 Valeria Dipasquale
Valeria Dipasquale Giuseppe Cicala
Giuseppe Cicala Edoardo Spina
Edoardo Spina Claudio Romano
Claudio Romano- 1Pediatric Gastroenterology and Cystic Fibrosis Unit, Department of Human Pathology in Adulthood and Childhood “G. Barresi”, University of Messina, Messina, Italy
- 2Department of Clinical and Experimental Medicine, University of Messina, Messina, Italy
Background: Many pediatric inflammatory bowel disease (IBD) patients are now using biosimilars of anti-tumor necrosis factor-α (TNF-α), with increasing trends in recent years. This study reviewed all available data regarding the use of biosimilars in children with IBD.
Methods: PubMed, Google Scholar, Scopus, and CENTRAL databases were searched through keywords; inflammatory bowel diseases, Crohn’s disease, ulcerative colitis, biosimilar and child were combined using “AND” and “OR.” Original research articles involving pediatric patients receiving one of the biosimilar medications based on the anti-TNF-α biologic drugs approved for pediatric IBD treatment, independently from efficacy and drug response, were included.
Results: Nine studies were included in the evidence synthesis. CT-P13 was the biosimilar used in all studies. Four studies assessed the induction effectiveness of CT-P13. Clinical response and remission rates of biosimilar treatment were 86–90% and 67–68%, respectively, and they were not significantly different to the originator group. Five prospective studies on patients elected to switch from originator IFX to CT-P13 yielded similar results. Adverse events related to CT-P13 were mostly mild. The most frequently reported were upper respiratory tract infections. The switch from the originator had no significant impact on immunogenicity.
Conclusion: The current review showed reported CT-P13 effectiveness as measured by clinical response and/or remission rates after induction or during maintenance and suggest that there is no significant difference with that of the originator IFX. Further studies are warranted, including clinical, and pharmacovigilance studies.
Introduction
Biologics were first introduced roughly 20 years ago, and have radically modified the treatment and prognosis of pediatric inflammatory bowel disease (IBD). Tumor necrosis factor-α (TNF-α), an inflammatory cytokine released by immune cells, was the target of the first biologics used to treat IBD patients (Laharie et al., 2005; Hyams et al., 2007; Hyams et al., 2012). The anti-TNF-α originator drugs available to treat IBD children are infliximab (IFX; Remicade©, Janssen) and adalimumab (Humira©, AbbVie). Their remarkable efficacy and safety profile has led to earlier (“top-down therapy”) and/or longer treatment duration, particularly in patients with a more severe course, and/or poor prognosis (Ruemmele et al., 2014; Turner et al., 2018). The patent on IFX expired in 2013, allowing the companies to launch its biosimilars. According to the World Health Organization, a biosimilar is defined as a “biotherapeutic product, which is similar in terms of quality, safety, and efficacy to an already licensed reference biotherapeutic product” (World Health Organization, 2009). CT-P13 was the first biosimilar IFX to be approved by the regulatory agencies, in 2013 by the European Medicine Agency (EMA) and in 2016 by the Food and Drug Administration (FDA) (Organization site European Medicines Agency, 2013; Organization site World Health Organization, 2017). IFX biosimilars are commercialized under different brand names, including Remsima© (Celltrion) and Inflectra© (Hospira) for CT-P13, or Flixabi© (Biogen) and Renflexis® (Merck) for SB2. ABP501 (Amgevita©, Amgen) was the first approved biosimilar to adalimumab. Based upon extrapolation of thorough in vivo experiments and two randomized controlled clinical studies in adult patients with rheumatologic diseases, biosimilars were authorized for the same indications as the original drug, including adult, and pediatric IBD (Park et al., 2013; Yoo et al., 2013; Alten and Cronstein, 2015). Extrapolation is the process of licensing a biosimilar for all the originator drug’s approved indications, even though the biosimilar has not been formally investigated in all the originator drug’s indications or populations (Weise et al., 2014; Alten and Cronstein, 2015; Vande Casteele and Sandborn, 2015). Extrapolation of compounds in the same class with the same mechanism of action from adult to pediatric or across indications is prevalent in clinical practice when there is insufficient evidence or clinical studies are underway (Weise et al., 2014; Vande Casteele and Sandborn, 2015). Adult patients have been the focus of studies evaluating the efficacy and safety of biosimilars in IBD (Farkas et al., 2015; Jahnsen et al., 2015; Gecse et al., 2016; Ye et al., 2019). According to the European Crohn’s and Colitis Organization’s (ECCO) guidelines, CT-P13’s effectiveness and safety are equivalent to those of its originator product drug in patients who are naïve to anti-TNF-α therapy or who have switched to CT-P13 (Danese et al., 2017). Many pediatric IBD patients are now using biosimilars, with growing trends in recent years. Data on the effectiveness and safety of biosimilars in pediatric IBD are steadily increasing (Dipasquale and Romano, 2020). CT-P13 can be regarded as a good alternative to the originator for induction and maintenance of remission in children with IBD, according to the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Pediatric IBD Porto Group (de Ridder et al., 2015; de Ridder et al., 2019). A recent nationwide web survey conducted in Italy showed that most pediatric IBD experts have good knowledge about biosimilars, with awareness of similar efficacy and safety in comparison to the originator (Dipasquale et al., 2021).
The aim of this review was to analyze all the literature data, published after biosimilar use approval in 2013, regarding the use of biosimilars of anti-TNF-α in pediatric IBD patients, and to assess effectiveness, immunogenicity, and safety profiles, as well as cost concerns.
Methods
Search Strategy
Studies identification, screening, and extraction of relevant data were conducted according to the 2020 version of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. Literature searches and screening of titles, abstracts and full text articles were conducted by two authors (VD; GC) independently. The research was conducted using the PubMed, Google Scholar, Scopus, and the Cochrane Central Register of Controlled Trials (CENTRAL) database—the latter also includes data from the clinicaltrials.gov and the World Health Organization International Clinical Trials Registry Platforms. Records provided by the academic search engine Google Scholar were also scanned. The considered timeframe for all scanned databases and searches was from 2013 to December 2021. For PubMed, Google Scholar and Scopus research, a query structure based on Boolean combinations of the terms “inflammatory bowel diseases,” “Crohn’s disease,” “ulcerative colitis,” “biosimilar” and “child,” with terms variations, was used. For Google scholar the search filter “only scientific articles” was also applied. For the complete query structure and the full list of filters and refinement used see Supplementary Box S1, S2. As for the CENTRAL database search, a multiple query strategy was used: a general query for IBDs, with Boolean combinations of the same terms used for other databases; two other queries of analogous structure to account for specific trials regarding Crohn’s disease and ulcerative colitis. For all the CENTRAL queries, the option of “search for word variations” was selected (full details are available in Supplementary Box S1). The references of all collected publications were also checked to find any missing relevant studies.
Inclusion and Exclusion Criteria
Papers that fulfilled the following criteria were included: original research articles involving pediatric patients of any gender and ethnicity receiving one of the biosimilar medications based on the anti-TNF-α biologic drugs approved for pediatric IBD treatment, independently from efficacy and drug response. Studies were excluded if 1) the originator drug only was used; 2) biosimilars were used to treat diseases other than IBDs; 3) articles were written in a language other than English.
Data Extraction and Management
Data of relevance were extracted by a single author (V.D.) by the means of a data extraction sheet. Data regarding 1) type of IBD treated, 2) number of patients, 3) type of biosimilar used, 4) study duration, 5) clinical evaluations, 6) direct costs of treatment, were extracted. Missing data entries were marked with N/A (not available). Clinical response and/or remission as measured by the Pediatric Crohn’s Disease Activity Index (PCDAI) for CD or the Pediatric Ulcerative Colitis Activity Index (PUCAI) for UC were the primary outcomes. In most studies, clinical response was defined by a PCDAI drop of >15 and a PUCAI score of >20, while remission was defined by a PCDAI or a PUCAI score of 10 or less. No statistical analyses were performed due to the limited number of available studies and the heterogeneity in the reported data. Thus, the findings are presented in a descriptive manner.
Results
In total, 384 records were retrieved, 9 of which met the inclusion criteria (Figure 1) (Sieczkowska et al., 2016; Sieczkowska-Golub et al., 2017; Chanchlani et al., 2018; Gervais et al., 2018; Kang et al., 2018; Richmond et al., 2018; van Hoeve et al., 2019; Nikkonen and Kolho, 2020; Cheon et al., 2021). A total of 394 pediatric IBD patients (316 CD, 61 UC, and 17 IBD-U) was comprised. CT-P13 was the biosimilar used in all studies. No studies on other biosimilars of IFX (PF-06438179/GP1111, SB2) or adalimumab biosimilars in pediatric IBD have been performed so far.
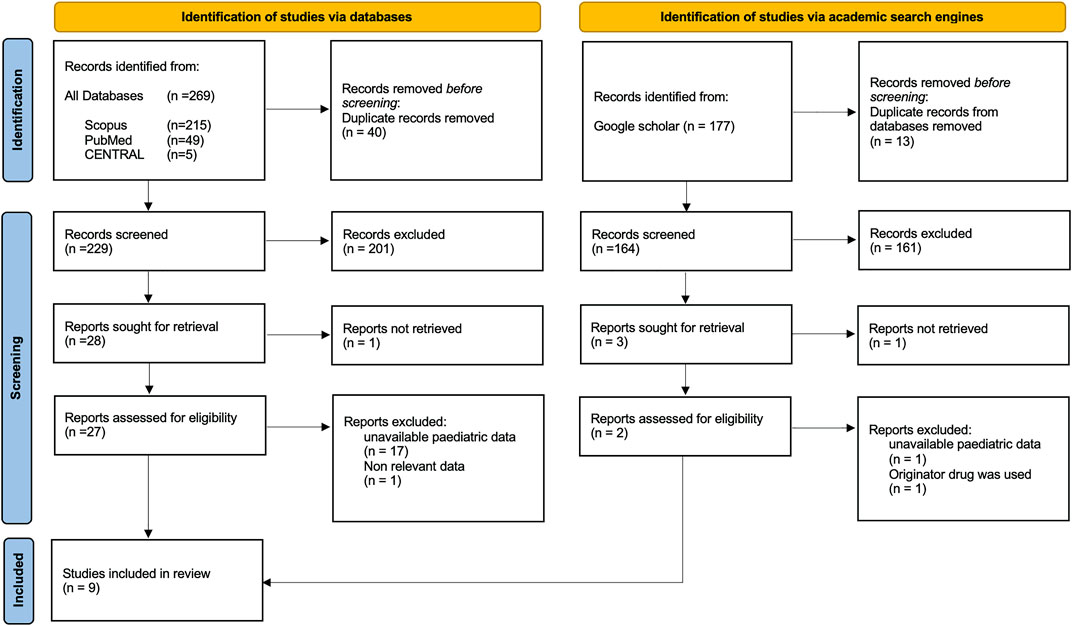
FIGURE 1. Flow chart for study retrieval and selection.
Clinical Endpoints
Each of the studies considered is summarized in Table 1. Some of them compared the outcomes with historical or reference cohorts. In most studies, patients received induction doses at 5 mg/kg at weeks 0, 2, and 6 (Sieczkowska-Golub et al., 2017; Kang et al., 2018; Richmond et al., 2018). In one study it was reported that 57% (16/28) of patients on CT-P13 received induction dose at > 5 mg/kg (Nikkonen and Kolho, 2020). The median age of included patients on CT-P13 was similar, ranging from approximately 11 to 14 years.
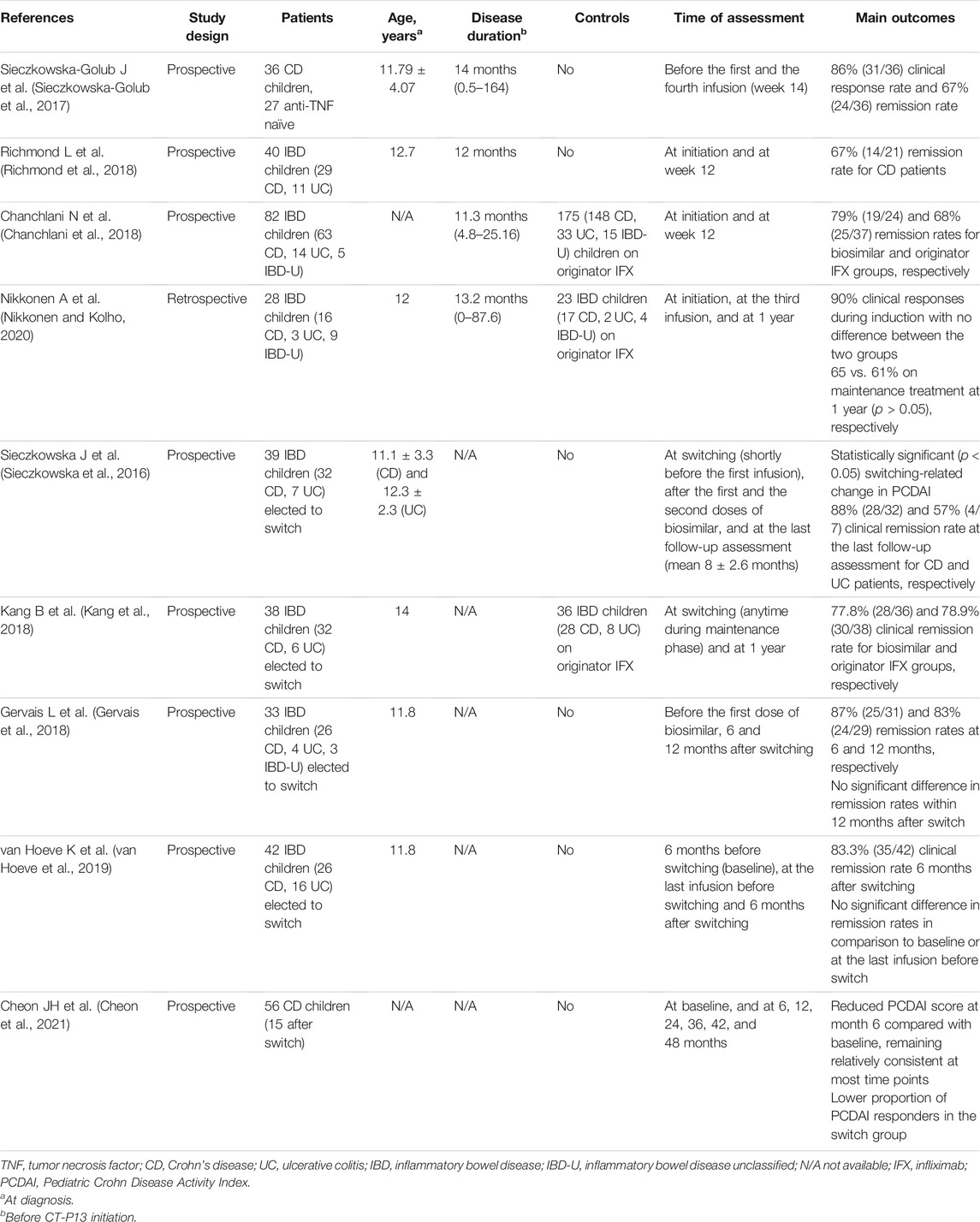
TABLE 1. Efficacy of biosimilars for pediatric inflammatory bowel disease.
Biosimilars as Primary Indication for anti-TNF-α
In a prospective Polish study, 36 pediatric CD patients were recruited from three institutions where the originator IFX was no longer accessible (Sieczkowska-Golub et al., 2017). CT-P13 treatment was indicated in the case of severe luminal CD and/or perianal disease that was resistant to standard treatment. Clinical response (a reduction of 12.5 points on the PCDAI) and remission (a PCDAI score of 10) were obtained in 86% and 67% of patients, respectively, at the end of the induction (week 14). No significant difference in remission rates between naïve and non-naive patients was found. The findings of this study were compared to those of the REACH study (Hyams et al., 2007), which established the efficacy and safety of the originator IFX, and identical clinical improvement and remission after three doses of biosimilar were shown. Other studies have shown similar remission rates (Chanchlani et al., 2018; Richmond et al., 2018). A prospective analysis of 278 IBD children from 27 UK sites found no differences in clinical response or remission rates after induction between the originator IFX (n = 82) and biosimilar IFX (n = 21) groups (Chanchlani et al., 2018). No significant difference in remission rates between the two groups was found. They were also compared new anti-TNF-α therapy patients to historical data from 398 patients who started on originator IFX in a prior United Kingdom IBD biologics audit (2011–2015) and they were found no significant differences in clinical response and remission rates at the same timepoint (Lynch et al., 2013; Russell et al., 2013). A retrospective Finnish study found that the originator IFX and biosimilar IFX therapies had similar first-year therapy outcomes, such as treatment intensification during follow-up (83 vs. 82%); treatment discontinuation during induction (8.7 vs. 3.6%) or follow-up (because of loss of response or adverse reaction; 39 vs. 36%); and treatment discontinuation due to anti drug antibodies (ADA) (17 vs. 3.4%) (Nikkonen and Kolho, 2020).
Biosimilars in Patients Switching From Originator anti-TNF-α
A total of 152 children (116 CD, 33 UC, and 3 IBD-U) were examined in five studies after switching from the originator IFX to CT-P13 (Sieczkowska et al., 2016; Gervais et al., 2018; Kang et al., 2018; van Hoeve et al., 2019; Cheon et al., 2021). In a prospective study, 39 IBD children were switched after (n = 37) or during (n = 2) induction (Sieczkowska et al., 2016). The effectiveness at the last biosimilar doses was assessed, and clinical remission rates for CD and UC patients were found to be 88% and 57%, respectively. Eighty percent of CD patients and all 4 UC patients who continued biosimilars at the last assessment visit (i.e., 11 months after the first patient had been switched, after a mean follow-up of 8 ± 2.6 months) were in remission (Sieczkowska et al., 2016). Later studies found similar results, with no clinically important changes in disease activity after switching. A prospective single-center study conducted in South Korea compared 38 IBD patients after the switch to CT-P13 with 36 patients remained on the originator IFX (Kang et al., 2018). Maintenance treatment of 1-year duration was continued by 86.1% of the patients on originator IFX, and 92.1% of those on biosimilar IFX. Eight patients did not complete the year of follow-up, because of complete remission (n = 3), loss of response and change to adalimumab (n = 3), and loss at follow-up (n = 2). Similar rates (77.8 vs. 78.9%) of sustained remission (i.e., 1 year of corticosteroid-free clinical remission with no further dose intensification) were observed in the two groups (Kang et al., 2018).
Biomarkers Changes
Seven out of nine studies evaluated inflammatory biomarker changes (Supplementary Box). The Polish study evaluated C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), platelets, and as well as hemoglobin (Hb) levels (Sieczkowska-Golub et al., 2017). CRP, ESR, and platelets had a significant reduction in all children who achieved a clinical response (Sieczkowska-Golub et al., 2017). More than half (59%) of individuals with elevated CRP levels at baseline had their CRP levels totally restored by week 14. In addition, one of the three children with anemia at week 0 had normalized Hb levels at week 14 (Sieczkowska-Golub et al., 2017). Similarly, Richmond et al. (Richmond et al., 2018) showed a significant decrease in CRP, ESR, and albumin serum levels at the end of induction with CT-P13. Studies investigating the switching from originator IFX to CT-P13 found no significant changes of inflammatory markers after switching (Sieczkowska et al., 2016; Gervais et al., 2018; Kang et al., 2018; van Hoeve et al., 2019). Fecal calprotectin was included in the analysis in four studies (Gervais et al., 2018; Kang et al., 2018; Richmond et al., 2018; Nikkonen and Kolho, 2020). Decreases were found to be not significant neither between baseline and follow-up visits, nor after switching from the originator IFX.
Through Concentration
Five studies evaluated trough levels (TL) of IFX biosimilar (Table 2) (Gervais et al., 2018; Kang et al., 2018; Richmond et al., 2018; van Hoeve et al., 2019; Nikkonen and Kolho, 2020). Therapeutic trough values, when reported, were assessed to be in the range of 3–7 mg/L post-induction. When comparing CT-P13 patients to those on originator IFX, there were no significant differences in TL. Likewise, there was no substantial difference in TL changes after switching from originator IFX to CT-P13. Dose escalation or treatment intensification were used to optimize treatment for patients with subtherapeutic levels at baseline (Nikkonen and Kolho, 2020). Switching on immunogenicity has been examined in five pediatric studies (Gervais et al., 2018; Kang et al., 2018; Richmond et al., 2018; van Hoeve et al., 2019; Nikkonen and Kolho, 2020). After switching to the biosimilar CT-P13, it was not found any substantial increase in immunogenicity. When available, mean ADA levels did not differ substantially.
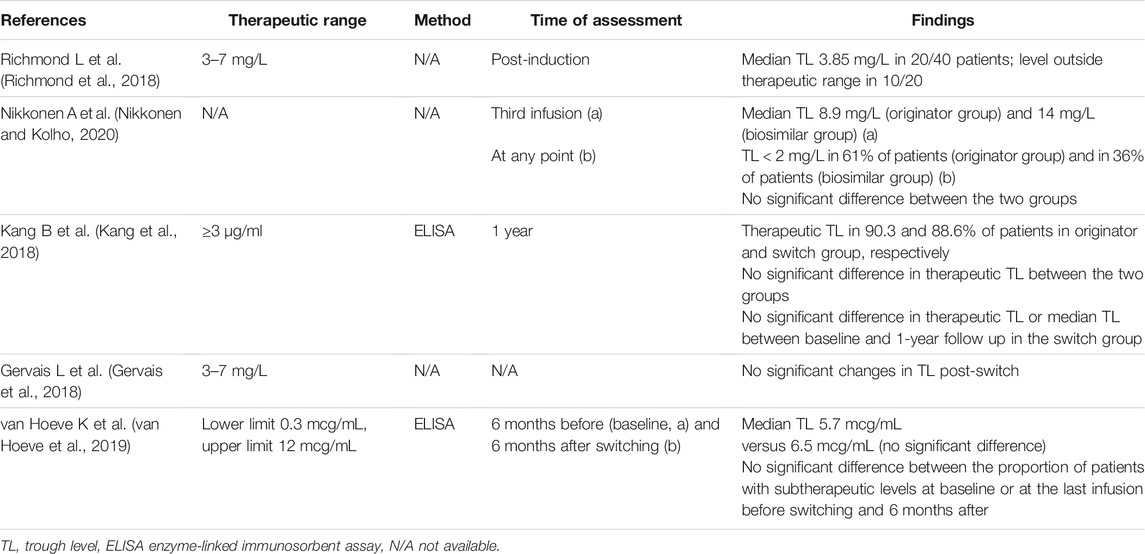
TABLE 2. Studies investigating trough levels.
Safety and Immunogenicity
Current available literature data reported only mildly to moderately severe adverse events (AEs) related to the IFX biosimilar. AEs related to IFX biosimilars in pediatric IBD patients were investigated in eight studies (Table 3) (Sieczkowska et al., 2016; Sieczkowska-Golub et al., 2017; Chanchlani et al., 2018; Gervais et al., 2018; Kang et al., 2018; Richmond et al., 2018; van Hoeve et al., 2019; Nikkonen and Kolho, 2020). In comparison to patients on originator IFX, CT-P13 patients had no significant differences in AE rates. Similarly, there was no significant difference when switching from originator IFX to CT-P13. Mild infections, predominantly upper respiratory tract infections, were the most commonly reported AEs. Three cases of Herpes zoster reactivation have been documented, one of which occurred after the first infusion of biosimilar IFX and necessitated therapy withdrawal (Sieczkowska et al., 2016). In seven cases, acute infusion reactions (AIRs) were observed, and in three of these, therapy was stopped (Sieczkowska et al., 2016; Sieczkowska-Golub et al., 2017; van Hoeve et al., 2019). During biosimilar treatment, one patient developed an ovarian teratoma (Sieczkowska et al., 2016). There was no information provided on demographics or disease progression. The patient had a total surgical ovary excision between consecutive biosimilar infusions. There was no need to adjust the dose. Cheon et al. (2021) found no additional safety findings in IBD patients treated with CT-P13 for up to 5 years, whether they were treated with or switched to CT-P13. In any case, there was no age-based subgroup analysis.
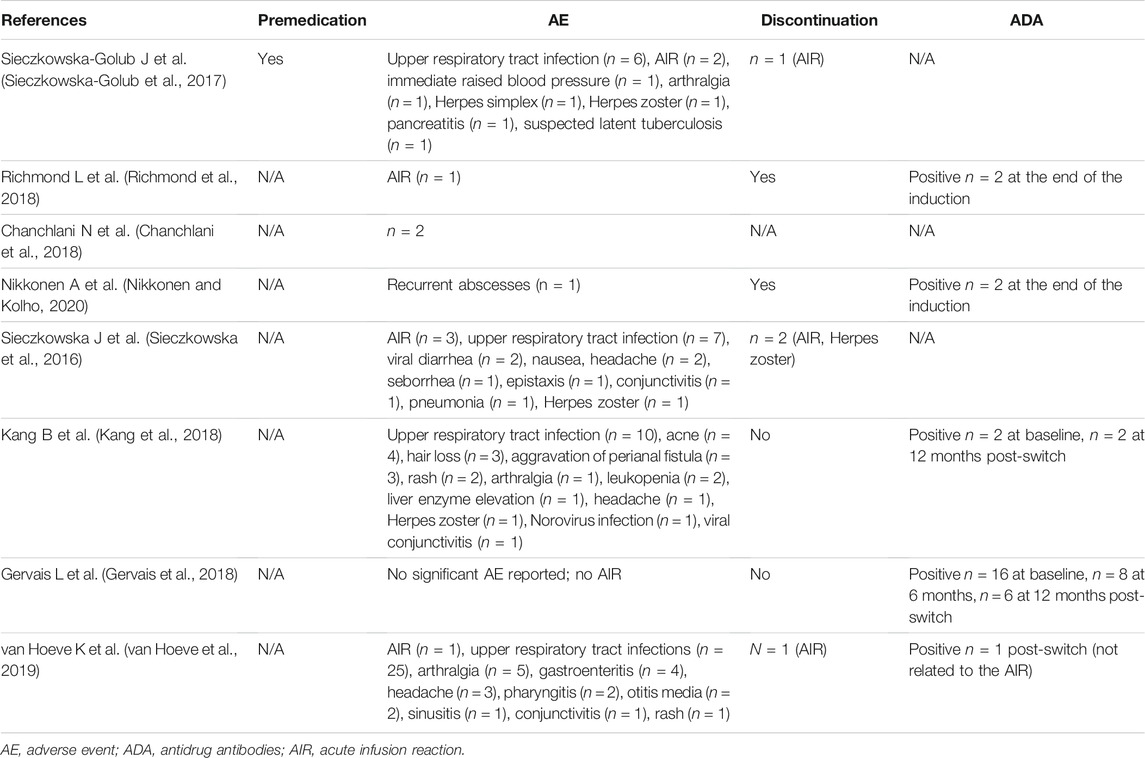
TABLE 3. Reported adverse events.
Costs
Three out of nine studies reported comparison of costs between originator IFX and CT-P13 (Table 4) (Chanchlani et al., 2018; Gervais et al., 2018; Richmond et al., 2018). All available data reported considerable cost reductions from using biosimilar IFX based on estimated and averaged local procurement rates.

TABLE 4. Cost saving in comparison to treatment with originator.
Discussion
Overall, the findings of this systematic review article establish CT-P13 effectiveness as measured by clinical response and/or remission rates after induction or during maintenance and suggest that it does not significantly differ from that of the originator IFX.
Because the originator IFX is often no longer available, most IBD units have had to switch to or to start with its biosimilars (de Ridder et al., 2019; Dipasquale and Romano, 2020). Access to the originator IFX is also often limited due to the originator’s relatively expensive cost (de Ridder et al., 2019; Hughes et al., 2021). A growing number of children with IBD who have used biologics are being elected to switch to biosimilars (de Ridder et al., 2019; Dipasquale and Romano, 2020). Children with IBD were effectively transitioned from the originator IFX to CTP13 in available studies, without affecting the effectiveness, pharmacokinetics, immunogenicity, and safety (Sieczkowska et al., 2016; Gervais et al., 2018; Kang et al., 2018; van Hoeve et al., 2019). Switching occurred primarily during the maintenance phase and did not appear to be associated with a loss of efficacy over time, even in patients with mild-to-moderate disease activity. Single switches have been used in all studies. Following at least three induction infusions, ESPGHAN guidelines recommend transitioning to CT-P13 in IBD children in clinical remission (de Ridder et al., 2019). Because evidence on interchangeability is still sparse, multiple switches (>1 switch) between different biosimilars or between biosimilars and the originator are not currently advised (de Ridder et al., 2019). Switching to biosimilar IFX might raise the risk of immunogenicity, which is one of the key concerns about biosimilar usage in the pediatric IBD group. Loss of response, AEs, and delayed hypersensitivity responses are all linked to immunogenicity, as well as the formation of IFX ADA (Allez et al., 2010). All biologics have varying degrees of immunogenicity, and even modest variations in the formulation, purity, or packaging of a biological medication might impact its immunogenicity pattern (Gabbani et al., 2017). The findings of this systematic review suggest that biosimilars appear to be safe in pediatric IBD patients. Additionally, switching from the originator drug does not appear to raise immunogenicity considerably.
Biosimilars offer a more advantageous costing and reimbursement strategy, with price cuts ranging from 25 to 70% in Europe when compared to originator products (Brodszky et al., 2016). More than 90% of respondents in the previously cited Italian survey believed biosimilars to be cost-effective, with cost savings being the most important benefit of using biosimilars (Dipasquale et al., 2021). If the cost savings from the use of biosimilars were used to fund more biological treatments, several more IBD patients could be treated.
The extensive and systematic literature search is one of the strengths of this systematic review. The limitations largely reflect the shortcomings of the studies reviewed. First, they are observational studies reporting real-life data. Second, some of the included studies were limited with respect to sampling and generalizability. Moreover, the efficacy of biosimilars in the induction of mucosal healing was not investigated. Pediatric clinical trials and eventually more research into post-marketing surveillance data on effectiveness, safety, and immunogenicity are highly needed. Data on the efficacy and safety of adalimumab biosimilars in children with IBD are also warranted.
Conclusion
More experiences regarding the effectiveness, immunogenicity, and interchangeability of biosimilars in pediatric IBD have been reported over the last few years. Their utilization has almost completely substituted that of the originator IFX due to greater availability and lower costs. There are no differences in efficacy and safety between originator IFX and CT-P13, according to current evidence. Nonetheless, regulatory legislation needs to be standardized, and more data on the interchangeability, pharmacokinetics, as well as pediatric specificities, are still desirable.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.846151/full#supplementary-material
References
Allez, M., Karmiris, K., Louis, E., Van Assche, G., Ben-Horin, S., Klein, A., et al. (2010). Report of the ECCO Pathogenesis Workshop on Anti-TNF Therapy Failures in Inflammatory Bowel Diseases: Definitions, Frequency and Pharmacological Aspects. J. Crohns. Colitis. 4, 355–366. doi:10.1016/j.crohns.2010.04.004
Alten, R., and Cronstein, B. N. (2015). Clinical Trial Development for Biosimilars. Semin. Arthritis Rheum. 44, S2–S8. doi:10.1016/j.semarthrit.2015.04.002
Brodszky, V., Rencz, F., Péntek, M., Baji, P., Lakatos, P. L., and Gulácsi, L. (2016). A Budget Impact Model for Biosimilar Infliximab in Crohn's Disease in Bulgaria, the Czech Republic, Hungary, Poland, Romania, and Slovakia. Expert Rev. Pharmacoecon. Outcomes Res. 16, 119–125. doi:10.1586/14737167.2015.1067142
Chanchlani, N., Mortier, K., Williams, L. J., Muhammed, R., Auth, M. K. H., Cosgrove, M., et al. (2018). Use of Infliximab Biosimilar versus Originator in a Pediatric United Kingdom Inflammatory Bowel Disease Induction Cohort. J. Pediatr. Gastroenterol. Nutr. 67, 513–519. doi:10.1097/MPG.0000000000002011
Cheon, J. H., Nah, S., Kang, H. W., Lim, Y. J., Lee, S. H., Lee, S. J., et al. (2021). Infliximab Biosimilar CT-P13 Observational Studies for Rheumatoid Arthritis, Inflammatory Bowel Diseases, and Ankylosing Spondylitis: Pooled Analysis of Long-Term Safety and Effectiveness. Adv. Ther. 38, 4366–4387. doi:10.1007/s12325-021-01834-3
Danese, S., Fiorino, G., Raine, T., Ferrante, M., Kemp, K., Kierkus, J., et al. (2017). ECCO Position Statement on the Use of Biosimilars for Inflammatory Bowel Disease-An Update. J. Crohns. Colitis. 11, 26–34. doi:10.1093/ecco-jcc/jjw198
de Ridder, L., Assa, A., Bronsky, J., Romano, C., Russell, R. K., Afzal, N. A., et al. (2019). Paediatric IBD Porto Group of ESPGHANUse of Biosimilars in Pediatric Inflammatory Bowel Disease: an Updated Position Statement of the Pediatric IBD Porto Group of ESPGHAN. J. Pediatr. Gastroenterol. Nutr. 68, 144–153. doi:10.1097/MPG.0000000000002141
de Ridder, L., Waterman, M., Turner, D., Bronsky, J., Hauer, A. C., Dias, J. A., et al. ESPGHAN Paediatric IBD Porto Group (2015). Use of Biosimilars in Paediatric Inflammatory Bowel Disease: a Position Statement of the ESPGHAN Paediatric IBD Porto Group. J. Pediatr. Gastroenterol. Nutr. 61, 503–508. doi:10.1097/MPG.0000000000000903
Dipasquale, V., and Romano, C. (2020). Biosimilar Infliximab in Paediatric Inflammatory Bowel Disease: Efficacy, Immunogenicity and Safety. J. Clin. Pharm. Ther. 45, 1228–1234. doi:10.1111/jcpt.13239
Dipasquale, V., Martinelli, M., Aloi, M., Accomando, S., Alvisi, P., Arrigo, S., et al. (2021). Real-life Use of Biosimilars in Pediatric Inflammatory Bowel Disease: a Nation-wide Web Survey on Behalf of the SIGENP IBD Working Group. Pediatr. Drugs 24, 57–62. doi:10.1007/s40272-021-00486-8
Farkas, K., Rutka, M., Bálint, A., Nagy, F., Bor, R., Milassin, Á., et al. (2015). Efficacy of the New Infliximab Biosimilar CT-P13 Induction Therapy in Crohn's Disease and Ulcerative Colitis - Experiences from a Single center. Expert Opin. Biol. Ther. 15, 1257–1262. doi:10.1517/14712598.2015.1064893
Gabbani, T., Deiana, S., and Annese, V. (2017). CT-P13: Design, Development, and Place in Therapy. Drug Des. Devel. Ther. 11, 1653–1661. doi:10.2147/DDDT.S109852
Gecse, K. B., Lovász, B. D., Farkas, K., Banai, J., Bene, L., Gasztonyi, B., et al. (2016). Efficacy and Safety of the Biosimilar Infliximab CT-P13 Treatment in Inflammatory Bowel Diseases: a Prospective, Multicentre, Nationwide Cohort. J. Crohns. Colitis. 10, 133–140. doi:10.1093/ecco-jcc/jjv220
Gervais, L., McLean, L. L., Wilson, M. L., Cameron, C., Curtis, L., Garrick, V., et al. (2018). Switching from Originator to Biosimilar Infliximab in Paediatric Inflammatory Bowel Disease Is Feasible and Uneventful. J. Pediatr. Gastroenterol. Nutr. 67, 745–748. doi:10.1097/MPG.0000000000002091
Hughes, A., Marshall, J. K., Moretti, M. E., and Ungar, W. J. (2021). A Cost-Utility Analysis of Switching from Reference to Biosimilar Infliximab Compared to Maintaining Reference Infliximab in Adult Patients with Crohn's Disease. J. Can. Assoc. Gastroenterol. 4, 48. doi:10.1093/jcag/gwz045
Hyams, J., Crandall, W., Kugathasan, S., Griffiths, A., Olson, A., Johanns, J., et al. REACH Study Group (2007). Induction and Maintenance Infliximab Therapy for the Treatment of Moderate-To-Severe Crohn's Disease in Children. Gastroenterology 132, 863–866. doi:10.1053/j.gastro.2006.12.003
Hyams, J., Damaraju, L., Blank, M., Johanns, J., Guzzo, C., Winter, H. S., et al. T72 Study Group (2012). Induction and Maintenance Therapy with Infliximab for Children with Moderate to Severe Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 10, 391–e1. doi:10.1016/j.cgh.2011.11.026
Jahnsen, J., Detlie, T. E., Vatn, S., and Ricanek, P. (2015). Biosimilar Infliximab (CT-P13) in the Treatment of Inflammatory Bowel Disease: a Norwegian Observational Study. Expert Rev. Gastroenterol. Hepatol. 9 (Suppl. 1), 45–52. doi:10.1586/17474124.2015.1091308
Kang, B., Lee, Y., Lee, K., Choi, Y. O., and Choe, Y. H. (2018). Long-term Outcomes after Switching to CT-P13 in Pediatric-Onset Inflammatory Bowel Disease: a Single-center Prospective Observational Study. Inflamm. Bowel Dis. 24, 607–616. doi:10.1093/ibd/izx047
Laharie, D., Salzmann, M., Boubekeur, H., Richy, F., Amouretti, M., Quinton, A., et al. (2005). Predictors of Response to Infliximab in Luminal Crohn's Disease. Gastroenterol. Clin. Biol. 29, 145–149. doi:10.1016/s0399-8320(05)80718-3
Lynch, R. W., Lowe, D., Protheroe, A., Driscoll, R., Rhodes, J. M., and Arnott, I. D. (2013). Outcomes of rescue Therapy in Acute Severe Ulcerative Colitis: Data from the United Kingdom Inflammatory Bowel Disease Audit. Aliment. Pharmacol. Ther. 38, 935–945. doi:10.1111/apt.12473
Nikkonen, A., and Kolho, K. L. (2020). Infliximab and its Biosimilar Produced Similar First-Year Therapy Outcomes in Patients with Inflammatory Bowel Disease. Acta Paediatr. 109, 836–841. doi:10.1111/apa.15026
Organization site European Medicines Agency, (2013). Committee for Medicinal Products for Human Use (CHMP). Assessment report: Inflectra (infliximab). Available at: http://www.ema.europa/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002778/WC500151490.pdf (Accessed August 3, 2018).
Organization site World Health Organization, (2017). Expert Committee on Biological Standardization Geneva. Report on a Collaborative Study for Proposed 1st International Standard for Infliximab. Available at: http://www.who.int/biologicals/expert_committee/BS2323_Infliximab_ECBS_2017_V.6.1.pdf (Accessed August 3, 2018).
Park, W., Hrycaj, P., Jeka, S., Kovalenko, V., Lysenko, G., Miranda, P., et al. (2013). A Randomised, Double-Blind, Multicentre, Parallel-Group, Prospective Study Comparing the Pharmacokinetics, Safety, and Efficacy of CT-P13 and Innovator Infliximab in Patients with Ankylosing Spondylitis: the PLANETAS Study. Ann. Rheum. Dis. 72, 1605–1612. doi:10.1136/annrheumdis-2012-203091
Richmond, L., Curtis, L., Garrick, V., Rogers, P., Wilson, M., Tayler, R., et al. (2018). Biosimilar Infliximab Use in Paediatric IBD. Arch. Dis. Child. 103, 89–91. doi:10.1136/archdischild-2017-313404
Ruemmele, F. M., Veres, G., Kolho, K. L., Griffiths, A., Levine, A., Escher, J. C., et al. (2014). Consensus Guidelines of ECCO/ESPGHAN on the Medical Management of Pediatric Crohn’s Disease. J. Crohns. Colitis. 8, 1179–1207. doi:10.1016/j.crohns.2014.04.005
Russell, R. K., Protheroe, A., Roughton, M., Croft, N. M., Murphy, M. S., Spray, C., et al. (2013). Contemporary Outcomes for Ulcerative Colitis Inpatients Admitted to Pediatric Hospitals in the United Kingdom. Inflamm. Bowel Dis. 19, 1434–1440. doi:10.1097/MIB.0b013e31828133d6
Sieczkowska, J., Jarzębicka, D., Banaszkiewicz, A., Plocek, A., Gawronska, A., Toporowska-Kowalska, E., et al. (2016). Switching between Infliximab Originator and Biosimilar in Paediatric Patients with Inflammatory Bowel Disease. Preliminary Observations. J. Crohns Colitisj. Crohns. Colitis. 10, 127–132. doi:10.1093/ecco-jcc/jjv233
Sieczkowska-Golub, J., Meglicka, M., Plocek, A., Banaszkiewicz, A., Jarzębicka, D., Toporowska-Kowalska, E., et al. (2017). Induction Therapy with Biosimilar Infliximab in Children with Crohn Disease. J. Pediatr. Gastroenterol. Nutr. 65, 285–288. doi:10.1097/MPG.0000000000001643
Turner, D., Ruemmele, F. M., Orlanski-Meyer, E., Griffiths, A. M., de Carpi, J. M., Bronsky, J., et al. (2018). Management of Paediatric Ulcerative Colitis, Part 1: Ambulatory Care-An Evidence-Based Guideline from European Crohn's and Colitis Organization and European Society of Paediatric Gastroenterology, Hepatology and Nutrition. J. Pediatr. Gastroenterol. Nutr. 67, 257–291. doi:10.1097/MPG.0000000000002035
van Hoeve, K., Dreesen, E., Hoffman, I., Van Assche, G., Ferrante, M., Gils, A., et al. (2019). Efficacy, Pharmacokinetics, and Immunogenicity Is Not Affected by Switching from Infliximab Originator to a Biosimilar in Pediatric Patients with Inflammatory Bowel Disease. Ther. Drug Monit. 41, 317–324. doi:10.1097/FTD.0000000000000601
Vande Casteele, N., and Sandborn, W. J. (2015). IBD: Indication Extrapolation for Anti-TNF Biosimilars. Nat. Rev. Gastroenterol. Hepatol. 12, 373–374. doi:10.1038/nrgastro.2015.104
Weise, M., Kurki, P., Wolff-Holz, E., Bielsky, M. C., and Schneider, C. K. (2014). Biosimilars: the Science of Extrapolation. Blood 124, 3191–3196. doi:10.1182/blood-2014-06-583617
World Health Organization (2009). Guidelines on Evaluation of Similar Biotherapeutic Products (SBPs), Expert Committee on Biological Standardization. Geneva: World Health Organization.
Ye, B. D., Pesegova, M., Alexeeva, O., Osipenko, M., Lahat, A., Dorofeyev, A., et al. (2019). Efficacy and Safety of Biosimilar CT-P13 Compared with Originator Infliximab in Patients with Active Crohn's Disease: an International, Randomised, Double-Blind, Phase 3 Non-inferiority Study. Lancet 393, 1699–1707. doi:10.1016/S0140-6736(18)32196-2
Yoo, D. H., Hrycaj, P., Miranda, P., Ramiterre, E., Piotrowski, M., Shevchuk, S., et al. (2013). A Randomised, Double-Blind, Parallel-Group Study to Demonstrate Equivalence in Efficacy and Safety of CT-P13 Compared with Innovator Infliximab when Coadministered with Methotrexate in Patients with Active Rheumatoid Arthritis: the PLANETRA Study. Ann. Rheum. Dis. 72, 1613–1620. doi:10.1136/annrheumdis-2012-203090
Keywords: biosimilar, crohn’s disease, CT-P13, inflammatory bowel disease, pediatrics, safety, ulcerative colitis, anti-TNF-α
Citation: Dipasquale V, Cicala G, Spina E and Romano C (2022) Biosimilars in Pediatric Inflammatory Bowel Diseases: A Systematic Review and Real Life-Based Evidence. Front. Pharmacol. 13:846151. doi: 10.3389/fphar.2022.846151
Received: 30 December 2021; Accepted: 24 February 2022;
Published: 17 March 2022.
Edited by:
Annalisa Capuano, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Prevost Jantchou, Division of Gastroenterology, Hepatology and Nutrition, CHU Sainte Justine, Montreal, QC, CanadaDaniela Pugliese, Fondazione Policlinico Universitario “A. Gemelli” IRCCS, Italy
Copyright © 2022 Dipasquale, Cicala, Spina and Romano. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Claudio Romano, cm9tYW5vY0B1bmltZS5pdA==