 Fabiana Neves Figueiredo1
Fabiana Neves Figueiredo1 Aline de Piano Ganen1Carolina Costa Figueiredo2Nara Michelle de Araújo Evangelista2Vânia de Fátima Tonetto Fernandes2Luciana de Aguiar Pacheco2Tatiana Kato2
Aline de Piano Ganen1Carolina Costa Figueiredo2Nara Michelle de Araújo Evangelista2Vânia de Fátima Tonetto Fernandes2Luciana de Aguiar Pacheco2Tatiana Kato2 Guido de Paula Colares Neto1,2*
Guido de Paula Colares Neto1,2*
- 1Nutrition Department, Centro Universitário São Camilo, São Paulo, Brazil
- 2Pediatric Endocrinology Department, Hospital Infantil Darcy Vargas, São Paulo, Brazil
Objective: To evaluate the nutritional status and dietary patterns of girls with central precocious puberty (CPP) undergoing treatment with leuprolide acetate during the COVID-19 pandemic.
Methods: A cross-sectional study was conducted with 59 girls, aged 5–13 years, diagnosed with CPP and treated with leuprolide acetate. Between May and December 2021, a food frequency questionnaire (FFQ) and a 24-hour dietary recall (24-h DR) were administered. The Fornés score was used to quantify consumption markers of healthy (beans, fruits, vegetables, and greens) and unhealthy (hamburgers, sugar-sweetened beverages, ultra-processed foods, and sweets) foods. Higher scores reflected greater intake of the respective food groups.
Results: Of the participants, 31 (52.5%) showed a reduction in their BMI Z-score (mean change: −0.32 ± 0.26), while 28 (47.5%) had an increase (mean change: 0.25 ± 0.22). Girls who reduced their BMI Z-score had significantly higher Fornés scores for healthy food markers (p = 0.02), particularly for fresh fruits (p = 0.04) and greens and vegetables (p = 0.01). A negative correlation was found between BMI Z-score variation and the Fornés score for healthy food markers (p = 0.02), including fruits (p = 0.02) and greens and vegetables (p = 0.02). No significant associations were observed between BMI Z-score variation and age at treatment onset (p = 0.22) or treatment duration (p = 0.43).
Conclusion: In girls with CPP treated with leuprolide acetate, greater consumption of healthy foods—especially fruits and vegetables—was associated with decreased BMI Z-scores. These findings underscore the role of dietary quality in energy balance and support nutritional monitoring during GnRHa therapy, particularly under lifestyle-altering conditions such as the COVID-19 pandemic.
1 Introduction
Central precocious puberty (CPP) is characterized by the early activation of the hypothalamic-pituitary-gonadal (HPG) axis, leading to pubertal development in girls younger than eight years of age (1, 2). The incidence of CPP is estimated to range from 1 in 5,000–1 in 10,000 children, occurring predominantly in girls. An increase in CPP cases was observed during the COVID-19 pandemic, a period marked by significant changes in dietary habits and a rise in obesity prevalence (3, 4).
Nutritional status is closely linked to the timing of pubertal onset. Activation of the HPG axis is associated with hormonal and metabolic changes induced by weight gain, which may lead to increased ovarian hormone production and earlier breast development. Thus, elevated body mass index (BMI) and overweight in girls may contribute to the higher prevalence of CPP (5–7).
In patients with CPP, treatment with leuprolide acetate—a gonadotropin-releasing hormone analog (GnRHa)—suppresses the production of sex hormones. This therapeutic approach delays skeletal maturation, promotes adequate linear growth, and reduces the risk of compromised adult height (3).
Although previous studies have reported an association between GnRHa treatment and increased BMI in girls with CPP, the literature remains unclear about the influence of dietary quality and quantity on anthropometric changes during this treatment, particularly in the context of lifestyle alterations brought on by the COVID-19 pandemic (8–13).
Therefore, the present study aims to assess the nutritional status and dietary patterns of girls with CPP undergoing treatment with leuprolide acetate during the COVID-19 pandemic.
2 Materials and methods
This study was submitted to the Research Ethics Committee of Centro Universitário São Camilo and approved under Certificate of Presentation for Ethical Consideration number 44087521.6.0000.0062 and opinion number 4.664.1111.
Participants were selected from pediatric endocrinology clinics at Hospital Infantil Darcy Vargas and the Vila Constância Specialty Outpatient Clinic in São Paulo, Brazil. Among 64 female patients aged 5–13 years, 59 met the inclusion criteria based on a diagnosis of CPP, defined as the presence of thelarche before eight years of age, accelerated growth velocity for age and sex, baseline luteinizing hormone (LH) levels above 0.3 mIU/ml, LH levels above 5 mIU/ml two hours after leuprolide acetate administration, and bone age advancement exceeding two standard deviations. All included patients were undergoing regular treatment with 11.25 mg of leuprolide acetate every 84 days for at least three months, without missed or delayed doses. Exclusion criteria included the use of other medications (glucocorticoids, anticonvulsants, antidepressants, antipsychotics) and the presence of thyroid disorders.
Data collection occurred between May and December 2021. Prior to participation, informed assent and consent were obtained from the patients and their guardians. After enrollment, data were collected from the first and last medical consultations during GnRHa treatment, and study questionnaires were administered to patients and caregivers.
Medical records included age, pubertal staging (Marshall and Tanner criteria), age at treatment onset, treatment duration, and leuprolide dosage. Anthropometric data—weight (kg), height (cm), and BMI—were collected. Height and BMI Z-scores were calculated using WHO reference standards. Nutritional status was classified by BMI-for-age-and-sex Z-scores as underweight (Z < –2), normal (–2 ≤ Z ≤ + 1), overweight (+1 < Z ≤ + 2), obesity (+2 < Z ≤ + 3), and severe obesity (Z > + 3) (14).
Food consumption was assessed using a Food Frequency Questionnaire (FFQ) and a 24 h dietary recall (24 hDR). Healthy food consumption markers (beans, fresh fruits, greens, and vegetables) and unhealthy markers (hamburgers, sweetened beverages, ultra-processed foods, and sweets) were classified according to the guidelines of the Brazilian Ministry of Health (15).
Quantitative analysis of dietary intake was conducted using the Fornés scoring system, a validated tool for assessing dietary patterns in pediatric populations, including Brazilian children and adolescents. In addition to evaluating eating behaviors, this system facilitates statistical analyses of diet quality and its associations with dietary habits (16–18).
In this method, foods reported in the FFQ and 24hDR are categorized into seven frequency ranges: f1—not consumed; f2—consumed daily; f3—once a week; f4—two to four times a week; f5—five to six times a week; f6—one to three times a month; and f7—rarely consumed (16). Each frequency category (fi) is assigned a score (Sf) based on estimated annual consumption. Daily consumption (f2) corresponds to a score of S = 1, while other categories are calculated using the formula: Sn = (1/365) × [(a + b)/2], where a and b represent the number of days in the respective frequency range (16).
For each participant, total scores were calculated separately for healthy and unhealthy food markers by summing the individual scores for the corresponding food groups. Higher scores reflect greater consumption within a given category, whereas lower scores indicate reduced intake. This approach enables a comprehensive evaluation of overall diet quality (16).
Descriptive statistics were used to summarize the data. Categorical variables were expressed as absolute and relative frequencies. Quantitative variables were presented as mean ± standard deviation (SD) for normally distributed data and median [minimum; maximum] for non-normally distributed data. Normality was assessed using the Kolmogorov–Smirnov test. Between-group comparisons were performed using the unpaired Student's t-test for parametric data and the Mann–Whitney U test for non-parametric data. Correlations between variables were analyzed using Pearson's test for normally distributed data and Spearman's test for non-normally data. A p-value < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS Statistics version 27.0 (SPSS Inc., Chicago, IL, USA).
3 Results
The demographic and clinical characteristics of the study population are summarized in Table 1. The median age at the onset of thelarche was 7.0 years (4.0; 7.9), and the median age at the time of questionnaire application was 9.0 years (6.0; 13.0). At the beginning of treatment, the median age was 8.2 years (4.5; 10.7), with 76.3% of participants classified as stage III according to the Tanner and Marshall criteria. The mean duration of treatment at the time of evaluation was 16.8 ± 12.3 months. Regression or stabilization of secondary sexual characteristics was observed in 83.1% of the patients.
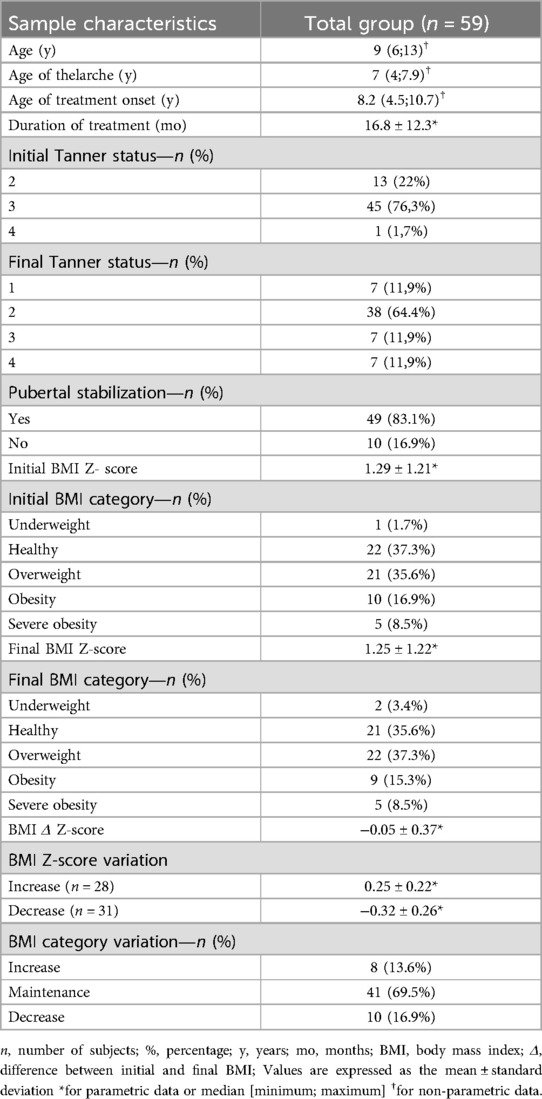
Table 1. Demographic and clinical characteristics of the study population.
A total of 57 patients (96.6%) had height classified as either adequate (78%) or tall (18.6%) for their age and sex, with a mean height Z-score of 0.84 ± 1.35. Interestingly, 30 of these children (50.8%) exceeded their predicted familial height range.
At the start of treatment, 36 patients (61%) were classified as overweight or obese—a proportion that remained unchanged by the end of the treatment period. Throughout the study, 31 patients (52.5%) showed a reduction in their BMI Z-score (mean change: −0.32 ± 0.26), while 28 patients (47.5%) experienced an increase (mean change: 0.25 ± 0.22). According to WHO classification parameters, 41 patients (69.5%) maintained their BMI category despite fluctuations in BMI Z-score.
No significant correlations were found between changes in BMI Z-score and either age at treatment onset (p = 0.22) or treatment duration (p = 0.43). Additionally, there were no significant differences between the groups with increased and decreased BMI Z-scores in terms of age at treatment initiation [8.3 (5.6; 10.7) vs. 8.1 (4.5; 10.0) years; p = 0.23], treatment duration (17.8 ± 12.8 vs. 15.6 ± 12.0 months; p = 0.50) or response to treatment (75% vs. 90%; p = 0.70).
Patients who experienced a reduction in their BMI Z-score during treatment showed significantly higher Fornés scores for healthy food consumption markers (p = 0.02), including fresh fruits (p = 0.04) and greens and vegetables (p = 0.01), compared to those whose BMI Z-score increased. Moreover, this group also presented lower Fornés scores for sweetened beverages, instant noodles, snacks, and cookies—Table 2.
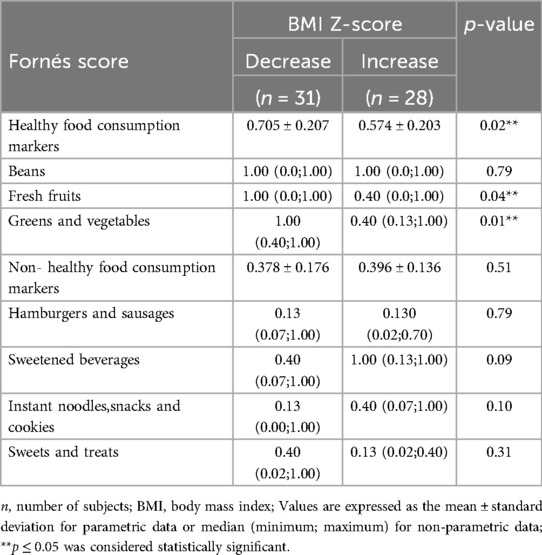
Table 2. Fornés score comparison between girls with central precocious puberty treated with leuprolide, showing whether BMI Z-score increased or decreased during the COVID-19 pandemic.
A negative correlation was observed between BMI Z-score variation and the Fornés score for healthy food consumption markers (r = −0.296; p = 0.02), particularly for fresh fruits (r = −0.288; p = 0.02) and greens and vegetables (r = −0.296; p = 0.02). In contrast, no significant correlations were found between BMI Z-score variation and the Fornés score for unhealthy food consumption markers—Table 3.
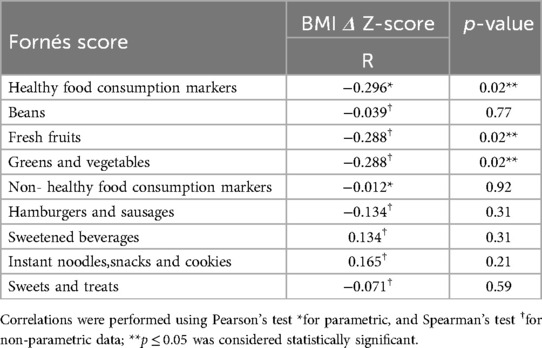
Table 3. Correlations between fornés scores for food consumption markers and BMI Z-score variation in girls with central precocious puberty treated with leuprolide during the COVID-19 pandemic.
Additionally, no significant differences were found between the healthy weight and overweight/obese groups in Fornés scores for either healthy (p = 0.24) or unhealthy (p = 0.44) food consumption markers.
4 Discussion
The initiation of treatment in the studied patients occurred later relative to the age of thelarche, with 76.3% already in Tanner stage 3 at the onset of leuprolide therapy. Despite this, 83.1% of the girls showed regression or stabilization of secondary sexual characteristics during treatment, indicating a satisfactory response to the medication and dosage regimen. These findings are consistent with previous results reported by Lee et al. and Klein et al. (19, 20). Moreover, no difference in treatment response was observed between the groups with increased vs. decreased BMI Z-scores.
Among the girls evaluated, 50.8% had a height exceeding their predicted familial growth range, a common finding in CPP. Elevated estrogen levels accelerate linear growth and bone maturation, which may ultimately result in compromised final adult height. Therefore, height monitoring plays a key role in both the diagnosis of CPP and the follow-up of GnRHa therapy, as leuprolide suppresses estrogen production and helps preserve height potential (21, 22).
Previous studies identified a correlation between BMI increase during GnRHa therapy and girls with CPP, particularly among those already overweight or obese. These findings suggest that suppression of the HPG axis by GnRHa may directly influence metabolic processes in this subgroup, thereby contributing to further increases in BMI. Specifically, the reduction of endogenous estrogen caused by treatment appears to lower basal growth rates and reduce energy expenditure. When dietary intake remains unchanged, this decrease in energy expenditure can result in additional weight gain and fat accumulation. Despite these mechanisms, 69.5% of the girls in our sample maintained their BMI category throughout the treatment period. Furthermore, no significant correlation was observed between variation in BMI Z-score and either age at treatment initiation or treatment duration (8, 9, 23–25).
Nevertheless, 61% of the girls in this study were classified as overweight or obese at the onset of treatment. Currently, the high prevalence of precocious puberty has been linked to several factors, including excess body weight and obesity, exposure to endocrine-disrupting chemicals, stressful environments, diet and adverse psychosocial conditions, especially in girls (26–29). These associations became particularly evident during the COVID-19 pandemic (2019–2022), a period marked by emergency containment measures adopted globally, including in Brazil. Social isolation, restricted mobility, and school closures contributed to changes in dietary habits, like fast food and packaged snacks, reduced physical activity, and increased sedentary behavior, ultimately leading to a rise in obesity rates (4, 30, 31).
Elevated BMI has been consistently linked to earlier pubertal onset (8). Diets high in animal protein and saturated fats, alongside low fiber intake, are also associated with premature activation of the HPG axis (32–34). This early activation is associated with elevated levels of leptin, insulin, and IGF-1. Diet-related changes in gut microbiota and inflammation may also play a role (35–37). Leptin, which is secreted in proportion to body fat, stimulates kisspeptin neurons in the hypothalamus. These neurons then trigger the release of GnRH to initiate pubertal development (38, 39). Insulin and IGF-1, often elevated in obesity, may further enhance central and peripheral HPG activation (33, 40). Additionally, the aromatization of androgens into estrogens can accelerate signs such as thelarche and menarche (33, 41, 42). Collectively, these pathways suggest that excess adiposity and poor diet contribute to both elevated BMI and earlier puberty.
During the COVID-19 pandemic, particularly following lockdown periods, an increase in the incidence of CPP and BMI gain in girls was reported (3, 7, 10–13).These observations suggest a potential causal relationship between pubertal progression and weight gain, likely driven by changes in dietary habits and lifestyle (31, 43–45). Furthermore, according to the WHO, emergency containment measures implemented to control the spread of COVID-19 may have influenced the frequency of household food purchases and dietary patterns among Brazilian families (46). In response, numerous recommendations promoting healthy eating were published during this critical period, emphasizing the role of adequate nutrition in both the prevention and management of COVID-19 infection (47–52).
In this study, the quantitative analysis of the 24hDR and FFQ using the Fornés score revealed a negative correlation between the variation in BMI Z-score and the intake of healthy food markers, including fresh fruits, greens, and vegetables (15). Additionally, the group that experienced a reduction in BMI Z-score reported lower consumption of sweetened beverages, instant noodles, snacks, and cookies compared to the group with increased BMI.
Consistent with part of our findings, Pietrobelli et al. observed an increase in fruit intake among obese Italian children during the COVID-19 pandemic; however, this was accompanied by a simultaneous rise in the consumption of processed and ultra-processed foods, such as French fries, red meat, and sugary drinks (53). Similarly, Ruiz-Roso et al. reported an increased intake of fruits, deep-fried foods, and sweets among adolescents from Spain, Italy, Brazil, Colombia, and Chile. Notably, a higher intake of greens and vegetables was observed, particularly among Brazilian girls (31). These patterns suggest that environmental factors—such as socioeconomic status, dietary trends, religious practices, and regional food traditions—may shape healthy eating behaviors. Furthermore, the WHO's guidance on promoting a healthy lifestyle during the pandemic may have contributed to an increase in the consumption of fresh fruits, greens, and vegetables (47, 50).
In our study, patients who experienced an increase in BMI tended to consume more ultra-processed foods. Eating patterns characterized by excessive and frequent intake of these products—often triggered by boredom and stress, particularly prevalent during the COVID-19 pandemic—are known to be associated with higher caloric intake and increased risk of obesity (29). According to the Brazilian Society of Pediatrics, strategies to contain the spread of COVID-19 directly impacted children's nutrition, as restrictions on mobility reduced the frequency of grocery shopping. Consequently, families may have turned to ultra-processed foods, which are easier to purchase, store, and consume due to their extended shelf life (53).
Among patients who showed a reduction in BMI Z-score, higher consumption of fruits and vegetables may have contributed to improved weight status by offsetting the caloric density and low nutritional value of ultra-processed foods.
A key strength of this study lies in the use of complementary tools to assess food consumption (24hDR, FFQ, and Fornés score), as well as the evaluation of girls with CPP undergoing GnRHa treatment during the COVID-19 pandemic—a period marked by significant lifestyle disruptions for children. Nonetheless, it is important to note that the cross-sectional design limits the ability to infer the long-term effects of the observed dietary patterns. In addition, although the 24hDR and FFQ are widely used in epidemiological research, they present limitations such as memory bias and limited accuracy in quantifying dietary intake (54).
As discussed above, among girls with CPP undergoing treatment with leuprolide acetate, higher consumption of healthy foods—particularly fruits and vegetables—was associated with a reduction in BMI Z-score. These findings underscore the important role of dietary quality in maintaining energy balance and regulating weight during GnRHa therapy, particularly during periods of lifestyle disruption, such as the COVID-19 pandemic. Clinicians must proactively incorporate tailored nutritional counseling as a standard component of CPP management. Based on these results, it is imperative to conduct robust longitudinal studies in the post-COVID period to determine if improvements in dietary habits and BMI are maintained as routines normalize with the return to in-person schooling.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Research Ethics Committee of Centro Universitário São Camilo and approved under Certificate of Presentation for Ethical Consideration number 44087521.6.0000.0062 and opinion number 4.664.1111. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
FF: Formal analysis, Methodology, Validation, Data curation, Conceptualization, Writing – original draft, Investigation. AG: Conceptualization, Validation, Project administration, Supervision, Writing – review & editing, Methodology, Investigation, Writing – original draft, Formal analysis. CF: Resources, Data curation, Investigation, Writing – review & editing. NE: Resources, Data curation, Investigation, Writing – review & editing. VF: Writing – review & editing, Investigation, Resources, Data curation. LP: Writing – review & editing, Investigation, Resources, Data curation. TK: Investigation, Writing – review & editing, Resources, Data curation. GC: Conceptualization, Supervision, Validation, Writing – review & editing, Formal analysis, Methodology, Project administration, Writing – original draft, Resources.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Carel JC, Eugster EA, Rogol A, Ghizzoni L, Palmert MR. Consensus statement on the use of gonadotropin-releasing hormone analogs in children. Pediatrics. (2009) 123(4):e752–62. doi: 10.1542/peds.2008-1783
2. Latronico AC, Brito VN, Carel JC. Causes, diagnosis, and treatment of central precocious puberty. Lancet Diabetes Endocrinol. (2016) 4(3):265–74. doi: 10.1016/S2213-8587(15)00380-0
3. Stagi S, De Masi S, Bencini E, Losi S, Paci S, Parpagnoli M, et al. Increased incidence of precocious and accelerated puberty in females during and after the Italian lockdown for the coronavirus 2019 (COVID-19) pandemic. Ital J Pediatr. (2020) 46(1):1–10. doi: 10.1186/s13052-020-00851-x
4. Street ME, Sartori C, Catellani C, Bernasconi S. Precocious puberty and COVID-19 into perspective: potential increased frequency, possible causes, and a potential emergency to be addressed. Front Pediatr. (2021) 9:1–6. doi: 10.3389/fped.2021.716718
5. Blank SK, McCartney CR, Marshall JC. Modulation of gonadotropin-releasing hormone pulse generator sensitivity to progesterone inhibition in hyperandrogenic adolescent girls: implications for regulation of pubertal maturation. J Clin Endocrinol Metab. (2009) 94(7):2360–6. doi: 10.1210/jc.2008-2424
6. Makki K, Froguel P, Wolowczuk I. Adipose tissue in obesity-related inflammation and insulin resistance: cells, cytokines, and chemokines. ISRN Inflamm. (2013) 2013:1–12. doi: 10.1155/2013/139239
7. Antoniazzi F, Zamboni G. Central precocious puberty: current treatment options. Paediatr Drugs. (2004) 6(4):211–31. doi: 10.2165/00148581-200406040-00003
8. Li W, Liu Q, Deng X, Chen Y, Liu S, Story M, et al. Association between obesity and puberty timing: a systematic review and meta-analysis. Int J Environ Res Public Health. (2017) 14(10):E1266. doi: 10.3390/ijerph14101266
9. Leite AL, Brito VN, Lemos-Marini SHV, Castro M, Martinelli CE Jr, Moreira AC. Do GnRH agonists really increase body weight gain? Evaluation of a multicentric Portuguese cohort of patients with central precocious puberty. Front Pediatr. (2022) 10:1–7. doi: 10.3389/fped.2022.794107
10. Itani A, Abou Hamdan A, Zgheib H, Ghandour Z, Costanian C, Azar A. Increased incidence of precocious puberty in girls during COVID-19 pandemic: early indicator of the upcoming childhood metabolic syndrome pandemic? Glob Pediatr Health. (2022) 9:1–6. doi: 10.1177/2333794X221104302
11. Prosperi S, Chiarelli F. Early and precocious puberty during the COVID-19 pandemic. Front Endocrinol (Lausanne). (2023) 13:1107911. doi: 10.3389/fendo.2022.1107911
12. Geniuk N, Suárez Mozo MJ, Pose MN, Vidaurreta S. Rapidly progressive precocious puberty during the COVID-19 lockdown. Arch Argent Pediatr. (2023) 121(3):e202202840. doi: 10.5546/aap.2022-02840.eng
13. Fava D, Pepino C, Tosto V, Gastaldi R, Pepe A, Paoloni D, et al. Precocious puberty diagnoses spike, COVID-19 pandemic, and body mass index: findings from a 4-year study. J Endocr Soc. (2023) 7(9):bvad094. doi: 10.1210/jendso/bvad094
14. WHO Multicentre Growth Reference Study Group. WHO Child growth standards. Dev Med Child Neurol. (2009) 51(12):1002. doi: 10.1111/j.1469-8749.2009.03503.x
15. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde; Departamento de Atenção Básica. Orientações Para Avaliação de Marcadores de Consumo Alimentar na Atenção Básica [recurso Eletrônico]. Brasília: Ministério da Saúde (2015). p. 33.
16. De Fornés NS, Sarti FM, Silva KS. Food consumption scores and serum lipid levels in the population of São Paulo, Brazil. Rev Saude Publica. (2002) 36(1):12–8. doi: 10.1590/S0034-89102002000100003
17. Ferreira RC, Barbosa LB, Vasconcelos SML. Studies assessing food consumption by the scores method: a systematic review. Ciênc Saúde Coletiva. (2019) 24(5):1777–92. doi: 10.1590/1413-81232018245.1236201
18. Neto ACB, Andrade MMB, Costa BMS, Nunes TM, Anunciação D, Gonçalves DA, et al. Body weight and food consumption scores in adolescents from northeast Brazil. Rev Paul Pediatr. (2015) 33(3):319–26. doi: 10.1016/j.rpped.2015.01.002
19. Lee PA, Klein K, Mauras N, Lev-Vaisler T, Bacher P. 36-month Treatment experience of two doses of leuprolide acetate 3-month depot for children with central precocious puberty. J Clin Endocrinol Metab. (2014) 99(9):3153–9. doi: 10.1210/jc.2014-1457
20. Klein KO, Freire A, Gryngarten M, Kletter G, Benson M, Miller B, et al. Phase 3 trial of a small volume subcutaneous 6-month duration leuprolide acetate treatment for central precocious puberty. J Clin Endocrinol Metab. (2020) 105(10):1–12. doi: 10.1210/clinem/dgaa418
21. Klein KO. Precocious puberty: who has it? Who should be treated? J Clin Endocrinol Metab. (1999) 84(2):411–14. doi: 10.1210/jcem.84.2.5575
22. Lee PA. Central precocious puberty: an overview of diagnosis, treatment, and outcome. Endocrinol Metab Clin North Am. (1999) 28(4):901–18. doi: 10.1016/s0889-8529(05)70108-0
23. Hou L, Ying Y, Wu W, Ye F, Zhang C, Luo X. The effect of GnRHa treatment on body mass index in central precocious puberty: a systematic review and meta-analysis. Horm Res Paediatr. (2024) 97(5):419–32. doi: 10.1159/000531216
24. Zhu X, Qin J, Xue W, Li S, Zhao M, Jin Y. The effect of GnRH analog treatment on BMI in children treated for precocious puberty: a systematic review and meta-analysis. J Pediatr Endocrinol Metab. (2024) 37(4):297–308. doi: 10.1515/jpem-2023-0416
25. Cammisa I, Malavolta E, Arzilli F, Rotunno G, Rigante D, Cipolla C. The effect of GnRH analogs on body mass index in girls with central precocious puberty: a single-center retrospective study with a literature review. Children (Basel). (2025) 12:336. doi: 10.3390/children12030336
26. Heras V, Castellano JM, Fernandois D, Velasco I, Rodriguez-Vazquez E, Roa J, et al. Central ceramide signaling mediates obesity-induced precocious puberty. Cell Metab. (2020) 32(6):951–66.e8. doi: 10.1016/j.cmet.2020.10.001
27. Brix N, Ernst A, Lauridsen LL, Parner ET, Arah OA, Olsen J, et al. Childhood overweight and obesity and timing of puberty in boys and girls: cohort and sibling-matched analyses. Int J Epidemiol. (2020) 49(5):834–44. doi: 10.1093/ije/dyaa056
28. La Rocca C, Maranghi F, Tait S, Tassinari R, Baldi F, Bottaro G, et al. The LIFE PERSUADED project approach on phthalates and bisphenol A biomonitoring in Italian mother-child pairs linking exposure and juvenile diseases. Environ Sci Pollut Res Int. (2018) 25(25):25618–25. doi: 10.1007/s11356-018-2660-4
29. Knight JA, Kehm RD, Schwartz L, Frost CJ, Chung WK, Colonna S, et al. Prepubertal internalizing symptoms and timing of puberty onset in girls. Am J Epidemiol. (2021) 190(3):431–8. doi: 10.1093/aje/kwaa223
30. Hu B, Guo H, Zhou P, Shi Z-L. Characteristics of SARS-CoV-2 and COVID-19. Nat Rev Microbiol. (2021) 19(3):141–54. doi: 10.1038/s41579-020-00459-7
31. Ruiz-Roso MB, de Carvalho Padilha P, Mantilla-Escalante DC, Ulloa N, Brun P, Acevedo-Correa D, et al. COVID-19 confinement and changes of adolescent’s dietary trends in Italy, Spain, Chile, Colombia and Brazil. Nutrients. (2020) 12(6):1807. doi: 10.3390/nu12061807
32. Günther AL, Karaolis-Danckert N, Kroke A, Remer T, Buyken AE. Dietary protein intake throughout childhood is associated with the timing of puberty. J Nutr. (2010) 140(3):565–71. doi: 10.3945/jn.109.114934
33. Tang J, Xue P, Huang X, Lin C, Liu S. Diet and nutrients intakes during infancy and childhood in relation to early puberty: a systematic review and meta-analysis. Nutrients. (2022) 14(23):5004. doi: 10.3390/nu14235004
34. Xu Y, Xiong J, Gao W, Wang X, Shan S, Zhao L, et al. Dietary fat and polyunsaturated fatty acid intakes during childhood are prospectively associated with puberty timing independent of dietary protein. Nutrients. (2022) 14(2):275. doi: 10.3390/nu14020275
35. Goldsammler M, Merhi Z, Buyuk E. Role of hormonal and inflammatory alterations in obesity-related reproductive dysfunction at the level of the hypothalamic-pituitary-ovarian axis. Reprod Biol Endocrinol. (2018) 16(1):45. doi: 10.1186/s12958-018-0366-6
36. Kaplowitz PB. Link between body fat and the timing of puberty. Pediatrics. (2008) 121(Suppl 3):S208–17. doi: 10.1542/peds.2007-1813F
37. Watling CZ, Kelly RK, Tong TY, Piernas C, Watts EL, Tin ST, et al. Associations of circulating insulin-like growth factor-I with intake of dietary proteins and other macronutrients. Clin Nutr. (2021) 40(9):4685–93. doi: 10.1016/j.clnu.2021.05.015
38. Skorupskaite K, George JT, Anderson RA. The kisspeptin-GnRH pathway in human reproductive health and disease. Hum Reprod Update. (2014) 20(4):485–500. doi: 10.1093/humupd/dmu009
39. Bruno C, Vergani E, Giusti M, Oliva A, Cipolla C, Pitocco D, et al. The “adipo-cerebral” dialogue in childhood obesity: focus on growth and puberty. Physiopathological and nutritional aspects. Nutrients. (2021) 13(10):3434. doi: 10.3390/nu13103434
40. Baier I, Pereira A, Ferrer P, Iñiguez G, Mericq V. Higher prepubertal IGF-1 concentrations associate to earlier pubertal tempo in both sexes. Horm Res Paediatr. (2023) 96(4):404–11. doi: 10.1159/000528662
41. Biro FM, Khoury P, Morrison JA. Influence of obesity on timing of puberty. Int J Androl. (2006) 29(1):272–7. doi: 10.1111/j.1365-2605.2005.00602.x
42. Bordini B, Rosenfield RL. Normal pubertal development: part II: clinical aspects of puberty. Pediatr Rev. (2011) 32(7):281–92. doi: 10.1542/pir.32-7-281
43. Brown S, Opitz MC, Peebles AI, Sharpe H, Duffy F, Newman E. A qualitative exploration of the impact of COVID-19 on individuals with eating disorders in the UK. Appetite. (2021) 156:104977. doi: 10.1016/j.appet.2020.104977
44. Phillipou A, Meyer D, Neill E, Tan EJ, Toh WL, Van Rheenen TE, et al. Eating and exercise behaviors in eating disorders and the general population during the COVID-19 pandemic in Australia: initial results from the COLLATE project. Int J Eat Disord. (2020) 53(7):1158–65. doi: 10.1002/eat.23317
45. Malta DC, de Almeida MF, Cardoso LO, Pinto ICM, Braga JU, Araújo VV, et al. A pandemia da COVID-19 e as mudanças no estilo de vida dos brasileiros adultos: um estudo transversal, 2020. Epidemiol Serv Saude. (2020) 29(4):e2020407. doi: 10.1590/S1679-49742020000400026
47. Silverio R, Gonçalves DC, Andrade MF, Seelaender M. Coronavirus disease 2019 (COVID-19) and nutritional status: the missing link? Adv Nutr. (2021) 12(3):682–92. doi: 10.1093/advances/nmaa125
48. Lana RM. Emergência do novo coronavírus (SARS-CoV-2) e o papel de uma vigilância nacional em saúde oportuna e efetiva. Cad Saude Publica. (2020) 36(3):e00000020.
49. Velly H, Britton RA, Preidis GA. Mechanisms of cross-talk between the diet, the intestinal microbiome, and the undernourished host. Gut Microbes. (2017) 8(2):98–112. doi: 10.1080/19490976.2016.1267888
50. Calder PC, Carr AC, Gombart AF, Eggersdorfer M. Reply to: “comment on: optimal nutritional status for a well-functioning immune system is an important factor to protect against viral infections. Nutrients. (2020) 12(8):1–3. doi: 10.3390/nu12082330
51. Associação Brasileira de Nutrição (ASBRAN). Guia Para uma Alimentação Saudável em Tempos de COVID-19. São Paulo: ASBRAN (2020).
52. Brasil. Ministério da Saúde; Fundação Oswaldo Cruz; Núcleo de Alimentação, Saúde e Ambiente (NASA). Guia de Orientação em Relação à Alimentação e Exercício Físico Diante da COVID-19. Rio de Janeiro: Fiocruz (2020).
53. Pietrobelli A, Pecoraro L, Ferruzzi A, Heo M, Faith MS, Zoller T, et al. Effects of COVID-19 lockdown on lifestyle behaviors in children with obesity living in verona, Italy: a longitudinal study. Obesity (Silver Spring). (. 2020) 28(8):1382–5. doi: 10.1002/oby.22861
Keywords: dietary pattern, nutritional status, COVID-19, precocious puberty, leuprolide
Citation: Figueiredo FN, Ganen AdP, Figueiredo CC, Evangelista NMdA, Fernandes VdFT, Pacheco LdA, Kato T and Colares Neto GdP (2025) Impact of dietary patterns on body weight in girls with central precocious puberty treated with leuprolide during the COVID-19 pandemic. Front. Pediatr. 13:1650247. doi: 10.3389/fped.2025.1650247
Received: 19 June 2025; Accepted: 5 August 2025;
Published: 26 August 2025.
Edited by:
Sally Radovick, The State University of New Jersey, United StatesReviewed by:
Takeshi Ninchoji, Harima himeji General Medical Hospital, JapanIgnazio Cammisa, Fondazione Policlinico Universitario A. Gemelli—IRCCS, Italy
Copyright: © 2025 Figueiredo, Ganen, Figueiredo, Evangelista, Fernandes, Pacheco, Kato and Colares Neto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guido de Paula Colares Neto, Z3VpZG8ubmV0b0Bwcm9mLnNhb2NhbWlsby1zcC5icg==