 Antonia Maximina Pfennigs
Antonia Maximina Pfennigs Manuel Besendörfer
Manuel Besendörfer Sonja Diez
Sonja Diez Bertram Reingruber
Bertram Reingruber- 1Clinic for Pediatric Surgery and Traumatology, Florence Nightingale Hospital, Düsseldorf, Germany
- 2Department of Pediatric Surgery, University Hospital Erlangen, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany
Background: A perfusion mismatch in the premature gut is the key component in the development of necrotizing enterocolitis (NEC). Resulting necroses need to be surgically excised, while intestinal salvage is crucial to the survival and rehabilitation of affected preterm neonates. Until now, resection margins have been based on standard visual inspection and surgical experience due to the lack of objective criteria for bowel viability. We hypothesize that by evaluating the vitality and perfusion during NEC surgery, necrosis margins can reliably be defined by indocyanine green (ICG) fluorescent imaging, a real-time visualization method, which has already been implemented safely in pediatric surgery for other indications.
Materials and methods: In a prospective study at our Level 1 Perinatal Center, patients were recruited after primary emergency surgery confirming NEC. Due to the acute phase of the inflammatory process, the extent and dynamics cannot be clearly defined at this point. Informed consent of the parents for the second-look surgery included ICG fluorescent imaging (0.04–0.7 mg/kg body weight), which was applied after completely exposing the intestinal bundle to visualize blood perfusion intraoperatively. ICG perfusion of intestinal tissue was visualized by a near-infrared camera and was compared with bowel vitality as judged conventionally by an experienced surgeon. Based on the findings, further treatment was specified. We correlated our surgical findings with subsequent histopathology.
Results: Six patients treated at our perinatal center met the inclusion criteria. In four patients, ICG-negative, non-vital gut areas were detected and resected with narrow margins of <1 mm. Histology and the further medical course proved to be consistent with these intraoperative results. In two patients, the clinical appearance of complete necrosis of the small intestines was confirmed by ICG fluorescence, supporting the decision to provide palliative treatment. In two out of six patients, clinical judgment and real-time ICG fluorescence were contradictory. Here, histopathology confirmed complete necrosis of the bowel in full accordance with ICG.
Conclusion: Our prospective cohort study gave evidence for ICG fluorescence to be useful and reliable in objectifying blood perfusion and intestinal vitality during NEC surgery, adding objectiveness to the surgeon's personal experience.
1 Introduction
Conditions consistent with necrotizing enterocolitis (NEC) were described two centuries ago by Charles Billard (1). Although there have been improvements in the care of neonates, especially those with very low birth weight (VLBW) or extremely low birth weight (ELBW), approximately 7% of VLBW infants in neonatal intensive care units (NICU) develop NEC (2–4).
Bell et al. (5) published a classification system for the diagnosis and staging of NEC in 1978, which was modified a few years later. Proven NEC at Bell Stage III, also referred to as advanced or surgical NEC, requires surgical intervention. Clinical trials showed no significant difference in the outcomes of interventional placement of an abdominal drainage to open surgical exploration (6). By the nature of the procedure, laparotomy provides a good overview of the spreading pattern and the severity of the disease. In any case, surgery should not take more than 45 min to minimize stress on the frail organism (7). Several revisions are usually necessary (8–11). Essential to all surgical procedures is the preservation of the maximum length of bowel, while avoiding intestinal spillage and sparing the organism from inflammation and the metabolic burden of necrosis (12–15). Limiting necrosectomy and maximizing bowel preservation are crucial, and yet it is challenging to avoid early complications such as anastomotic leakage and late complications such as intestinal failure and short bowel syndrome (SBS).
As neonatal care has improved, the incidence of NEC has declined. Case numbers dropped by nearly 50% over the last two decades in Germany (16), and there was a corresponding drop in the surgical intervention rate. Consequently, surgical training and the multiplication of surgical experience in NEC surgery have become challenging. With less practice, the surgeon's ability to assess gut recovery may decline, potentially provoking multiple revision laparotomies. New methods for intraoperative judgment of intestinal vitality, including the pattern and the extent of visceral blood perfusion, may provide enough safety to refrain from multiple revisions. This technique should be sensitive, specific, reliable, and safe, especially in the early phase of the disease, as a conventional and clearly visible clinical demarcation of necrotic bowel tissue can take several days to develop and might otherwise increase the number of revision laparotomies.
A method to visualize intestinal perfusion via near-infrared fluorescence optical imaging (FOI) is indocyanine green (ICG) optical imaging. Originally developed for near-infrared photography, ICG was approved for clinical use in 1956. Binding with blood lipoproteins, ICG shows little tissue leakage, making it ideal to visualize tissue blood perfusion. When illuminated at 750–800 nm wavelength, emissions can be observed at a wavelength shortly over 800 nm with a near-infrared camera (17). It has found multiple applications over the last few decades, which led to great improvements in diagnostic methods and surgical outcomes in a variety of applications where perfusion is of key importance, such as anastomosis, tumor margins, chronic inflammation, or visualization of blood circulation patterns (18, 19). ICG is a non-toxic, non-ionic molecule, and its adverse effects, such as allergic flush or discoloration of the skin, range between 0.15% and 0.05% with no deaths reported so far (17, 20). Recent publications have shown that ICG has already found its way into pediatric surgical procedures, where it, for example, can be used to map the thoracic duct during esophageal atresia procedures and to prevent chylothorax or to visualize the perfusion during reconstructive surgery of anorectal malformations or during a Palomo procedure in pediatric urology (21–23). A pilot study using ICG as an additive during the Kasai procedure in neonates with biliary atresia showed an improved postoperative normalization of bilirubin levels (24, 25). Furthermore, in a prospective mixed clinical trial, ICG proved to be a safe and feasible tool for visualizing blood perfusion during pediatric intestinal resections (26).
Piglet models have shown promising advantages and high practicability in assessing intestinal perfusion in induced ischemia and inflammatory processes of the small intestine (27). ICG has been shown to be beneficial in evaluating intestinal perfusion in a piglet model of induced NEC (28). We therefore suggest introducing this well-established method into perinatal surgery and specifically NEC surgery, thereby implementing a tool that will objectify intraoperative and real-time judgment of intestinal viability and perfusion in cases of NEC.
2 Materials and methods
2.1 Patient population
The study's cohort was generated prospectively, including patients treated from 2018 to 2024 in the NICU department of the Florence Nightingale Hospital, Düsseldorf, Germany. The inclusion criteria included NEC Stage Bell III with indication for surgical treatment in the neonatal period and extensive bowel inflammation over a major portion of the intestines, necessitating a second-look procedure. Furthermore, imminent short gut syndrome or complete bowel ischemia were used as criteria for inclusion, whereas patients with a substantial length of healthy gut were excluded. Patients with focal intestinal perforation (FIP), meconium ileus, and limited, uni-segmental or focal NEC were excluded, as they would not benefit from a second-look operation (Figure 1). Informed consent was obtained for all participants from their next of kin.
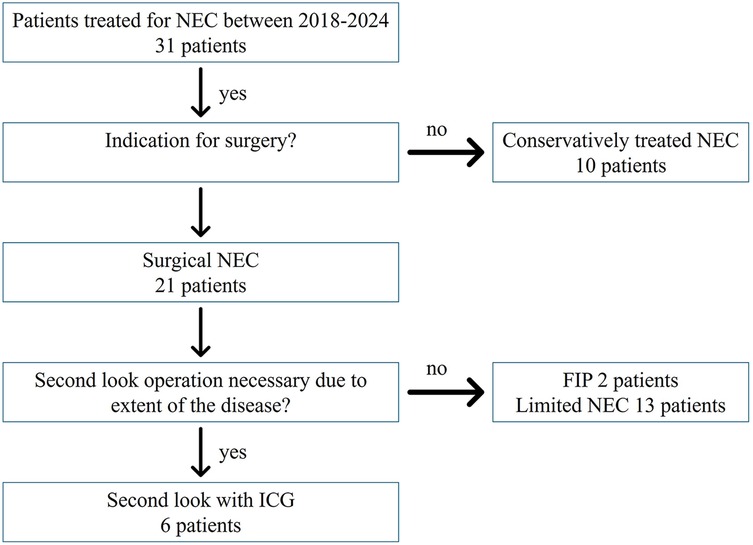
Figure 1. With a total cohort of 31 patients treated for NEC at our hospital, 10 patients were managed conservatively. Out of 21 patients with surgical intervention, 2 had a FIP, and 13 had only limited NEC. Six patients underwent a second-look operation with ICG and were analyzed for this study.
2.2 Clinical findings, diagnostic imaging, and indication for surgery
Patients received enteral feeding either via nasogastric tube or per mouth with breast milk or, if not available, preterm infant formula and NEC prevention with probiotics according to the standard in our German Level 1 NICU (corresponding levels: UK: 3; USA: 4) (29). Diagnostic imaging upon suspected NEC included bedside ultrasound with findings of portal venous gas and bedside x-rays to look for pneumoperitoneum. In case of NEC diagnosis, conservative treatment was initiated, including antibiotic treatment and fasting. To monitor disease progression, blood tests included leucocyte count, C-reactive protein, and IL6. There was an interdisciplinary discussion about the indication for surgery, considering the signs of pneumoperitoneum and clinical deterioration despite fully escalated conservative management.
Primary exploratory laparotomy was performed bedside in the NICU by an experienced pediatric surgeon, and unmistakably necrotic and disintegrated bowel was removed. Any bowel segments still showing intact wall structures were preserved, even if appearing non-vital, and a second-look procedure was scheduled 2–4 days later. A bowel ostomy was created at the most proximal point of the disease. If the extent of the disease in the first exploratory surgery was of critical extent, suggesting that ICG visualization could be beneficial to improve the identification of resection margins in the second-look operation, the second-look procedure was planned with ICG. In between the procedures, the patients received parenteral nutrition and empirical antibiotic treatment with vancomycin and meropenem, which was adapted based on the subsequent pattern of antibiotic sensitivity further on. Patients were continuously monitored in the NICU, thereby optimizing blood pressure and oxygenation, while remaining intubated and mechanically ventilated.
2.3 Application of ICG
ICG visualization was performed during the scheduled second-look surgery either in the NICU or operating room, depending on the patient's hemodynamic stability. Upon second-look laparotomy and after adhesiolysis of the intestines, 0.04–0.7 mg/kg Verdye® (Diagnostic Green Ltd., Athlone, Westmeath, Ireland) according to the manufacturer's recommendations was intravenously applied unfiltered by the anesthesiologist once the bowel was fully exposed. As a useful monitoring device to track the onset of ICG flow, we used the oxygen saturation sensor, which monitors ventilation and oxygenation by the anesthesiologist as part of the regular anesthesia setup. The flow and spreading of ICG were monitored through subtle changes within a few seconds in the sensor, as this also operates within the near-infrared spectrum. The effect of the ICG on the sensor was observed as a drop in the saturation of <15%, only lasting a few seconds, while the ICG fluorescence persisted. Visualization of intestinal perfusion was achieved using either the mobile Novadaq® Pinpoint Endoscopic Fluorescence imaging system or the Storz Image1 4K endoscopic tower, immediately after application of ICG. With the assistant holding the camera device at a 90° angle, approximately 30 cm above the exposed bowel, the intestine was systematically inspected by the senior surgeon. The direct clinical appearance in the operating field was compared with the blood perfusion as visualized by ICG imaging. The colon and stomach served as reliable positive controls for a solid ICG signal. Any fluorescence signal similar to the stomach and colon was regarded as a positive signal; a faint or non-existent signal was regarded as ICG negative. All non-perfused segments of bowel were resected precisely at their demarcation. Finally, ICG imaging was conducted to confirm perfusion of the remaining bowel. Surgical sites were documented by digital photography (Figure 2).
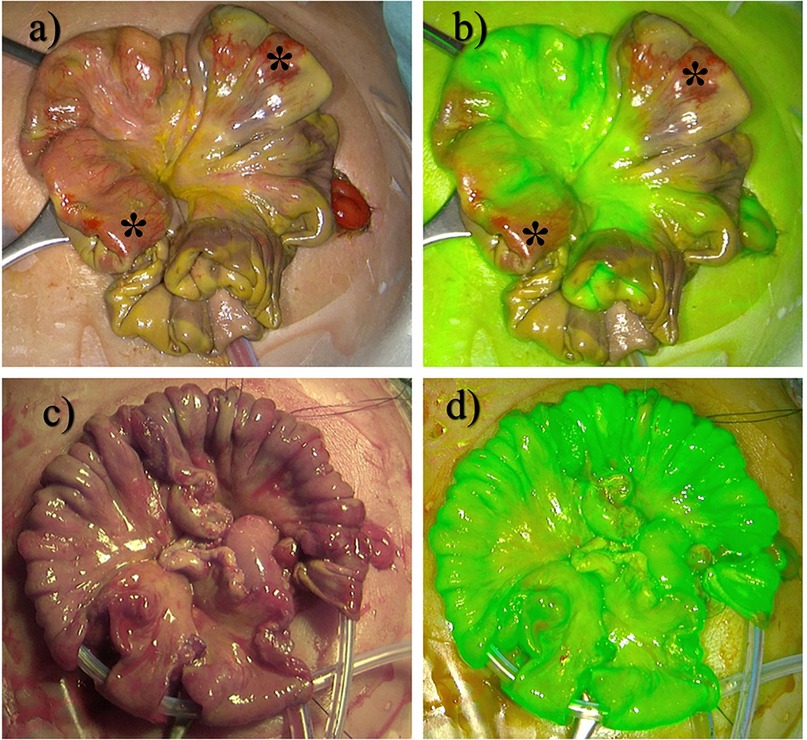
Figure 2. (a) Intraoperative site of a patient with NEC Stage Bell III. (b) ICG visualization of (a). (c) Successful resection of necrotic areas. (d) ICG fluorescence control after resection. *indicates non-perfused areas still looking vital.
2.4 Statistical analyses
Data were recorded as quantitative variables or categorical factors. For quantitative or ordinally scaled data, the median value together with the minimum and maximum values were given. For qualitative factors, absolute and relative frequencies were assessed. Imaging ICG diagnostics were compared with macroscopic intra-abdominal findings during the surgical procedures.
3 Results
3.1 Demographic data
Between 2018 and 2024, a total of 31 patients were treated for NEC in our hospital. In 21 patients (68%), the indication for surgery was Bell Stage III. Of the 21 patients, 2 (10%) whose intraoperative findings showed a FIP and 13 (62%) with focal or limited NEC were excluded from the case series. In 6 (29%) out of 21 patients, intraoperative findings showed extensive disease, meeting our criteria for ICG imaging. Demographic data are summarized in Table 1. Patients included were born between 24 and 27 weeks of gestational age, with a median age at surgery of 24 days (range 4–44 days). Birth weight ranged between 400 and 1,030 g with a median of 1,700 g.

Table 1. Demographic data of the participants.
3.2 Surgical management
To increase reproducibility, the comparison between macroscopic findings and ICG was carried out by the same senior surgeon. First-look surgery of our study cohort without ICG was 75 min (range 36–144 min), median operation time in second-look surgery including ICG was 11% higher at 83 min (range 27–228 min).
In four out of six patients in the study group, clinical judgment of critical bowel lesions was consistent with ICG imaging, leading to resection in one session and restoring continuity by end-to-end anastomoses. In two of these patients, ICG imaging showed no perfusion, whereas the intestine appeared healthy on standard visual inspection. These areas were inspected thoroughly by the operating senior surgeon, which were subsequently proven non-vital by carefully controlled incision and absence of bleeding and therefore dissected. Histopathology later confirmed these findings. A reason for this mismatch of the surgeon's perception and the ICG signal could not be identified, as there were no differences regarding disease severity or medical handling, including a constant team of medical personnel. A diverting ostomy was created at the most proximal defect to allow for early enteral feeding while the multiple anastomoses of the distal, aboral intestine were allowed to heal. Antibiotics were continued and, if necessary, adapted to microbiological findings.
In the other two patients, complete ischemia of the entire small intestine was already suspected at the primary operation. A diverting proximal jejunostomy was performed. By the time of the scheduled second-look operation, the whole small intestine was thoroughly examined macroscopically and via ICG for any signs of substantial blood perfusion and was judged completely ischemic on macroscopic examination, as well as by ICG imaging (Figure 3). The presumed occlusion of the superior mesenteric artery resulting in complete bowel necrosis was subsequently confirmed by histopathology. Surgical findings are summarized in Table 2.
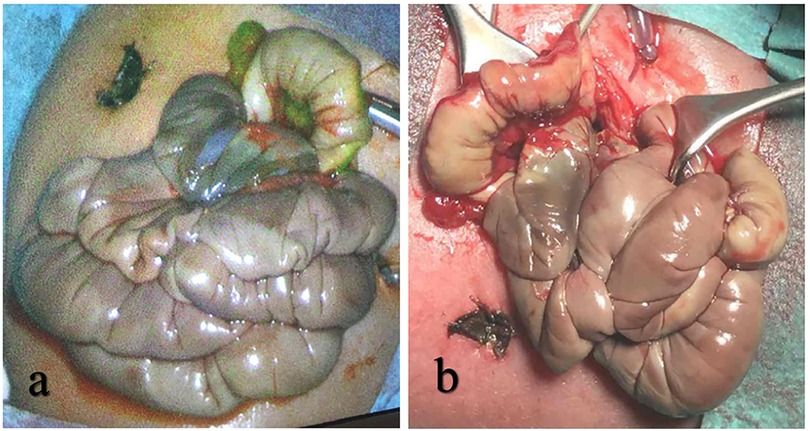
Figure 3. (a) ICG fluorescence shows no signal of blood perfusion. (b) Examination of the gut reveals non-vital and necrotic tissue.

Table 2. Surgical data and outcome of participants.
3.3 Postoperative management and follow-up
Histopathological examination of the resected specimens confirmed complete necrosis with barely recognizable wall structures or full-thickness bowel necrosis and extensive pneumatosis intestinalis, notably so in all areas where a negative ICG signal stood in contrast to conventional macroscopic findings.
Oral feeding started only a few days after surgery. Once the critical phase was managed, radiologic contrast imaging of the efferent bowel loop was carried out to confirm bowel sufficiency. Antibiotic treatment was terminated once blood parameters had normalized. The defunctioning stoma was reversed in a limited local procedure after 8–21 weeks.
Two patients died within 2 weeks of second-look surgery under palliative care following the occlusion of the superior mesenteric artery. Follow-up of the four remaining patients was conducted at a median interval of 16.5 months (range 8–45 months). SBS persisted for 7–9 months postoperatively in all four patients. At the final follow-up, the weaning process of parenteral nutrition was successful in 75% (n = 3), with one patient in need of parenteral nutrition for a few hours during the night. In summary, in the six patients evaluated with ICG during second-look surgery, the operating surgeon's perception was supported in four out of six cases. In two out of six cases, ICG proved to be superior to the surgeon's assessment of the gut, where a negative ICG signal was confirmed as a complete necrosis afterwards by histopathology. We monitored our patients closely for potential side effects such as signs of an allergic reaction due to the dye's iodine base or persistent discoloration of any tissue. No side effects of ICG described in the literature, such as allergic reaction, flush, or persistent discoloration of the skin, were detected during the course of our study.
4 Discussion
We present a prospective study of intravenous application of ICG in six preterm infants with NEC aiming to improve assessment of gut perfusion during second-look surgery. In our study, ICG appeared to be superior in terms of indicating blood perfusion and tissue vitality, even to the judgment of an experienced senior pediatric surgeon. Only a few comparable studies exist, none of which investigated the safety and benefit of ICG for this indication and in this population and age group. Previous studies were able to demonstrate that the use of ICG in neonates is safe for multiple indications, including surgery in biliary atresia and esophageal atresia (17). A study conducted in Canada investigated the safety and feasibility of ICG imaging in pediatric bowel resections in general, including, but not particularly for, NEC. A substantial ICG signal could be observed even during emergency surgeries and NEC surgery in premature infants. While the general safety and feasibility of the method could be confirmed, a higher mismatch rate of 62% compared with our mismatch rate of 33% between the surgeon's perception and ICG fluorescence was described (26).
Even though ICG has been applied for various surgical indications within adult surgery for more than half a century, its implementation in pediatric surgery started less than half a decade ago. It has been approved for intravenous use in adults, adolescents, and children (21–23). We hypothesize its feasibility in a neonatal population with NEC based on the following aspects:
1. Whenever surgery is indicated in NEC, its primary aim should be to preserve as much bowel as possible while clearing the abdomen and the organism from the metabolic load of toxic bowel necrosis. SBS is a severe, life-altering, and determining condition, which must be avoided by any means. Any additional diagnostic measure to visualize intestinal perfusion might help improve the outcome of this population and prevent an excessive bowel resection. It can be discussed whether ICG might already add benefit during the primary exploratory surgery. However, the primary surgery in NEC is characterized as a short damage control procedure within an ongoing inflammatory process, aiming at intestinal rescue by diversion ostomy as a gentle procedure with the shortest possible operating time to protect the frail organism. Second-look surgery, as a scheduled surgery after several days of stabilization, presents an opportunity to take reconstructive steps. Improved identification of the resection margins of vital bowel by visualizing blood perfusion via ICG fluorescence can help avoid excessive resection and promote bowel reconstruction by avoiding multiple revision operations. This aligns with the observations previously described in the literature, where areas with mixed ICG signal during NEC surgery showed a subsequent stenosis on a revision later on (26).
2. As understanding, prophylaxis, and conservative treatment of NEC continue to improve, the incidence of advanced NEC in Germany declines, as well as the number and proportion of surgical interventions and therefore surgical experience for this condition in general. Therapeutic success depends on experience and diagnostic precision. Even with long surgical experience, the real-time judgment of intestinal perfusion can be challenging and, if indeterminate, might demand several revision laparotomies or risk an extensive loss of intestinal length. Intraoperative fluorescent imaging with ICG supports the discrimination of intestinal tissue worth preserving via real-time blood perfusion in a non-invasive, radiation-free manner to increase diagnostic precision safety and thereby assist clinical judgment in case of prognostic uncertainty. In two cases in our study, ICG proved to be superior even to the experienced surgeon's eye, facilitating an easier and quicker removal of non-vital gut sections. Histopathology showed a full necrosis in these cases. However, these cases were neither more severe nor were the blood circulation exceedingly impaired compared with the other cases. ICG might therefore have shown a perfusion mismatch before the full necrotic demarcation took place.
3. Centralization in healthcare is often used to aggregate surgical experience when facing small operative numbers in elective procedures. However, any centralization of NEC treatment in specialized, high-volume hospitals must be weighed against studies that have shown that emergency transport prior to surgery might not only cause time delay but also generate additional complications and increase mortality of these frail neonates (30–32).
Having been used for retinal screening and measuring cardiac output since the 1960s, ICG has more recently found its way into several segments of surgical and interventional medicine (33). It proved useful to detect sentinel lymph nodes in breast cancer, to clarify anatomic structures in hepatobiliary surgery, and to increase the safety of anastomoses in colorectal surgery. Lately, it has also been successfully implemented in emergency surgery, and a variety of handheld or endoscopic camera-bound visualizing devices are on the market (34–39). Recently, it has found its way into pediatric surgery and urology, with so far limited experience in neonates and preterm infants (21, 23). A potentially beneficial role in the context of NEC surgery has been shown by Knudsen et al. (28) in a piglet model. Based on the experience of over sixty years, ICG acts with only a few side effects, such as subcutaneous retention and rare allergic reactions, and appears safe to use in the latest pediatric analyses (26, 40, 41). However, larger population studies are also needed to address possible side effects. In our study, ICG proved to be superior to the surgeon's assessment alone, as some portions of bowel, conventionally judged vital, showed no ICG signal. All areas demonstrated no bleeding upon incision and proved to be necrotic in histopathological examination. However, the surgeon's assessment should remain cautious as reduced perfusion rates in hemodynamically unstable patients might have an influence on ICG distribution and therefore its value. Further studies are needed to evaluate this important aspect.
Surgery for NEC can be challenging even for the experienced surgeon, and the outcome is often dependent on subjective variables and intraoperative decisions. Therefore, a reliable, efficient, and widely available diagnostic tool such as ICG may not only compensate for decreasing surgical exposure to this condition but may also decisively contribute to improving intraoperative decision making, standardization, and possibly even case discussion via telemedicine. Prospectively, ICG visualization could add safety in cases with limited NEC, which could be suitable for primary anastomosis. This might be especially interesting for higher volume centers, in which ICG might reduce a dependence on subjective interpretation of gut vitality. In addition, in the case of defining fatal intestinal ischemia, the extent of the disease can be visualized and demonstrated objectively and earlier in its course. In these cases, therapeutic limits can be discussed with the parents under ethical criteria, avoiding prolonged periods of uncertainty.
This study has several limitations. Based on the low incidence of NEC, the study population is small. Although we included the study's participants prospectively, indications for ICG might be biased in this heterogeneous population, including a large age span at primary operation, cardiac abnormalities, and differences in feeding. A control group without ICG would have been helpful to show whether the application of the ICG procedure time or shortens the operating time by improving efficiency. Other aspects of interest would be a comparison of the potential benefits of time to oral feeding in the ICG group, length of hospital stay, and length of dependence on parenteral nutrition. A historical matched pair analysis would be useful; however, due to the individuality of each case, comparability might be limited. In addition, ICG was solely administered during second-look surgery in our study population. Therefore, the patients had already reached stability in blood circulatory support. Additional exploratory research is needed to ascertain whether the ICG signal is reliable when used in a hemodynamically unstable patient. In general, ICG visualization has proven to be safe and feasible in NEC surgery in our institution, and we will continue to recruit patients and to increase data on the benefit of this new indication. Multicentric studies would also be desirable.
5 Summary
ICG fluorescence imaging is a widely available and safe diagnostic tool. With its reliability in visualizing real-time intestinal perfusion, ICG can be used to significantly improve the judgment of gut viability during exploratory laparotomy, as could be demonstrated in this present prospective study. This allows for an early and precise definition of the resection margins of necrotic bowel, regardless of patient specificities or the individual experience of the performing surgeon. Hereby, the metabolic burden of gut necrosis can be eliminated early, and the number of surgical interventions can be minimized without sacrificing bowel length preemptively or due to the limits of conventional discrimination in surgical perception. ICG can support the prognosis of intestinal restitution and, if unfavorable, support a decision for palliative treatment to avoid unnecessary suffering. In the future, a multicenter study comparing outcomes considering overall survival, enteric independence, and time to recovery between ICG-guided resection and conventional procedures could further illuminate the benefit of ICG in NEC surgery while also evaluating possible adverse effects of ICG administration.
Author's note
The present work was performed in fulfillment of the requirements for obtaining the degree “Dr. med.” of Antonia Maximina Pfennigs.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethikkommission des Fachbereichs Medizin der Goethe-Universität Frankfurt am Main. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
AP: Conceptualization, Writing – original draft. MB: Writing – review & editing. SD: Supervision, Writing – review & editing. BR: Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence, and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Hackam D, Caplan M. Necrotizing enterocolitis: pathophysiology from a historical context. Semin Pediatr Surg. (2018) 27(1):11–8. doi: 10.1053/j.sempedsurg.2017.11.003
2. Alsaied A, Islam N, Thalib L. Global incidence of necrotizing enterocolitis: a systematic review and meta-analysis. BMC Pediatr. (2020) 20:344. doi: 10.1186/s12887-020-02231-5
3. Guthrie SO, Gordon PV, Thomas V, Thorp JA, Peabody J, Clark RH. Necrotizing enterocolitis among neonates in the United States. J Perinatol. (2003) 23(4):278–85. doi: 10.1038/sj.jp.7210892
4. Llanos AR, Moss ME, Pinzòn MC, Dye T, Sinkin RA, Kendig JW. Epidemiology of neonatal necrotising enterocolitis: a population-based study. Paediatr Perinat Epidemiol. (2002) 16(4):342–9. doi: 10.1046/j.1365-3016.2002.00445.x
5. Bell MJ, Ternberg JL, Feigin RD, Keating JP, Marshall R, Barton L, et al. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann Surg. (1978) 187(1):1–7. doi: 10.1097/00000658-197801000-00001
6. Blakely ML, Tyson JE, Lally KP, Hintz SR, Eggleston B, Stevenson DK, et al. Initial laparotomy versus peritoneal drainage in extremely low birthweight infants with surgical necrotizing enterocolitis or isolated intestinal perforation: a multi center randomized clinical trial. Ann Surg. (2021) 274(4):e370–80. doi: 10.1097/SLA.0000000000005099
7. Arul GS, Singh M, Ali AM, Gee OJ. Damage control surgery in neonates: lessons learned from the battlefield. J Pediatr Surg. (2019) 54(10):2069–74. doi: 10.1016/j.jpedsurg.2019.04.001
8. Pang KKY, Chao NSY, Wong BPY, Leung MWY, Liu KKW. The clip and drop back technique in the management of multifocal necrotizing enterocolitis: a single centre experience. Eur J Pediatr Surg. (2012) 22(1):85–90. doi: 10.1055/s-0031-1291287
9. Yue M, Yang H, Cui M, Yuan Y, Zhang N, Zhang X, et al. The safety and effectiveness of Santulli enterostomy in neonatal intestinal conditions. Front Pediatr. (2023) 10:1077346. doi: 10.3389/fped.2022.1077346
10. Gfroerer S, Fiegel H, Schloesser RL, Rolle U. Primary laparotomy is effective and safe in the treatment of necrotizing enterocolitis. World J Surg. (2014) 38(10):1. doi: 10.1007/s00268-014-2615-y
11. Svenningsson A, Borg H, Hagander L, Engstrand Lilja H. Surgical management of necrotising enterocolitis in Sweden: a national cohort study. Acta Paediatr. (2023) 112(8):1683–8. doi: 10.1111/apa.16836
12. Golubkova A, Hunter CJ. Updates and recommendations on the surgical management of NEC. Semin Perinatol. (2023) 47(1):151698. doi: 10.1016/j.semperi.2022.151698
13. Davidson JR, Omran K, Chong CKL, Eaton S, Edwards AD, Yardley IE. Exploring growth failure in neonates with enterostomy. J Pediatr Surg. (2024) 59(2):211–5. doi: 10.1016/j.jpedsurg.2023.10.010
14. Peter C, Abukhris A, Brendel J, Böhne C, Bohnhorst B, Pirr S. Growth and duration of inflammation determine short- and long-term outcome in very-low-birth-weight infants requiring abdominal surgery. Nutrients. (2023) 15(7):1668. doi: 10.3390/nu15071668
15. Pardy C, Berkes S, D’Souza R, Fox G, Davidson JR, Yardley IE. Complete resection of necrotic bowel improves survival in NEC without compromising enteral autonomy. J Pediatr Surg. (2024) 59(2):206–10. doi: 10.1016/j.jpedsurg.2023.10.012
16. GENESIS-Online. Krankenhauspatienten: Deutschland, Jahre, Hauptdiagnose ICD-10 (1-3-Steller Hierarchie) (2024). Available online at: https://www-genesis.destatis.de/datenbank/online/ (Accessed November 12, 2024).
17. Alander JT, Kaartinen I, Laakso A, Pätilä T, Spillmann T, Tuchin VV, et al. A review of indocyanine green fluorescent imaging in surgery. Int J Biomed Imaging. (2012) 2012:940585. doi: 10.1155/2012/940585
18. Reinhart MB, Huntington CR, Blair LJ, Heniford BT, Augenstein VA. Indocyanine green: historical context, current applications, and future considerations. Surg Innov. (2016) 23(2):166–75. doi: 10.1177/1553350615604053
19. Son GM, Ahn HM, Lee IY, Ha GW. Multifunctional indocyanine green applications for fluorescence-guided laparoscopic colorectal surgery. Ann Coloproctology. (2021) 37(3):133–40. doi: 10.3393/ac.2021.05.07
20. Hope-Ross M, Yannuzzi LA, Gragoudas ES, Guyer DR, Slakter JS, Sorenson JA, et al. Adverse reactions due to indocyanine green. Ophthalmology. (1994) 101(3):529–33. doi: 10.1016/S0161-6420(94)31303-0
21. Delgado-Miguel C, Camps J, Hernandez Oliveros F. The role of indocyanine green in pediatric gastrointestinal surgery: systematic review. Eur J Pediatr Surg. (2024) 34(1):2–8. doi: 10.1055/a-2123-5433
22. Zundel S, Szavay P. Para-testicular injection of indocyanine green for laparoscopic immunofluorescence-guided lymphatic-sparing Palomo procedure: promising preliminary results. J Pediatr Urol. (2024) 20(3):530–2. doi: 10.1016/j.jpurol.2024.02.023
23. Esposito C, Coppola V, Conte FD, Cerulo M, Esposito G, Farina A, et al. Near-infrared fluorescence imaging using indocyanine green (ICG): emerging applications in pediatric urology. J Pediatr Urol. (2020) 16(5):700–7. doi: 10.1016/j.jpurol.2020.07.008
24. Hirayama Y, Iinuma Y, Yokoyama N, Otani T, Masui D, Komatsuzaki N, et al. Near-infrared fluorescence cholangiography with indocyanine green for biliary atresia. Real-time imaging during the Kasai procedure: a pilot study. Pediatr Surg Int. (2015) 31(12):1177–82. doi: 10.1007/s00383-015-3799-4
25. Sincavage J, Gulack BC, Zamora IJ. Indocyanine green (ICG) fluorescence-enhanced applications in pediatric surgery. Semin Pediatr Surg. (2024) 33(1):151384. doi: 10.1016/j.sempedsurg.2024.151384
26. Le-Nguyen A, Bourque CJ, Trudeau MO, Ducruet T, Faure C, Piché N. Indocyanine green fluorescence angiography in pediatric intestinal resections: a first prospective mixed methods clinical trial. J Pediatr Surg. (2023) 58(1):82–8. doi: 10.1016/j.jpedsurg.2022.09.020
27. Duprée A, Rieß H, von Kroge PH, Izbicki JR, Debus ES, Mann O, et al. Intraoperative quality assessment of tissue perfusion with indocyanine green (ICG) in a porcine model of mesenteric ischemia. PLoS One. (2021) 16(7):e0254144. doi: 10.1371/journal.pone.0254144
28. Knudsen KBK, Nerup N, Thorup J, Thymann T, Sangild PT, Svendsen LB, et al. Intestinal perfusion assessed by quantitative fluorescence angiography in piglets with necrotizing enterocolitis. J Pediatr Surg. (2022) 57(4):747–52. doi: 10.1016/j.jpedsurg.2021.10.021
29. Gemeinsamer Bundesausschuss. Qualitätssicherungs-Richtlinie Früh- und Reifgeborene (2005). Available online at: https://www.g-ba.de/richtlinien/41/ (Accessed July 6, 2025).
30. Lacher M, Barthlen W, Eckoldt F, Fitze G, Fuchs J, Hosie S, et al. Operative volume of newborn surgery in German university hospitals: high volume versus low volume centers. Eur J Pediatr Surg. (2022) 32(5):391–8. doi: 10.1055/s-0041-1740479
31. Granger CL, Mukherjee K, Embleton ND, Tinnion RJ, Berrington JE. Impact of transfer for surgical management of preterm necrotising enterocolitis or focal intestinal perforation. J Pediatr Surg. (2023) 58(10):1976–81. doi: 10.1016/j.jpedsurg.2023.03.016
32. Loh M, Osborn DA, Lui K. Outcome of very premature infants with necrotising enterocolitis cared for in centres with or without on site surgical facilities. Arch Dis Child Fetal Neonatal Ed. (2001) 85(2):F114–8. doi: 10.1136/fn.85.2.F114
33. Giraudeau C, Moussaron A, Stallivieri A, Mordon S, Frochot C. Indocyanine green: photosensitizer or chromophore? Still a debate. Curr Med Chem. (2014) 21(16):1871–97. doi: 10.2174/0929867321666131218095802
34. Kitai T, Inomoto T, Miwa M, Shikayama T. Fluorescence navigation with indocyanine green for detecting sentinel lymph nodes in breast cancer. Breast Cancer. (2005) 12(3):211–5. doi: 10.2325/jbcs.12.211
35. Nitta T, Kataoka J, Ohta M, Ueda Y, Senpuku S, Kurashima Y, et al. Laparoscopic cholecystectomy for cholecystitis using direct gallbladder indocyanine green injection fluorescence cholangiography: a case report. Ann Med Surg. (2020) 57:218–22. doi: 10.1016/j.amsu.2020.07.057
36. Patel I, Rehman S, McKay S, Bartlett D, Mirza D. Use of near-infrared fluorescence techniques in minimally invasive surgery for colorectal liver metastases. J Clin Med. (2023) 12(17):5536. doi: 10.3390/jcm12175536
37. Hagiwara C, Wakabayashi T, Tsutsui A, Sakamoto J, Fujita S, Fujiyama Y, et al. Time required for indocyanine green fluorescence emission for evaluating bowel perfusion in left-sided colon and rectal cancer surgery. Surg Endosc. (2023) 37(10):7876–83. doi: 10.1007/s00464-023-10356-8
38. Fenn G, Kennedy S, Morrison C, Dolan RT. Indocyanine green fluorescence angiography: a critical intra-operative assessment tool to aid decision making in complex hand trauma. Trauma Case Rep. (2023) 48:100923. doi: 10.1016/j.tcr.2023.100923
39. Fransvea P, Fico V, Puccioni C, D’Agostino L, Costa G, Biondi A, et al. Application of fluorescence-guided surgery in the acute care setting: a systematic literature review. Langenbecks Arch Surg. (2023) 408(1):375. doi: 10.1007/s00423-023-03109-7
40. Breuking EA, Varsseveld Ov, Harms M, Tytgat SHAJ, Hulscher JBF, Ruiterkamp J. Safety and feasibility of indocyanine green fluorescence angiography in pediatric gastrointestinal surgery: a systematic review. J Pediatr Surg. (2023) 58(8):1534–42. doi: 10.1016/j.jpedsurg.2022.10.045
41. VERDYE. Pulver zur Herstellung einer Injektionslösung (2022). Available online at: https://www.rote-liste.de/suche/praep/12640-0/VERDYE%20Pulver%20zur%20Herstellung%20einer%20Injektionsl%C3%B6sung (Accessed February 15, 2025).
Keywords: necrotizing enterocolitis, indocyanine green, fluorescence, blood perfusion, short bowel syndrome
Citation: Pfennigs AM, Besendörfer M, Diez S and Reingruber B (2025) Indocyanine green fluorescence in second-look surgery for necrotizing enterocolitis: enhancing the surgeon's perception. Front. Pediatr. 13:1641794. doi: 10.3389/fped.2025.1641794
Received: 5 June 2025; Accepted: 20 August 2025;
Published: 29 September 2025.
Edited by:
Augusto Zani, University of Toronto, CanadaReviewed by:
Erik David Skarsgard, British Columbia Children’s Hospital, CanadaCarlos Zozaya, University of Toronto, Canada
Copyright: © 2025 Pfennigs, Besendörfer, Diez and Reingruber. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonia Maximina Pfennigs, bWF4aS5mYXVzdEBnbXguZGU=;Bertram ReingruberUmVpbmdydWJlckBrYWlzZXJzd2VydGhlci1kaWFrb25pZS5kZQ==
†Present Address: Antonia Maximina Pfennigs,Department for Pediatric Surgery, Asklepios Pediatric Hospital Sankt Augustin, St. Augustin, Germany
‡These authors contributed equally to this work and share senior authorship