 Wen Liu1,†
Wen Liu1,† Ling Qin
Ling Qin- 1Department of Pediatric, The Third People’s Hospital of Chengdu, Chengdu, Sichuan, China
- 2Department of Ophthalmology, The Third People’s Hospital of Chengdu, Chengdu, Sichuan, China
- 3College of Nursing, Xinjiang Medical University, Urumqi, Xinjiang, China
Background: Vaccination effectively prevents various infectious diseases and represents one of the most cost-effective health interventions. In China, childhood immunization programs have achieved remarkable success, but guardian knowledge, attitudes, and practices (KAP) regarding vaccination significantly influence immunization coverage. Understanding vaccination KAP among children's guardians in Chengdu is crucial for optimizing immunization programs.
Aim: To assess knowledge, attitudes, and practices regarding childhood vaccination among guardians in Chengdu's Third People's Hospital and identify associated factors to improve vaccination service quality.
Methods: A cross-sectional survey was conducted among 612 guardians of children aged 0–6 years between January and June 2023. Participants were recruited through systematic sampling during vaccination visits, telephone appointments, and household surveys. A structured questionnaire assessed vaccination knowledge (13 items), attitudes (11 items), and practices (9 items). Data were analyzed using χ2 tests and logistic regression analysis (P < 0.05).
Results: Among 612 participants (response rate 90.1%), 97.7% were aware that newborns require vaccination within 24 hours, but knowledge gaps existed regarding vaccine classifications (56.1% aware of Category I vaccines), adverse reactions (61.8%), and specific vaccines like meningococcal (47.1%) and hepatitis A (41.5%). Most guardians (85.1%) considered vaccination necessary, and 69.9% proactively sought vaccination services. However, only 23.4% were unaffected by negative media reports. Logistic regression revealed that higher education levels (OR = 1.51, 95%CI: 1.02–2.24), higher family income (OR = 1.80, 95%CI: 1.09–2.96), and better housing conditions (OR = 1.89, 95%CI: 1.03–3.45) were associated with better vaccination knowledge.
Conclusion: Guardians in Chengdu demonstrate positive attitudes toward vaccination but require improved knowledge, particularly regarding vaccine categories and safety. Targeted education programs should focus on vulnerable populations with lower education and income levels to enhance vaccination coverage and child health protection.
Introduction
Vaccination represents one of the most effective public health interventions for preventing infectious diseases and protecting child health (1, 2). Vaccines have contributed significantly to reducing childhood morbidity and mortality worldwide, making immunization programs essential components of comprehensive healthcare systems (3).
China has implemented extensive childhood immunization programs for decades, achieving substantial improvements in child health outcomes (4). Following the promulgation of regulations on vaccine circulation and vaccination administration, various regions have actively developed immunization programs according to local conditions (5). However, vaccination policy implementation varies significantly across different local governments (6). With rapid economic development, Chengdu has experienced dramatic increases in migrant populations, with many migrant children accompanying their working parents to urban areas, creating new challenges for routine immunization management (7).
In China's National Immunization Program, vaccines are classified into two categories: Category I vaccines are mandatory and provided free of charge by the government, while Category II vaccines are optional and require out-of-pocket payment (8). This classification system significantly influences parents' vaccination decisions and knowledge needs, particularly regarding the importance and safety of Category II vaccines (9).
Parents and guardians serve as primary decision-makers for children's vaccination, and their knowledge, attitudes, and practices directly affect vaccination uptake and immunization coverage rates (10, 11). Recent studies have demonstrated positive correlations between guardian vaccination knowledge levels and successful immunization program implementation (12, 13). Furthermore, educated guardians can serve as health educators within migrant communities through “peer education” mechanisms, extending vaccination knowledge to broader populations (14).
Guardian participation in vaccination decisions proves valuable for smooth immunization program implementation and reduction of vaccine-preventable diseases (15, 16). Research from various settings has shown that comprehensive knowledge-attitude-practice (KAP) assessments provide essential insights for developing targeted health education interventions and improving vaccination services (17, 18).
However, limited research has examined vaccination KAP among guardians in major Chinese cities like Chengdu, particularly considering the unique challenges posed by mixed local and migrant populations. This study was conducted to assess vaccination knowledge, attitudes, and practices among guardians of preschool children in Chengdu, providing evidence for developing improved immunization strategies, enhancing vaccination service quality, and better controlling vaccine-preventable diseases.
Participants and methods
Study design and participants
This cross-sectional study was conducted at the Third People's Hospital of Chengdu, Sichuan Province, between January and June 2023. A total of 679 guardians of children aged 0–6 years were initially screened, of whom 612 (90.1%) voluntarily agreed to participate and completed the questionnaire effectively.
Guardians were defined as individuals primarily responsible for children's daily care, including parents, maternal grandparents, paternal grandparents, or other caregivers. Inclusion criteria were: guardians seeking vaccination services at the study hospital; local residence duration exceeding three months. Exclusion criteria included: children with vaccination contraindications; institutionalized children; guardians with cognitive impairments. One guardian per household was surveyed to avoid clustering effects.
Data collection methods
Data collection employed three approaches with specific recruitment numbers:Systematic sampling during routine vaccination visits on randomly selected service days: 245 participants (40.0%).Scheduled interviews with guardians contacted via telephone appointments: 198 participants (32.4%).Community-based household surveys using random address selection: 169 participants (27.6%).
Vaccination days were randomly selected using a random number generator. Telephone contacts were systematically sampled from the hospital's immunization registry. Household surveys employed random street address selection within the hospital's catchment area.
Participants did not receive monetary compensation. On-site participants received priority service without queuing, while telephone and household survey participants received 20 yuan transportation subsidies.
Survey instrument
The structured questionnaire was developed following extensive literature review and expert consultation (19, 20). Content validity was assessed by 13 immunization experts, achieving a Content Validity Index (CVI) of 0.87. Face validity was evaluated through cognitive interviews with 30 guardians. A pilot study with 30 participants demonstrated good internal consistency (Cronbach's α = 0.82) (21).
The questionnaire comprised four main sections:
Demographic information
Gender, household registration, occupation, education level, monthly family income, housing situation, and vaccination notification receipt.
Vaccination knowledge assessment (13 items)
Covering vaccination requirements, contraindications, vaccine categories, adverse reactions, and specific vaccine awareness.
Vaccination attitudes (11 items)
assessing perceptions of vaccination necessity, willingness to receive optional vaccines, and trust in vaccination services.
Vaccination practices (9 items)
Evaluating actual vaccination behaviors, appointment compliance, and health information seeking. See Supplementary Material for the complete questionnaire.
Statistical analysis
Data were double-entered using EpiData 3.0 and analyzed with IBM SPSS 21.0 (22). Descriptive statistics included frequencies and percentages for categorical variables and means ± standard deviations for continuous variables. Knowledge scores were analyzed as continuous variables and categorized using quartile distributions for comparative analysis.
Chi-square tests examined associations between demographic characteristics and vaccination knowledge levels. Variables showing significant associations (P < 0.05) in univariate analysis were included in binary logistic regression models to identify independent predictors of vaccination knowledge. All statistical tests were two-tailed with significance set at P < 0.05.
Ethics approval
This study was conducted according to the Declaration of Helsinki and approved by the Ethics Committee of The Third People's Hospital of Chengdu (SC-CD-34) (23). All participants provided written informed consent before participation.
Results
Participant characteristics
A total of 679 questionnaires were distributed and 612 were completed, yielding a response rate of 90.1%. Among participants, 311 (50.8%) were male and 301 (49.2%) were female guardians. The sample included 89 (14.5%) fathers, 121 (19.8%) mothers, and 402 (65.7%) other relatives including grandparents.
Educational levels comprised: elementary school or below 144 (23.5%), junior high school 155 (25.3%), high school/technical secondary school 181 (29.6%), and college or above 132 (21.6%). A total of 389 (63.6%) participants held urban registration, while 223 (36.4%) were non-local residents.
Monthly per capita family income distribution included: <1,000 yuan 97 (15.9%), 1,000–3,000 yuan 158 (25.8%), 3,000–5,000 yuan 176 (28.8%), and ≥5,000 yuan 181 (29.6%).
Vaccination knowledge assessment
Guardians demonstrated highest awareness rates for newborn vaccination requirements within 24 hours (97.7%) and fever contraindications (94.1%). However, substantial knowledge gaps existed regarding Category II vaccination necessity (32.8%) and specific vaccination schedules (46.9%).
Among common childhood vaccines, guardians showed greater familiarity with hepatitis B vaccine (95.8%) and BCG vaccine (92.2%), while knowledge was limited for meningococcal vaccine (47.1%) and hepatitis A vaccine (41.5%). Regarding vaccine-preventable diseases, awareness was highest for polio (88.9%) and tuberculosis (85.3%), but lower for Japanese encephalitis (45.1%) and meningococcal disease (39.7%) (Table 1).

Table 1. Guardian knowledge of key vaccination topics (n = 612).
Factors associated with vaccination knowledge
Univariate analysis revealed significant associations between vaccination knowledge and guardian education level (χ2 = 8.719, df = 3, P = 0.033), monthly family income (χ2 = 10.001, df = 3, P = 0.018), household registration status (χ2 = 10.235, df = 2, P = 0.006), occupation (χ2 = 10.781, df = 3, P = 0.013), and housing situation (χ2 = 7.027, df = 2, P = 0.029). No significant associations were found with child gender or vaccination notification receipt (Table 2).
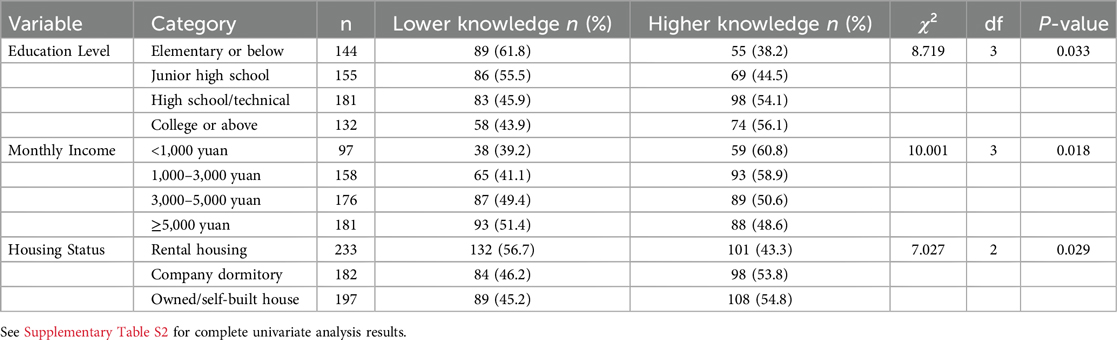
Table 2. Factors associated with vaccination knowledge - univariate analysis.
Logistic regression analysis identified education level, family income, and housing situation as independent predictors of vaccination knowledge. Guardians with higher education levels (OR = 1.51, 95%CI: 1.02–2.24, P = 0.041), higher family income (OR = 1.80, 95%CI: 1.09–2.96, P = 0.021), and better housing conditions (OR = 1.89, 95%CI: 1.03–3.45, P = 0.039) demonstrated significantly better vaccination knowledge.
Vaccination attitudes and practices
Most guardians (85.1%) considered vaccination necessary for children, while 70.6% viewed vaccination as the most cost-effective method for controlling infectious diseases. However, only 23.4% reported being unaffected by negative media coverage regarding vaccination.
Regarding vaccination practices, 69.9% of guardians proactively sought vaccination services for their children, while 41.5% were willing to pay for optional Category II vaccines. Compliance with post-vaccination observation requirements was reported by 31.9% of participants (Table 3).
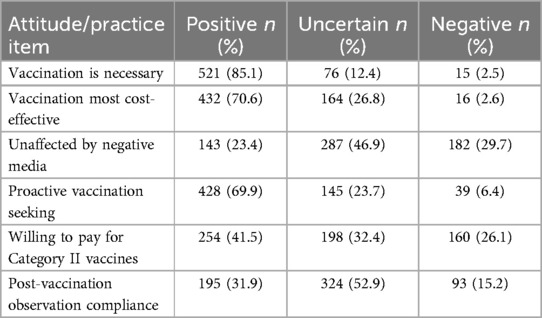
Table 3. Guardian attitudes and practices toward vaccination.
Information sources and service preferences
Primary sources of vaccination information included bulletin boards/brochures (21.9%), television/radio (18.3%), relatives/fellow residents (17.5%), vaccination certificates (15.0%), and medical personnel (14.5%). Internet sources accounted for 12.8% of information seeking.
Guardians expressed greatest concern about vaccine safety (25.2%) and effectiveness (20.8%), while cost concerns were relatively lower (15.5%). Preferred appointment notification methods included vaccination certificates (23.4%) and telephone calls (20.3%).
Desired services during vaccination included enhanced physician explanations about vaccines and related knowledge (17.3%), professional consultation services (16.8%), and reduced waiting times (13.4%).
Discussion
This cross-sectional study is the first to quantify childhood-vaccination knowledge, attitudes and practices (KAP) among guardians in a rapidly urbanising district of Chengdu that hosts a large migrant population. Three headline findings emerged. First, overall attitudes were strongly positive—more than four in five guardians endorsed the necessity of vaccination—yet substantial knowledge gaps remained, especially for Category II (self-paid) vaccines, with only one third recognising their importance. Second, socioeconomic gradients were pronounced: higher education, income and home ownership independently predicted better knowledge scores. Third, exposure to negative media reports was common and strongly associated with hesitant attitudes. Taken together, these results identify an urgent need for more nuanced, equity-focused communication strategies.
Participants in our study displayed a level of knowledge about Category II vaccines that aligns with results from an earlier investigation conducted in an inland setting, yet still trails behind the knowledge documented in a more economically developed coastal metropolis (24, 25). This gap is probably shaped by a combination of factors, including local economic conditions, the distribution of educational resources, the reach and intensity of public-health messaging, and how readily residents can access trustworthy health information. The regional discrepancy supports the notion that economic development and health-information infrastructure jointly shape vaccine awareness. Outside China, Wilson et al. reported that only 60% of French nurses recommended routine childhood immunisation (26), illustrating that professional endorsement alone does not guarantee universal parental confidence. Conversely, the 85.1% positive-attitude rate in our study exceeds the 71.0% reported in a United States HealthStyles survey during the same period (27), suggesting that guardians in Chengdu remain broadly supportive of the national immunisation programme despite media scandals.
The socioeconomic patterning we observed aligns with health-literacy theory, which posits that people with greater resources have better access to information and a higher capacity to evaluate conflicting claims (28, 29). For migrant families, structural barriers—unstable housing, time-poor employment and weaker social networks—likely limit exposure to reliable sources and magnify the impact of sensational online content. Kata has shown that anti-vaccine messages circulate rapidly on social media platforms by exploiting emotive storytelling and distrust of authorities (30). Our finding that barely a quarter of guardians remain unaffected by negative media underscores the need to inoculate parents against misinformation before crises erupt.
Based on these insights, three tiers of intervention appear feasible. First, strengthen point-of-care education: brief, image-rich modules delivered by vaccination nurses during observation periods can cover Category II indications, safety profiles and adverse-reaction management. Evidence from Hu et al. indicates that such micro-learning sessions significantly improve COVID-19 vaccine intent (31), and the same principle should translate to routine childhood vaccines. Second, leverage digital tools already embedded in daily life. Integrating a “smart reminder” function into existing WeChat health mini-programmes would allow guardians to scan the child's vaccination certificate and receive algorithm-tailored messages at key decision points, an approach supported by the favourable uptake of QR-code health passes during the pandemic. Third, embed vaccination messaging in migrant-friendly community venues—factory dormitories, urban villages and evening clinics—because caretakers in these settings report trusting peer advice over official brochures (32). Materials must be linguistically plain and visually guided to accommodate low functional literacy.
Economic considerations also merit attention. Although willingness to pay for Category II vaccines in our sample was only 41.5%, the figure exceeds the uptake recorded in Shanghai's migrant districts (<30%) (10). Progressive subsidy schemes—partial reimbursement for children from low-income households—could close the affordability gap while preserving consumer choice. Policymakers should pilot such schemes in high-migration wards and evaluate cost-effectiveness alongside educational interventions.
Several limitations warrant caution. The cross-sectional design precludes causal inference, and self-report may inflate desirable practices through social-desirability bias. Although we attained a 90% response rate, the single-centre setting may limit generalisability to rural Sichuan or other megacities. In addition, the KAP instrument, while demonstrating acceptable reliability (α = 0.82), has yet to be validated in non-Mandarin-speaking populations. Future work should (i) employ longitudinal designs to test whether tailored education improves actual Category II vaccination uptake over time, (ii) replicate our survey in multiple provinces to examine regional heterogeneity, and (iii) apply item-response theory to refine the questionnaire and establish normative cut-offs for “adequate” knowledge.
Conclusion
Guardians in Chengdu demonstrate positive attitudes toward childhood vaccination but require enhanced knowledge, particularly regarding vaccine categories, safety profiles, and adverse reaction management. Socioeconomic factors significantly influence vaccination knowledge levels, suggesting need for targeted educational interventions among vulnerable populations. Strengthening healthcare provider communication skills and developing comprehensive, culturally appropriate educational materials could substantially improve vaccination coverage and child health outcomes in this rapidly urbanizing population.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethics Committee of The Third People's Hospital of Chengdu (SC-CD-34). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements. The manuscript presents research on animals that do not require ethical approval for their study.
Author contributions
WL: Conceptualization, Writing – original draft. HL: Visualization, Writing – original draft. LQ: Methodology, Project administration, Writing – review & editing. HW: Data curation, Writing – original draft. KZ: Data curation, Writing – original draft. TY: Resources, Writing – original draft. XJ: Data curation, Writing – original draft. LX: Supervision, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2025.1511018/full#supplementary-material
References
2. Andre FE, Booy R, Bock HL, Clemens J, Datta SK, John TJ, et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull World Health Organ. (2008) 86(2):140–6. doi: 10.2471/BLT.07.040089
4. Liang X, Bi S, Yang W, Wang L, Cui G, Cui F, et al. Epidemiological serosurvey of hepatitis B in China–declining HBV prevalence due to hepatitis B vaccination. Vaccine. (2009) 27(47):6550–7. doi: 10.1016/j.vaccine.2009.08.048
5. National Health Commission of China. Regulations on Vaccine Circulation and Vaccination. Beijing: NHC (2019).
6. He S, Zhu C, Liu X, Wang Y. Parental knowledge, attitudes, and practices toward vaccinating their children against influenza: a cross-sectional study from China. Front Public Health. (2024 Jul 10) 12:1404506. doi: 10.3389/fpubh.2024.1404506
7. Zou B, Tan C, Deng R, Chen Q, Peng Q, Xu D, et al. Parents’ knowledge, attitude and practice regarding childhood circumcision: a cross-sectional study in the central region of sichuan, China. Front Pediatr. (2025) 13:1465998. doi: 10.3389/fped.2025.1465998
8. Ministry of Health of China. National Immunization Program Technical Guidelines. Beijing: People’s Medical Publishing House (2016).
9. Zhang Y, Wang Q, Xu J, Li M, Shao J, Liu Y. Effect evaluation of rubella knowledge attitudes and practices (KAP) intervention on parents of 0 to 2 year old children in Chongqing, China. Medicine (Baltimore). (2023) 102(45):e35709. doi: 10.1097/MD.0000000000035709
10. Wu J, Wei Z, Yang Y, Sun X, Zhan S, Jiang Q, et al. Gap between cognitions and behaviors among children’s guardians of influenza vaccination: the role of social influence and vaccine-related knowledge. Hum Vaccin Immunother. (2023) 19(1):2166285. doi: 10.1080/21645515.2023.2166285
11. Qian G, Yang J, Ding X, Xu M, Yue Q, Shen H, et al. Parental/guardians’ satisfaction with vaccination service and its associated factors: a cross-sectional study from Eastern China. BMC Public Health. (2024) 24(1):3574. doi: 10.1186/s12889-024-20980-1
12. Gust DA, Darling N, Kennedy A, Schwartz B. Parents with doubts about vaccines: which vaccines and reasons why. Pediatrics. (2008) 122(4):718–25. doi: 10.1542/peds.2007-0538
13. Benin AL, Wisler-Sher DJ, Colson E, Shapiro ED, Holmboe ES. Qualitative analysis of mothers’ decision-making about vaccines for infants: the importance of trust. Pediatrics. (2006) 117(5):1532–41. doi: 10.1542/peds.2005-1728
14. Opel DJ, Mangione-Smith R, Taylor JA, Korfiatis C, Wiese C, Catz S, et al. Development of a survey to identify vaccine-hesitant parents: the parent attitudes about childhood vaccines survey. Hum Vaccin. (2011) 7(4):419–25. doi: 10.4161/hv.7.4.14120
15. Dubé E, Laberge C, Guay M, Bramadat P, Roy R, Bettinger JA. Vaccine hesitancy: an overview. Hum Vaccin Immunother. (2013) 9(8):1763–73. doi: 10.4161/hv.24657
16. Larson HJ, Jarrett C, Eckersberger E, Smith DM, Paterson P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: a systematic review of published literature, 2007–2012. Vaccine. (2014) 32(19):2150–9. doi: 10.1016/j.vaccine.2014.01.081
17. MacDonald NE, SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: definition, scope and determinants. Vaccine. (2015) 33(34):4161–4. doi: 10.1016/j.vaccine.2015.04.036
18. Yaqub O, Castle-Clarke S, Sevdalis N, Chataway J. Attitudes to vaccination: a critical review. Soc Sci Med. (2014) 112:1–11. doi: 10.1016/j.socscimed.2014.04.018
19. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. 10th ed Philadelphia: Lippincott Williams & Wilkins (2017).
20. DeVellis RF. Scale Development: Theory and Applications. 4th ed. Thousand Oaks: Sage Publications (2016).
21. Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. (1951) 16(3):297–334. doi: 10.1007/BF02310555
23. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. (2013) 310(20):2191–4. doi: 10.1001/jama.2013.281053
24. Zhang KC, Fang Y, Cao H, Chen H, Hu T, Chen Y, et al. Behavioral intention to receive a COVID-19 vaccination among Chinese factory workers: cross-sectional online survey. J Med Internet Res. (2021) 23(3):e24673. doi: 10.2196/24673
25. Li T, Qiu X, Gong X, Zhan R, Zheng X. The cross-sectional survey on COVID-19 vaccine hesitancy and it predictors among Chinese parents of 3–17 years aged children in Shenzhen city. Ann Agric Environ Med. (2022) 29(1):120–5. doi: 10.26444/aaem/146263
26. Wilson R, Zaytseva A, Bocquier A, Nokri A, Fressard L, Chamboredon P, et al. Vaccine hesitancy and self-vaccination behaviors among nurses in southeastern France. Vaccine. (2020) 38(5):1144–51. doi: 10.1016/j.vaccine.2019.11.018
27. Kennedy A, Basket M, Sheedy K. Vaccine attitudes, concerns, and information sources reported by parents of young children: results from the 2009 HealthStyles survey. Pediatrics. (2011) 127(Suppl 1):S92–99. doi: 10.1542/peds.2010-1722N
28. Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. (2011) 155(2):97–107. doi: 10.7326/0003-4819-155-2-201107190-00005
29. Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int. (2000) 15(3):259–67. doi: 10.1093/heapro/15.3.259
30. Kata A. Anti-vaccine activists, web 2.0, and the postmodern paradigm–an overview of tactics and tropes used online by the anti-vaccination movement. Vaccine. (2012) 30(25):3778–89. doi: 10.1016/j.vaccine.2011.11.112
31. Gao H, Hu R, Yin L, Yuan X, Tang H, Luo L, et al. Knowledge, attitudes and practices of the Chinese public with respect to coronavirus disease (COVID-19): an online cross-sectional survey. BMC Public Health. (2020) 20(1):1816. doi: 10.1186/s12889-020-09961-2
Keywords: children's guardians, vaccines, vaccination, knowledge, attitudes, practices, influencing factors
Citation: Liu W, Li H, Qin L, Wang H, Zhu K, Yang T, Jia X and Xu L (2025) Knowledge, attitudes and practices toward childhood vaccination among guardians in Chengdu, China: a cross-sectional study. Front. Pediatr. 13:1511018. doi: 10.3389/fped.2025.1511018
Received: 14 October 2024; Accepted: 6 June 2025;
Published: 14 July 2025.
Edited by:
Chiara de Waure, University of Perugia, ItalyReviewed by:
Shrijana Shrestha, Patan Academy of Health Sciences, NepalHarpaljit Kaur, Taylor’s University, Malaysia
Copyright: © 2025 Liu, Li, Qin, Wang, Zhu, Yang, Jia and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ling Qin, MTg5ODA1MDU5MDNAMTYzLmNvbQ==
†These authors share first authorship