 Wolfgang Kamin1*
Wolfgang Kamin1* Georg Seifert2
Georg Seifert2 Karl Zwiauer3
Karl Zwiauer3 Jan Bonhoeffer4Veerle De Ketelaere5Antonio D'Avino6Jakub Štádler7Juan Carlos Bustamante-Ogando8Ateş Kara9
Jan Bonhoeffer4Veerle De Ketelaere5Antonio D'Avino6Jakub Štádler7Juan Carlos Bustamante-Ogando8Ateş Kara9
- 1Department of Pediatrics, Clinic for Pediatrics and Adolescent Medicine, EVK Hamm, Hamm, Germany
- 2Department of Pediatrics with a Focus on Oncology and Hematology, Campus Virchow-Klinikum (CVK), Charité—University Medicine Berlin, Berlin, Germany
- 3Clinical Department of Pediatrics and Adolescent Medicine, St. Pölten University Hospital, Sankt Pölten, Austria
- 4Department of Infectiology and Vaccinology, University Children’s Hospital of Basel, Basel, Switzerland
- 5Pediatric Practice, Veldegem, Belgium
- 6FIMP (Italian Federation of Primary Care Pediatricians), National Health Care Service, Naples, Italy
- 7Children’s Immunology and Allergy Outpatient Centre, MY CLINIC Family Medical Clinic, Prague, Czechia
- 8Primary Immunodeficiencies Research Laboratory, National Institute of Pediatrics, Mexico City, Mexico
- 9Department of Pediatrics, Pediatric Infectious Disease, Hacettepe University, Ankara, Türkiye
Background: The need to reduce the inappropriate use of antibiotics for the treatment of pediatric acute respiratory tract infections (ARTIs) calls for therapeutic alternatives. The use of herbal medicines (phytopharmaceuticals) to treat ARTIs has increased worldwide. However, the evidence of phytopharmaceutical treatment, especially for children with ARTIs, has not yet been comprehensively presented.
Objective: To identify evidence on the efficacy and tolerability of phytopharmaceuticals in children suffering from ARTIs.
Methods: We searched the literature using two databases (PubMed and Cochrane Library) in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to identify records of clinical studies investigating the administration of phytopharmaceuticals in children with upper ARTIs (AURTIs) and/or lower ARTIs (ALRTIs).
Results: A total of 45 reports met the eligibility criteria and were included in our review. Of these, only nine reported double-blind, placebo-controlled trials investigating the efficacy and tolerability of phytopharmaceuticals in pediatric ARTIs. Overall, the included reports covered phytopharmaceuticals with the following single active ingredients: various purple coneflower (Echinacea purpurea L.) preparations, ivy (Hedera helix L.) leaf dry extract, African geranium (Pelargonium sidoides L.) root extract (EPs 7630), and pineapple fruit and stem extract preparation. In addition, various reports were included for fixed combination phytopharmaceutical products: eucalyptus oil combinations, five-herb fixed combination extract [BNO 1012 syrup], seven-herb fixed preparation [BNO 1030 solution], thyme herb and ivy leaf extracts, purple coneflower and sage leaf spray, thyme and primrose root extracts, and a preparation containing upper plant parts and roots of purple coneflower, propolis and vitamin C. The most robust efficacy and tolerability evidence available was found for EPs 7630: six double-blind, placebo-controlled trials, eight meta-analyses, four prospective open-label studies, and two observational studies, demonstrating efficacy and good tolerability.
Conclusion: Among the phytopharmaceuticals identified by our systematically conducted, comprehensive literature review, EPs 7630 is supported by sufficient evidence to be regarded as an appropriate treatment to reduce the severity and duration of AURTIs and ALRTIs in children. Regarding other phytopharmaceuticals reported in the literature for the treatment of pediatric ARTIs, further research is needed to close existing evidence gaps.
1 Introduction
Pediatric acute respiratory tract infections (ARTIs) are responsible for approximately 70% of antibiotic prescriptions in children (1). Current evidence-based practice guidelines consider almost 50% of these prescriptions unnecessary or problematic (2, 3). Moreover, inappropriate antibiotic treatment of ARTIs in children has contributed to the global problem of antibiotic resistance (4). The European Centre for Disease Prevention and Control (ECDC) endorses antimicrobial stewardship (AMS) as a strategy to help stop the current spread of antimicrobial resistance in Europe (4). The European Academy of Pediatrics (EAP) Curriculum for Common Trunk Training in Pediatrics also recommends that all European physicians practicing in pediatric healthcare should be educated to prescribe antibiotics to children in a rational way (4). Parents also play an important role in antibiotic prescription practices, and clinicians often cite parental misconceptions and expectations for antibiotics as reasons for unwarranted antibiotic prescribing (5–7). To reduce antibiotic expectations, communication within the consultation, prescribing behavior, as well as lay beliefs need to be addressed (8). In this regard, conducting pediatric clinical trials and educating physicians about the rational prescribing of medications to treat RTIs in children are of the utmost importance.
Plants represent potential sources of bioactive compounds such as essential oils, polyphenols, flavonoids, saponins, and alkaloids, which have been reported to relieve symptoms of acute upper respiratory tract infections (AURTIs) such as tonsillitis, tonsillopharyngitis, and rhinitis (9–13) and acute lower respiratory tract infections (ALRTIs) such as acute bronchitis and acute cough (12, 14, 15). Indeed, herbal medicines have traditionally been used to prevent and treat ARTIs and are scientifically valued (16). Phytotherapy is the contemporary definition for using preparations from plants, their parts, or active ingredients prepared from plants, purified and/or standardized using specific pharmaceutical technologies and proper galenic preparations for medicinal use (17). Phytopharmaceuticals are, therefore, final medicinal products with active ingredients derived from plants, parts of plants, or preparations made from plants or parts of plants (18). In accordance with the World Health Organization's (WHO) Traditional Medicine Strategy for 2014–2023, 179 member countries have advocated for the safety, quality, and efficacy of traditional and complementary medicine (19). This includes the correct use of medicinal plants and their derivatives for preventive or curative purposes according to the pharmacological properties of their chemical constituents (20).
Despite the existing scientific recognition of phytopharmaceuticals by regulatory authorities and WHO, many physicians and parents may still consider their medicinal properties to be based on “old wives’ tales” or “folklore” rather than evidence-based medicine (EBM) (21–23). Nevertheless, due to the significant increase in the prevalence of multidrug-resistant bacterial infections in children during the past couple of decades, phytopharmaceuticals have gained a resurgence of interest and popularity among allied health professionals in Western countries and worldwide. Real-world evidence from a retrospective cohort study evaluating 64,836 pediatric outpatients with RTIs showed that phytopharmaceuticals as first-line treatment for acute RTIs significantly reduced antibiotic prescriptions in the further course of the disease (24). Furthermore, a qualitative study from the UK reported that many patients would be willing to try phytopharmaceuticals to treat specific RTI symptoms if advised by their physician, whereas most physicians reported that they would recommend phytopharmaceuticals if evidence-based guidelines were available (25). Without the mention of suitable phytopharmaceuticals in many existing guidelines, a conscious effort is needed to enable physicians to identify, recognize correctly, and position phytopharmaceuticals in the clinical treatment pathway (25).
Education about the indications and uses of phytopharmaceuticals in pediatric RTIs is both reasonable and justified. Continuous critical assessment in accordance with EBM standards is required to demonstrate the efficacy of phytopharmaceuticals in children (26). However, most clinical evidence so far has only been in adults and is thus inadequate to support recommendations of phytopharmaceuticals for preventing or treating ARTIs in children (27, 28). To address this unmet need and identify gaps in existing evidence, we systematically searched the literature for clinical studies evaluating the efficacy and tolerability of phytopharmaceuticals in treating ARTIs in children.
2 Methods
2.1 Specifications
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline methodology (29) was used for a systematic search to identify reports on the use of phytopharmaceuticals in the treatment of ARTIs in children. Diseases of interest were the common cold, sore throat, acute bronchitis (AB), acute tonsillopharyngitis (ATP), and acute rhinosinusitis (ARS). Pneumonia, influenza, and obliterative bronchiolitis were not considered under the term ALRTI.
2.2 Search strategy
A comprehensive search was conducted using the PubMed and Cochrane Library databases, covering literature from January 1, 2000, to February 21, 2023. Both databases provide comprehensive, high quality reporting according to PRISMA guidelines. To ensure high coverage of the existing literature, a comprehensive search strategy was developed using the following terms in the Title/Abstract: (common cold; upper respiratory tract infection; acute respiratory tract infection; acute bronchitis; acute tonsillopharyngitis; sore throat; acute sinusitis; acute rhinosinusitis); AND (clinical trial; clinical study; randomized; randomised; OR meta-analysis); AND (therapy or treatment); NOT (Covid). No language restrictions were applied. Results were combined and exported to Endnote, where duplicate records and clinical registry records were removed. Manual internet searching was also performed without time period restrictions to identify additional relevant records.
2.3 Eligibility criteria and data extraction
Records were single-screened, first by examining the title and second by examining the abstract based on the inclusion/exclusion criteria. The full text report was retrieved and screened if the title or abstract met the inclusion criteria (or if eligibility was unclear). Three independent reviewers applied the eligibility criteria to all the retrieved reports. Full-text reports of systematic reviews with meta-analyses and clinical studies covering randomized trials or non-randomized studies (i.e., prospective cohort and observational studies), with efficacy and tolerability data regarding phytopharmaceuticals in children and/or adolescents with ARTIs, were included. Reports were excluded for the following reasons: abstract only, commentary, narrative review article, no phytopharmaceutical, and adults-only study. Non-English language reports retrieved in full were translated into English for review. Disputes were resolved by discussion. Eligible reports were grouped as relating to AURTIs or ALRTIs and reviewed in full.
2.4 Levels of evidence
Individual clinical studies were evaluated in accordance with the Oxford Center for Evidence-Based Medicine 2011 Levels of Evidence (OCEBM) (30). Table 1 shows the adapted version of the OCEBM levels of evidence used.
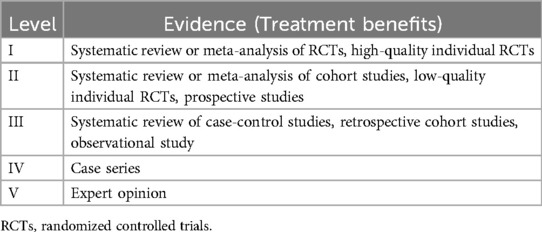
Table 1. Levels of evidence—adapted from Oxford center for evidence-based medicine (OCEBM) 2011 (30).
2.5 Grade of recommendation
Grades of recommendation for included phytopharmaceuticals were assigned according to the strength of evidence defined in Table 2. For example, to obtain the highest grade of recommendation (Grade A), consistent Level 1 studies had to be available.
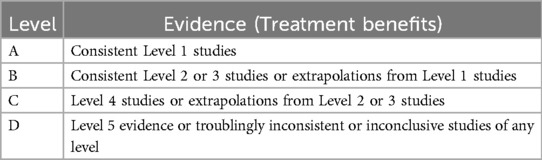
Table 2. Grades of recommendation—adapted from Oxford center for evidence-based medicine (OCEBM) 2011 (30, 85).
3 Results and discussion
3.1 Included reports
The database searches identified 8,192 database records. Of these, 218 were duplicates or removed for other reasons, resulting in 7,974 records to be screened by title and abstract. An additional 36 records (18 for AURTIs and 18 for ALRTIs) were identified from manual citation searching in parallel. Overall, 554 (413 for AURTIs and 141 for ALRTIs) reports were reviewed in full for eligibility and grouped according to phytopharmaceutical. Flowcharts of the literature search are depicted in Figures 1, 2.
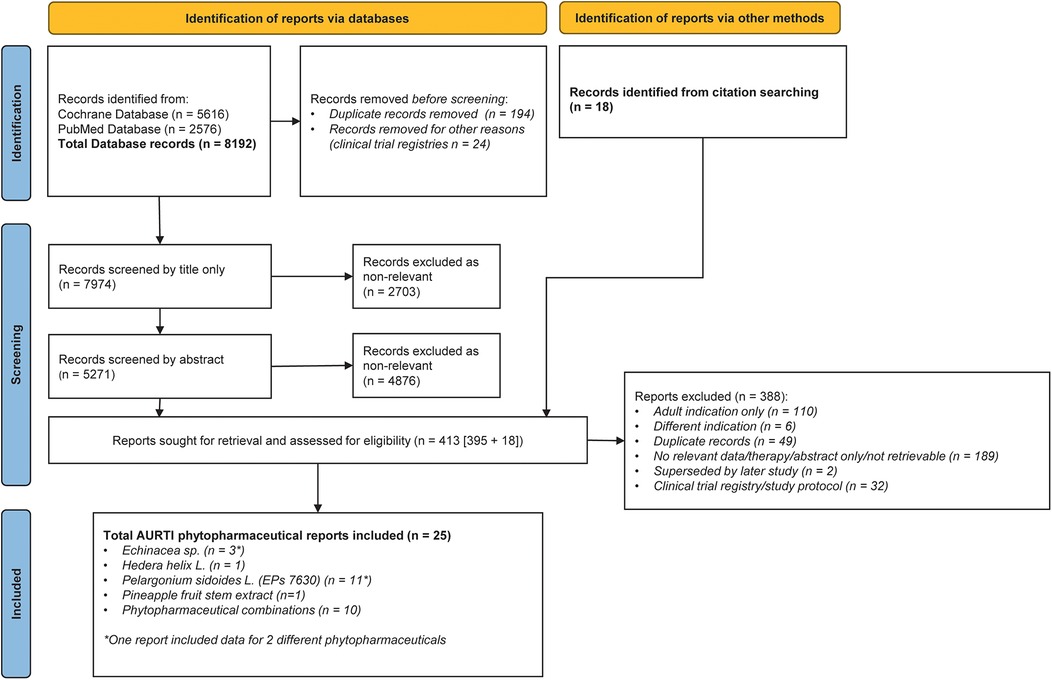
Figure 1. PRISMA diagram of reports relating to pediatric acute upper respiratory tract infections (AURTIs).

Figure 2. PRISMA diagram of reports relating to pediatric acute lower respiratory tract infections (ALRTIs).
For AURTIs, a total of 25 reports investigating the efficacy and tolerability of phytopharmaceuticals with single active ingredients or combinations in children met the eligibility criteria and could therefore be included for evidence evaluation (Table 3): one systematic review and meta-analysis of five relevant placebo-controlled, randomized controlled trials (RCTs) of which two were relevant in AURTIs (31)—this report was included twice for two different phytopharmaceutical groups; one systematic review with two relevant RCTs included in a meta-analysis (32); four meta-analyses of double-blind, placebo-controlled trials (12, 13, 33, 34); seven double-blind placebo-controlled trials (35–41); one triple-parallel group randomized trial (42); one single-blind, placebo-controlled randomized trial (43); five open-label randomized controlled trials (44–48); two prospective open-label studies (49, 50); two observational studies (51, 52); and one case-controlled study (53).

Table 3. Summary of phytopharmaceutical reports and level of evidence for AURTIs in children.
For ALRTIs, a total of 27 reports on studies investigating the efficacy and tolerability of phytopharmaceuticals with single active ingredients or combinations in children met the eligibility criteria and could therefore be included for evaluating evidence (Table 4): one systematic review and meta-analysis of 11 RCTs of which three double-blind placebo-controlled trials were relevant (54); one systematic review and meta-analysis of eight double-blind, placebo-controlled studies of which three were relevant (55); one systematic review and meta-analysis of five double-blind, placebo-controlled RCTs of which three were relevant (31); one meta-analysis of six RCTs that included three relevant RCTs (12); one meta-analysis of 7 RCTs of which three RCTs included children (34); one double-blind active comparator RCT (56); one Cochrane review and meta-analysis of three double-blind, placebo-controlled trials (57); five double-blind, placebo-controlled randomized trials (38, 41, 58–60); one open-label active-controlled RCT (61); one single-blind, placebo-controlled RCTs (62); four prospective studies (63–66); eight observational studies (51, 67–73); and one case-controlled study (53).
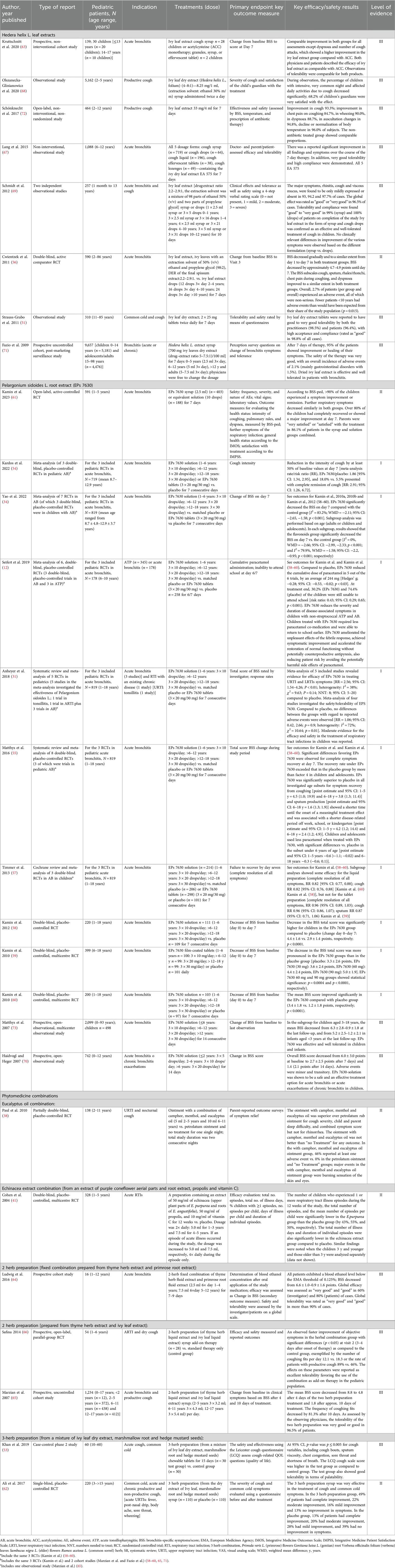
Table 4. Summary of phytopharmaceutical reports and level of evidence for ALRTIs in children.
Of the included reports for AURTIs and ALRTIs, seven reports (three meta-analyses/systematic reviews (12, 31, 34), one double-blind, placebo-controlled randomized trial (41), one partly double-blind placebo-controlled trial (38), one observational study (51) and one case-controlled study (53) contained relevant data on phytopharmaceuticals for the treatment of both AURTIs and ALRTIs. Both primary research (randomized trials and other types of studies) and secondary research (systematic reviews and meta-analyses) were included to capture essential information on efficacy and safety while providing a broader context through summarised findings. Therefore, the overall number of full text reports meeting the eligibility criteria for evaluating the efficacy and tolerability of phytopharmaceuticals for the treatment of children with URTIs and/or LRTIs combined was 45.
Below is a summary of the included studies by phytopharmaceutical group and indication (AURTI or ALRTI).
3.2 Preparations from Echinacea purpurea L. (purple coneflower)
A total of three reports (a systematic review/meta-analysis in AURTIs; one double-blind placebo-controlled randomized controlled trial; and one triple parallel-group randomized trial in AURTIs) could be evaluated for evidence of efficacy and tolerability of preparations from Echinacea purpurea L. for the treatment of children with AURTIs. In these reports, indications reporting on the efficacy and tolerability of preparations from Echinacea purpurea L. in treating symptoms of AURTI included common cold symptoms, otitis media, and unspecified ARTIs in a total of 1,498 children (Table 3).
3.2.1 Evidence in AURTIs
A double-blind, placebo-controlled randomized trial by Taylor et al. (36) conducted in 407 children showed no difference in AURTI symptom severity between Echinacea purpurea L. dried herb extract and placebo. A systematic review by Anheyer et al. identified four randomized controlled trials investigating the efficacy of various preparations from above-ground plant parts and/or roots, which, however, could not be subjected to a meta-analysis (Table 3) due to the heterogeneity of outcome measures and control conditions of these studies (31). A triple parallel-group, randomized trial in children with common cold symptoms compared an Echinacea preparation in combination with usual treatment, a herbal preparation containing Andrographis paniculata N. (green chiretta) in combination with usual treatment, and usual treatment alone (42). The results of the study indicated that all three groups experienced improvements in symptoms throughout the treatment period. However, children additionally receiving Echinacea also recovered faster from common cold symptoms compared to those who only received the usual treatment, although the authors did not specifically compare the effectiveness of Echinacea in these two groups (42).
3.2.2 Evidence in ALRTIs
No studies were available to evaluate the evidence of efficacy and tolerability of preparations from Echinacea purpurea L. for the treatment of children with ALRTIs.
3.3 Hedera helix L. (ivy) leaf dry extracts
A total of eight studies could be evaluated for evidence of the efficacy and tolerability of ivy leaf dry extracts for AURTIs and ALRTIs in children (Tables 3, 4): one double-blind, active comparator trial (56); two prospective cohort studies (63, 71); one open-label, non-interventional study (72); and four observational studies (51, 67–69); of note, one of these observational studies investigated the effectiveness of ivy leaf dry extract drops or syrup, with each treatment group evaluated as an independent non-interventional observational study (69).
3.3.1 Evidence in AURTIs
One observational study could be evaluated as evidence of the efficacy and tolerability of preparations from ivy leaf dry extracts for the treatment of children with AURTIs (51). An observational study published by Stauss-Grabo et al. showed positive results regarding the tolerability and safety of film-coated tablets containing ivy extract (cough tablets) for treating the common cold accompanied by coughing (51). However, results for children could not be separated from the overall group that also included adults (51).
3.3.2 Evidence in ALRTIs
A double-blind, active-controlled randomized trial published by Cwientzek et al. confirmed the safety/tolerability profile of ivy leaf, showing comparable beneficial effects of two different ivy leaf dry extract preparations on acute bronchitis in children (56).
One open-label, non-interventional study by Schönknecht et al. reported improvement in cough, chest pain on coughing, wheezing and dyspnea, auscultation changes and decline or normalization of body temperature in the majority of pediatric participants receiving a specific ivy leaf dry extract preparation for seven days (72). A prospective study by Fazio et al. indicated that ivy leaf dry extract might relieve cough and expectoration in acute and chronic bronchitis in children (71). This study also reported that ivy leaf dry extract treatment in children is well tolerated and shows a favorable safety profile (71). A prospective study by Kruttschnitt et al. (63) in children with acute bronchitis and an observational study by Olszanecka-Glinianowicz et al. (68) in children with productive cough also both reported improvement of symptoms using ivy leaf dry extract syrup. A specific ivy leaf dry extract given for ten days effectively reduced major acute bronchitis and cough symptoms in two pediatric observational studies on 257 children reported by Schmidt et al. (69).
A non-interventional, observational study by Lang et al. was conducted to assess the effectiveness and tolerability of five different dosage forms containing the ivy extract EA 575® in over 1,000 school children (ages 6–12 years) with acute bronchitis (67).The children's symptoms and overall condition significantly improved over the course of a seven-day therapy, and the dosage forms were well-tolerated with high compliance (67). All five EA 575 dosage forms were found to provide an effective and safe treatment for acute bronchitis in this group of children (67).
As mentioned above, the observational study published by Stauss-Grabo et al. demonstrated positive efficacy and safety results in children and adults taking film-coated tablets containing ivy extract (cough tablets) for treating the common cold accompanied by coughing (51). However, results for children could not be separated from the overall group that also included adults (51).
3.4 Pelargonium sidoides L. (African geranium) root extract (EPs® 7630)
A total of 20 reports were included showing evidence of EPs 7630 for the treatment of AURTIs and ALRTIs in children. Notably, three of the reports are included for both AURTI and ALRTI indications (12, 31, 34).
A total of 11 reports are included as evidence of clinical efficacy and tolerability of EPs 7630 in children with AURTI [acute tonsillopharyngitis (ATP) or sore throat]: three double-blind, placebo-controlled randomized trials (35, 39, 40); one systematic review of two randomized trials in children with tonsillitis or ARTIs (31); four meta-analyses of double-blind, placebo-controlled randomized trials (12, 13, 33, 34); one prospective, open randomized pilot study (48); and two prospective, open-label, non-controlled multicenter studies (49, 50). Notably, three of the meta-analyses evaluated varying aspects of the same three double-blind, placebo-controlled randomized controlled trials, which were Timen et al., Bereznoy et al., and Bereznoy et al. (35, 39, 40) (Table 3). A fourth meta-analysis by Kamin et al. (33) evaluated two double-blind, placebo-controlled, randomized controlled trials reported by Bereznoy et al. (35, 40).
A total of 12 reports are included as evidence of clinical efficacy and tolerability of EPs 7630 in children with ALRTI (acute bronchitis): three double-blind, placebo-controlled randomized trials (58–60); one open-label, active-controlled, randomized trial (61); one Cochrane review and meta-analysis (57); five meta-analyses and systematic reviews of various aspects of the same three double-blind, placebo-controlled trials in pediatric acute brocnhitis (12, 31, 34, 54, 55); and two prospective, open, observational studies (70, 73) (Table 4).
3.4.1 Evidence in AURTIs
Three double-blinded, placebo-controlled randomized trials—Bereznoy et al., Timen et al. and Bereznoy et al.—investigated the administration of EPs 7630 to children suffering from ATP (35, 39, 40). Bereznoy et al. reported that treatment with EPs 7630 reduced the severity of symptoms and shortened the duration of illness by at least two days (35). Similarly, Timen et al. and Bereznoy et al. provide evidence that EPs 7630 is superior compared to placebo for the treatment of acute tonsillopharyngitis in children and is well tolerated (39, 40).
The identified meta-analyses reported by Seifert et al. and Anheyer et al. are described in Section 3.4.3 because results were pooled for AURTIs and ALRTIs indications (12, 31). Two more meta-analyses reported by Seifert et al. and Yao et al. included the three above-mentioned double-blind, placebo-controlled trials in children with ATP (13, 34). The analysis by Seifert et al. showed that, compared with placebo, EPs 7630 reduced the cumulative paracetamol dose by an average of 449 mg [95% confidence interval (CI): 252, 646 mg; p < 0.001] (13). A total of 19.1% (EPs 7630) and 71.5% (placebo) of children with ATP were still unable to attend school at the end of the treatment. According to the authors, the meta-analysis results demonstrate that EPs 7630 reduces the use of antipyretic comedication and accelerated recovery in children with ATP (13). Similarly, the meta-analysis by Yao et al. showed that EPs 7630 significantly decreased the TSS on day seven compared with the control group with no heterogeneity (34). This meta-analysis pooled the above mentioned three double-blind, placebo-controlled RCTs to analyze the primary outcome measure change of tonsillitis severity score (TSS) on day seven compared to baseline in patients with acute non-streptococcal tonsillopharyngitis. In the EPs 7630 group, the TSS was significantly decreased on day seven compared with the control group (p < 0.001). In addition, the complete improvement rate of symptoms, including fever, headache, difficulty in swallowing, sore throat, salivation, and pharyngeal erythema was significantly increased in the EPs 7630 group vs. the control group on day four (p < 0.001 for all). Pooled results of these three RCTs (35, 39, 40) with 345 children also showed that the incidence of adverse events did not differ between EPs 7630 and placebo groups (34).
A meta-analysis by Kamin et al. (33), which included the two double-blind, placebo-controlled randomized trials by Bereznoy et al. (35) and Bereznoy et al. (40), reported significantly pronounced improvement of the symptom “sore throat” after four days compared to placebo treatment, and a significant advantage of EPs 7630 compared to placebo for patients with complete remission of the symptom “sore throat” by day four. Therapy response rates under EPs 7630 by day four were reported to be significantly higher than those achieved under placebo. These results show that EPs 7630 effectively reduces the severity and time to remission of the symptom “sore throat” in children with acute non-streptococcal tonsillopharyngitis.
In a prospective, open, single-center randomized pilot study by Blochin and Heger (48), the efficacy and tolerability of EPs 7630 was compared to symptomatic treatment in children with acute tonsillitis. Results showed that EPs 7630 improved symptoms more rapidly, was better tolerated by the children, and was therefore concluded by the authors to be a superior choice for treating acute tonsillitis (48).
In a prospective, open-label study reported by Schapowal and Heger (49), EPs 7630 effectively relieved or improved symptoms of acute sinusitis in adults and children. Notably, a separate effectiveness analysis in children was not conducted. However, a subgroup analysis of a self- assessed health compliant questionnaire (HCQ-5) was analyzed for 30 children; the HCQ-5 score decreased from an initial 14.2 points to 6.8 points after 28 days (49).
A second prospective open-label study reported by Bereznoy et al. in over 1,000 patients (adults and children) with acute tonsillitis or chronic recurrent tonsillitis showed remission and/or improvements in symptoms for patients treated with EPs 7630, which was also well tolerated. The overall responder rate by day seven was 88.2% (50). However, results for children could not be separated from the overall group that also included adults.
3.4.2 Evidence in ALRTIs
In three double-blind, placebo-controlled randomized trials [Kamin et al. (59), Kamin et al. (60) and Kamin et al. (58)], it was demonstrated that EPs 7630 treatment for seven days decreased the bronchitis symptom score in children with acute bronchitis as compared to baseline and to a significantly greater extent compared to placebo. Results from a recent open-label, active-controlled randomized trial conducted by Kamin et al. (61) in children under six years are also in line with the efficacy and safety/tolerability results reported in the three previously mentioned double-blind, randomized trials. In addition, the open-label study reported that the majority of parents (86.1%) were “very satisfied” or “satisfied” with the EPs 7630 treatment of their child (61).
A Cochrane review and meta-analysis by Timmer et al. (57) analyzed, among others, the above three double-blind, placebo-controlled trials [i.e., Kamin et al. (58–60)] and found that EPs 7630 may effectively relieve acute bronchitis symptoms in children. The authors of the meta-analysis reported, however, that the narrow spectrum of included studies could compromise the representativeness of the evidence (57).
A meta-analysis by Yao et al. (34) pooled seven RCTs investigating the efficacy and safety/tolerability of EPs 7630, which included a subgroup analysis of children and adolescents in the already mentioned three double-blinded, placebo-controlled randomized trials in children with acute bronchitis [i.e., Kamin et al. (58–60)]. Overall, the authors concluded that EPs 7630 may effectively relieve symptoms of acute bronchitis in children (and adults). The overall quality of the evidence was considered low for primary outcomes in acute bronchitis in children and adults. Still, it is not possible to extract the data on children only.
A meta-analysis by Kardos et al. (54) pooled data from the same three double-blind, placebo-controlled randomized trials in pediatric acute bronchitis [i.e., Kamin et al. (59), Kamin et al. (60) and Kamin et al. (58)]. A decrease in cough intensity was observed by at least 50% of children with EPs 7630 vs. placebo, as well as complete remission in cough for 18.0% of children in the EPs 7630 group compared to 5.5% in the placebo group.
In a meta-analysis by Matthys et al. (55) evaluating the change of BSS total score between baseline and treatment day seven in patients with acute bronchitis, five randomized trials were pooled, including the same three double-blind, placebo-controlled randomized trials in pediatric acute bronchitis [i.e., Kamin et al. (59), Kamin et al. (60) and Kamin et al. (58)]. The authors concluded that EPs 7630 is an efficacious, safe, and well-tolerated phytomedicine in managing acute RTIs, including acute bronchitis, in children, adolescents, and adults (55). A separate analysis in children only was not conducted.
In two prospective, open-observational studies [Matthys et al. (73) and Haidvogl and Heger (70)], EPs 7630 was also shown to be a safe and effective treatment option for acute bronchitis in children and infants.
3.4.3 Pooled evidence in AURTIs and ALRTIs
Results for AURTIs and ALRTIs are pooled in two meta-analyses reported by Seifert et al. (12) and Anheyer et al. (31). The meta-analysis reported by Seifert et al. evaluated average cumulative paracetamol use and the number of children unable to go to school at day six (acute tonsillopharyngitis) or day seven (acute bronchitis) after start of EPs 7630 treatment compared to placebo in 523 children aged six to ten years (12). Compared with placebo, EPs 7630 reduced the cumulative paracetamol dose significantly by an average of 244 mg (p < 0.03) (12). A total of 30.2% (EPs 7630 group) and 74.4% (placebo group) of children with acute tonsillopharyngitis or acute bronchitis were still unable to attend school at the end of the treatment, corresponding to a meta-analysis risk ratio of 0.43 (p < 0.001) favoring EPs 7630. (p < 0.001) (12). The systematic review and meta-analysis by Anheyer et al. (31) reported separate analyses showing evidence of EPs 7630 compared to placebo in treating ARTI symptoms for efficacy, based on five pooled placebo-controlled RCTs (35, 58–60, 74) and for tolerability/safety, based on four pooled placebo-controlled RCTs (35, 58–60). The authors reported that EPs 7630 showed moderate evidence of efficacy and safety in treating AURTIs and ALRTIs (tonsillitis, acute bronchitis, ARTIs with transient hypogammaglobulinemia) in children and concluded that EPs 7630 could thus be considered an adjunctive therapy option for RTIs in children.
3.5 Pineapple fruit and stem extract
3.5.1 Evidence in AURTIs
One report is included as evidence of pineapple fruit and stem extract for the treatment of AURTIs, namely rhinosinusitis, in children: The meta-analysis of two double-blind, randomized trials in children, adolescents, and adults (9 years–74 years) showed small but statistically significant intergroup differences that favored pineapple fruit and stem extract vs. standard treatment (antibiotics, antihistamines or analgesics) for nasal mucosal inflammation, nasal discomfort, breathing difficulty, and overall rating, but not for nasal discharge (32). However, results for children could not be separated from the overall group that also included adults.
3.5.2 Evidence in ALRTIs
No reports could be evaluated for evidence of the efficacy and tolerability of pineapple fruit and stem extract for treating children with AURTIs.
3.6 Various fixed combination herbal preparations—evidence in AURTIs and ALRTIs
3.6.1 Combined preparations with eucalyptus oil
Two studies evaluated the effectiveness and tolerability of combination products containing eucalyptus oil for symptoms of AURTIs such as acute rhinosinusitis [one observational study (52)] or nocturnal cough [one partially double-blind placebo-controlled trial (38)].
In an observational study by Karpova et al. (52), the duration of nasal vasoconstrictor use as a symptomatic therapy was reduced in children taking a preparation containing eucalyptus oil, among other ingredients [monoterpenes (orange oil)/d-limonene (lemon oil)/1,8-cineole (eucalyptus oil)/alpha-pinene (myrtle oil)] by 2.2 days vs. 3.6 days in the children from the control group.
An ointment containing camphor, menthol, and eucalyptus oil was compared with petroleum ointment and no treatment in a double-blind, randomized trial in 138 children with nocturnal cough (38). Parents rated the camphor, menthol, and eucalyptus oil ointment (applied on one evening only) as more favorable than petroleum ointment and no treatment for symptomatic relief of their child's nocturnal cough, congestion, and sleep difficulty caused by URTIs (38). Petroleum ointment alone was marginally better for no cough frequency treatment but not better for cough severity than no treatment (38). Although irritant adverse effects were more common among participants treated with the eucalyptus oil combination, child and parent sleep was reported to be improved overall compared with petroleum and no treatment (38). Notably, the study lasted for only two consecutive days with one single application of the camphor, menthol, and eucalyptus oil ointment for symptoms of RTIs in children.
3.6.1.1 Echinacea extract combination [from an extract echinacea (aerial parts of Echinacea purpurea L. and roots Echinacea angustifolia), propolis and vitamin C]
In a randomized, double-blind, placebo-controlled study, Cohen et al. evaluated a herbal preparation containing echinacea extract, propolis and vitamin C (10 mg/ml) in order to assess its effectiveness in preventing RTIs in children from 1 to 5 years (of age) (41). Children receiving the combination experienced a 55% reduction in the number of illness episodes and a 62% reduction in the number of days with fever, as well as an overall decrease in the total number of days with symptomatic illness (41).
3.6.1.2 Two-herb preparation [from a mixture of Echinacea purpurea L. (purple coneflower) aerial herb parts and root extract and Salvia officinalis L. (sage) leaves]
A double-blind, double-dummy controlled trial reported by Schapowal et al. (37) found that a spray of a two herb preparation containing an aerial herb and root extract from purple coneflower and the leaves from sage herb was at least as effective as over-the-counter chlorhexidine/lidocaine spray for sore throat in children (Table 3).
3.6.1.3 Two-herb preparation [from a fixed combination of Thymus vulgaris L. (thyme) herb extract and Primula veris L./Primulus elatior L. (primrose) root extract]
One observational study by Ludwig et al. (64) documented the effectiveness of the fixed combination of a thyme herb extract and primrose root extract for treating acute bronchitis in children. The study reported that blood ethanol concentrations after oral administration of the ethanol-containing preparation in children from 1 to 12 years of age remain considerably below the EMA safety threshold (64).
3.6.1.4 Two-herb preparation [from a mixture of Thymus vulgaris L. (thyme) herb liquid extract and Hedera helix L. (ivy) leaf liquid extract]
In an open-label, prospective, randomized, parallel-group study, a two-herb preparation with thyme herb extract and ivy leaf extract was investigated as an add-on therapy to standard medication in children with recurrent acute viral respiratory tract infections (66). The study found that during one week of treatment, the group receiving the two-herb preparation showed a faster improvement in objective symptoms compared to the control group with standard medication alone. There were significant differences in coughing fits per day and the rate of patients with productive cough, with the two-herb preparation group showing better outcomes (66). The two-herb preparation was well-tolerated, and based on the study's findings, it suggests that this preparation could be considered an effective add-on therapy for children with recurrent respiratory tract infections accompanied by dry cough (66).
A prospective, uncontrolled cohort study by Marzian et al. evaluated a two-herb preparation of thyme herb liquid extract and ivy leaf liquid extract for treating acute bronchitis and productive cough in 1,234 children (65). The study reported decreased clinical symptoms with the two-herb preparation, including cough from baseline and good tolerability in 96.5% of pediatric subjects (65).
3.6.2 Three-herb preparation [from a mixture of althea officinalis L. [marshmallow] root, Sisymbrium irio L. [hedge mustard] seeds and Hedera helix L. [ivy] leaf dry extract]
The safety and efficacy of a three-herb preparation (chewable tablets) were evaluated for the treatment of ARTIs, including the common cold and cough, compared to control tablets (53). After 15 days of treatment, the effectiveness of the chewable tablets was assessed using a clinical trial questionnaire and a validated quality of life questionnaire. The results showed significant improvements in cough variables such as cough bouts, sputum viscosity, chest congestion, sore throat, and shortness of breath (53). The test group also had a higher cough scale score on the LCQ and was well-tolerated in terms of palatability. No side effects were reported, and the recipients of the three-herb preparation showed good compliance with the medication compared to the control group (53).
A single-blind, placebo-controlled randomized study by Khan et al. (43) reported that cough granules containing a mixture of marshmallow root, hedge mustard seed and ivy leaf powdered extract was effective in relieving AURTI symptoms in children (i.e., sneezing, stuffy nose, sore throat/chest discomfort, fatigue/weakness, post nasal drip) (43). This study also evaluated the effectiveness of this preparation in children with ALRTI symptoms, including chronic cough (Table 3).
A single-blind, randomized trial by Ali et al. evaluated syrup containing powdered extract of ivy leaf dry extract, marshmallow root and mustard seeds, and reported the three-herb preparation to be effective compared to placebo at reducing cough and common cold symptoms in children (62).
3.6.3 Five-herb extract (prepared from extracts of Primula veris L. [primrose] flowers/Gentiana lutea L. [gentian] root/Verbena officinalis folium [verbena] leaves/Sambucus nigra L. [elder] flowers/Rumex acetosa L. [common sorrel] herb)
For AURTIs, three open-label prospective randomized studies evaluated the efficacy of a five-herb extract preparation (extracts of primrose flowers, gentian root, verbena leaves, elder flowers and common sorrel herb) for treating acute rhinosinusitis symptoms in children (44, 45, 47).
The open-label, prospective study published by Sen'kevich et al. compared the five-herb extract preparation (oral drops) with topical decongestants and topical decongestants plus antibiotics in 107 children with ARTIs, including acute rhinosinusitis symptoms (44). The study found that after a 14-day treatment period with the five-herb extract preparation, there was a notable decrease in nasal congestion, a reduction in nasal discharge, and a decrease in the quantity of blocked nasal passages (44). Moreover, the five-herb extract combination eliminated mucositis, which contributed to faster restoration of the drainage and ventilation function of the auditory tube, restored mucociliary clearance, improved the condition and well-being of children, improved the effectiveness of therapy and shortened the treatment time (44). A second open-label prospective study by Popovych et al. also reported positive effects with a five-herb extract syrup preparation, including a clinically significant, adequate reduction in the severity of rhinorrhea, nasal congestion and post-nasal drip, as well as a reduction in the prescription of antibiotics in children with acute rhinosinusitis (47). A third study investigated the efficacy and tolerability of a five-herb extract preparation (extract BNO 1012 syrup) in another open-label, prospective, interventional randomized study (45). The authors concluded that extract BNO 1012, in addition to standard symptomatic treatment of acute rhinosinusitis, provides a clinically significant, adequate reduction in the severity of rhinorrhea, nasal congestion and post-nasal drip and also leads to a reduction in the need for antibiotic use in children with acute rhinosinusitis (45) (Table 3).
3.6.4 Seven-herb extract (prepared from a mixture of Equisetum arvense L. [horsetail] herb/Achillea millefolium L. [yarrow] herb/Althaea officinalis L. [marshmallow] root/Juglans regia L. [walnut] leaves Taraxacum officinale FH Wigg. [dandelion] plant greens Matricaria recutita L. [chamomile]/Quercus robur L. and Quercus pubescens Willd [oak bark])
The safety and tolerability of a seven-herb preparation (extract BNO 1030 solution containing a mixture of marshmallow root, chamomile flowers, horsetail herb, walnut leaves, yarrow herb, oak bark, and dandelion herb) plus standard antipyretic symptomatic therapy was evaluated in one open-label, randomized trial vs. standard therapy in 238 children with acute non-bacterial tonsillitis (46). The authors reported that the extract preparation of the seven-herb mixture plus standard symptomatic therapy alleviated local and general symptoms starting from day two of the disease compared with standard therapy alone. Moreover, adding the seven-herb mixed extract to standard antipyretic therapy enabled a withdrawal of antipyretics from day four (46) (Table 3).
No reports could be evaluated for evidence of efficacy and tolerability of the seven-herb extract preparation for the treatment of children with ALRTIs.
4 Discussion
Overall, nine of the 45 reports included were double-blind, placebo-controlled trials. Of these, six RCTs investigated the treatment of ARTIs with EPs 7630 in children. EPs 7630 was the only phytopharmaceutical with sufficient evidence to make a strong recommendation for the treatment of ARTIs in children (level of evidence/grade of recommendation: IA). One double-blind, placebo-controlled trial indicated that an Echinacea extract preparation was not effective in pediatric AURTIs. However, in contrast, one double-blind, placebo-controlled randomized study suggested the possible efficacy of an Echinacea extract combination (from an extract of purple coneflower aerial parts and root extract, propolis and vitamin C) in ARTIs (level of evidence/grade of recommendation: IIC). Weak evidence from one partially double-blind, placebo-controlled trial suggested that a camphor, menthol and eucalyptus oil ointment may help relieve sleep disturbances and reduce symptoms in children with RTIs (level of evidence/grade of recommendation: IIC). In addition to the nine double-blind, placebo-controlled trials, one double-blind, active-controlled randomized study suggests possible efficacy and safety of ivy leaf dry extract in ALRTIs (level of evidence/grade of recommendation: IIC).
Evidence that other phytopharmaceuticals phytopharmaceutical combinations are beneficial in the treatment of pediatric AURTIs and ALRTIs is limited. A summary of the evidence and recommendations by phytomedicine is provided below.
4.1 Echinacea herb preparations
Echinacea purpurea L. is a medicinal herb that contains various constituents reported to have various pharmacological and clinical effects (75). Preparations from Echinacea purpurea L. have been reported to have immunomodulatory, antiviral, and anti-inflammatory effects that have been suggested to contribute to the observed clinical benefits in adults to lower the risk of recurrent respiratory infections (76). Overall, our literature search identified weak evidence from studies in children to recommend Echinacea purpurea L. preparations as an effective treatment for AURTI symptoms such as otitis media and common cold in children. Due to a complete lack of reports, it is also not possible to recommend Echinacea purpurea L. preparations for treating pediatric ALRTIs.
4.2 Hedera helix L. leaf dry extract
Hedera helix L. contains saponins that are considered to have mucolytic, spasmolytic, bronchodilatory, and antibacterial effects (77). Our research retrieved only one double-blind, active-controlled randomized study as evidence for the possible efficacy and safety of ivy leaf dry extract in ALRTIs (level of evidence/grade of recommendation: IIC). Insufficient evidence was found that ivy leaf dry extracts might effectively improve AURTI symptoms in children. Therefore, randomized controlled trials in children with URTIs and LRTIs treated with ivy leaf dry extracts are warranted.
4.3 Pelargonium sidoides root extract (EPs 7630)
The Pelargonium sidoides root extract EPs 7630 (Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany) is a proprietary extract from the roots of the native South African plant Pelargonium sidoides L., drug extract ratio 1:8–10, extraction solvent: ethanol 11% (w/w), which is widely used to treat AURTI and ALRTI (78). It is approved as a medicinal product in numerous countries in Europe, Asia, Australia, and Central and South America for the treatment of children, adolescents, and adults (78). EPs 7630 has been shown to exhibit multiple pharmacological properties, including antiviral and immunomodulatory effects (79–83). Moreover, EPs 7630 and other Pelargonium sidoides extracts contain a variety of constituents from different compound classes, including amino acids, polyphenols, flavonoids, coumarins, vitamins, and minerals. EPs 7630 in various application forms is approved in Germany and other countries inside and outside Europe for treatment of, e.g., acute bronchitis, but also for other acute respiratory tract infections in children aged one year and over. A total of 20 reports from 45 (44.4%) are included as evidence for the efficacy and tolerability of EPs 7630 treatment for AURTIs and ALRTIs in children. The most extensive randomized clinical data in children in our study was retrieved for EPs 7630 in ARTIs (six double-blind, placebo-controlled, randomized trials). Overall, the clinical evidence strongly suggests that EPs 7630 solution is superior to placebo in reducing the severity and duration of disease-associated symptoms in children with acute non-streptococcal ATP (Table 3; level of evidence/grade of recommendation: IA). Similarly, the clinical evidence strongly suggests that EPs 7630 is an appropriate treatment to reduce the severity and duration of ARTI-related symptoms in children with acute bronchitis (Table 4; level of evidence/grade of recommendation: IA).
4.4 Pineapple fruit and stem extract preparation
Due to limited evidence, it is currently not possible to recommend pineapple fruit and stem extract preparations as an effective treatment for ARTIs in children.
4.5 Herbal preparations with eucalyptus oil
Eucalyptus oil has antitussive effects, among other benefits, and is primarily used to treat coughs, colds, and bronchitis and for symptomatic relief of common cold and catarrh of the upper respiratory tract (84). It is obtained by steam distillation and rectification from the fresh leaves or the fresh terminal branchlets of various species of Eucalyptus rich in 1,8-cineole (84). Due to limited evidence, it is currently not possible to recommend eucalyptus oil preparations as an effective treatment for ARTIs in children.
4.6 Other combinations of herb extracts/preparations
Although one randomized double-dummy trial indicated that the two-herb preparation with a mixture of purple coneflower aerial herb parts and root extract might help alleviate symptoms in children with sore, further randomized trials are required. Although other two-herb preparations such as a combination of thyme herb extract and ivy leaf dry extract showed promise in prospective studies, robust clinical data is lacking and randomized controlled studies in pediatric RTI populations are warranted. Similarly, evidence of the effectiveness and safety of a three herb preparation from a mixture of ivy leaf dry extract, marshmallow root and hedge mustard seeds are lacking. Therefore, there is insufficient evidence to recommend any of the cited two- or three-herb preparations as effective treatments for symptoms of AURTIs or ALRTIs in children.
A five-herb extract (prepared from extracts of primrose flowers, elder flowers, common sorrel herb, gentian root and lemon verbena leaves) is reported to have various pharmacological activities, such as secretolytic, expectorant, anti-inflammatory, diuretic, antimicrobial, antifungal, and sedative [7–10]. Overall, the clinical evidence suggests that the five-herb extract may be an effective adjunctive treatment for AURTI symptoms such as acute rhinosinusitis in children (level of evidence/grade of recommendation: IIC). Due to the paucity of evidence, however, it is currently not possible to recommend this five-herb extract as an effective treatment for ALRTIs in children.
Due to the limited clinical evidence, it is also not currently possible to recommend a seven-herb extract (prepared from a mixture of horsetail herb, yarrow herb, marshmallow root, walnut leaves, dandelion herb, chamomile flowers and oak bark) as an effective treatment for symptoms of AURTIs or ALRTIs in children.
We acknowledge that our findings may be subject to the general limitations of systematic reviews pertaining to potential incompleteness of the reviewed evidence and searched databases. Publication bias and location bias cannot be completely ruled out, including the tendency for negative trials to remain unpublished. Moreover, no formal assessment of bias or meta-analysis could be realized due to the heterogeneity of included study types and their variable quality. Although we performed a broad search for all RTIs in children, only a limited number of conditions were covered in the included clinical trials.
5 Conclusion
This systematically conducted, comprehensive literature review presents a comprehensive summary of the available evidence regarding the effectiveness and safety of phytopharmaceuticals for treating acute respiratory tract infections in children. The review found a lack of high-quality randomized controlled trials assessing the efficacy and tolerability of many phytopharmaceuticals in children with ARTI. Evidence for the safety and efficacy of several phytopharmaceutical preparations for the treatment of ARTIs in children are available: echinacea extract combination (from an extract of purple coneflower aerial parts and root extract, propolis and vitamin C), camphor, menthol and eucalyptus oil ointment, ivy leaf dry extract and EPs 7630. However, Pelargonium sidoides L. root extract (EPs 7630) had the strongest evidence in the pediatric population. Robust data from six double-blind, randomized, placebo-controlled clinical trials demonstrates that EPs 7630 administration in children might alleviate ARTI symptoms, reduce their severity, expedite functional recovery and decrease the need for paracetamol use. There remains a need for well-designed, randomized, placebo-controlled clinical trials to investigate the efficacy and safety of other phytopharmaceuticals for pediatric ARTI treatment.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
WK: Conceptualization, Data curation, Formal analysis, Validation, Writing – original draft, Writing – review & editing. GS: Conceptualization, Data curation, Formal analysis, Validation, Writing – original draft, Writing – review & editing. KZ: Conceptualization, Data curation, Formal analysis, Validation, Writing – original draft, Writing – review & editing. JB: Conceptualization, Data curation, Formal analysis, Validation, Writing – review & editing. VDK: Data curation, Formal analysis, Validation, Writing – original draft, Writing – review & editing. AD’A: Data curation, Formal analysis, Validation, Writing – original draft, Writing – review & editing. JŠ: Data curation, Formal analysis, Validation, Writing – original draft, Writing – review & editing. JCB-O: Data curation, Formal analysis, Validation, Writing – original draft, Writing – review & editing. AK: Data curation, Formal analysis, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The authors declare that this study received funding from X Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Acknowledgments
Ellen Heitlinger (EH), H+O communications Ltd., Zurich, Switzerland, provided medical writing services and editorial assistance. An independent review of the systematic search results was conducted by three reviewers of H+O communications Ltd., Zurich, Switzerland. Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany, funded the medical writing services and editorial assistance.
Conflict of interest
The authors declare that this research received funding from Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany. The funder was not involved in the literature search presented. Medical writing services and editorial assistance provided by Ellen Heitlinger (EH), H+O communications Ltd., Zurich, Switzerland, were funded by Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany. This study is independent of any bias based on the funding source. Final decision to submit the manuscript for publication remained with the authors. WK, GS, KZ, JB, VDK, AD'A, JŠ, JCB-O and AK (all authors) have received fees from Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany for their contribution to this work. GS has received fees for lectures and scientific advice from the companies Schwabe and Engelhardt. JB has served as an independent member of the scientific advisory board of Dr Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany and was reimbursement as a speaker in two scientific conferences. JCB-O has served as a speaker for Schwabe, Novartis, Takeda, Carnot, CSL Behring.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. O'Brien K, Bellis TW, Kelson M, Hood K, Butler CC, Edwards A. Clinical predictors of antibiotic prescribing for acutely ill children in primary care: an observational study. Br J Gen Pract. (2015) 65(638):e585–92. doi: 10.3399/bjgp15x686497
2. Mbakwa CA, Scheres L, Penders J, Mommers M, Thijs C, Arts ICW. Early life antibiotic exposure and weight development in children. J Pediatr. (2016) 176:105–13.e2. doi: 10.1016/j.jpeds.2016.06.015
3. Kourlaba G, Kourkouni E, Spyridis N, Gerber JS, Kopsidas J, Mougkou K, et al. Antibiotic prescribing and expenditures in outpatient paediatrics in Greece, 2010–13. J Antimicrob Chemother. (2015) 70(8):2405–8. doi: 10.1093/jac/dkv091
4. Schrier L, Hadjipanayis A, del Torso S, Stiris T, Emonts M, Dornbusch HJ. European Antibiotic awareness day 2017: training the next generation of health care professionals in antibiotic stewardship. Eur J Pediatr. (2018) 177(2):279–83. doi: 10.1007/s00431-017-3055-0
5. Albayrak A, Karakaş NM, Karahalil B. Evaluation of parental knowledge, attitudes and practices regarding antibiotic use in acute upper respiratory tract infections in children under 18 years of age: a cross-sectional study in Turkey. BMC Pediatr. (2021) 21(1):554. doi: 10.1186/s12887-021-03020-4
6. Mangione-Smith R, Zhou C, Robinson JD, Taylor JA, Elliott MN, Heritage J. Communication practices and antibiotic use for acute respiratory tract infections in children. Ann Fam Med. (2015) 13(3):221–7. doi: 10.1370/afm.1785
7. Stivers T. Managing patient pressure to prescribe antibiotics in the clinic. Paediatr Drugs. (2021) 23(5):437–43. doi: 10.1007/s40272-021-00466-y
8. Cabral C, Ingram J, Lucas PJ, Redmond NM, Kai J, Hay AD, et al. Influence of clinical communication on Parents’ antibiotic expectations for children with respiratory tract infections. Ann Fam Med. (2016) 14(2):141–7. doi: 10.1370/afm.1892
9. Mammari N, Albert Q, Devocelle M, Kenda M, Kočevar Glavač N, Sollner Dolenc M, et al. Natural products for the prevention and treatment of common cold and viral respiratory infections. Pharmaceuticals. (2023) 16(5):662. doi: 10.3390/ph16050662
10. Ciprandi G, Tosca MA. Non-pharmacological remedies for post-viral acute cough. Monaldi Arch Chest Dis. (2021) 92(1). doi: 10.4081/monaldi.2021.1821
11. Adeleye OA, Bamiro OA, Bakre LG, Odeleye FO, Adebowale MN, Okunye OL, et al. Medicinal plants with potential inhibitory bioactive compounds against coronaviruses. Adv Pharm Bull. (2022) 12(1):7–16. doi: 10.34172/apb.2022.003
12. Seifert G, Brandes-Schramm J, Zimmermann A, Lehmacher W, Kamin W. Faster recovery and reduced paracetamol use—a meta-analysis of eps 7630 in children with acute respiratory tract infections. BMC Pediatr. (2019) 19(1):119. doi: 10.1186/s12887-019-1473-z
13. Seifert G, Funk P, Reineke T, Lehmacher W. Influence of eps 7630 on antipyretic comedication and recovery from acute tonsillopharyngitis in children: a meta-analysis of randomized, placebo-controlled, clinical trials. J Pediatr Infect Dis. (2021) 16:122–8. doi: 10.1055/s-0040-1722205
14. Matthys H, Heger M. Treatment of acute bronchitis with a liquid herbal drug preparation from Pelargonium Sidoides (eps 7630): a randomised, double-blind, placebo-controlled, multicentre study. Curr Med Res Opin. (2007) 23(2):323–31. 10.1185/030079906×16731817288687
15. Kardos P, Bittner CB, Seibel J, Abramov-Sommariva D, Birring SS. Effectiveness and tolerability of the thyme/ivy herbal fluid extract bno 1200 for the treatment of acute cough: an observational pharmacy-based study. Curr Med Res Opin. (2021) 37(10):1837–44. doi: 10.1080/03007995.2021.1960493
16. Mousa HA-L. Prevention and treatment of influenza, influenza-like illness, and common cold by herbal, complementary, and natural therapies. J Evid Based Complementary Altern Med. (2017) 22(1):166–74. doi: 10.1177/2156587216641831
17. Firenzuoli F, Gori L, Neri D. Clinical phytotherapy: opportunities and problematics. Ann Ist Super Sanita. (2005) 41(1):27–33.16037646
18. Choi SH. Who traditional medicine strategy and activities. “standardization with evidence-based approaches”. J Acupunct Meridian Stud. (2008) 1(2):153–4. doi: 10.1016/s2005-2901(09)60037-6
19. World Health Organization (WHO). Who Global Report on Traditional and Complimentary Medicine. Geneva: World Health Organization (WHO) (2019). Available at: https://iris.who.int/bitstream/handle/10665/312342/9789241515436-eng.pdf?sequence=1 (Accessed February 2024)
20. World Health Organization (WHO). Annex 5—Cumulative Index of Major Chemical Constituents. Monographs on Selected Medicinal Plants. Geneva: World Health Organization (WHO) (2009) 4. p. 406.
21. Dias DA, Urban S, Roessner U. A historical overview of natural products in drug discovery. Metabolites. (2012) 2(2):303–36. doi: 10.3390/metabo2020303
22. Jütte R, Heinrich M, Helmstädter A, Langhorst J, Meng G, Niebling W, et al. Herbal medicinal products—evidence and tradition from a historical perspective. J Ethnopharmacol. (2017) 207:220–5. doi: 10.1016/j.jep.2017.06.047
23. Graham-Brown RAC, Healsmith MF. From folklore to pharmacy: putting plants into practice. Clin Dermatol. (2018) 36(3):282–8. doi: 10.1016/j.clindermatol.2018.03.002
24. Martin D, Konrad M, Adarkwah CC, Kostev K. Reduced antibiotic use after initial treatment of acute respiratory infections with phytopharmaceuticals- a retrospective cohort study. Postgrad Med. (2020) 132(5):412–8. doi: 10.1080/00325481.2020.1751497
25. Soilemezi D, Leydon GM, Yan R, Simpson C, Bell M, Bostock J, et al. Herbal medicine for acute bronchitis: a qualitative interview study of Patients’ and health Professionals’ views. Complement Ther Med. (2020) 55:102613. doi: 10.1016/j.ctim.2020.102613
26. Meyer S, Gortner L, Larsen A, Kutschke G, Gottschling S, Graber S, et al. Complementary and alternative medicine in paediatrics: a systematic overview/synthesis of cochrane collaboration reviews. Swiss Med Wkly. (2013) 143:w13794. doi: 10.4414/smw.2013.13794
27. Carr RR, Nahata MC. Complementary and alternative medicine for upper-respiratory-tract infection in children. Am J Health Syst Pharm. (2006) 63(1):33–9. doi: 10.2146/ajhp040613
28. Holzinger F, Chenot JF. Systematic review of clinical trials assessing the effectiveness of ivy leaf (Hedera Helix) for acute upper respiratory tract infections. Evid Based Complement Alternat Med. (2011) 2011:382789. doi: 10.1155/2011/382789
29. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the prisma statement. PLoS Med. (2009) 6(7):e1000097. doi: 10.1371/journal.pmed.1000097
30. Howick J, Chalmers I, Glasziou P, Greenhalgh T, Heneghan C, Liberati A, et al. Explanation of the 2011 Oxford Centre for Evidence-Based Medicine (Ocebm) Levels of Evidence (Background Document). Oxford: Centre for Evidence-Based Medicine (2011). Available at: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/explanation-of-the-2011-ocebm-levels-of-evidence (Accessed August 2022)
31. Anheyer D, Cramer H, Lauche R, Saha FJ, Dobos G. Herbal medicine in children with respiratory tract infection: systematic review and meta-analysis. Acad Pediatr. (2018) 18(1):8–19. doi: 10.1016/j.acap.2017.06.006
32. Guo R, Canter PH, Ernst E. Herbal medicines for the treatment of rhinosinusitis: a systematic review. Otolaryngol Head Neck Surg. (2006) 135(4):496–506. doi: 10.1016/j.otohns.2006.06.1254
33. Kamin W, Lehmacher W, Zimmermann A, Brandes-Schramm J, Funk P, Seifert GJ, et al. Treatment of sore throat and hoarseness with Pelargonium Sidoides extract eps 7630: a meta analysis. Pharmadv. (2022) 4(2):88–103. doi: 10.36118/pharmadvances.2022.33
34. Yao J, Zhang Y, Wang XZ, Zhao J, Yang ZJ, Lin YP, et al. Flavonoids for treating viral acute respiratory tract infections: a systematic review and meta-analysis of 30 randomized controlled trials. Front Public Health. (2022) 10:814669. doi: 10.3389/fpubh.2022.814669
35. Bereznoy VV, Riley DS, Wassmer G, Heger M. Efficacy of extract of Pelargonium Sidoides in children with acute non-group a Beta-hemolytic Streptococcus tonsillopharyngitis: a randomized, double-blind, placebo-controlled trial. Altern Ther Health Med. (2003) 9(5):68–79.14526713
36. Taylor JA, Weber W, Standish L, Quinn H, Goesling J, McGann M, et al. Efficacy and safety of Echinacea in treating upper respiratory tract infections in children: a randomized controlled trial. JAMA. (2003) 290(21):2824–30. doi: 10.1001/jama.290.21.2824
37. Schapowal A, Berger D, Klein P, Suter A. Echinacea/sage or chlorhexidine/lidocaine for treating acute sore throats: a randomized double-blind trial. Eur J Med Res. (2009) 14(9):406–12. doi: 10.1186/2047-783x-14-9-406
38. Paul IM, Beiler JS, King TS, Clapp ER, Vallati J, Berlin CM Jr. Vapor rub, petrolatum, and no treatment for children with nocturnal cough and cold symptoms. Pediatrics. (2010) 126(6):1092–9. doi: 10.1542/peds.2010-1601
39. Timen G, Zabolotnyi D, Heger M, Lehmacher W. Eps 7630 is effective in children with acure, non-Β-haemolytic streptococcal tonsillopharyngitis results of a double-blind, placebo-controlled, multicentre trial. Malay J Pediatr Child Health. (2015) 21:36–50.
40. Bereznoy VV, Heger M, Lehmacher W, Seifert G. Clinical efficacy and safety of liquid Pelargonium Sidoides preparation (eps 7630) in children with acute non-streptococcal tonsillopharyngitis. J Compr Pediatr. (2016) 7(4). doi: 10.17795/compreped-42158
41. Cohen HA, Varsano I, Kahan E, Sarrell EM, Uziel Y. Effectiveness of an herbal preparation containing Echinacea, propolis, and vitamin C in preventing respiratory tract infections in children: a randomized, double-blind, placebo-controlled, multicenter study. Arch Pediatr Adolesc Med. (2004) 158(3):217–21. doi: 10.1001/archpedi.158.3.217
42. Spasov AA, Ostrovskij OV, Chernikov MV, Wikman G. Comparative controlled study of Andrographis Paniculata fixed combination, kan jang and an Echinacea preparation as adjuvant, in the treatment of uncomplicated respiratory disease in children. Phytother Res. (2004) 18(1):47–53. doi: 10.1002/ptr.1359
43. Khan MF, Akram M, Akhter N, Mukhtiar M, Zahid R, Khan FS, et al. The evaluation of efficacy and safety of cough (ema) granules used for upper respiratory disorders. Pak J Pharm Sci. (2018) 31(6):2617–22.30587469
44. Sen'kevich OA, Sidorenko SV, Ditrikh OA. Comparative efficacy of various treatment regimens for children 2–5 years old with symptoms of acute viral rhinosinusitis. Vestn Otorinolaringol. (2021) 86(1):46–50. doi: 10.17116/otorino20218601146
45. Popovych VI, Beketova HV, Koshel IV, Tsodikova OA, Kriuchko TA, Abaturov AE, et al. An open-label, multicentre, randomized comparative study of efficacy, safety and tolerability of the 5 plant—extract bno 1012 in the delayed antibiotic prescription method in children, aged 6 to 11 years with acute viral and post-viral rhinosinusitis. Am J Otolaryngol. (2020) 41(5):102564. doi: 10.1016/j.amjoto.2020.102564
46. Popovych V, Koshel I, Malofiichuk A, Pyletska L, Semeniuk A, Filippova O, et al. A randomized, open-label, multicenter, comparative study of therapeutic efficacy, safety and tolerability of bno 1030 extract, containing marshmallow root, chamomile flowers, horsetail herb, walnut leaves, yarrow herb, oak bark, dandelion herb in the treatment of acute non-bacterial tonsillitis in children aged 6 to 18years. Am J Otolaryngol. (2019) 40(2):265–73. doi: 10.1016/j.amjoto.2018.10.012
47. Popovych VI, Beketova HV. Results of a randomised controlled study on the efficacy of a combination of saline irrigation and sinupret syrup phytopreparation in the treatment of acute viral rhinosinusitis in children aged 6 to 11 years. Clinic Phytosci. (2018) 4(1):21. doi: 10.1186/s40816-018-0082-y
48. Blochin B, Heger M. Umckaloabo Versus Symptomatische Therapie in Der Behandlung Der Akuen Angina Catarrhalis. Germany: OmniMed-Verlag-Ges (2000).
49. Schapowal A, Heger M. Eps® 7630 solution (Umckaloabo®) in the treatment of sinusitis. Zeitschrift für Phytotherapie. (2007) 28(2):58–65. doi: 10.1055/s-2007-981621
50. Bereznoy V, Heger M, Iljenko L, Tischko F. Eps® 7630 bei erwachsenen und kindern mit angina tonsillaris. Zeitschrift für Phytotherapie. (2009) 30(1):6–13. doi: 10.1055/s-0029-1213421
51. Stauss-Grabo M, Atiye S, Warnke A, Wedemeyer RS, Donath F, Blume HH. Observational study on the tolerability and safety of film-coated tablets containing ivy extract (prospan® cough tablets) in the treatment of colds accompanied by coughing. Phytomedicine. (2011) 18(6):433–6. doi: 10.1016/j.phymed.2010.11.009
52. Karpova EP, Tulupov DA, Emel'yanova MP. Use of myrtol standardized in the treatment of children with acute rhinosinusitis. Vestn Otorinolaringol. (2016) 81(1):47–50. doi: 10.17116/otorino201681147-50
53. Khan M, Rehman H, Naveed S, Zaidi SF, Ayaz S, Owais A, et al. Chewable cough tablets with improved palatability: a comparative phase ii clinical trial. Pak J Pharm Sci. (2019) 32(1(Supplementary)):339–43.30829213
54. Kardos P, Lehmacher W, Zimmermann A, Brandes-Schramm J, Funk P, Matthys H, et al. Effects of Pelargonium Sidoides extract eps 7630 on acute cough and quality of life—a meta-analysis of randomized, placebo-controlled trials. Multidiscip Respir Med. (2022) 17:868. doi: 10.4081/mrm.2022.868
55. Matthys M, Lehmacher W, Zimmermann A, Brandes J, Kamin W. EPs 7630 in acute respiratory tract infections—a systematic review and meta-analysis of randomized clinical trials. J Lung Pulmonary Respir Res. (2016) 3(1):4–15. doi: 10.15406/jlprr.2016.03.00068
56. Cwientzek U, Ottillinger B, Arenberger P. Acute bronchitis therapy with ivy leaves extracts in a two-arm study. A double-blind, randomised study vs. an other ivy leaves extract. Phytomed. (2011) 18(13):1105–9. doi: 10.1016/j.phymed.2011.06.014
57. Timmer A, Gunther J, Motschall E, Rucker G, Antes G, Kern WV. Pelargonium sidoides extract for treating acute respiratory tract infections. Cochrane Database Syst Rev. (2013) 10:Cd006323. doi: 10.1002/14651858.CD006323.pub3
58. Kamin W, Ilyenko LI, Malek FA, Kieser M. Treatment of acute bronchitis with eps 7630: randomized, controlled trial in children and adolescents. Pediatr Int. (2012) 54(2):219–26. doi: 10.1111/j.1442-200X.2012.03598.x
59. Kamin W, Maydannik V, Malek F, Kieser M. Efficacy and tolerability of eps 7630 in patients (aged 6–18 years old) with acute bronchitis. Acta Paediatr. (2010a) 99(4):537–43. doi: 10.1111/j.1651-2227.2009.01656.x
60. Kamin W, Maydannik V, Malek FA, Kieser M. Efficacy and tolerability of eps 7630 in children and adolescents with acute bronchitis—a randomized, double-blind, placebo-controlled multicenter trial with a herbal drug preparation from Pelargonium Sidoides roots. Int J Clin Pharmacol Ther. (2010b) 48(3):184–91. doi: 10.5414/cpp48184
61. Kamin W, Behre U, Helm K, Reling B, Funk P, Malek FA. Safety of Pelargonium extract eps 7630 in young children with acute bronchitis. Front Pediatr. (2023) 11. doi: 10.3389/fped.2023.1107984
62. Ali Z, Daniyal M, Adhia MK, Alam A, Sarfaraz B, Sattar A, et al. To evaluate the efficacy and safety of cofnovex plus (ema) syrup. Pak J Pharm Sci. (2017) 30(2(Suppl.)):591–6.28650326
63. Kruttschnitt E, Wegener T, Zahner C, Henzen-Bücking S. Assessment of the efficacy and safety of ivy leaf (Hedera Helix) cough syrup compared with acetylcysteine in adults and children with acute bronchitis. Evid Based Complement Alternat Med. (2020) 2020:1910656. doi: 10.1155/2020/1910656
64. Ludwig S, Stier H, Weykam S. Evaluation of blood alcohol concentrations after oral administration of a fixed combination of thyme herb and primrose root fluid extract to children with acute bronchitis. Drug Res (Stuttg). (2016) 66(2):69–73. doi: 10.1055/s-0034-1398543
65. Marzian O. Treatment of acute bronchitis in children and adolescents. Non-interventional postmarketing surveillance study confirms the benefit and safety of a syrup made of extracts from thyme and ivy leaves. MMW Fortschr Med. (2007) 149(27–28 Suppl):69–74.17619603
66. Safina AI. Treatment of young children with recurrent acute respiratory tract infections with a herbal combination of thyme herb and ivy leaf. Zeitschrift für Phytotherapie. (2015) 35:262–7. doi: 10.1055/s-0034-1395797
67. Lang C, Staiger C, Wegener T. Ivy in everyday paediatric use: administration of ea 575® to schoolchildren for the treatment of acute bronchitis. Zeitschrift für Phytotherapie. (2015) 36(5):192–96. doi: 10.1055/s-0041-105237
68. Olszanecka-Glinianowicz M, Doniec Z, Schönknecht K, Almgren-Rachtan A. The herbal medicine containing of ivy leaf dry extract in the treatment of productive cough in children. Wiad Lek. (2020) 73(4):668–73.32731694
69. Schmidt M, Thomsen M, Schmidt U. Suitability of ivy extract for the treatment of paediatric cough. Phytother Res. (2012) 26(12):1942–7. doi: 10.1002/ptr.4671
70. Haidvogl M, Heger M. Treatment effect and safety of eps 7630-solution in acute bronchitis in childhood: report of a multicentre observational study. Phytomedicine. (2007) 14(Suppl 6):60–4. doi: 10.1016/j.phymed.2006.11.014
71. Fazio S, Pouso J, Dolinsky D, Fernandez A, Hernandez M, Clavier G, et al. Tolerance, safety and efficacy of Hedera helix extract in inflammatory bronchial diseases under clinical practice conditions: a prospective, open, multicentre postmarketing study in 9657 patients. Phytomedicine. (2009) 16(1):17–24. doi: 10.1016/j.phymed.2006.05.003
72. Schönknecht K, Fal A, Mastalerz-Migas A, Joachimiak M, Doniec Z. Efficacy of dry extract of ivy leaves in the treatment of productive cough. Wiad Lek. (2017) 70:1026–33.
73. Matthys H, Kamin W, Funk P, Heger M. Pelargonium Sidoides preparation (eps 7630) in the treatment of acute bronchitis in adults and children. Phytomedicine. (2007) 14(Suppl 6):69–73. doi: 10.1016/j.phymed.2006.11.015
74. Patiroglu T, Tunc A, Eke Gungor H, Unal E. The efficacy of Pelargonium Sidoides in the treatment of upper respiratory tract infections in children with transient hypogammaglobulinemia of infancy. Phytomedicine. (2012) 19(11):958–61. doi: 10.1016/j.phymed.2012.06.004
75. Braun L, Cohen M. Herbs and Natural Supplements: An Evidence-Based Guide Herbs and Natural Supplements: An Evidence-Based Guide. 4th ed Chatswood, NSW: Elsevier (2015).
76. Schapowal A, Klein P, Johnston SL. Echinacea reduces the risk of recurrent respiratory tract infections and complications: a meta-analysis of randomized controlled trials. Adv Ther. (2015) 32(3):187–200. doi: 10.1007/s12325-015-0194-4
77. Lutsenko Y, Bylka W, Matławska I, Darmohray R. Hedera helix as a medicinal plant. Herba Pol. (2010) 56(1):83–96.
78. Matthys H, Malek FA, Kamin W. Eps® 7630 in acute respiratory tract infections—a systematic review and meta-analysis of randomised clinical research. Forsch Komplentaermed. (2014) 21:57–8. doi: 10.15406/jlprr.2015.03.00068
79. Emanuel J, Papies J, Galander C, Adler JM, Heinemann N, Eschke K, et al. In vitro and in vivo effects of Pelargonium Sidoides dc. Root extract eps(®) 7630 and selected constituents against sars-cov-2 B.1, Delta ay.4/ay.117 and omicron ba.2. Front Pharmacol. (2023) 14:1214351. doi: 10.3389/fphar.2023.1214351
80. Papies J, Emanuel J, Heinemann N, Kulić Ž, Schroeder S, Tenner B, et al. Antiviral and immunomodulatory effects of Pelargonium Sidoides dc. Root extract eps® 7630 in sars-cov-2-infected human lung cells. Front Pharmacol. (2021) 12:757666. doi: 10.3389/fphar.2021.757666
81. Roth M, Fang L, Stolz D, Tamm M. Pelargonium Sidoides radix extract eps 7630 reduces rhinovirus infection through modulation of viral binding proteins on human bronchial epithelial cells. PLoS One. (2019) 14(2):e0210702. doi: 10.1371/journal.pone.0210702
82. Theisen LL, Muller CP. Eps® 7630 (umckaloabo®), an extract from Pelargonium Sidoides roots, exerts anti-influenza virus activity in vitro and in vivo. Antiviral Res. (2012) 94(2):147–56. doi: 10.1016/j.antiviral.2012.03.006
83. Michaelis M, Doerr HW, Cinatl J Jr. Investigation of the influence of eps® 7630, a herbal drug preparation from Pelargonium Sidoides, on replication of a broad panel of respiratory viruses. Phytomedicine. (2011) 18(5):384–6. doi: 10.1016/j.phymed.2010.09.008
84. Horváth G, Ács K. Essential oils in the treatment of respiratory tract diseases highlighting their role in bacterial infections and their anti-inflammatory action: a review. Flavour Fragr J. (2015) 30(5):331–41. doi: 10.1002/ffj.3252
Keywords: children, antibiotic resistance, phytomedicine, phytotherapy, complementary therapies, herbal medicine, acute respiratory tract infections
Citation: Kamin W, Seifert G, Zwiauer K, Bonhoeffer J, De Ketelaere V, D'Avino A, Štádler J, Bustamante-Ogando JC and Kara A (2025) Phytotherapy for acute respiratory tract infections in children: a systematically conducted, comprehensive review. Front. Pediatr. 13:1423250. doi: 10.3389/fped.2025.1423250
Received: 25 April 2024; Accepted: 9 April 2025;
Published: 1 May 2025.
Edited by:
Andrew S. Day, University of Otago, New ZealandReviewed by:
Rehab Ahmed, University of Tabuk, Saudi ArabiaKerry Bone, Integria Healthcare, Australia
Copyright: © 2025 Kamin, Seifert, Zwiauer, Bonhoeffer, De Ketelaere, D'Avino, Štádler, Bustamante-Ogando and Kara. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wolfgang Kamin, d29sZmdhbmcua2FtaW5AdmFsZW8ta2xpbmlrZW4uZGU=