 Huihui Zhu
Huihui Zhu Fangfang Lv2
Fangfang Lv2 Ming Xu
Ming Xu Hailin Zhang
Hailin Zhang- 1Department of Child Health Care, The Second Affiliated Hospital & Yuying Children’s Hospital, Wenzhou Medical University, Wenzhou, China
- 2Department of Pediatric Pulmonology, The Second Affiliated Hospital & Yuying Children’s Hospital, Wenzhou Medical University, Wenzhou, China
Background: Pertussis, a highly contagious respiratory disease caused by Bordetella pertussis, traditionally associated with children, is now increasingly transmitted by adolescents (ages 10–19) and adults. Using data from the Global Burden of Diseases, Injuries, and Risk Factors Study 2021 (GBD 2021), we estimated the disease burden of pertussis among adolescents.
Methods: We analyzed adolescent pertussis data from GBD 2021, assessing prevalence, incidence, mortality, and Disability-Adjusted Life Year (DALY) rate across global, regional, and national levels. Temporal trends were quantified with the Estimated Annual Percentage Change (EAPC), and decomposition and prediction models were employed for further insights.
Results: From 1990 to 2021, adolescent pertussis prevalence, incidence, mortality, and DALY rate declined markedly worldwide. Declines were most pronounced in High and High-middle Socio-Demographic Index (SDI) regions, whereas Low SDI regions maintained the highest burden in 2021. Across the 21 GBD regions, the prevalence, incidence, mortality, and DALY rates have all declined. However, in Central Sub-Saharan Africa, the number of prevalence cases, incidence cases, deaths, and DALYs have increased, while these values have significantly decreased among adolescents in the other 20 GBD regions. Nationally and territorially, the study found substantial variability in the burden of pertussis among adolescents. Decomposition analysis indicated that epidemiological changes primarily drove the decline in most regions, though population growth contributed to increases in some areas. Projection models suggest that the global adolescent pertussis burden will reach its peak in 2022, followed by a gradual decline through 2046.
Conclusions: Despite an overall global decline, pertussis remains a public health concern among adolescents due to their role in disease transmission. Strengthening epidemiological understanding in this age group is essential for effective prevention and control strategies.
Background
Despite widespread vaccination, pertussis has re-emerged as a global public health challenge (1), characterized by a critical shift in transmission dynamics from children to adolescents and adults acting as the primary reservoir for infants (2–5). The World Health Organization (WHO) has explicitly acknowledged the central role of adolescents in this transmission chain (6); however, prior iterations of the Global Burden of Disease (GBD) studies have not systematically quantified the adolescent-specific burden of pertussis, creating a significant void in the evidence base (7). This is particularly concerning given that protective immunity following primary childhood vaccination wanes rapidly; within 5 to 10 years, a substantial majority of adolescents no longer maintain anti-pertussis toxin (PT) IgG antibody levels above the protective threshold, leaving them susceptible to infection and capable of transmitting the bacterium (8, 9). Infections in this age group consequently fuel a dual burden: they directly increase the risk of infant hospitalization and mortality, and impose a measurable socioeconomic burden through significant school absenteeism—averaging 5.5 days lost per adolescent case—and substantial work absenteeism among their parents (10). Analyses from Canadian models further indicate that these indirect costs substantially surpass the direct medical expenditures associated with treatment (11). Collectively, this lack of age-specific burden data represents a critical evidence gap, hindering the development of targeted booster immunization strategies and effective public health interventions.
To address this evidence gap, we analysed GBD 2021 data on prevalence, incidence, deaths and DALYs due to pertussis in adolescents. We used the EAPC, along with decomposition and prediction models, to analyze global, regional, and national trends in whooping cough from 1990 to 2021. This research provides data and recommendations for global pertussis prevention, aiming to reduce the disease burden and improve adolescent health.
Methods
Data source
The data were derived from the GBD study, which spans the period from 1980 to 2021 and includes 204 countries and territories across 21 geographic regions (12). The GBD study comprehensively assesses 369 diseases and injuries and 88 risk factors. The Socio-demographic Index (SDI) ranges from 0 to 1, with a higher score denoting a higher level of socioeconomic development. Based on this metric, regions are categorized into five groups: Low (<0.45), Low-middle (≥ 0.45 to <0.61), Middle (≥0.61 to <0.69), High-middle (≥0.69 to <0.80), and High (≥0.80) (13). All data and methodological details are publicly accessible through the GBD website and the Global Health Data Exchange (GHDx) query tools. The study adheres to the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER), ensuring transparency, reproducibility, and reliability of the estimates.
EAPC model analysis
The EAPC model evaluates changes in disease rates over time by calculating the average annual percentage change. It's useful for identifying trends, comparing changes across periods or populations, and is commonly used in epidemiology to guide public health interventions (14).
Decomposition model analysis
We used Das Gupta's decomposition method to break down changes in pertussis incidence, prevalence, deaths, and DALYs into three factors: population aging, population growth, and epidemiological changes, quantifying each factor's impact on overall trends (15).
Nordpred model analysis
We applied the Nordpred model, which is grounded in the Age-Period-Cohort (APC) framework, to forecast the adolescent pertussis burden based on its specific suitability for surveillance data structured in 5-year age groups and 5-year calendar intervals—matching exactly the format of GBD 2021 data (16). This approach allowed us to explicitly model age, period, and cohort effects, thereby capturing key demographic and immunization-related trends that are often neglected by simpler time-series or machine learning models. Additionally, the model's integration of smoothing techniques helped reduce random noise, while the inclusion of more recent data improved medium- and long-term prediction accuracy. All statistics were done in R (v 4.3.3).
Results
Global level
From 1990 to 2021, the global burden of pertussis among adolescents showed a consistent and substantial decline in prevalence, incidence, deaths, and DALYs (see Figure 1, Table 1 and Supplementary Tables S1–S3). The total number of prevalent cases decreased by 74.87%, while incidence cases, deaths, and DALYs also fell markedly over this period. By 2021, the global prevalence rate had dropped to 2.33 per 100,000 people, down from 11.36 in 1990, and the incidence rate fell from 82.94 to 17.04 per 100,000. Mortality and DALYs similarly exhibited significant reductions. The EAPC in global adolescent pertussis burden from 1990 to 2021 were −2.44 for prevalence and incidence, −3.25 for mortality, and −3.24 for DALYs, all indicating significant declines (see Supplementary Results for detailed data).
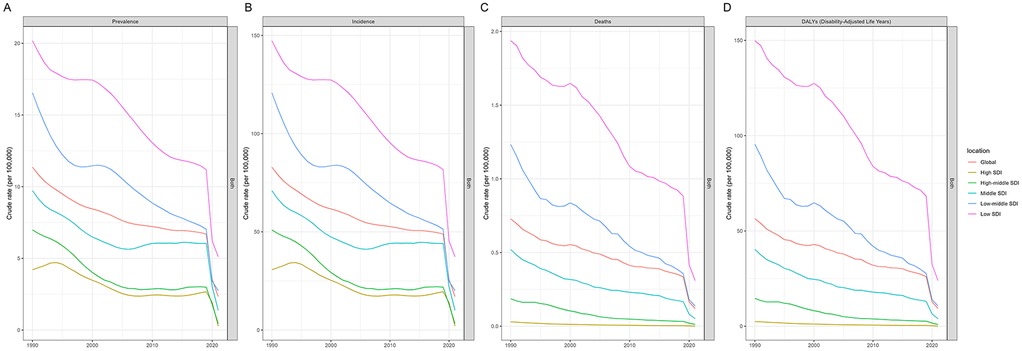
Figure 1. Global and SDI region trajectories of adolescent pertussis prevalence (A), incidence (B), mortality (C), and DALYs rates (D), 1990 to 2021.
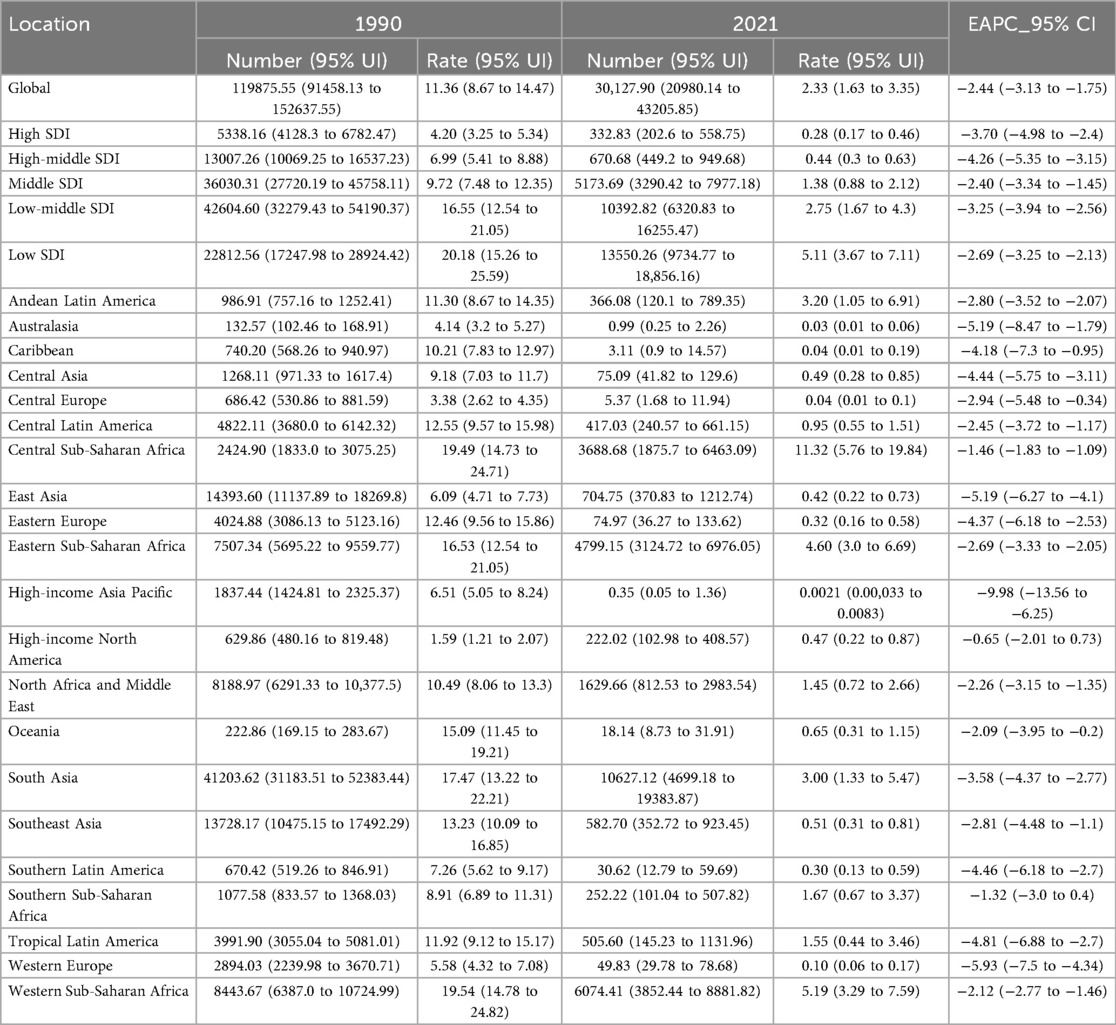
Table 1. Global and regional prevalence of adolescent pertussis from 1990 to 2021.
SDI regional level
Between 1990 and 2021, adolescent pertussis burden decreased across all five SDI regions, with significant disparities in the magnitude of reduction observed (see Figure 1, Table 1, and Supplementary Tables S1–S3). The High-middle SDI region demonstrated the most substantial improvements in prevalent and incident cases, with the number of prevalent cases declining by 94.84% and incident cases decreasing by 94.26%, both with an EAPC of −4.26. For mortality and DALYs, the High SDI region showed the most pronounced reductions, with deaths decreasing by 97.05% (EAPC: −7.83) and DALYs by 96.77% (EAPC: −7.03). In contrast, the Low SDI region exhibited the most modest improvements across all indicators: prevalent cases decreased by 40.60% (EAPC: −2.69), incident cases by 34.81% (EAPC: −2.69), deaths by 62.53% (EAPC: −3.65), and DALYs by 62.43% (EAPC: −3.65). Consequently, the Low SDI region maintained the highest disease burden rates in 2021 (see Supplementary Results for detailed data).
GBD regional level
Between 1990 and 2021, adolescent pertussis rates (prevalence, incidence, mortality, and DALYs) declined across all 21 GBD regions. However, in terms of absolute numbers, Central Sub-Saharan Africa experienced an increase in prevalent cases, incident cases, deaths, and DALYs. In contrast, the other 20 GBD regions showed a substantial decrease in the absolute burden across all these indicators (see Table 1, Supplementary Tables S1–S3). In 2021, Central Sub-Saharan Africa not only had the highest prevalence and incidence rates (11.32 and 82.66 per 100,000, respectively) but also recorded the highest mortality and DALY rates (0.72 deaths and 55.61 DALYs per 100,000). South Asia reported the highest absolute disease burden, with over 10,600 prevalent cases and 500 deaths in 2021. Conversely, High-income Asia Pacific and Australasia demonstrated the most successful control of adolescent pertussis, both achieving near-elimination status with the lowest absolute numbers and rates globally (see Supplementary Results for detailed data).
From 1990 to 2021, the High-income Asia Pacific region demonstrated the most rapid decline in adolescent pertussis burden, with EAPC values of −9.98 for prevalence, −9.98 for incidence, −11.56 for mortality, and −11.31 for DALYs. In contrast, High-income North America showed the slowest progress, with EAPCs of −0.65 for prevalence, −0.65 for incidence, −0.07 for mortality, and −0.57 for DALYs. A strong inverse correlation was observed between regional SDI and disease burden, with higher SDI regions generally experiencing faster declines (see Supplementary Figure S1). Notably, Western, Eastern, and Central Sub-Saharan Africa regions, along with Andean Latin America and South Asia, consistently exhibited burden rates above the global average (see Supplementary Results for detailed data).
Countries level
The burden of adolescent pertussis exhibited substantial heterogeneity at the national level from 1990 to 2021. In 2021, India reported the highest absolute numbers across all four indicators—prevalence, incidence, deaths, and DALYs-representing the greatest overall disease burden globally. Meanwhile, Angola and Kiribati showed the highest prevalence and mortality rates, respectively. Several countries and territories, including Niue, Bermuda, and the Republic of Korea, achieved near-elimination status with the lowest reported burden worldwide (see Figure 2, Supplementary Figure S2, Supplementary Tables S4–S7, and Supplementary Results for detailed data).
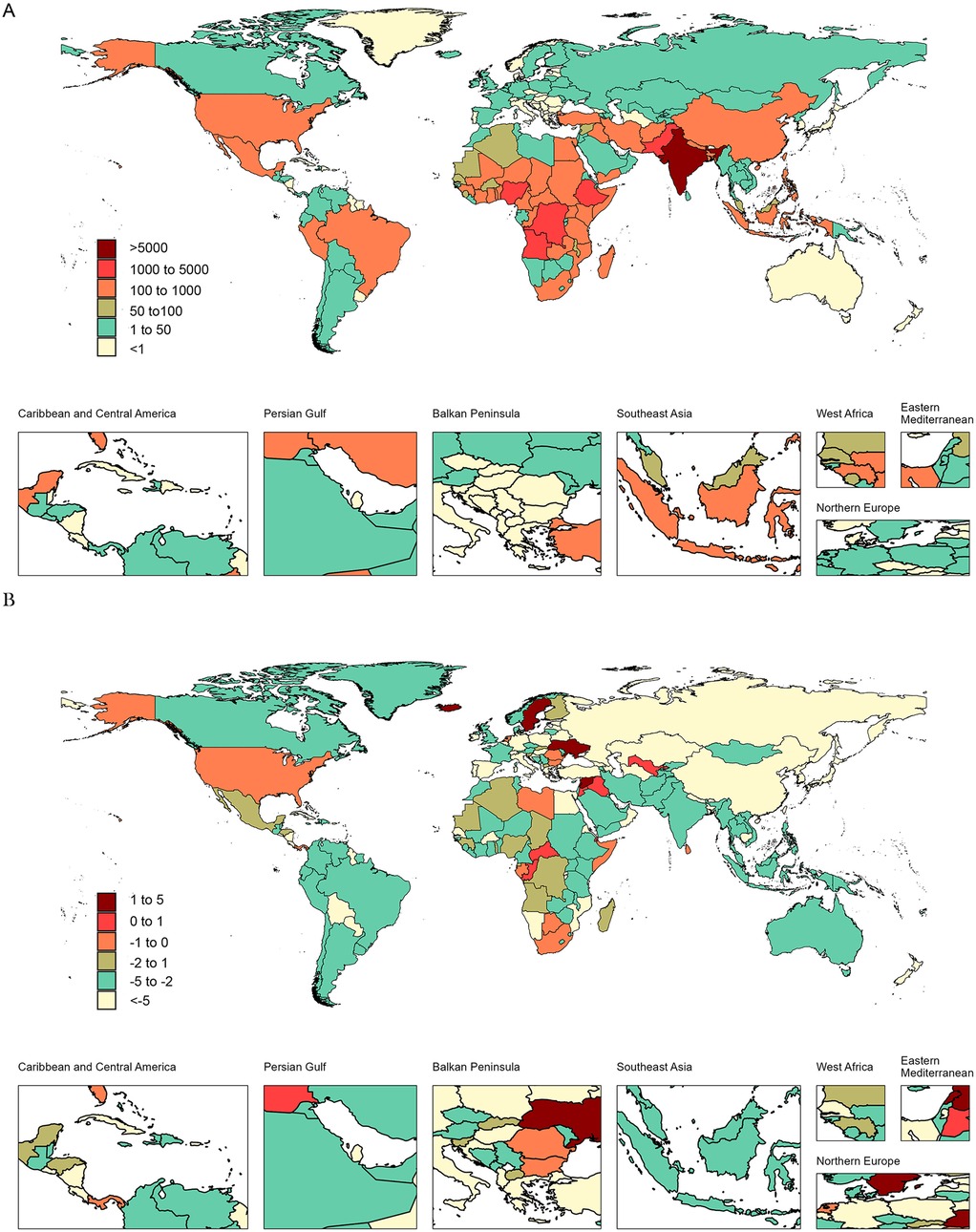
Figure 2. Global maps of adolescent pertussis prevalence cases in 2021 (A) EAPC for adolescent Pertussis prevalence (B), 1990 to 2021.
Between 1990 and 2021, adolescent pertussis burden decreased in most countries, though several notable exceptions emerged. Nicaragua demonstrated the most substantial declines across all indicators, with EAPCs of −16.72 for prevalence and incidence, −18.74 for mortality, and −18.72 for DALYs. Conversely, Iceland showed significant increases in prevalence and incidence (EAPC: 5.38), while Spain experienced the sharpest rise in mortality (EAPC: 15.54). Ukraine recorded the greatest increase in DALYs (EAPC: 3.3) during this period (see Figure 2, Supplementary Figure S3, Supplementary Tables S8–S11, and Supplementary Results for detailed data).
Decomposition analysis of global, SDI regions and 21 GBD regions adolescent pertussis trends, 1990 to 2021
We used decomposition methods to analyze the contributions of population aging, population growth, and epidemiological changes to the variation in prevalence, incidence, deaths, and DALYs of adolescent pertussis globally, across five SDI regions, and 21 GBD regions (Figure 3, Supplementary Tables S12–S15). Globally, the overall burden of adolescent pertussis has declined, mainly due to epidemiological changes, while population growth has contributed to an increased burden. Among SDI regions, epidemiological changes were the main driver of burden reduction. The Low SDI region saw the slowest reduction, while the High-middle SDI region experienced the fastest decline in prevalence and incidence, and the High SDI region saw the fastest decline in deaths and DALYs. Among GBD regions, Central Sub-Saharan Africa was the only region to see an increase, driven by population growth, while other regions, especially high-income Asia Pacific, saw declines mainly due to epidemiological changes.
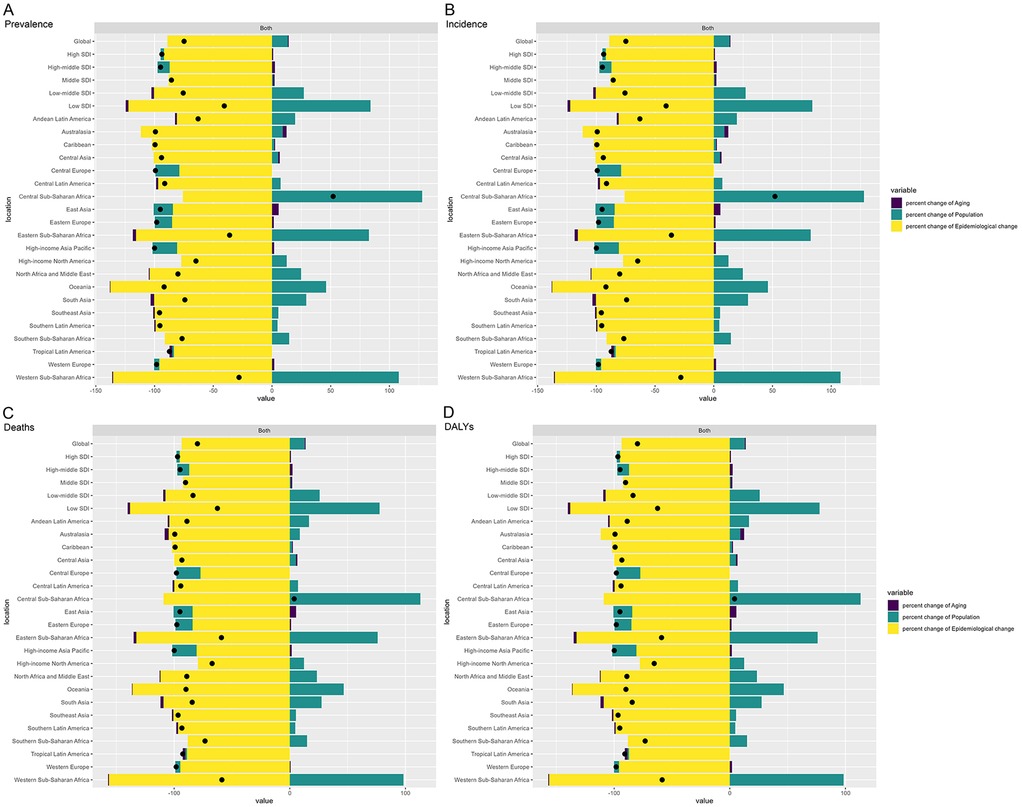
Figure 3. Decomposition analysis of the burden of adolescent pertussis prevalence (A), incidence (B), deaths (C), and DALYs (D), 1990 to 2021.
Future burden of pertussis among adolescents worldwide
We predicted future trends in the global burden of adolescent pertussis (Figure 4, Supplementary Tables S16–S19). The burden is expected to increase until 2022, followed by a gradual decline from 2023 onward. In 2022, the prevalence rate was 4.79 per 100,000 people (61,612 cases), an increase of 51.1% from 2021. The incidence rate was 35.02 per 100,000 people (449,961 cases), up 51.12%, the mortality rate was 0.24 per 100,000 (3,045 deaths), up 49.2%, and the DALYs rate was 18.48 years per 100,000 (237,412 DALYs), up 49.4%. Despite the expected decline over the next 20 years, the burden will remain higher than in 2021. By 2046, the predicted prevalence rate is 3.59 per 100,000 people (45,936 cases), incidence rate is 26.31 per 100,000 (336,210 cases), mortality rate is 0.16 per 100,000 (2,053 deaths), and DALYs rate is 12.70 years per 100,000 (162,069 DALYs), all showing increases compared to 2021.
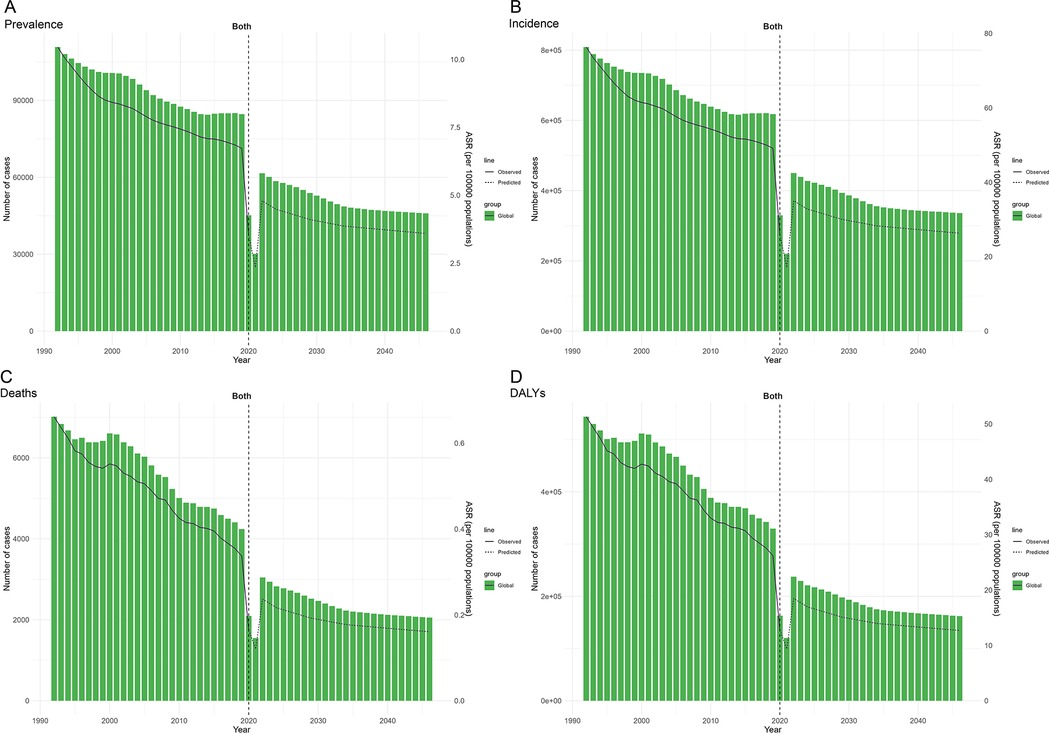
Figure 4. Global adolescent pertussis forecasts: prevalence (A), incidence (B), deaths (C), and DALYs (D) from 1992 to 2046.
Discussion
Our study leverages the latest GBD 2021 data to provide contemporary epidemiological insights into adolescent pertussis. Over the past three decades, there has been a general decline in the burden of this disease globally, as well as in five SDI regions and 21 GBD regions, highlighting the success of improved prevention and treatment strategies. However, although the disease burden of pertussis among adolescents in Central Sub-Saharan Africa is declining, the prevalence, incidence, deaths, and DALYs are rising. Our decomposition analysis reveals that population growth is the primary factor driving the increase in Central Sub-Saharan Africa, whereas epidemiological changes are responsible for reductions in other regions. Significant disparities exist among countries. For instance, India reports the highest numbers in prevalence, incidence, deaths, and DALYs, largely due to its vast population. Factors such as access to healthcare, environmental conditions, and cultural influences also play crucial roles (6). Our analysis found a negative correlation between the burden of adolescent pertussis and SDI, with higher SDI regions typically reporting lower rates of prevalence, incidence, mortality, and DALYs due to socioeconomic advancement and stronger healthcare systems. Lower SDI regions should focus on reducing health disparities by improving education, healthcare, and public health awareness. Despite the overall decline in burden, emerging data suggest it may be underestimated. Over the past two decades, there has been a shift in pertussis cases toward older children and adults (17, 18). This aligns with broader multinational analyses pointing to waning immunity and improved diagnosis in older age groups as key drivers of this global phenomenon. For instance, studies in China noted increasing positivity rates among adolescents (19). Similarly, the Netherlands observed a 60% increase in incidence among those aged 10–19 (20), and South Korea reported an incidence of 9.2 per 100,000 in adolescents aged 10–14 in 2018 (21). EU surveillance data further indicate that individuals aged 15 and above accounted for 62% of all pertussis cases (22). This widespread shift in epidemiology is further supported by a large Asian study, in which 4.8% of adolescents showed serological evidence of recent pertussis infection, confirming significant undetected transmission across the region (23). Similarly, Latin America mirrors this trend. Mexico now reports the highest case rates in 10–14-year-olds; however, only Argentina, Chile, Uruguay, and Venezuela include an adolescent Tdap booster in their national schedules. This has resulted in substantial immunity gaps and ongoing silent transmission (24). Collectively, these findings highlight the urgent need for adaptive public health strategies.
The clinical manifestations of pertussis in adolescents are often mild or atypical, such as a chronic cough, making diagnosis challenging and leading to potential underestimation in this population (25). Factors like atypical symptoms, low awareness, and healthcare limitations further complicate the epidemiology and burden of adolescent pertussis, contributing to underdiagnosis and underreporting (26). Predictive analysis shows a significant increase in adolescent pertussis followed by a gradual decline, with a turning point in 2022. This decrease may be partly attributable to global COVID-19 control measures—such as mask-wearing and social distancing—which likely reduced the transmission of respiratory pathogens. However, this remains a speculative interpretation, and our model cannot definitively establish causation; the observed turning point may also be influenced by other factors, such as immunity gaps or reporting disruptions from the pandemic itself. Thus, these predictions must be interpreted with caution due to the inherent limitations of modeling and warrant further investigation.
This study acknowledges limitations of the GBD 2021 study, such as reliance on incomplete or unreliable health data, especially in low- and middle-income countries. Variability in data quality and assumptions in statistical models affect accuracy. Changes in risk factor definitions and delays in data updates complicate comparisons. The GBD also oversimplifies cultural, socioeconomic factors, and health interventions, requiring cautious interpretation.
In summary, despite a significant global decline from 1990 to 2021, the burden of adolescent pertussis remains substantial and is likely underreported. The shifting epidemiology, coupled with significant regional disparities driven by population growth and socioeconomic factors, calls for enhanced age-specific surveillance, vaccination strategies that address waning immunity, and targeted international cooperation to mitigate the burden in this key age group.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not required for the studies involving humans because This study utilized anonymized, aggregated data from the Global Burden of Disease Study 2021, which is a publicly available dataset containing no personally identifiable information. As such, ethical approval was not required for this secondary analysis in accordance with institutional and national guidelines. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements because This study utilized anonymized, aggregated data from the Global Burden of Disease Study 2021, which is a publicly available dataset containing no personally identifiable information. As such, ethical approval was not required for this secondary analysis in accordance with institutional and national guidelines.
Author contributions
HZ: Writing – original draft, Writing – review & editing. FL: Writing – review & editing. SW: Writing – review & editing. MX: Writing – review & editing. HZ: Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was funded by the Wenzhou Science and Technology Project (No. Y20220270).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2025.1601110/full#supplementary-material
Abbreviations
DALYs, Disability-adjusted Life-years; SDI, Sociodemographic Index; GBD, Global Burden of Disease; EAPC, Estimated Annual Percentage Change.
References
1. Böhme M, Voigt K, Balogh E, Bergmann A, Horváth F, Kugler J, et al. Pertussis vaccination status and vaccine acceptance among medical students: multicenter study in Germany and Hungary. BMC Public Health. (2019) 19(1):182. doi: 10.1186/s12889-019-6516-8
2. Herzog C. Changing from whole-cell to acellular pertussis vaccines would trade superior tolerability for inferior protection. Expert Rev Vaccines. (2015) 14(8):1065–72. doi: 10.1586/14760584.2015.1059759
3. Zhang J, Zhang D, Wang X, Wei X, Li H. Macrolide susceptibility and molecular characteristics of Bordetella pertussis. J Int Med Res. (2022) 50(2):3000605221078782. doi: 10.1177/03000605221078782
4. Xu H, Huang J, Liu Z, Li X, Wang K, Feng E, et al. Expression of Bordetella pertussis antigens fused to different vectors and their effectiveness as vaccines. Vaccines. (2021) 9(6):542. doi: 10.3390/vaccines9060542
5. Schellekens J, von König CH, Gardner P. Pertussis sources of infection and routes of transmission in the vaccination era. Pediatr Infect Dis J. (2005) 24(5):S19–24. doi: 10.1097/01.inf.0000160909.24879.e6
6. WHO. Pertussis vaccines: WHO position paper, August 2015–recommendations. Vaccine. (2016) 34(12):1423–5. doi: 10.1016/j.vaccine.2015.10.136
7. GBD, 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2024) 403(10440):2100–32. doi: 10.1016/S0140-6736(24)00367-2
8. Liu Y, Yu D, Wang K, Ye Q. Global resurgence of pertussis: a perspective from China. J Infect. (2024) 89(5):106289. doi: 10.1016/j.jinf.2024.106289
9. Warfel JM, Zimmerman LI, Merkel TJ. Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model. Proc Natl Acad Sci U S A. (2014) 111(2):787–92. doi: 10.1073/pnas.1314688110
10. Hay JW, Ward JI. Economic considerations for pertussis booster vaccination in adolescents. Pediatr Infect Dis J. (2005) 24(6):S127–33. doi: 10.1097/01.inf.0000166160.23976.35
11. McGirr A, Fisman DN, Tuite AR. The health and economic burden of pertussis in Canada: a microsimulation study. Vaccine. (2019) 37(49):7240–7. doi: 10.1016/j.vaccine.2019.09.070
12. Collaborators GRF. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990−2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2024) 403(10440):2162–203. doi: 10.1016/S0140-6736(24)00933-4
13. Jiang Q, Shu Y, Jiang Z, Zhang Y, Pan S, Jiang W, et al. Burdens of stomach and esophageal cancer from 1990 to 2019 and projection to 2030 in China: findings from the 2019 global burden of disease study. J Glob Health. (2024) 14:04025. doi: 10.7189/jogh.14.04025
14. GBD, 2021 Sickle Cell Disease Collaborators. Global, regional, and national prevalence and mortality burden of sickle cell disease, 2000−2021: a systematic analysis from the global burden of disease study 2021. Lancet Haematol. (2023) 10(8):e585–99. doi: 10.1016/S2352-3026(23)00118-7
15. Das Gupta P. Standardization and decomposition of rates from cross-classified data. Genus. (1994) 50(3–4):171–96.12319256
16. Liu Y, Zhang C, Wang Q, Wu K, Sun Z, Tang Z, et al. Temporal trends in the disease burden of colorectal cancer with its risk factors at the global and national level from 1990 to 2019, and projections until 2044. Clin Epidemiol. (2023) 15:55–71. doi: 10.2147/CLEP.S388323
17. Quinn HE, McIntyre PB. Pertussis epidemiology in Australia over the decade 1995−2005–trends by region and age group. Commun Dis Intell Q Rep. (2007) 31(2):205–15. doi: 10.33321/cdi.2007.31.18
18. Wang H, Fu M, Chen W, Ma Y. Post-COVID-19 pandemic changes in pertussis incidence among patients with acute respiratory tract infections in Zhejiang, China. Front Microbiol. (2024) 15:1448997. doi: 10.3389/fmicb.2024.1448997
19. Homaira N, He WQ, McRae J, Macartney K, Liu B. Coverage and predictors of influenza and pertussis vaccination during pregnancy: a whole of population-based study. Vaccine. (2023) 41(43):6522–9. doi: 10.1016/j.vaccine.2023.09.008
20. de Greeff SC, Mooi FR, Schellekens JF, de Melker HE. Impact of acellular pertussis preschool booster vaccination on disease burden of pertussis in The Netherlands. Pediatr Infect Dis J. (2008) 27(3):218–23. doi: 10.1097/INF.0b013e318161a2b9
21. Jog P, Memon IA, Thisyakorn U, Hozbor D, Heininger U, von König CHW, et al. Pertussis in Asia: recent country-specific data and recommendations. Vaccine. (2022) 40(8):1170–9. doi: 10.1016/j.vaccine.2021.12.004
22. European Centre for Disease Prevention and Control. Pertussis in: ECDC. Annual epidemiological report for 2018. (2020). Available online at: https://www.ecdc.europa.eu/en/publications-data/pertussis-annual-epidemiological-report-2018 (Accessed 12 January, 2021).
23. Son S, Thamlikitkul V, Chokephaibulkit K, Perera J, Jayatilleke K, Hsueh PR, et al. Prospective multinational serosurveillance study of Bordetella pertussis infection among 10- to 18-year-old Asian children and adolescents. Clin Microbiol Infect. (2019) 25(2):250.e1–e7. doi: 10.1016/j.cmi.2018.04.013
24. Ulloa-Gutierrez R, Hozbor D, Avila-Aguero ML, Echániz-Aviles G, Gentile A, Torres Torretti JP, et al. Country-specific data and priorities for pertussis in Latin America: recent findings from the global Pertussis initiative. Open Forum Infect Dis. (2025) 12(5):ofaf154. doi: 10.1093/ofid/ofaf154
25. Howard Ludlam A, Paynter J, Goodyear-Smith F, Petousis-Harris H. Pertussis epidemiology in adults: retrospective analysis of pertussis incidence and association with comorbidities among adult populations in Aotearoa New Zealand, using national administrative datasets. Vaccine. (2024) 42(23):126048. doi: 10.1016/j.vaccine.2024.06.016
Keywords: pertussis, global burden of disease, socio-demographic index, adolescent, estimated annual percentage change
Citation: Zhu H, Lv F, Wen S, Xu M and Zhang H (2025) Trends in adolescent pertussis burden: a systematic analysis from 1990 to 2021 in global, regional, and national within the global burden of disease study 2021, with forecasts for 2046. Front. Pediatr. 13:1601110. doi: 10.3389/fped.2025.1601110
Received: 27 March 2025; Accepted: 10 September 2025;
Published: 24 September 2025.
Edited by:
Hanani Abdul Manan, Universiti Kebangsaan Malaysia Medical Center (UKMMC), MalaysiaReviewed by:
Mercedes Macías Parra, National Institute of Pediatrics, MexicoMohammed Hasen Badeso, Ethiopian Public Health Institute, Ethiopia
Vinh Ngo, Vietnam National Hospital of Pediatrics, Vietnam
Copyright: © 2025 Zhu, Lv, Wen, Xu and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hailin Zhang, emhsd3o5N0Bob3RtYWlsLmNvbQ==