 Weronika Pawlik
Weronika Pawlik Joanna Strzemecka
Joanna Strzemecka Albert Stachura
Albert Stachura Aleksandra Królak
Aleksandra Królak Tomasz Ociepa
Tomasz Ociepa- 1Department of Pediatrics, Haemato-Oncology and Gastroenterology, Pomeranian Medical University, Szczecin, Poland
- 2Department of Methodology, Medical University of Warsaw, Warsaw, Poland
Hematologic malignancies are a well-known risk factor for cardiovascular disease development. Chemotherapeutic protocols commonly include intensive fluid therapy (IFT), which may negatively influence the cardiovascular system and predispose to arterial hypertension. This study aims to evaluate atrial natriuretic peptide (NT-proBNP), high-sensitivity troponin T (hs-TnT), and changes in blood pressure in children with hematological malignancies undergoing intensive fluid therapy. This prospective cohort study comprised thirteen children. 24-h ambulatory blood pressure monitoring (ABPM) and concentrations of NT-proBNP and hs-TnT were performed on the first day of IFT and during follow-up. There were no statistically significant differences in 24-h, daytime, night-time systolic (SBP) and diastolic blood pressure (DBP), SBP and DBP dipping, and the number of non-dippers during intensive fluid therapy compared to the control points. The mean NT-proBNP concentration at 24 h was 321.27 ± 318.08 pg/mL and was significantly higher compared with baseline (79.13 ± 105.42 pg/mL) and follow-up (175.92 ± 241.48 pg/mL); p-values 0.005 and p = 0.006 respectively. Troponin T concentration at 24 h was not significantly different compared with baseline and follow-up. These results show no significant influence of intensive fluid therapy on blood pressure profile. In contrast, an increase in NT-proBNP values 24 h after the start of fluid therapy may reflect the impact of fluid overload on the cardiovascular system.
1 Introduction
Elevated blood pressure (BP) and cardiac failure, as evidenced by studies, are common complications that occur after long-term anti-cancer therapy (1–5). The developing cardiovascular system in children is highly susceptible to the toxic effects of chemotherapy (e.g., anthracyclines), and damage of the blood vessel wall, including the endothelium (6, 7). The prevalence of atrial hypertension (AH) is significantly increased in a group of pediatric patients with hematopoietic and lymphatic malignancies (8). It is also well known that the rate of AH in childhood acute lymphoblastic leukemia (ALL) survivors is significantly higher than in the healthy pediatric population (9, 10).
Fluid overload and hypertension are related health conditions that often coexist, creating a complex interplay between fluid balance and blood pressure regulation. Fluid overload occurs when the body accumulates an excessive amount of extracellular fluid (11). This can result from various factors such as kidney dysfunction, heart failure, liver disease, or excessive fluid intake (12). In arterial hypertension, fluid overload contributes to an increased blood volume, exacerbating the pressure on arterial walls. Understanding the relationship between these two conditions is crucial for effective management and prevention of associated complications.
Therapeutic protocols used to treat children with leukemia or lymphoma include continuous coadministration of intravenous fluids. Numerous side effects of chemotherapy, mainly when cyclophosphamide, high-dose cytarabine, or high-dose methotrexate are given, may be minimized using intensive intravenous fluid therapy (13). Intravenous hydration of 3,000 mL/m2/day is usually recommended even several days after the drug administration, far exceeding a child's standard fluid requirement (14). However, the impact of such overhydration needs to be studied more, especially if it could increase the risk of cardiovascular complications. It is suggested that electrolyte disturbances and unrecognized fluid overload may negatively influence the cardiovascular system, predispose to arterial hypertension development, left ventricular hypertrophy and at last increases morbidity in patients with leukemia and lymphomas (15, 16).
A meta-analysis involving 7,507 children demonstrated an association between fluid overload and poorer outcomes of the underlying disease, worsening respiratory function, development of acute kidney injury, and mortality (17). Other observations also support an increased risk of developing respiratory adverse events in patients who are overhydrated during the induction phase of treatment for acute myeloid leukemia (18). What is more a study of patients with chronic kidney disease regularly undergoing hemodialysis demonstrated an association of chronic hypervolemia with blood pressure values and left ventricular hypertrophy (19–23). It appears that HSCT procedure in children who had a >10% overload of fluids during the initiation of hemodialysis increased the level of mortality (24). Conversely, some studies showed that even very aggressive hydration brings more positive outcomes than delay in methotrexate elimination (25–27).
For proper diagnosis and monitoring of AH, ambulatory blood pressure monitoring (ABPM) is currently considered the gold standard (28, 29). In children, a single blood pressure measurement has been shown to be significantly different from measurements obtained by ABPM in up to 40% of cases (30). ABPM, in addition to its ability to measure blood pressure almost continuously, allows assessment of blood pressure variability (BPV) throughout the day and night (31). Sustained increases in BPV are associated with increased incidence and progression of organ damage (renal dysfunction, left ventricular hypertrophy and cardiac dysfunction) (32–34).
Moreover, to assess the degree of myocardial overload or damage, methods include measurement of N-terminal natriuretic propeptide type B (NT-proBNP) and high-sensitivity troponin T (hs-TnT) (35). Changes in NT-pro BNP and hs-TnT may reflect the initial stage of cardiotoxicity even before the onset of signs suggestive of heart failure visible in imaging studies (echocardiography) (36, 37). NT-pro BNP levels have been shown to reflect left ventricular volume or pressure overload (38). Sommer et al. demonstrated the relationship between NT-proBNP levels and the degree of hydration in patients with heart disease and confirmed that an increased concentration of NT-proBNP is a factor in a poorer prognosis (39). It was also found that using NT-proBNP to monitor the hydration status of hemodialysis patients may have prognostic significance (40, 41). Highly sensitive troponin T (hs-TnT) is a marker of acute myocardial ischemia (42, 43). Increased troponin T levels and its association with an increased risk of cardiomyopathy have been demonstrated in children with ALL receiving anthracycline drugs (44). Higher hs-TnT levels and poorer left ventricular function have also been found in adults treated for childhood acute lymphoblastic leukemia (45).
This pilot study aimed to evaluate the impact of intensive intravenous fluid therapy on blood pressure values and biomarkers of myocardial function - atrial natriuretic peptide (NT-proBNP) and high-sensitivity troponin T (hs-TnT) in children with hematologic and lymphoid malignancies.
2 Material and methods
2.1 Study design
This study was conducted as a hospital-based single-arm longitudinal observational study and was granted the approval by the Bioethical Committee of Pomeranian Medical University in Szczecin, Poland (approval no. KB-0012/46/2021-A-3381). Informed consent was obtained from all parents or legal guardians and all children older than 13 years in compliance with the Declaration of Helsinki.
2.2 Setting
The analysis included the results of the NT-proBNP, hs-TnT concentrations and 24-h blood pressure monitoring (ABPM) performed on children aged 3–18 on the day when intensive fluid therapy was administered in parallel with cytostatic drugs. Patients included in the study were hospitalized in the Department of Pediatric, Hemato-Oncology and Gastroeneterology of Pomeranian Medical University in Szczecin, from December 2021 to May 2023 and met the inclusion criteria of the study. The study group served as a control group, and the control point was set weeks further in the therapy plan when children had not received intensive fluid therapy for at least 14 days. 24-h ABPM and blood sampling for NT-proBNP and hs-TnT concentrations measurements were performed again. Data were collected from December 2021 to May 2023.
2.3 Participants
The study group comprised 13 patients (five girls and eight boys, aged 3–18 years, mean 10.21 ± 5.51 years) with newly diagnosed leukemia or lymphoma, in whom intensive fluid therapy of 3 L/m2 of body surface/24 h was given to increase elimination and minimize cytostatics toxicity. Exclusion criteria were as follows: age above 18 years, diagnosed arterial hypertension, treatment with angiotensin-converting-enzyme (ACE) inhibitors or other antihypertensive drugs, a chronic or severe medical condition possibly resulting in the development of arterial hypertension (e.g., renal disorders, hyperthyroidism, congenital heart disease).
2.4 Variables and data sources
All patients underwent a complete physical examination with an assessment of weight, height, and body mass index (BMI). During fluid therapy, each patient had a fluid balance carried out. When the fluid balance exceeded 250 mL/m2, children were given a loop diuretic (Furosemide) at a dose of 0.5 mg/kg body weight.
Blood samples for NT-proBNP and hs-TnT concentrations were collected on admission and 24 h after the start of intensive fluid treatment. Pediatric reference intervals and cut-off points for NT-proBNP and hs-cTnT were determined in a study on a large group of healthy children without coexisting clinical indications (46). For children aged one to nine, the upper limit (>90%) was set at 178 ng/L for NT-proBNP and 9 ng/L for troponin T concentrations. These cut-off points were used in our study.
Blood pressure assessments were performed using Spacelabs ABP model 90227 OnTrak, the ambulatory blood pressure monitor (Spacelabs Healthcare Ltd) validated for children. An appropriately sized cuff was chosen out of three available sizes. The ABPM device was placed on the child's non-dominant arm two hours before intensive fluid therapy to allow the child to perform daily activities. Measurements were taken automatically every 20 min during the day (8:00 am–10:00 pm), and every 30 min during sleep (10:01 pm–7:59 am). The ABPM recording was considered acceptable when a minimum of correctly performed measurements was at least 70% - a minimum of 20 readings during the day and 7 at rest. Blood pressure values were recorded during the 24 h (daytime and night-time, respectively) as systolic, diastolic, and mean arterial blood pressure (MAP).
Blood pressure (BP) in children is significantly affected by both gender and age. While reference values for ambulatory blood pressure monitoring (ABPM) in pediatrics exist, using them in standard statistical procedures can be challenging due to the uneven distribution of BP in children. Reference values were established by Wuhl et al. based on ABPM values in 949 healthy children and adolescents aged 5–20 years (47). ABPM values (systolic, diastolic and mean arterial pressure; MAP) at Wuhl et al. work were recalculated and expressed as 24h-SDS (standard deviation score), day-time-SDS as well as night-time-SDS using the LMS (least mean squares) formula for SDS analysis: SDS = {[Y/M(t)]L(t)-1}/[L(t) × S(t)] where Y is the child's individual arterial blood pressure (systolic, diastolic or mean), M(t) is median of Y, L(t) is the measure of skewness and S(t) is the coefficient of variation (47, 48).
Statement from the American Heart Association confirms that the ABP values in the Wühl dataset remain the best available reference (49). Kliknij lub naciśnij tutaj, aby wprowadzić tekst. Due to the small sample size of this study, we compare the ABPM results of our patients based on the reference values created by Wuhl et al. standardizing them using the LMS method.
2.5 Statistical methods
All continuous variables were presented as means ± standard deviations unless otherwise indicated. Categorical variables were presented as absolute numbers and percentages. Due to the small number of participants at the preliminary stage of the study, non-parametric tests were used. For continuous variables (NT-proBNP, hs-TnT concentrations), the Kruskal-Walli's test was used to compare outcome measures between the studied time points. In case of significant between-group differences, a post hoc paired Wilcoxon test was used for pairwise comparisons. The student's t-test was used to compare the means of measured blood pressure values. The Wilcoxon signed-rank test was used to analyze non-parametric paired data (SD score of ambulatory blood pressure measurement). The threshold for statistical significance was assumed at a p-value below 0.05. For multiple pairwise comparisons, the Bonferroni correction was applied. In the case of three between-group comparisons, the statistical significance threshold was lowered to 0.0167.
3 Results
Thirteen children under treatment were enrolled in the study. The mean age of the study group was 10.21 ± 5.51 years (range 3–18), and there was a predominance of males (62.0%). The mean height was 1.4 ± 0.32 meters (range 1–1.79), and the mean BMI was 17.89 ± 4.25 (range 13.11–27.26). Only one child was obese (BMI above 97 percentile), and two of the patients were underweight (BMI under 3 percentile). Eight (62.0%) of the patients had acute lymphoblastic leukemia, three (23.0%) patients had non-Hodgkin lymphoma (NHL), and two (15.0%) patients had Hodgkin lymphoma (HL). Patients’ characteristics are presented in Table 1.
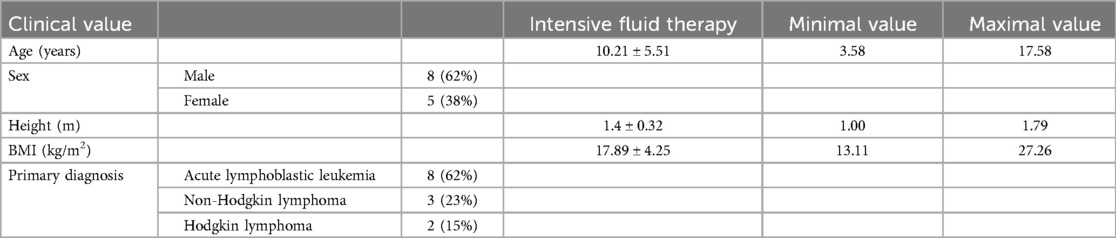
Table 1. Patient's characteristics.
There were no statistically significant differences in 24-h, daytime, night-time systolic (SBP) and diastolic blood pressure (DBP), MAP, and HR recorded during intensive fluid therapy compared to the control point. There were no significant differences in SBP and DBP dipping and the number of non-dippers during IFT compared to the control point. These data are presented in Table 2. There were also no significant differences in 24-h MAP, HR, systolic, and diastolic blood pressure SDS during IFT compared to the control point. These data are presented in Table 3.
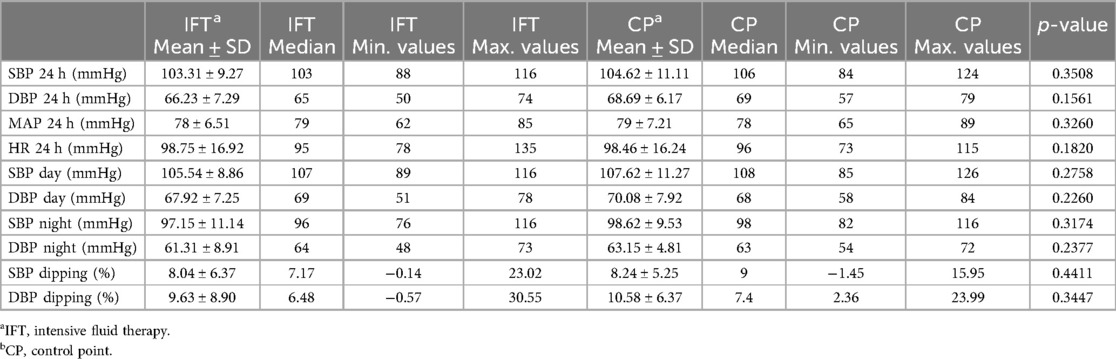
Table 2. Comparison of ambulatory blood pressure monitoring results during intensive fluid therapy and in control point.
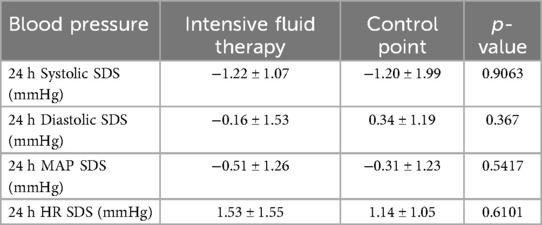
Table 3. Standard deviation scores of ABPM.
NT-proBNP concentrations differed significantly between time points (p = 0.022); therefore, post-hoc pairwise analyses were performed. The mean NT-proBNP concentration at 24 h was 321.27 ± 318.08 pg/mL and was significantly higher compared with baseline (79.13 ± 105.42 pg/mL) and follow-up (175.92 ± 241.48 pg/mL); p-values 0.005 and p = 0.006 respectively. The median NT-proBNP concentration at baseline was 33.4 pg/mL (range: 5.92–380 pg/mL), at 24 h was 188 pg/mL (range 13, 4–1,181 pg/mL) and at follow-up was 56 pg/mL (range: 12.9–729 pg/mL). These data are presented in Figure 1. Troponin T concentration at 24 h was 16.26 ± 14.13 ng/L and was not significantly different compared with baseline (18.47 ± 14.13 ng/L) and follow-up (15.27 ± 11 ng/L); p = 0.84. The median Troponin-T concentration at baseline was 11.5 ng/L (range: 3–53.1 ng/L), at 24 h was 10.1 ng/L (range 6.69–53.5 ng/L) and at follow-up was 9.63 pg/mL (range: 3–37.2 ng/L). These data are presented in Figure 2.
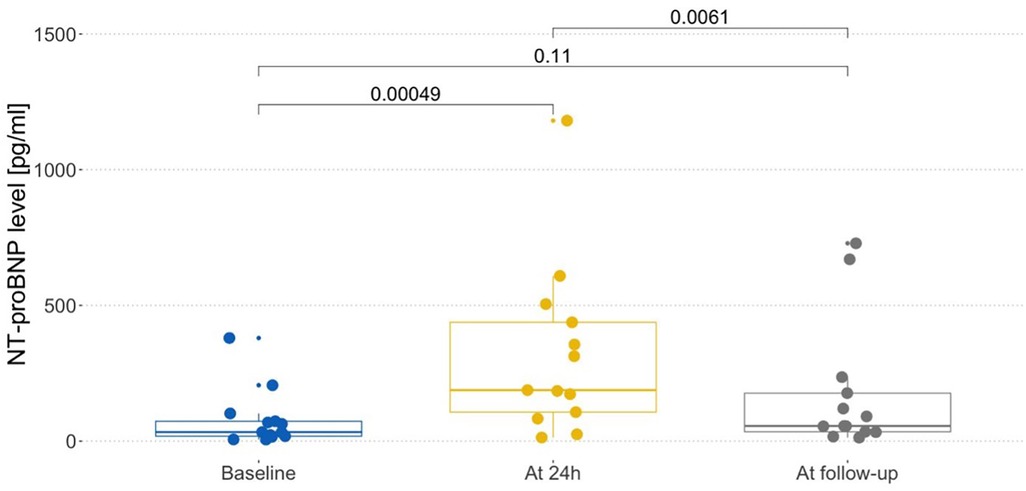
Figure 1. NTproBNP level in different time points.
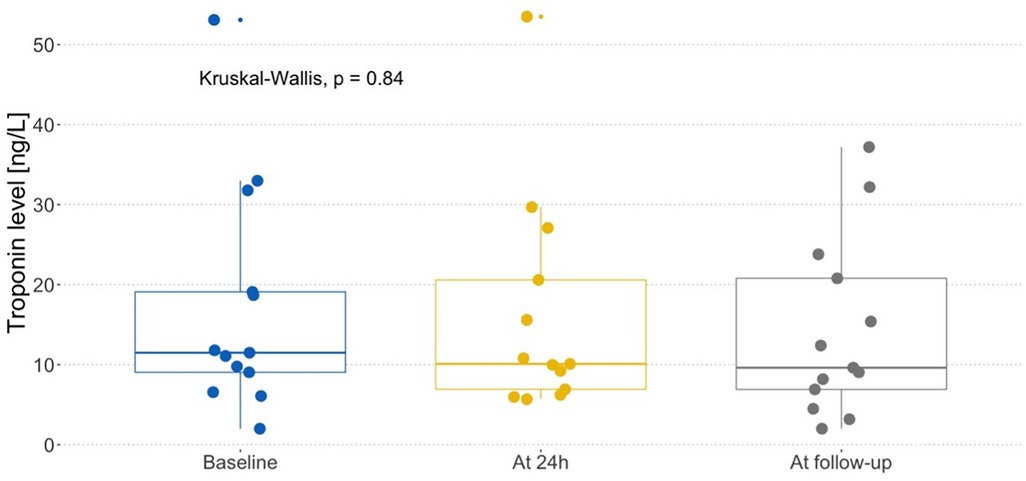
Figure 2. Troponin T level in different time points.
4 Discussion
Pediatric patients treated for leukemia and lymphomas are seven times more likely to die from complications, compared to healthy individuals (50). Furthermore, childhood cancer survivors have a higher risk of developing heart failure, coronary heart disease, heart valve insufficiency or stenosis, and inflammation of the heart epithelium after intensive systemic treatment, than non-cancer survivors (51–54). The burden on the heart is multifactorial, caused by various components of anticancer treatment, such as steroids, anthracycline chemotherapy, asparaginase administration, and concomitant fluids overload (51, 55). In severe sepsis, fluid boluses increase arterial blood pressure and lead to a significant decrease in HR and significant increases in cardiac output (56). However, it all may lead to many late-onset comorbidities (57).
Despite the routine use of IFT in children with hematologic and lymphoid malignancies at various stages of chemotherapy, its direct effect on the cardiovascular system, including blood pressure and its profile, as well as cardiac biomarkers, has yet to be studied. The standard is careful monitoring of the patient's water balance, control of renal and electrolyte parameters, and occasional (with varying frequency) blood pressure measurement. However, these procedures do not elucidate the direct effect of intensive fluid therapy on the cardiovascular system in children with hematological malignancies.
Some published papers confirm an increased prevalence of hypertension detected by ABPM in children with hematological malignancies a few years after diagnosis (4, 5, 58, 59). Moreover, Kumar et al. showed impaired nocturnal dipping, which may be evidence of an increased risk for cardiovascular ischemic events in children surviving acute lymphoblastic leukemia (59). Conversely, Hsiao W. et al. showed a significant reduction in median blood pressure loads many years after first diagnosis, which may reflect the transient nature of abnormalities in blood pressure parameters after the treatment termination (58).
This study is one of the few showing the profile of ambulatory 24-h blood pressure measurement in patients treated for hematologic malignancy, but to the best of the author's knowledge, the first one that aims to analyze diurnal changes in blood pressure in children undergoing intensive fluid therapy.
Our ABPM results show no statistically significant differences between the group of patients intensively hydrated and the controls. It was logical to expect that recorded ABPM values (means and SDS) should be higher during IFT than at the control point. However, we found no significant differences in 24-h, daytime, night-time systolic (SBP) and diastolic (DBP) blood pressure, MAP, and HR recorded during intensive fluid therapy compared to the control point. We also found no significant differences in 24-h MAP, HR, systolic, and diastolic blood pressure SDS in the same time points. True is that each patient received a loop diuretic during intensive hydration when the fluid balance exceeded 250 mL/m2. It needs further analysis if it would influence the values of recorded blood pressure in the patient's cohort. Small study groups may significantly impact results in both groups of patients. Although intensive fluid treatment continued during the night, we found no significant difference in SBP and DBP dipping and the number of non-dippers during IFT compared to the control point. Fluid overload and cardiac biomarkers are intricately linked, providing valuable insights into the cardiovascular status of patients (60). In fluid overload, the heart releases more NT-proBNP to counteract the increased workload. Troponins are elevated in conditions causing myocardial strain, including heart failure. Compromised cardiac function can lead to myocardial injury, triggering an increase in troponin levels.
So far, N-terminal pro-brain natriuretic peptide has been used as a prognostic marker for response to intensive chemotherapy and overall survival of patients with hematological malignancies (61–64). However, in the context of heart failure, NT-proBNP and troponin T was usually investigated to assess the development of anthracycline-induced cardiomyopathy (3, 36, 45, 65). This study investigated changes in cardiac biomarkers during excessive fluid supply and post-treatment follow-up, separately of the supply of drugs directly causing cardiotoxicity.
Our study showed a statistically significant increase in NT-proBNP concentration after 24 h of intensive fluid treatment (p < 0.005). Moreover, mean NT-proBNP concentration at this time was well above the upper limit (321.27 ± 318.08 pg/mL) established for the studied age group. It is also worth mentioning that the NT-proBNP levels had normalized by follow-up. Significant increase of NT-proBNP after 24-h of fluid therapy reflect the expected left ventricular and pressure overload, although it proved to be temporary.
The mean pre-IFT troponin T level was not significantly different from the concentration recorded after 24 h of intensive fluid treatment (p = 0.84).
It was a single-center, prospective study with a relatively small sample size, which limits generalizability. It is necessary to conduct the survey for several consecutive years to capture enough patients. For this reason, we conducted a preliminary study, which was necessary to minimize the risk of errors and adjust the methodology with subsequent patients.
These results may confirm only the transient influence of intensive fluid therapy on myocardial overload associated with acute neurohumoral activation (temporary elevation of NT-proBNP) indicating acute subclinical cardiotoxicity. If repeated or prolonged IFT significantly impairs left ventricular ejection fraction (LVEF) in children receiving intensive fluid treatment, it still needs to be assessed. Taking all these data into consideration, we speculate that IFT, if properly monitored and managed, has minimal impact on blood pressure and dipping status in children with a hematopoietic or lymphatic malignant disorder. Intensive fluid therapy should not be restricted, so that many of the adverse effects of cytostatic drugs can be avoided.
Although intensive fluid administration given concomitantly to anticancer treatment in children with hematological malignant conditions seems not to impact blood pressure negatively, an increase in NT-proBNP values 24 h after fluid therapy may reflect the level of fluid overload. If it will lead to further myocardial damage, a larger group of patients and longer follow-ups are needed to verify the accuracy of our findings. This study provides a prelude to further research into the negative effects of intensive therapy during chemotherapy.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Bioethical Committee of Pomeranian Medical University in Szczecin, Poland. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
WP: Conceptualization, Funding acquisition, Investigation, Methodology, Writing – original draft, Writing – review & editing. JS: Investigation, Writing – original draft, Writing – review & editing. AS: Methodology, Visualization, Writing – original draft, Writing – review & editing. AK: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. TO: Conceptualization, Formal Analysis, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Pomeranian Medical University in Szczecin (Grant FSN-122-07-23).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Cohen JB, Brown NJ, Brown SA, Dent S, Van Dorst DCH, Herrmann SM, et al. Cancer therapy-related hypertension: a scientific statement from the American Heart Association. Hypertension. (2023) 80(3):46–57. doi: 10.1161/HYP.0000000000000224
2. Guo X, Qian X, Jin Y, Kong X, Qi Z, Cai T, et al. Hypertension induced by combination therapy of cancer: a systematic review and meta-analysis of global clinical trials. Front Pharmacol. (2021) 12:3–16. doi: 10.3389/FPHAR.2021.712995
3. Sparano JA, Brown DL, Wolff AC. Predicting cancer therapy-induced cardiotoxicity: the role of troponins and other markers. Drug Saf. (2002) 25(5):301–11. doi: 10.2165/00002018-200225050-00001
4. Guler E, Col N, Buyukcelik M, Balat A. Prevalence of hypertension determined by ambulatory blood pressure monitoring (ABPM) and body composition in long-term survivors of childhood cancer. Pediatr Hematol Oncol. (2018) 35(1):1–10. doi: 10.1080/08880018.2018.1425784
5. Roa-Chamorro R, Jaén-Águila F, Puerta-Puerta JM, Torres-Quintero L, González-Bustos P, Mediavilla-García JD. Arterial hypertension assessment in a population with chronic myeloid leukemia. Sci Rep. (2021) 11(1):2–6. doi: 10.1038/s41598-021-94127-2
6. Lazǎr DR, Farcaş AD, Blag C, Neaga A, Zdrenghea MT, Cǎinap C, et al. Cardiotoxicity: a major setback in childhood leukemia treatment. Dis Markers. (2021) 2021:2–5. doi: 10.1155/2021/8828410
7. Bhagat A, Kleinerman ES. Anthracycline-induced cardiotoxicity: causes, mechanisms, and prevention. Adv Exp Med Biol. (2020) 1257:181–92. doi: 10.1007/978-3-030-43032-0_15
8. Gavriilaki E, Gkaliagkousi E, Grigoriadis S, Anyfanti P, Douma S, Anagnostopoulos A. Hypertension in hematologic malignancies and hematopoietic cell transplantation: an emerging issue with the introduction of novel treatments. Blood Rev. (2019) 35:51–8. doi: 10.1016/j.blre.2019.03.003
9. Murphy L, Maloney K, Gore L, Blanchette E. Hypertension in pediatric acute lymphoblastic leukemia patients: prevalence, impact, and management strategies. Integr Blood Press Control. (2022) 15:1. doi: 10.2147/IBPC.S242244
10. Ociepa T, Bartnik M, Zielezińska K, Urasiński T. Prevalence and risk factors for arterial hypertension development in childhood acute lymphoblastic leukemia survivors. J Pediatr Hematol Oncol. (2019) 41(3):175–80. doi: 10.1097/MPH.0000000000001349
11. Masters BR. Harrisons’s principles of internal medicine, 18th edition, two volumes and DVD. Eds: Dan L. Longo, Anthony S. Fauci, dennis L. Kasper, Stephen L. Hauser, J. Larry Jameson and Joseph Loscalzo, ISBN-13: 9780071748896 McGraw Hill. Graefes Arch Clin Exp Ophthalmol. (2012) 250(9):1407–8. doi: 10.1007/s00417-012-1940-9
12. Kitada K, Nishiyama A. Revisiting blood pressure and body fluid status. Clin Sci (Lond). (2023) 137(9):755–67. doi: 10.1042/CS20220500
13. Pui CH. Acute Leukemias Edited by New Directions for Clinical Research. New Jork: Humana Press (2003).
14. Texas Children’s Cancer & Hematology Centers. Pediatric Haematology/Oncology Ward Officer’s Handbook (2015).
15. da Silva AT, Hauschild DB, de Almeida Oliveira LD, de Fragas Hinnig P, Franco Moreno YM, Wazlawik E. Association of hyperhydration evaluated by bioelectrical impedance analysis and mortality in patients with different medical conditions: systematic review and meta-analyses. Clin Nutr ESPEN. (2018) 28:12–20. doi: 10.1016/j.clnesp.2018.08.022
16. Chamoun K, Kantarjian HM, Wang X, Naqvi K, Aung F, Garcia-Manero G, et al. Unrecognized fluid overload during induction therapy increases morbidity in patients with acute promyelocytic leukemia. Cancer. (2019) 125(18):3219–24. doi: 10.1002/cncr.32196
17. Alobaidi R, Morgan C, Basu RK, Stenson E, Featherstone R, Majumdar SR, et al. Association between fluid balance and outcomes in critically ill children: a systematic review and meta-analysis. JAMA Pediatr. (2018) 172(3):257. doi: 10.1001/jamapediatrics.2017.4540
18. Miller LH, Keller F, Mertens A, Klein M, Allen K, Castellino S, et al. Impact of fluid overload and infection on respiratory adverse event development during induction therapy for childhood acute myeloid leukemia. Pediatr Blood Cancer. (2019) 66(12):e27975. doi: 10.1002/pbc.27975
19. Zoccali C, Moissl U, Chazot C, Mallamaci F, Tripepi G, Arkossy O, et al. Chronic fluid overload and mortality in ESRD. J Am Soc Nephrol. (2017) 28(8):2491–7. doi: 10.1681/ASN.2016121341
20. Chazot C, Wabel P, Chamney P, Moissl U, Wieskotten S, Wizemann V. Importance of normohydration for the long-term survival of haemodialysis patients. Nephrol Dial Transplant. (2012) 27(6):2404–10. doi: 10.1093/ndt/gfr678
21. Nescolarde L, Bogónez P, Calpe J, Hernández R, Doñate T, Rosell J. Whole-body and thoracic bioimpedance measurement: hypertension and hyperhydration in hemodialyisis patients. Annual International Conference of the IEEE Engineering in Medicine and Biology—proceedings. Vol 2007 (2007). p. 3593–6. doi: 10.1109/IEMBS.2007.4353108. >
22. Shamszad P, Slesnick TC, Smith EOB, Taylor MD, Feig DI. Association between left ventricular mass index and cardiac function in pediatric dialysis patients. Pediatr Nephrol. (2012) 27(5):835–41. doi: 10.1007/s00467-011-2060-1
23. Ekart R, Kanič V, Pečovnik-Balon B, Bevc S, Dvoršak B, Hojs R. Blood pressure measurements and left ventricular mass Index in hemodialysis patients. Artif Organs. (2012) 36(6):517–24. doi: 10.1111/j.1525-1594.2011.01401.x
24. Lane PH, Mauer SM, Blazar BR, Ramsay NK, Kashtan CE. Outcome of dialysis for acute renal failure in pediatric bone marrow transplant patients. Bone Marrow Transplant. (2016) 13(5):1–23.
25. Connors NJ, Sise ME, Nelson LS, Hoffman RS, Smith SW. Methotrexate toxicity treated with continuous venovenous hemofiltration, leucovorin and glucarpidase. Clin Kidney J. (2014) 7(6):590–2. doi: 10.1093/ckj/sfu093
26. Kawaguchi S, Sichiro F, Murahashi R, Nakashima H, Matsuoka S, Ikeda T, et al. Risk factors for high-dose methotrexate-induced nephrotoxicity. Int J Hematol. (2021) 114(1):79–84. doi: 10.1007/s12185-021-03132-8
27. Xu W, Tang Y, Song H, Shi S, Yang S. Retrospective study on elimination delay of methotrexate in high-dose therapy of childhood acute lymphoblastic leukemia in China. J Pediatr Hematol Oncol. (2007) 29(10):688–93. doi: 10.1097/MPH.0b013e31814d6777
28. Sega R, Facchetti R, Bombelli M, Cesana G, Corrao G, Grassi G, et al. Prognostic value of ambulatory and home blood pressures compared with office blood pressure in the general population: follow-up results from the pressioni arteriose monitorate e loro associazioni (PAMELA) study. Circulation. (2005) 111(14):1777–83. doi: 10.1161/01.CIR.0000160923.04524.5B
29. O’Brien E, Parati G, Stergiou G, Asmar R, Beilin L, Bilo G, et al. European society of hypertension position paper on ambulatory blood pressure monitoring. J Hypertens. (2013) 31(9):1731–68. doi: 10.1097/HJH.0b013e328363e964
30. Samuel JP, Bell CS, Hebert SA, Varughese A, Samuels JA, Tyson JE. Office blood pressure measurement alone often misclassifies treatment status in children with primary hypertension. Blood Press Monit. (2017) 22(6):328–32. doi: 10.1097/MBP.0000000000000299
31. Magdás A, Szilágyi L, Incze A. Can ambulatory blood pressure variability contribute to individual cardiovascular risk stratification? Comput Math Methods Med. (2016) 2016:2–5. doi: 10.1155/2016/7816830
32. Tatasciore A, Zimarino M, Tommasi R, Renda G, Schillaci G, Parati G, et al. Increased short-term blood pressure variability is associated with early left ventricular systolic dysfunction in newly diagnosed untreated hypertensive patients. J Hypertens. (2013) 31(8):1653–61. doi: 10.1097/HJH.0b013e328361e4a6
33. Tatasciore A, Renda G, Zimarino M, Soccio M, Bilo G, Parati G, et al. Awake systolic blood pressure variability correlates with target-organ damage in hypertensive subjects. Hypertension. (2007) 50(2):325–32. doi: 10.1161/HYPERTENSIONAHA.107.090084
34. Manios E, Tsagalis G, Tsivgoulis G, Barlas G, Koroboki E, Michas F, et al. Time rate of blood pressure variation is associated with impaired renal function in hypertensive patients. J Hypertens. (2009) 27(11):2244–8. doi: 10.1097/HJH.0b013e328330a94f
35. Antlanger M, Hecking M, Haidinger M, Werzowa J, Kovarik JJ, Paul G, et al. Fluid overload in hemodialysis patients: a cross-sectional study to determine its association with cardiac biomarkers and nutritional status. BMC Nephrol. (2013) 14(1):266. doi: 10.1186/1471-2369-14-266
36. Bisoc A, Ciurescu D, Rădoi M, Tântu MM, Rogozea L, Sweidan AJ, et al. Elevations in high-sensitive cardiac troponin T and N-terminal prohormone brain natriuretic peptide levels in the Serum can predict the development of anthracycline-induced cardiomyopathy. Am J Ther. (2020) 27(2):e142–50. doi: 10.1097/MJT.0000000000000930
37. Cainap C, Maniu DR, Blag C, Popa G, Bota M, Vlad C, et al. The role of biomarkers and echocardiography in the evaluation of cardiotoxicity risk in children treated for leukemia. JBUON. (2018) 23(1):122–31.30722121
38. Booth J, Pinney J, Davenport A. N-terminal proBNP—marker of cardiac dysfunction, fluid overload, or malnutrition in hemodialysis patients? Clin J Am Soc Nephrol. (2010) 5(6):1036. doi: 10.2215/CJN.09001209
39. Sommerer C, Beimler J, Schwenger V, Heckele N, Katus HA, Giannitsis E, et al. Cardiac biomarkers and survival in haemodialysis patients. Eur J Clin Invest. (2007) 37(5):350–6. doi: 10.1111/j.1365-2362.2007.01785.x
40. Jacobs LH, Van De Kerkhof JJ, Mingels AM, Passos VL, Kleijnen VW, Mazairac AH, et al. Inflammation, overhydration and cardiac biomarkers in haemodialysis patients: a longitudinal study. Nephrol Dial Transplant. (2010) 25(1):243–8. doi: 10.1093/ndt/gfp417
41. Andreu A, Guglin M. Exaggerated NT-proBNP production in patients with hematologic malignancies: a case series. Congest Heart Fail. (2012) 18(6):333–6. doi: 10.1111/j.1751-7133.2011.00258.x
42. Wajdlich MJ, Podlejska P, Rosół D, Wynimko M, Kolejwa M, Sajdok M, et al. Effect of hydration status and variability of blood pressure and heart rate induced by hemodialysis on intradialytic changes of high sensitive troponin T. Arter Hypertens. (2017) 21(4):186–94. doi: 10.5603/AH.a2017.0023
43. Lipshultz SE, Rifai N, Sallan SE, Lipsitz SR, Dalton V, Sacks DB, et al. Predictive value of cardiac troponin T in pediatric patients at risk for myocardial injury. Circulation. (1997) 96(8):2641–8. doi: 10.1161/01.CIR.96.8.2641
44. Cheung Y-f, Yu W, Cheuk D-l, Cheng F-t, Yang J-k, Yau J-w, et al. Plasma high sensitivity troponin T levels in adult survivors of childhood leukaemias: determinants and associations with cardiac function. PLoS One. (2013) 8(10):3–8. doi: 10.1371/JOURNAL.PONE.0077063
45. Mladosievicova B, Urbanova D, Radvanska E, Slavkovsky P, Simkova I. Role of NT-proBNP in detection of myocardial damage in childhood leukemia survivors treated with and without anthracyclines. J Exp Clin Cancer Res. (2012) 31(1):86. doi: 10.1186/1756-9966-31-86
46. Kiess A, Green J, Willenberg A, Ceglarek U, Dähnert I, Jurkutat A, et al. Age-dependent reference values for hstroponin T and NT-proBNP and determining factors in a cohort of healthy children (the LIFE child study). Pediatr Cardiol. (2022) 43(5):1071–83. doi: 10.1007/s00246-022-02827-x
47. Wühl E, Witte K, Soergel M, Mehls O, Schaefer F. Distribution of 24-h ambulatory blood pressure in children: normalized reference values and role of body dimensions. J Hypertens. (2002) 20(10):1995–2007. doi: 10.1097/00004872-200210000-00019
48. Cole TJ, Green PJ. Smoothing reference centile curves: the LMS method and penalized likelihood. Stat Med. (1992) 11:1305–19. doi: 10.1002/sim.4780111005
49. Flynn JT, Urbina EM, Brady TM, Baker-Smith C, Daniels SR, Hayman LL, et al. Ambulatory blood pressure monitoring in children and adolescents: 2022 update: a scientific statement from the American Heart Association. Hypertension. (2022) 79(7):E114–24. doi: 10.1161/HYP.0000000000000215
50. Armstrong GT, Liu Q, Yasui Y, Neglia JP, Leisenring W, Robison LL, et al. Late mortality among 5-year survivors of childhood cancer: a summary from the childhood cancer survivor study. J Clin Oncol. (2009) 27(14):2328–38. doi: 10.1200/JCO.2008.21.1425
51. Lipshultz SE, Adams MJ, Colan SD, Constine LS, Herman EH, Hsu DT, et al. Long-term cardiovascular toxicity in children, adolescents, and young adults who receive cancer therapy: pathophysiology, course, monitoring, management, prevention, and research directions. Circulation. (2013) 128(17):1927–55. doi: 10.1161/CIR.0b013e3182a88099
52. Malkan UY, Haznedaroglu IC. Chronic myeloid leukemia, tyrosine kinase inhibitors and cardiovascular system. Eur Rev Med Pharmacol Sci. (2023) 27(12):5493–506. doi: 10.26355/EURREV_202306_32786
53. Giordano P, Muggeo P, Delvecchio M, et al. Endothelial dysfunction and cardiovascular risk factors in childhood acute lymphoblastic leukemia survivors. Int J Cardiol. (2017) 228:621–7. doi: 10.1016/j.ijcard.2016.11.025
54. Jacob A, Thyagarajan B, Kumar MP, Shaikh N, Sharon D. Cardiovascular effects of Hodgkin’s lymphoma: a review of literature. J Cancer Res Clin Oncol. (2018) 144(1):99–107. doi: 10.1007/s00432-017-2560-x
55. Bhojwani D, Darbandi R, Pei D, et al. Severe hypertriglyceridaemia during therapy for childhood acute lymphoblastic leukaemia. Eur J Cancer. (2014) 50(15):2685–94. doi: 10.1016/j.ejca.2014.06.023
56. Loomba RS, Villarreal EG, Farias JS, Flores S, Bronicki RA. Fluid bolus administration in children, who responds and how? A systematic review and meta-analysis. Paediatr Anaesth. (2022) 32(9):993–9. doi: 10.1111/pan.14512
57. Oeffinger KC, Mertens AC, Sklar CA, et al. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med. (2006) 355(15):1572–82. doi: 10.1056/NEJMsa060185
58. Hsiao W, Lapite A, Faig W, Abdel-Megid M, Carlson C, Hobbie W, et al. Long-term kidney and cardiovascular complications in pediatric cancer survivors. J Pediatr. (2023) 255:89–97.e1. doi: 10.1016/j.jpeds.2022.10.029
59. Kumar R, Mahan JD, Stanek JR, Reed S. Extent of hypertension and renal injury in children surviving acute lymphoblastic leukemia. Pediatr Blood Cancer. (2022) 69(9):e29628. doi: 10.1002/pbc.29628
60. Koratala A, Ronco C, Kazory A. Diagnosis of fluid overload: from conventional to contemporary concepts. Cardiorenal Med. (2022) 12(4):141–54. doi: 10.1159/000526902
61. Graf I, Greiner G, Marculescu R, et al. N-terminal pro-brain natriuretic peptide is a prognostic marker for response to intensive chemotherapy, early death, and overall survival in acute myeloid leukemia. Am J Hematol. (2023) 98(2):290. doi: 10.1002/ajh.26805
62. Gimeno E, Gómez M, González JR, Comín J, Alvarez-Larrán A, Sánchez-González B, et al. NT-proBNP: a cardiac biomarker to assess prognosis in non-Hodgkin lymphoma. Leuk Res. (2011) 35(6):715–20. doi: 10.1016/j.leukres.2011.01.018
63. Maitra P, Caughey M, Robinson L, Desai PC, Jones S, Nouraie M, et al. Risk factors for mortality in adult patients with sickle cell disease: a meta-analysis of studies in North America and Europe. Haematologica. (2017) 102(4):626–36. doi: 10.3324/haematol.2016.153791
64. Hosnijeh FS, Krop EJM, Scoccianti C, Krogh V, Palli D, Panico S, et al. Plasma cytokines and future risk of non-Hodgkin lymphoma (NHL): a case-control study nested in the Italian European prospective investigation into cancer and nutrition. Cancer Epidemiol Biomarkers Prev. (2010) 19(6):1577–84. doi: 10.1158/1055-9965.EPI-09-1237
65. Lipshultz SE, Miller TL, Scully RE, Lipsitz SR, Rifai N, Silverman LB, et al. Changes in cardiac biomarkers during doxorubicin treatment of pediatric patients with high-risk acute lymphoblastic leukemia: associations with long-term echocardiographic outcomes. J Clin Oncol. (2012) 30(10):1042–9. doi: 10.1200/JCO.2010.30.3404
Keywords: ambulatory blood pressure monitoring, children, hematological malignancies, intensive fluid therapy, cardiac biomarkers, atrial natriuretic peptide (NT-proBNP), high-sensitivity troponin t (hs-TnT)
Citation: Pawlik W, Strzemecka J, Stachura A, Królak A and Ociepa T (2024) High NT pro-BNP levels in children with malignant disorder receiving intensive fluid treatment: a prospective comparative study. Front. Pediatr. 12:1408231. doi: 10.3389/fped.2024.1408231
Received: 27 March 2024; Accepted: 1 November 2024;
Published: 27 November 2024.
Edited by:
Carsten Heilmann, Rigshospitalet, DenmarkReviewed by:
Grace Nnadozie, The MetroHealth System, United StatesVasiliki Karava, Aristotle University of Thessaloniki, Greece
Copyright: © 2024 Pawlik, Strzemecka, Stachura, Królak and Ociepa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Weronika Pawlik, d2Vyb25pa2EucGF3bGlrQHB1bS5lZHUucGw=