 Harvinder Kaur
Harvinder Kaur Anil Kumar Bhalla1,†
Anil Kumar Bhalla1,† Inusha Panigrahi
Inusha Panigrahi- 1Child Growth & Anthropology Unit, Department of Pediatrics, Postgraduate Institute of Medical Education & Research (PGIMER), Chandigarh, India
- 2Genetics & Metabolic Unit, Department of Pediatrics, Postgraduate Institute of Medical Education & Research (PGIMER), Chandigarh, India
This study aimed to construct age- and sex-specific growth percentiles for head circumference (HC) that can be used as a reference for Indian children with Down syndrome (DS). Over 24 years, following a mixed-longitudinal growth research design, 2,327 head circumference measurements were performed on 1,125 (boys: 752, girls: 373) children with DS karyotypically proven as cases of free trisomy 21 who were aged <1 month to 10 years, following a standardized anthropometric technique. A steady increase in the mean head circumference of male and female children with DS was noted. Boys with DS had significantly larger HCs than girls. Our study showed that 12.9% of Down syndrome cases had normal head circumference, 27.2% had small heads, and the majority, 59.9%, had microcephaly. Head circumference percentiles for boys and girls with Down syndrome were constructed for ages <1 month to 10 years. There is a need to monitor the growth of children with Down syndrome using population-specific and specialized growth charts. The age- and sex-specific head circumference growth percentiles presented for Indian children with Down syndrome can be used for growth monitoring and inter-population comparison.
Introduction
A small head (microcephaly) and a broad head (brachycephaly) are universally accepted as diagnostic criteria of Down syndrome (DS). In addition, growth retardation and compromised development of the brain along with several other features (sloping forehead, flat occipital bone, etc.) are frequently observed in these patients. While there have been studies examining the growth of children with DS in terms of body weight and height (1–4), published longitudinal information on the growth of head circumference (HC) is lacking worldwide. In the Indian context, a recent study by Priya et al. (5) and some information based on pilot research (6, 7) has been published.
Because the growth patterns of children with DS differ biologically from those of the normal population, as do the growth patterns of patients with DS in different population groups/races, using growth curves/charts developed for a specific racial/ethnic group may not be appropriate for making precise diagnoses and quantifying the extent of auxological insults experienced by these patients. Given the critical role that early identification of growth deviations plays in managing health outcomes, it is essential to have population-specific growth charts that reflect the unique genetic, environmental, and socioeconomic factors influencing the growth of children in different regions. Early identification of a range of pathologies such as microcephaly, intellectual disability, growth retardation, and delayed neurodevelopment can be best made by using syndrome-specific charts developed for patients belonging to the same population.
This study contributes to clinical practice by providing the first longitudinal, age- and sex-specific growth percentiles for head circumference in Indian children with DS. These data can help pediatricians, genetic counselors, and healthcare providers identify abnormal growth patterns early, allowing timely intervention. Furthermore, it will serve as a reference for assessing how children with DS from northwestern India grow relative to international standards and other ethnic groups, highlighting potential regional disparities that may affect health interventions.
Material and methods
The sample for this serial study conducted over a 24-year period (August 1994–November 2018) consisted of 1,125 (boys: 752, girls: 373) children with Down syndrome aged <1 month to 10 years, who were karyotypically proven as cases of free trisomy 21. Patients with translocations or mosaicism were excluded from the study sample. These children hailed from the northwestern parts of India and were enrolled from the “Genetic Clinic” of the Department of Pediatrics. The clinical and demographic characteristics of the study participants have been published elsewhere (1).
The study protocol was approved by the Institutional Ethics Committee of Postgraduate Institute of Medical Education & Research (PGIMER). Prior to their enrollment, informed consent to participate in this study was obtained from the parents of these children. As the study spanned several years, the authors ensured compliance with ethical standards, ensuring participant rights and maintaining the confidentiality of the data throughout the extended research period. Various safeguards were implemented: informed consent was reaffirmed periodically, all data collected during the study were kept strictly confidential, patient identities were anonymized, and the data were coded to prevent the identification of individual participants.
The head circumference of each child was measured at the Growth Clinic to the nearest 0.1 cm using a standardized anthropometric technique with a non-stretchable fiberglass tape at monthly age intervals (time tolerance ±3 days) during the first year of life, at 6-month age intervals (time tolerance ±15 days) from 1 to 5 years of age, and at yearly intervals (time tolerance ±1 month) thereafter, following a mixed-longitudinal growth research design. The head circumference measurement was taken by a trained anthropometrist, and another person helped to gently restrain uncooperative young children while taking their measurements.
The Kolmogorov–Smirnov test was employed to check the normality of the data gathered from all patients with DS. As our data were normally distributed, the mean and standard deviation (SD) for head circumference at each age among the children with DS were calculated. A total of nine age- and sex-specific percentiles (i.e., 3rd, 5th, 10th, 25th, 50th, 75th, 90th, 95th, and 97th) were obtained for head circumference at each age.
The percentiles were calculated using the formula
where P denotes the percentile, n indicates the number, and N represents the total population count.
An unpaired t-test was applied to quantify the magnitude of sex differences. Statistical analyses were carried out using SPSS version 20 (SPSS Inc., Chicago, IL, USA).
Children with DS with a head circumference of ≤3SDS (standard deviation score) were categorized as having microcephaly, those with a head circumference between ≤2SDS and ≥3SDS as having a small head, and those with a head circumference between −2SDS and +2SDS as having a normal head (8, 9). For the same specified purpose, normal reference data for head circumference from the WHO (10) were used for comparison up to 5 years of age. Beyond 5 years of age, the International and Interracial graphs published by Nellhaus (11) were used. The MedCalc (12) calculator was used to compare the mean values of our children with DS with the mean values of normal children. A p-value <0.05 was considered significant.
Results
A total of 2,327 head circumference measurements were taken from 1,125 children with DS over 24 years. A steady increase in the mean head circumference of both male and female children with DS was found throughout the study period. Except for having a smaller head circumference at 4 months, the boys with Down syndrome had a larger head circumference than the girls, with statistically significant differences (p < 0.05) at most age levels (Table 1). The mean increase in head circumference of the boys with DS (9.8 cm) was greater than that of the girls (8.43 cm) during the first year of life. Although reduced in magnitude, the mean increase was also greater in the male patients with DS (1.92 cm) than in their female counterparts (1.38 cm) during the second year of life. During the third year of life, the increase in head circumference was 1 cm among both male and female subjects with DS. The mean percent increase in HC from <1 month to 10 years was 47.9% (15.5 cm) in the boys and 40.9% (13.6 cm) in the girls.
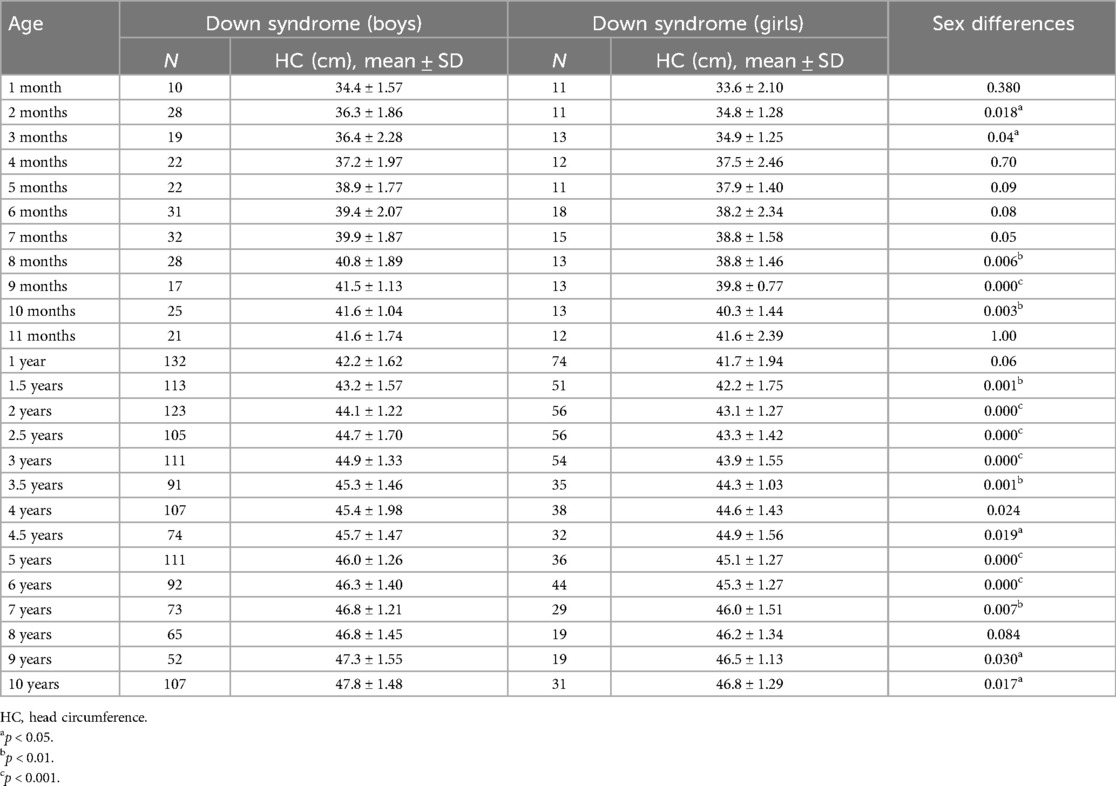
Table 1. Mean (SD) and sex differences for head circumference (cm) in male and female children with Down syndrome.
Compared to their normal WHO Multicentre Growth Reference Study (MGRS) counterparts (10), our children with DS had a significantly (p < 0.001) smaller head circumference up to 5 years of age (Supplementary Table). Because comparative reference data for the head circumference of Indian children with DS are not available beyond 5 years, inter-population comparisons could not be made.
Microcephaly was found in 59.9% (n = 1,394) of our study children, while 27.2% (n = 633) had a small head. Interestingly, a normal head circumference was detected in 12.9% (n = 300) of our children with DS. Head circumference-for-age percentiles are presented in Tables 2, 3.

Table 2. Head circumference-for-age percentiles for boys with Down syndrome.
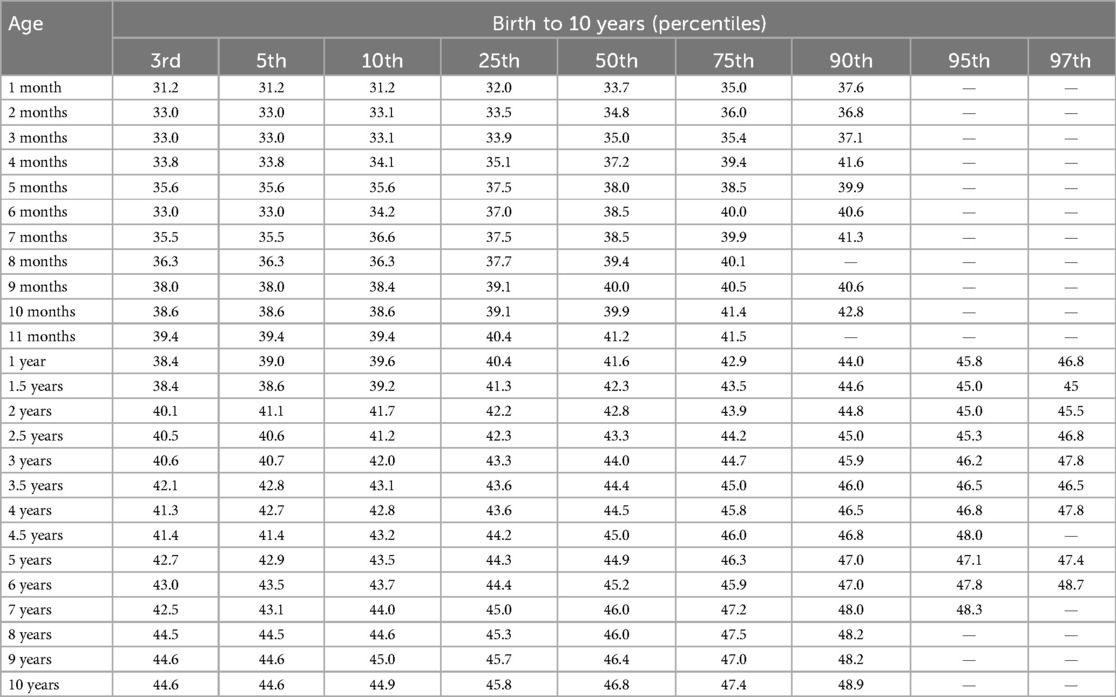
Table 3. Head circumference-for-age percentiles for girls with Down syndrome.
Discussion
This is a single-center prospective study on the growth pattern of head circumference of karyotypically confirmed cases of DS from the northwestern regions of India. The age- and sex-specific percentile growth charts for head circumference presented in this article relate to serial observations made on children with DS from the age of <1 month to 10 years. A steady increase in the mean pattern of growth (50th percentile) of head circumference of the children with DS was recorded during the entire duration of this study. However, the scale of this increase was found to be greater up to the age of 3.5 years, after which it became substantially smaller up to the age of 10 years (Figure 1).
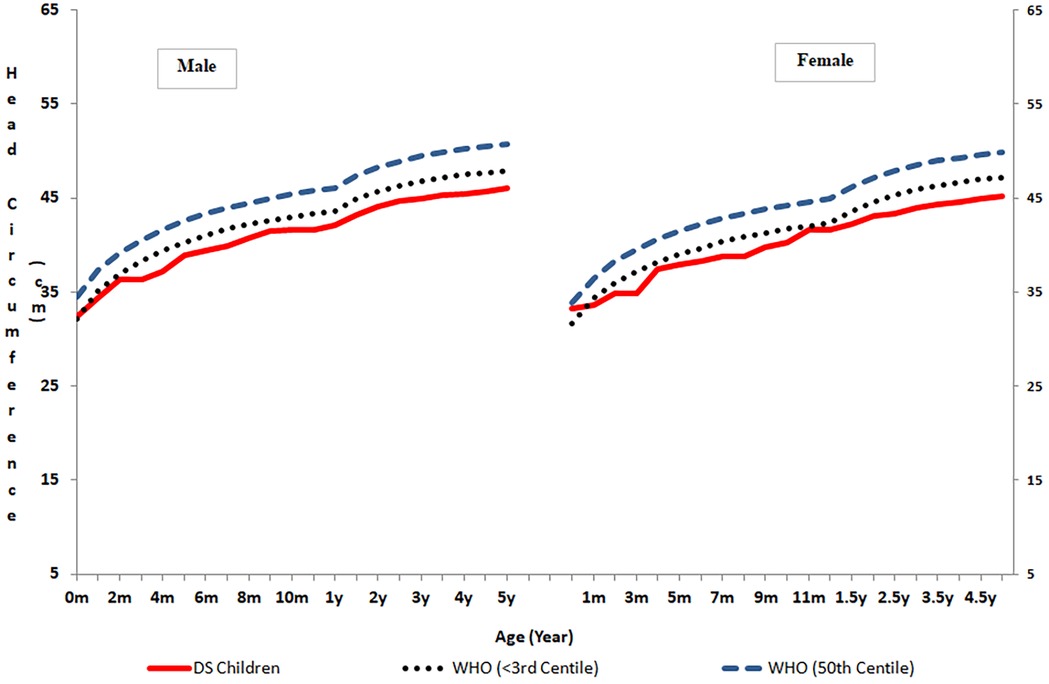
Figure 1. Comparison of head circumference in normal children and children with Down syndrome.
Patients with Down syndrome are characterized by impaired growth, and our results show that the mean head circumference of the children with DS was significantly smaller than that of healthy children. Furthermore, the mean increase in head circumference of the male (9.8 cm) and female (8.43 cm) children with DS during the first year of life substantially lagged behind the expected 12 cm gain in the first year of life (13). Despite experiencing much slower head growth than their healthy peers (10), our children with DS were able to complete 88% of their head growth by the age of 5. Interestingly, ∼13% of our children with Down syndrome had a normal head circumference, and ∼60% had microcephaly. Similar to our findings, normal head circumference in approximately 20% of Down syndrome cases has also been reported (14). However, Palmar et al. (15) observed that a staggering 50% of children with DS between the ages of 0 and 36 months had head circumferences similar to that of the general population range. Remarkably similar to our findings, Priya et al. (5) reported that approximately 25% of Indian children with DS had head circumferences between −2 and −3 SD.
As head circumference is considered a proxy for brain growth, head size, particularly in the early years of life, correlates with cognitive, motor, and adaptive development. The observed differences in head circumference growth in children with DS not only provide valuable insights into their physical development but also have important implications for neurodevelopmental outcomes. Children with Down syndrome with smaller head circumferences are known to exhibit developmental and motor delays (16). Hence, by tracking head circumference along with neurodevelopmental milestones, healthcare providers can better predict potential developmental delays and implement early interventions to support cognitive, motor, and adaptive skills.
Comparison of our data with other studies revealed that in Türkiye(17) and the United States (3), at <1 month to 10 years of age and in Brazil at 0–24 months of age (18), children with DS possessed larger HCs, as the 50th percentile plotted for our children with Down syndrome corresponded with their 10th percentiles. Similarly, the head circumferences of our girls with DS grew to approximately the 10th percentile when compared with the Down syndrome head circumference chart for the United Kingdom and the Republic of Ireland (19). Although small, the head circumferences of our children with DS were close to their Chinese peers (2), as the 50th percentile of our study children was close to their 25th percentile. At 3 years, the mean head circumference of our boys with DS was similar to their Egyptian counterparts (20). Surprisingly, when compared to their South Indian counterparts (6, 7), our children with DS from northwest India had smaller head circumferences. Because the study by Chandrasekhar and Ramachandran (6, 7) was conducted with a small population (n = 60), the discrepancies observed may have been an artifact of the small sample size, obscuring the true picture. The consistently lower placement on the growth curves plotted for the patients with DS in the present study than those of their Western and Chinese counterparts reveals that the growth of head circumference in our patients with DS remains impaired throughout as compared to their peers representing other racial groups. The significant inter-population variability observed in the head circumference growth of children with DS from northwestern India compared to children from other populations may be due to variability in their genetic make-up or availability of better healthcare, socioeconomic and environmental conditions, and sound nutritional and feeding practices. While all the participants in this study were diagnosed with free trisomy 21, there may be genetic diversity among children with DS in other studies. These differences highlight the importance of using population-specific growth charts and exploring the underlying causes of such variation to better understand the growth patterns of children with DS and how they may be influenced by these factors.
This study presents the first comprehensive set of age- and sex-specific longitudinal data on head circumference in children with DS of northwestern Indian origin. These growth percentiles are based on high-quality precision data acquired by a skilled anthropometrist and technician using a standardized anthropometric approach in karyotypically proven trisomy 21 cases with a known date of birth. The data provided can be used to monitor and assess the impact of different need-based interventions on the growth of Indian children with DS from northwest India. However, the findings may not reflect the head growth of children with DS from other population groups due to population-specific variability.
Notably, the study relies on international and interracial growth charts for children older than 5 years (11). Ideally, more current and population-specific reference data should have been utilized, as there is a significant gap in the literature regarding Indian-specific reference data for this age range. In addition, the study does not account for unmeasured confounders such as socioeconomic status, parental education, and access to healthcare. While the study excluded children with translocations or mosaicism, it did not consider other health conditions, such as concurrent cardiac or gastrointestinal disorders, that are often observed in children with DS.
Future research should aim to validate these findings in a larger, multi-center study including children from diverse regions of India, ensuring greater representativeness and broader applicability of the growth percentiles. This would help identify whether the observed trends hold true across different population groups and contribute to the development of national growth charts specific to Indian children with DS. In addition, future studies should consider integrating neurodevelopmental assessments to better understand the relationship between head circumference growth and cognitive or developmental outcomes of children with Down syndrome across diverse populations.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors upon reasonable request. Requests should be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Institutional Ethics Committee of Postgraduate Institute of Medical Education & Research (PGIMER), Chandigarh, India (71/20-Edu/94/10188-226, dated: 24.04.1995). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
HK: Conceptualization, Data curation, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing. AB: Conceptualization, Methodology, Project administration, Supervision, Writing – review & editing. IP: Data curation, Investigation, Supervision, Writing – review & editing. RK: Data curation, Project administration, Supervision, Writing – review & editing. NS: Formal analysis, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2025.1563501/full#supplementary-material
References
1. Bhalla AK, Kaur H, Kaur R, Panigrahi I. Growth charts for weight and height of Indian children with Down syndrome. Am J Med Genet A. (2024) 194(7):e63571. doi: 10.1002/ajmg.a.63571
2. Su X, Lau TF, Yu CM, Chow CB, Lee LP, Man But BW, et al. Growth charts for Chinese Down syndrome children from birth to 14 years. Arch Dis Child. (2014) 99(9):824–9. doi: 10.1136/archdischild-2013-304494
3. Zemel BS, Pipan M, Stallings VA, Hall W, Schadt K, Freedman DS, et al. Growth charts for children with Down syndrome in the United States. Pediatrics. (2015) 136(5):e1204–11. doi: 10.1542/peds.2015-1652
4. Aburawi EH, Nagelkerke N, Deeb A, Abdulla S, Abdulrazzaq YM. National growth charts for United Arab Emirates children with Down syndrome from birth to 15 years of age. J Epidemiol. (2015) 25(1):20–9. doi: 10.2188/jea.JE20130081
5. Priya MP, Gupta N, Nagori A, Lodha R, Jain V, Pandey RM, et al. Physical growth and its determinants in Indian children with Down syndrome, from 3 months to 5 years of age. Indian J Pediatr. (2022) 89(2):141–7. doi: 10.1007/s12098-021-03864-9
6. Chandrasekhar P, Ramachandran S. Growth chart of Indian girls with Down syndrome from birth to three years-a pilot study. J Down Syndr Chr Abnorm. (2018) 4:130. doi: 10.4172/2472-1115.1000130
7. Chandrasekhar P, Ramachandran S. Growth charts for Indian boys (0–36 months) with Down syndrome: a pilot study. Int J Contemp Pediatr. (2018) 5(6):2156–60. doi: 10.18203/2349-3291.ijcp20184272
8. Woods CG. Human microcephaly. Curr Opin Neurobiol. (2004) 14(1):112–7. doi: 10.1016/j.conb.2004.01.003
9. Leviton A, Holmes LB, Allred EN, Vargas J. Methodologic issues in epidemiologic studies of congenital microcephaly. Early Hum Dev. (2002) 69:91–105. doi: 10.1016/S0378-3782(02)00065-8
10. WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards: Head Circumference-for-Age, Arm Circumference-for-Age, Triceps Skinfold-for-Age and Subscapular Skinfold-for-Age: Methods and Development. Geneva: World Health Organization (2007).
11. Nellhaus G. Head circumference from birth to eighteen years: practical composite international and interracial graphs. Pediatrics. (1968) 41:106–14. doi: 10.1542/peds.41.1.106
12. MedCalc Software. MedCalc Statistical Software Version 20.0. Ostend: MedCalc Software Ltd. (2025). Available at: https://www.medcalc.org (Accessed December 28, 2024).
13. Jones SG, Samanta D. Macrocephaly. In: StatPearls. Treasure Island, FL: Stat Pearls Publishing (2023).
14. Wisniewski KE. Down syndrome children often have brain with maturation delay, retardation of growth and cortical dysgenesis. Am J Med Genet. (1990) 7:274–28. doi: 10.1002/ajmg.1320370755
15. Palmar CG, Cronk C, Pueschel SM, Wisniewski KE, Laxova R, Crocker AC, et al. Head circumference of children with Down syndrome (0–36 months). Am J Med Genet. (1992) 42(1):61–7. doi: 10.1002/ajmg.1320420114
16. Malak R, Kostiukow A, Krawczyk-Wasielewska A, Mojs E, Samborski W. Delays in motor development in children with Down syndrome. Med Sci Monit. (2015) 21:1904–10. doi: 10.12659/MSM.893377
17. Tüysüz B, Göknar NT, Öztürk B. Growth charts of Turkish children with Down syndrome. Am J Med Genet Part A. (2012) 158A:2656–64. doi: 10.1002/ajmg.a.35710
18. Bertapelli F, Agiovlasitis S, Machado MR, do Val Roso R, Guerra-Junior G. Growth charts for Brazilian children with Down syndrome: birth to 20 years of age. J Epidemiol. (2017) 27(6):265–73. doi: 10.1016/j.je.2016.06.009
19. Styles ME, Cole TJ, Dennis J, Preece MA. New cross sectional stature, weight and head circumference references of Down’s syndrome in the UK and Republic of Ireland. Arch Dis Child. (2002) 87:104–8. doi: 10.1136/adc.87.2.104
Keywords: percentiles, trisomy 21, microcephaly, small head, northwest India
Citation: Kaur H, Bhalla AK, Panigrahi I, Kaur R and Sudhera N (2025) Head circumference percentiles in Indian children with Down syndrome. Front. Pediatr. 13:1563501. doi: 10.3389/fped.2025.1563501
Received: 20 January 2025; Accepted: 24 March 2025;
Published: 28 April 2025.
Edited by:
Deborah Sokol, Indiana University, United StatesReviewed by:
G. P. Prashanth, National University of Science and Technology, OmanKayleigh Avery, Indiana University Bloomington, United States
Copyright: © 2025 Kaur, Bhalla, Panigrahi, Kaur and Sudhera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Harvinder Kaur, aGFydmluZGVya2F1cjMxNUBnbWFpbC5jb20=; Inusha Panigrahi, aW51cGFuQHlhaG9vLmNvbQ==
†ORCID:
Harvinder Kaur
orcid.org/0000-0003-1991-0584
Anil Kumar Bhalla
orcid.org/0000-0003-4998-9385
Inusha Panigrahi
orcid.org/0000-0001-7375-9892
Rupinder Kaur
orcid.org/0009-0001-8211-5025
Neha Sudhera
orcid.org/0000-0002-6422-5052