 Barnabás Rózsai
Barnabás Rózsai Diána Simon
Diána Simon Tímea Berki
Tímea Berki Gabriella Kiss1
Gabriella Kiss1 Bernadett Mosdósi
Bernadett Mosdósi- 1Department of Pediatrics, Medical School, University of Pécs, Pécs, Hungary
- 2Department of Immunology and Biotechnology, Medical School, University of Pécs, Pécs, Hungary
Purpose: Despite the worldwide decrease in the incidence of serious pneumococcal infections following the introduction of the 13-valent pneumococcal conjugate vaccines (PCV13), invasive infections still occur. This study aimed to investigate the immunological function of children with severe parapneumonic effusion (PPE) both during their hospitalization and after full recovery.
Methods: This was a prospective, single-center study. Children with PPE were admitted to our clinic between 1 January 2011 and 30 June 2023, and participated in the study. Due to the severity of the effusion, all PPE cases required thoracic drainage and some children also underwent fibrinolysis and/or video-assisted thoracoscopic surgery. Demographic and clinical data and laboratory results were collected at admission. Extended immunological testing was performed at the time of clinical admission and again 6–8 weeks after discharge.
Results: A total of 66 episodes of PPE were identified. During hospitalization, one patient was diagnosed with human immunodeficiency virus infection and another with immunoglobulin A deficiency. Extended immunological evaluation was performed during follow-up in 49 patients. Within this cohort, seven patients were diagnosed with mannose-binding lectin deficiency and three with specific antibody deficiency. In total, immune dysfunction was confirmed in 12 patients. When comparing the immunocompromised and non-immunocompromised groups, the duration of hospitalization was longer in the immunocompromised group, with no other differences observed.
Conclusion: Although the incidence of severe PPE has declined since the introduction of PCV13, immunological evaluation remains essential for identifying underlying immunodeficiencies. Despite vaccination, screening patients with PPE for immune dysfunction is crucial. Early diagnosis and timely treatment can help prevent organ damage and reduce long-term morbidity.
Introduction
Pleural effusions can stem from a variety of infectious and non-infectious disorders. Infection is the most common cause (50%–70%), with parapneumonic effusion (PPE) being a prominent example. Less frequent causes include malignancy and congestive heart failure (1).
Despite the widespread use of pneumococcal conjugate vaccines since the early 2010s, Streptococcus pneumoniae remains the leading cause of PPE worldwide (2). Asymptomatic nasopharyngeal carriage of this pathogen occurs in up to 60% of healthy young children (3), with even higher rates observed in low- and lower-middle-income countries (4). S. pneumoniae can cause a spectrum of illnesses, ranging from mild infections to severe diseases, such as pneumonia, PPE, septicemia, and meningitis, all associated with significant morbidity and mortality (5). PPE remains a severe complication of community-acquired pneumonia, with a considerable number of affected children requiring admission to the intensive care unit (2).
The introduction of the pneumococcal conjugate vaccine (PCV) between 2008 and 2010 significantly reduced both the incidence of pneumonia and its complications, including the PPE incidence rate (1). In the United States, the incidence of PPE peaked at 4.2 cases per 100,000 children annually prior to the PCV era. Following vaccine implementation, this number decreased to approximately two hospital admissions per 100,000 children per year between 2008 and 2014 (6). A similar trend was observed in the United Kingdom. Saxena et al. reported that, before the introduction of PCV13 in 2010, the annual hospitalization rate for PPE was 3.9 per 100,000 children. By 2013, this rate had declined to 1.9 per 100,000 children (7).
However, data also indicate that while the incidence of pneumococcal PPE has declined, there has been a corresponding increase in infections caused by Streptococcus pyogenes (8).
In patients with inborn errors of immunity (IEI), severe bacterial infections commonly manifest around 4 months of age, coinciding with the waning of maternally acquired immunoglobulins. IEIs represent a genetically and clinically heterogeneous group of disorders, currently comprising at least 500 genetically defined single-gene defects (9). The hallmark of immunodeficiency (ID) is increased susceptibility to infection; however, the affected organs and pathogens vary depending on the type of immune defect. In immunocompromised patients, invasive pneumococcal disease (IPD) can lead to life-threatening complications. A meta-analysis by van Aalst et al. found that the incidence of IPD is approximately 6–30 times higher in patients with different types of ID compared to healthy controls (10). Despite this, limited data are available regarding the immune function of children with PPE. The primary aim of this study was to evaluate the immunological function and immune response to infection in children with PPE. Additionally, we aimed to estimate the prevalence of different types of immune deficiencies within this patient population.
Materials and methods
Patients and methods
This was a single-center, prospective study conducted at the Department of Pediatrics, Medical School, University of Pécs. A total of 66 children (41 girls and 25 boys) were enrolled in the analysis between 1 January 2011 and 30 June 2023. Exclusion criteria included pleural fluid due to malignancy or trauma (hemothorax), iatrogenic causes of immunodeficiency (such as medications, nutritional status, or anatomic abnormalities), a known family history of immunodeficiency or autoimmune disease, and a history of previous bacterial infections.
The average age of the patients at admission was 4.8 ± 3.7 years (average ± SD). Before hospitalization, 60 patients (90.9%) had received prior vaccination with either PCV7 or PCV13, and 49 patients (74.2%) had received oral antibiotic treatment.
Upon hospitalization, all patients were treated empirically with parenteral antibiotic therapy with ceftriaxone (80 mg/kg/day), with or without clindamycin (40 mg/kg/day); this treatment was later adjusted based on microbiological results or the clinical response. Additionally, a thoracic drain was performed in all cases using an 8–12-Fr pigtail catheter. Indications for thoracic drainage included pleural fluid wider than 2 cm at the level of the hilus, the presence of septation or loculation in the pleural space (as detected by thoracic ultrasound), or severe respiratory distress in the presence of any pleural fluid. The thoracic drainage was initiated on the second (median) day of hospitalization [interquartile range (IQR): 1–3.5 days] and lasted for 6 (4–11.5) days. In cases of inadequate drainage or the appearance of loculation, intrapleural fibrinolytic therapy with tissue plasminogen activator (Alteplase, Genentech, USA) and/or thoracic surgery—either video-assisted thoracoscopic surgery (VATS) or decortication—was performed. Fibrinolytic treatment was administered in 56.1% (37/66) of cases. Due to insufficient conservative therapy, 18 patients (27.3%) required surgical intervention (decortication and/or VATS).
Extensive microbiological analysis of the pleural effusion was performed, utilizing standard culture, urinary antigen testing, and polymerase chain reaction (PCR) techniques. Simultaneously, blood culture was also obtained. At the beginning of hospitalization, an initial immunological screening test and routine blood tests, including complete blood count, C-reactive protein (CRP), procalcitonin, and blood culture, were performed. This included measuring serum immunoglobulin levels (IgA, IgE, IgG, IgM) and multiparameter flow cytometry analysis of lymphocyte subsets. Extended immunological evaluation was conducted 6–8 weeks after hospital discharge at the Allergy and Immunology Outpatient Care Unit of our clinic. At the outpatient unit, patients were clinically assessed, and peripheral venous blood samples were collected from all participants. Routine laboratory tests included complete blood count, CRP, serum immunoglobulin levels (IgA, IgE, IgG, IgM), and complement components (C3, C4). We also performed functional assessments of the classical, alternative, and lectin complement pathways. Additionally, peripheral blood lymphocytes were analyzed using multiparameter flow cytometry (Beckton Dickson and Company Biosciences, San Jose, USA). The following cell types were evaluated: CD56+ natural killer cells, CD3 + CD56+ natural killer T cells, CD3 + CD8+ cytotoxic and CD3 + CD4+ helper T lymphocytes, CD19 + CD5+ B1 and CD19 + CD5− B2 B lymphocytes, CD4 + CD25 high+ regulatory T and CD3 + CD25 medium+ activated T cells, CD3 + HLADR+ activated T cells, CD8 + HLADR+ activated T cytotoxic cell, CD3 + CD45RA+ naïve and CD3 + CD45RO+ memory T cells, CD19 + IgD + CD27− naïve B cells, and CD19 + IgD + CD27+ non-switched B and CD19 + CD27 + IgD− switched B cells. Specific antibody titers (against S. pneumoniae, tetanus, diphtheria, and Haemophilus influenzae type b) were also measured.
The classical complement pathway was assessed using a hemolytic complement assay with sheep red blood cells. The alternative and lectin complement pathways were evaluated by ELISA. The results for the lectin complement pathways were expressed as a percentage of a standard control, with values below 30% considered abnormal. Abdominal ultrasound was performed to exclude asplenia. Immunodeficiencies were defined according to the criteria of the International Union of Immunological Societies(11). Based on the results of the immunological investigations, the patients were categorized into two groups: those with and those without impaired immune function.
The study was approved by the Local Ethics Committee (Medical School, University of Pécs). Informed consent was obtained from the parents or legal guardians of all participants.
Data analysis and statistics
SPSS for Windows 28.0 statistical software was used. Data distributions were tested for normality using the Kolmogorov–Smirnov test. Given that age, time and length of the drainage, lymphocyte count, the pleural fluid lactate dehydrogenase concentration, levels of the classical and alternative complement pathways, C3 and C4 levels, and pneumococcal antibody titer did not exhibit normal distribution, their median and IQR values are provided. For assessing statistically significant differences, Student's t-test (for normally distributed data), the Mann–Whitney test (for non-normally distributed data), and the χ2 test or Fisher’s exact test (for dichotomous variables) were used. A p-value of <0.05 was considered to be statistically significant.
Results
Clinical data
In this prospective study, S. pneumoniae was identified as the main etiological agent in 48 of 66 cases (72.7%). Only four patients (6.0%) required mechanical ventilation, while the remaining 60 children (90.9%) received supplemental oxygen therapy. The median duration of hospitalization was 16 days [interquartile range (IQR): 12–23.2], and no deaths occurred in the study population.
Seventeen patients were unavailable for follow-up and were therefore excluded from further analysis. Ultimately, 49 children were included in the extended immunological evaluation. There were no significant differences in age, sex, duration of drainage, length of oxygen therapy, or total hospital stay between those who participated in follow-up examinations and those who did not.
Immunological data
Impaired immune function was identified in 12 of 49 patients (24.5%). Of these, seven patients were diagnosed with mannose-binding lectin (MBL) deficiency, three with specific antibody deficiency (SAD), one with IgA deficiency, and one with human immunodeficiency virus (HIV) infection. Demographic characteristics of patients with and without immunodeficiency are summarized in Table 1. No significant differences were observed between the two groups regarding age, gender, the start of drainage, or the frequency of use of fibrinolytic and VATS/decortication procedures. However, the duration of hospitalization was significantly longer in immunocompromised patients than in those without immune dysfunction [19.0 (16.5–22.5) vs. 14.0 (12–20) days; p = 0.006].
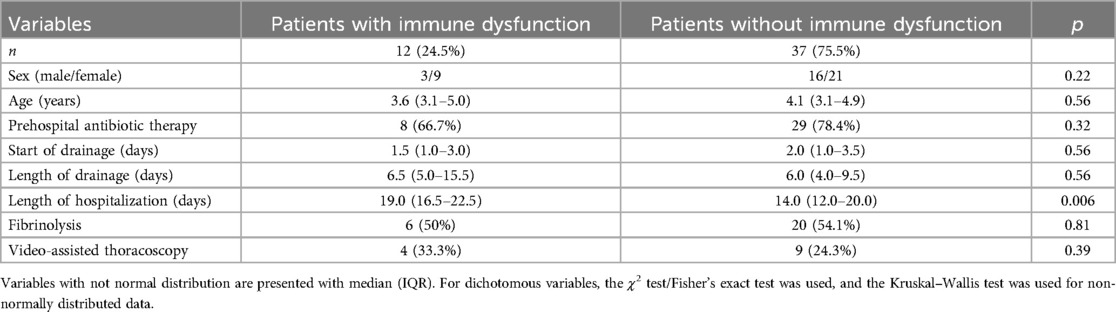
Table 1. Demographic data and clinical characteristics of the participants.
Table 2 presents the pleural fluid characteristics and basic immunological findings of patients at ICU admission. Biochemical parameters of pleural fluid did not differ significantly between groups. Both groups exhibited elevated white blood cell and absolute neutrophil count levels without significant difference. Neutropenia was not observed in any patient. One 5-year-old patient, diagnosed with IgA deficiency, had an IgA level below 0.05 g/L. In the immunocompromised group, both IgM and IgG levels showed a non-significant increase. While median lymphocyte counts and subpopulations remained within the normal range, the percentage of CD3+CD25+ activated T cells was significantly higher in patients with immune dysfunction [2.8 (1.2–5.0) vs. 0.8 (0.7–1.8)%; p = 0.006]. Severe CD4+ lymphopenia (146/μl) was detected in a patient with confirmed HIV infection by serology.
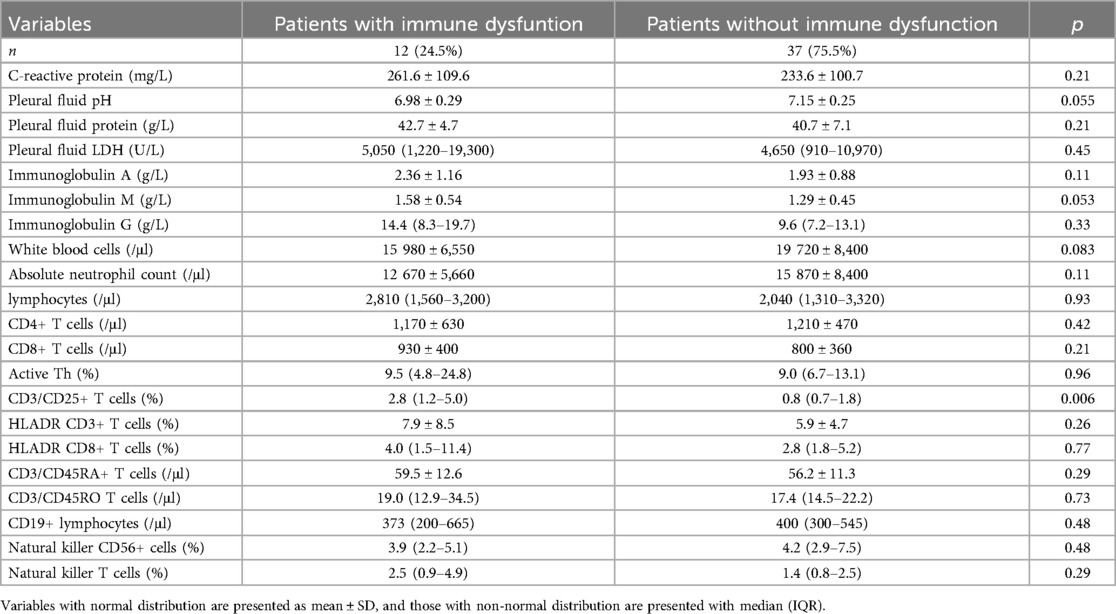
Table 2. Common laboratory and basic immunological values at hospitalization of the participants.
Table 3 details the extended immunological findings from outpatient follow-up. The total CD19+ naïve B lymphocyte counts and the age-matched Ig levels were within the normal range and did not differ significantly between groups. However, three patients exhibited low pneumococcal antibody concentrations (19.6, 26.3, and 37.2 mg/L; normal range: >50 mg/L) despite confirmed severe infection and vaccination. Since revaccination did not increase antibody titers, they were diagnosed with specific antibody deficiency. All three patients began immunoglobulin replacement therapy.
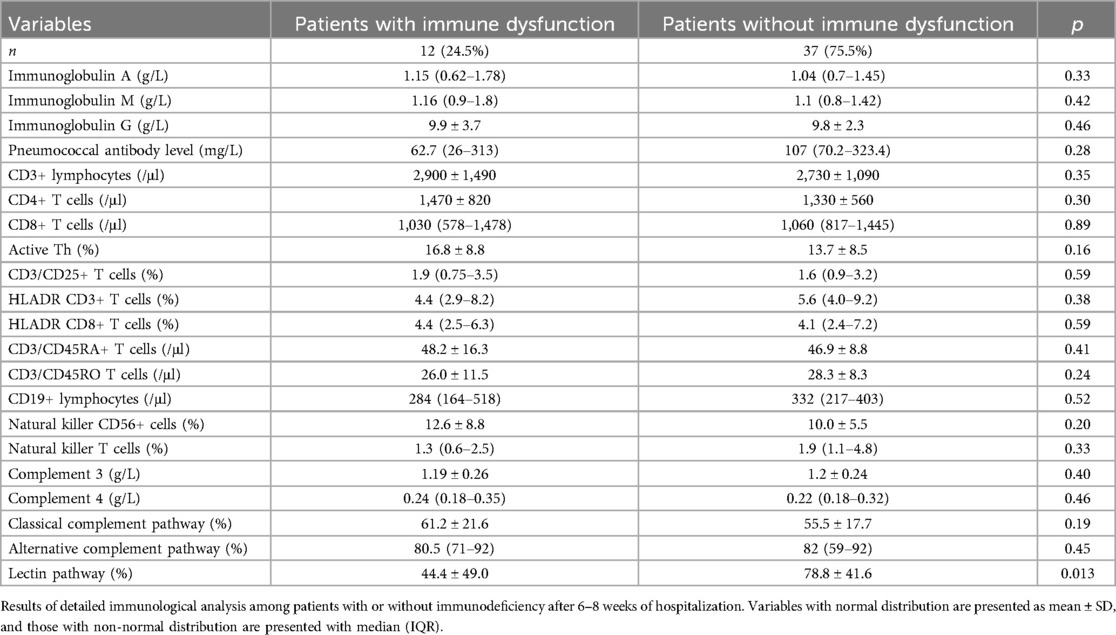
Table 3. Detailed immunological characteristics of patients at the outpatient unit.
Antibody titers for tetanus, diphtheria, and Haemophilus were within the normal range in both groups. T-cell numbers, subsets, and activation markers were also within the normal range, with no significant difference observed between groups.
The classical and alternative complement pathways were within normal ranges; however, seven children exhibited reduced lectin pathway activity and were diagnosed with MBL deficiency.
No cases of asplenia were detected by abdominal ultrasound examination.
Discussion
To our knowledge, the study represents the first investigation into extended immune function within a homogeneous cohort of children presenting with severe PPE and requiring intensive care treatment. Our screening protocol revealed that approximately one in four children with severe PPE exhibited some degree of immune dysfunction.
Severe infections can occur in vulnerable patients who are immunocompromised by immunosuppressive treatment, HIV infection, or chronic inflammatory diseases (12). For cases where no identifiable risk factor is apparent at presentation, comprehensive immunological exploration is crucial for detecting potential primary or acquired immunodeficiencies (13). While severe bacterial infection may be the initial presenting symptom of IEI, immunological screening is not yet standard practice in many clinical settings (14).
A retrospective study by Strasser et al. identified significantly impaired immune function in 6% of pediatric patients with severe bacterial infection requiring intensive care (15). Furthermore, an additional 11% of subjects exhibited mild immunological abnormalities, which were potentially attributable to delayed immune system maturation. This suggests that approximately 17% of their heterogeneous patient population—which included children with sepsis, meningitis, and PPE—demonstrated varying degrees of immune dysfunction. Our prospective study, focusing exclusively on a homogeneous PPE cohort, found a similar prevalence (15). Previous studies indicate that 1%–10% of children presenting with invasive pneumococcal disease possess an underlying IEI (16–18).
Pulmonary disease is common among patients with IEI (19). While individual disorders are rare, collectively, they represent a significant cause of morbidity and mortality (20).
S. pneumoniae is the primary pathogen responsible for PPE. The severity and localization of pneumococcal infection vary from asymptomatic colonization to invasive disease. The pathomechanism underlying the progression from asymptomatic colonization to invasive pneumococcal infection remains poorly understood. Factors such as strain-specific virulence and the presence of underlying chronic disorders or immunodeficiencies may contribute to this progression (21).
The immune defense against pneumococcal infection involves complex pathomechanisms. The innate immune system functions as the first line of defense. Peptidoglycans found in Gram-positive bacteria primarily activate the complement system via the alternative pathway. Additionally, bacteria expressing mannose residues on their surface can bind MBL, thereby facilitating opsonization and activating the complement system via the lectin pathway (22). MBL, a soluble pattern recognition molecule, contributes to the elimination of a broad spectrum of pathogenic microorganisms by activating the lectin complement pathway and promoting opsonophagocytosis (22).
The synthesis of MBL is influenced by polymorphisms in the MBL2 gene. However, serum MBL levels are not solely determined by genotype, as other genetic and environmental factors also affect their expression. Therefore, measuring serum MBL levels is considered a more reliable method for diagnosing MBL deficiency than relying solely on genotyping (23). Clinical studies have demonstrated that MBL deficiency predisposes individuals to severe respiratory tract infections (24).
Nasopharyngeal carriage of S. pneumoniae is approximately twice as prevalent in MBL-deficient children compared to healthy controls (25). Furthermore, MBL deficiency plays a more prominent role in infection susceptibility in individuals with predisposing risk factors, such as chronic lung disease and cystic fibrosis, and in infants with immature adaptive immune systems (24). The absence of these above-mentioned risk factors in our patients underscores the importance of comprehensive immunological screening.
Several studies have reported an increased risk of invasive pneumococcal disease in MBL-deficient children and adults (26–28). In our study, MBL deficiency was the most common immunodeficiency identified. Although no serious infections occurred during the follow-up period, upper respiratory tract infections were more frequent in these patients than in healthy controls. Currently, no specific therapy exists for this complement deficiency; however, immunization of family members and household contacts is recommended to reduce the risk of infections (29).
The cellular immune response also plays a critical role in protection against pneumococcal infection (30). The Th17 response has been shown to be a key component of pneumococcal immunity in both mouse models and immunodeficiency conditions, such as hyper-IgE syndrome (31, 32). Serum immunoglobulin E levels in our patients were below 2,000 IU/ml, thereby effectively ruling out hyper-IgE syndrome. The severe CD4+ lymphopenia in our HIV-infected patient further highlights the importance of screening for secondary immunodeficiencies. The significantly elevated CD3+CD25+ T-cell count within the immunocompromised group is likely indicative of immunocompensatory mechanisms.
Recurrent sinopulmonary infections represent a typical symptom of humoral immune deficiency (33), which is the most common form of IEI. This condition can result from defects in B-cell development, abnormal B-cell activation, or impaired antibody synthesis. Screening for humoral IEI typically involves flow cytometric analysis of B-cell subsets, quantitative measurement of serum immunoglobulin levels, and evaluation of specific antibody responses to infection and/or vaccination (34, 35).
Within our cohort, one patient was diagnosed with selective IgA deficiency (sIgAD). Most individuals with sIgAD are asymptomatic or experience mild sinopulmonary and gastrointestinal infections (36). However, Gaschignard et al. reported a notably higher prevalence of IgA deficiency (5%–7%) in children with severe bacterial infection compared to the general population (<1%) (16). It is important to emphasize that during immunological follow-up, 20%–30% of patients with IgA deficiency may develop autoimmune disorders, such as celiac disease or thyroiditis (37).
Three patients were diagnosed with SAD, which is characterized by an isolated, impaired antibody response to polysaccharide antigens despite normal levels of serum IgG, IgG subclass, IgA, and IgM, as well as normal T-cell subpopulations (38). Several monogenic disorders, including common variable immunodeficiency disorders, ataxia telangiectasia, Wiskott–Aldrich syndrome, and nuclear factor-kappa-B essential modulator deficiency, are associated with SAD. Identification of these patients is critical for appropriate management and prevention of complications. Early antibiotic treatment and regular immunoglobulin replacement therapy can prevent long-term complications such as mastoiditis and bronchiectasis (39). In our cohort, we observed no infections after initiating immunoglobulin substitution therapy. In addition to infectious complications, non-infectious manifestations such as autoimmunity and hematopoietic malignancies have also been reported in patients with SAD.
Rare primary immunodeficiency syndromes may also predispose patients to severe pneumococcal infections. Autosomal recessive disorders, such as NF-kappa-B essential modulator (NEMO) or NF-kappa-B alpha inhibitor (IKBA) deficiency, along with IL-1 receptor-associated kinase type 4 (IRAK-4) and myeloid differentiation primary response 88 (MyD88) deficiency, disrupt Toll-like receptor and interleukin-1 receptor signaling pathways, leading to increased susceptibility to severe infections (40).
In our study, it was not possible to investigate interleukin 6 production by white blood cells; therefore, the presence of MyD88 deficiency and disruptions in Toll-like receptor signaling were not assessed. Additionally, genetic testing was not performed on our patients. It is worth noting that, however, genetic testing is not routinely performed in clinical practice (41).
Primary immunodeficiency diseases and acquired immunodeficiencies can also predispose to severe infection. HIV infection is the most common acquired immunodeficiency. The prevalence of pleural effusion among patients hospitalized with AIDS ranges from 2% to 20%, often caused by bacterial infection, tuberculous pleuritis, or other malignancies (42). Staphylococcus aureus was more common in the HIV-positive group, along with anaerobic and opportunistic infections. In our study, the patient's severe infection, dystrophic appearance, and severe stomatitis raised suspicion of HIV infection, which was subsequently confirmed by serological testing.
Conclusion
Pulmonary disease is a common manifestation of many IEIs and continues to be a leading cause of morbidity and mortality. In our study, varying degrees of immune impairment were identified in approximately one-quarter of children presenting with severe PPE. We advocate for detailed immunological screening in children with severe PPE. Early diagnosis and timely initiation of appropriate treatment are crucial for improving the prognosis of patients with primary immunodeficiencies.
Study limitations
Our study has several limitations. First, it single-hospital setting may limit the generalizability of our findings. Second, not all children with PPE were tested for detailed immune function; therefore, the true prevalence of immunodeficiencies in this population may differ from that reported here. However, basic physiological and laboratory parameters did not significantly differ between the tested and untested groups. Additionally, pneumococcal serotyping of patients has only been feasible in recent years, so serotype data are not available for all cases. Among the serotyped isolates, serotype 3 was the predominant strain (unpublished data).
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Ethics statement
The studies involving humans were approved by the Local Ethics Committee, Medical School, University of Pécs. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
BR: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing. DS: Methodology, Validation, Writing – review & editing. TB: Methodology, Supervision, Validation, Writing – review & editing. GK: Data curation, Investigation, Project administration, Writing – original draft. BM: Conceptualization, Formal analysis, Investigation, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The publication fee was supported by the Medical School, University of Pécs.
Acknowledgments
The authors thank the nurses and doctors who participated in the assessment and treatment of the patients. The authors are grateful to Tamás Tirczka (†) and Tímea Erdősi for their conscientious and prompt PCR testing and thank Professor Gyula Soltész for the grammatical check of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ANC, absolute neutrophil count; CAP, community-acquired pneumonia; CD, cluster of differentiation; CVID, common variable immunodeficiency disorder; CRP, C-reactive protein; HIV, human immunodeficiency virus; ID, immunodeficiency; IEI, inborn errors of immunity; Ig, immunoglobulin; IKBA, NF-kappa-B alpha inhibitor; IPD, invasive pneumococcal disease; IRAK-4, IL-1 receptor-associated kinase type 4; NEMO, NF-kappa-B essential modulator; MyD88, myeloid differentiation primary response 88; PCV, pneumococcal conjugate vaccine; PPE, parapneumonic effusion; SAD, specific antibody deficiency; VATS, video-assisted thoracoscopic surgery; WBC, white blood cell.
References
1. Efrati O, Barak A. Pleural effusions in the pediatric population. Pediatr Rev. (2002) 23(12):417–26. doi: 10.1542/pir.23.12.417
2. de Benedictis FM, Kerem E, Chang AB, Colin AA, Zar HJ, Bush A. Complicated pneumonia in children. Lancet. (2020) 396(10253):786–98. doi: 10.1016/S0140-6736(20)31550-6
3. Zemlicková H, Urbásková P, Adámková V, Motlová J, Lebedová V, Procházka B. Characteristics of Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis and Staphylococcus aureus isolated from the nasopharynx of healthy children attending day-care centres in the Czech republic. Epidemiol Infect. (2006) 134(6):1179–87. doi: 10.1017/S0950268806006157
4. Tvedskov ESF, Hovmand N, Benfield T, Tinggaard M. Pneumococcal carriage among children in low and lower-middle-income countries: a systematic review. Int J Infect Dis. (2022) 115:1–7. doi: 10.1016/j.ijid.2021.11.021
5. Backhaus E, Berg S, Andersson R, Ockborn G, Malmström P, Dahl M, et al. Epidemiology of invasive pneumococcal infections: manifestations, incidence and case fatality rate correlated to age, gender and risk factors. BMC Infect Dis. (2016) 16:367. doi: 10.1186/s12879-016-1648-2
6. Kelly MM, Coller RJ, Kohler JE, Zhao Q, Sklansky DJ, Shadman KA, et al. Trends in hospital treatment of empyema in children in the United States. J Pediatr. (2018) 202:245–51. doi: 10.1016/j.jpeds.2018.07.004
7. Saxena S, Atchison C, Cecil E, Sharland M, Koshy E, Bottle A. Additive impact of pneumococcal conjugate vaccines on pneumonia and empyema hospital admissions in England. J Infect. (2015) 71(4):428–36. doi: 10.1016/j.jinf.2015.06.011
8. Liese JG, Schoen C, van der Linden M, Lehmann L, Goettler D, Keller S, et al. Changes in the incidence and bacterial aetiology of paediatric parapneumonic pleural effusion/empyema in Germany, 2010–2017: a nationwide surveillance study. Clin Microbiol Infect. (2019) 25(7):857–64. doi: 10.1016/j.cmi.2018.10.020
9. Notarangelo LD, Bacchetta R, Casanova JL, Su HC. Human inborn errors of immunity: an expanding universe. Sci Immunol. (2020) 5(49):eabb1662. doi: 10.1126/sciimmunol.abb1662
10. van Aalst M, Lötsch F, Spijker R, van der Meer JTM, Langendam MW, Goorhuis A, et al. Incidence of invasive pneumococcal disease in immunocompromised patients: a systematic review and meta-analysis. Travel Med Infect Dis. (2018) 24:89–100. doi: 10.1016/j.tmaid.2018.05.016
11. Bousfiha A, Moundir A, Tangye SG, Picard C, Jeddane L, Al-Herz W, et al. The 2022 update of IUIS phenotypical classification for human inborn errors of immunity. J Clin Immunol. (2022) 42(7):1508–20. doi: 10.1007/s10875-022-01352-z
12. Agyeman PKA, Schlapbach LJ, Giannoni E, Stocker M, Posfay-Barbe KM, Heininger U, et al. Epidemiology of blood culture-proven bacterial sepsis in children in Switzerland: a population-based cohort study. Lancet Child Adolesc Heal. (2017) 1:124–33. doi: 10.1016/S2352-4642(17)30010-X
13. De Vries E, European Society for Immunodeficiencies (ESID) members. Patient-centred screening for primary immunodeficiency, a multi-stage diagnostic protocol designed for non-immunologists: 2011 update. Clin Exp Immunol. (2012) 167:108–19. doi: 10.1111/j.1365-2249.2011.04461.x
14. Bijker EM, van Well GTJ. Immunological evaluation of children with a first severe bacterial infection: standard of care? J Infect Dis. (2023) 228(1):1–3. doi: 10.1093/infdis/jiad099
15. Strasser S, Relly C, Berger C, Trück J. Structured immune workup in healthy children with a first episode of severe bacterial infection: a 7-year single-center study. J Infect Dis. (2023) 228(1):8–17. doi: 10.1093/infdis/jiad098
16. Gaschignard J, Levy C, Chrabieh M, Boisson B, Bost-Bru C, Dauger S, et al. Invasive pneumococcal disease in children can reveal a primary immunodeficiency. Clin Infect Dis. (2014) 59:244–51. doi: 10.1093/cid/ciu274
17. Bijker EM, Bateman EA, Trück J, Patel S, Kelly DF. Screening for immunodeficiencies in children with invasive pneumococcal disease: six-year experience from a UK children’s hospital. Pediatr Infect Dis J. (2022) 41:575–8. doi: 10.1097/INF.0000000000003554
18. Butters C, Phuong LK, Cole T, Gwee A. Prevalence of immunodeficiency in children with invasive pneumococcal disease in the pneumococcal vaccine era. JAMA Pediatr. (2019) 173(11):1084–94. doi: 10.1001/jamapediatrics.2019.3203
19. Yazdani R, Abolhassani H, Asgardoon MH, Shaghaghi M, Modaresi M, Azizi G, et al. Infectious and noninfectious pulmonary complications in patients with primary immunodeficiency disorders. J Investig Allergol Clin Immunol. (2017) 27(4):213–24. doi: 10.18176/jiaci.0166
20. Joshi AY, Iyer VN, Hagan JB, St Sauver JL, Boyce TG. Incidence and temporal trends of primary immunodeficiency: a population-based cohort study. Mayo Clin Proc. (2009) 84:16–22. doi: 10.4065/84.1.16
21. Henriques-Normark B, Tuomanen EI. The pneumococcus: epidemiology, microbiology, and pathogenesis. Cold Spring Harb Perspect Med. (2013) 3(7):a010215. doi: 10.1101/cshperspect.a010215
22. Eisen DP, Minchinton RM. Impact of mannose-binding lectin on susceptibility to infectious diseases. Clin Infect Dis. (2003) 37(11):1496–505. doi: 10.1086/379324
23. Madsen HO, Garred P, Thiel S, Kurtzhals JA, Lamm LU, Ryder LP, et al. Interplay between promoter and structural gene variants control basal serum level of mannan-binding protein. J Immunol. (1995) 155(6):3013–20. doi: 10.4049/jimmunol.155.6.3013
24. Eisen DP. Mannose-binding lectin deficiency and respiratory tract infection. J Innate Immun. (2010) 2(2):114–22. doi: 10.1159/000228159
25. Vuononvirta J, Toivonen L, Gröndahl-Yli-Hannuksela K, Barkoff AM, Lindholm L, Mertsola J, et al. Nasopharyngeal bacterial colonization and gene polymorphisms of mannose-binding lectin and toll-like receptors 2 and 4 in infants. PLoS One. (2011) 6(10):e26198. doi: 10.1371/journal.pone.0026198
26. Bautista-Rodriguez C, Launes C, Jordan I, Andres M, Arias MT, Lozano F, et al. Mannose-binding lectin-deficient genotypes as a risk factor of pneumococcal meningitis in infants. PLoS One. (2017) 12(5):e0178377. doi: 10.1371/journal.pone.0178377
27. Muñoz-Almagro C, Bautista C, Arias MT, Boixeda R, Del Amo E, Borrás C, et al. High prevalence of genetically-determined mannose binding lectin deficiency in young children with invasive pneumococcal disease. Clin Microbiol Infect. (2014) 20(10):O745–52. doi: 10.1111/1469-0691.12615
28. Vallès X, Roca A, Lozano F, Morais L, Suárez B, Casals F, et al. Serotype-specific pneumococcal disease may be influenced by mannose-binding lectin deficiency. Eur Respir J. (2010) 36(4):856–63. doi: 10.1183/09031936.00171409
29. Shearer WT, Fleisher TA, Buckley RH, Ballas Z, Ballow M, Blaese RM, et al. Recommendations for live viral and bacterial vaccines in immunodeficient patients and their close contacts. J Allergy Clin Immunol. (2014) 133(4):961–6. doi: 10.1016/j.jaci.2013.11.043
30. Malley R, Trzcinski K, Srivastava A, Thompson CM, Anderson PW, Lipsitch M. CD4T cells mediate antibody-independent acquired immunity to pneumococcal colonization. Proc Natl Acad Sci U S A. (2005) 102:4848–53. doi: 10.1073/pnas.0501254102
31. Lu YJ, Gross J, Bogaert D, Finn A, Bagrade L, Zhang Q, et al. Interleukin-17A mediates acquired immunity to pneumococcal colonization. PLoS Pathog. (2008) 4(9):e1000159. doi: 10.1371/journal.ppat.1000159
32. Su HC. Dedicator of cytokinesis 8 (DOCK8) deficiency. Curr Opin Allergy Clin Immunol. (2010) 10(6):515–20. doi: 10.1097/ACI.0b013e32833fd718
33. El-Bohy M, Poowuttikul P, Secord E. Humoral immune deficiencies of childhood. Immunol Allergy Clin North Am. (2021) 41(4):527–33. doi: 10.1016/j.iac.2021.07.004
34. Sullivan KE, Puck JM, Notarangelo LD, Fuleihan R, Caulder T, Wang C, et al. USIDNET: a strategy to build a community of clinical immunologists. J Clin Immunol. (2014) 34(4):428–35. doi: 10.1007/s10875-014-0028-1
35. Hansen AT, Söderström A, Jørgensen CS, Larsen CS, Petersen MS, Bernth Jensen JM. Diagnostic vaccination in clinical practice. Front Immunol. (2021) 12:717873. doi: 10.3389/fimmu.2021.717873
36. Koenen MH, Bosma M, Roorda UA, Wopereis FM, Roos A, van der Vries E, et al. A novel method to standardise serum IgA measurements shows an increased prevalence of IgA deficiency in young children with recurrent respiratory tract infections. Clin Transl Immunol. (2021) 10:1–10. doi: 10.1002/cti2.1344
37. Wang N, Shen N, Vyse TJ, Anand V, Gunnarson I, Sturfelt G, et al. Selective IgA deficiency in autoimmune diseases. Mol Med. (2011) 17(11–12):1383–96. doi: 10.2119/molmed.2011.00195
38. Lawrence MG, Borish L. Specific antibody deficiency: pearls and pitfalls for diagnosis. Ann Allergy Asthma Immunol. (2022) 129(5):572–8. doi: 10.1016/j.anai.2022.05.028
39. Seymour B, Miles J, Haeney M. Primary antibody deficiency and diagnostic delay. J Clin Pathol. (2005) 58:546–7. doi: 10.1136/jcp.2004.016204
40. Picard C, Casanova JL, Puel A. Infectious diseases in patients with IRAK-4, MyD88, NEMO, or IκBα deficiency. Clin Microbiol Rev. (2011) 24:490–7. doi: 10.1128/CMR.00001-11
41. Chinn IK, Orange JS. A 2020 update on the use of genetic testing for patients with primary immunodeficiency. Expert Rev Clin Immunol. (2020) 16:897–909. doi: 10.1080/1744666X.2020.1814145
Keywords: parapneumonic effusion, community-acquired pneumonia, pneumococcal conjugate vaccine, immunodeficiency, children
Citation: Rózsai B, Simon D, Berki T, Kiss G and Mosdósi B (2025) Immunological dysfunction of children with severe parapneumonic effusion. Front. Pediatr. 13:1547146. doi: 10.3389/fped.2025.1547146
Received: 17 December 2024; Accepted: 9 June 2025;
Published: 27 June 2025.
Edited by:
Jani Almeida, University of Coimbra, PortugalReviewed by:
Angelo Mazza, Papa Giovanni XXIII Hospital, ItalyMichael James Carter, King's College London, United Kingdom
Copyright: © 2025 Rózsai, Simon, Berki, Kiss and Mosdósi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Barnabás Rózsai, cm96c2FpLmJhcm5hYmFzQHB0ZS5odQ==
†ORCID:
Barnabás Rózsai
orcid.org/0000-0002-8401-5415