 Rodrigo Sini de Almeida1*
Rodrigo Sini de Almeida1* João Leite2
João Leite2 Jessica E. Atwell3
Jessica E. Atwell3 Malak Elsobky4
Malak Elsobky4 Jorge LaRotta5
Jorge LaRotta5 Mostafa Mousa6
Mostafa Mousa6 Karan Thakkar7
Karan Thakkar7 Mark A. Fletcher8
Mark A. Fletcher8
- 1Vaccines and Antivirals Medical Affairs, Emerging Markets Region, Pfizer, São Paulo, Brazil
- 2IQVIA, Inc., Porto Salvo, Portugal
- 3Global Respiratory Vaccines and Antivirals, Pfizer, Collegeville, PA, United States
- 4Vaccines and Antivirals Medical Affairs, Emerging Markets Region, Pfizer Canada ULC, Kirkland, QC, Canada
- 5Latin America Vaccines Medical Affairs, Pfizer, Bogota, Colombia
- 6Pfizer Vaccines Medical Affairs, Riyadh, Saudi Arabia
- 7Emerging Asia Vaccines Medical Affairs, Pfizer, Singapore, Singapore
- 8Vaccines and Antivirals Medical Affairs, Emerging Markets Region, Pfizer, Paris, France
Background: We evaluated published evidence (2012–2022) on pediatric RSV burden in 149 countries within World Health Organization (WHO) regions of Africa (AFRO), Americas (AMRO, excluding Canada and the USA), Eastern Mediterranean (EMRO), Europe (EURO, excluding European Union countries and the UK), Southeast Asia (SEARO), and Western Pacific (WPRO, excluding Australia, China, Japan, New Zealand, and South Korea).
Methods: Gap analysis on RSV-associated disease (hospitalizations, hospital course, mortality or case fatality, detection, and incidence) in children ≤2 years old, where hospitalization rates, hospital course, mortality rate, case fatality rate (CFR), and postmortem detection rates were summarized, by region, for each country.
Results: Forty-two publications were identified covering 19% of included countries in AFRO, 18% in AMRO, 14% in EMRO, 15% in EURO, 18% in SEARO, and 13% in WPRO. Methods, case definitions, and age groups varied widely across studies. Of these 42 publications, 25 countries reported hospitalization rate, hospital course, mortality rate, CFR, and/or postmortem detection rate. RSV hospitalization rate (per 1,000 children per year/child-years) was higher among ≤3-month-olds (range, 38 in Nicaragua to 138 in the Philippines) and ≤6-month-olds (range, 2.6 in Singapore to 70 in South Africa) than in 1–2-year-olds (from 0.7 in Guatemala to 19 in Nicaragua). Based on 11 studies, in AFRO (South Africa), AMRO (Chile and Mexico), EMRO (Lebanon and Jordan), EURO (Israel and Turkey), and SEARO (India), hospitalized children ≤2 years old remained hospitalized for 3–8 days, with 9%–30% requiring intensive care and 4%–26% needing mechanical ventilation. Based on a study in India, community-based CFR was considerably higher than that in the hospital (9.1% vs. 0% in ≤3-month-olds; 7.1% vs. 2.8% in ≤6-month-olds).
Conclusions: National and regional heterogeneity of evidence limits estimates of RSV burden in ≤2-year-olds in many WHO region countries, where further country-specific epidemiology is needed to guide prioritization, implementation, and impact assessment of RSV prevention strategies.
Introduction
The burden of neonatal and infant respiratory syncytial virus (RSV) disease is mostly due to lower respiratory tract infection (LRTI) such as bronchiolitis and pneumonia (1, 2). Although prematurity or cardiopulmonary comorbidities can increase the severity of RSV illness (3), young age remains a crucial risk factor (4). This has been well documented in the USA, for example, where a comprehensive, nationally representative analysis underscored that RSV bronchiolitis is the leading cause of hospitalization in infants <1 year old (5). Other studies in Australia, China, Japan, and New Zealand confirm the substantial burden of RSV-LRTI in the neonatal and infant period of the first 6 months of life, notwithstanding any comorbid conditions (6–9). Likewise, a European, prospective birth cohort study of children born between 2017 and 2020 documented that two-thirds of RSV-LRTI hospitalizations were among neonates and young infants (≤3 months old), and half occurred in full-term, otherwise healthy, infants (10).
Despite the substantial RSV burden literature, evidence gaps still exist worldwide, especially outside of North America, the European Union (EU), and some Western Pacific countries, likely due to challenges in establishing an infectious etiology based on incomplete surveillance or inconsistency in viral testing (11). Nonetheless, it is estimated that low-resource countries account for both >95% of global pediatric RSV-LRTI and associated deaths and 65% of global costs associated with pediatric RSV hospitalizations, posing a drain on already overwhelmed local health systems (2, 12). The World Health Organization (WHO) has emphasized the need for additional evidence from these countries to inform decision-making on RSV prevention strategies. Specifically, the WHO highlighted the importance of an availability of RSV hospitalization and mortality rates, which are often inadequately substantiated (13).
We conducted a targeted literature review (TLR) and gap analysis in countries that are typically underrepresented in the pediatric RSV-LRTI literature. We highlighted neonatal and infant hospitalization rates, hospital course, and mortality, as well as fatality and postmortem RSV positivity proportions, to underscore the burden of disease on healthcare systems and contemporary possibilities for prevention strategies.
Methods
Literature search
This TLR/gap analysis was conducted in accordance with guidelines from the Cochrane Handbook for Systematic Reviews of Interventions (14), the Centre for Reviews and Dissemination (University of York) (15), and PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) (16). The OvidSP interface and PICOS (patient/population, intervention, comparison, outcomes, and study) framework were used to identify English-language publications indexed in Embase and Medline between 2012 and 2022. We chose this timeframe to cover up to 11 years of existing research, incorporating more recent evidence compared to previously published global reviews (1, 2). Conference abstracts published between 2020 and (up to 29 September) 2022 were also captured within Embase.
Search strategies for the terms relevant to disease area, interventions, and study designs were developed through the combination of free-text words, indexing terms (e.g., Emtree terms for Embase), and by using Boolean terms (e.g., “and” and “or”). These relevant words and terms were reflected in the search strings (presented in Supplementary Table S1), which were appropriately modified to fit each database-specific syntax.
Abstracts and titles identified during the search were screened by a reviewer against predetermined eligibility criteria outlined in Supplementary Table S2 using the PICOS framework. Publications selected as potentially relevant were retained for full-text review. A second reviewer assessed all abstracts and publications where uncertainty existed.
Data were extracted from the selected full texts using a standardized data extraction template (MS Excel). The list of variables for extraction is outlined in Supplementary Table S3.
Geographic coverage
The search comprised 149 countries within the WHO regions of Africa (AFRO), Americas (AMRO, excluding Canada and USA), Eastern Mediterranean (EMRO), Europe (EURO, excluding EU countries and the UK), Southeast Asia (SEARO), and Western Pacific (WPRO, excluding Australia, China, Japan, New Zealand, and South Korea) (17). The full list of included countries is presented in Table 1.
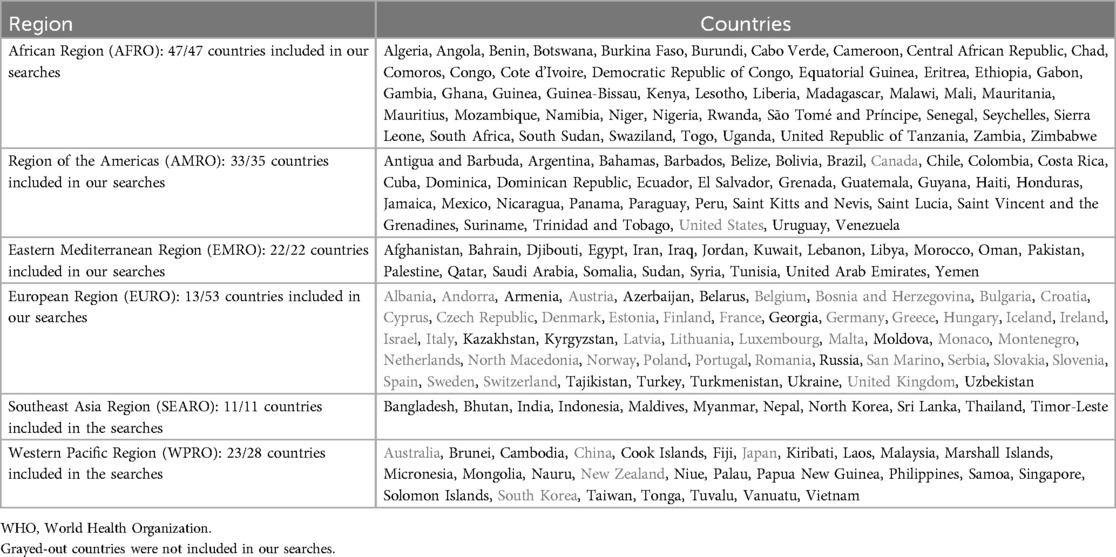
Table 1. List of countries included in the six WHO regions.
Gap analysis and RSV burden description
The burden of RSV-LRTI is specified characteristically by epidemiological parameters like detection rate, incidence, hospitalization rate, hospital course, and mortality. To better identify published data on RSV disease burden, we evaluated data availability for each of these parameters. To summarize the available evidence, we focused especially on hospitalization and death, which have been highlighted by WHO as influential for decision-making around prevention strategies (13). This evidence included RSV-associated hospitalization and mortality rates, lethality (i.e., the proportion of deaths among children with confirmed RSV infection), and postmortem RSV detection rates. The hospital course was summarized where available.
This TLR/gap analysis aimed to describe the burden of RSV regardless of risk factors; thus, we do not highlight in the body of the manuscript the few studies stratifying hospitalizations by gestational age. Nonetheless, for completeness, details are presented from these studies in pre-term children that estimated RSV-associated hospitalizations (Supplementary Table S4), hospital course (Supplementary Table S5), RSV detection rates/RSV-positive cases among hospitalized children (Supplementary Table S6), and RSV infection incidence and outpatient visit rates (Supplementary Table S7).
Data reporting
RSV-associated hospitalization and mortality rates (as well as incidence rates in Supplementary Table S7) were standardized to 1,000 children per year, 1,000 child-years, or 1,000 live births. Fatality is described as case fatality rate (CFR) with confirmed RSV, and CFR is presented as in-hospital-based (a percentage of deaths among hospitalized children) or as community-based (a percentage of deaths among non-hospitalized children). Postmortem RSV detection rate is reported as a percentage of RSV-positive cases among all-cause or respiratory deaths. To try to systematize the substantial variability in age group categories applied across studies, we grouped the age range used by each investigator within one of four strata: ≤3 months, ≤6 months, ≤1 year, or ≤2 years.
Across all outcomes, data are reported with one decimal place for numbers <10 and rounded to the nearest whole number for values 10 or greater.
Results
Literature search outcomes and study characteristics
Of the 1,975 references screened, 42 publications (18–59) that reported at least incidence, hospitalization rate, hospital course, detection rate, or mortality were selected (Figure 1). Sample sizes varied greatly, from 16 neonates admitted to the neonatal intensive care unit (ICU) with acute respiratory infection (ARI) in India (37) to 530,345 children hospitalized for all respiratory/circulatory causes including pneumonia and influenza in South Africa (43). Community data were available in 29% (12/42) of studies. Study designs also varied, encompassing “surveillance” (16 studies), “cross-sectional design” (5 studies), “retrospective” cohort (5 studies), “prospective” cohort (12 studies), both “retrospective and prospective” cohort (1 study), or statistical modeling (3 studies). Clinical case definitions for RSV positivity spanned from ARI (12 studies), lower respiratory tract infections (ranging from LRTI in general to specific clinical presentations like pneumonia and bronchiolitis, 19 studies) to fever-based definitions [influenza-like infection (ILI) or severe ARI (SARI), 7 studies], or a general definition of “symptomatic illness” (4 studies). RSV detection was based exclusively on polymerase chain reaction (PCR) in more than half of the studies (60%, 25/42). Other detection methods included immunoassays (14%, 6/42) and antigen tests (14%, 6/42). Some studies incorporated more than one method (i.e., some of the study samples were analyzed with one method and others used another method), specifically immunofluorescence and PCR (4.8%, 2/42) or antigen test and PCR (2.4%, 1/42). The detection method was not reported in two studies. More details on the study characteristics are described in Supplementary Table S8.
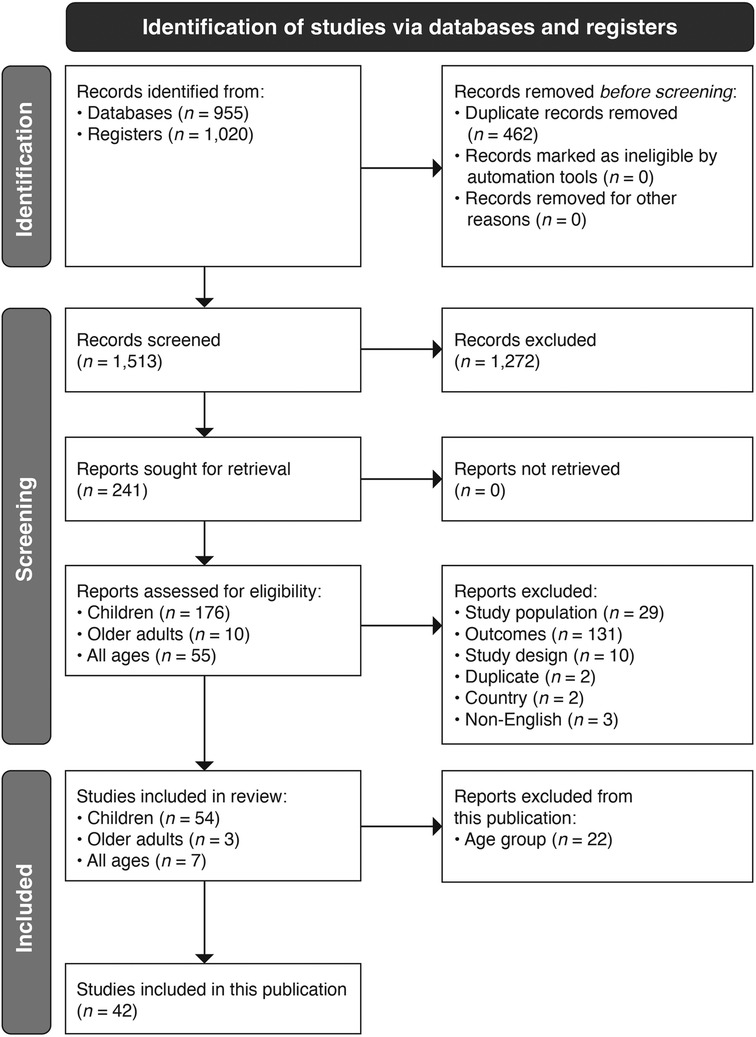
Figure 1. PRISMA flow diagram for study identification, screening, and inclusion.
GAP analysis
The 42 publications identified in this study covered 17% (25/149) of the targeted countries (18–59). By WHO region, this represented 19% (9/47) of countries in AFRO, 18% (6/33) in AMRO, 14% (3/22) in EMRO, 15% (2/13) in EURO, 18% (2/11) in SEARO, and 13% (3/23) in WPRO.
Details on the availability of evidence on RSV-associated hospitalization rate, hospital course, RSV-associated mortality/CFR, RSV viral detection rate, and incidence of RSV disease are presented by WHO regions/countries in Figure 2.
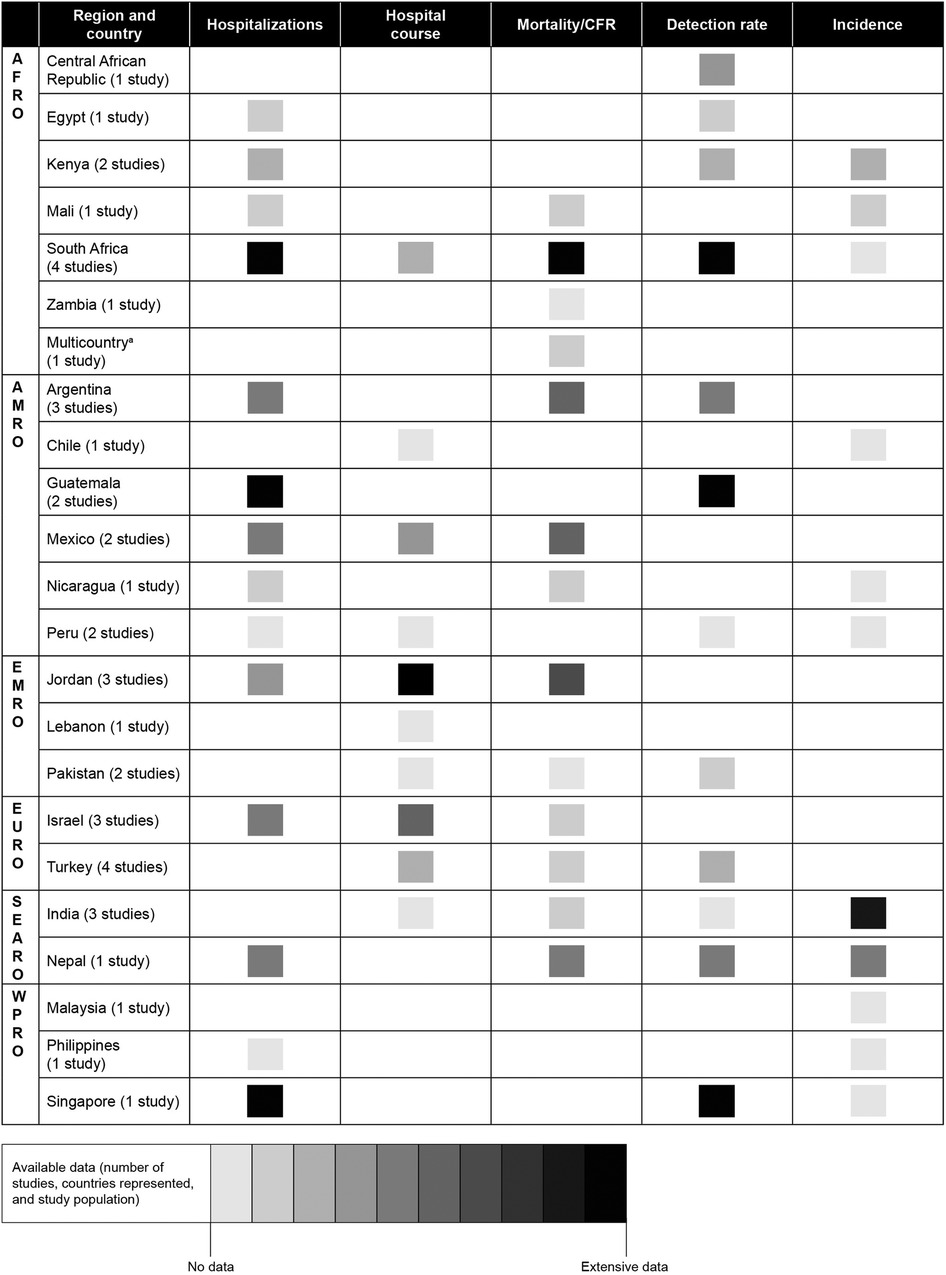
Figure 2. Data availability for children ≤2 years old in countries of the WHO regions of AFRO, AMRO (except Canada and USA), EMRO, EURO (except for European Union countries and the UK), SEARO, and WPRO (excluding Australia, China, Japan, New Zealand, and South Korea). AFRO, African Region; AMRO, Region of the Americas; EMRO, Eastern Mediterranean Region; EURO, European Region; SEARO, Southeast Asia Region; WPRO, Western Pacific Region. aEthiopia, Kenya, Mali, Mozambique, Sierra Leone, and South Africa. Country coverage within each region: AFRO, 19% (9 of 47 countries); AMRO 18% (6 of 33 countries); EMRO, 14% (3 of 22 countries); EURO, 15% (2 of 13 countries); SEARO 18% (2 of 11 countries); WPRO 13% (3 of 23 countries).
In AFRO, 5 of 11 studies were conducted in South Africa (23, 26, 27, 43, 59). The most available information in South Africa pertained to RSV-associated hospitalization, mortality or CFR, and viral detection rates, while hospital course and incidence rates were scarce. From other countries in AFRO beyond South Africa, only sparse information was available on hospitalizations (Egypt, Kenya, and Mali) (24, 28, 49), mortality or CFR (Ethiopia, Kenya, Mali, Mozambique, Sierra Leone, and Zambia) (23, 24, 31), viral detection rates (Central African Republic, Egypt, and Kenya) (28, 41, 49), and disease incidence (Kenya and Mali) (24, 47).
In AMRO, 7 of 11 studies in this region were concentrated in Argentina, Guatemala, and Mexico (21, 22, 29, 30, 33, 45, 56). Most evidence primarily pertained to RSV-associated hospitalizations and viral detection rates from Guatemala (30, 45), although Argentina and Mexico reported hospitalization, mortality or CFR, and viral detection rates (21, 22, 29, 33, 56). Only limited evidence was available on hospital course and incidence of RSV disease in this region, based on sparse information from Chile, Mexico, Nicaragua, and Peru (42, 44, 56, 57).
In EMRO, evidence came mainly from Jordan, with 3 of 6 studies conducted in this country (32, 40, 58). The most substantial Jordan data pertained to hospitalizations, hospital course, and mortality or CFR, while Lebanon and Pakistan provided limited information on hospital course, mortality, and viral detection rates (18, 20, 39). Notably, evidence on the incidence of RSV disease was completely lacking in EMRO.
In EURO, data were only available from Israel and Turkey (seven studies in total) (19, 34–36, 38, 48, 52), with most evidence from Israel that pertained to hospitalization rates and hospital course (36, 38). Only limited data were available for mortality and viral detection rates in these countries (19, 36, 48). As with EMRO, evidence on the incidence of RSV disease was completely lacking in EURO.
In SEARO, India and Nepal provided incidence estimations (25, 50), while some evidence from a single study in Nepal was available for hospitalizations, mortality or CFR, and viral detection rates (25). Limited data were available in India on hospital course (37).
In WPRO, Singapore provided clear results about hospitalization and viral detection rates (53), and there was some information on disease incidence from Singapore, as well as Malaysia and the Philippines (53–55). Hospital course and mortality were unavailable from this region.
In the following sections of this manuscript, we summarize data—available from 31 studies covering 25 countries across the six WHO regions—for RSV-associated hospitalization rates and hospital course, mortality rates, and CFR.
Hospitalization rates and hospital course
Hospitalization rates per 1,000 children per year or per child-years are presented in Table 2 and hospital course in Table 3.
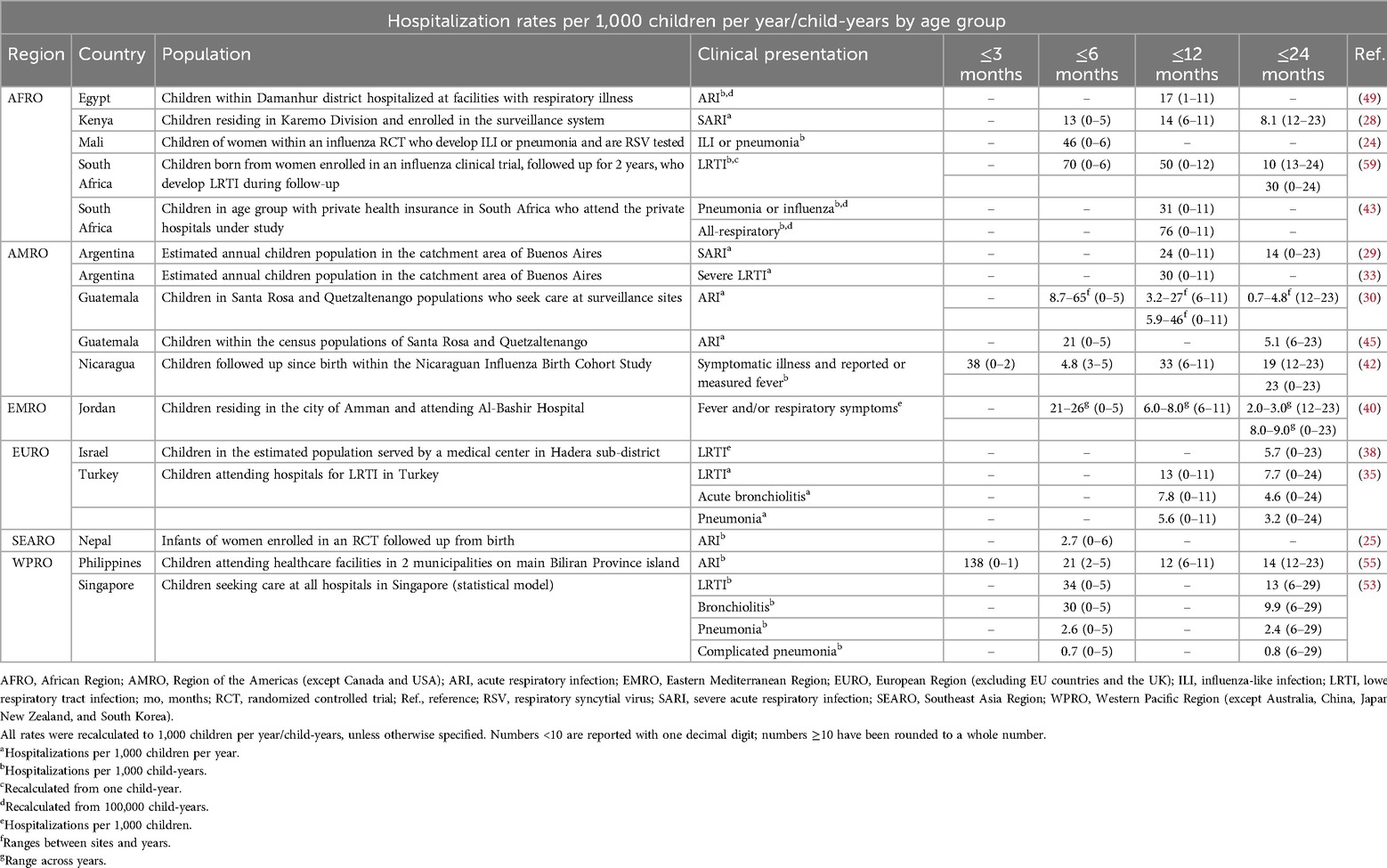
Table 2. RSV-associated hospitalization rates per 1,000 children per year/child-years grouped by upper age-range categories ≤3 months, ≤6 months, ≤12 months, and ≤24 months (with the age group as reported by the investigators).
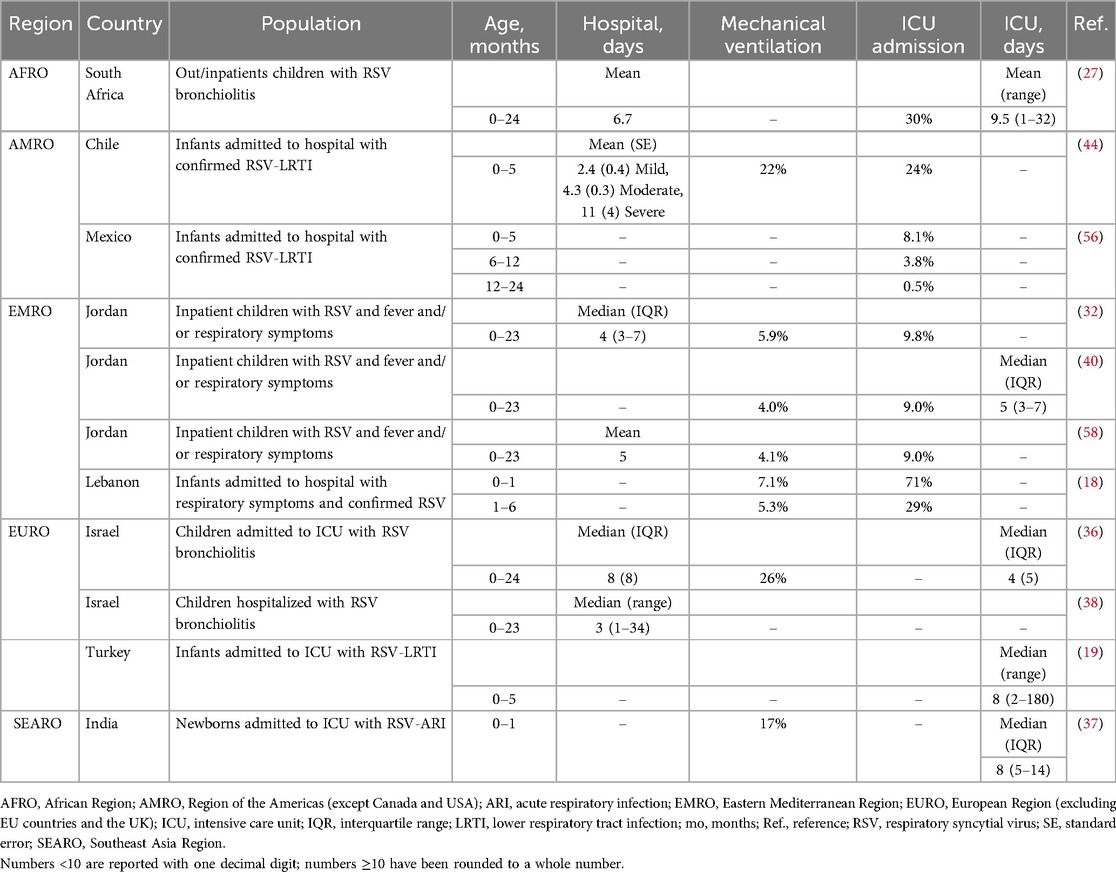
Table 3. Summary of information on hospital course available from the reviewed studies.
In AFRO, hospitalization details were available from six studies in four countries for the age groups 0–6 months and 1–2 years, specifically Egypt, Kenya, Mali, and South Africa (24, 27, 28, 43, 49, 59). Conversely, there was no information specific to newborns ≤3 months old.
Age-specific hospitalization rates decreased with older age. Among young infants 0–6 months old, the rates ranged from 13 per 1,000 child-years in Kenya (28) to 70 per 1,000 child-years in South Africa (59); among older infants 6–11 months old, the rate was 14 per 1,000 children per year in Kenya (28); and among children 1–2 years old, the rate ranged from 8.1 per 1,000 children per year in Kenya (28) to 10 per 1,000 child-years in South Africa (59). In South Africa, children ≤2 years old with RSV-LRTI spent on average 7 days in the hospital, and 30% of them were admitted to the ICU with an average stay of 9–10 days (27).
In AMRO, there were seven studies in five countries across the age ranges of 0–2 months to 1–2 years, specifically from Argentina, Chile, Guatemala, Mexico, and Nicaragua (29, 30, 33, 42, 44, 45, 56). Hospitalization rates among neonates aged 0–2 months old were 38 per 1,000 child-years in Nicaragua (42); among infants 0–5 months old, rates ranged from 8.7 to 65 per 1,000 children per year in Guatemala (30); among older infants aged 6–11 months, from 3.2 per 1,000 children per year in Guatemala (30) to 33 per 1,000 child-years in Nicaragua (42); and among children 1–2 years old, from 0.7 per 1,000 children per year in Guatemala (30) to 19 per 1,000 child-years in Nicaragua (42). In two studies, one each in Chile and Mexico, documenting hospital course among infants 0–5 months old, the average length of stay varied by RSV-LRTI severity, from 2 days for mild illness to 4 days for moderate illness and 11 days for severe illness; ICU admission rates were 8%–24%, with 22% requiring mechanical ventilation (44, 56).
In EMRO, hospitalization data were available from four studies in two countries, specifically Jordan and Lebanon (18, 32, 40, 58). Hospitalization rates were only available in Jordan, with the age ranges of 0–5 months to 1–2 years: among young infants 0–5 months old, the rates were 21–26 per 1,000 children per year; among older infants, the rates for 6–11 months were 6–8 per 1,000 children per year, and among children 1–2 years old, the rates were 2–3 per 1,000 children per year (40). Average hospital stay duration, available only for infants 0–23 months old in Jordan, was 4–5 days (32, 58), while in Lebanon, ICU admission rates were 71% for neonates (0–1 month old), 29% for infants (1–6 months old), and 13% for children (6–24 months old) (18).
In EURO, hospitalization details were available in children—although not specifically for the ≤6-month-old age group—from two studies in Turkey (19, 35) and two studies in Israel (36, 38). RSV-LRTI hospitalization rate among infants 0–11 months old in Turkey was 13 per 1,000 children per year (35), while in children ≤2 years old values ranged from 6 per 1,000 children per year in Israel (38) to 8 per 1,000 children per year in Turkey (35). In RSV-LRTI-hospitalized children ≤2 years old, the average hospital stay was 3 to 8 days in Israel, the average ICU stay was from 4 days in Israel to 8 days in Turkey, and of the children in Israel admitted to the ICU, 27% required mechanical ventilation (19, 36, 38).
In SEARO, hospitalization rates were available from one study in Nepal (25), and there was hospital course information from one study in India (37). The Nepal study reported a 2.7 per 1,000 child-years RSV-ARI hospitalization rate in young infants ≤6 months old (25). In India, 17% of neonates (0–1 month old) admitted to the ICU with RSV-ARI required mechanical ventilation with an average length of ICU stay of 8 days (37).
In WPRO, hospitalization was investigated in one study from Singapore (53) and one in the Philippines (55). In Singapore, the hospitalization rates were 34 per 1,000 child-years in infants 0–5 months old and 13 per 1,000 child-years in infants and children 6–29 months old (53). The Philippines study focused on neonates 0–1 month old, reporting an RSV-ARI hospitalization rate of 138 per 1,000 child-years, the highest documented across all countries and regions (55). No data on hospital course were available from WPRO.
Mortality rates
Mortality rates per 1,000 child-years or children per year (Table 4) were available from five studies in four countries, specifically one study in AFRO (South Africa) (26), three studies in AMRO (Argentina and Nicaragua) (29, 33, 42), and one study in SEARO (India) (51). In AMRO, in infants 0–12 months old, the mortality rate in Argentina was 0.3 per 1,000 child-years in the hospital (29) and ranged between 0.7 per 1,000 child-years and 0.9 per 1,000 live births when hospital and community deaths were combined (29, 33). Among children 0–23 months old, the community-based mortality rate was 2.8–4.2 per 1,000 child-years in Nicaragua (42). In SEARO, only the study in India had data for the ≤6-month-old age group, with combined community and hospital mortality rates per 1,000 child-years of 3.0 for newborns 0–3 months old, 2.5 for young infants 0–6 months old, 1.6 for infants 0–12 months old, and 1.0 for children 0–23 months old (51). The authors also compared community and hospital mortality rates in India and found that the mortality rates per 1,000 child-years, by age group, were substantially greater in the community as compared with the hospital: 3.0 vs. 0 (0–3 months old); 2.3 vs. 0.3 (0–6 months old); 1.5 vs. 0.1 (0–12 months old); and 0.9 vs. 0.1 (0–23 months old) (51).
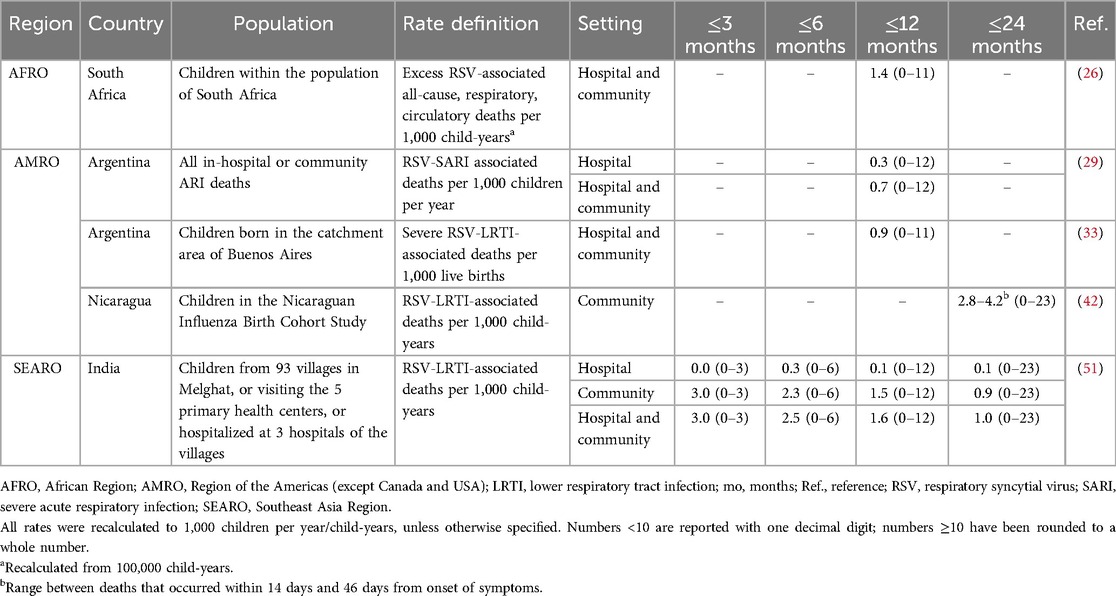
Table 4. RSV-associated mortality rates per 1,000 children per year/child-years, grouped by upper age-range categories ≤3 months, ≤6 months, ≤12 months, and ≤24 months (with the age group as reported by the investigators).
Case fatality rate (CFR)
CFR, in-hospital (Table 5) or community-based (Table 6), was documented among 13 studies in nine countries: specifically, 2 studies in AFRO (Mali and South Africa) (24, 27); 4 studies in AMRO (Argentina and Mexico) (21, 29, 33, 56); 3 studies in EMRO (Jordan) (32, 40, 58); 2 studies in EURO (Israel and Turkey) (19, 36); and 2 studies in SEARO (India and Nepal) (25, 51). Only the study in India documented CFR in newborns 0–3 months old (51), and only three studies from Mali (24), India (51), and Nepal (25) reported community CFR.
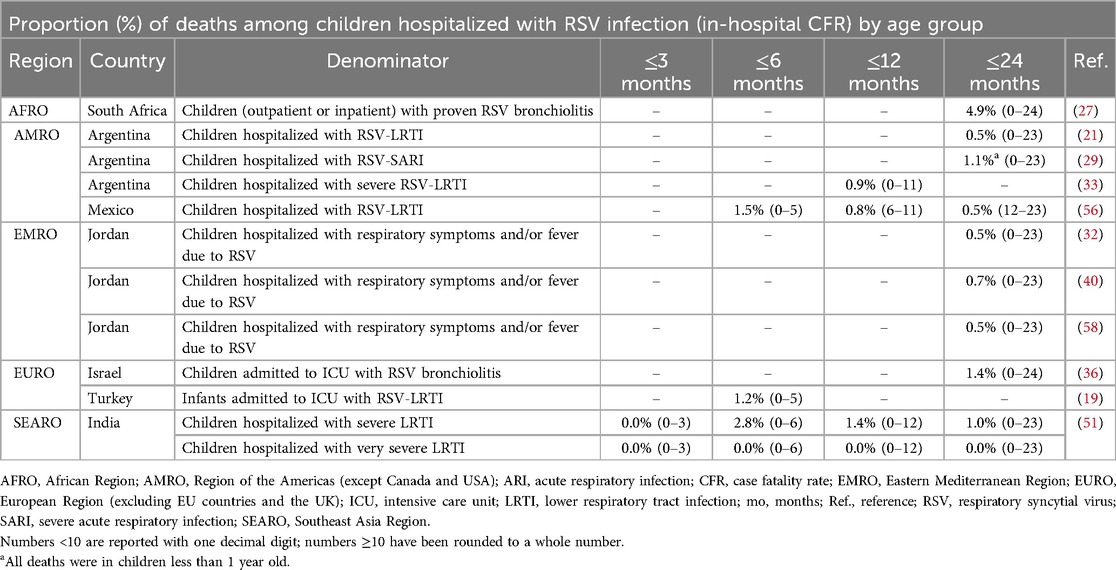
Table 5. RSV-associated in-hospital CFR grouped by upper age-range categories ≤3 months, ≤6 months, ≤12 months and ≤24 months (with the age group as reported by the investigators).
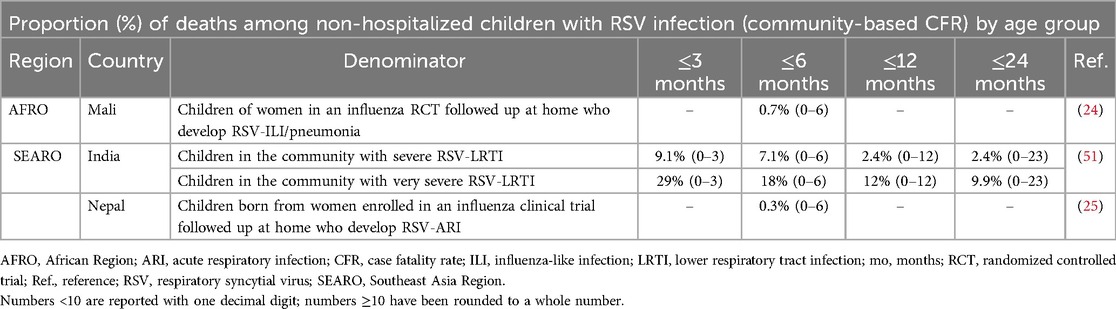
Table 6. RSV-associated community-based CFR grouped by upper age-range categories ≤3 months, ≤6 months, ≤12 months, and ≤24 months (with the age group as reported by the investigators).
In AFRO, age-specific CFR (RSV-ILI and RSV-pneumonia deaths) was 0.7% among ≤6-month-old infants in the community, followed within a maternal influenza vaccination trial, in Mali (24), and 4.9% (RSV bronchiolitis deaths) in children ≤2 years old from both in-hospital and outpatient settings in South Africa (27). In AMRO, in-hospital CFR was 1.5% in young infants 0–5 months old (Mexico), 0.9% in infants 0–11 months old (Argentina), and 0.5% in children 1–2 years old (Mexico) (33, 56). In EMRO, CFR was available only in the hospital setting from Jordan and ranged between 0.5% and 0.7% among infants 0–23 months old (32, 40, 58). In EMRO, CFRs were reported among infants and children admitted to the ICU: 1.2% among infants 0–5 months old in Turkey and 1.4% among children 0–24 months old in Israel (19, 36). In SEARO, the infant CFR in India associated with severe RSV-LRTI was substantially lower in the hospital than in the community: 0% vs. 9.1% among neonates and young infants 0–3 months old and 2.8% vs. 7.1% among infants 0–6 months old (51).
Postmortem RSV detection
Four AFRO studies covering seven countries (Ethiopia, Kenya, Mali, Mozambique, Sierra Leone, South Africa, and Zambia) (23, 31), one AMRO study in Argentina (33), and one EMRO study in Pakistan (39) evaluated the proportion of RSV-positive test results among infants who died from any cause in the hospital or the community (Table 7).
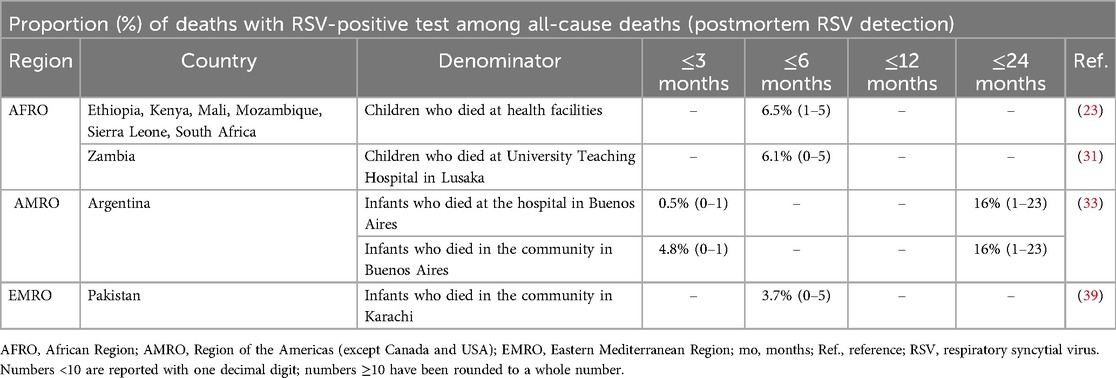
Table 7. Postmortem RSV positivity by upper age-range categories ≤3 months, ≤6 months, ≤12 months, and ≤24 months (with the age group as reported by the investigators).
Only the study in Argentina reported data for neonates 0–1 month old and children 1–23 months old comparing hospital and community deaths (33). The authors found that while the 0.5% proportion of RSV-related hospital deaths in neonates was significantly lower than the 16% in children, in the community the rate increased to 4.8% in neonates whereas it remained at 16% in children (33). All other studies reported data for infants ≤6 months old (23, 31, 39). In the AFRO countries, the proportion ranged between 6.1% among hospital deaths and 6.5% among community deaths (23, 31). In Pakistan, the RSV-related proportion was 3.7% among community deaths (39).
Discussion
This gap analysis is based on the understanding that policymakers require national-level estimates to inform decisions regarding the introduction of prevention strategies for RSV and to assess their subsequent effects (60, 61). We reviewed the evidence published between 2012 and 2022 available on RSV burden in 149 countries across six WHO regions, excluding some countries in AMRO (Canada and USA), EURO (the EU countries and the UK), and WPRO (Australia, China, Japan, New Zealand, and South Korea). Only 17% (25 of 149) of the investigated countries had published details in children ≤2 years old when considering hospitalization rate, hospital course, mortality rate, CFR, and postmortem detection rates, as well as viral detection rate, disease incidence, and outpatient visit rates. This suggests that national evidence is limited to one-quarter of the countries considered in this WHO region gap analysis and is unavailable from more than three-quarters of the possible countries. The WHO supports evidence-based RSV prevention strategies in understudied countries, particularly identifying RSV hospitalization and death rates as crucial parameters for decision-making (13).
Based on the results of this review, evidence for these outcomes remains incomplete. First, RSV-associated hospitalization and mortality (fatality) statistics were available from only 11% of the 149 countries among children (≤24 months old), although there were few epidemiology studies among neonates and young infants (≤3 months old) who are most often severely affected by RSV-LRTI (5–10), with one study in Nicaragua and one in the Philippines reporting hospitalization rates and one study in India reporting death rates (42, 51, 55).
RSV hospitalization rates in this TLR/gap analysis for neonates and young infants (≤3 months old) ranged from 38 to 138 per 1,000 child-years. With the limited data, ranges varied widely by WHO region, and as suggested by global estimates (1, 2) they were consistently higher in younger infants (0–6 months old) than in children (1–2 years old): AFRO, 13 per 1,000 children per year to 70 per 1,000 child-years vs. 8.1 per 1,000 children per year to 10 per 1,000 child-years; AMRO, 8.7–65 per 1,000 children per year vs. 0.7 per 1,000 children per year to 19 per 1,000 child-years; EMRO, 21–26 vs. 2.0–3.0 per 1,000 children per year; and WPRO, 2.6–34 vs. 2.4–14 per 1,000 child-years. (No data for infants ≤6 months old were available in EURO, and no data in children 1–2 years old were available in SEARO.) Based on 11 hospitalization course studies in eight countries (AFRO, South Africa; AMRO, Chile, Mexico; EMRO, Jordan, Lebanon; EURO, Israel, Turkey; and SEARO, India), admitted children ≤2 years old remained in the hospital for 3–8 days, with 8%–30% of them requiring ICU admission and 4%–26% needing mechanical ventilation. Although not investigated in this TLR/gap analysis, the cost to treat and manage each severe RSV episode in low- and middle-income countries has been estimated to be $4,114, with a cost of illness accounting for almost 40% of household monthly income (62). Taken together, these data highlight the great burden on healthcare systems and on families alike, which is particularly challenging in resource-deprived countries.
Studies in EU and the USA reported that RSV-associated deaths among hospitalized infants are infrequent and can span from a value of 0 deaths in one active surveillance study covering five countries between 2017 and 2019 in Europe to 6.9 per 1,000,000 live births in a national statistics analysis in the USA between 1999 and 2018 (10, 63). In contrast, previous global systematic reviews and meta-analyses reported that there is a higher burden associated with RSV deaths in other parts of the world (1, 2, 64), like this TLR/gap analysis shows, specifically from published studies in Argentina, India, and South Africa. In neonates and infants ≤3 months old, India reported a combined hospital and community-based mortality rate associated with RSV-LRTI of 3 per 1,000 child-years (51). Most of these deaths occurred in the community with a hospital-based CFR of 0% but a community-based CFR of 9% for severe and 29% for very severe cases (51). In infants ≤1 year old, mortality rates ranged from 0.1 per 1,000 child-years (India) to 0.3 per 1,000 children per year (Argentina) in the hospital setting and from 0.7 per 1,000 children per year (Argentina) to 1.6 per 1,000 child-years (India) when community deaths were also considered (29, 51). CFR was up to 12% in India in the community among infants ≤1 year old (51) and up to 4.8% in South Africa in the hospital among children ≤2 years old (27). These RSV-associated death statistics likely reflect lower access to care and availability of resources in more vulnerable healthcare systems, as compared to the values reported from the EU and USA (2, 64).
Despite the RSV-LRTI burden that can vary by calendar year across geographies, the substantial differences between countries revealed by this TLR/gap analysis could also be attributable to methodological inconsistencies (61, 65). Research settings (e.g., hospital vs. community or inpatient vs. outpatient) can contribute to the variability, as well as can access to care that varies across economies (2, 27). Inconsistency in case definitions also contributes to data heterogeneity. For example, case definitions based on the requirement of fever, such as for ILI and SARI, might underestimate the RSV burden because many clinical cases present without fever (66, 67). Some methods of sample collection and viral detection have higher sensitivity and specificity than others, and some patient sampling sites are more suited for identifying certain viruses (68). Altogether, this highlights the urgent need for standardized protocols as a foundation for surveillance.
One of our TLR's key strengths is that it encompasses evidence from 149 countries worldwide that historically have been understudied. Over an 11-year publication period (2012–2022), we assembled results reported in these studies across five possible clinical outcomes to identify and highlight gaps in the RSV burden epidemiology for children aged ≤2 years within countries across all six WHO regions. As with all TLRs, missing relevant publications, due to English-language and period-of publication restrictions, represent inherent limitations.
Conclusions
The WHO has long identified RSV-LRTI as a major cause of infant morbidity and mortality, but the existing evidence is still sparse and varies considerably both among countries and within regions. Our gap analysis—conducted outside North America, the EU, and a few Western Pacific nations—could find published evidence for only 13%–19% of the investigated countries within the WHO regions. When considering age groups, this TLR/gap analysis underscored missing evidence across all WHO regions in the neonate and infant age groups (≤3 and ≤6 months of age), even though they are most susceptible to RSV disease across all clinical outcomes and severities. Most of the reported outcomes pertained to hospitalizations, mortality or CFR, and viral detection rates, as available from AFRO (South Africa), AMRO (Argentina, Guatemala, and Mexico), EMRO (Jordan), EURO (Israel and Turkey), SEARO (India), and WPRO (Singapore). In contrast, information on hospital course and disease incidence was scant across regions. In addition to an underlying scarcity of published results, limitations in the study methodologies as well as a substantial variability in the reported outcomes might result both in an underestimation of burden and in challenges to any cross-study comparisons between countries or across WHO regions. To facilitate impact assessment of prevention strategies, research based on well-established methods and standardized protocols is needed to enhance the accuracy of national disease burden estimates.
Author contributions
RS: Conceptualization, Methodology, Validation, Writing – original draft, Writing – review & editing. JL: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. JA: Methodology, Validation, Writing – original draft, Writing – review & editing. ME: Validation, Writing – original draft, Writing – review & editing. JR: Validation, Writing – original draft, Writing – review & editing. MM: Validation, Writing – original draft, Writing – review & editing. KT: Conceptualization, Methodology, Project administration, Validation, Writing – original draft, Writing – review & editing. MF: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article. This study was sponsored by Pfizer.
Acknowledgments
The authors thank Cristiana Miglio and Daria Renshaw of IQVIA for medical writing and editorial support, which was funded by Pfizer.
Conflict of interest
RS, JA, ME, JLR, MM, KT, and MF are employees of Pfizer. JL is an employee of IQVIA, which received funding from Pfizer in connection with the development of this article and conducting the research.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2024.1452267/full#supplementary-material
References
1. Shi T, McAllister DA, O’Brien KL, Simoes EAF, Madhi SA, Gessner BD, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. (2017) 390(10098):946–58. doi: 10.1016/S0140-6736(17)30938-8
2. Li Y, Wang X, Blau DM, Caballero MT, Feikin DR, Gill CJ, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet. (2022) 399(10340):2047–64. doi: 10.1016/S0140-6736(22)00478-0
3. U.S. Centers for Disease Control and Prevention (CDC). RSV in Infants and Young Children. U.S. Centers for Disease Control and Prevention (CDC) (2024). Available online at: https://www.cdc.gov/rsv/infants-young-children/index.html (accessed June 1, 2024).
4. Vartiainen P, Jukarainen S, Rhedin SA, Prinz A, Hartonen T, Vabalas A, et al. Risk factors for severe respiratory syncytial virus infection during the first year of life: development and validation of a clinical prediction model. Lancet Digit Health. (2023) 5(11):e821–30. doi: 10.1016/S2589-7500(23)00175-9
5. Suh M, Movva N, Jiang X, Bylsma LC, Reichert H, Fryzek JP, et al. Respiratory syncytial virus is the leading cause of United States infant hospitalizations, 2009–2019: a study of the national (nationwide) inpatient sample. J Infect Dis. (2022) 226(Suppl 2):S154–63. doi: 10.1093/infdis/jiac120
6. Xie Z, Qin Q, Shen K, Fang C, Li Y, Deng T. The burden of respiratory syncytial virus associated with acute lower respiratory tract infections in Chinese children: a meta-analysis. Transl Pediatr. (2020) 9(4):496–506. doi: 10.21037/tp-20-148
7. Gebremedhin AT, Hogan AB, Blyth CC, Glass K, Moore HC. Developing a prediction model to estimate the true burden of respiratory syncytial virus (RSV) in hospitalised children in western Australia. Sci Rep. (2022) 12(1):332. doi: 10.1038/s41598-021-04080-3
8. Prasad N, Newbern EC, Trenholme AA, Wood T, Thompson MG, Aminisani N, et al. Respiratory syncytial virus hospitalisations among young children: a data linkage study. Epidemiol Infect. (2019) 147:e246. doi: 10.1017/S0950268819001377
9. Kobayashi Y, Togo K, Agosti Y, McLaughlin JM. Epidemiology of respiratory syncytial virus in Japan: a nationwide claims database analysis. Pediatr Int. (2022) 64(1):e14957. doi: 10.1111/ped.14957
10. Wildenbeest JG, Billard MN, Zuurbier RP, Korsten K, Langedijk AC, van de Ven PM, et al. The burden of respiratory syncytial virus in healthy term-born infants in Europe: a prospective birth cohort study. Lancet Respir Med. (2023) 11(4):341–53. doi: 10.1016/S2213-2600(22)00414-3
11. Carbonell-Estrany X, Simões EAF, Bont LJ, Gentile A, Homaira N, Scotta MC, et al. Identifying the research, advocacy, policy and implementation needs for the prevention and management of respiratory syncytial virus lower respiratory tract infection in low- and middle-income countries. Front Pediatr. (2022) 10:1033125. doi: 10.3389/fped.2022.1033125
12. Zhang S, Akmar LZ, Bailey F, Rath BA, Alchikh M, Schweiger B, et al. Cost of respiratory syncytial virus-associated acute lower respiratory infection management in young children at the regional and global level: a systematic review and meta-analysis. J Infect Dis. (2020) 222(Suppl 7):S680–7. doi: 10.1093/infdis/jiz683
13. Fitzpatrick MC, Laufer RS, Baral R, Driscoll AJ, Feikin DR, Fleming JA, et al. Report of the WHO technical consultation on the evaluation of respiratory syncytial virus prevention cost effectiveness in low- and middle-income countries, April 7–8, 2022. Vaccine. (2023) 41(48):7047–59. doi: 10.1016/j.vaccine.2023.09.040
14. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch WA, editors. Cochrane Handbook for Systematic Reviews of Interventions version 6.5. Cochrane (2024). Available online at: https://training.cochrane.org/handbook (updated August 2023) (accessed June 1, 2024).
15. Centre for Reviews and Dissemination. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care. York: Centre for Reviews and Dissemination, University of York (2009). Available online at: https://www.york.ac.uk/media/crd/Systematic_Reviews.pdf (accessed June 01, 2024).
16. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6(7):e1000097. doi: 10.1371/journal.pmed.1000097
17. World Health Organization. WHO Regional Offices. Geneva: WHO Headquarters (2024). Available online at: https://www.who.int/about/who-we-are/regional-offices (accessed June 01, 2024).
18. Assaf-Casals A, Ghanem S, Rajab M. Respiratory syncytial virus: prevalence and features among hospitalized Lebanese children. Br J Med Med Res. (2015) 6(1):77–87. doi: 10.9734/BJMMR/2015/12608
19. Alan S, Erdeve O, Cakir U, Akduman H, Zenciroglu A, Akcakus M, et al. Outcome of the respiratory syncytial virus related acute lower respiratory tract infection among hospitalized newborns: a prospective multicenter study. J Matern Fetal Neonatal Med. (2016) 29(13):2186–93. doi: 10.3109/14767058.2015.1079614
20. Ali A, Yousafzai MT, Waris R, Jafri F, Aziz F, Abbasi IN, et al. RSV associated hospitalizations in children in Karachi, Pakistan: implications for vaccine prevention strategies. J Med Virol. (2017) 89(7):1151–7. doi: 10.1002/jmv.24768
21. Atwell JE, Geoghegan S, Karron RA, Polack FP. Clinical predictors of critical lower respiratory tract illness due to respiratory syncytial virus in infants and children: data to inform case definitions for efficacy trials. J Infect Dis. (2016) 214(11):1712–6. doi: 10.1093/infdis/jiw447
22. Benitez-Guerra D, Pina-Flores C, Zamora-Lopez M, Escalante-Padron F, Lima-Rogel V, Gonzalez-Ortiz AM, et al. Respiratory syncytial virus acute respiratory infection-associated hospitalizations in preterm Mexican infants: A cohort study. Influenza Other Respir Viruses. (2020) 14(2):182–8. doi: 10.1111/irv.12708
23. Blau DM, Baillie VL, Els T, Mahtab S, Mutevedzi P, Keita AM, et al. Deaths attributed to respiratory syncytial virus in young children in high-mortality rate settings: report from child health and mortality prevention surveillance (CHAMPS). Clin Infect Dis. (2021) 73(Suppl_3):S218–28. doi: 10.1093/cid/ciab509
24. Buchwald AG, Tamboura B, Tennant SM, Haidara FC, Coulibaly F, Doumbia M, et al. Epidemiology, risk factors, and outcomes of respiratory syncytial virus infections in newborns in Bamako, Mali. Clin Infect Dis. (2020) 70(1):59–66. doi: 10.1093/cid/ciz157
25. Chu HY, Katz J, Tielsch J, Khatry SK, Shrestha L, LeClerq SC, et al. Respiratory syncytial virus infection in infants in rural Nepal. J Infect. (2016) 73(2):145–54. doi: 10.1016/j.jinf.2016.05.007
26. Cohen C, Walaza S, Treurnicht FK, McMorrow M, Madhi SA, McAnerney JM, et al. In- and out-of-hospital mortality associated with seasonal and pandemic influenza and respiratory syncytial virus in South Africa, 2009–2013. Clin Infect Dis. (2018) 66(1):95–103. doi: 10.1093/cid/cix740
27. Dearden CX, Jeevarathnum AC, Havinga J, Green RJ. The epidemiology of respiratory syncytial virus: a retrospective review from Steve Biko academic hospital 2013–2016. Afr J Thorac Crit Care Med. (2018) 24(1):30–5. doi: 10.7196/AJTCCM.2017.v24i1.163
28. Emukule GO, Khagayi S, McMorrow ML, Ochola R, Otieno N, Widdowson MA, et al. The burden of influenza and RSV among inpatients and outpatients in rural western Kenya, 2009–2012. PLoS One. (2014) 9(8):e105543. doi: 10.1371/journal.pone.0105543
29. Ferolla FM, Hijano DR, Acosta PL, Rodríguez A, Dueñas K, Sancilio A, et al. Macronutrients during pregnancy and life-threatening respiratory syncytial virus infections in children. Am J Respir Crit Care Med. (2013) 187(9):983–90. doi: 10.1164/rccm.201301-0016OC
30. Fischer Langley G, McCracken J, Arvelo W, Estevez A, Villarruel G, Prill M, et al. The epidemiology and clinical characteristics of young children hospitalized with respiratory syncytial virus infections in Guatemala (2007–2010). Pediatr Infect Dis J. (2013) 32(6):629–35. doi: 10.1097/INF.0b013e318289e3bc
31. Forman LS, Macleod W, Mwananyanda L, Kwenda G, Pieciak R, Mupila Z, et al. Association of respiratory syncytial virus infection and underlying risk factors for death among young infants who died at university teaching hospital, Lusaka Zambia. Clin Infect Dis. (2021) 73(Suppl_3):S180–6. doi: 10.1093/cid/ciab466
32. Freeman MC, Haddadin Z, Lawrence L, Piya B, Krishnaswami S, Faouri S, et al. Utility of RSV rapid diagnostic assays in hospitalized children in Amman, Jordan. J Med Virol. (2021) 93(6):3420–7. doi: 10.1002/jmv.26546
33. Geoghegan S, Erviti A, Caballero MT, Vallone F, Zanone SM, Losada JV, et al. Mortality due to respiratory syncytial virus. Burden and risk factors. Am J Respir Crit Care Med. (2017) 195(1):96–103. doi: 10.1164/rccm.201603-0658OC
34. Greenberg D, Dagan R, Shany E, Bar-Ziv J, Givon-Lavi N. Increased risk for respiratory syncytial virus-associated, community-acquired alveolar pneumonia in infants born at 31–36 weeks of gestation. Pediatr Infect Dis J. (2014) 33(4):381–6. doi: 10.1097/INF.0000000000000130
35. Hacimustafaoglu M, Celebi S, Bozdemir SE, Ozgur T, Ozcan I, Guray A, et al. RSV frequency in children below 2 years hospitalized for lower respiratory tract infections. Turk J Pediatr. (2013) 55(2):130–9.24192672
36. Kadmon G, Feinstein Y, Lazar I, Nahum E, Sadot E, Adam D, et al. Variability of care of infants with severe respiratory syncytial virus bronchiolitis. Pediatr Infect Dis J. (2020) 39(9):808–13. doi: 10.1097/INF.0000000000002707
37. Kalane SU, Somendra S, Patwardhan S, Joshi SA, Rajhans AP, Joshi RV. Clinical profile and outcome of respiratory syncytial virus-infected neonates—a single center experience. J Neonatol. (2022) 36(2):95–8. doi: 10.1177/09732179221100662
38. Kassem E, Na’amnih W, Bdair-Amsha A, Zahalkah H, Muhsen K. Comparisons between ethnic groups in hospitalizations for respiratory syncytial virus bronchiolitis in Israel. PLoS One. (2019) 14(4):e0214197. doi: 10.1371/journal.pone.0214197
39. Kazi AM, Aguolu OG, Mughis W, Ahsan N, Jamal S, Khan A, et al. Respiratory syncytial virus-associated mortality among young infants in Karachi, Pakistan: a prospective postmortem surveillance study. Clin Infect Dis. (2021) 73(Suppl_3):S203–9. doi: 10.1093/cid/ciab488
40. Khuri-Bulos N, Lawrence L, Piya B, Wang L, Fonnesbeck C, Faouri S, et al. Severe outcomes associated with respiratory viruses in newborns and infants: a prospective viral surveillance study in Jordan. BMJ Open. (2018) 8(5):e021898. doi: 10.1136/bmjopen-2018-021898
41. Komoyo GF, Yambiyo BM, Manirakiza A, Gody JC, Muller CP, Hubschen JM, et al. Epidemiology and genetic characterization of respiratory syncytial virus in children with acute respiratory infections: findings from the influenza sentinel surveillance network in Central African Republic, 2015 to 2018. Health Sci Rep. (2021) 4(2):e298. doi: 10.1002/hsr2.298
42. Kubale J, Kuan G, Gresh L, Ojeda S, Azziz-Baumgartner E, Sanchez N, et al. Assessing the incidence of symptomatic respiratory syncytial virus illness within a prospective birth cohort in Managua, Nicaragua. Clin Infect Dis. (2020) 70(10):2029–35. doi: 10.1093/cid/ciz585
43. Kyeyagalire R, Tempia S, Cohen AL, Smith AD, McAnerney JM, Dermaux-Msimang V, et al. Hospitalizations associated with influenza and respiratory syncytial virus among patients attending a network of private hospitals in South Africa, 2007–2012. BMC Infect Dis. (2014) 14:694. doi: 10.1186/s12879-014-0694-x
44. Luchsinger V, Ampuero S, Palomino MA, Chnaiderman J, Levican J, Gaggero A, et al. Comparison of virological profiles of respiratory syncytial virus and rhinovirus in acute lower tract respiratory infections in very young Chilean infants, according to their clinical outcome. J Clin Virol. (2014) 61(1):138–44. doi: 10.1016/j.jcv.2014.06.004
45. McCracken JP, Prill MM, Arvelo W, Lindblade KA, Lopez MR, Estevez A, et al. Respiratory syncytial virus infection in Guatemala, 2007–2012. J Infect Dis. (2013) 208(Suppl 3):S197–206. doi: 10.1093/infdis/jit517
46. Ochoa TJ, Bautista R, Davila C, Salazar JA, Bazan C, Guerra O, et al. Respiratory syncytial virus-associated hospitalizations in pre-mature infants in Lima, Peru. Am J Trop Med Hyg. (2014) 91(5):1029–34. doi: 10.4269/ajtmh.13-0648
47. Okiro EA, Ngama M, Bett A, Nokes DJ. The incidence and clinical burden of respiratory syncytial virus disease identified through hospital outpatient presentations in Kenyan children. PLoS One. (2012) 7(12):e52520. doi: 10.1371/journal.pone.0052520
48. Ozkan H, Celebi S, Koksal N, Hacimustafaoglu M, Koc E, Tezer H, et al. Risk factors for respiratory syncytial virus infections in moderate/late premature infants in Turkey: a prospective multicenter epidemiological study. Am J Perinatol. (2021) 38(14):1540–6. doi: 10.1055/s-0040-1713928
49. Rowlinson E, Dueger E, Taylor T, Mansour A, Van Beneden C, Abukela M, et al. Incidence and clinical features of respiratory syncytial virus infections in a population-based surveillance site in the Nile Delta region. J Infect Dis. (2013) 208(Suppl 3):S189–96. doi: 10.1093/infdis/jit457
50. Satav A, Crow R, Potdar V, Dani V, Satav S, Chadha M, et al. The burden of respiratory syncytial virus in children under 2 years of age in a rural community in Maharashtra, India. Clin Infect Dis. (2021) 73(Suppl_3):S238–47. doi: 10.1093/cid/ciab508
51. Simoes EAF, Dani V, Potdar V, Crow R, Satav S, Chadha MS, et al. Mortality from respiratory syncytial virus in children under 2 years of age: a prospective community cohort study in rural Maharashtra, India. Clin Infect Dis. (2021) 73(Suppl_3):S193–202. doi: 10.1093/cid/ciab481
52. Turkish Neonatal Society. The seasonal variations of respiratory syncytial virus infections in Turkey: a 2-year epidemiological study. Turk J Pediatr. (2012) 54(3):216–22.23094529
53. Tam CC, Yeo KT, Tee N, Lin R, Mak TM, Thoon KC, et al. Burden and cost of hospitalization for respiratory syncytial virus in young children, Singapore. Emerg Infect Dis. (2020) 26(7):1489–96. doi: 10.3201/eid2607.190539
54. Teck KS, Mac Guad R, Van Rostenberghe AH, Hua GS. Prevalence, risk factors and clinical characteristics of respiratory syncytial virus-associated lower respiratory tract infections in Kelantan, Malaysia. J Med Virol. (2019) 91(9):1608–15. doi: 10.1002/jmv.25500
55. Ueno F, Tamaki R, Saito M, Okamoto M, Saito-Obata M, Kamigaki T, et al. Age-specific incidence rates and risk factors for respiratory syncytial virus-associated lower respiratory tract illness in cohort children under 5 years old in the Philippines. Influenza Other Respir Viruses. (2019) 13(4):339–53. doi: 10.1111/irv.12639
56. Vizcarra-Ugalde S, Rico-Hernandez M, Monjaras-Avila C, Bernal-Silva S, Garrocho-Rangel ME, Ochoa-Perez UR, et al. Intensive care unit admission and death rates of infants admitted with respiratory syncytial virus lower respiratory tract infection in Mexico. Pediatr Infect Dis J. (2016) 35(11):1199–203. doi: 10.1097/INF.0000000000001262
57. Wu A, Budge PJ, Williams J, Griffin MR, Edwards KM, Johnson M, et al. Incidence and risk factors for respiratory syncytial virus and human metapneumovirus infections among children in the remote highlands of Peru. PLoS One. (2015) 10(6):e0130233. doi: 10.1371/journal.pone.0130233
58. Yanis A, Haddadin Z, Rahman H, Guevara C, McKay KG, Probst V, et al. The clinical characteristics, severity, and seasonality of RSV subtypes among hospitalized children in Jordan. Pediatr Infect Dis J. (2021) 40(9):808–13. doi: 10.1097/INF.0000000000003193
59. Zar HJ, Nduru P, Stadler JAM, Gray D, Barnett W, Lesosky M, et al. Early-life respiratory syncytial virus lower respiratory tract infection in a South African birth cohort: epidemiology and effect on lung health. Lancet Glob Health. (2020) 8(10):e1316–25. doi: 10.1016/S2214-109X(20)30251-5
60. Li Y, Johnson EK, Shi T, Campbell H, Chaves SS, Commaille-Chapus C, et al. National burden estimates of hospitalisations for acute lower respiratory infections due to respiratory syncytial virus in young children in 2019 among 58 countries: a modelling study. Lancet Respir Med. (2021) 9(2):175–85. doi: 10.1016/S2213-2600(20)30322-2
61. Welliver R. The relationship of meteorological conditions to the epidemic activity of respiratory syncytial virus. Paediatr Respir Rev. (2009) 10(Suppl 1):6–8. doi: 10.1016/S1526-0542(09)70004-1
62. Wittenauer R, Pecenka C, Baral R. Cost of childhood RSV management and cost-effectiveness of RSV interventions: a systematic review from a low- and middle-income country perspective. BMC Med. (2023) 21(1):121. doi: 10.1186/s12916-023-02792-z
63. Reichert H, Suh M, Jiang X, Movva N, Bylsma LC, Fryzek JP, et al. Mortality associated with respiratory syncytial virus, bronchiolitis, and influenza among infants in the United States: a birth cohort study from 1999 to 2018. J Infect Dis. (2022) 226(Suppl 2):S246–54. doi: 10.1093/infdis/jiac127
64. Duan Y, Jiang M, Huang Q, Jia M, Yang W, Feng L. Incidence, hospitalization, and mortality in children aged 5 years and younger with respiratory syncytial virus-related diseases: a systematic review and meta-analysis. Influenza Other Respir Viruses. (2023) 17(5):e13145. doi: 10.1111/irv.13145
65. Zheng Z, Warren JL, Artin I, Pitzer VE, Weinberger DM. Relative timing of respiratory syncytial virus epidemics in summer 2021 across the United States was similar to a typical winter season. Influenza Other Respir Viruses. (2022) 16(4):617–20. doi: 10.1111/irv.12965
66. Korsten K, Adriaenssens N, Coenen S, Butler CC, Verheij TJM, Bont LJ, et al. World health organization influenza-like illness underestimates the burden of respiratory syncytial virus infection in community-dwelling older adults. J Infect Dis. (2022) 226(Suppl 1):S71–8. doi: 10.1093/infdis/jiab452
67. Rha B, Dahl RM, Moyes J, Binder AM, Tempia S, Walaza S, et al. Performance of surveillance case definitions in detecting respiratory syncytial virus infection among young children hospitalized with severe respiratory illness-South Africa, 2009–2014. J Pediatric Infect Dis Soc. (2019) 8(4):325–33. doi: 10.1093/jpids/piy055
Keywords: respiratory syncytial virus, gap analysis, hospitalization rate, mortality, infants, lower respiratory tract infections, bronchiolitis, pneumonia
Citation: Sini de Almeida R, Leite J, Atwell JE, Elsobky M, LaRotta J, Mousa M, Thakkar K and Fletcher MA (2024) Respiratory syncytial virus burden in children under 2 years old in understudied areas worldwide: gap analysis of available evidence, 2012–2022. Front. Pediatr. 12:1452267. doi: 10.3389/fped.2024.1452267
Received: 20 June 2024; Accepted: 14 October 2024;
Published: 21 November 2024.
Edited by:
George A. Syrogiannopoulos, University of Thessaly, GreeceReviewed by:
Athanasios Michos, National and Kapodistrian University of Athens, GreeceHelena C. Maltezou, National Public Health Organization (EHEA), Greece
Copyright: © 2024 Sini de Almeida, Leite, Atwell, Elsobky, LaRotta, Mousa, Thakkar and Fletcher. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rodrigo Sini de Almeida, cm9kcmlnby5qLnNpbmlAcGZpemVyLmNvbQ==