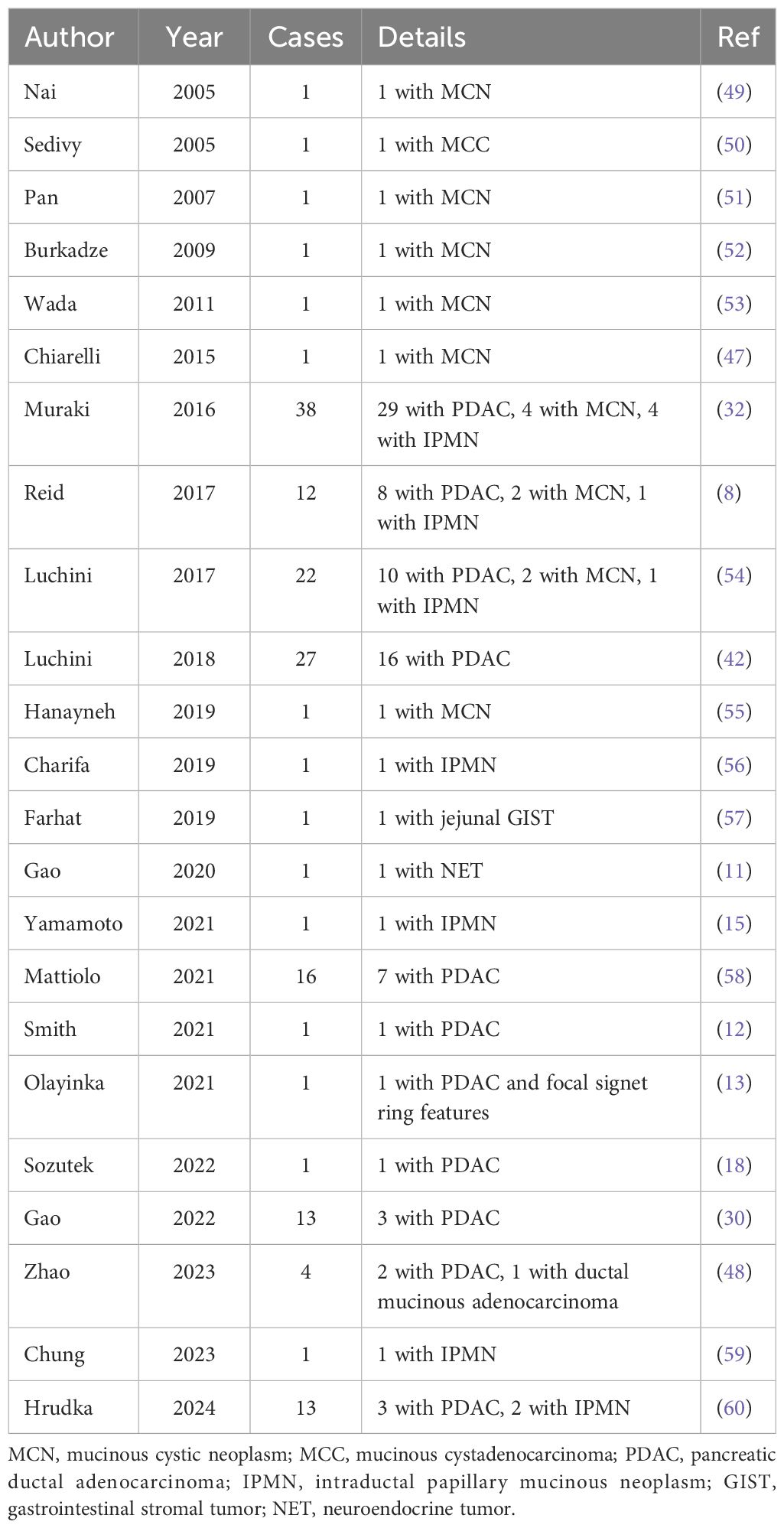
Table 2 Reports of UCOGCP associated with other types of tumors.
Genetic characteristics
Modern gene sequencing technologies such as next-generation sequencing (NGS) have been widely used. In addition to long-term follow-up, investigation of the genomic alterations in confirmed and surviving patients can also help guide the selection of treatment options and prognostic analysis. To better understand UCOGCP, many genetic features have been identified. The most frequently mentioned gene mutation of UCOGCP in literature reports is the KRAS gene (59, 61). Most KRAS mutations were found in codon 12, including the G12V, G12D and G12R mutations. KRAS is one of the most common oncogenes in human cancer. KRAS activation is an early event in the pathogenesis of pancreatic cancer. KRAS mutations are present in approximately ~85% of PDAC patients (62). Whole-exome sequencing (WES) of eight cases showed that UCOGCP has surprisingly similar molecular characteristics compared with conventional PDAC (54). In addition to the common KRAS oncogenic mutations, other typical mutated genes including TP53, CDKN2A and SMAD4 were found in UCOGCP, which further confirm that UCOGCP is a unique variant of PDAC. Mutations in SERPINA3, GLI3, MAGEB4, MEGF8 and TTN have also been detected. Some of them may act as pathogenic or likely pathogenic mutations. Zhao et al. detected 6 potentially clinically significant genes through NGS: AR, FBXW7, CCNE1, BTK, KRAS, TP53 (48). Somatic BRCA2 alterations were also detected by WES in one case (6). Recently, Hrudka et al. performed molecular genetic analysis of 13 UCOGCP cases with varying survival time (60). This is the largest NGS examined UCOGCP cohort to date. The results showed that the mutant spectrum of UCOGCP is very similar to that of PDAC. Unfortunately, UCOGCP-specific genomic signatures remain mainly unknown and no somatic genetic aberrations were found that were clearly related to patient prognosis or PD-L1 status. Gene characteristics of UCOGCP in literatures are summarized in Table 3. MicroRNAs (miRNAs) play a variety of important regulatory roles in both healthy and cancer cells. Popov et al. evaluated the expression of seven previously clinically significant miRNAs in UCOGCP and poorly differentiated (grade 3, G3) PDACs (65). Except for miR-155, there were no significant differences in the expression of other miRNAs in the two tumors.
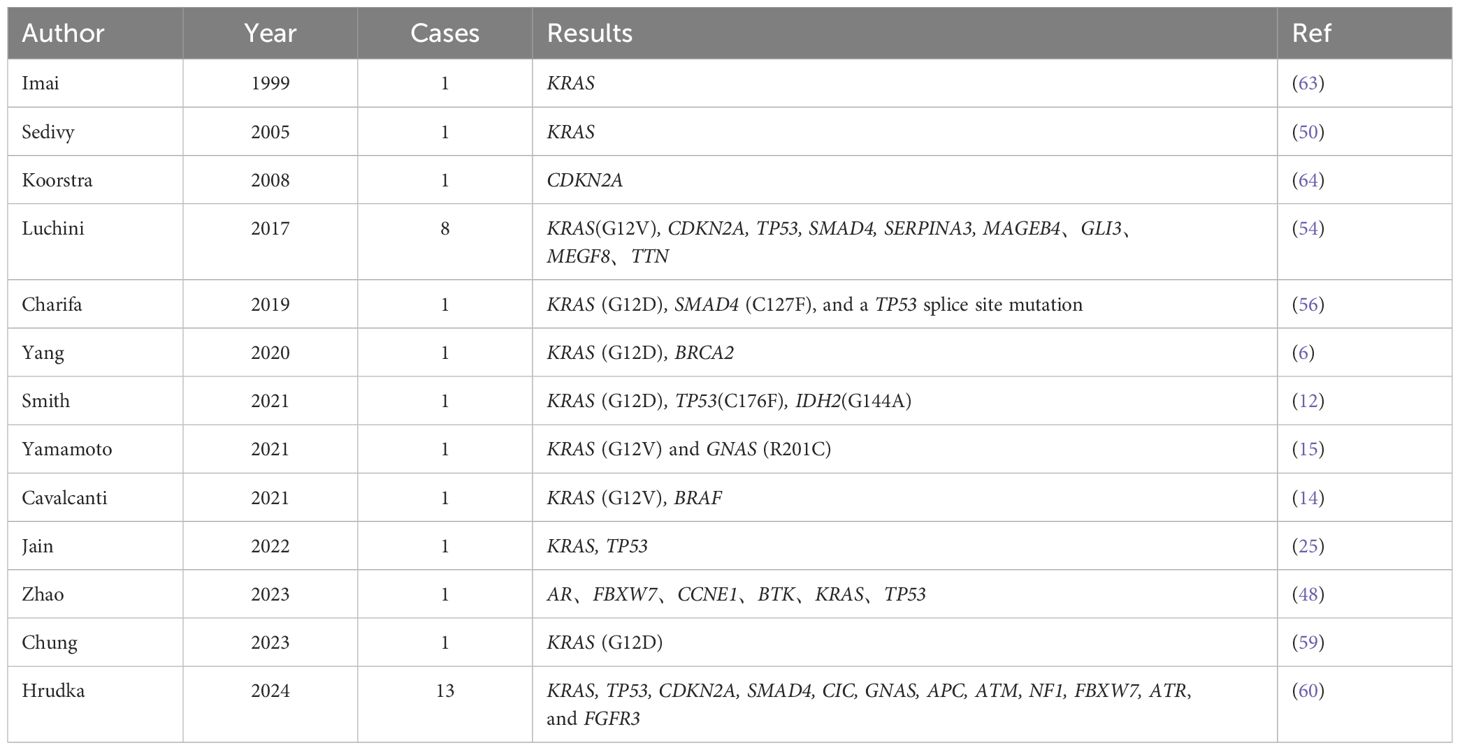
Table 3 Reports on UCOGCP gene characteristics.
Treatments
Surgery
Regarding UCOGCP, because its incidence is very low, most literatures are case reports, there are few randomized controlled studies of large cohorts, and there are no relevant guidelines for reference. Consequently, the clinical course of this disease remains poorly understood. Overall, radical surgical resection with negative margins (R0 resection) is the optimal treatment when surgical indications are met. The selection of surgical method and the scope of lymph node dissection can refer to PDAC, which mainly depends on the location of the tumor, regional lymph node involvement and intraoperative exploration. If nearby organs such as the stomach, jejunum, colon, and kidneys are invaded, they may need to be resected together. Because this type of tumor has large lesions and rich blood supply, careful preoperative imaging evaluation can help improve the complete resection rate and safety of surgery.
Chemotherapy
Pancreatic cancer is the most aggressive solid tumor in humans with a very poor prognosis. The treatment of pancreatic cancer is based on tumor histology. Because UCOGCP is so rare, the optimal treatment approach for this kind of tumor has not yet been determined. Several randomized clinical trials have confirmed that patients with PDAC at all stages need to receive chemotherapy. Since UCOGCP is a variant of pancreatic ductal adenocarcinoma, the common chemotherapy regimen for PDAC such as FOLFIRINOX(combination of oxaliplatin, irinotecan, fluorouracil and leucovorin) and gemcitabine can be often seen in case reports of UCOGCP. On the other hand, it has been reported in the literature that the comprehensive treatment strategy for UCOGCP can refer to undifferentiated pancreatic cancer. And a retrospective multicenter cohort study suggests that for patients with UCP, nab-paclitaxel-based combination chemotherapy may be more advantageous and significantly improved OS compared with non-paclitaxel-containing regimens (6.94 months vs. 3.75 months, respectively; P = 0.041) (66). For unresectable locally advanced or borderline resectable UCOGCP, there are reports in the literature that FOLFIRINOX regimen and modified FOLFIRINOX can be used for downstaging before surgery (18, 24). Neoadjuvant chemotherapy (NACT) can help reduce tumor size and alleviate local progression, thereby creating opportunities for R0 resection of the tumor without the need for resection of major blood vessels or adjacent organs. And it can also select patients with good tumor biological characteristics, who will benefit from curative resection surgery.
Immunotherapy
For PDAC, immunotherapy regimens have always had poor efficacy, while there are relatively few reports on the application of immunotherapy in UCOGCP. UCOGCP seems to exhibit high expression of universal programmed death ligand-1 (PD-L1), which may be used as an effective prognostic marker (41, 42, 67). PD-L1 expression was more frequent in UC compared with conventional PDAC (63% vs 15%, P < 0.01) (67). For UCOGCP, PD-L1 was expressed on tumor cells in 17 of 27 cases (63%) and was more often in patients associated with PDAC (42). Moreover, multivariate analysis confirmed that PD-L1 expression was associated with poor prognosis (HR = 3.397; 95% CI, 1.023–18.375; P = 0.034). The reason behind this may be that PD-L1 suppresses anti-tumor immunity and allows tumor cells to evade the cytotoxic activity of host T lymphocytes.
Another study including 13 UCOGC patients demonstrated similar conclusions (41). UCOGC expressed PD-L1 significantly more frequently and had greater numbers of CD3+ and CD8+ tumor-infiltrating lymphocytes (TILs) compared with PDAC. Among the 3 PD-L1 negative UCOGCP cases, none of them reached the death end point. The median survival time of PD-L1-positive patients was 5.7 months. However, due to the small cohort size, the comparison was not statistically significant. Immunotherapy may exert anti-tumor effects on UCOGCP with distant metastasis. Obayashi et al. (68) reported a UCOGCP patient with pancreatic body and tail tumors and lung metastases who achieved clinical complete remission of lung metastases after monotherapy with pembrolizumab monoclonal antibody. The patient achieved disease-free survival after subsequent resection of the pancreatic body and tail tumors. For a patient with unresectable UCOGCP with lung metastases, whose tumor mutation burden (TMB) was high as measured by NGS, he started to receive third-line pembrolizumab monotherapy after palliative radiotherapy. After 32 months of treatment, the primary tumor and metastases achieved sustained remission (16). So far, the effectiveness of immunotherapy in patients with UCOGCP still needs to be verified in large cohorts and more clinical trials.
Prognosis
Prognostic data with varying outcomes
Reports on UCOGCP are scarce and the terminology and classification of UCOGCP are not uniformly standardized. As a result, the prognostic data is fairly limited and vary greatly. Large survival differences may be related to tumor tissue heterogeneity and different tumor stages at diagnosis. Overall, UCOGCP is a highly aggressive tumor. UCOGCP lacks typical clinical symptoms and imaging features, and has poor tissue differentiation and strong invasiveness. UCOGCP is often diagnosed in the advanced stages with large tumor size, and many patients cannot get complete surgical resection. There is also a lack of effective therapeutic drugs. Even if it can be resected, early recurrences are also common. So the overall prognosis is poor. The opinion given in the WHO 2019 Digestive System Tumors Volume is that patients may survive for 1 year or more (9). The survival time of UCOGCP reported in most existing literature also shows similar or better results (30, 41, 69). Based on the data analysis of UCP patients in the National Cancer Database (NCDB), the median survival time of UCOGCP patients was 24.8 months and the estimate 3-year and 5-year survival rates were 42.54% and 39.01%, respectively (70). The difference in survival is also related to the stage of the tumor. By integrating previous literature reports, the median overall survival time of UCOGCP patients who underwent surgical resection was found to be 48 months (29). For unresectable UCOGCP patients with locally advanced tumors or distant metastasis, the prognosis is significantly worse and median survival time is less than 6 months (71, 72). Table 4 lists more detailed prognostic data of UCOGCP based on reported case series.
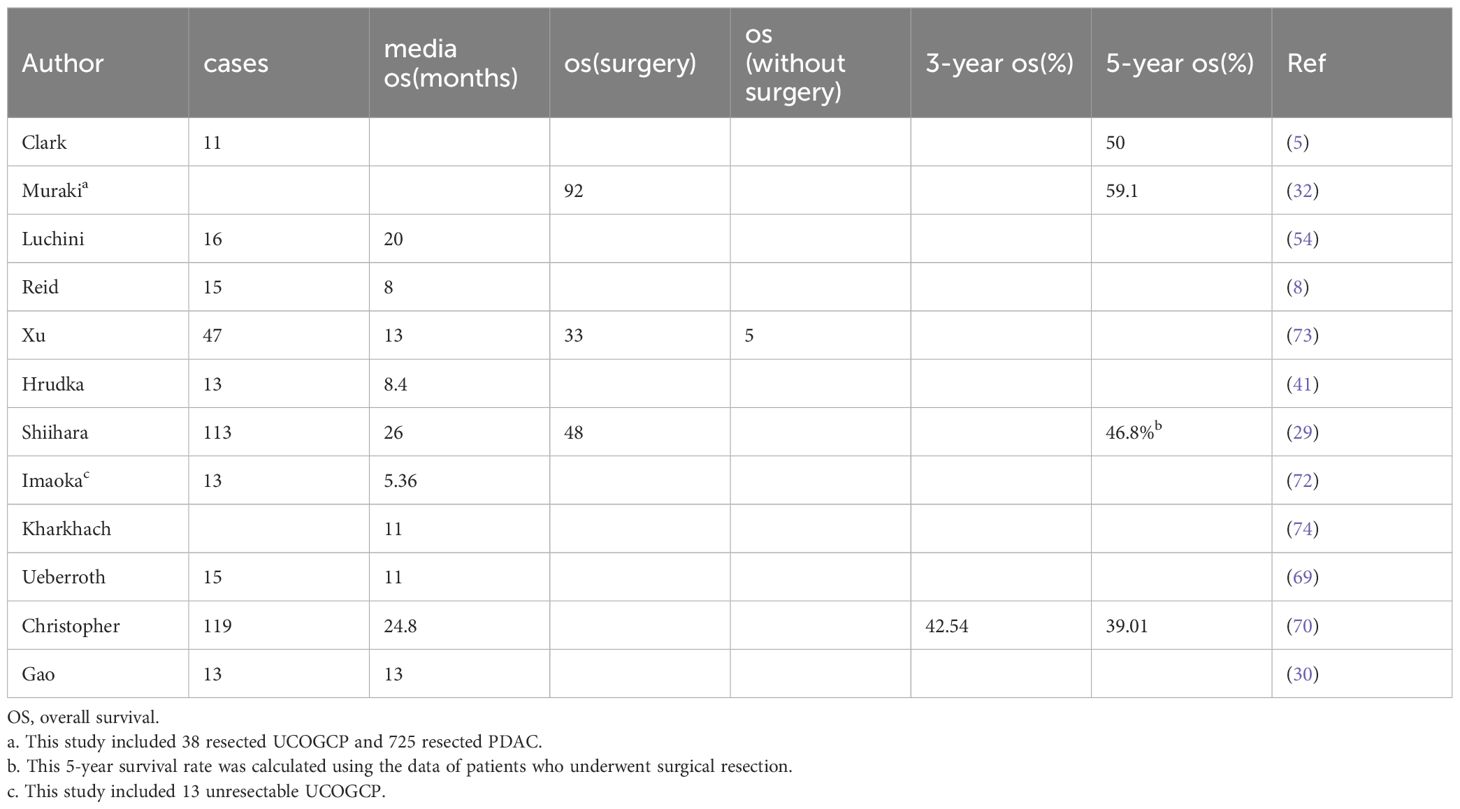
Table 4 Reports on UCOGCP survival data based on case series.
Pure UCOGCP seems to have a better prognosis
Pure UCP is highly malignant and has a poor prognosis. It is worth noting that UCOGCP is slightly less malignant than conventional PDAC and undifferentiated carcinoma without OGCs. In Strobel’s study, median survival for patients with anaplastic pancreatic cancer was 5.7 months, compared with 15.7 months for control patients with pancreatic ductal adenocarcinoma (75). The survival times of the three UCOGCP patients were even significantly longer, 33, 49, and 161 months respectively. The tumor resection rate of UCOGCP was also unexpectedly found to be higher than other types of UCP (29). In a recent large database review of UCP, patients with OGCs (UCOGCP) had longer median OS (aHR 0.52: 95% CI 0.41–0.67) compared with patients without OGCs (70). A proportion of UCOGCP patients in previous publications are still alive many years after diagnosis. A patient with locally advanced UCOGCP survived for even 10 years after undergoing surgery and adjuvant therapy (33). In one literature report, the patient’s survival time was even 15 years (76). Despite its rapid growth and large tumor size, the biological behavior of UCOGCP is different from that of common PDAC (77). Although UCOGCP grows rapidly, recent reports suggest that perineural invasion and lymph node metastasis are rare, and its prognosis is relatively better than that of PDAC and pleomorphic giant cell tumor (32, 78). According to Muraki’s study, the five-year survival rate of resected UCOGCP is 59.1%, while the five-year survival rate of resected PDAC is 15.7% (32). However, some research results showed that the prognosis of UCOGCP patients may be worse than that of PDAC patients, and there is a lack of effective large sample data to further clarify this issue (30).
However, some literature demonstrated different results. One retrospective study evaluated 55 patients with unresectable UCP. Final survival analysis showed that there is no significant difference in OS between the UC with OGCs group and the UC without OGCs group (72). Apart from tumor stages at diagnosis, the possible reasons behind may be related to the pathological components and the different roles of OGCs. More detailed pathological differences may have an impact on the prognosis of UCOGCP patients. As mentioned before, UCOGCP can be categorized into 2 distinct pathological subtypes: pure UCOGCP, and UCOGCP associated with other epithelial tumors. Patients with UCOGCP alone seem to survive longer than patients with UCOGCP accompanied by PDAC (30, 32, 54, 79). A meta-analysis using previous reported data showed that major prognostic factors of UCOGCP include age, sex, tumor size, lymph node metastasis, and concomitant PDAC component (79). However, concomitant MCN component did not affect prognosis.
Conclusions and future perspectives
UCOGCP is an extremely rare pancreatic malignant tumor with no specific clinical manifestations, imaging features and blood tumor markers. The diagnosis mainly relies on postoperative pathology examination. Currently, the underlying mechanism of UCOGCP’s distinctive morphological features remains incompletely understood. Additionally, prognostic information also needs to be further explored. In the future, a lot of further research work can be carried out to prolong the survival time of UCOGCP patients. In terms of clinical research, more cases and long term follow-up data can be collected to obtain more detailed information. At the same time, the level of early detection and diagnosis should be improved, and the treatment regimen should be unified and standardized. In terms of basic research, more latest technological means such as artificial intelligence and multi-omics can be used to explore the underlying pathogenesis and provide more precise and effective treatment strategies.
Author contributions
HW: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin. (2021) 71:7–33. doi: 10.3322/caac.21654
3. Rosai J. Carcinoma of pancreas simulating giant cell tumor of bone. Electron-microscopic evidence of its acinar cell origin. Cancer. (1968) 22:333–44. doi: 10.1002/(ISSN)1097-0142
4. Bosman FT, Carneiro F, Hruban RH, Theise ND. Who Classification of Tumours of the Digestive System. World Health Organization (2010).
5. Clark CJ, Graham RP, Arun JS, Harmsen WS, Reid-Lombardo KM. Clinical outcomes for anaplastic pancreatic cancer: A population-based study. J Am Coll Surg. (2012) 215:627–34. doi: 10.1016/j.jamcollsurg.2012.06.418
6. Yang G, Yin J, Ou K, Du Q, Ren W, Jin Y, et al. Undifferentiated carcinoma with osteoclast-like giant cells of the pancreas harboring kras and brca mutations: case report and whole exome sequencing analysis. BMC Gastroenterol. (2020) 20:202. doi: 10.1186/s12876–020-01351–7
7. Jo S. Huge undifferentiated carcinoma of the pancreas with osteoclast-like giant cells. World J Gastroenterol. (2014) 20:2725–30. doi: 10.3748/wjg.v20.i10.2725
8. Reid MD, Muraki T, HooKim K, Memis B, Graham RP, Allende D, et al. Cytologic features and clinical implications of undifferentiated carcinoma with osteoclastic giant cells of the pancreas: an analysis of 15 cases. Cancer Cytopathol. (2017) 125:563–75. doi: 10.1002/cncy.21859
9. Nagtegaal ID, Odze RD, Klimstra D, Paradis V, Rugge M, Schirmacher P, et al. The 2019 who classification of tumours of the digestive system. Histopathology. (2020) 76:182–8. doi: 10.1111/his.13975
10. Cai Y, Chen Y, Wu X, Yin Y, Cao L, Liu X. Seven-year disease-free survival in a patient with osteoclast-like giant cell-containing pancreatic undifferentiated carcinoma: A case report and literature review. Int J Clin Exp Pathol. (2020) 13:3200–5.
11. Gao G, Qorbani A, Zhou CH. A pancreatic mixed neuroendocrine-non-neuroendocrine neoplasms (Minen) (Net and undifferentiated carcinoma of the pancreas with osteoclast-like giant cells) with metastatic neuroendocrine component to the liver. Autops Case Rep. (2021) 11:e2020201. doi: 10.4322/acr.2020.201
12. Smith JL, Jacovides CL, Tucker CM, Jiang W, Prestipino AJ, Yeo CJ. Sequencing of an undifferentiated carcinoma with osteoclast-like giant cells of the pancreas: A case report. J Pancreat Cancer. (2021) 7:71–3. doi: 10.1089/pancan.2021.0004
13. Olayinka O, Kaur G, Gupta G. Undifferentiated pancreatic carcinoma with osteoclast-like giant cells and associated ductal adenocarcinoma with focal signet-ring features. Cureus. (2021) 13:e14988. doi: 10.7759/cureus.14988
14. Cavalcanti E, Schena N, Serino G, Lantone G, Armentano R. Assessment and management of undifferentiated carcinoma with osteoclastic like giant cells of the pancreas: A case report and revision of literature. BMC Gastroenterol. (2021) 21:247. doi: 10.1186/s12876–021-01779–5
15. Yamamoto S, Sakai Y. A case of undifferentiated carcinoma with osteoclast-like giant cells of the pancreas derived from an intraductal papillary mucinous neoplasm. Clin J Gastroenterol. (2021) 14:1263–8. doi: 10.1007/s12328–021-01415–5
16. Besaw RJ, Terra AR, Malvar GL, Chapman TR, Hertan LM, Schlechter BL. Durable response to pd-1 blockade in a patient with metastatic pancreatic undifferentiated carcinoma with osteoclast-like giant cells. J Natl Compr Canc Netw. (2021) 19:247–52. doi: 10.6004/jnccn.2021.7001
17. Jiang J, Luo J. Osteoclast-like giant cell undifferentiated carcinoma of the pancreas: A case report. Int J Clin Exp Pathol. (2021) 14:179–85.
18. Sozutek A, Aktas E. Borderline-resectable undifferentiated carcinoma with osteoclast-like giant cells of the pancreas: upfront surgery or neoadjuvant chemotherapy? J Coll Physicians Surg Pak. (2022) 32:934–7. doi: 10.29271/jcpsp.2022.07.934
19. Talakić E, Igrec J, Kaufmann-Bühler AK, Janek E, Stephan S, Schemmer P, et al. Undifferentiated carcinoma with osteoclast-like giant cells of the pancreas mimicking pancreatic pseudocyst. Hepatobiliary Pancreat Dis Int. (2022) 21:403–5. doi: 10.1016/j.hbpd.2022.06.011
20. Kitazono M, Fujita M, Ito A, Oyama T, Ikeda N, Eguchi M, et al. Case report of anaplastic carcinoma with osteoclast-like giant cells arising in the pancreatic body. J Surg Case Rep. (2022) 2022:rjac288. doi: 10.1093/jscr/rjac288
21. Ashfaq A, Thalambedu N, Atiq MU. A rare case of pancreatic cancer: undifferentiated carcinoma of the pancreas with osteoclast-like giant cells. Cureus. (2022) 14:e25118. doi: 10.7759/cureus.25118
22. Gupta K, Goyal S, Chaudhary D, Sakhuja P, Narang P, Nag HH. Undifferentiated carcinoma with osteoclast-like giant cells of pancreas on cytology: A case report with review of literature. Diagn Cytopathol. (2022) 50:E289–e94. doi: 10.1002/dc.25001
23. Tomihara H, Hashimoto K, Ishikawa H, Terashita D, Gakuhara A, Fukuda S, et al. Spontaneous rupture of an undifferentiated carcinoma with osteoclast-like giant cells of the pancreas presenting as intra-abdominal bleeding: A case report. Surg Case Rep. (2022) 8:79. doi: 10.1186/s40792–022-01437–2
24. Igarashi Y, Gocho T, Taniai T, Uwagawa T, Hamura R, Shirai Y, et al. Conversion surgery for undifferentiated carcinoma with osteoclast-like giant cells of the pancreas: A case report. Surg Case Rep. (2022) 8:42. doi: 10.1186/s40792-022-01385-x
25. Jain PV, Griffin M, Hunt B, Ward E, Tsai S, Doucette S. Undifferentiated carcinoma with osteoclast-like giant cells: A pathologic-radiologic correlation of a rare histologic subtype of pancreatic ductal adenocarcinoma. Ann Diagn Pathol. (2022) 57:151884. doi: 10.1016/j.anndiagpath.2021.151884
26. Swaid MB, Vitale E, Alatassi N, Siddiqui H, Yazdani H. Metastatic undifferentiated osteoclast-like giant cell pancreatic carcinoma. Cureus. (2022) 14:e27586. doi: 10.7759/cureus.27586
27. Chan W, Park S, Shirkhoda L, O’Connell R, Houshyar R. Undifferentiated carcinoma of the pancreas with osteoclast-like giant cells: A case report. J Med Case Rep. (2023) 17:477. doi: 10.1186/s13256–023-04213–4
28. Ran H, Chen G, He Y, Yu Q, Xie Y, Liu J, et al. Undifferentiated carcinoma with osteoclast−Like giant cells of the pancreas: A case report. Oncol Lett. (2023) 25:252. doi: 10.3892/ol.2023.13838
29. Shiihara M, Higuchi R, Izumo W, Furukawa T, Yamamoto M. A comparison of the pathological types of undifferentiated carcinoma of the pancreas. Pancreas. (2020) 49:230–5. doi: 10.1097/mpa.0000000000001483
30. Gao Y, Cai B, Yin L, Song G, Lu Z, Guo F, et al. Undifferentiated carcinoma of pancreas with osteoclast-like giant cells: one center’s experience of 13 cases and characteristic pre-operative images. Cancer Manag Res. (2022) 14:1409–19. doi: 10.2147/cmar.S349625
31. Guo YL, Ruan LT, Wang QP, Lian J. Undifferentiated carcinoma with osteoclast-like giant cells of pancreas: A case report with review of the computed tomography findings. Med (Baltimore). (2018) 97:e13516. doi: 10.1097/md.0000000000013516
32. Muraki T, Reid MD, Basturk O, Jang KT, Bedolla G, Bagci P, et al. Undifferentiated carcinoma with osteoclastic giant cells of the pancreas: clinicopathologic analysis of 38 cases highlights a more protracted clinical course than currently appreciated. Am J Surg Pathol. (2016) 40:1203–16. doi: 10.1097/pas.0000000000000689
33. Gao HQ, Yang YM, Zhuang Y, Liu P. Locally advanced undifferentiated carcinoma with osteoclast-like giant cells of the pancreas. World J Gastroenterol. (2015) 21:694–8. doi: 10.3748/wjg.v21.i2.694
34. Fukukura Y, Kumagae Y, Hirahara M, Hakamada H, Nagano H, Nakajo M, et al. Ct and mri features of undifferentiated carcinomas with osteoclast-like giant cells of the pancreas: A case series. Abdom Radiol (NY). (2019) 44:1246–55. doi: 10.1007/s00261–019-01958–9
35. Sato K, Urakawa H, Sakamoto K, Ito E, Hamada Y, Yoshimitsu K. Undifferentiated carcinoma of the pancreas with osteoclast-like giant cells showing intraductal growth and intratumoral hemorrhage: mri features. Radiol Case Rep. (2019) 14:1283–7. doi: 10.1016/j.radcr.2019.07.020
36. Moore JC, Bentz JS, Hilden K, Adler DG. Osteoclastic and pleomorphic giant cell tumors of the pancreas: A review of clinical, endoscopic, and pathologic features. World J Gastrointest Endosc. (2010) 2:15–9. doi: 10.4253/wjge.v2.i1.15
37. Fu LP, Cheng AP, Wang XG, Fu JL, Jin L. 18f-fdg pet/ct in the detection of undifferentiated carcinoma with osteoclast-like giant cells of the pancreas. Clin Nucl Med. (2017) 42:615–6. doi: 10.1097/rlu.0000000000001719
38. Imaoka H, Sasaki M, Hashimoto Y, Watanabe K, Ikeda M. New era of endoscopic ultrasound-guided tissue acquisition: next-generation sequencing by endoscopic ultrasound-guided sampling for pancreatic cancer. J Clin Med. (2019) 8. doi: 10.3390/jcm8081173
39. Crinò SF, Le Grazie M, Manfrin E, Conti Bellocchi MC, Bernardoni L, Granato A, et al. Randomized trial comparing fork-tip and side-fenestrated needles for eus-guided fine-needle biopsy of solid pancreatic lesions. Gastrointest Endosc. (2020) 92:648–58.e2. doi: 10.1016/j.gie.2020.05.016
40. Togawa Y, Tonouchi A, Chiku T, Sano W, Doki T, Yano K, et al. A case report of undifferentiated carcinoma with osteoclast-like giant cells of the pancreas and literature review. Clin J Gastroenterol. (2010) 3:195–203. doi: 10.1007/s12328–010-0160–2
41. Hrudka J, Lawrie K, Waldauf P, Ciprová V, Moravcová J, Matěj R. Negative prognostic impact of pd-L1 expression in tumor cells of undifferentiated (Anaplastic) carcinoma with osteoclast-like giant cells of the pancreas: study of 13 cases comparing ductal pancreatic carcinoma and review of the literature. Virchows Archiv. (2020) 477:687–96. doi: 10.1007/s00428–020-02830–8
42. Luchini C, Cros J, Pea A, Pilati C, Veronese N, Rusev B, et al. Pd-1, pd-L1, and cd163 in pancreatic undifferentiated carcinoma with osteoclast-like giant cells: expression patterns and clinical implications. Hum Pathol. (2018) 81:157–65. doi: 10.1016/j.humpath.2018.07.006
43. Kosmahl M, Pauser U, Anlauf M, Klöppel G. Pancreatic ductal adenocarcinomas with cystic features: neither rare nor uniform. Mod Pathol. (2005) 18:1157–64. doi: 10.1038/modpathol.3800446
44. Bergmann F, Esposito I, Michalski CW, Herpel E, Friess H, Schirmacher P. Early undifferentiated pancreatic carcinoma with osteoclastlike giant cells: direct evidence for ductal evolution. Am J Surg Pathol. (2007) 31:1919–25. doi: 10.1097/PAS.0b013e318067bca8
45. Schawkat K, Manning MA, Glickman JN, Mortele KJ. Pancreatic ductal adenocarcinoma and its variants: pearls and perils. Radiographics. (2020) 40:1219–39. doi: 10.1148/rg.2020190184
46. Wang X, Miao J, Wang S, Shen R, Zhang S, Tian Y, et al. Single-cell rna-seq reveals the genesis and heterogeneity of tumor microenvironment in pancreatic undifferentiated carcinoma with osteoclast-like giant-cells. Mol Cancer. (2022) 21:133. doi: 10.1186/s12943–022-01596–8
47. Chiarelli M, Guttadauro A, Gerosa M, Marando A, Gabrielli F, De Simone M, et al. An indeterminate mucin-producing cystic neoplasm containing an undifferentiated carcinoma with osteoclast-like giant cells: A case report of a rare association of pancreatic tumors. BMC Gastroenterol. (2015) 15:161. doi: 10.1186/s12876–015-0391–2
48. Zhao N, Mei N, Yi Y, Wang H, Wang Y, Yao Y, et al. Case report: pathological and genetic features of pancreatic undifferentiated carcinoma with osteoclast-like giant cells. Pathol Oncol Res. (2023) 29:1610983. doi: 10.3389/pore.2023.1610983
49. Nai GA, Amico E, Gimenez VR, Guilmar M. Osteoclast-like giant cell tumor of the pancreas associated with mucus-secreting adenocarcinoma. Case report and discussion of the histogenesis. Pancreatology. (2005) 5:279–84. doi: 10.1159/000085283
50. Sedivy R, Kalipciyan M, Mazal PR, Wolf B, Wrba F, Karner-Hanusch J, et al. Osteoclast-like giant cell tumor in mucinous cystadenocarcinoma of the pancreas: an immunohistochemical and molecular analysis. Cancer Detect Prev. (2005) 29:8–14. doi: 10.1016/j.cdp.2004.10.006
51. Pan ZG, Wang B. Anaplastic carcinoma of the pancreas associated with a mucinous cystic adenocarcinoma. A case report and review of the literature. Jop. (2007) 8:775–82.
52. Burkadze G, Turashvili G. A case of osteoclast-like giant cell tumor of the pancreas associated with borderline mucinous cystic neoplasm. Pathol Oncol Res. (2009) 15:129–31. doi: 10.1007/s12253–008-9053–9
53. Wada T, Itano O, Oshima G, Chiba N, Ishikawa H, Koyama Y, et al. A male case of an undifferentiated carcinoma with osteoclast-like giant cells originating in an indeterminate mucin-producing cystic neoplasm of the pancreas. A case report and review of the literature. World J Surg Oncol. (2011) 9:100. doi: 10.1186/1477–7819-9–100
54. Luchini C, Pea A, Lionheart G, Mafficini A, Nottegar A, Veronese N, et al. Pancreatic Undifferentiated Carcinoma with Osteoclast-Like Giant Cells Is Genetically Similar to, but Clinically Distinct from, Conventional Ductal Adenocarcinoma. J Pathol. (2017) 243:148–54. doi: 10.1002/path.4941
55. Hanayneh W, Parekh H, Fitzpatrick G, Feely M, George TJ, Starr JS. Two cases of rare pancreatic Malignancies. J Pancreat Cancer. (2019) 5:26–33. doi: 10.1089/pancan.2019.0007
56. Charifa A, Walther Z, Salem RR, Jain D. Undifferentiated carcinoma with osteoclast-like giant cells of the pancreas arising from an intraductal papillary mucinous neoplasm. Hum Pathology: Case Rep. (2019) 15:95–8. doi: 10.1016/j.ehpc.2018.12.007
57. Farhat W, Ammar H, Mizouni A, Harrabi F, Bouazzi A, Hammami E, et al. Osteoclastic giant cell tumor of the pancreas with synchronous jejunal gastrointestinal stromal tumor: A case report. Ann Med Surg (Lond). (2020) 51:28–30. doi: 10.1016/j.amsu.2019.11.008
58. Mattiolo P, Fiadone G, Paolino G, Chatterjee D, Bernasconi R, Piccoli P, et al. Epithelial-mesenchymal transition in undifferentiated carcinoma of the pancreas with and without osteoclast-like giant cells. Virchows Archiv. (2021) 478:319–26. doi: 10.1007/s00428–020-02889–3
59. Chung K, Nawazish A, Chai SM, Bhandari M, Uthamalingam P. Undifferentiated carcinoma of the pancreas with osteoclast-like giant cells arising from an intraductal papillary mucinous neoplasm: report of a rare case highlighting diagnostic difficulties. Pathology. (2024) 56:594–7. doi: 10.1016/j.pathol.2023.09.016
60. Hrudka J, Kalinová M, Ciprová V, Moravcová J, Dvořák R, Matěj R. Undifferentiated carcinoma with osteoclast-like giant cells of the pancreas: molecular genetic analysis of 13 cases. Int J Mol Sci. (2024) 25. doi: 10.3390/ijms25063285
61. Bazzichetto C, Luchini C, Conciatori F, Vaccaro V, Di Cello I, Mattiolo P, et al. Morphologic and molecular landscape of pancreatic cancer variants as the basis of new therapeutic strategies for precision oncology. Int J Mol Sci. (2020) 21. doi: 10.3390/ijms21228841
62. Luo J. Kras mutation in pancreatic cancer. Semin Oncol. (2021) 48:10–8. doi: 10.1053/j.seminoncol.2021.02.003
63. Imai Y, Morishita S, Ikeda Y, Toyoda M, Ashizawa T, Yamamoto K, et al. Immunohistochemical and molecular analysis of giant cell carcinoma of the pancreas: A report of three cases. Pancreas. (1999) 18:308–15. doi: 10.1097/00006676–199904000–00013
64. Koorstra JB, Maitra A, Morsink FH, Drillenburg P, ten Kate FJ, Hruban RH, et al. Undifferentiated carcinoma with osteoclastic giant cells (Ucocgc) of the pancreas associated with the familial atypical multiple mole melanoma syndrome (Fammm). Am J Surg Pathol. (2008) 32:1905–9. doi: 10.1097/PAS.0b013e31818371cd
65. Popov A, Hrudka J, Szabó A, Oliverius M, Šubrt Z, Vránová J, et al. Expression of selected mirnas in undifferentiated carcinoma with osteoclast-like giant cells (Ucogc) of the pancreas: comparison with poorly differentiated pancreatic ductal adenocarcinoma. #N/A. (2024) 12:962. doi: 10.3390/biomedicines12050962
66. Imaoka H, Ikeda M, Maehara K, Umemoto K, Ozaka M, Kobayashi S, et al. Clinical outcomes of chemotherapy in patients with undifferentiated carcinoma of the pancreas: A retrospective multicenter cohort study. BMC Cancer. (2020) 20:946. doi: 10.1186/s12885–020-07462–4
67. Lehrke HD, Graham RP, McWilliams RR, Lam-Himlin DM, Smyrk TC, Jenkins S, et al. Undifferentiated pancreatic carcinomas display enrichment for frequency and extent of pd-L1 expression by tumor cells. Am J Clin Pathol. (2017) 148:441–9. doi: 10.1093/ajcp/aqx092
68. Obayashi M, Shibasaki Y, Koakutsu T, Hayashi Y, Shoji T, Hirayama K, et al. Pancreatic undifferentiated carcinoma with osteoclast-like giant cells curatively resected after pembrolizumab therapy for lung metastases: A case report. BMC Gastroenterol. (2020) 20:220. doi: 10.1186/s12876–020-01362–4
69. Ueberroth BE, Liu AJ, Graham RP, Bekaii-Saab TS, McWilliams RR, Mahipal A, et al. Osteoclast-like giant cell tumors of the pancreas: clinical characteristics, genetic testing, and treatment modalities. Pancreas. (2021) 50:952–6. doi: 10.1097/mpa.0000000000001858
70. Christopher W, Nassoiy S, Marcus R, Keller J, Chang SC, Fischer T, et al. Prognostic indicators for undifferentiated carcinoma with/without osteoclast-like giant cells of the pancreas. HPB (Oxford). (2022) 24:1757–69. doi: 10.1016/j.hpb.2022.05.1344
71. Singhal A, Shrago SS, Li SF, Huang Y, Kohli V. Giant cell tumor of the pancreas: A pathological diagnosis with poor prognosis. Hepatobiliary Pancreat Dis Int. (2010) 9:433–7.
72. Imaoka H, Ikeda M, Maehara K, Umemoto K, Ozaka M, Kobayashi S, et al. Risk stratification and prognostic factors in patients with unresectable undifferentiated carcinoma of the pancreas. Pancreatology. (2021) 21:738–45. doi: 10.1016/j.pan.2021.02.008
73. Xu M, Chen W, Wang D, Nie M. Clinical characteristics and prognosis of osteoclast-like giant cell tumors of the pancreas compared with pancreatic adenocarcinomas: A population-based study. Med Sci Monit. (2020) 26:e922585. doi: 10.12659/msm.922585
74. Kharkhach A, Bouhout T, Serji B, El Harroudi T. Undifferentiated pancreatic carcinoma with osteoclast-like giant cells: A review and case report analysis. J Gastrointest Cancer. (2021) 52:1106–13. doi: 10.1007/s12029–021-00583–4
75. Strobel O, Hartwig W, Bergmann F, Hinz U, Hackert T, Grenacher L, et al. Anaplastic pancreatic cancer: presentation, surgical management, and outcome. Surgery. (2011) 149:200–8. doi: 10.1016/j.surg.2010.04.026
76. Shiozawa M, Imada T, Ishiwa N, Rino Y, Hasuo K, Takanashi Y, et al. Osteoclast-like giant cell tumor of the pancreas. Int J Clin Oncol. (2002) 7:376–80. doi: 10.1007/s101470200059
77. Saito H, Kashiyama H, Murohashi T, Sasaki K, Misawa R, Ohwada S. Case of six-year disease-free survival with undifferentiated carcinoma of the pancreas. Case Rep Gastroenterol. (2016) 10:472–8. doi: 10.1159/000448878
78. Shah A, Khurana T, Freid L, Siddiqui AA. Undifferentiated carcinoma with osteoclast-like giant cells of the pancreas in a patient with new diagnosis of follicular non-hodgkin’s lymphoma. ACG Case Rep J. (2014) 1:109–11. doi: 10.14309/crj.2014.17
79. Kobayashi S, Nakano H, Ooike N, Oohashi M, Koizumi S, Otsubo T. Long-term survivor of a resected undifferentiated pancreatic carcinoma with osteoclast-like giant cells who underwent a second curative resection: A case report and review of the literature. Oncol Lett. (2014) 8:1499–504. doi: 10.3892/ol.2014.2325
Keywords: pancreatic cancer, variants, undifferentiated carcinoma, osteoclast-like giant cells, prognosis
Citation: Wu H (2024) Undifferentiated carcinoma with osteoclast-like giant cells of the pancreas: a narrative review. Front. Oncol. 14:1409197. doi: 10.3389/fonc.2024.1409197
Received: 29 March 2024; Accepted: 28 May 2024;
Published: 19 June 2024.
Edited by:
Stefano Francesco Crinò, University of Verona, ItalyReviewed by:
Rahul Gupta, Synergy Institute of Medical Sciences, IndiaJan Hrudka, Charles University, Czechia
Copyright © 2024 Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Haoxiang Wu, aGFveGlhbmdfd3VAMTYzLmNvbQ==