 Perihan Cam Ray
Perihan Cam Ray Merve Doğan1,‡
Merve Doğan1,‡ Hülya Binokay
Hülya Binokay- 1Department of Child and Adolescent Psychiatry, Cukurova University Faculty of Medicine, Adana, Türkiye
- 2Department of Medical Genetics, Cukurova University Faculty of Medicine, Adana, Türkiye
- 3Department of Biostatistics, Cukurova University Faculty of Medicine, Adana, Türkiye
Objective: Autism Spectrum Disorder (ASD) is a complex neurodevelopmental condition influencyed by genetic and environmental factors. There is emerging evidence of an association between hereditary thrombophilia and ASD, potentially mediated by impaired placental perfusion and resultant neuroinflammatory processes. This study aimed to investigate the frequency of thrombophilia-related genetic polymorphisms in children diagnosed with ASD and their mothers.
Methods: A total of 24 children with ASD aged 2-6 and their mothers were compared with 24 age-matched healthy children and their mothers. Sociodemographic, developmental and genetic data were collected. A psychiatric evaluation was performed according to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), and the children were assessed using the Autism Behavior Checklist (ABC), the Modified Checklist for Autism in Toddlers (M-CHAT) and the Ankara Developmental Screening Inventory (ADSI). Thrombophilia-related polymorphisms, including FVL G1691A, FII G20210A, C677T MTHFR and 1298AC MTHFR, FXIII-Val34Leu and PAI-1 4G/5G, were analyzed using PCR-based methods. Statistical comparisons and logistic regression analyses were performed to evaluate associations with ASD.
Results: The FXIII-Val34Leu heterozygous variant was significantly more prevalent in children with ASD (37.5% vs. 8.3%, p = 0.036) and their mothers (54.2% vs. 16.7%, p = 0.015) than in the control group. Logistic regression analysis revealed that the presence of the FXIII-Val34Leu heterozygous polymorphism in either the mother or child was associated with an approximately 4.130-fold increase in the odds of ASD (adjusted odds ratio = 4.130, 95% confidence interval = 1.180–5.300, p = 0.027). Other thrombophilia polymorphisms did not differ significantly between groups. Additionally, children with ASD exhibited significant delays in speech development and lower developmental scores across several domains.
Conclusion: This study is among the first to examine the FXIII Val34Leu mutation in children with ASD and their mothers. Further large-scale, longitudinal studies are needed to investigate thrombophilia markers in relation to ASD.
Introduction
Autism Spectrum Disorder (ASD) is a neurodevelopmental condition characterized by deficits in social communication and interaction, as well as restricted and repetitive patterns of behavior, emerging in early childhood (1). The etiopathogenesis of ASD is complex and believed to result from the interaction of genetic, epigenetic, and environmental factors (2). Genomic-level research has identified numerous genetic variants that influence synaptic function, neuronal migration, and neuroinflammation. These variants may disrupt neurodevelopmental processes by affecting the development of the cerebral cortex, particularly during the prenatal period (3). Additionally, mechanisms critical to nervous system development—synaptic plasticity, cytoskeletal organization, and blood–brain barrier integrity—have been implicated in the pathogenesis of ASD.
In recent years, increasing evidence suggests that ASD may be associated not only with neuronal mechanisms but also with vascular and hematologic pathways. In particular, alterations in cerebral blood flow, abnormal vascular development, and coagulation system dysfunctions have been proposed to be associated with ASD (4). Hereditary thrombophilia, which increases the tendency for thrombosis in both the mother and fetus, may indirectly influence brain development during the intrauterine period and thereby elevate the risk of ASD (5). Microthrombi resulting from thrombophilia may trigger neuroinflammation and exert adverse effects on neurodevelopmental outcomes.
Hereditary thrombophilia is a condition that arises due to mutations causing a genetic predisposition to venous thromboembolism (6). Polymorphisms in genes such as 5,10-methylenetetrahydrofolate reductase (MTHFR), Factor V Leiden (FVL), factor II prothrombin (FII), Factor XIII (FXIII) Val34Leu, and plasminogen activator inhibitor-1 (PAI-1) are known to contribute to this condition (7). It has been suggested that genetic coagulation disorders in pregnant women may impair placental circulation by disrupting uteroplacental perfusion, potentially leading to adverse effects on fetal neurodevelopment (8).
The aim of this study is to investigate whether there is a relationship between ASD and hereditary thrombophilia by examining thrombophilia parameters in children diagnosed with ASD and their mothers. In addition, the study aims to explore whether these parameters could serve as potential screening biomarkers. The lack of comprehensive studies in the literature that simultaneously assess both maternal and child thrombophilia profiles highlights the potential significance and contribution of this research to the existing body of knowledge.
Materials and methods
Sample
This study included 24 children (5 girls, 19 boys), aged 2–6 years who were diagnosed with ASD according to DSM-5 criteria, and their mothers (9). These participants were recruited from the Child and Adolescent Psychiatry Outpatient Clinic at Çukurova University Faculty of Medicine. An additional 24 age-matched healthy children (10 girls, 14 boys) and their mothers were enrolled as the control group. Written informed consent was obtained from all parents after detailed information about the study's purpose and procedures was provided. The researchers (M.D. and P.Ç.R.) collected data and performed evaluations through face-to-face interviews. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Çukurova University Non-Interventional Clinical Research Ethics Committee (April 2, 2021; Approval no.: 110).
Procedure
Assessment of the patient group
The ASD group comprises children aged 2–6 who have been diagnosed with ASD and assessed functioning class according to DSM-5 criteria (9). At the clinic, patients are evaluated by research assistants, pediatric psychiatrists, and faculty members. The research assistants assess the patients and then consult with the faculty members to create a diagnosis and treatment plan. During the evaluation, forms are used to collect sociodemographic information and diagnostic criteria from the DSM-5, as well as standard psychometric measurements, to support diagnoses. The Modified Checklist for Autism in Toddlers (M-CHAT), the Autism Behavior Checklist (ABC) and the Ankara Developmental Screening Inventory (ADSI) are routinely administered to children under six who are referred to our outpatient clinic with suspected developmental delay. In this study, all participants were evaluated by researchers M.D., P.Ç.R. or G.Ç., with the scales being administered by M.D. However, due to age considerations, the M-CHAT remained descriptive only. Patients received treatment in accordance with clinical guidelines and protocols. The data were thoroughly analyzed, including demographics, prenatal and perinatal history, birth history, other early symptoms, coexisting conditions, and neurodevelopmental and medical data. The parents' demographic data were also analyzed (e.g., age, educational qualifications, and mental and medical conditions). Children with major physical/medical problems, a confirmed diagnosis of a genetic syndrome or inherited metabolic disease, intellectual disability, bipolar disorder, or psychotic disorders were excluded.
Assessment of the control group
The group included 24 age-matched children. This group was selected from children who had been assessed by the same team of child and adolescent psychiatrists and were found to have no such disorders. Data from control parents/children were collected in a similar way to that from the patient group. Children with major physical/medical problems, genetic syndromes or inherited metabolic diseases, or mental disorders were excluded.
The Ankara developmental screening inventory (ADSI)
The ADSI is used in Turkey to assess children's development from 0–6 years. In this study, language, motor, and general development were evaluated using the tool. It was developed for Turkish children by Savasir et al. (1998) (10). It comprises four subscales: communication–language–cognitive, fine motor, gross motor, and social skills–self-care. Administration takes 30–45 min, depending on age and skills. The inventory consists of 154 items, organized by age group, answered by mothers with “Yes,” “No,” or “I don't know.” It is a valid and reliable way of assessing children's development in the Turkish population (10, 11).
Autism behavior checklist (ABC)
Developed by Krug et al. in 1993, the ABC is a 57-item questionnaire about symptoms of autism (12). Parents/guardians score sensory, relating, body concept and object use, language, social and self-help on a 4-point scale from 0 (no problem) to 3 (severe problem). Total scores range from 0–159, with higher scores indicating greater severity. Irmak et al. (2007) conducted a Turkish study into the scale's validity and reliability (13). They found the correct classification rate of the ABC to be 88%. The cut-off score for the scale was set at 39. The Cronbach's alpha coefficient and the split-half test reliability were found to be 0.92.
Laboratory and molecular genetic analyses
Peripheral blood samples collected from children and their mothers in EDTA tubes were used for molecular analyses. The polymerase chain reaction (PCR) technique was used to amplify six specific regions to detect polymorphisms in the following genes: FVL G1691A (Factor V Leiden), FII G20210A (prothrombin), C677T, MTHFR A1298C, PAI-1 4G/5G, FXIII Val34Leu polymorphism. The amplified gene products were separated by electrophoresis, and fragment analysis was performed using specialized software to determine the genotypic profiles. Three genotypes of each gene were investigated: normal, heterozygous and variant. In addition, the results of the following tests performed by our outpatient clinic were included: routine vitamin B12 level (pg/mL), vitamin D level (ng/mL) and anti-streptolysin O (ASO) titer (IU/mL).
In the control group, all loci conformed to the expectations of the Hardy–Weinberg principle (exact test: all p > 0.05; BH-adjusted q-values = 1.00). The smallest p value was observed for PAI 4G/5G [p = 0.194; minor allele frequency (MAF) = 0.375], whereas the other loci ranged from p = 0.683–1.000 (e.g., MTHFR A1298C: p = 0.683; FII G20210A: p = 1.000; FVL G1691A: p = 1.000; MTHFR C677T: p = 1.000; FXIII Val34Leu: p = 1.000). Control-group MAFs ranged from 0.021–0.396. In the control group of mothers (n = 24), all six maternal loci were broadly consistent with Hardy–Weinberg expectations based on exact tests. The smallest p-value occurred at the PAI 4G/5G locus (p-exact = 0.024), but this was not significant after Benjamini–Hochberg correction across loci (q = 0.146). Exact p values for the remaining loci ranged from 0.135–1.000. The minor-allele frequencies (MAF) spanned 0.000–0.354 (FII G20210A = 0.000; FVL G1691A = 0.0625; FXIII Val34Leu = 0.0833; MTHFR C677T = 0.2708; PAI 4G/5G = 0.3333; MTHFR A1298C = 0.3542). FII G20210A was monomorphic among mothers and was therefore uninformative for association testing. Overall, these maternal genotype results suggest that the control sample was adequately genotyped.
Statistical analysis
Categorical variables were expressed as counts and percentages, whereas continuous variables were summarized as mean ± standard deviation or median (minimum–maximum). Comparisons between the ASD and control groups were performed using chi-square or Fisher's exact test for categorical variables. Categorical comparisons used Pearson's χ² test when assumptions were met; when ≥1 expected cell count was <5 (or any observed count was 0), two-sided Fisher's exact test was used. The normality of distribution for continuous variables was confirmed with the Kolmogorov–Smirnov and Shapiro Wilk test. For comparison of continuous variables between two groups, the student's t test or Mann–Whitney U test was used depending on whether the statistical hypotheses were fulfilled or not. Firth bias-reduced logistic regression analysis was performed to determine significant predictors of autism variable. Multiple group comparisons between the ASD and control groups were conducted using chi-square and t-tests, as appropriate. To control the potential increase in false positives due to multiple testing, the Benjamini-Hochberg procedure was applied across the main families of comparisons. Hardy–Weinberg equilibrium (HWE) was evaluated for each maternal locus in the control group using two-sided exact tests, with multiple comparisons controlled by the Benjamini–Hochberg procedure (q < 0.05), and monomorphic loci excluded from association analyses. Analyses were performed in R studio 4.2.2 and IBM SPSS Statistics Version 20.0 statistical software package. The statistical level of significance for all tests was considered to be 0.05.
Figure 1 shows a flow chart of the study design.
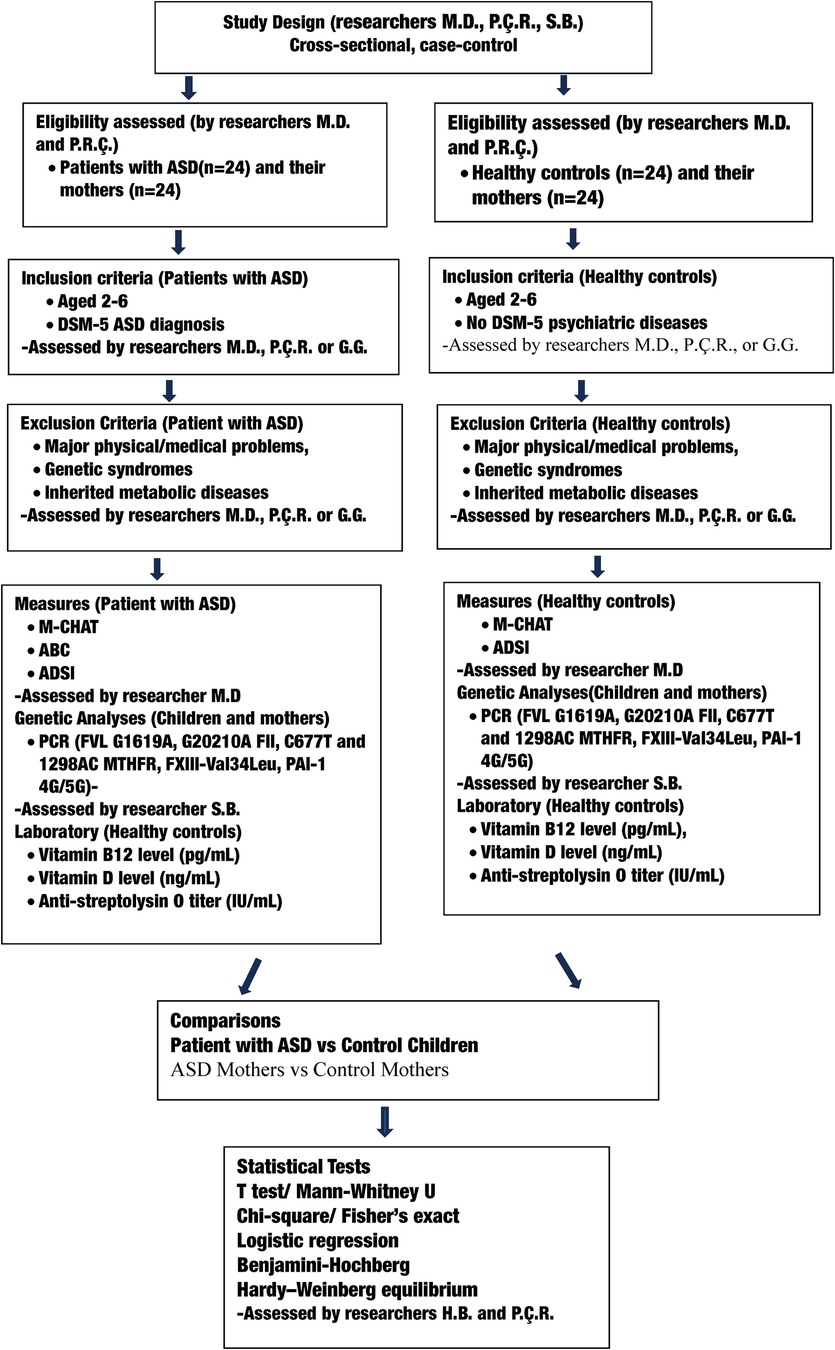
Figure 1. Flow chart of study design, participant selection, measures, comparisons, and statistical analyses. M-CHAT, the modified checklist for autism in toddlers, ABC, autism behavior checklist; ADSI, Ankara development screening inventory; PCR, polymerase chain reaction.

Figure 2. The FXIII-Val34Leu mutation in mothers of children with ASD compared to mothers of healthy children.
Results
In terms of gender distribution, 79.2% (n = 19) of the children in the ASD group were male, whereas the proportion of males in the healthy control group was 58.3% (n = 14). Although the groups were not fully matched by sex, this difference was not statistically significant (adjusted p = 0.238) (Table 1). Regarding ASD severity level, 6 children (25.0%) had ASD level 1, and 11 (45.8%) had ASD level 2, 7 (29.2%) had ASD level 3. Eleven of the children with ASD (45.8%) were non-verbal. Children with ASD scored lower than healthy children in all domains of the ADSI developmental assessment except the gross motor domain. Articulation disorder was present in 3 patients (12.5%). No statistically significant differences were observed between the groups in terms of paternal or maternal educational level or the presence of medical disease or psychiatric disorder in the parents (all p > 0.05) (Table 1).

Table 1. Sociodemographic characteristics and comorbidity status of families of children with ASD and healthy controls.
A history of developmental regression was reported in 62.5% of children with ASD (n = 11), while no cases were observed in the healthy control group (0.0%). This difference was found to be statistically significant (adjusted p = 0.009). In terms of speech development, 45.8% of children with ASD (n = 11) had no speech development, whereas all healthy controls (100%, n = 24) demonstrated normal speech development. This difference was also statistically significant (adjusted p = 0.009). Other variables including abortion history, cesarean delivery, prematurity, birth complications, neonatal incubator care, and presence of comorbid illness did not show statistically significant differences between groups (all p > 0.05) (Table 2).

Table 2. Birth history, developmental characteristics, and comorbidity status in children with autism spectrum disorder and healthy controls.
A statistically significant difference was detected in the FXIII-Val34Leu polymorphism: 8 of the 24 children with ASD (33.3%) had the heterozygous FXIII-Val34Leu genotype, compared to 2 of 24 controls (8.3%), a difference that was statistically significant (p = 0.036) However, no statistically significant differences were observed between groups for the G20210A FII, FVL G1691A, C677T MTHFR, A1298C MTHFR or PAI-1 4G/5G polymorphisms (all p > 0.05) (see Table 3).

Table 3. Distribution of thrombophilia-related genetic polymorphisms in children with ASD and healthy controls.
There was no significant difference in the mean age between the ASD and control groups. (4.3 ± 1.0 vs. 4.7 ± 1.2 years, adjusted p = 0.317). The age at onset of speech was markedly delayed in the ASD group (35.8 ± 9.7 months) compared to the control group (20.5 ± 8.4 months), and this difference was statistically significant (adjusted p = 0.004) (see Table 4).

Table 4. Demographic features, developmental scale scores, and biochemical parameters of children with ASD and healthy controls.
The mean ABC score for children with ASD was 50.4 (±21.5). The ABC score for the control group was 0. All subdomains of the ADSI developmental assessment, except for the gross motor domain, yielded significantly lower scores in children diagnosed with ASD compared to healthy controls. Specifically, the language and cognitive subscale scores were markedly reduced in the ASD group (37.5 ± 9.5) relative to controls (48.0 ± 9.8; (adjusted p = 0.004). The total ADSI score was significantly reduced in the ASD group (107.1 ± 18.6) compared to healthy peers (125.7 ± 17.7; adjusted p = 0.004), indicating a generalized developmental delay in multiple domains among children with ASD. No statistically significant differences were observed in birth weight, parental ages, breastfeeding duration, or biochemical markers such as vitamin B12, vitamin D, and anti-streptolysin O (ASO) titers (all p > 0.05) (Table 4).
The frequencies of genetic polymorphisms were compared between mothers of children with ASD and control group mothers. A significant difference was found for the FXIII Val34Leu polymorphism. The heterozygous variant was more prevalent among mothers of children with ASD (54.2%) than control mothers (16.7%), while the normal genotype was more prevalent in the control group (83.3%) than among mothers of children with ASD (45.8%) (p = 0.015) (see Table 5 and Figure 2). However, no statistically significant differences were found between the ASD and control mothers for any of the other polymorphisms examined (FII G20210A, FVL G1691A, MTHFR C677T, MTHFR A1298C, or PAI-1 4G/5G; see Table 5).

Table 5. Distribution of thrombophilia-related genetic polymorphisms in mothers of children with ASD and mothers of healthy children.
Bias-reduced logistic regression analysis employing the Firth's method revealed a positive association between the FXIII Val34Leu heterozygous polymorphism and ASD in both mothers and children. In the parsimonious Firth logistic regression model, both child age and the combined maternal–child genotype variable (FXIII Val34Leu mother–child) were significant predictors. This variable was coded as “1” if either the mother or child carried the polymorphism, and as “0” if neither did. However, because the minor allele frequency was low and several contingency table cells had expected counts of less than five, modelling maternal and child genotypes as two separate predictors led to non-convergence, quasi-complete separation, and unstable estimates under limited events per parameter. To preserve identifiability and reduce variance inflation, a dyad-level indicator was specified (coded 1 if either the mother or the child carried the risk allele, and 0 otherwise; variable name: FXIII V34L mother-child). This specification was predefined as an exploratory, stability-oriented analytical choice and does not imply the biological equivalence of maternal and fetal genetic effects.
The presence of the FXIII Val34Leu mother-child polymorphism in either the mother or the child increased the odds of the outcome by a factor of approximately 4.130 [adjusted odds ratio (AOR) = 4.130, 95% confidence interval (CI) = 1.180–5.300, p = 0.027] (see Table 6). Although the confidence intervals were relatively wide due to the small sample size and low mutation frequency, the direction and magnitude of the effect were consistent with the hypothesized biological mechanism. Combining maternal and child genotypes into a single variable improved model stability and provided a more meaningful representation of familial genetic predisposition (see Table 6).

Table 6. Results of logistic regression analysis for variables associated with ASD risk.
Discussion
This pioneering study provides a detailed examination of a hereditary thrombophilia panel in children with ASD and their mothers, with a particular focus on the FXIII Val34Leu variant and its relationship to ASD. Significant differences were identified in children with ASD in terms of a history of developmental regression, delayed speech development and pronounced delays in the language and social domains during early childhood. From a genetic perspective, Factor XIII V34L polymorphism was significantly more prevalent in both children with ASD and their mothers. Furthermore, regression analysis revealed significant associations between the Factor XIII V34L mutation and ASD. These findings raise the question of whether hereditary thrombophilia contributes to ASD pathogenesis through intrauterine vascular mechanisms. Given the small sample size and pilot nature of our study, these results cannot be generalized. Therefore, further large-scale, longitudinal studies are required to investigate the relationship between thrombophilia markers and ASD.
In the etiopathogenesis of ASD, abnormalities in vasculogenesis and angiogenesis, structural alterations of the blood-brain barrier, and dysfunctions of the neurovascular unit have been emphasized (14). Particularly, genetic abnormalities affecting neuronal migration and signaling in the cerebral cortex during the intrauterine period are reported to trigger neurodevelopmental disorders (15, 16). In our study, we detected a significantly higher frequency of the FXIII Val34Leu polymorphism in children diagnosed with ASD and their mothers compared to healthy controls. This finding has not been reported in previous ASD literature, highlighting its significance and providing a new perspective on etiological mechanisms. Thrombophilia mutations are generally known to affect placental circulation and lead to pregnancy complications, thereby influencing fetal brain development (17). From this perspective, it seems likely that thrombotic events during the fetal period could lead to neuroinflammation. Moreover, vascular abnormalities in the perinatal period have been reported to increase the risk of ischemic and hemorrhagic stroke, resulting in neurodevelopmental problems (18, 19). Therefore, further studies are warranted to explore the role of thrombophilia parameters such as Factor XIII V34L in the development of ASD.
The FVL G1691A mutation is a common hereditary thrombophilia variant in the general population and is associated with an increased risk of thrombosis. This mutation may lead to complications such as venous thromboembolism (VTE) and small for gestational age (SGA) infants during pregnancy (20). In our study, the frequency of Factor V Leiden mutation was lower in both children with ASD and their mothers compared to the control group, and no statistically significant difference was observed.
The G20210A FII mutation is another important variant that increases the risk of thrombosis by elevating circulating prothrombin levels (21). In our cohort, this mutation was found at similarly low frequencies across groups. Among MTHFR enzyme mutations, the most common C677T variant is known to elevate plasma homocysteine levels and has been associated with preeclampsia, neural tube defects, and thrombotic events (22). Although experimental models and meta-analyses in the literature suggest a potential role of MTHFR variants in increasing ASD risk (23, 24), no significant differences were found in the distribution of C677T and A1298C MTHFR variants between the ASD and control groups in our study. These findings are consistent with those reported by Sener et al. (2014) and suggest that the role of these mutations in ASD risk warrants further investigation (25).
In our study, no statistically significant difference was found between the ASD and control groups in terms of PAI-1 4G/5G polymorphism. However, the literature indicates that the 4G/4G and 4G/5G genotypes of the PAI-1 gene are associated with thrombosis and early pregnancy complications, particularly with a significantly increased risk of miscarriage (26). Although the underlying mechanisms of the relationship between ASD and thrombophilia remain unclear, it has been proposed that hypercoagulability may lead to early spontaneous clot formation, triggering neuroinflammation and subsequently increasing autism risk (27). Recent studies have reported a positive correlation between hypercoagulability and neuroimmune parameters in children with ASD, particularly with elevated levels of antibodies against myelin basic protein (28). Furthermore, there is emerging evidence of associations between placental inflammation, maternal vascular pathology, and ASD risk. These findings support the hypothesis that ASD may be a neuroinflammatory disorder of vascular origin and underscore the role of cerebrovascular and immunological factors in its etiopathogenesis (29). The current body of evidence highlights the need for further comprehensive research into the pathophysiology of ASD.
The perinatal period is a critical phase characterized by a high risk of stroke and is associated with long-term neurological morbidities such as motor delay, cognitive impairments, speech disorders, and epilepsy (19). In pediatric populations, one of the major causes of hemorrhagic strokes is inherited coagulation disorders, particularly those related to factor deficiencies such as hemophilia (19). Both ischemic and hemorrhagic strokes during the perinatal period have been reported to increase the risk of neurodevelopmental disorders such as ASD and ADHD (18, 19, 30, 31). Notably, post-ischemic epilepsy is frequently observed, and ASD risk is significantly higher in children with comorbid epilepsy following ischemic stroke (30, 32). Although this was not directly evaluated in our study, these findings emphasize the need for a more detailed investigation into the relationship between ASD risk and neurovascular and thrombotic events.
It is established that hereditary thrombophilia mutations may trigger vascular complications during pregnancy via placental mechanisms, potentially leading to conditions such as fetal growth restriction (8). Notably, maternal FVL mutation may adversely affect fetal growth independently of placental pathology (8). Maternal metabolic and cardiovascular conditions (obesity, diabetes, underlying cardiac disease) increase the risk of preeclampsia (33, 34). Preeclampsia, in turn, can lead to severe complications such as fetal death, intrauterine growth restriction, and prematurity (33, 34). Furthermore, maternal metabolic syndrome, hypertension, and diabetes have been associated with an increased risk of thrombosis during pregnancy, which may impair fetal circulation and predispose to various neurodevelopmental disorders, including ASD (34). The literature also indicates that perinatal factors such as prematurity, preeclampsia, fetal distress, and cesarean delivery are associated with an increased risk of ASD (14, 35). In this context, our study supports further investigation into the role of perinatal and vascular factors in assessing the risk of ASD.
The primary limitations of our study are its pilot nature, cross-sectional design, multiple testing, sex imbalance, small sample size, and lack of investigation into complications such as perinatal stroke. Furthermore, this small-scale study did not group patients based on other mental health conditions or the severity of ASD. Key strengths of this study include the inclusion of both ASD children and their mothers (a family-based approach), the presence of a well-matched healthy control group, and a detailed, comprehensive analysis of an extended thrombophilia panel.
The study found that children diagnosed with ASD and their mothers had a higher frequency of the FXIII-Val34Leu polymorphism than healthy controls. Logistic regression analysis suggests this polymorphism may be a risk factor for ASD. Although no significant differences were observed between the groups regarding other thrombophilia-related genetic parameters, the high overall prevalence of certain thrombophilia polymorphisms among all children is noteworthy. In conclusion, our findings, representing the preliminary results of a potential link between the FXIII-Val34Leu mutation and ASD, are expected to contribute to the elucidation of underlying pathogenic mechanisms and should be supported by future molecular and clinical research.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
Ethics statement
The studies involving humans were approved by Çukurova University Non-Interventional Clinical Research Ethics Committee (Date: 02.04.2021, Approval No: 110). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
PR: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing, Resources, Visualization. MD: Conceptualization, Data curation, Investigation, Methodology, Resources, Writing – original draft, Visualization. SB: Conceptualization, Investigation, Methodology, Resources, Supervision, Writing – review & editing. GG: Conceptualization, Investigation, Methodology, Resources, Supervision, Writing – review & editing. HB: Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by the Çukurova University Research Fund (Project No: 13989), approved on 29.11.2021 (Meeting No: 2021/8).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Hirota T, King BH. Autism spectrum disorder: a review. Jama. (2023) 329(2):157–68. doi: 10.1001/jama.2022.23661
2. Wang L, Wang B, Wu C, Wang J, Sun M. Autism spectrum disorder: neurodevelopmental risk factors, biological mechanism, and precision therapy. Int J Mol Sci. (2023) 24(3):1819. doi: 10.3390/ijms24031819
3. Love C, Sominsky L, O'Hely M, Berk M, Vuillermin P, Dawson SL. Prenatal environmental risk factors for autism spectrum disorder and their potential mechanisms. BMC Med. (2024) 22(1):393. doi: 10.1186/s12916-024-03617-3
4. Cao X, Tang X, Feng C, Lin J, Zhang H, Liu Q, et al. A systematic investigation of complement and coagulation-related protein in autism spectrum disorder using multiple reaction monitoring technology. Neurosci Bull. (2023) 39(11):1623–37. doi: 10.1007/s12264-023-01055-4
5. Abisror N, Mekinian A, Lachassinne E, Nicaise-Roland P, De Pontual L, Chollet-Martin S, et al. Autism spectrum disorders in babies born to mothers with antiphospholipid syndrome. Semin Arthritis Rheum. (2013) 43(3):348–51. doi: 10.1016/j.semarthrit.2013.07.001
6. Liu X, Chen Y, Ye C, Xing D, Wu R, Li F, et al. Hereditary thrombophilia and recurrent pregnancy loss: a systematic review and meta-analysis. Hum Reprod. (2021) 36(5):1213–29. doi: 10.1093/humrep/deab010
7. Fevraleva I, Mamchich D, Vinogradov D, Chabaeva Y, Kulikov S, Makarik T, et al. Role of genetic thrombophilia markers in thrombosis events in elderly patients with COVID-19. Genes (Basel). (2023) 14(3):644. doi: 10.3390/genes14030644
8. Freedman AA, Hogue CJ, Dudley DJ, Silver RM, Stoll BJ, Pinar H, et al. Associations between maternal and fetal inherited thrombophilias, placental characteristics associated with vascular malperfusion, and fetal growth. TH Open. (2017) 1(1):e43–55. doi: 10.1055/s-0037-1603925
9. American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders (DSM-V). 5th edn Washington DC: American Psychiatric Publishing (2013).
10. Savaşır I, Sezgin N, Erol N. Ankara Gelişim Tarama Envanteri El Kitabı. Genişletilmiş 2. basım Ankara: Rekmay Ltd fiti (1998).
11. Sezgin N. Two different validity study of Ankara developmental screening inventory (ADSI): criterion-related validity and concurrent discrimination validity. Turk J Child Adolesc Ment Health. (2011) 18:185–96.
12. Krug DA, Arick JR, Almond PA. Autism Screening Instrument for Educational Planning. 2nd edn Austin, Texas: Pro-ed Inc (1993).
13. Yılmaz-Irmak T, Tekinsav-Sütçü S, Aydın A, Sorias O. An investigation of validity and reliabilty of autism behavior checklist (ABC). Çocuk ve Gençlik Ruh Sağlığı Dergisi. (2007) 14(1):13–23.
14. Wang Y, Yu S, Li M. Neurovascular crosstalk and cerebrovascular alterations: an underestimated therapeutic target in autism spectrum disorders. Front Cell Neurosci. (2023) 17:1226580. doi: 10.3389/fncel.2023.1226580
15. Prem S, Millonig JH, DiCicco-Bloom E. Dysregulation of neurite outgrowth and cell migration in autism and other neurodevelopmental disorders. Adv Neurobiol. (2020) 25:109–53. doi: 10.1007/978-3-030-45493-7_5
16. Bicks LK, Geschwind DH. Functional neurogenomics in autism spectrum disorders: a decade of progress. Curr Opin Neurobiol. (2024) 86:102858. doi: 10.1016/j.conb.2024.102858
17. Mitriuc D, Popuşoi O, Catrinici R, Friptu V. The obstetric complications in women with hereditary thrombophilia. Med Pharm Rep. (2019) 92(2):106–10. doi: 10.15386/cjmed-1097
18. Hamner T, Shih E, Ichord R, Krivitzky L. Children with perinatal stroke are at increased risk for autism spectrum disorder: prevalence and co-occurring conditions within a clinically followed sample. Clin Neuropsychol. (2022) 36(5):981–92. doi: 10.1080/13854046.2021.1955150
19. Janas AM, Barry M, Lee S. Epidemiology, causes, and morbidities of stroke in the young. Curr Opin Pediatr. (2023) 35(6):641–7. doi: 10.1097/MOP.0000000000001294
20. Hemsworth EM, O'Reilly AM, Allen VM, Kuhle S, Brock JK. Association between factor V leiden mutation, small for gestational age, and preterm birth: a systematic review and meta-analysis. J Obstet Gynaecol Can. (2016) 38(10):897–908. doi: 10.1016/j.jogc.2016.08.001
21. Khan S, Dickerman JD. Hereditary thrombophilia. Thromb J. (2006) 4:15. doi: 10.1186/1477-9560-4-15
22. den Heijer M, Koster T, Blom HJ, Bos GM, Briet E, Reitsma PH, et al. Hyperhomocysteinemia as a risk factor for deep-vein thrombosis. N Engl J Med. (1996) 334(12):759–62. doi: 10.1056/NEJM199603213341203
23. Rai V. Association of methylenetetrahydrofolate reductase (MTHFR) gene C677T polymorphism with autism: evidence of genetic susceptibility. Metab Brain Dis. (2016) 31(4):727–35. doi: 10.1007/s11011-016-9815-0
24. Li CX, Liu YG, Che YP, Ou JL, Ruan WC, Yu YL, et al. Association between MTHFR C677T polymorphism and susceptibility to autism spectrum disorders: a meta-analysis in Chinese han population. Front Pediatr. (2021) 9:598805. doi: 10.3389/fped.2021.598805
25. Sener EF, Oztop DB, Ozkul Y. MTHFR Gene C677T polymorphism in autism spectrum disorders. Genet Res Int. (2014) 2014:698574. doi: 10.1155/2014/698574
26. Yıldırım M, Dağ Ş, Kurtulgan H, Karakuş S. Plazminojen aktivatör inhibitor-1 (PAI-1) 4 g/4 g polimorfizminin gebelik kayıplarıyla ilişkisi. Cumhuriyet Med J. (2014) 36(3):350–5. doi: 10.7197/cmj.v36i3.5000060803
27. Brusov O, Klyushnik T, Simashkova N, Karpova N, Faktor M, Zozulya S, et al. A combined marker of catatonia severity including autoimmune and thrombodynamic parameters in patients with autism spectrum disorder. Zh Nevrol Psikhiatr Im S S Korsakova. (2020) 120(7):86–93. doi: 10.17116/jnevro202012007186
28. Brusov OS, Klyushnik TP, Zozulya SA, Karpova NS, Shilov YE, Nikitina SG, et al. Paired and partial correlations of immune parameters of neuro-immuno-test and coagulation parameters of thrombodynamics test in children with children’s autism. Zh Nevrol Psikhiatr Im S S Korsakova. (2022) 122(9. Vyp. 2):68–73. doi: 10.17116/jnevro202212209268
29. Ouellette J, Crouch EE, Morel JL, Coelho-Santos V, Lacoste B. A vascular-centric approach to autism spectrum disorders. Neurosci Insights. (2024) 19:26331055241235921. doi: 10.1177/26331055241235921
30. Sundelin H, Söderling J, Bang P, Bolk J. Risk of autism after pediatric ischemic stroke: a nationwide cohort study. Neurology. (2022) 98(19):e1953–e63. doi: 10.1212/WNL.0000000000200253
31. Wu CM, Zhang B, Trenor CC, Rivkin MJ, Danehy A, Lehman LL. Autism spectrum disorder in children with perinatal ischemic stroke varies by stroke type. J Child Neurol. (2023) 38(8-9):513–7. doi: 10.1177/08830738231188395
32. Sundelin HEK, Tomson T, Zelano J, Söderling J, Bang P, Ludvigsson JF. Pediatric ischemic stroke and epilepsy: a nationwide cohort study. Stroke. (2021) 52(11):3532–40. doi: 10.1161/STROKEAHA.121.034796
33. Bohiltea RE, Cirstoiu MM, Turcan N, Stoian AP, Zugravu CA, Munteanu O, et al. Inherited thrombophilia is significantly associated with severe preeclampsia. Exp Ther Med. (2021) 21(3):261. doi: 10.3892/etm.2021.9691
34. Katz J, Reichenberg A, Kolevzon A. Prenatal and perinatal metabolic risk factors for autism: a review and integration of findings from population-based studies. Curr Opin Psychiatry. (2021) 34(2):94–104. doi: 10.1097/YCO.0000000000000673
Keywords: autism spectrum disorder, hereditary thrombophilia, factor XIII Va34Leu, neurodevelopment, genetic polymorphism, MTHFR gene mutation
Citation: Ray PC, Doğan M, Bozdoğan S, Gül G and Binokay Hülya (2025) Hereditary thrombophilia parameters in children with autism spectrum disorder and their mothers. Front. Pediatr. 13:1680354. doi: 10.3389/fped.2025.1680354
Received: 6 August 2025; Revised: 3 November 2025;
Accepted: 10 November 2025;
Published: 11 December 2025.
Edited by:
Anjana Munshi, Central University of Punjab, IndiaReviewed by:
Canan Kuygun Karcı, Adana Dr. Ekrem Tok Mental Health and Diseases Hospital, TürkiyeAdil Abdul-Rehman Siddiq Al-Salihy, Psychological Research Center, Iraq
Copyright: © 2025 Ray, Doğan, Bozdoğan, Gül and Binokay. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Perihan Cam Ray, cGVyaWNhbTIwQGhvdG1haWwuY29t
†Present Address Sevcan Bozdoğan, Variantgen, Genetic Diagnosis, Treatment and Health Services Center, Adana, Türkiye
‡ORCID:
Perihan Cam Ray
orcid.org/0000-0002-6254-6055
Merve Doğan
orcid.org/0000-0002-4682-9469
Sevcan Bozdoğan
orcid.org/0000-0003-3853-8212
Gonca Gül
orcid.org/0000-0001-6101-0796
Hülya Binokay
orcid.org/0000-0002-0162-4574