 Naveen Bajaj1,†R. Kishore Kumar2,3,†
Naveen Bajaj1,†R. Kishore Kumar2,3,† Arun Inamadar4,†Alok Bhandari5,†Rajesh Kumar6,†Kheya Ghosh Uttam7,†Jaikrishan Mittal8,†
Arun Inamadar4,†Alok Bhandari5,†Rajesh Kumar6,†Kheya Ghosh Uttam7,†Jaikrishan Mittal8,† Pradeep Suryawanshi9,†
Pradeep Suryawanshi9,† Sanjay Wazir10,†Satyen Hemrajani11,†
Sanjay Wazir10,†Satyen Hemrajani11,† Priti Thakor12*†
Priti Thakor12*†
- 1Sapling Hospital, Ludhiana, India
- 2Cloudnine Group of Hospitals, Jayanagar, Bengaluru, India
- 3Department of Neonatology, Notre Dame University, Perth, WA, Australia
- 4Department of Dermatology, Venereology & Leprosy, Sri B. M. Patil Medical College, Hospital & Research Center, BLDE University, Karnataka, India
- 5Kukreja Hospital, New Delhi, India
- 6Rani Hospital and Rani Children Hospital, Jharkhand, India
- 7Pediatric Medicine Department, ICH, Kolkata, India
- 8Neoclinic, Jaipur, India
- 9Department of Neonatology, BVU Medical College, Pune, India
- 10Motherhood Hospitals, Gurgaon, India
- 11Mahatma Gandhi Medical College and Hospital, Jaipur, India
- 12Department of Medical Affairs, JNTL Consumer Health (India) Pvt. Ltd., Mumbai, Maharashtra, India
Introduction: Infants in a neonatal intensive care unit (NICU) face a significant risk of skin barrier damage due to various factors related to their condition and the medical interventions they receive. The Neonatology Chapter of the Indian Academy of Pediatrics aimed to develop a comprehensive guidance document on evidence-based clinical practices for neonatal skin care in hospitalized infants, focusing on scientific principles and empirical evidence.
Method: The modified Delphi method, involving a panel of 10 experts including neonatologists and pediatricians, was utilized to reach a consensus on clinical statements.
Results: Out of 132 clinical statements formulated, 127 achieved consensus, while 5 did not. The experts advised implementing screening tools and risk assessment frameworks for skin injuries as part of the NICU's quality of care assessment. They emphasized the need for gentle cleansing of newborns to prevent skin or eye irritation and reduce the risk of skin infections. When determining the mode and method of skin cleansing in neonates, factors such as weight, gestational age (GA), and the severity of illness should be taken into account. Emollients may effectively prevent transepidermal water loss (TEWL) and be well-tolerated by NICU infants. Considering topical emollient therapy may significantly reduce mortality and hospital-acquired infections and improve weight gain. Multisensory stimulation in preterm infants has the potential to enhance feeding, psychomotor development, and visual function. Providing parents with a booklet that includes skincare regimens for cleansing the baby and protecting the skin barrier is essential for home care of their baby.
Conclusion: This consensus aims to fill this void by offering clinical recommendations for the care of neonatal skin in hospitalized infants.
Introduction
The skin, being the largest organ of the body, plays a crucial role in helping newborns adapt to life outside the womb (1). While structurally similar to adult skin, newborn skin differs in several key ways. It has a higher surface area to weight ratio (700 cm2/kg compared to 250 cm2/kg in adults), a weaker connection between the dermis and epidermis, thinner and less elastic properties, higher permeability in the stratum corneum, an underdeveloped epidermal barrier, reduced melanin production, and sweat glands that are dense but less active (2). Additionally, the skin of newborns and young infants tends to have a higher pH and lower free fatty acid content compared to adult skin (3). These distinctions render a newborn's skin more prone to injury and infection, necessitating specialized care. It is crucial to communicate certain principles of skin care to the mother or caregiver (2). Although prematurity is the primary reason for babies being admitted to a NICU, 42% of admissions involve term babies with certain complications (2).
Aside from the unique anatomy and physiology of immature skin, infants in NICUs face heightened risks of skin injuries due to the frequent need for procedures and essential invasive devices for their survival. Standard invasive procedures like venous or arterial punctures and the application or removal of adhesives can lead to skin rupture. Therefore, it is essential to implement evidence-based skin care practices and use appropriate products to enhance neonatal outcomes (3). These factors underscore the importance of providing meticulous care for neonatal skin and implementing appropriate measures for antisepsis. A recent study highlighted significant variation in bathing, asepsis, and skin care practices in Indian NICUs. The study found that 65% of NICUs did not use any scales or tools for skin assessment. Additionally, 90% of NICUs used sponging for hygiene, despite evidence favouring immersion/swaddle bathing. Only 14% of NICUs used wipes, while 50% expressed interest in using them, as studies suggest that wipes may aid in infection control and barrier repair. These discrepancies underscore the need for evidence-based guidelines for skincare and the use of antisepsis measures in Indian NICUs (4).
Studies indicate that the NICU environment can lead to abnormal sensory stimulation, with certain systems such as visual and auditory being overstimulated, while others like tactile and vestibular are under stimulated, which could disrupt brain development, particularly during the first year of life when critical periods for sensory system maturation occur. This sensory imbalance can significantly impact hospitalized neonates (5). Recognizing the existing need, the goal of organizing this expert group meeting was to establish evidence-based recommendations for practices and protocols in NICUs.
Methods
Process overview
A panel of 10 experts (neonatologists and pediatricians) participated in a Delphi process to identify consensus on about 10 domains. Importance of skincare in NICUs, neonatal skin assessment, skin hygiene in NICU babies, umbilical cord care, perineal care, TEWL and thermoregulation in NICUs: role of skin care in fluid and electrolyte balance, iatrogenic injuries, management of pressure injuries/wounds, neurodevelopmental care/developmental supportive care in NICUs and skin care regimen and parent education at discharge. Consensus was developed using the 3-step Delphi method, which took place between October 2022 and December 2022.
Initially, a thorough list of statements was formulated and distributed to an expert panel through an online platform for voting. Subsequently, a virtual meeting was conducted with the expert panel to discuss statements where consensus was not reached or which required further discussion. This allowed panel members to provide additional clarification on certain issues and present arguments to support their perspectives. Following this discussion, a second round of voting was conducted for the revised statements.
Data extraction and statement development
Relevant information was extracted from a literature review and full-text publications focusing on best practices for assessing, caring for, treating, and providing skin care advice for hospitalized neonates, as well as best practices in neurodevelopmental care. This extracted information served as the basis for developing consensus statements. Members of the expert group reviewed these statements and convened as a group to discuss them (see Table 1). Panelists’ anonymity was preserved throughout the process, with all comments being incorporated anonymously into the statements and questionnaires distributed to panelists in each round.
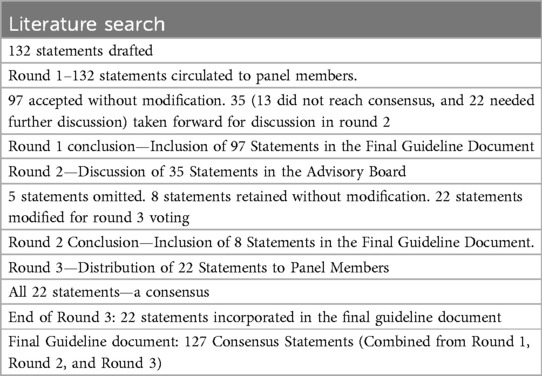
Table 1. Delphi methodology and results.
Round 1
The initial draft document, comprising 132 statements, was distributed via email to all 10-panel members along with a detailed explanation of the study's objectives and specific instructions for participation. Each expert was requested to vote by indicating their level of agreement with each statement as “strongly agree,” “agree,” “neutral,” or “disagree.” Experts were also encouraged to provide comments and suggest additional items that may have been overlooked during the initial statement development. In round 1, the aim was to record the panel's agreement or disagreement with each statement and address any redundancies or issues related to the clarity or syntax of the statements. Response frequencies for each statement were calculated and entered anonymously into a database by a research assistant. Thirteen statements did not achieve 100% agreement, and 22 statements achieved agreement but required further discussion, which took place during a face-to-face meeting of the expert panel in round 2.
Round 2
During round 1, a total of 35 statements were identified, with 13 statements failing to achieve 100% agreement and 22 statements reaching agreement but requiring further discussion. All 10 members participated in a virtual face-to-face meeting to discuss these statements. Panel members were encouraged to discuss the remaining statements until a consensus was reached on whether to retain, modify, or eliminate them from the final guideline document. Consequently, five statements were removed, 22 were modified, and 8 were included based on the discussions. The revised 22 statements were then circulated to panel members for voting in round 3.
Round 3
In Round 2, 22 statements were revised and distributed to all panel members via email. Each expert was requested to vote by indicating their level of agreement with each statement as “strongly agree,” “agree,” “neutral,” or “disagree.” All 22 statements reached 100% agreement, and the final consensus arrived at 127 statements, which centered around primarily 10 domains viz. importance of skincare in NICUs, neonatal skin assessment, skin hygiene in NICU babies, umbilical cord care, perineal care, TEWL and thermoregulation in NICUs: role of skin care in fluid and electrolyte balance, iatrogenic injuries, management of pressure injuries/wounds, neurodevelopmental care/developmental supportive care in NICUs and skin care regimen and parent education at discharge (Table 2).

Table 2. List of final consensus statements to which 100 % agreement was obtained.
Discussion
The fragile nature of newborn skin makes it prone to injury and infection, particularly in NICU neonates, necessitating specialized care to mitigate harm and promote optimal skin development (6). However, existing guidelines often overlook the unique challenges of NICU skin care, highlighting the need for evidence-based recommendations. This expert consensus on neonatal skin management in the NICU aims to align with evidence-based practices and enhance routine skin care. It also focuses on preventing and treating iatrogenic skin injuries in neonates, ultimately leading to improved patient outcomes.
Tools like the NSCS and SRAMT aid in skin assessment, with the latter being preferred for high-risk neonates (7). The experts have underscored the importance of preserving neonatal skin integrity and preventing skin injuries in the NICU. Strategies include using topical emollients to strengthen the skin barrier, thereby reducing the risk of invasive infections (8). Emollients such as sunflower seed oil, coconut oil, or mineral oil can help prevent TEWL and lower the risk of mortality and infections in NICU settings (9, 10).
Due to their thinner and less developed skin, neonates are highly vulnerable to medical adhesive-related skin injuries (MARSI), which can include mechanical issues and dermatitis reactions (11). Thus, cautious selection of less damaging adhesives, such as hydrogel, silicone-based, or hydrocolloid types, is crucial while avoiding leukoplast tapes and using fixation methods that minimize skin pressure and displacement of devices. Research suggests that newer formulations of silicone-based adhesives could be less disruptive to the skin barrier than acrylate adhesive tapes, and may also adhere to plastic, and could be used for tubing securement devices (7, 12).
Research suggests a possible connection between neonatal exposure to iodine-containing disinfectants and thyroid dysfunction in infants born before 32 weeks. This highlights the critical need for careful practices when using chlorhexidine in the NICU environment, also before any invasive interventions (13). Additionally, preventing pressure ulcers in neonates necessitates a comprehensive approach to skincare, incorporating hygiene, moisture control, and pressure management, with particular attention to nutritional support (14).
Emphasizing skin hygiene and meticulous care, including hand hygiene, can reduce infections and sepsis (15). On the other hand, maintaining proper skin care practices, including perineal care and the use of superabsorbent diapers and barrier creams, is crucial for promoting skin health (7). Maintaining the proper pH balance for the skin is crucial for both immediate skin health and long-term well-being. Newborn infection protection relies on staff and parent hygiene, as well as routine disinfection of catheter insertion sites and aseptic handling of central venous catheters.
Additionally, strategies to minimize IWL and prevent iatrogenic pressure injuries are crucial in the NICU setting. Careful assessment and management of neonatal skin injuries by health care physicians at each of the NICU visits, along with environmental factors like sensory stimulation and family-integrated care, are essential for optimal neurodevelopmental outcomes (16). Integrating these practices into routine care and providing education to parents can enhance the well-being of NICU infants and improve overall outcomes (58).
Babies from the NICU need strong skin barrier protection and skincare education for parents, including proper cleansing and emollient use, outlined in discharge materials. Cleansing approaches should focus on swaddle immersion bathing and avoid sponge bathing to reduce heat loss and stress, promote healthy skin flora, and involve parents in skincare routines (7).
There is a further need to develop an appropriate customized recommendations for stratified gestational age in neonates, while also considering complexities of the profiles under consideration. These would include benefits over both the short-term, and long-term (hydration, TEWL, skin pH, maternal satisfaction, skin colonization, erythema, etc.).
Following these expert consensuses and their clinical recommendations for neonatal skin care in hospitalized neonates may ultimately lead to improved patient outcomes. Adherence to these guidelines ensures comprehensive and effective management of neonatal skin conditions, promoting the well-being of newborns in hospital settings. Further research on the management of sensitive skin in the pediatric population is warranted.
Author contributions
NB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. RK: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. AI: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. AB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. RK: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. KU: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. JM: Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. PS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. SW: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. SH: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. PT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research is funded by JNTL Consumer Health (India) Pvt Ltd.
Acknowledgments
The authors thank Eien Biosciences, Mumbai, India, for the medical writing support.
Conflict of interest
PT is an employee of JNTL Consumer Health (India) Pvt Ltd. The advisory board was conducted by JNTL Consumer Health (India) Pvt Ltd.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that this study received funding from JNTL Consumer Health (India) Pvt Ltd. The funder had the following involvement in the study: study design, collection, analysis, interpretation of data, the writing of this article, and the decision to submit it for publication.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Correction note
A correction has been made to this article. Details can be found at: 10.3389/fped.2025.1667273.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kuller JM, Lund C, Nonato LB. Neonatal Integumentary System. Clinical Education Series. Ross Pediatrics. USA (2002).
2. Khasawneh W, Sindiani A, Rawabdeh SA, Aleshawi A, Kanaan D. Indications and clinical profile of neonatal admissions: a cross-sectional descriptive analysis from a single academic center in Jordan. J Multidiscip Healthc. (2020) 13:997–1006. doi: 10.2147/JMDH.S275267
3. Broom M, Dunk AM, Mohamed AL E. Predicting neonatal skin injury: the first step to reducing skin injuries in neonates. Health Serv Insights. (2019) 12:1178632919845630. doi: 10.1177/1178632919845630
4. Kusari A, Han AM, Virgen CA, Matiz C, Rasmussen M, Friedlander SF, et al. Evidence-based skin care in preterm infants. Pediatr Dermatol. (2019) 36(1):16–23. doi: 10.1111/pde.13725
5. Visscher M, Taylor T. Pressure ulcers in the hospitalized neonate: rates and risk factors. Sci Rep. (2014) 4:7429. doi: 10.1038/srep07429
6. Oranges T, Dini V, Romanelli M. Skin physiology of the neonate and infant: clinical implications. Adv Wound Care (New Rochelle). (2015) 4(10):587–95. doi: 10.1089/wound.2015.0642
7. Brandon D, Hill CM, Heimall L, Lund CH, Kuller J, McEwan T, et al. Neonatal Skin Care: Evidence-Based Clinical Practice Guideline. Washington, D.C.: Association of Women’s Health, Obstetric and Neonatal Nurses (2018).
8. Salam RA, Das JK, Darmstadt GL, Bhutta ZA. Emollient therapy for preterm newborn infants–evidence from the developing world. BMC Public Health. (2013) 13(Suppl 3):S31. doi: 10.1186/1471-2458-13-S3-S31
9. Cleminson J, McGuire W. Topical emollient for preventing infection in preterm infants. Cochrane Database Syst Rev (2016) 2016(1):CD001150. doi: 10.1002/14651858.CD001150.pub3
10. Kumar A, Mishra S, Singh S, Ashraf S, Kan P, Ghosh AK, et al. Effect of sunflower seed oil emollient therapy on newborn infant survival in Uttar Pradesh, India: a community-based, cluster randomized, open-label controlled trial. PLoS Med. (2021) 18(9):e1003680. doi: 10.1371/journal.pmed.1003680
11. Evidence-Based Medicine G, Neonatologist S, Chinese Medical Doctor A. Guidelines for neonatal skin management in the neonatal intensive care unit (2021). Zhongguo Dang Dai Er Ke Za Zhi. (2021) 23(7):659–70.34266521
12. Turnbull MJ, Grigsby I, Unertl K, Sokol K, Nordby T, Liu C, et al. Comparison of medical tape performance using skin response quantitative measurements on healthy volunteers. Cureus. (2024) 16(3):e56548. doi: 10.7759/cureus.56548
13. Aitken J, Williams FLR. A systematic review of thyroid dysfunction in preterm neonates exposed to topical iodine. Arch Dis Child Fetal Neonatal Ed. (2014) 99(1):F21–28. doi: 10.1136/archdischild-2013-303799
14. García-Molina P, Alfaro-López A, García-Rodríguez SM, Brotons-Payá C, Rodríguez-Dolz MC, Balaguer-López E. Neonatal pressure ulcers: prevention and treatment. RRN. (2017) 7:29–39. doi: 10.2147/RRN.S98755
15. Kuti BP, Ogunlesi TA, Oduwole O, Oringanje C, Udoh EE, Meremikwu MM. Hand hygiene for the prevention of infections in neonates. Cochrane Database Syst Rev. (2019) 2019(5):CD013326.
16. Hee Chung E, Chou J, Brown KA. Neurodevelopmental outcomes of preterm infants: a recent literature review. Transl Pediatr. (2020) 9(Suppl 1):S3–8. doi: 10.21037/tp.2019.09.10
18. Garegrat RA, Banait N, Pareek P, Gupta R, Suryawanshi P. National Survey of Routine Bathing and Antisepsis Practices in Neonatal Intensive Care Units of India. J Neonatol. (2021) 35(4):209–13. doi: 10.1177/09732179211051307
19. Kutlubay Z, Tanakol A, Engýn B, Onel C, Sýmsek E, Serdaroglu S, et al. Newborn Skin: Common Skin Problems. Maedica (Bucur). (2017) 12(1):42–7.28878836
20. CAHS. Child and Adolescent Health Service. Available at: https://cahs.health.wa.gov.au/ (Accessed December 12, 2023).
21. Lund CH, Osborne JW. Validity and reliability of the neonatal skin condition score. J Obstet Gynecol Neonatal Nurs. (2004) 33(3):320–7. doi: 10.1177/0884217504265174
22. Moore ZE, Patton D. Risk assessment tools for the prevention of pressure ulcers. Cochrane Database Syst Rev. (2019) 1(1):CD006471.30702158
23. Liao Y, Gao G, Mo L. Predictive accuracy of the Braden Q Scale in risk assessment for paediatric pressure ulcer: A meta-analysis. Int J Nurs Sci. (2018) 5(4):419–26.31406858
24. Puspitasari JD, Nurhaeni N, Waluyanti FT. Testing of Braden QD Scale for predicting pressure ulcer risk in the Pediatric Intensive Care Unit. Pediatr Rep. (2020) 12(Suppl 1):8694. doi: 10.4081/pr.2020.8694
25. Healthcare Improvement Scotland. Adapted Glamorgan Pressure Ulcer Risk Assessment Scale - Suitable for use from Birth-18yrs (2020). Available at: https://www.healthcareimprovementscotland.org/programmes/patient_safety/tissue_viability_resources/paediatric_glamorgan_tool.aspx (Accessed December 12, 2023).
26. Patro P, Kothari N, Jain P. Infection control protocol in NICU suitable for a peripheral newborn care unit. Journal of the Pediatrics Association of India. (2016) 5(2):81. doi: 10.4103/2667-3592.300887
27. Hennig TJ, Werner S, Naujox K, Arndt A. Chlorhexidine is not an essential component in alcohol-based surgical hand preparation: a comparative study of two handrubs based on a modified EN 12791 test protocol. Antimicrob Resist Infect Control. (2017) 6(96).28924473
28. Madhu R, Vijayabhaskar C, Anandan V, Nedunchelian K, Thangavelu S, Soans ST, et al. Indian Academy of Pediatrics Guidelines for Pediatric Skin Care. Indian Pediatr. (2021) 58(2):153–61. doi: 10.1007/s13312-021-2133-6
29. Visscher M, Odio M, Taylor T, White T, Sargent S, Sluder L, et al. Skin care in the NICU patient: effects of wipes versus cloth and water on stratum corneum integrity. Neonatology. (2009) 96(4):226–34. doi: 10.1159/000215593
30. Rodriguez KJ, Cunningham C, Foxenberg R, Hoffman D, Vongsa R. The science behind wet wipes for infant skin: Ingredient review, safety, and efficacy. Pediatr Dermatol. (2020) 37(3):447–54. doi: 10.1111/pde.14112
31. Nickel N, Brooks S, Mize C, Messina A. Reducing Staphylococcus aureus infections in the neonatal intensive care unit. J Perinatol. (2022) 42(11):1540–5. doi: 10.1038/s41372-022-01407-4
32. Ness MJ, Davis DMR, Carey WA. Neonatal skin care: a concise review. Int J Dermatol. (2013) 52(1):14–22. doi: 10.1111/j.1365-4632.2012.05687.x
33. Rogers S, Thomas M, Chan B, Hinckley SK, Henderson C. A Quality Improvement Approach to Perineal Skin Care: Using Standardized Guidelines and Novel Diaper Wipes to Reduce Diaper Dermatitis in NICU Infants. Adv Neonatal Care. (2021) 21(3):189–97. doi: 10.1097/ANC.0000000000000795
34. Gustin J, Bohman L, Ogle J, Fadayel G, Mitchell MC, Narendran V, et al. Improving newborn skin health: Effects of diaper care regimens on skin pH and erythema. Pediatr Dermatol. (2021) 38(4):768–74. doi: 10.1111/pde.14602
35. Simpson EL, Chalmers JR, Hanifin JM, Thomas KS, Cork MJ, McLean WHI, et al. Emollient enhancement of the skin barrier from birth offers effective atopic dermatitis prevention. J Allergy Clin Immunol. (2014) 134(4):818–23. doi: 10.1016/j.jaci.2014.08.005
36. Benitez Ojeda AB, Mendez MD. Diaper Dermatitis. In: StatPearls. Treasure Island, FL: StatPearls Publishing (2023). Available at: http://www.ncbi.nlm.nih.gov/books/NBK559067/ (Accessed December 13, 2023).
37. Kaushal M, Agarwal R, Aggarwal R, Singal A, Upadhyay M, Srinivas V, et al. Cling wrap, an innovative intervention for temperature maintenance and reduction of insensible water loss in very low-birthweight babies nursed under radiant warmers: a randomized, controlled trial. Ann Trop Paediatr. (2005) 25(2):111–8. doi: 10.1179/146532805X45700
38. Grünhagen DJ, de Boer MGJ, de Beaufort AJ, Walther FJ. Transepidermal water loss during halogen spotlight phototherapy in preterm infants. Pediatr Res. (2002) 51(3):402–5. doi: 10.1203/00006450-200203000-00022
39. Kuip DVD, Opperbeck A. Current Risk Factors for Iatrogenic Pressure Injuries in Neonates : A Literature Review. (2016). Available at: https://www.semanticscholar.org/paper/Current-Risk-Factors-for-Iatrogenic-Pressure-in-%3A-A-Kuip-Opperbeck/14ccac482b62edbd412cb773684a2bc50188e441 (Accessed December 13, 2023).
40. August D, Edmonds L, Brown D, Murphy M, Kandasamy Y. Pressure injuries to the skin in a neonatal unit: Fact or fiction. Journal of Neonatal Nursing. (2013) 20:129–137. doi: 10.1016/j.jnn.2013.08.006
41. Litchford MD, Dorner B, Posthauer ME. Malnutrition as a Precursor of Pressure Ulcers. Adv Wound Care (New Rochelle). (2014) 3(1):54–63. doi: 10.1089/wound.2012.0385
42. McNichol L, Mackey D, Watts C, Zuecca N. Choosing a support surface for pressure injury prevention and treatment. Nursing. (2020) 50(2):41–4. doi: 10.1097/01.NURSE.0000651620.87023.d5
43. National Clinical Guideline Centre (UK). The Prevention and Management of Pressure Ulcers in Primary and Secondary Care. London: National Institute for Health and Care Excellence (NICE) (2014). Available at: http://www.ncbi.nlm.nih.gov/books/NBK248068/ (Accessed December 13, 2023).
44. Lund C. Medical Adhesives in the NICU. Newborn and Infant Nursing Reviews. (2014) 14(4):160–5. doi: 10.1053/j.nainr.2014.10.001
45. Gopalakrishnan PN, Goel N, Banerjee S. Saline irrigation for the management of skin extravasation injury in neonates. Cochrane Database of Systematic Reviews. (2017) 2017(7). doi: 10.1002/14651858.CD008404.pub3
46. Aita M, De Clifford Faugère G, Lavallée A, Feeley N, Stremler R, Rioux É, et al. Effectiveness of interventions on early neurodevelopment of preterm infants: a systematic review and meta-analysis. BMC Pediatr. (2021) 21(1):210. doi: 10.1186/s12887-021-02559-6
47. Als H, McAnulty GB. The Newborn Individualized Developmental Care and Assessment Program (NIDCAP) with Kangaroo Mother Care (KMC): Comprehensive Care for Preterm Infants. Curr Womens Health Rev. (2011) 7(3):288–301. doi: 10.2174/157340411796355216
48. Embarek-Hernández M, Güeita-Rodríguez J, Molina-Rueda F. Multisensory stimulation to promote feeding and psychomotor development in preterm infants: A systematic review. Pediatr Neonatol. (2022) 63(5):452–61. doi: 10.1016/j.pedneo.2022.07.001
49. Chan GJ, Valsangkar B, Kajeepeta S, Boundy EO, Wall S. What is kangaroo mother care? Systematic review of the literature. J Glob Health. (2016) 6(1):010701. doi: 10.7189/jogh.06.010701
50. NICU Family & Visitor Resources. Children’s Hospital of Orange County. Available at: https://www.choc.org/programs-services/nicu/family-and-visitor-resources/ (Accessed December 13, 2023).
51. The Royal Children's Hospital Melbourne. Nursing guidelines: Skin to skin care for the newborn. Available at: https://www.rch.org.au/rchcpg/hospital_clinical_guideline_index/Skin_to_skin_care_for_the_newborn/ (Accessed December 13, 2023).
52. van Veenendaal NR, van Kempen AAMW, Broekman BFP, de Groof F, van Laerhoven H, van den Heuvel MEN, et al. Association of a Zero-Separation Neonatal Care Model With Stress in Mothers of Preterm Infants. JAMA Netw Open. (2022) 5(3):e224514. doi: 10.1001/jamanetworkopen.2022.4514
53. Practical Dermatology, Bryn Mawr Communications. Guiding Parents Through A Safe and Effective Pediatric Skincare Routine. Available at: https://practicaldermatology.com/articles/2019-aug/guiding-parents-through-a-safe-and-effectivepediatric-skincare-routine (Accessed December 13, 2023).
54. Jain A, Sekhar J, Kumari N, Jain N. Innovative need-based low-cost kangaroo mother care (KMC) chair. BMJ Innovations. (2020) 6:bmjinnov-2018. doi: 10.1136/bmjinnov-2018-000322
55. Altimier L, Phillips R. The Neonatal Integrative Developmental Care Model: Advanced Clinical Applications of the Seven Core Measures for Neuroprotective Family-centered Developmental Care. Newborn and Infant Nursing Reviews. (2016) 16(4):230–44. doi: 10.1053/j.nainr.2016.09.030
56. Gupta P, Nagesh K, Garg P, Thomas J, Suryawanshi P, Sethuraman G, et al. Evidence-Based Consensus Recommendations for Skin Care in Healthy, Full-Term Neonates in India. Pediatric Health Med Ther. (2023) 14:249–65. doi: 10.2147/PHMT.S414091
57. Pados BF, McGlothen-Bell K. Benefits of Infant Massage for Infants and Parents in the NICU. Nurs Womens Health. (2019) 23(3):265–71. doi: 10.1016/j.nwh.2019.03.004
58. Royal Children’s Hospital. Neonatal and infant skin care. (n.d.). Available at: https://www.rch.org.au/rchcpg/hospital_clinical_guideline_index/neonatal___infant_skin_care/ (retrieved October 15, 2023; viewed on 15th February 2025).
Keywords: intensive care units, neonatal, consensus, skin care, hospitals, emollients, parents
Citation: Bajaj N, Kumar RK, Inamadar A, Bhandari A, Kumar R, Uttam KG, Mittal J, Suryawanshi P, Wazir S, Hemrajani S and Thakor P (2025) Indian academy of pediatrics (neonatology chapter) recommendations for evidence-based neonatal skincare and protocols for hospitalized neonates. Front. Pediatr. 13:1433792. doi: 10.3389/fped.2025.1433792
Received: 16 May 2024; Accepted: 27 February 2025;
Published: 12 June 2025;
Corrected: 29 July 2025.
Edited by:
Andrew S. Day, University of Otago, New ZealandReviewed by:
Enrique Gomez-Pomar, University of Kentucky, United StatesCarolyn Lund, UCSF Benioff Children's Hospital Oakland, United States
Copyright: © 2025 Bajaj, Kumar, Inamadar, Bhandari, Kumar, Uttam, Mittal, Suryawanshi, Wazir, Hemrajani and Thakor. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Priti Thakor, ZG9jcHJpdEBnbWFpbC5jb20=
†These authors have contributed equally to this work and share first authorship