 Carlos Augusto Cuadros Mendoza1,2,†Mario Javier Rosero Portilla2,†Verónica Pico Quintero2,†
Carlos Augusto Cuadros Mendoza1,2,†Mario Javier Rosero Portilla2,†Verónica Pico Quintero2,† Edgar Fabián Manrique-Hernández3*†
Edgar Fabián Manrique-Hernández3*† Alexandra Hurtado-Ortiz3,†Maricel Licht-Ardila3,†Alejandra Mendoza-Monsalve3,†
Alexandra Hurtado-Ortiz3,†Maricel Licht-Ardila3,†Alejandra Mendoza-Monsalve3,†
- 1Department of Gastroenterology, Fundación Cardiovascular de Colombia, Piedecuesta, Colombia
- 2Postgraduate Department in Pediatric Critical Care, Universidad de Santander, Bucaramanga, Colombia
- 3Epidemiology Department, Fundación Cardiovascular de Colombia, Piedecuesta, Colombia
Introduction: Malnutrition significantly impairs both physical and cognitive function, increasing the risk of morbidity and mortality, especially in patients lacking a safe and effective route for enteral nutrition. Percutaneous endoscopic gastrostomy offers a minimally invasive solution for long-term enteral nutrition in pediatric patients, with a lower risk of perioperative complications compared to surgical alternatives.
Objective: To evaluate the frequency, timing, and clinical factors associated with postoperative complications following pediatric percutaneous endoscopic gastrostomy.
Methods: A retrospective analytical cohort study was conducted, including pediatric patients (≤18 years) who underwent Percutaneous endoscopic gastrostomy placement between January 2018 and December 2024. Bivariate analyses and Kaplan–Meier survival curves were used to assess the frequency of complications and complication-free survival time.
Results: A total of 86 pediatric patients underwent Percutaneous endoscopic gastrostomy during the study period, of whom 12 (14%) experienced major postoperative complications. The median age was 4.53 years (interquartile range: 1.56–9.46 years). The most frequent major complication was Buried Bumper Syndrome, observed in 9 patients (10.47%). Minor complications included mild peristomal infection (8.14%) and feeding intolerance (5.81%). A complication-free survival of 96.73% (95% CI: 87.26–99.19) by day 12 and 69.35% (95% CI: 45.33–84.43) by day 40 was determined.
Discussion: This study underscores the importance of systematic nutritional assessment and optimized post-operative care to reduce complications following PEG in pediatric patients. The high incidence of Buried Bumper Syndrome calls for more stringent follow-up protocols, especially in resource-limited settings. Close monitoring during the early post-operative period can prevent complications.
Introduction
Malnutrition is defined by alterations in body composition that negatively impact both physical and cognitive function, increasing morbidity and mortality, particularly in patients with underlying medical conditions (1). Its consequences include sarcopenia, immunosuppression, delayed wound healing, and a higher susceptibility to infections (2). The absence of a safe and effective route for enteral nutrition may exacerbate malnutrition, leading to further complications such as bronchial microaspirations and increased dependence on parenteral nutrition (3, 4).
Establishing adequate enteral access is therefore critical for meeting nutritional requirements, especially during periods of metabolic stress (5). The choice of access route depends on the underlying pathology and expected duration of nutritional support (6). While nasogastric tubes are typically used for short-term feeding, gastrostomy is recommended when enteral nutrition is anticipated to last longer than 4–6 weeks (7). In pediatric patients, percutaneous endoscopic gastrostomy (PEG) has become the preferred method, offering a minimally invasive alternative to surgical approaches, with a lower risk of perioperative complications and faster recovery (4).
PEG is particularly advantageous in children with complex comorbidities—such as congenital heart disease or neurological disorders—where timely and sustained nutritional support can improve clinical stability and quality of life (7). Nonetheless, the indications for PEG vary by clinical context and population, encompassing conditions like neurogenic dysphagia, congenital oropharyngeal anomalies, and oncological diseases (8). These differences underscore the importance of a context-specific evaluation when determining candidacy for the procedure (9).
In addition to appropriate patient selection, monitoring and understanding both early and late complications are essential for optimizing care and minimizing risks (10). Complications such as infections, tube dislodgement, and respiratory issues must be identified and managed proactively to improve outcomes and guide preventive strategies (9, 11). In this context, the present study aims to evaluate the frequency, timing, and clinical factors associated with postoperative complications following pediatric PEG.
Methods
A retrospective analytical cohort study was conducted, including all pediatric patients (≤18 years) who underwent PEG at a high-complexity hospital in northeastern Colombia between 01 January 2018 and 08 December 2024. Data were extracted from the institutional electronic medical records and correspond to the hospitalization during which the gastrostomy procedure was performed (Figure 1). All researchers involved in data collection and processing received training to minimize potential errors and ensure data reliability.
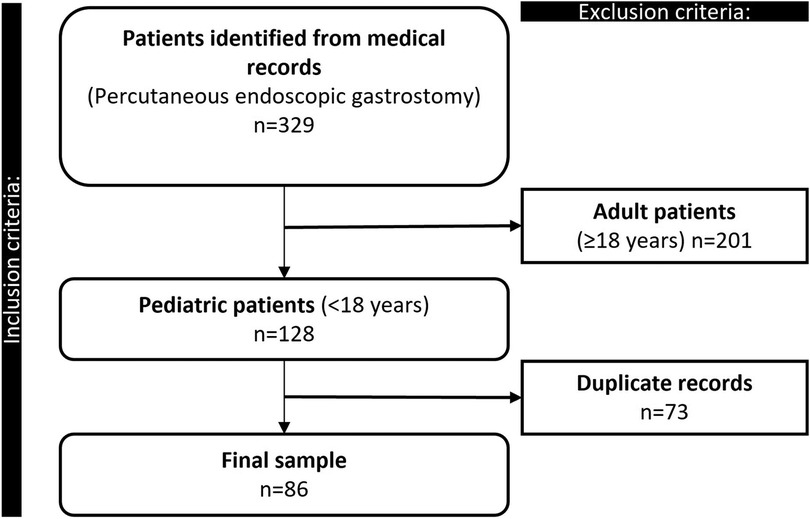
Figure 1. Flowchart summarizing the selection process of pediatric patients undergoing endoscopic gastrostomy.
The following variables were collected: Sociodemographic variables: sex, age, weight and height at the time of the procedure and discharge. Clinical variables: nutritional status at the time of the procedure, and pre-existing comorbidities, including cystic fibrosis, chronic kidney disease, non-progressive or progressive encephalopathy, neuromuscular or neurometabolic diseases, congenital heart disease, sequelae of traumatic brain injury or cerebrovascular events, gastroesophageal reflux disease, and recent extracorporeal membrane oxygenation (ECMO) use within the past 3 months. Pre-procedure laboratory values were also recorded: albumin level, hemoglobin, and international normalized ratio (INR).
Procedure-related variables included the indication for PEG—such as severe oral hypersensitivity, refractory dysphagia, refractory failure to thrive, eating behavior disorders, and craniofacial malformations—date of the procedure, occurrence of intraoperative complications, and type of post-procedural enteral nutrition (normocaloric vs. hypercaloric; elemental vs. polymeric). Additional data included changes in the gastrostomy tube (e.g., removal with internal bumper), reasons for removal (routine replacement, accidental displacement, or complications), the need for laparoscopic gastrostomy, and length of hospital stay (from admission for the procedure to discharge).
Outcomes: The primary outcome was the occurrence of postoperative complications, classified as major or minor, according to the Dindo-Clavien classification (12). Major complications included Buried Bumper Syndrome (BBS), peritonitis, significant gastrointestinal bleeding (requiring hemostatic intervention, transfusion, or endoscopic/surgical therapy), severe peristomal infection, soft tissue sepsis (complete blood count and acute-phase reactants), gastrocutaneous or enterocutaneous fistula (contrast-enhanced digestive tract radiography with water-soluble contrast and digestive endoscopy), peristomal abscess, fascial necrosis (surgical confirmation is necessary), visceral perforation, tension pneumoperitoneum (plain abdominal x-ray), and death. Minor complications comprised mild peristomal infections, leakage, ostomy dilation, granuloma formation, accidental tube removal, tube displacement without evidence of peritonitis or pneumoperitoneum, pain unresponsive to The World Health Organization step-1 analgesics, and feeding intolerance.
The procedures were performed by a pediatric surgeon with over 10 years of experience in minimally invasive surgery, who conducted 3.3% of the cases. A recently graduated pediatric surgeon performed an additional 3.3% of the procedures. The majority of the procedures (73.3%) were carried out by a pediatric gastroenterologist with more than 10 years of experience in endoscopic techniques. Additionally, a pediatric gastroenterologist-nutritionist, also with extensive experience, was responsible for 22% of the procedures. All professionals had significant prior experience in performing PEG and adhered to standardized institutional protocols, ensuring the safety and consistency of the procedure throughout the study cohort.
Surgical technique
Following the identification of the indication for PEG, a consultation is requested with the pediatric gastroenterology service to confirm the indication and determine the optimal timing for the procedure, based on the patient's nutritional status and clinical stability. The procedure is scheduled electively in the operating room, following informed consent. Sedation is administered, and depending on the clinical context, the airway is secured via endotracheal intubation.
In the standard technique, the pediatric gastroenterologist performs an upper endoscopy to identify the optimal site for insertion under aseptic conditions. A long guidewire is introduced endoluminally into the stomach and retrieved percutaneously using the pull-through technique. An age- and size-appropriate gastrostomy tube is inserted as follows: 14 Fr for small children under 5 years of age, 20 Fr for older children aged 5–12 years, and 22–24 Fr for adolescents over 11 years of age. The tube is secured with an internal retention dome, and proper intragastric positioning is confirmed endoscopically. The tube is kept closed for 24 h with monitoring of clinical signs; feeding is initiated thereafter according to clinical status.
Follow-up protocol
Patients are routinely monitored in the pediatric ward or intensive care unit until full enteral feeding volume is achieved. Upon discharge, a follow-up visit is scheduled at 1 month, during which the internal bolster gastrostomy tube is electively replaced with a balloon gastrostomy tube. This replacement is performed endoscopically in a planned manner.
Statistical analysis
Categorical variables were reported as absolute frequencies and percentages, while continuous variables were tested for normality using the Shapiro–Wilk test. Variables with non-normal distribution were expressed as medians with interquartile ranges (IQR). Bivariate analyses were conducted to explore associations between independent variables and the occurrence of major complications. Categorical variables were compared using the chi-square or Fisher's exact test, and non-normally distributed continuous variables were compared using the Mann–Whitney U test. Survival analysis was performed using Kaplan–Meier curves to estimate complication-free survival, with comparisons made using the log-rank test. A two-tailed p-value <0.05 was considered statistically significant. All analyses were performed using STATA version 16 (StataCorp, USA).
Results
Patients were classified into two groups based on the presence or absence of postoperative complications (Figure 1). A total of 86 pediatric patients were included, of whom 51 (59.30%) were male and 35 (40.70%) were female. In the group without complications, 46 patients (62.16%) were male, whereas in the group with complications, 5 (41.67%) were male. The overall median age was 4.53 years, with similar values observed across both groups (no complications: 4.53 and complications: 4.39). Weight and height at the time of the procedure were also comparable, with a median weight of 12.60 kg and a median height of 94.50 cm. At hospital discharge, the median weight and height remained similar between groups, at 12.45 kg and 93.00 cm, respectively (Table 1).
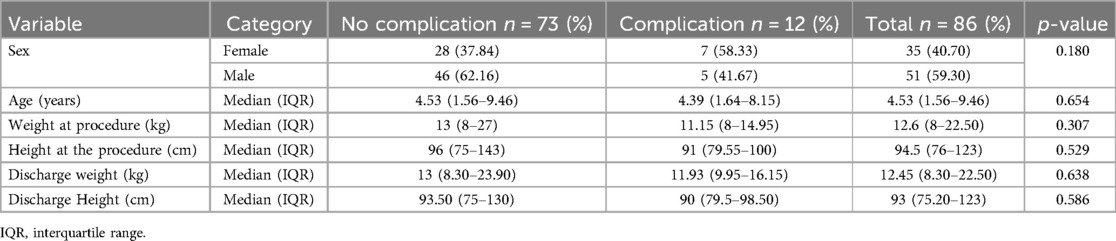
Table 1. Sociodemographic characteristics of pediatric patients according to the presence of major complications.
The analysis of clinical history revealed no statistically significant differences in most of the variables assessed. Severe acute malnutrition and exacerbated chronic malnutrition were more frequent among patients who developed complications (16.67% and 25.00%, respectively). Similarly, no significant associations were found with encephalopathy, neuromuscular diseases, congenital heart disease, chronic lung disease, or sequelae of cerebrovascular events. Swallowing disorders were present in 94.19% of patients. Although a higher proportion of patients with complications received a hypercaloric diet compared to those without complications (33.33% vs. 13.70%, p = 0.089). Additionally, pre-procedure levels of albumin, hemoglobin, and INR were not associated with the development of complications (Table 2).
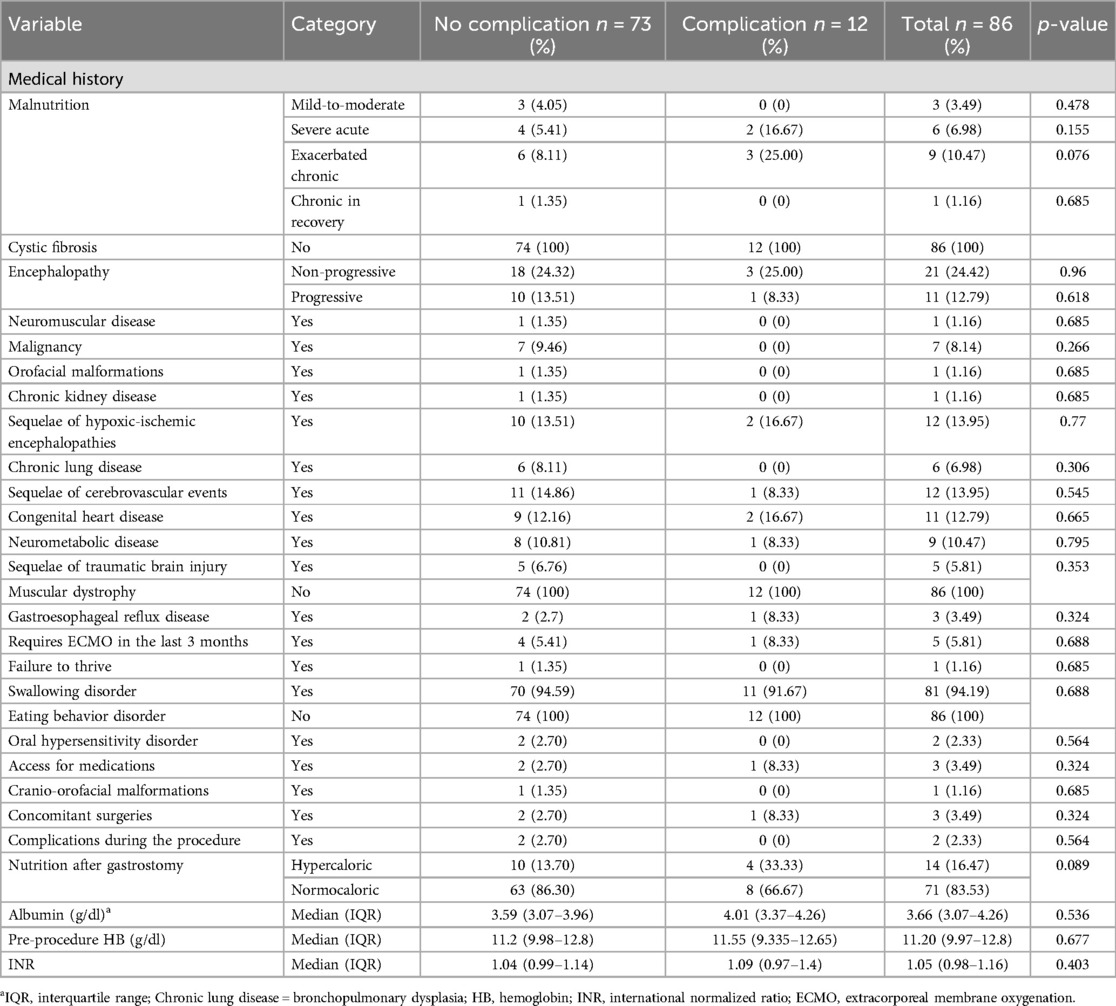
Table 2. Clinical characteristics of pediatric patients according to the presence of major complications.
A total of 37 complications, 23 minor identified in 20 patients and 14 major in 12 patients, indicating that some individuals experienced more than one event. Major complications were observed in 16.30% of cases, with BBS being the most frequent (10.47%), followed by severe peristomal infection (3.49%), gastrostomy-related sepsis (1.16%), and gastrocutaneous fistula (1.16%). Minor complications were more prevalent and included mild peristomal infection (8.14%), feeding intolerance (5.81%), granuloma formation (3.49%) and accidental tube removal (3.49%) (Table 3).

Table 3. Frequency and types of complications in pediatric patients undergoing endoscopic gastrostomy.
Kaplan–Meier analysis revealed a progressive decline in major complication-free survival following the procedure. The probability of remaining free of major complications by day 12 was 96.73% [95% Confidence Interval (CI): 87.26–99.19], and by day 29, it was 90.28% (95% CI: 74.84–96.46). The most pronounced drop occurred after day 36, with the probability decreasing to 75.13% (95% CI: 52.24–88.17) by day 38 and to 69.35% (95% CI: 45.33–84.43) by the end of follow-up (day 40) (Figure 2).
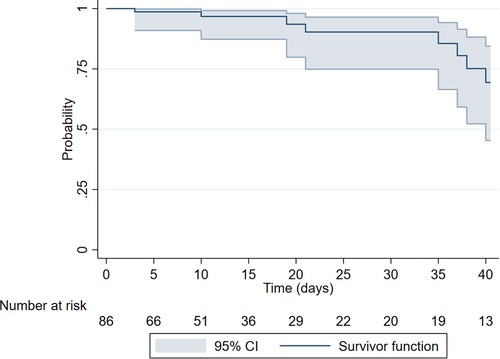
Figure 2. Kaplan–Meier curve of 40-day major complication-free survival following endoscopic gastrostomy.
The analysis of hospital length of stay after gastrostomy demonstrated differences based on the presence of major complications. In patients without major complications, the probability of remaining hospitalized progressively decreased, with only 25.68% (95% CI: 16.40–35.98) still hospitalized by day 20, suggesting that 74.32% had been discharged by that point. In contrast, patients who experienced a major complication showed a more pronounced decline in the probability of remaining hospitalized, with only 33.33% (95% CI: 10.27–58.84) still inpatient by day 15 (p = 0.400) (Figure 3).
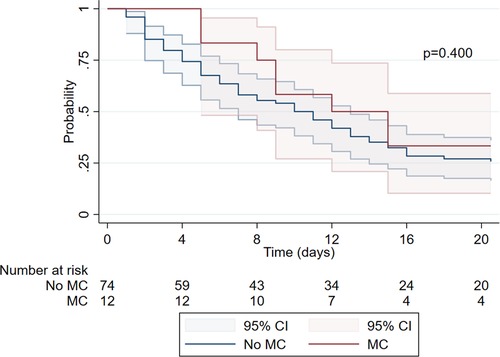
Figure 3. Kaplan–Meier analysis, length of stay post-gastrostomy. MC, major complications present; No MC, no major complications.
Discussion
In this cohort of 86 pediatric patients who underwent PEG, the overall complication rate was 13.95%, which aligns with data reported in the pediatric literature. A similar complication rate of 14% was found in a prospective study involving 103 children, suggesting that the safety profile observed in our population is consistent with previous findings (13). The complication profile was heterogeneous, with minor complications such as mild peristomal infections and feeding intolerance being more frequent than major complications. Of particular note, the presence of severe acute malnutrition and exacerbated chronic malnutrition was more common among those who experienced complications, which, although not statistically significant in our sample, aligns with evidence linking malnutrition to impaired wound healing and infection risk (14). This highlights the need to systematically assess and optimize nutritional status before to PEG placement to reduce the likelihood of postoperative complications.
The occurrence of granulomas and feeding intolerance in our cohort reflects patterns similar to those described internationally; however, the incidence of granuloma formation was lower than in larger studies. This difference suggests that local factors, such as stoma care protocols, caregiver education, nutritional management, and tube selection, may play a critical role in reducing complication rates. Proper wound care and close postoperative monitoring could help prevent excessive tissue irritation and promote better stoma healing, ultimately leading to fewer granulomas and improved feeding tolerance in pediatric patients (15).
BBS emerged as the most frequent major complication. This finding is particularly relevant, as the incidence reported in the literature ranges from 1% to 8%, with some recent studies indicating an increase in specific populations (16, 17). Factors such as the rigidity and material of the gastrostomy tube, as well as the external fixation device's position, can significantly influence the development of BBS. A tight external fixator, improper positioning, and excessive compression between the internal and external bumpers are key etiological factors leading to this complication, as noted in several studies (16, 18). This association is of particular interest in Latin American settings, where variations in resource availability and follow-up protocols may influence both the rate and management of complications (19).
In our cohort, peristomal infections ranked second among major complications and were the most frequent minor complication. This finding is consistent with previous literature, which identifies peristomal infection as one of the most common complications following PEG, with reported rates ranging from 4% to 30% depending on prophylactic measures, postoperative care, and the experience of the clinical team (20). Severe infections, such as gastrostomy-related sepsis, highlight the critical importance of close monitoring and meticulous stoma care to prevent the progression of local infection to systemic complications (21). Factors such as malnutrition, immune compromise, suboptimal hygiene, and variability in follow-up protocols further increase this risk, particularly in pediatric populations (22). Moreover, the lack of standardized caregiver education and perioperative antibiotic prophylaxis can significantly influence infection rates, emphasizing the need for preventive strategies based on international guidelines adapted to local contexts (20, 22).
Our Kaplan–Meier analysis revealed a progressive decline in complication-free survival over the 40-day follow-up period, with the majority of complications occurring within the first few weeks after the procedure. This finding aligns with the international literature, which consistently reports that most complications following PEG placement in pediatric populations arise within the initial 2–4 postoperative weeks. This underscores the critical importance of intensive clinical monitoring during this early post-operative period to promptly identify and manage potential complications, thereby improving patient outcomes and minimizing long-term risks (15).
The analysis of post-PEG hospital stay duration revealed that patients without major complications were typically discharged earlier, demonstrating a reduced probability of prolonged hospitalization. In contrast, those who experienced major complications required longer stays, likely due to the need for more intensive and complex post-operative management. These findings align with those reported by Fox et al. (23), who observed a similar trend in their cohort. The extended hospital stays in patients with complications highlight the critical role of early detection and timely interventions in preventing the escalation of post-operative issues, ultimately contributing to more efficient resource utilization and improved patient outcomes.
This study provides valuable data that enrich the limited evidence available on PEG outcomes in middle-income countries, particularly in Latin America, where original studies on complications are scarce. However, its retrospective design limits the ability to establish causal relationships, and the relatively small sample size may affect the generalizability of the findings, especially regarding the analysis of major complications, which were infrequent. Despite these limitations, our results offer relevant insights into the safety profile and specific challenges faced by pediatric patients in the region, contributing important context to the global understanding of PEG outcomes.
Conclusion
PEG in the pediatric population proved to be a safe procedure, with a low overall complication rate, predominantly involving minor events. However, the relatively high incidence of BBS observed in this cohort underscores the need to strengthen postoperative follow-up, particularly during the early weeks after the procedure.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Comité de Ética en Investigación—CEI de la Fundación Cardiovascular de Colombia. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin. Written informed consent was obtained from the minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Author contributions
CC: Writing – review & editing, Writing – original draft. MR: Data curation, Writing – original draft, Writing – review & editing. VP: Data curation, Writing – review & editing, Writing – original draft. EM: Formal analysis, Methodology, Writing – original draft, Writing – review & editing. AH-O: Formal analysis, Methodology, Writing – original draft, Writing – review & editing. ML-A: Formal analysis, Methodology, Writing – original draft, Writing – review & editing. AM-M: Data curation, Supervision, Conceptualization, Project administration, Validation, Investigation, Resources, Visualization, Software Formal analysis, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Correction Note
A correction has been made to this article. Details can be found at: 10.3389/fped.2025.1701519.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mohajir WA, O’Keefe SJ, Seres DS. Disease-related malnutrition and enteral nutrition. Med Clin North Am. (2022) 106(5S):e1–16. doi: 10.1016/j.mcna.2022.10.002
2. Morales F, Montserrat-de la Paz S, Leon MJ, Rivero-Pino F. Effects of malnutrition on the immune system and infection and the role of nutritional strategies regarding improvements in children’s health status: a literature review. Nutrients. (2023) 16(1):1. doi: 10.3390/nu16010001
3. Pournasiri Z, Bakhtiary M, Nikparast A, Hashemi SM, Ahmadizadeh SN, Behzad A, et al. The association between nutritional status measured by body mass index and outcomes in the pediatric intensive care unit. Front Pediatr. (2024) 12:1421155. doi: 10.3389/fped.2024.1421155
4. Molina VC, Ja VR, Gallardo SF. Percutaneous endoscopic gastrostomy. Indications, care and complications. Med Clin. (2019) 152(6):229–36. doi: 10.1016/j.medcli.2018.09.008
5. Preiser JC, van Zanten ARH, Berger MM, Biolo G, Casaer MP, Doig GS, et al. Metabolic and nutritional support of critically ill patients: consensus and controversies. Critical Care. (2015) 19(1):35. doi: 10.1186/s13054-015-0737-8
6. Estevão-Costa J. Artificial nutrition in children (I): enteral access. Acta Med Port. (2014) 27(5):634–40. doi: 10.20344/amp.5312
7. Tae CH, Lee JY, Joo MK, Park CH, Gong EJ, Shin CM, et al. Clinical practice guideline for percutaneous endoscopic gastrostomy. Gut Liver. (2024) 18(1):10–26. doi: 10.5009/gnl230146
8. Rahnemai-Azar AA, Rahnemaiazar AA, Naghshizadian R, Kurtz A, Farkas DT. Percutaneous endoscopic gastrostomy: indications, technique, complications and management. World J Gastroenterol. (2014) 20(24):7739. doi: 10.3748/wjg.v20.i24.7739
9. Boeykens K, Duysburgh I, Verlinden W. Prevention and management of minor complications in percutaneous endoscopic gastrostomy. BMJ Open Gastroenterol. (2022) 9(1):e000975. doi: 10.1136/bmjgast-2022-000975
10. Tazi K, Kotilea K, Dassonville M, Bontems P. Complications of percutaneous and surgical gastrostomy placements in children: a single-centre series. JPGN Rep. (2023) 4(2):e316. doi: 10.1097/PG9.0000000000000316
11. McCarthy A, Delvin E, Marcil V, Belanger V, Marchand V, Boctor D, et al. Prevalence of malnutrition in pediatric hospitals in developed and in-transition countries: the impact of hospital practices. Nutrients. (2019) 11(2):236. doi: 10.3390/nu11020236
12. Clavien PA, Sanabria JR, Strasberg SM. Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery. (1992) 111(5):518–26.1598671
13. Brewster BD, Weil BR, Ladd AP. Prospective determination of percutaneous endoscopic gastrostomy complication rates in children: still a safe procedure. Surgery. (2012) 152(4):714–9; discussion 719–21. doi: 10.1016/j.surg.2012.07.018
14. Wondemagegnehu BD, Aklilu WK, Beyene MD, Nonyane BAS. Impact of malnutrition on the outcome and length of hospital stay in elective pediatric surgical patients: prospective cohort study at tertiary hospitals in Ethiopia. BMC Nutr. (2023) 9(1):127. doi: 10.1186/s40795-023-00788-9
15. Balogh B, Kovács T, Saxena AK. Complications in children with percutaneous endoscopic gastrostomy (PEG) placement. World J Pediatr. (2019) 15(1):12–6. doi: 10.1007/s12519-018-0206-y
16. Cyrany J, Rejchrt S, Kopacova M, Bures J. Buried bumper syndrome: a complication of percutaneous endoscopic gastrostomy. World J Gastroenterol. (2016) 22(2):618–27. doi: 10.3748/wjg.v22.i2.618
17. Menni A, Tzikos G, Chatziantoniou G, Gionga P, Papavramidis TS, Shrewsbury A, et al. Buried bumper syndrome: a critical analysis of endoscopic release techniques. World J Gastrointest Endosc. (2023) 15(2):44–55. doi: 10.4253/wjge.v15.i2.44
18. Stewart CE, Mutalib M, Pradhan A, Bassett C, Drake D, Upadhyaya M. Short article: buried bumper syndrome in children: incidence and risk factors. Eur J Gastroenterol Hepatol. (2017) 29(2):181–4. doi: 10.1097/MEG.0000000000000758
19. Devia J, Santivañez JJ, Rodríguez M, Rojas S, Cadena M, Vergara A. Early recognition and diagnosis of buried bumper syndrome: a report of three cases. Surg J. (2019) 5(3):e76–81. doi: 10.1055/s-0039-1692148
20. Summers BB, Yates M, Cleveland KO, Gelfand MS, Usery J. Fidaxomicin compared with oral vancomycin for the treatment of severe clostridium difficile-associated diarrhea: a retrospective review. Hosp Pharm. (2020) 55(4):268–72. doi: 10.1177/0018578719844165
21. Saito T, Tatara K, Kawai M. Changes in clinical condition and causes of death of inpatients with Duchenne muscular dystrophy in Japan from 1999 to 2012. Rinsho Shinkeigaku. (2014) 54(10):783–90. doi: 10.5692/clinicalneurol.54.783
22. Park SW, Do HS, Kim D, Ko JY, Lee SH, Han YM. Transcriptional profiles of imprinted genes in human embryonic stem cells during in vitro differentiation. Int J Stem Cells. (2014) 7(2):108–17. doi: 10.15283/ijsc.2014.7.2.108
Keywords: endoscopy, gastrostomy, pediatrics, postoperative complications, enteral nutrition
Citation: Cuadros Mendoza CA, Rosero Portilla MJ, Pico Quintero V, Manrique-Hernández EF, Hurtado-Ortiz A, Licht-Ardila M and Mendoza-Monsalve A (2025) Complications and clinical factors associated with pediatric percutaneous endoscopic gastrostomy in a Colombian cohort. Front. Pediatr. 13:1623355. doi: 10.3389/fped.2025.1623355
Received: 5 May 2025; Accepted: 18 July 2025;
Published: 11 August 2025;
Corrected: 18 September 2025.
Edited by:
Anna Maria Lavezzi, University of Milan, ItalyReviewed by:
Michael Wilsey, University of South Florida, United StatesRajmohan Dharmaraj, University of New Mexico, United States
Copyright: © 2025 Cuadros Mendoza, Rosero Portilla, Pico Quintero, Manrique-Hernández, Hurtado-Ortiz, Licht-Ardila and Mendoza-Monsalve. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Edgar Fabián Manrique-Hernández, ZmFiaWFubWgxOTkzQGdtYWlsLmNvbQ==
†ORCID:
Carlos Augusto Cuadros Mendoza
orcid.org/0000-0003-3336-4575
Mario Javier Rosero Portilla
orcid.org/0009-0000-3105-9134
Verónica Pico Quintero
orcid.org/0009-0006-5855-9431
Edgar Fabián Manrique-Hernández
orcid.org/0000-0002-3634-8821
Alexandra Hurtado-Ortiz
orcid.org/0000-0002-3001-2374
Maricel Licht-Ardila
orcid.org/0000-0002-1629-9890
Alejandra Mendoza-Monsalve
orcid.org/0000-0002-6556-1808