 Saeed Y. Eleyyan
Saeed Y. Eleyyan Bothyna B. ELssyed Etewa1
Bothyna B. ELssyed Etewa1 Abdel Hamid El Bilbeisi
Abdel Hamid El Bilbeisi- 1Department of Pediatric Nursing, School of Nursing, University of Albutana, Rufaa, Sudan
- 2Department of Clinical Nutrition, Faculty of Applied Medical Sciences, Al Azhar University of Gaza, Gaza Strip, Palestine
- 3Department of Nutrition, School of Medicine and Health Sciences, University of Palestine, Gaza Strip, Palestine
Background: This study aimed to assess the quality of pediatric care in Gaza Strip hospitals using the World Health Organization (WHO) integrated tool.
Method: A cross-sectional study was conducted in 2023 before Gaza war, with a census sample of healthcare providers at three major governmental pediatric hospitals: Al-Nasr, Al-Durra, and Al-Rantisi. Data were collected through an interview-based questionnaire, and statistical analysis was performed using SPSS version 26.
Results: A total of 336 participants were included (59.5% male, 40.5% female). Of these, 13% were pediatricians, 16% general doctors, 1% pediatric nurses, and 70% were general nurses. The overall total scores for healthcare providers' responses to the eight WHO quality standards was 29.5%; in addition, it was varied across hospitals: Al-Nasr (29.1%), EL-Rantisi (31.9%), and Al-Durra (28.4%). The lowest score was for Standard VIII (8.3%), related to the physical environment, while the highest score was for Standard V (70.9%) related to rights of children. Statistically significant differences were found for standards I, II, IV, VII, and VIII between the hospitals (P-values < 0.05 for all). Additionally, the health care providers aged 31–35 years were three times more likely to have better overall total scores compared to other age groups [Adjusted Odds Ratio = 3.014, 95% Confidence Interval = (1.255–7.241), P value = 0.014].
Conclusion: The study revealed suboptimal pediatric care quality in Gaza Strip hospitals. The lowest scores for the healthcare providers, was 8.3% for standard (VIII), which pertains to the physical environment, emphasizing the need for infrastructural improvements, while the highest scores 70.9% was for standard (V) shows the providers respectful view and acts for children rights without discrimination. There is a need to prioritize upgrading the physical environment and ensuring the availability of essential resources, such as water, sanitation, and medical supplies, to enhance the overall quality of care for children in these hospitals. This study provides valuable insights for policymakers and healthcare professionals working to improve pediatric care in Gaza.
1 Introduction
The quality of pediatric care is a critical determinant of health outcomes for children, influencing both their short-term recovery and long-term well-being (1). Globally, pediatric care faces numerous challenges, including resource limitations, workforce shortages, and gaps in specialized care (2). In conflict zones, such as the Gaza Strip, these challenges are magnified due to the ongoing socio-political instability and limited access to health resources (3). Quality healthcare for children in the Gaza Strip is essential, not only for addressing immediate health needs but also for promoting sustainable development in the region (4). The World Health Organization (WHO) has developed an integrated tool for improving the quality of pediatric care in health facilities, designed to assist healthcare providers in delivering comprehensive, evidence-based care. This tool assesses various domains of care, including evidence-based illness management, health information systems, referral efficiency, effective communication with families, staff competency, and the adequacy of the physical environment (5).
In Gaza, pediatric healthcare services are provided by several governmental hospitals, including Al-Nasr Pediatric Hospital, Al-Durra Pediatric Hospital, and Al-Rantisi Pediatric Hospital. These institutions serve a crucial role in managing childhood illnesses and providing care to children up to 12 years old (6). Despite the critical nature of their services, little is known about the overall quality of pediatric care in these facilities. To the best of our knowledge, the healthcare providers' perspectives on the quality of care they deliver remain underexplored, particularly within the context of the WHO's integrated tool for pediatric care. Therefore, assessing healthcare providers' perceptions of quality care in the Gaza Strip is crucial for identifying strengths, gaps, and areas for improvement within these hospitals. Previous studies on pediatric care in the Middle East highlight several factors influencing the quality of care, including access to trained personnel, availability of medical supplies, and the physical infrastructure of healthcare facilities (7, 8). For instance, a study by Sami et al. (9) examined the challenges faced by pediatric hospitals in conflict-affected regions, noting that limited resources and overcrowded facilities were major barriers to providing high-quality care. Similarly, a study by Leary et al. (10) found that inadequate training for healthcare providers and insufficient pediatric-specific knowledge negatively impacted the quality of care in public hospitals.
The WHO tool is an essential resource for improving pediatric care, as it provides a comprehensive framework for evaluating the quality of care across different domains, including the physical environment, communication with families, and the competence of healthcare providers (5). However, the application of this tool in conflict zones, such as the Gaza Strip, requires particular attention to contextual factors, including ongoing shortages in medical staff, limited access to resources, and the political climate. The purpose of this study is to evaluate the quality of pediatric care in the Gaza Strip through the lens of healthcare providers' perspectives, using the WHO integrated tool as a framework. By assessing the quality of care provided in pediatric hospitals, this study aims to identify strengths and areas for improvement in these institutions. Furthermore, it seeks to understand the challenges faced by healthcare providers in delivering high-quality care under difficult circumstances. Ultimately, the findings of this research will serve as a valuable resource for policymakers, healthcare professionals, and planners, providing insights into the necessary steps to improve pediatric care in the region.
2 Materials and methods
2.1 Study design
This research is an observational, descriptive, and analytical cross-sectional study designed to assess healthcare providers' perspectives on the quality of pediatric care in Gaza hospitals, focusing on the integration of evidence-based practices, illness management, health information systems, and referral efficiency.
2.2 Study location and period
The current study was conducted in 2023 before Gaza war, in three major governmental pediatric hospitals in the Gaza Strip: Al-Nasr Pediatric Hospital, Al-Durra Pediatric Hospital, and Al-Rantisi Specialized Pediatric Hospital.
(1) Al-Nasr Pediatric Hospital: Established in 1962, it is the oldest pediatric hospital in Gaza, providing secondary healthcare services for children up to 12 years old. The hospital has 292 staff members and 121 beds, offering emergency, pediatric, intensive care, and neonatal services; (2) Al-Durra Pediatric Hospital: Opened in 2000, this hospital provides emergency, admission, and specialized services for children. It has 140 staff and 87 beds, with a radiology department managing 1,000–1,800 referrals annually; and (3) EL-Rantisi Specialized Pediatric Hospital: Founded in 2003 and fully operational by 2006, it is a tertiary facility with 287 staff members. The hospital offers 56 beds for children and 30 for adults across 15 specialized departments, including radiology, handling about 7,800 radiology referrals annually (6).
2.3 Study population
The study included all healthcare providers, regardless of gender, working in the selected hospitals in the Gaza Strip, including pediatricians, general doctors, pediatric nurses, and general nurses, who met the inclusion criteria and were present during the study period. Healthcare providers employed for less than six months, volunteers, and those who chose not to participate were excluded from the study.
2.4 Sample size and sampling technique
All participants working in the three selected hospitals at the time of data collection and meeting the inclusion criteria were included using a census sampling method. A total of 402 healthcare providers (pediatricians, general doctors, pediatric nurses, and general nurses) were eligible, with 336 participating, resulting in a 94% response rate. Sixty-six healthcare providers either refused to participate or were absent during the data collection period.
2.5 Data collection
2.5.1 Interview-based questionnaire
A structured, pre-tested, and validated questionnaire was employed to gather data from each participant. The survey consisted of two sections:
2.5.1.1 Assessment of participant characteristics
Data including age, gender, job role, qualifications, specialized pediatric studies, pediatric training courses, years of experience, and training duration, among others, were collected using an interview-based questionnaire.
2.5.1.2 Assessment of the quality of care
The WHO integrated tool, “Standards for Improving the Quality of Care for Children in Health Facilities” was used to assess the quality of care provided to children in pediatrics hospitals in the Gaza Strip. The WHO integrated tool is structured into eight domains that focus on ensuring comprehensive, high-quality care for children. These include providing evidence-based care and management of illness according to WHO guidelines, ensuring effective health information systems for data collection and analysis, and facilitating timely referrals for conditions beyond available resources. Effective communication with children and their families is emphasized, ensuring their meaningful participation and respecting their needs and preferences. The tool highlights the importance of safeguarding children's rights, offering educational, emotional, and psychosocial support tailored to their needs. It also stresses the need for competent, motivated staff to provide consistent care, as well as maintaining a child-friendly physical environment in healthcare facilities, equipped with adequate resources like water, sanitation, and medical supplies for routine care (5).
2.5.2 Translation and validation of the questionnaire
The translation of the questionnaire followed a cross-cultural adaptation process, as outlined in established guidelines (11). A five-step procedure was employed: (1) forward translation into Arabic by two native Arabic-speaking translators, (2) back-translation into English by two native English-speaking translators, (3) review by an expert committee, (4) pre-testing, and (5) finalization of the Arabic version.
Face and content validity of the final Arabic draft were independently assessed by a panel of eight experts, including researchers, academics, healthcare professionals, a head nurse, and pediatric doctors. The Content Validity Index (CVI) was calculated to evaluate the relevance of the questionnaire items (12), with all items receiving scores above 0.82, indicating strong relevance. Minor revisions in wording and structure were made following a consensus among the primary author (SYE), two pediatricians, and a head nurse. Subsequently, the questionnaire was piloted among 20 eligible healthcare professionals. The pilot study demonstrated good internal consistency, with a Cronbach's alpha of 0.84.
2.6 Pilot study
A pilot study was carried out with 20 participants to evaluate the questionnaire and data collection methods. Feedback from the pilot study led to adjustments being made to the questionnaire to improve clarity and accuracy for the main study.
2.7 Data analysis
Statistical analysis was conducted using SPSS version 26. The data analysis process included defining variables, data entry, cleaning, and analysis. Continuous variables were expressed as means ± SD, while categorical variables were presented as percentages. The Chi-square test was applied to assess differences between categorical variables. Adjusted Odds Ratio and 95% Confidence Interval (CI) was calculated using multinomial logistic regression analysis. A p-value of less than 0.05 was considered statistically significant. The total scores of the health care provider's responses (agree and strongly agree) to the eight standards of quality of care was calculated based on the average of eight domains, and was calculated for each domain separately for the three hospitals in Gaza Strip.
3 Results
This study was conducted in the pediatric departments of three major hospitals in the Gaza Strip under the Palestinian Ministry of Health: Al-Nasr Pediatric Hospital, Al-Durra Pediatric Hospital, and Al-Rantisi Pediatric Hospital, which provide care for children up to 12 years old. The study included a total of 336 participants, with 59.5% males and 40.5% females, with an average age of 36.20 ± 8.73 years. The majority (71%) were nurses, while only 0.6% specialized as pediatric nurses. About 64.6% held a bachelor's degree, with significant differences noted between job classification and qualifications across the hospitals (P-value = 0.003). Most participants (83.3%) had not completed specialized pediatric studies, although 58.3% had attended pediatric care training courses. Furthermore, 23.2% had less than five years of experience, with an average of 12.6 ± 5.7 years of total work experience and 9 ± 4.8 years specifically in pediatric care. The average duration of training was 10.3 ± 13 weeks. Statistically significant differences were observed in both specialized studies in pediatric care and training duration across the hospitals (P-value = 0.002 and 0.020, respectively) (Table 1).
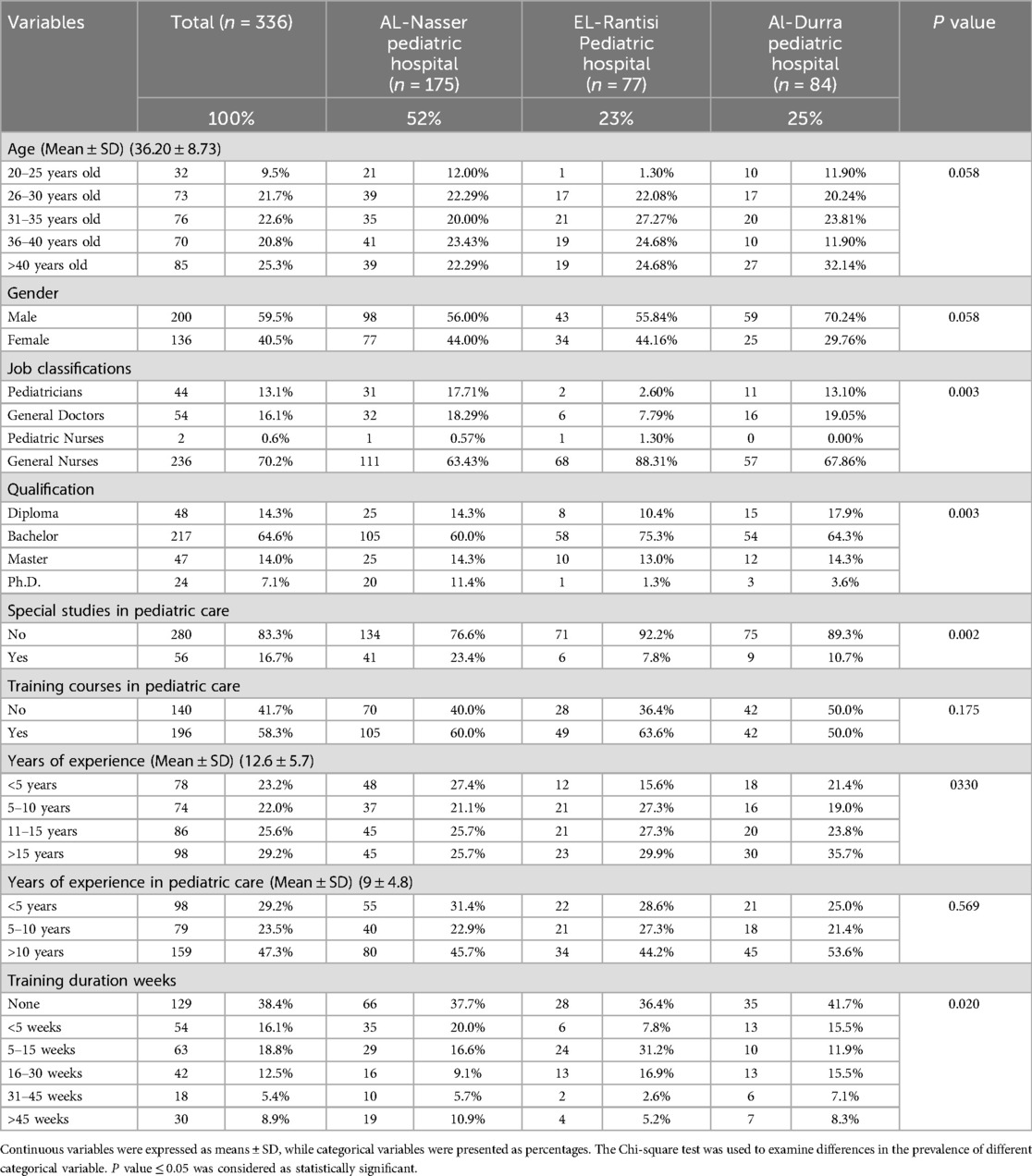
Table 1. Characteristics of the study participants by hospitals.
Table 2 presents the findings on the healthcare providers' adherence to the WHO guidelines for pediatric care across eight standards. For Standard I (“Evidence-based care and illness management”), 66.7% of healthcare providers met the guidelines, with a significant difference across hospitals (P = 0.005). For Standard II (“Health information system ensuring timely data collection and analysis”), 63.7% of providers were compliant, with significant variation between hospitals (P = 0.002). Standard III (“Appropriate referrals for unmanageable conditions”) showed 65.2% adherence, but no significant hospital differences (P = 0.208). For Standard IV (“Effective communication with children and families”), 69.3% met the criteria, with a significant difference by hospital (P = 0.008). Standard V (“Respecting and fulfilling children's rights”) had 70.9% compliance, but no significant variation by hospital (P = 0.547). Standard VI (“Protecting children's rights”) showed 64.9% adherence, with no significant differences (P = 0.421). Standard VII (“Competent, motivated, empathetic staff”) had 64.6% compliance, with significant hospital differences (P = 0.034). Lastly, Standard VIII (“Child-friendly physical environment and necessary resources”) had the lowest adherence at 8.3%, with significant variation by hospital (P = 0.001).
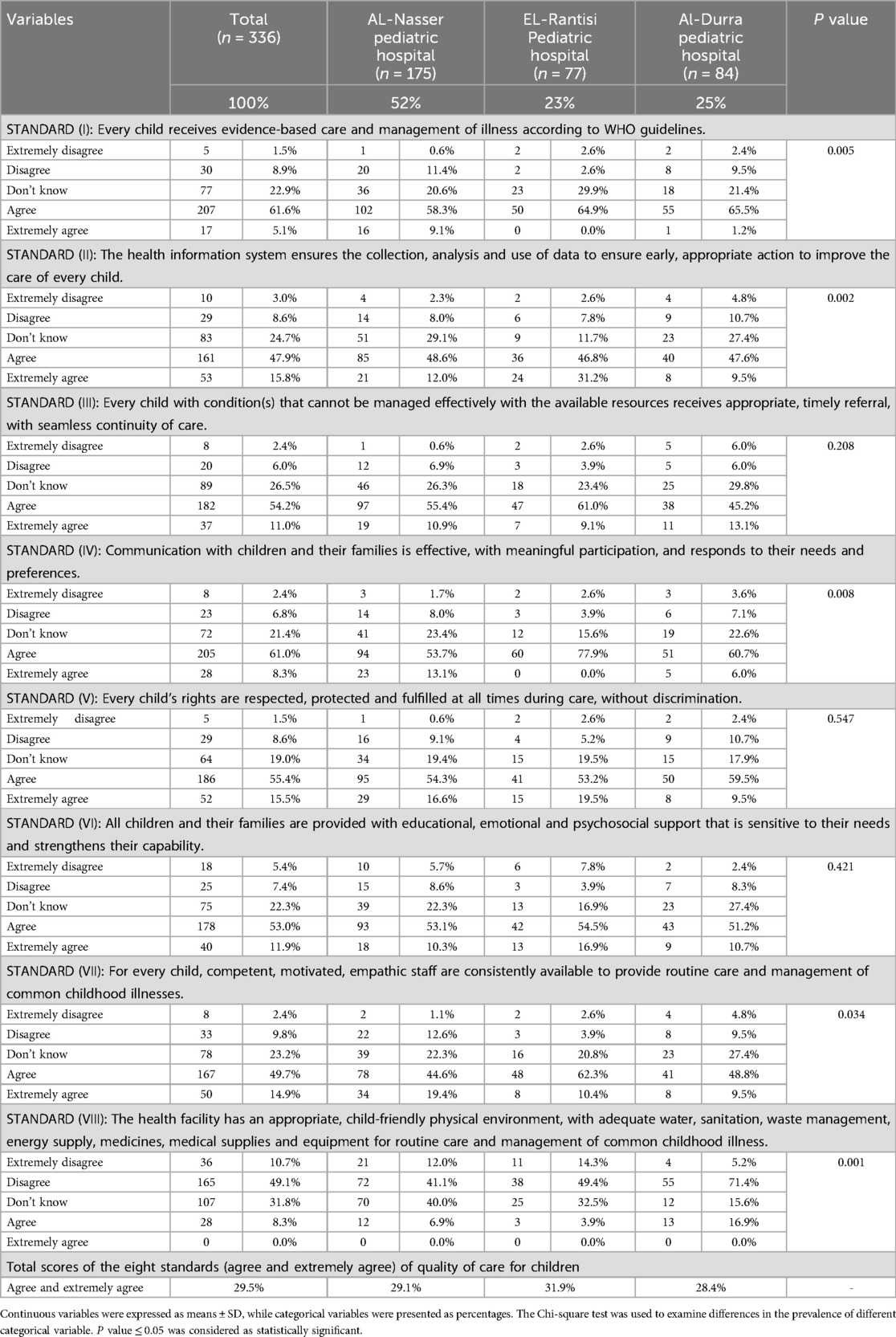
Table 2. The health care provider's responses to the eight standards of quality of care for children at the three main pediatric hospitals in the Gaza Strip.
Overall, the total scores of healthcare providers who agreed or strongly agreed with the standards were 29.5%; in addition, it was 29.1% for AL-Nasser Pediatric Hospital, 31.9% for EL-Rantisi Pediatric Hospital, and 28.4% for AL-Durra Pediatric Hospital.
Figure 1 shows that the lowest percentage of healthcare providers (agree and strongly agree) for the included standards was for standard (VIII) at 8.3%, while the highest percentage was for standard (V) at 70.9%. The distribution of the total scores for the healthcare providers (agree and strongly agree) across the WHO quality of pediatric care integrated tool standards was as follows: 8.3% for standard (VIII), 63.7% for standard (II), 64.6% for standard (VII), 64.9% for standard (VI), 65.2% for standard (III), 66.7% for standard (I), 69.3% for standard (IV), and 70.9% for standard (V), all as confirmed by the study participants.
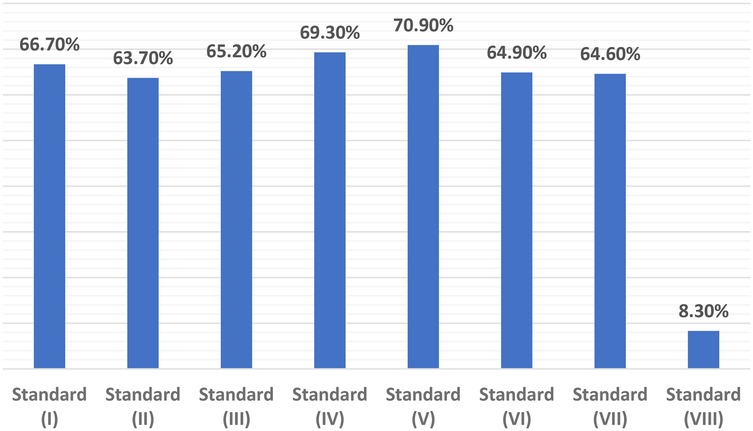
Figure 1. The distribution of the total scores for the healthcare providers (agree and strongly agree) for the included standards of the WHO quality of pediatric care integrated tool.
Table 3 presents the association between the overall total scores of health care providers' responses to the eight standards of quality care for children and the characteristics of the study participants. The findings revealed that health care providers aged 31–35 years were three times more likely to have better overall total scores compared to other age groups [Adjusted Odds Ratio = 3.014, 95% Confidence Interval = (1.255–7.241), P value = 0.014]. No significant associations were observed with any of the other variables.
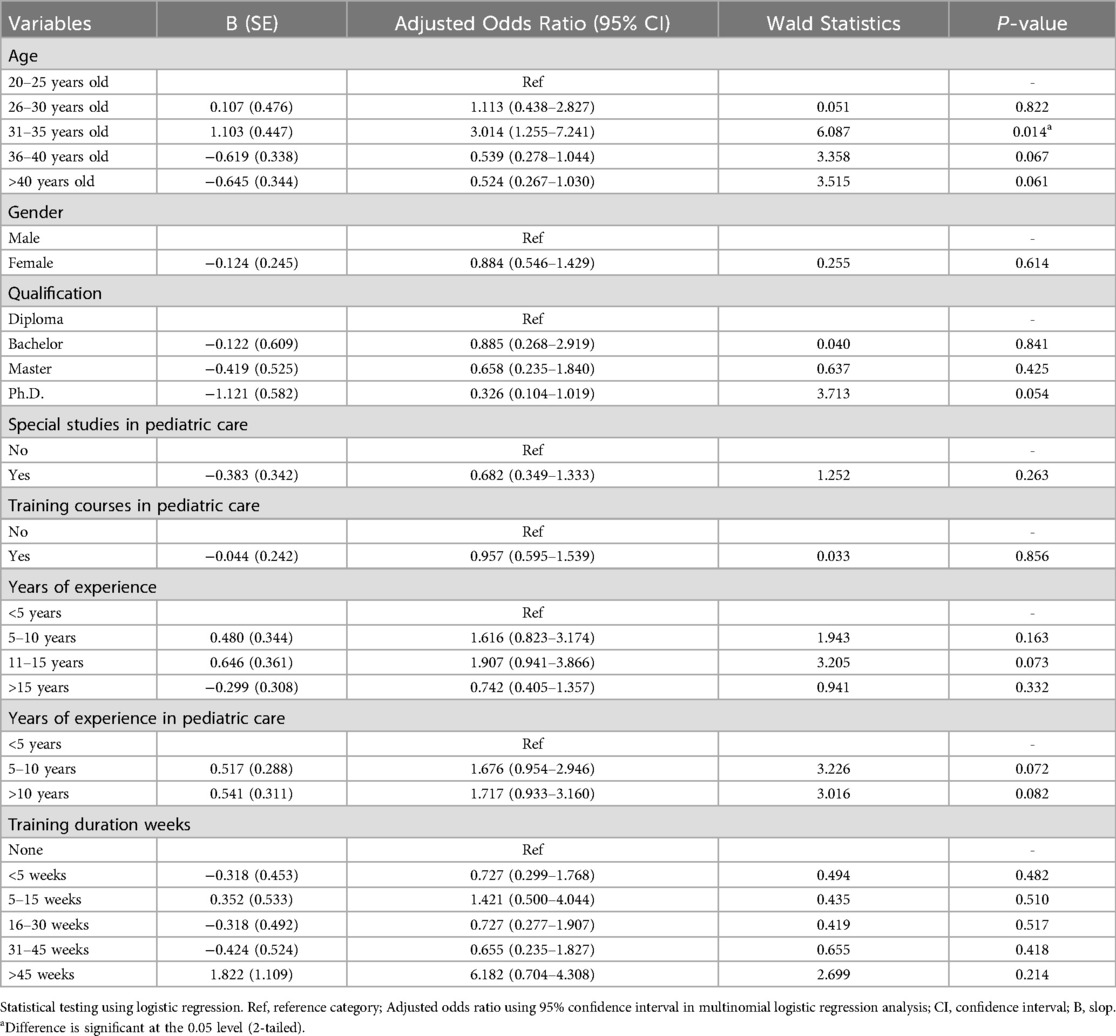
Table 3. The association between the overall total scores of the health care provider's responses to the eight standards of quality of care for children with the characteristics of the study participants.
5 Discussion
The findings of this study provide valuable insights into the quality of pediatric care in the Gaza Strip, specifically in the three major governmental pediatric hospitals: Al-Nasr Pediatric Hospital, Al-Durra Pediatric Hospital, and Al-Rantisi Pediatric Hospital. Using the WHO integrated tool for assessing the quality of care, the results revealed suboptimal levels of healthcare provision, with the lowest scores noted for certain standards, particularly in the physical environment of the healthcare facilities. These results suggest a need for systemic improvements to ensure the quality of pediatric care, in line with WHO guidelines, which is essential for improving health outcomes for children.
Several studies have examined the quality of pediatric care in different regions, including resource-limited settings. A previous study found that healthcare facilities often struggled with providing high-quality care due to inadequate resources, poor physical infrastructure, and limited staff training, which are similar challenges identified in our study (13). Likewise, another study on the quality of pediatric care in public hospitals also revealed suboptimal performance in standards related to facility infrastructure, including water, sanitation, and waste management, similar to our findings regarding standard VIII (14). This emphasizes the universal need for improvements in physical infrastructure to provide an appropriate child-friendly environment.
In contrast, studies in more developed healthcare systems, such as those in Europe, show higher adherence to WHO standards, especially in areas like effective health information systems, timely referrals, and evidence-based care (15–17). These findings suggest that while the Gaza Strip faces significant challenges, particularly in terms of healthcare infrastructure, there are still areas where significant improvements can be made, especially by adopting strategies from successful healthcare models in developed countries.
For standard VIII: Physical environment, the results of this study highlight the stark need for improvement in the physical environment of pediatric hospitals. Only 8.3% of healthcare providers at the three hospitals agreed or strongly agreed with the statements related to having an appropriate, child-friendly environment. This is one of the lowest scores in the study, indicating that infrastructure challenges are a significant barrier to quality pediatric care. The lack of adequate water, sanitation, waste management, energy supply, medicines, and medical supplies not only affects day-to-day operations but also poses significant risks to patient safety and care quality. This is consistent with findings from other studies conducted in conflict zones or low-resource settings, where physical infrastructure issues are often a key limitation (18, 19).
For standard V: Rights of children, while the physical environment remains a challenge, the study found a relatively higher score for Standard V (70.9%), indicating that healthcare providers were relatively confident that children's rights were respected, protected, and fulfilled during care. This could be a result of training programs or policies that aim to ensure children's rights are upheld despite the challenging conditions. Nevertheless, while healthcare providers may have knowledge of child rights, the implementation of these rights in practice, particularly in the context of resource scarcity, remains a complex issue. A recent study in Palestine also emphasized the importance of children's rights within the healthcare setting, noting that while policy frameworks exist, challenges persist in their operationalization (20).
For standard II: Health information systems, the study showed that 63.7% of healthcare providers reported having adequate health information systems in place. This finding is consistent with research conducted in similar settings, where health information systems were found to be an important factor in ensuring timely and appropriate care (21). However, despite the relatively positive response regarding the use of health information systems, the differences observed between hospitals in the implementation of these systems underscore the variability in data management practices, which could impact decision-making processes and the overall quality of care.
For standard I: Evidence-based care, in terms of evidence-based care, 66.7% of participants reported adherence to WHO guidelines for illness management. While this figure is relatively high compared to other standards, it still reflects the need for ongoing training and the integration of evidence-based practices into routine pediatric care. Evidence from a similar study in Jordan (22) suggests that despite the presence of evidence-based guidelines, healthcare providers may face challenges in consistent implementation due to time constraints, resource limitations, and other external factors.
Finally, the findings of this study revealed that health care providers aged 31–35 years were significantly more likely to achieve higher overall total scores in their responses to the eight standards of quality care for children. One possible explanation is that this age group may be more actively engaged in continuous education, familiar with updated guidelines, and still adaptable to evolving best practices. In contrast, younger providers may lack sufficient clinical experience, while older providers may rely more heavily on past practices. However, it is also important to consider contextual factors such as institutional support, workload, and access to training opportunities, which may vary across settings.
6 Strength and limitations
The study's strengths include a comprehensive assessment of pediatric care quality in Gaza hospitals, a large sample size with a 94% response rate, and the use of standardized WHO tools for data collection. However, its limitations include the cross-sectional design, limiting the ability to assess trends or causal relationships, potential response bias, and limited generalizability to smaller or private healthcare facilities. Additionally, the study primarily focused on internal factors without fully exploring the external influences, such as political instability or external healthcare support.
7 Conclusion
This study highlights the gaps in the quality of pediatric care in the Gaza Strip, as perceived by healthcare providers, particularly in the domains of child-friendly environments, evidence-based care, and healthcare infrastructure. Despite the challenges, healthcare providers are committed to adhering to the WHO standards where feasible. It is imperative for stakeholders, including the Ministry of Health, international health organizations, and local policymakers, to focus on improving hospital infrastructure, ensuring better resource allocation, and enhancing healthcare providers' training to address the deficiencies highlighted in this study. The findings emphasize the need for a comprehensive approach to improving pediatric care, focusing on both the physical environment and the provision of adequate resources, alongside strengthening evidence-based practices and data-driven decision-making processes. The results serve as a crucial resource for future health policy and strategy development in the Gaza Strip.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by The study protocol received approval from the Palestinian Health Research Council (Helsinki Committee approval No. PHRC/HC/1202/22). In addition, written informed consent was obtained from all participants. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SE: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Writing – original draft, Writing – review & editing. BE: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Writing – original draft, Writing – review & editing. FA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Writing – original draft, Writing – review & editing. AE: Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors wish to thank and appreciate the study participants and their parents for their significant participation in the study.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Long DA, Fink EL. Transitions from short to long-term outcomes in pediatric critical care: considerations for clinical practice. Transl Pediatr. (2021) 10(10):2858. doi: 10.21037/tp-21-61
2. Berbenyuk A, Alameeri A, Ismail AB, Zary N, Sultan MA. Empowering primary care physicians in child and adolescent psychiatry: a needs assessment on collaborative care in Dubai. Front Med. (2024) 11:1456212. doi: 10.3389/fmed.2024.1456212
3. LaGore A, Kridli S, Piscotty R. Contraceptive use in the Gaza Strip: a systematic review. J Nurs Educ Pract. (2024) 14(11):e1006–13. doi: 10.5430/jnep.v14n11p27
4. Alkhaldi M, Akilan B, Hoteit M, Elhadidy M, Morrison S. Suboptimal attainment of global goals of human rights, universal health coverage, and sustainable development goals in Gaza during 2023–2024. Risk Manag Healthc Policy. (2024) 17:3207–16. doi: 10.2147/RMHP.S488944
5. Duke T. New WHO standards for improving the quality of healthcare for children and adolescents. Arch Dis Child. (2018) 103(7):625–7. doi: 10.1136/archdischild-2018-315423
6. El Aila NA, Al Laham NA, Doijad SP, Imirzalioglu C, Mraheil MA. First report of carbapenems encoding multidrug-resistant gram-negative bacteria from a pediatric hospital in Gaza Strip, Palestine. BMC Microbiol. (2024) 24(1):393. doi: 10.1186/s12866-024-03550-8
7. Dawkins B, Renwick C, Ensor T, Shinkins B, Jayne D, Meads D. What factors affect patients’ ability to access healthcare? An overview of systematic reviews. Trop Med Int Health. (2021) 26(10):1177–88. doi: 10.1111/tmi.13651
8. Mugo NS, Dibley MJ, Damundu EY, Alam A. Barriers faced by the health workers to deliver maternal care services and their perceptions of the factors preventing their clients from receiving the services: a qualitative study in South Sudan. Matern Child Health J. (2018) 22:1598–606. doi: 10.1007/s10995-018-2555-5
9. Sami S, Mayai A, Sheehy G, Lightman N, Boerma T, Wild H, et al. Maternal and child health service delivery in conflict-affected settings: a case study example from upper Nile and unity states, South Sudan. Conflict Health. (2020) 14:1–12. doi: 10.1186/s13031-020-00272-2
10. Leary JC, Walsh KE, Morin RA, Schainker EG, Leyenaar JK. Quality and safety of pediatric inpatient care in community hospitals: a scoping review. J Hosp Med. (2019) 14(11):694–703. doi: 10.12788/jhm.3268
11. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. (2000) 25(24):3186–91. doi: 10.1097/00007632-200012150-00014
12. Lynn MR. Determination and quantification of content validity. Nurs Res. (1986) 35(6):382–6. doi: 10.1097/00006199-198611000-00017
13. Nesengani TV, Downing C, ten Ham-Baloyi W. Barriers to effective patient care as experienced by nurses in primary healthcare clinics in African countries: a systematic review of qualitative studies. BMC Nurs. (2025) 24(1):232. doi: 10.1186/s12912-025-02877-5
14. Maina M, Tosas-Auguet O, McKnight J, Zosi M, Kimemia G, Mwaniki P, et al. Evaluating the foundations that help avert antimicrobial resistance: performance of essential water sanitation and hygiene functions in hospitals and requirements for action in Kenya. PLoS One. (2019) 14(10):e0222922. doi: 10.1371/journal.pone.0222922
15. Legido-Quigley H. Assuring the Quality of Health Care in the European Union: A Case for Action (No. 12). Geneva: World Health Organization (2008).
16. Campbell H, Duke T, Weber M, English M, Carai S, Tamburlini G. Pediatric hospital improvement group. Global initiatives for improving hospital care for children: state of the art and future prospects. Pediatrics. (2008) 121(4):e984–92. doi: 10.1542/peds.2007-1395
17. Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, Roder-DeWan S, et al. High-quality health systems in the sustainable development goals era: time for a revolution. Lancet Glob Health. (2018) 6(11):e1196–252. doi: 10.1016/S2214-109X(18)30386-3
18. Kiragu AW, Dunlop SJ, Mwarumba N, Gidado S, Adesina A, Mwachiro M, et al. Pediatric trauma care in low resource settings: challenges, opportunities, and solutions. Front Pediatr. (2018) 6:155. doi: 10.3389/fped.2018.00155
19. Olatunji G, Kokori E, Aderinto N, Eltayeb Muhammad Ibrahim D, Alhadheri A, Alsabri MAH. Pediatric emergency care in low-resource settings. Curr Emerg Hosp Med Rep. (2024) 12(2):82–7. doi: 10.1007/s40138-024-00291-w
20. Chaney P. Civil society perspectives on children’s rights in the occupied Palestinian territories: analysis of universal periodic review discourse 2013–2018. Int J Child Rights. (2022) 30(1):7–40. doi: 10.1163/15718182-30010003
21. Muthumani A. Safeguarding children through pediatric surgical care in war and humanitarian settings: a call to action for pediatric patients in Gaza. World J Pediatr Surg. (2024) 7(1):e000719. doi: 10.1136/wjps-2023-000719
Keywords: assessment, children, Gaza Strip, pediatric hospitals, quality of care, WHO
Citation: Eleyyan SY, ELssyed Etewa BB, Al’Haj Ahmad F and El Bilbeisi AH (2025) Evaluation of the quality of care in pediatric hospitals in the Gaza Strip using the WHO integrated tool: the healthcare providers' perspective. Front. Pediatr. 13:1589092. doi: 10.3389/fped.2025.1589092
Received: 6 March 2025; Accepted: 22 April 2025;
Published: 30 April 2025.
Edited by:
Stephen Aronoff, Temple University, United StatesCopyright: © 2025 Eleyyan, ELssyed Etewa, Al’Haj Ahmad and El Bilbeisi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abdel Hamid El Bilbeisi, YWJlZF9hekBob3RtYWlsLmNvbQ==