 Diocésio Alves Pinto Andrade1
Diocésio Alves Pinto Andrade1 Murilo Bonatelli2
Murilo Bonatelli2 Flávia Escremim de Paula2
Flávia Escremim de Paula2 Gustavo Noriz Berardinelli2
Gustavo Noriz Berardinelli2 Gustavo Ramos Teixeira2,3,4Monise Tadin dos Reis3Flávia Fazzio Barbin3Carlos Eduardo Mattos da Cunha Andrade4,5Vinicius Pereira Aguiar6
Gustavo Ramos Teixeira2,3,4Monise Tadin dos Reis3Flávia Fazzio Barbin3Carlos Eduardo Mattos da Cunha Andrade4,5Vinicius Pereira Aguiar6 Alejandro Delfos Hermoza5Welinton Yoshio Hirai7Ronaldo Luís Schmidt8
Alejandro Delfos Hermoza5Welinton Yoshio Hirai7Ronaldo Luís Schmidt8 Rui Manuel Reis2,9,10
Rui Manuel Reis2,9,10 Ricardos dos Reis5*
Ricardos dos Reis5*- 1Oncoclínicas&CO, Medica Scientia Innovation Research (MEDSIR)/MedSir, Ribeirão Preto, São Paulo, Brazil
- 2Molecular Diagnostic Laboratory, Barretos Cancer Hospital, São Paulo, Brazil
- 3Pathology Laboratory, Barretos Cancer Hospital, São Paulo, Brazil
- 4Barretos School of Health Sciences Dr. Paulo Prata, FACISB, São Paulo, Brazil
- 5Gynecologic Oncology Department, Barretos Cancer Hospital, São Paulo, Brazil
- 6Gynecologic Oncology Department, Patrocinio Cancer Hospital, Minas Gerais, Brazil
- 7Department of Epidemiology and Biostatistics, Barretos Cancer Hospital, São Paulo, Brazil
- 8Department of Surgical Oncology, Lagarto Unit, Barretos Cancer Hospital, Sergipe, Brazil
- 9Molecular Oncology Research Center, Barretos Cancer Hospital, São Paulo, Brazil
- 10Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, Braga, Portugal
Purpose: Molecular classification of endometrial cancer (EC) has emerged as a key approach to individualize therapy and define prognostic outcomes. This study aimed to implement the traditional ProMisE classification in a Brazilian population, compared with a molecular setting of ProMisE biomarkers, and evaluate its impact on patients’ prognosis.
Patient and methods: A prospective cohort of 114 patients with primary EC treated at Barretos Cancer Hospital (BCH) between October 2020 and December 2022 was conducted. Pathology diagnosis, staging, treatment, and follow-up data were collected. The traditional ProMisE methodology was carried out by POLE hotspot sequencing and immunohistochemistry (IHC) for p53 and mismatch repair (MMR) proteins. We further evaluate the MMR and TP53 status by molecular approach, namely microsatellite instability (MSI) by PCR-based and TP53 mutation analysis by next-generation sequencing (NGS). The results of the 4 molecular groups in both methodologies were compared regarding agreement accuracy and survival outcomes.
Results: Among the 114 cases, the traditional ProMisE groups were: POLEmut 15.8%, MMRd 28.1%, p53abn 27.2%, and no specific molecular profile (NSMP) 28.9%. Considering the molecular classification approach, we observed a POLEmut group of 15.8%, MSI group of 23.7%, TP53 mutation of 27.2%, and NSMP of 33.3%. The concordance rate of both approaches was 86.8% (99/114 cases) with an overall accuracy of 0.87. Importantly, both traditional and molecular ProMisE approaches were associated with significant distinct overall survival (OS) and progression-free survival (PFS) outcomes, with POLEmut patients exhibiting a better prognosis (93.8% OS, at 24 months), whereas the p53abn having a worse survival time (68.9% of OS, at 24 months).
Conclusion: We reported for the first time the Brazilian profile of the ProMisE classification of endometrial cancer and demonstrated the prognostic impact of the traditional and molecular ProMisE classification on patient outcomes.
1 Introduction
Endometrial cancer (EC) is the 6th most prevalent neoplasm among women worldwide, representing 4.5% of cancer diagnoses in females. There are an estimated 420,000 new cases per year, and just over 97,000 women will die from this neoplasm in the same period (1). In Brazil, EC is the 7th most prevalent tumor among women, with approximately 8,000 new diagnoses per year (2). Although the absolute numbers are not that impactful, a significant increase in new cases was observed in Brazil, probably related to the rise in obesity rates (3).
For years, the understanding of the pathophysiology of EC was based on the dualistic model proposed in the early 1980s, classifying it into type I (endometrioid) and type II (non-endometrioid) (4). In 2013, with the publication of The Cancer Genome Atlas (TCGA), this neoplasm was molecularly classified into four groups with different prognoses: POLE ultramutated (POLE), microsatellite instability hypermutated (MSI), copy-number low (endometrioid), and copy-number high (serous-like) (5). Due to a complex multi-omics methodology, it was difficult to reproduce and implement in daily practice.
Subsequently, two independent groups developed more straightforward methods to classify EC molecularly. The Proactive Molecular Risk Classifier for Endometrial Cancer (ProMisE) and Leiden/TransPORTEC classification used immunohistochemistry to detect the presence/absence of mismatch repair (MMR) proteins and to evaluate p53 expression, using, in both methodologies, the molecular analysis of POLE hotspot mutations. Based on this classification, EC patients were classified into one of four molecular subtypes: POLE mutated (POLEmut), mismatch repair deficient (MMRd), p53 abnormal (p53abn), and no specific molecular profile (NSMP) (6, 7). To simplify the analysis of molecular subgroups of EC in a single exam with a single sample, the Canadian group that created the ProMisE methodology carried out a study comparing the standard method with next-generation sequencing methodology (ProMisE NGS). Of the 164 samples tested in this study, there was disagreement in only 5, with an overall accuracy of 0.97 (8).
In 2021, the European Societies of Gynaecological Oncology, Radiotherapy, and Pathology (ESGO/ESTRO/ESP) published a consensus where, for the first time, the ProMisE molecular classification began to be considered for the therapeutic management of patients with EC (9). Based on this, patients in the p53abn subgroup, even in less advanced stages, are considered high risk and undergo an upgrade in their risk stratification. In contrast, patients in the POLEmut subgroup, who have suffered downgrades in their risk stratification, may have a de-escalation in their adjuvant treatment (9). Moreover, ProMisE was included in the new FIGO staging published in 2023 (10). Therefore, the molecular classification will become part of the therapeutic definition of patients with EC, even more so with the future results of phase 3 studies that base their treatment protocols on this novel stratification (11, 12). Recently, the lack of diversity in genomics studies has been highlighted, leading to unmet scientific needs and health disparities (13). In this context, the knowledge of endometrial cancer molecular profile in the Latin-American population, particularly the Brazilian, is scarce.
The present study aimed to describe the implementation of the ProMisE classification for routine endometrial cancer evaluation in a Brazilian tertiary public cancer center hospital, to compare it with a molecular approach of MSI and TP53 mutation, and to evaluate ProMisE impact on patients’ prognosis.
2 Methods
2.1 Patients
This prospective cohort study of EC attended and followed at the Gynecologic Oncology Department at Barretos Cancer Hospital (BCH), between October 2020 and December 2022. A REDCap database was created with pertinent clinical-pathological and molecular features (14). The Institutional Review Board approval was obtained from the BCH Office of Protocol Research (65587622.7.0000.5437).
The medical records of all patients who underwent total hysterectomy were prospectively reviewed. The information collected included demographics, surgical–pathology reports, and clinical outcomes. We included patients aged 18 or older diagnosed with low, intermediate, and high-risk EC, treated by surgery or systemic treatment. Exclusion criteria included patients treated surgically outside the institution referred to ours for adjuvant treatment and/or follow-up without a treatment registry or incomplete medical records. All patients underwent a pretreatment evaluation, including a physical examination, pelvic magnetic resonance imaging (MRI), and chest and abdomen computed tomography (CT). Primary surgery included a total hysterectomy and bilateral salpingo-oophorectomy. Sentinel lymph node mapping and/or systematic lymphadenectomy (pelvic and/or para-aortic) were performed according to the pre-operative data and/or intraoperative frozen section analysis. Adjuvant treatment was given at the discretion of a multidisciplinary conference. The follow-up data were obtained from clinic visits, every three months in the first two years, and every six months during years 3 to 5. Patients with high-risk EC do chest and abdominal computed tomography every 12 months in the first two years. Patients who were no longer being followed clinically by BCH were contacted by the Institution’s Department of Research to obtain information about cancer status and general medical problems. The patients were characterized into the prognostic risk groups (low, intermediate, high-intermediate, high, and advanced metastatic) according to the 2020 ESGO/ESTRO/ESP guidelines (9). All cases were histologically reviewed by GRT, MTR, and FFB, confirming the initial diagnosis (Supplementary Figure 1).
2.2 ProMisE classification
The ProMisE molecular profile was performed by Talhouk et al. (15), using MMR immunohistochemistry (IHC), followed by POLE hotspot mutation of the MMR proficient cases, and then p53 IHC of the POLE wildtype cases, leading to the following classification: MMRd, POLEmut, p53abn, and NSMP.
2.2.1 Mismatch repair and p53 immunohistochemistry
Formalin-fixed paraffin-embedded (FFPE) tissue blocks were cut into 3 μm sections for IHC. For MMR enzymes, the Dako EnVision™ FLEX detection system Kit (Dako, Glostrup, Denmark) and Autostainer Link 48 equipment (Dako, Glostrup, Denmark) were used as previously described (16). The antigen retrieval process was done at 97°C for 20 minutes (pH 9.0). Endogenous peroxidases were blocked with EnVision™ FLEX Peroxidase-Blocking Reagent (Dako, Glostrup, Denmark). The primary antibodies used were: FLEX monoclonal mouse anti-MutL protein homolog 1 (MLH1) (clone ES05, ref IS079, Dako, Glostrup, Denmark); FLEX monoclonal mouse anti-MutS protein homolog 2 (MSH2) (clone FE11, ref IR085, Dako, Glostrup, Denmark); FLEX monoclonal rabbit anti-postmeiotic segregation increased 2 (PMS2) (clone EP51, ref IR087, Dako, Glostrup, Denmark); and FLEX monoclonal rabbit anti-MutS protein homolog 6 (MSH6) (clone EP49, ref IR086, Dako, Glostrup, Denmark). The DAB solution was used for immunostaining visualization. Slides were counterstained with hematoxylin. In each case, nuclear staining of normal epithelial cells, lymphocytes, and stromal cells served as positive internal controls. All cases were analyzed by expert pathologists (GRT, MTR, and FFB) who, based on nuclear staining, classified each protein by its expression. Regardless of the intensity or the extent of cell staining, the positive status was found for the cases that showed staining (presence of the expression of the protein under analysis) and the negative status when no staining was present (absence of expression of the protein under analysis) in tumor cells.
For p53, immunostaining was performed using the BenchMark Ultra platform (Ventana Medical System, Arizona, USA) with the UltraView® signal detection kit (Ventana Medical System, Arizona, USA). The primary antibody was anti-p53 (clone DO-7, Roche Diagnostics, Indiana, USA). Immunoexpression was considered abnormal when it was positive, strong, and diffuse in more than 80% of tumor cells (positive pattern) or entirely negative with positive intern control (null pattern), as reported (17).
2.2.2 POLE mutation detection
Tumor FFPE DNA was isolated using QIAamp DNA Micro Kit (Qiagen, Hilden, Germany) as previously reported (18). The hotspot exonuclease domain of POLE (exons 9-14) was evaluated by Sanger sequencing. Polymerase chain reaction (PCR) was performed using M13-tailed primers as described elsewhere (19). The PCR products were purified using Exo+Sap (Cellco), followed by bidirectional sequencing with universal M13 tags and the BigDye Terminator v3.1 Cycle Sequencing Kit (Thermo Fisher Scientific). Capillary electrophoresis was carried out on an ABI 3500xL Genetic Analyzer (Applied Biosystems), and the resulting chromatograms were analyzed using SeqScape software v3.0 (Applied Biosystems) in addition to manual inspection.
2.3 ProMisE molecular approach
MMR and TP53 status were molecularly evaluated. For MMR, a PCR-based approach was used with the HT-MSI+ Kit (Cellco), which comprises six repeat markers (NR27, NR21, NR24, BAT25, BAT26, and HSP110), following the manufacturer’s instructions. Capillary electrophoresis was performed on an ABI 3500 Genetic Analyzer (Applied Biosystems), and the results were analyzed using GeneMapper v4.1 software (Applied Biosystems). Cases demonstrating the presence of two or more markers falling outside the quasimonomorphic variation range (QMVR) were categorized as MSI-H (high microsatellite instability), while cases without markers outside the QMVR were classified as MSS (microsatellite stable) (20).
The mutational analysis of TP53 coding region was assessed by NGS using the TruSight Tumor 15 Panel (Illumina) on the MiSeq System (Illumina). The analysis was carried out in the Sophia DDM® software v4.2 (Sophia Genetics). Variants were filtered out according to the following criteria: intronic (except splicing variants), synonymous singles nucleotide variants (SNVs), populational frequency >1%, poor quality of the read depth <500x, allele frequency <10%, and non-pathogenic variants (21).
2.4 Statistical analysis
Both quantitative and qualitative variables were initially explored using descriptive statistics. Quantitative variables were presented as mean and standard deviation or median and 25-75 percentiles, according to the data distribution measured by the Kolmigorov-Smirnov test. Qualitative variables were described using absolute and relative frequencies. Statistical analysis was carried out using Student’s T-test if the sample had a normal distribution or McNemar’s test if the sample was non-parametric. For categorical variables, the Chi-square or Fisher’s Exact test were used to compare the proportions between groups. When appropriate, 95% confidence intervals were calculated, for detecting a true effect considered a reasonable threshold in fields of research with risk of falsely decteing (type II error). The multivariate Cox regression model was analyzed to interpret prognostic information that can complement the molecular classification (demographic, surgical–pathology characteristics, and oncology outcomes). The Kappa coefficient was used to assess the concordance and accuracy between both methods evaluated (ProMise and ProMisE molecular approach).
Overall survival (OS) and progression-free survival (PFS) were estimated using the Kaplan-Meier method along with the Log-rank test, stratified by molecular classification. If necessary, we used Cox regression analysis techniques. Overall survival was defined as the time between the initial diagnosis and the date of the patient’s death from any cause or last contact. Progression-free survival was defined as the time between the initial diagnosis and the date on which disease progression was proven or the last contact. The data was analyzed using SPSS (Statistical Package for the Social Sciences) version 21.0 and R program version 4.4.0 (2024). Statistical significance was defined as p <0.05 with probability for level false positive rate (type I error rate) provides a likelihood inference.
3 Results
A total of 114 EC samples were analyzed prospectively. Clinicopathologic characteristics related to ProMisE classification are shown in Table 1. Approximately 50% of patients were stage I, while 10.5% were metastatic at diagnosis. Sixty-eight (59.6%) patients had histological grade 3, 30 (26.3%) of which had non-endometrioid histology. Considering ESGO risk stratification, 63 (55.3%) patients were considered high-risk, supporting adjuvant treatment (Table 1).
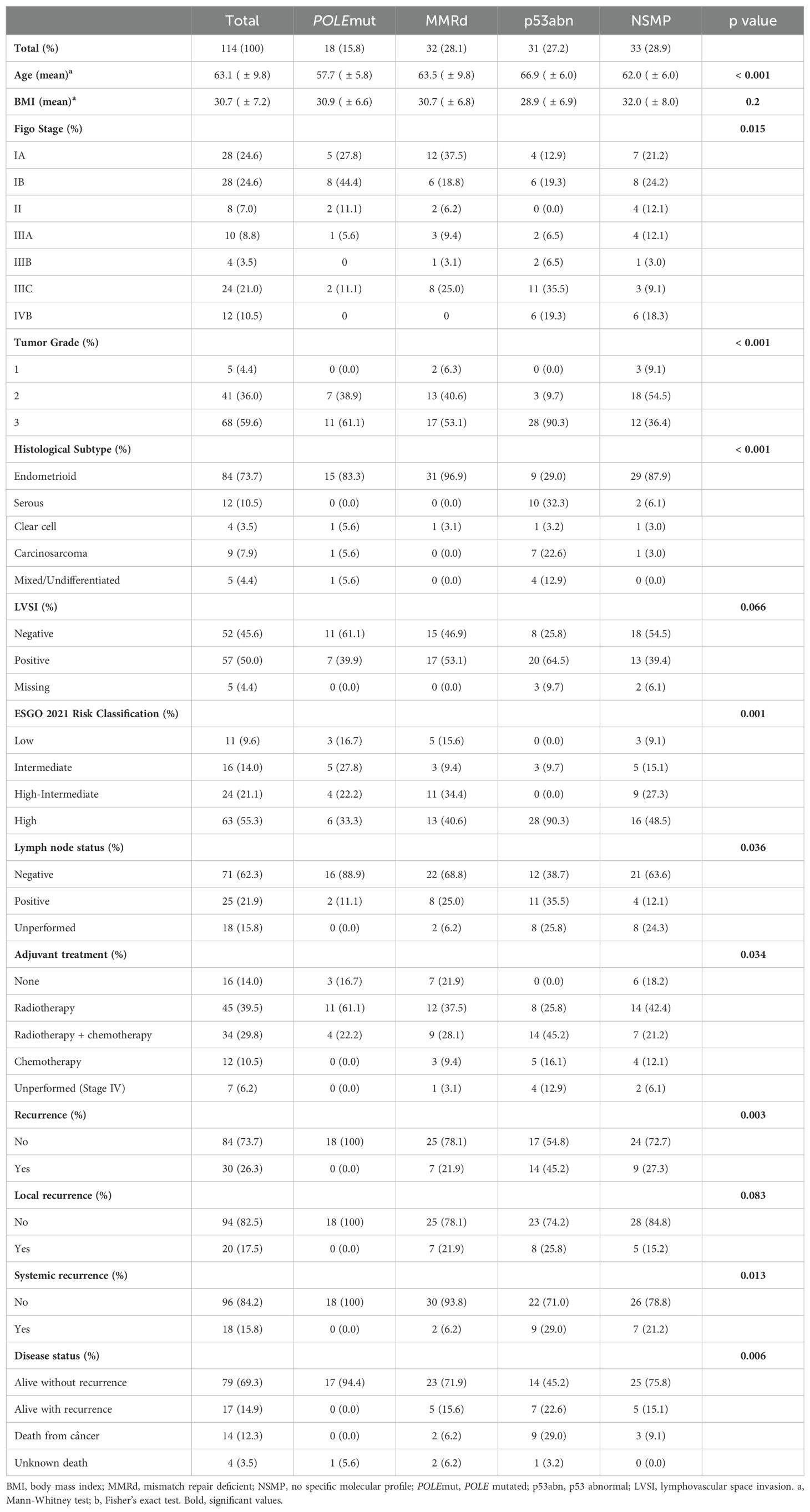
Table 1. Clinicopathologic features of the total cohort by ProMisE classifier.
Evaluating ProMisE classification (Table 1), we observed 18 (15.8%) POLEmut (Supplementary Figure 2), 32 (28.1%) MMRd (Supplementary Figure 3), 31 (27.2%) p53abn (Supplementary Figure 4), and 33 (28.9%) NSMP EC. There was a statistical difference between the groups in age, FIGO stage, tumor grade, histological subtype, ESGO risk classification, lymph node status, recurrence, and disease status. Namely, the recurrence rate, a significant unfavorable association was found for the p53abn and NSMP subgroup (p=0.013) (Table 1). Furthermore, the cancer mortality rate was more prevalent in the p53abn subgroup, with 29.0% of deaths (p=0.006) (Table 1).
Next, we compared the classification of the traditional ProMisE with the molecular approach (Table 2). Among the 114, we had 10 (8.7%) with discordant results between the MMR and MSI status (Supplementary Figure 5 and Table 3). Eight cases depicted the loss of one or more MMR proteins but showed an MSS phenotype, and two cases displayed an MSI-H status despite the expression of all MMR proteins (Table 3). Concerning TP53 status, among the 114, we observed 31 (27.2%) mutated cases (Supplementary Figure 6) and found six discordances methodologies (Table 4). Overall, the traditional and molecular PROMISE approaches showed a concordance rate of 86.8% (99/114 cases) with an overall accuracy of 0.87 and a Kappa coefficient of 0.82 (Table 5).
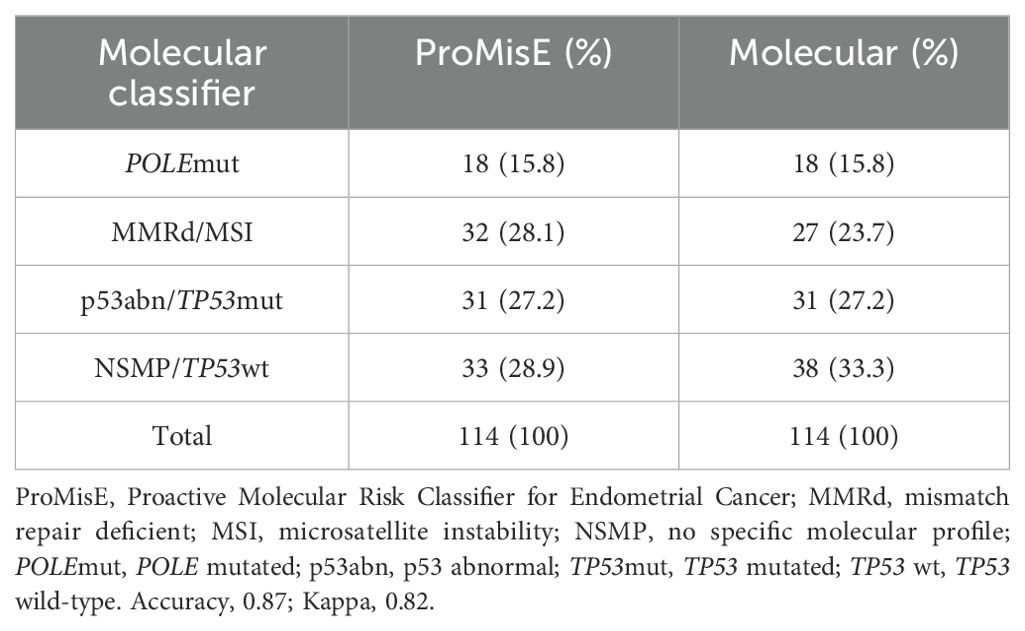
Table 2. Prevalence of subgroups by ProMisE and molecular classification.
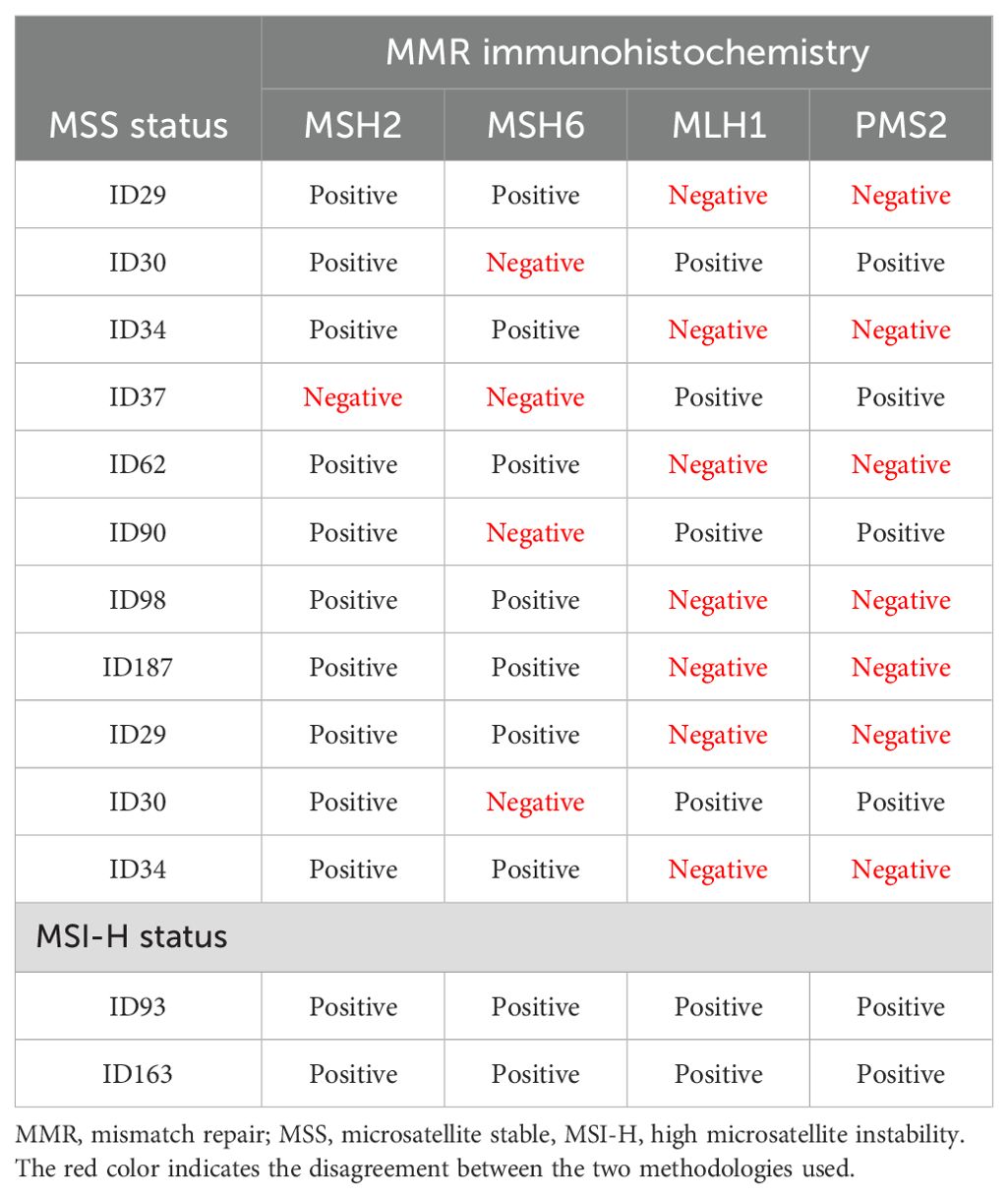
Table 3. Discordant MMR and MSI cases.
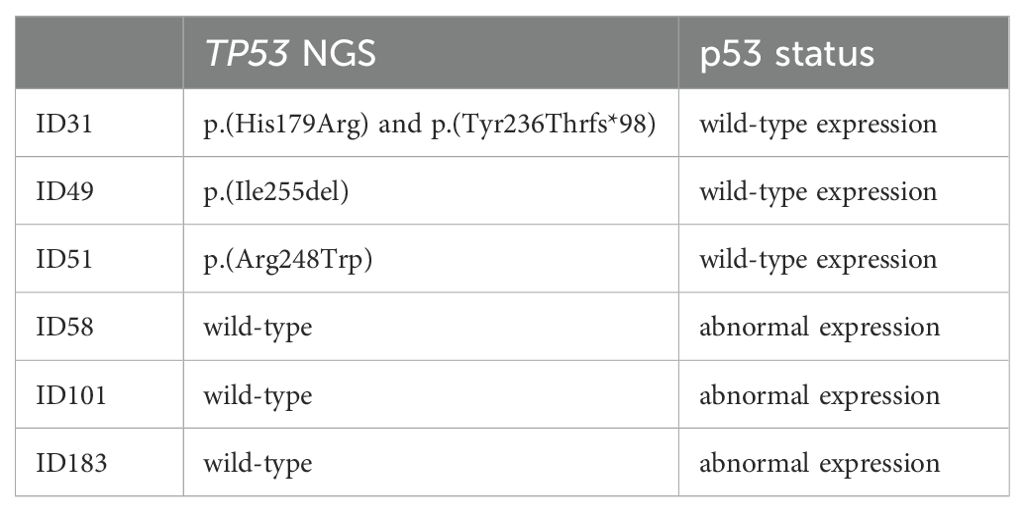
Table 4. Discordant p53 IHC and TP53 NGS cases.
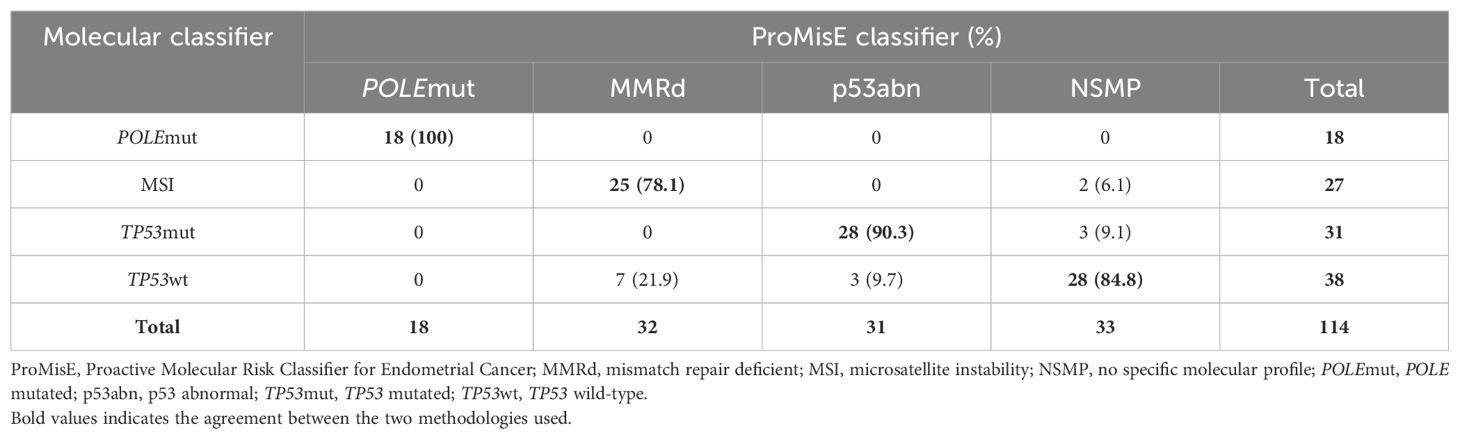
Table 5. Shifting of cases between molecular profiles using ProMisE and molecular classifier.
We further evaluated the prognostic impact of ProMisE classification, both traditional and molecular approaches. After a median follow-up of 23.2 months (± 10.6 months), a statistically significant difference was observed in terms of OS (p=0.027) and PFS (p=0.0034) related to the four molecular subtypes using the ProMisE classifier (Figure 1 and Table 6). Assessed by molecular classification, both outcomes maintain statistically significant differences with curves very similar to those of the traditional methodology (OS: p = 0.0036; PFS: p = 0.0023) (Figure 1 and Table 6). In this prospective cohort, attention is drawn to the excellent overall survival not only of the POLEmut subgroup, but also of MMRd and NSMP.
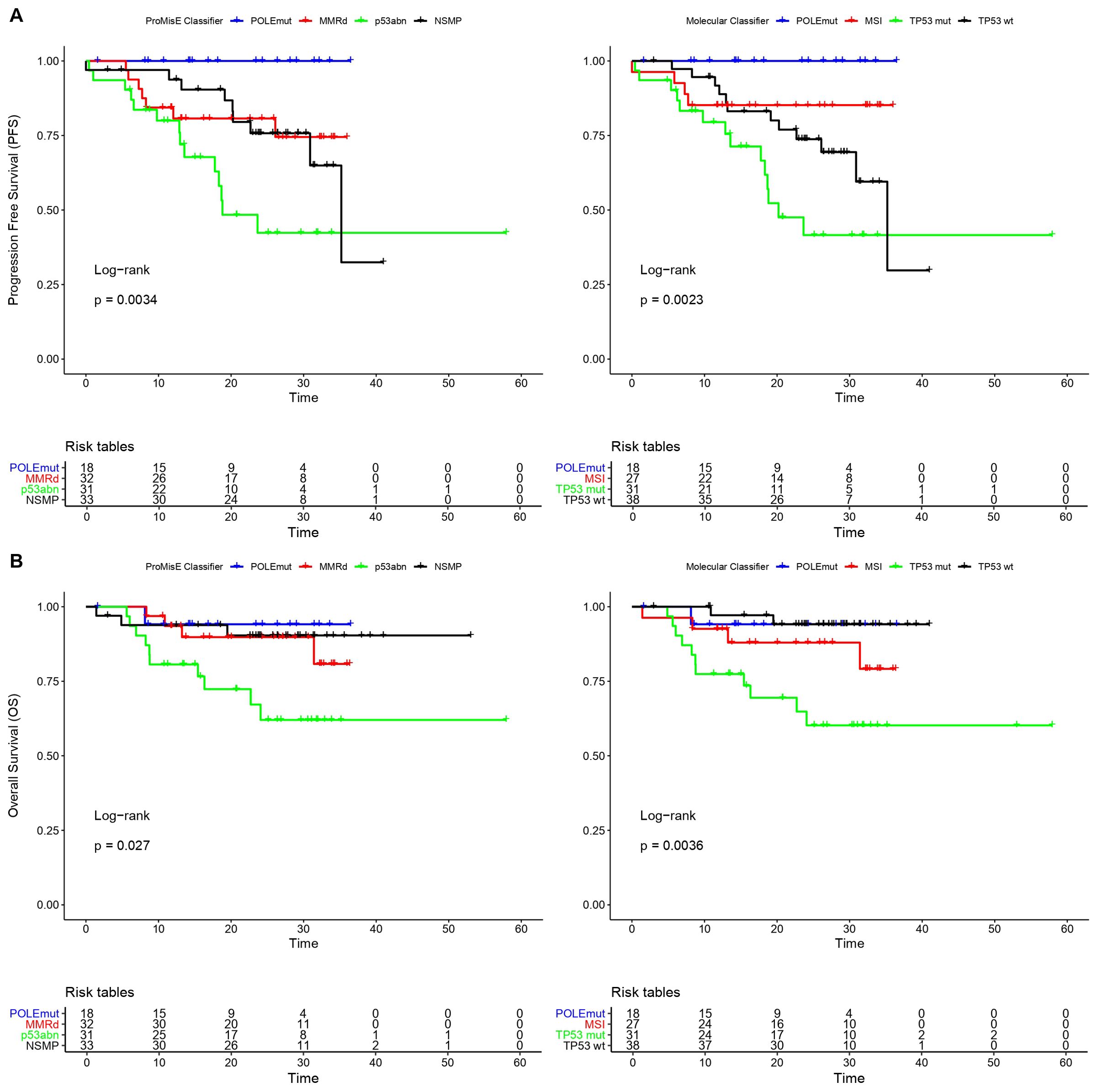
Figure 1. Kaplan-Meier survival analyses of both methods evaluated (ProMisE and ProMisE molecular approach). (A) Progression-free survival. (B) Overall survival.
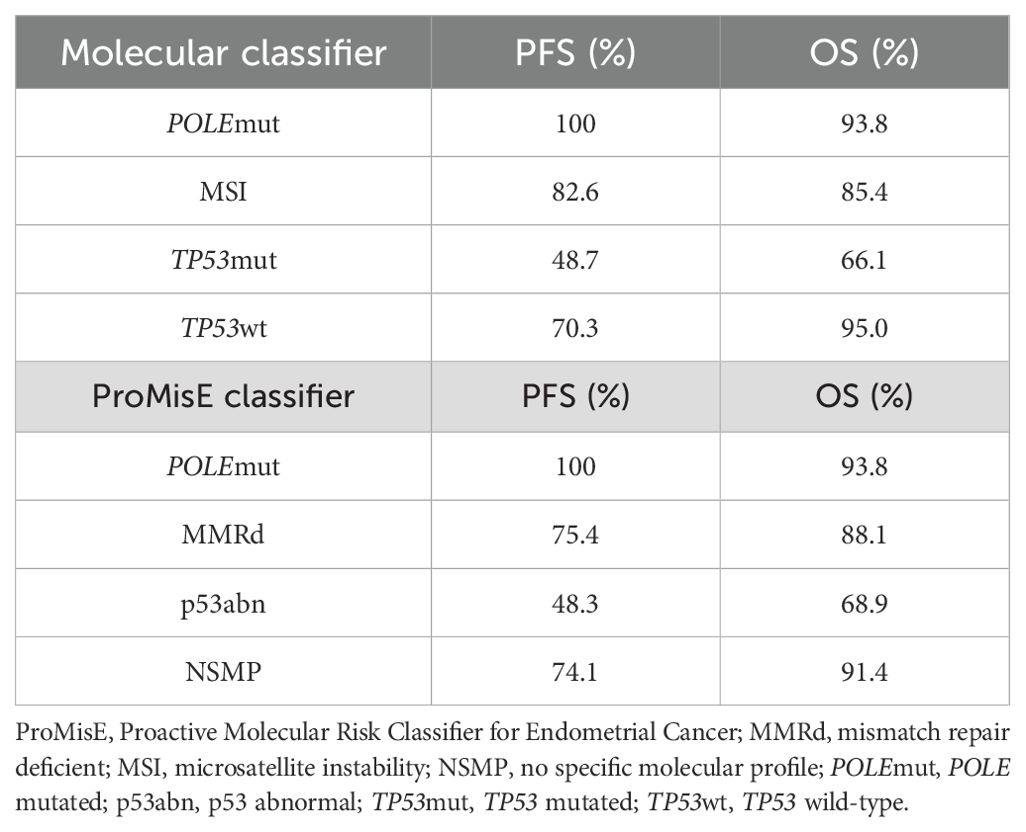
Table 6. Overall survival (OS) and progression-free survival (PFS) outcomes in both methodologies (24 months of follow-up).
4 Discussion
In the present study, we implemented the ProMisE classifier in a Brazilian prospective cohort of patients with EC from a tertiary cancer hospital. Furthermore, we proposed comparing this traditional methodology with a molecular methodology to evaluate its accuracy and reproducibility.
We observed that the proportion of patients in each of the four subgroups considering the ProMisE classifier was 15.8% POLEmut, 28.1% MMRd, 27.2% p53abn, and 28.9% NSMP. Overall, our findings align with the range reported in populations, namely from North America, Europe, Asia, and Oceania, which showed prevalence rates of these subgroups of 4-15% POLEmut, 17-38% MMRd, 9-25% p53abn, and 40-64% NSMP (6, 8, 14, 22–25). Proportionally, we had fewer cases in the NSMP subgroup and slightly higher cases in the p53abn subgroup. Further studies are needed to elucidate these differences, mainly the higher frequency of p53abn cases. Nevertheless, we can hypothesize that it could be due to the reference nature of our hospital, which receives cases with more advanced diagnoses (26). Additionally, it could be related to distinct exposure or the admixture ethnicity of the Brazilian population, as we recently reported the higher frequency of TP53 mutations in lung cancer patients associated with African ancestry (21). Notably, the p53abn subgroup classification was a significant factor for both PFS and OS, exhibiting the poorest outcomes.
Considering the histological subtypes and their molecular profile, we had 84 patients (73.7%) with endometrioid histology, 17.9% of these in the POLEmut subgroup, 36.9% in the MMRd subgroup, 10.7% in the p53abn subgroup, and 34.5% in the NSMP subgroup. The other 30 patients (26.3%) had non-endometrioid histologies (serous, clear cell, carcinosarcoma), with a prevalence of molecular profile represented as follows: 10.0% POLEmut, 3.3% MMRd, 73.4% p53abn, and 13.3% NSMP subgroup. Compared with TCGA data, the enormous prevalence of patients with p53 mutation is represented by non-endometrioid histologies, and less than 5% of patients with POLE mutation are in this histological subgroup. The present cohort has less than a third of patients when compared to the TCGA study, which makes it difficult to perform more detailed subgroup analyses such as that carried out in the pivotal study (low-grade endometrioid versus high-grade endometrioid; serous versus clear cell versus carcinosarcoma) (5, 27). Further studies in a more extensive Brazilian series of endometrioid and non-endometrioid histologies are warranted to compare the differences in molecular subgroups among them.
In our study, the concordance and accuracy comparing ProMisE and molecular classifiers were 86.8% and 87%, respectively. Two studies, one Canadian led by Jessica McAlpine (8), and the other Chinese led by Jinaliu Wang (28), evaluated the comparison between two methodologies, the traditional ProMisE classifier and another using next-generation sequencing (NGS) molecular classifier (ProMisE NGS) and found slightly higher values, probably due to higher number of cases assessed. The Canadian study identified a concordance rate of 97% (159/164), whereas in the Chinese study, this rate was 94.1% (451/479) (8, 28). Concerning the MSI, we evaluated using a PCR-based approach previously validated at BCH for distinct tumor types (18, 20, 29, 30). The concordance rate was 86.8% (99/114) and is in accordance with reported discrepancies in methodological agreement in endometrial cancer. Dedeurwaerdere and colleagues evaluated three different molecular techniques, including one using PCR, to compare with immunohistochemistry results to define colorectal and EC patients with MSI. The concordance rate for patients with colorectal cancer was 100%, while for patients with EC, it ranged from 58% to 75% (31). A Spanish study also evaluated different methodologies for defining MMR status (IHC, PCR, NGS) in EC. The results showed discordance rates among the three techniques (32), which in part could be due to the known discordant behavior of the MSH6 pattern loss (33). McConechy et al. demonstrated a 93.3% concordance rate comparing pentaplex mono and di-nucleotide PCR tests for MSI with MMR status by IHC, suggesting that further studies are needed to define the best diagnostic technique for MMRd in EC (34).
The concordance rate for p53 by IHC and TP53 sequencing by NGS was 90.3%, similar to other reports. Singh et al. conducted a study with just over 200 patients, comparing p53 status by IHC and TP53 sequencing by NGS, demonstrating an overall agreement rate of 92.3% (35). Another study evaluating patients with high-risk EC in the PORTEC-3 trial reported a 90.7% concordance rate between p53 IHC and TP53 NGS analysis (36).
Although the ProMisE methodology has been well documented internationally (6), there has never been a report of its use in Brazilian endometrial cancer patients. Furthermore, we conducted a second classification, based only on molecular methodologies, and carried it out in a public hospital in Brazil. Additionally, this is a prospective cohort where we included all cases referred for treatment at the BCH, thus minimizing selection bias that could influence the results demonstrated. Of note, the entire therapeutic definition of the patients was discussed in a weekly tumor board of the gynecologic oncology department of the aforementioned hospital, thus minimizing possible influences on the oncological outcomes of these patients.
Despite our study’s significant findings and relevance, it also exhibits some limitations. The number of patients included is a limiting factor for a large and significant statistical association, as is the short follow-up time to define oncological outcomes in patients with EC. Furthermore, the molecular approach using distinct methodologies is not ideal, and we are currently working on a single NGS assay to assess all the biomarkers of the ProMisE classifier.
5 Conclusion
In this prospective cohort of endometrial cancer treated at a single public institution in Brazil, we successfully implemented the ProMisE classification for all patients and demonstrated its impact on stratifying patients’ outcomes. The molecular subgroups were in line with the international literature, with a slight increase in the proportion of TP53 mutated patients. Furthermore, with the current development of more comprehensive NGS panels, with the inclusion of POLE, TP53 genes, MSI, and other putative actionable endometrial genes, we foresee that a single NGS methodology would be the most effective, quick, objective, and cost-effective approach for endometrial cancer molecular classification.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by the Institutional BCH Ethical Review Board. The study was conducted in accordance with the local legislation and institutional requirements. The informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
DAPA: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MB: Data curation, Formal analysis, Writing – original draft, Writing – review & editing. FdP: Data curation, Formal analysis, Writing – original draft, Writing – review & editing. GB: Data curation, Formal analysis, Writing – original draft, Writing – review & editing. GT: Formal analysis, Writing – original draft, Writing – review & editing. MdR: Formal analysis, Writing – original draft, Writing – review & editing. FB: Formal analysis, Writing – original draft, Writing – review & editing. CA: Writing – original draft, Writing – review & editing. VA: Writing – original draft, Writing – review & editing. AH: Writing – original draft, Writing – review & editing. WH: Data curation, Formal analysis, Writing – original draft, Writing – review & editing. RS: Writing – original draft, Writing – review & editing. RMR: Conceptualization, Formal analysis, Funding acquisition, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. RDR: Conceptualization, Formal analysis, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The present study was funded by the Public Ministry of Labor Campinas (Research, Prevention, and Education of Occupational Cancer), and Barretos Cancer Hospital, Brazil. RMR is the recipient of the National Council for Scientific and Technological Development (CNPq, Brazil) Productivity Fellowship.
Conflict of interest
Author DAPA works at the company Oncoclínicas&CO.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1503901/full#supplementary-material
Supplementary Figure 1 | Illustrative cases of endometrioid carcinomas with different molecular subtypes (20X objective). (A) No specific molecular profile (NSMP); (B) p53 abnormal (p53abn); (C) POLE mutated (POLEmut); and (D) Mismatch repair deficient (MMRd).
Supplementary Figure 2 | Sanger sequencing electropherogram of hotspot POLE mutations.
Supplementary Figure 3 | An illustrative case of mismatch repair proteins by immunohistochemistry. (A, B) reveal MSH2 and MSH6 intact nuclear expression by tumor cells, as (C, D) reveal PMS2 and MLH1 loss of nuclear expression, respectively (20X objective).
Supplementary Figure 4 | Illustrative cases with P53 abnormal immunoexpression: overexpression in (A), demonstrated by strong and diffuse nuclear positivity in more than 90% of tumor cells; null pattern in (B), lack of nuclear or cytoplasmic expression in tumor cells (10X objective).
Supplementary Figure 5 | Molecular fragment analysis for MSI with hexaplex panel marker. (A) Sample with presence of MSI (MSI-H). (B) Sample with absence of MSI (MSS). Arrow indicates the allele outside of the QMVR (gray zone) demonstrating instability.
Supplementary Figure 6 | Molecular analysis of TP53 in endometrial cancer patients. (A) Sequenced reads of a TP53 mutation depicted in Integrative Genomics Viewer (IGV) tool. (B) Sanger sequencing electropherogram of a TP53 mutation previously identified in NGS test. (C) Lollipop plot of all TP53 mutations identified in EC patients.
References
1. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834
2. Estimativa 2023: Incidência de Câncer no Brasil. Rio de Janeiro: INCA - Instituto Nacional de Câncer José Alencar Gomes da Silva (2022). Available at: www.inca.gov.br/estimativa/2022/ (accessed September 19, 2024).
3. Paulino E, de Melo AC, Silva-Filho AL, Maciel LF, Thuler LCS, Goss P, et al. Panorama of gynecologic cancer in Brazil. JCO Glob Oncol. (2020) 6:1617–30. doi: 10.1200/GO.20.00099
4. Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecol Oncol. (1983) 15:10–7. doi: 10.1016/0090-8258(83)90111-7
5. Kandoth C, Schultz N, Cherniack AD, Akbani R, Liu Y, Shen H, et al. Integrated genomic characterization of endometrial carcinoma. Nature. (2013) 497:67–73. doi: 10.1038/nature12113
6. Talhouk A, McConechy MK, Leung S, Li-Chang HH, Kwon JS, Melnyk N, et al. A clinically applicable molecular-based classification for endometrial cancers. Br J Cancer. (2015) 113:299–310. doi: 10.1038/bjc.2015.190
7. Stelloo E, Bosse T, Nout RA, MacKay HJ, Church DN, Nijman HW, et al. Refining prognosis and identifying targetable pathways for high-risk endometrial cancer; a TransPORTEC initiative. Mod Pathol. (2015) 28:836–44. doi: 10.1038/modpathol.2015.43
8. Jamieson A, McConechy MK, Lum A, Leung S, Thompson EF, Senz J, et al. Harmonized molecular classification; assessment of a single-test ProMisE NGS tool. Gynecol Oncol. (2023) 175:45–52. doi: 10.1016/j.ygyno.2023.05.073
9. Concin N, Matias-Guiu X, Vergote I, Cibula D, Mirza MR, Marnitz S, et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer. (2021) 31:12–39. doi: 10.1136/ijgc-2020-002230
10. Berek JS, Matias-Guiu X, Creutzberg C, Fotopoulou C, Gaffney D, Kehoe S, et al. FIGO staging of endometrial cancer: 2023. Int J Gynaecol Obstet. (2023) 162:383–94. doi: 10.1002/ijgo.v162.2
11. van den Heerik A, Horeweg N, Nout RA, Lutgens L, van der Steen-Banasik EM, Westerveld GH, et al. PORTEC-4a: international randomized trial of molecular profile-based adjuvant treatment for women with high-intermediate risk endometrial cancer. Int J Gynecol Cancer. (2020) 30:2002–7. doi: 10.1136/ijgc-2020-001929
12. RAINBO Research Consortium. Refining adjuvant treatment in endometrial cancer based on molecular features: the RAINBO clinical trial program. Int J Gynecol Cancer. (2022) 33:109–17. doi: 10.1136/ijgc-2022-004039
13. Madden EB, Hindorff LA, Bonham VL, Akintobi TB, Burchard EG, Baker KE, et al. Advancing genomics to improve health equity. Nat Genet. (2024) 56:752–57. doi: 10.1038/s41588-024-01711-z
14. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J BioMed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
15. Talhouk A, McConechy MK, Leung S, Yang W, Lum A, Senz J, et al. Confirmation of ProMisE: A simple, genomics-based clinical classifier for endometrial cancer. Cancer. (2017) 123:802–13. doi: 10.1002/cncr.v123.5
16. Berardinelli GN, Scapulatempo-Neto C, Durães R, Antônio de Oliveira M, Guimarães D, Reis RM. Advantage of HSP110 (T17) marker inclusion for microsatellite instability (MSI) detection in colorectal cancer patients. Oncotarget. (2018) 9:28691–701. doi: 10.18632/oncotarget.25611
17. Köbel M, Piskorz AM, Lee S, Lui S, LePage C, Marass F, et al. Optimized p53 immunohistochemistry is an accurate predictor of TP53 mutation in ovarian carcinoma. J Pathol Clin Res. (2016) 2:247–58. doi: 10.1002/cjp2.v2.4
18. Berardinelli GN, Durães R, Mafra da Costa A, Bragagnoli A, Antônio de Oliveira M, Pereira R, et al. Association of microsatellite instability (MSI) status with the 5-year outcome and genetic ancestry in a large Brazilian cohort of colorectal cancer. Eur J Hum Genet. (2022) 30:824–32. doi: 10.1038/s41431-022-01104-y
19. Britton H, Huang L, Lum A, Leung S, Shum K, Kale M, et al. Molecular classification defines outcomes and opportunities in young women with endometrial carcinoma. Gynecol Oncol. (2019) 153:487–95. doi: 10.1016/j.ygyno.2019.03.098
20. Campanella NC, Berardinelli GN, Scapulatempo-Neto C, Viana D, Palmero EI, Pereira R, et al. Optimization of a pentaplex panel for MSI analysis without control DNA in a Brazilian population: correlation with ancestry markers. Eur J Hum Genet. (2014) 22:875–80. doi: 10.1038/ejhg.2013.256
21. Cavagna RO, Pinto IA, Escremim de Paula F, Berardinelli GN, Sant’Anna D, Santana I, et al. Disruptive and truncating TP53 mutations are associated with African-ancestry and worse prognosis in Brazilian patients with lung adenocarcinoma. Pathobiology. (2023) 90:344–55. doi: 10.1159/000530587
22. Kommoss S, McConechy MK, Kommoss F, Leung S, Bunz A, Magrill J, et al. Final validation of the ProMisE molecular classifier for endometrial carcinoma in a large population-based case series. Ann Oncol. (2018) 29:1180–8. doi: 10.1093/annonc/mdy058
23. Henry CE, Phan K, Orsman EJ, Kenwright D, Thunders MC, Filoche SK. Molecular profiling of endometrial cancer: an exploartory study in Aotearoa, New Zealand. Cancers (Basel). (2021) 13:5641. doi: 10.3390/cancers13225641
24. Dankai W, Pongsuvareeyakul T, Phinyo P, Tejamai C, Teerapakpinyo C, Cheewakriangkrai C, et al. Molecular-based classification of endometrial carcinoma in Northern Thailand: impact on prognosis and potential for implementation in resource-limited settings. BMC Womens Health. (2023) 23:605. doi: 10.1186/s12905-023-02677-6
25. Asami Y, Kato MK, Hiranuma K, Matsuda M, Shimada Y, Ishikawa M, et al. Utility of molecular subtypes and genetic alterations for evaluating clinical outcomes in 1029 patients with endometrial cancer. Br J Cancer. (2023) 128:1582–91. doi: 10.1038/s41416-023-02203-3
26. Ribeiro AG, Ferlay J, Vaccarella S, Latorre M, Fregnani J, Bray F. Cancer inequalities in incidence and mortality in the State of São Paulo, Brazil 2001-17. Cancer Med. (2023) 12:16615–25. doi: 10.1002/cam4.v12.15
27. Santoro A, Angelico G, Travaglino A, Inzani F, Arciuolo D, Valente M, et al. New pathological and clinical insights in endometrial cancer in view of the updated ESGO/ESTRO/ESP guidelines. Cancers (Basel). (2021) 13:2623. doi: 10.3390/cancers13112623
28. Kang N, Zhang X, Wang Z, Dai Y, Lu S, Su W, et al. Validation of a one-step genomics-based molecular classifier for endometrial carcinoma in a large Chinese population. Pathol Res Pract. (2024) 254:155152. doi: 10.1016/j.prp.2024.155152
29. De Marchi P, Berardinelli GN, Cavagna RO, Pinto IA, da Silva FAF, da Silva VD, et al. Microsatellite instability is rare in the admixed Brazilian population of non-small cell lung cancer: A cohort of 526 cases. Pathobiology. (2022) 89:101–6. doi: 10.1159/000520023
30. Nshizirungu JP, Bennis S, Mellouki I, Sekal M, Benajah DA, Lahmidani N, et al. Reproduction of the cancer genome atlas (TCGA) and Asian cancer research group (ACRG) gastric cancer molecular classifications and their association with clinicopathological characteristics and overall survival in Moroccan patients. Dis Markers. (2021) 2021:9980410. doi: 10.1155/2021/9980410
31. Dedeurwaerdere F, Claes KB, Van Dorpe J, Rottiers I, van der Meulen J, Breyne J, et al. Comparison of microsatellite instability detection by immunohistochemistry and molecular techniques in colorectal and endometrial cancer. Sci Rep. (2021) 11:12880. doi: 10.1038/s41598-021-91974-x
32. Mendiola M, Heredia-Soto V, Ruz-Caracuel I, Baillo A, Ramon-Patino JL, Escudero FJ, et al. Comparison of methods for testing mismatch repair status in endometrial cancer. Int J Mol Sci. (2023) 24:14468. doi: 10.3390/ijms241914468
33. van der Werf’t Lam AS, Terlouw D, Tops CM, van Kan MS, van Hest LP, Gille HJP, et al. Discordant staining patterns and microsatellite results in tumors of MSH6 pathogenic variant carriers. Mod Pathol. (2023) 36:100240. doi: 10.1016/j.modpat.2023.100240
34. McConechy MK, Talhouk A, Li-Chang HH, Leung S, Huntsman DG, Gilks CB, et al. Detection of DNA mismatch repair (MMR) deficiencies by immunohistochemistry can effectively diagnose the microsatellite instability (MSI) phenotype in endometrial carcinomas. Gynecol Oncol. (2015) 137:306–10. doi: 10.1016/j.ygyno.2015.01.541
35. Singh N, Piskorz AM, Bosse T, Jimenez-Linan M, Rous B, Brenton JD, et al. p53 immunohistochemistry is an accurate surrogate for TP53 mutational analysis in endometrial carcinoma biopsies. J Pathol. (2020) 250:336–45. doi: 10.1002/path.v250.3
Keywords: endometrial cancer, molecular classification, ProMisE, biomarkers, Latin-America
Citation: Andrade DAP, Bonatelli M, de Paula FE, Berardinelli GN, Teixeira GR, dos Reis MT, Barbin FF, Andrade CEMdC, Aguiar VP, Hermoza AD, Hirai WY, Schmidt RL, Reis RM and dos Reis R (2024) Implementation of the ProMisE classifier and validation of its prognostic impact in Brazilian endometrial carcinomas. Front. Oncol. 14:1503901. doi: 10.3389/fonc.2024.1503901
Received: 29 September 2024; Accepted: 25 November 2024;
Published: 13 December 2024.
Edited by:
Sufian Zaheer, Vardhman Mahavir Medical College & Safdarjung Hospital, IndiaReviewed by:
Giuseppe Angelico, Agostino Gemelli University Polyclinic (IRCCS), ItalyJianing Li, Heilongjiang University of Chinese Medicine, China
Copyright © 2024 Andrade, Bonatelli, de Paula, Berardinelli, Teixeira, dos Reis, Barbin, Andrade, Aguiar, Hermoza, Hirai, Schmidt, Reis and dos Reis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ricardos dos Reis, ZHJyaWNhcmRvcmVpc0BnbWFpbC5jb20=