 Robyn Brown
Robyn Brown Caryl James Bateman
Caryl James Bateman Maxine Gossell-Williams
Maxine Gossell-Williams- 1Department of Sociology, Psychology, and Social Work, Faculty of Social Sciences, The University of the West Indies, Mona Campus, Kingston, Jamaica
- 2Section of Pharmacology and Pharmacy, Faculty of Medical Sciences, The University of the West Indies, Mona Campus, Kingston, Jamaica
Worldwide, socio-cultural determinants have been shown to influence the beliefs of patients about their health and decision making for treatment. This is consistent with the evidence that cultural and religious beliefs affect illness conceptualization and behaviors of Jamaican patients living with non-communicable diseases, such as diabetes mellitus and hypertension. Despite these known socio-cultural influences, an acknowledgment of relevance of adherence to pharmacotherapy has been grossly understudied. Furthermore, while poor adherence to pharmacotherapy, especially in the management of patients living with non-communicable diseases is associated with adverse drug reactions; reporting of such information in the pharmacovigilance process is inadequate. We review previous studies on the cultural and religious beliefs within the Jamaican context that may contribute to poor adherence to pharmacotherapy, especially among those patients living with non-communicable diseases. We support the ongoing perspective that current pharmacovigilance processes need retooling with the inclusion of socio-cultural influences on adherence to pharmacotherapy.
Introduction
Non-communicable diseases (NCDs) represent a significant portion of the global disease burden and are managed by lifelong pharmacotherapy. According to the World Health Organization (WHO), NCDs disproportionally affect developing countries and among these patients, adherence to pharmacotherapy rates is less than fifty percent (Sabaté, 2003). These challenges coupled with the limited resources to care for the health needs of its population increases the morbidity and mortality rates of NCDs in developing countries (Rose et al., 2016). Developing countries, such as Jamaica, encounter unique challenges at the various levels of the healthcare system (Figueroa et al., 1999; Wilks et al., 2001; Gossell-Williams et al., 2014; Hartzler et al., 2014; Mitchell-Fearon et al., 2015; Wilson et al., 2018). However, arguably and more important in impacting public health is having a health-conscious populace that is motivated to leverage the health system to the betterment of their overall well-being.
According to terminology agreed by European consensus, adherence to pharmacotherapy is defined as the process by which patients take their medications as prescribed (Vrijens et al., 2012). A major contributor to adherence to pharmacotherapy is culture which is defined as a decision-making heuristic that can be found in values, beliefs, or social norms (Nunn, 2012). More specifically, various sociocultural factors have been found to affect patient health behaviours, decision-making and health outcomes (Oates et al., 2020), of which multidimensional factors, such as cultural and religious beliefs are among the most recognized (Leporini et al., 2014). Hordern (2016) emphasized the need for physicians to understand and respect the significance of cultural and religious beliefs of patients, as they inform the manner of their engagement with recommended treatment.
The goal of this paper is to explore how these socio-cultural factors impact adherence to pharmacotherapy for common NCDs in Jamaica, as well as to highlight their potential role in the pharmacovigilance process. We highlight peer reviewed publications reporting adherence to pharmacotherapy in Jamaican patients with NCDs after 2003, the year of implementation of the National Health Fund, which subsidizes the cost of drugs to Jamaicans (https://www.nhf.org.jm/images/pdfs/nhf_act_merged.pdf). The available studies involving Jamaican patients with NCDs suggest their adherence to pharmacotherapy is poor, with concerns about adverse drug reactions, having to take the drugs consistently even when no symptoms are being experienced and the general inconvenience featuring prominently. (Table 1) (Duff et al., 2006; Chambers et al., 2008; Pusey-Murray et al., 2010; Mowatt, 2013; Gossell-Williams et al., 2014; Welsh et al., 2015; Bridgelal-Nagassar et al., 2016; Wilson et al., 2018; Adeniyi et al., 2021; Barrett-Brown et al., 2021).
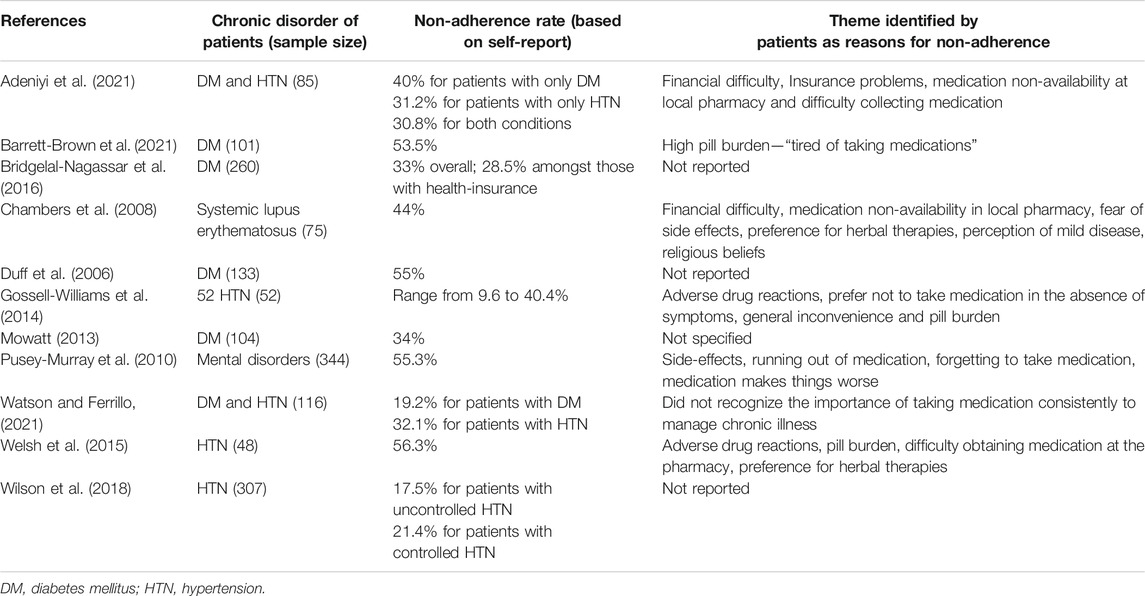
TABLE 1. Overview of the studies presenting measures of non-adherences among Jamaicans living with NCDs. For all studies the measure of adherence.
Beliefs About Illness
Beliefs as defined by Macionis (2015, p. 95) are “specific thoughts or ideas that people hold to be true”. Understanding patients’ health beliefs is imperative as research has consistently shown that this predicts their health behaviors, including adherence to pharmacotherapy (Street and Haidet, 2011). Cultural beliefs relate to what is internalized to inform thinking and actions, while religious beliefs relate to beliefs in a social institution based on recognizing the sacred (Macionis, 2015). These terms are not mutually exclusive, as religion may be considered a cultural system (Bonney, 2004).
The way illness is conceptualized through a particular cultural lens has a direct impact on the kinds of actions taken in its management. Considering the diversity implicit within the Jamaican experience, it is difficult to define a cultural attitude towards pharmacological intervention which is all encompassing. However, insights have been offered to explain relevant ethnographic factors. Mitchell (1983) gave a comprehensive description of the ethnomedical landscape in Jamaica during the 1980s which is still relevant nearly 40 years later. The way in which Jamaicans conceptualize and treat diseases involve an emphasis on symptomatology and bodily-feeling; there is a need to feel a “cure” working in the body to counteract a particular ill-effect and the elimination of symptoms through treatment signifies the elimination of the disease, regardless of whether it is chronic and incurable (Mitchell, 1983). These perceptions have been corroborated in survey studies done amongst patients in Jamaica and the Jamaican diaspora living in the United Kingdom and the United States of America where poor adherence to pharmacotherapy was related to the practice of “leaving-off” pills, which was justified by the idea that illness exists only in the presence of symptoms (Myfanwy and Watkins, 1988; Brown et al., 2007; Alhomoud et al., 2013; Smith, 2012; Gossell-Williams et al., 2014; Welsh et al., 2015).
Beliefs About Alternative Treatments
The desire to feel a cure working is one potential explanation for the cultural beliefs in herbal preparations observed throughout Jamaican society. Many herbal preparations, especially in the form of teas, elicit instantaneous bodily sensations, such as “warmth” or “bitterness.” For example, Cerasee tea (made from the plant Momordica charantia) is viewed as an effective treatment for diabetes mellitus because of the perceived counteracting or balancing effect of the bitter taste (Mitchell, 1983; Smith, 2012). It is important to explore not only whether herbal preparations are efficacious, but also the cultural cognitions that lead Jamaican’s to combat illness in a particular way. Sobo (1993) examined the health perspectives of impoverished rural Jamaicans and how they approach well-being. There was an emphasis on natural, easily accessible options with attention being paid most carefully to the balancing of the system through “washouts” and “purification” rather than taking prescription drugs.
Considering Jamaica’s extensive history of traditional knowledge systems (Payne-Jackson and Alleyne, 2004; Seaga, 2005; Delgoda et al., 2010; Picking et al., 2019; Adeniyi et al., 2021; Bateman James, 2021), it is not surprising that Jamaicans from various backgrounds turn regularly to alternative treatments. Records of the 1866 Commission investigating the Morant Bay Rebellion highlight the long history of Jamaicans consulting physicians on current medicine, but then relying on alternative treatments (Barima, 2016). Payne-Jackson and Alleyne (2004) in their 1991–1992 questionnaire-based survey of rural communities in Jamaica highlighted the involvement of physicians and alternative practitioners (e.g., bush-doctors, spiritual mothers and occult healers) in the treatment of illness, which inevitably leads to several treatment recommendations being used sequentially and simultaneously. This approach towards managing illness remains popular and thus the prescribed pharmacotherapy is often replaced or supplemented with alternative treatment options, popularly believed to be effective (Mitchell, 1983; Gardner et al., 2000; Delgoda et al., 2004; Gossell-Williams et al., 2008; Delgoda et al., 2010; Picking et al., 2011; Welsh et al., 2015; Foster et al., 2017; Owusu et al., 2020; Adeniyi et al., 2021). Patient testimonials about the anti-cancer benefits of herbal preparations travel by word of mouth, reaffirming their perceived efficacy and swaying others towards their utilization. Owusu et al. (2020) found in a western Jamaican sample of patients with hypertension and type two diabetes mellitus that the motivation for an alternative treatment plan included the belief that it is the more natural choice, and the belief that it is beneficial to utilize pharmacological and herbal preparations concurrently.
In exploring the factors which contribute to the popularity of herbal preparations in Jamaica, especially for the treatment of cancer, Foster et al. (2017) found that 80% of patients surveyed used them, often without the knowledge of their oncologist. In a survey canvasing the level of herbal preparation use concomitantly with pharmacological interventions amongst Jamaicans in both urban and rural settings, Picking et al. (2011) found that 72.6% of respondents had used herbal preparations in the last 12 months. Additionally, of those who were using both forms of treatment simultaneously, only 19.4% shared this information with their physician (Picking et al., 2011) corroborating the findings of Foster et al. (2017). One reason cited for withholding the self-administering of herbal preparations is that the physician simply did not ask (Picking et al., 2011; Smith 2012; Owusu et al., 2020). This presents a major concern about the risk of adverse drug reactions to concomitant users and reasons for this gap in patient-physician communication need to be explored.
Religious Beliefs About Illness and Pharmacotherapy
Several religions are practiced in Jamaica and although the influence of religious beliefs on illness and healing perception have been reviewed (Sutherland et al., 2014), the relationship between religious beliefs and adherence to pharmacotherapy has been minimally explored. At an individual level, the influence of religion is highly subjective with some patients interpreting their healthcare provider’s recommendations as God’s way of helping them to help themselves, while others take a more fatalistic approach believing that their illness is God’s will and therefore how it unfolds is out of their hands (Brown et al., 2007; Shahin et al., 2019; Smith, 2012; Hope et al., 2020). Taking this line of reasoning one step further, some highly religious patients may believe that their illness is a punishment from God for improper religious adherence and although they may respect their physician’s diagnosis and recommendations, their ultimate concern rests with the judgement of their higher power (Rumun, 2014).
Chambers et al. (2008) explored the influence of Christianity among Jamaicans living with systemic lupus erythematosus; they found that several of the patients held a “strong belief in the possibility that they could be healed of lupus at any time” p.767. Amongst this cohort however these beliefs did not appear to hinder their adherence to pharmacotherapy. Anecdotal reports included the belief that healing was obtained at a crusade, leading to a patient ceasing to take their medication and their eventual death. Another patient reported finding prayer to be an effective way for them to relieve some of their pain and discomfort until they were able to replenish their medication (Chambers et al., 2008).
A Role for Cultural and Religious Beliefs in the Pharmacovigilance Process
Jamaica, as a full member of the World Health Organization global database since 2012, collects individual case safety reports of adverse drug reactions following guidelines established by the International Conference on Harmonization (E2B (R3) Individual case Safety Report Specification and Related Files; https://www.ich.org/page/e2br3-individual-case-safety-report-icsr-specification-and-related-files). This global pharmacovigilance database facilitates detection of possible adverse drug reactions; however, the processes of data analysis and whether there is adequate focus on patient safety has been questioned (Edwards, 2017; Streefland, 2018; Ibrahim et al., 2021). According to Edwards (2017, p. 365) “We must develop a more holistic evaluation of suboptimal therapeutic outcomes, and do this without apportioning unnecessary blame”.
Recent systematic reviews and observational studies highlight the relevance of socio-cultural determinants on adherence to pharmacotherapy among patients living with NCDs (Dhar et al., 2017; Niriayo et al., 2018; Swihart et al., 2018; Shahin et al., 2019; Al-Ganmi et al., 2020; Park et al., 2020; Raza et al., 2020; Świątoniowska-Lonc et al., 2021); however, the dearth of published literature suggests such awareness in pharmacovigilance processes is yet to be realized. Although poor adherence to pharmacotherapy is a common predictor of adverse drug reactions; the converse is also true (Gellad et al., 2011; Adem et al., 2021; Elangwe et al., 2020) and therefore enriching pharmacovigilance processes with what is referred to as ‘the patient’s voice’ may facilitate causality analysis of adverse drug reactions (Simon et al., 2020).
Conclusion
Cultural and religious beliefs have been shown to negatively impact adherence to pharmacotherapy in patients living with NCDs; despite this, current pharmacovigilance processes fail to give these beliefs much consideration in understanding poor adherence to pharmacotherapy, a known contributor to adverse drug reaction occurrences. Elaborating on the possible relationship between these factors and poor adherence to pharmacotherapy in the Jamaican context was the goal of this article, with several notable themes emerging. Among these were the cultural perception of illness as existing only in the presence of symptoms, and the importance of combating illness by targeting symptoms with treatments that one can feel acting in the body. Also featured were religious influences on the way patients make meaning of their experience of illness, along with the role they ascribe to physicians in facilitating their treatment.
Based on the empirical articles reviewed, the cultural and religious beliefs of Jamaicans about pharmacotherapy may be a significant contributor to poor adherence rates among patients living with NCDs. Adding this information is important in a comprehensive pharmacovigilance process, and future research should explore the optimization of adverse drug reaction reporting with patient data in these domains.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Materials, further inquiries can be directed to the corresponding author.
Author Contributions
MG-W and RB conceived the study. RB led the sourcing of the relevant literature and worked with MG-W to analyse the literature. MG-W and RB worked together to complete the first draft of the article. CB reviewed the draft and made substantial intellectual contributions, including addition of personal work done on the topic. All subsequent drafts were reviewed by all authors, including the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Adem, F., Abdela, J., Edessa, D., Hagos, B., Nigussie, A., and Mohammed, M. A. (2021). Drug-related Problems and Associated Factors in Ethiopia: a Systematic Review and Meta-Analysis. J. Pharm. Pol. Pract 14 (1), 36–24. doi:10.1186/s40545-021-00312-z
Adeniyi, O., Washington, L., Glenn, C. J., Franklin, S. G., Scott, A., Aung, M., et al. (2021). The Use of Complementary and Alternative Medicine Among Hypertensive and Type 2 Diabetic Patients in Western Jamaica: A Mixed Methods Study. PLoS One 16 (2), e0245163. doi:10.1371/journal.pone.0245163
Al-Ganmi, A. H. A., Alotaibi, A., Gholizadeh, L., and Perry, L. (2020). Medication Adherence and Predictive Factors in Patients with Cardiovascular Disease: A Cross-Sectional Study. Nurs. Health Sci. 22 (2), 454–463. doi:10.1111/nhs.12681
Alhomoud, F., Dhillon, S., Aslanpour, Z., and Smith, F. (2013). Medicine Use and Medicine-Related Problems Experienced by Ethnic Minority Patients in the United Kingdom: a Review. Int. J. Pharm. Pract. 21 (5), 277–287. doi:10.1111/ijpp.12007
Barima, K. B. (2016). Cutting across Space and Time: Obeah’s Service to Jamaica’s freedom Struggle in Slavery and Emancipation. J. Pan Afr. Stud. 9 (4), 16–31.
Barrett-Brown, P., McGrowder, D., and Ragoobirsingh, D. (2021). Diabetes Education—Cornerstone in Management of Diabetes Mellitus in Jamaica. AIMS Med. Sci. 8 (3), 89–202. doi:10.3934/medsci.2021017
Bateman James, C. (2021). Traditional and Western Medicine: Voices from Jamaican Psychiatric Patients. University of the West Indies Press.
Bonney, R. (2004). Reflections on the Differences between Religion and Culture. Clin. Cornerstone 6 (1), 25–33. doi:10.1016/S1098-3597(04)90004-X
Bridgelal-Nagassar, R. J., James, K., Nagassar, R. P., and Maharaj, S. (2016). Medication Adherence and Health Insurance/health Benefit in Adult Diabetics in Kingston, Jamaica. West. Indian Med. J. 65 (2), 320–322. doi:10.7727/wimj.2014.282
Brown, K., Avis, M., and Hubbard, M. (2007). Health Beliefs of African-Caribbean People with Type 2 Diabetes: A Qualitative Study. Br. J. Gen. Pract. 57 (539), 461–469.
Chambers, S., Raine, R., Rahman, A., Hagley, K., De Ceulaer, K., and Isenberg, D. (2008). Factors Influencing Adherence to Medications in a Group of Patients with Systemic Lupus Erythematosus in Jamaica. Lupus 17 (8), 761–769. doi:10.1177/0961203308089404
Delgoda, R., Ellington, C., Barrett, S., Gordon, N., Clarke, N., and Younger, N. (2004). The Practice of Polypharmacy Involving Herbal and Prescription Medicines in the Treatment of Diabetes Mellitus, Hypertension and Gastrointestinal Disorders in Jamaica. West. Indian Med. J. 53 (6), 400–405.
Delgoda, R., Younger, N., Barrett, C., Braithwaite, J., and Davis, D. (2010). The Prevalence of Herbs Use in Conjunction with Conventional Medicines in Jamaica. Complement. Ther. Med. 18 (1), 13–20. doi:10.1016/j.ctim.2010.01.002
Dhar, L., Dantas, J., and Ali, M. (2017). A Systematic Review of Factors Influencing Medication Adherence to Hypertension Treatment in Developing Countries. OJEpi 07 (03), 211–250. doi:10.4236/ojepi.2017.73018
Duff, E. M., O'Connor, A., McFarlane-Anderson, N., Wint, Y. B., Bailey, E. Y., and Wright-Pascoe, R. A. (2006). Self-care, Compliance and Glycaemic Control in Jamaican Adults with Diabetes Mellitus. West. Indian Med. J. 55 (4), 232–236. doi:10.1590/s0043-31442006000400006
Elangwe, A., Katte, J. C., Tchapmi, D., Figueras, A., and Mbanya, J. C. (2020). Adverse Drug Reactions to Anti-diabetic Drugs Are Commonest in Patients Whose Treatment Do Not Adhere to Diabetes Management Clinical Guidelines: Cross-Sectional Study in a Tertiary Care Service in Sub-saharan Africa. Eur. J. Clin. Pharmacol. 76 (11), 1601–1605. doi:10.1007/s00228-020-02949-2
Figueroa, J. P., Fox, K., and Minor, K. (1999). A Behaviour Risk Factor Survey in Jamaica. West. Indian Med. J. 48 (1), 9–15.
Foster, K., Younger, N., Aiken, W., Brady-West, D., and Delgoda, R. (2017). Reliance on Medicinal Plant Therapy Among Cancer Patients in Jamaica. Cancer Causes Control 28 (11), 1349–1356. doi:10.1007/s10552-017-0924-9
Gardner, J. M., Grant, D., Hutchinson, S., and Wilks, R. (2000). The Use of Herbal Teas and Remedies in Jamaica. West. Indian Med. J. 49 (4), 331–335.
Gellad, W. F., Grenard, J. L., and Marcum, Z. A. (2011). A Systematic Review of Barriers to Medication Adherence in the Elderly: Looking beyond Cost and Regimen Complexity. Am. J. Geriatr. Pharmacother. 9 (1), 11–23. doi:10.1016/j.amjopharm.2011.02.004
Gossell-Williams, M., Davis, A., Aiken, W., and Mayhew, R. (2008). Herbal Preparation Use Among Patients with Benign Prostatic Hyperplasia Attending a Urology Clinic in Jamaica, West Indies. West. Indian Med. J. 57 (1), 75–76.
Gossell-Williams, M., Williams-Johnson, J., Williams, E. W., and Levy, P. (2014). A Case for a Holistic Approach to the Improvement of Compliance Among Hypertensive Patients: A Hospital Review. West. Indian Med. J. 63 (3), 271–273. doi:10.7727/wimj.2013.156
Hartzler, M., Chen, A. H. M., Murphy, B. L., and Rodewald, S. J. (2014). Evaluation of Jamaican Knowledge of Diabetes and Health Beliefs. Cjgh 1 (2), 19–28. doi:10.15566/cjgh.v1i2.13
Hope, M. O., Taggart, T., Galbraith-Gyan, K. V., and Nyhan, K. (2020). Black Caribbean Emerging Adults: A Systematic Review of Religion and Health. J. Relig Health 59 (1), 431–451. doi:10.1007/s10943-019-00932-5
Hordern, J. (2016). Religion and Culture. Medicine (Abingdon) 44 (10), 589–592. doi:10.1016/j.mpmed.2016.07.011
Ibrahim, H., Abdo, A., El Kerdawy, A. M., and Eldin, A. S. (2021). Signal Detection in Pharmacovigilance: A Review of Informatics-Driven Approaches for the Discovery of Drug-Drug Interaction Signals in Different Data Sources. Artif. Intelligence Life Sci. 1, 100005. doi:10.1016/j.ailsci.2021.100005
Leporini, C., De Sarro, G., and Russo, E. (2014). Adherence to Therapy and Adverse Drug Reactions: Is There a Link? Expert Opin. Drug Saf. 13 (Suppl. 1), S41–S55. doi:10.1517/14740338.2014.947260
Macionis, J. J. (2015). “Sociology,” in Global Edition, 15th edn. Harlow, England: Pearson Education Limited.
Mitchell, M. F. (1983). Popular Medical Concepts in Jamaica and Their Impact on Drug Use. West. J. Med. 139 (6), 841–847.
Mitchell-Fearon, K., Willie-Tyndale, D., Waldron, N., Holder-Nevins, D., James, K., Laws, H., et al. (2015). Cardio-Vascular Disease and Cancer: A Dichotomy in Utilization of Clinical Preventive Services by Older Adults in a Developing Country. Gerontol. Geriatr. Med. 1 (1), 2333721415611821. doi:10.1177/2333721415611821
Mowatt, L. (2013). Diabetic Retinopathy and its Risk Factors at the University Hospital in Jamaica. Middle East. Afr. J. Ophthalmol. 20 (4), 321–326. doi:10.4103/0974-9233.120017
Myfanwy, M., and Watkins, C. J. (1988). Hypertension : Beliefs and Responses to Medication Among Cultural Groups. Sociol. Health Illn 10 (4), 561–578. doi:10.1111/1467-9566.ep10837256
Niriayo, Y. L., Kumela, K., Kassa, T. D., and Angamo, M. T. (2018). Drug Therapy Problems and Contributing Factors in the Management of Heart Failure Patients in Jimma University Specialized Hospital, Southwest Ethiopia. PLoS One 13 (10), e0206120. doi:10.1371/journal.pone.0206120
Nunn, N. (2012). Culture and the Historical Process. Econ. Hist. Developing Regions 27 (Suppl. 1), S108–S126. doi:10.1080/20780389.2012.664864
Oates, G. R., Juarez, L. D., Hansen, B., Kiefe, C. I., and Shikany, J. M. (2020). Social Risk Factors for Medication Nonadherence: Findings from the CARDIA Study. Am. J. Health Behav. 44 (2), 232–243. doi:10.5993/AJHB.44.2.10
Owusu, S., Gaye, Y. E., Hall, S., Junkins, A., Sohail, M., Franklin, S., et al. (2020). Factors Associated with the Use of Complementary and Alternative Therapies Among Patients with Hypertension and Type 2 Diabetes Mellitus in Western Jamaica: a Cross-Sectional Study. BMC Complement. Med. Ther. 20 (1), 314. doi:10.1186/s12906-020-03109-w
Park, Y., Park, Y.-H., and Park, K.-S. (2020). Determinants of Non-adherences to Long-Term Medical Therapy after Myocardial Infarction: a Cross-Sectional Study. Ijerph 17 (10), 3585. doi:10.3390/ijerph17103585
Payne-Jackson, A., and Alleyne, M. C. (2004). Jamaican Folk Medicine: A Source of Healing. Mona, Jamaica: University of West Indies Press.
Picking, D., Younger, N., Mitchell, S., and Delgoda, R. (2011). The Prevalence of Herbal Medicine Home Use and Concomitant Use with Pharmaceutical Medicines in Jamaica. J. Ethnopharmacol 137 (1), 305–311. doi:10.1016/j.jep.2011.05.025
Picking, D., Delgoda, R., and Vandebroek, I. (2019). Traditional Knowledge Systems and the Role of Traditional Medicine in Jamaica. CAB Rev. 14 (45). doi:10.1079/PAVSNNR201914045
Pusey-Murray, A. E., Bourne, P. A., Warren, S., LaGrenade, J., and Charles, C. A. D. (2010). Medication Compliance Among Mentally Ill Patients in Public Clinics in Kingston and St. Andrew, Jamaica. JBiSE 03 (06), 602–611. doi:10.4236/jbise.2010.36082
Ralph Edwards, I. (2017). Causality Assessment in Pharmacovigilance: Still a challenge. Drug Saf. 40 (5), 365–372. doi:10.1007/s40264-017-0509-2
Raza, S., Iqbal, Q., Haider, S., Khalid, A., Hassali, M. A., and Saleem, F. (2020). Beliefs about Medicines Among Type 2 Diabetes Mellitus Patients in Quetta City, Pakistan: a Cross-Sectional Assessment. J. Public Health (Berl.) 28 (3), 277–283. doi:10.1007/s10389-019-01046-8
Rose, A. M., Hambleton, I. R., Jeyaseelan, S. M., Howitt, C., Harewood, R., Campbell, J., et al. (2016). Establishing National Noncommunicable Disease Surveillance in a Developing Country: a Model for Small Island Nations. Rev. Panam Salud Publica 39, 76–85.
Rumun, A. J. (2014). Influence of Religious Beliefs on Healthcare Practice. Int. J. Educ. Res. 2 (4), 37–48.
Sabaté, E. (2003). Adherence to Long-Term Therapies: Evidence for Action. World Health Organization, Technical Report. Available at: http://whqlibdoc.who.int/publications/2003/9241545992.pdf.
Seaga, E. (2005). The Folk Roots of Jamaican Cultural Identity. Caribbean Q. 51 (2), 79–95. doi:10.1080/00086495.2005.11672268
Shahin, W., Kennedy, G. A., and Stupans, I. (2019). The Impact of Personal and Cultural Beliefs on Medication Adherence of Patients with Chronic Illnesses: a Systematic Review. Patient Prefer Adherence 13, 1019–1035. doi:10.2147/PPA.S212046
Simon, T. A., Khouri, M. S., Kou, T. D., and Gomez-Caminero, A. (2020). Realizing the Potential of the Patient Perspective. Patient Prefer Adherence 14, 2001–2007. doi:10.2147/PPA.S257355
Smith, C. A. (2012). Living with Sugar: Influence of Cultural Beliefs on Type 2 Diabetes Self-Management of English-speaking Afro-Caribbean Women. J. Immigr Minor. Health 14 (4), 640–647. doi:10.1007/s10903-011-9513-2
Streefland, M. B. (2018). Why Are We Still Creating Individual Case Safety Reports? Clin. Ther. 40 (12), 1973–1980. doi:10.1016/j.clinthera.2018.10.012
Street, R. L., and Haidet, P. (2011). How Well Do Doctors Know Their Patients? Factors Affecting Physician Understanding of Patients' Health Beliefs. J. Gen. Intern. Med. 26 (1), 21–27. doi:10.1007/s11606-010-1453-3
Sutherland, P., Moodley, R., Chevannes, B., and Chevannes, P. (2014). Caribbean Healing Traditions. London: Routledge. Chapter 12.
Świątoniowska-Lonc, N., Polański, J., Mazur, G., and Jankowska-Polańska, B. (2021). Impact of Beliefs about Medicines on the Level of Intentional Non-adherence to the Recommendations of Elderly Patients with Hypertension. Int. J. Environ. Res. Public Health 18 (6), 2825. doi:10.3390/ijerph18062825
Swihart, D. L., Yarrarapu, S. N. S., and Martin, R. L. (20182021). “Cultural Religious Competence in Clinical Practice,” in StatPearls (Treasure Island (FL): StatPearls Publishing).
Vrijens, B., De Geest, S., Hughes, D. A., Przemyslaw, K., Demonceau, J., Ruppar, T., et al. (2012). A New Taxonomy for Describing and Defining Adherence to Medications. Br. J. Clin. Pharmacol. 73, 691–705. doi:10.1111/j.1365-2125.2012.04167.x
Watson, S. M., and Ferrillo, H. (2021). Effectiveness of Short-Term Medical Missions on Chronic Disease in Underserved Communities. West. J. Nurs. Res. 43 (4), 323–329. doi:10.1177/0193945920944809
Welsh, F. E., Duff, E. M., Campbell-Taffe, K., and Lindo, J. L. (2015). Lifestyles of Jamaican Men with Hypertension. J. Transcult Nurs. 26 (5), 507–513. doi:10.1177/1043659614531794
Wilks, R. J., Sargeant, L. A., Gulliford, M. C., Reid, M. E., and Forrester, T. E. (2001). Management of Diabetes Mellitus in Three Settings in Jamaica. Rev. Panam Salud Publica 9, 65–72. doi:10.1590/s1020-49892001000200002
Keywords: adherence, pharmacotherapy beliefs, cultural, religious, pharmacovigilance
Citation: Brown R, Bateman CJ and Gossell-Williams M (2022) Influence of Jamaican Cultural and Religious Beliefs on Adherence to Pharmacotherapy for Non-Communicable Diseases: A Pharmacovigilance Perspective. Front. Pharmacol. 13:858947. doi: 10.3389/fphar.2022.858947
Received: 20 January 2022; Accepted: 25 February 2022;
Published: 14 March 2022.
Edited by:
Joseph O. Fadare, Ekiti State University, NigeriaReviewed by:
Kwame Ohene Buabeng, Kwame Nkrumah University of Science and Technology, GhanaCopyright © 2022 Brown, Bateman and Gossell-Williams. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maxine Gossell-Williams, TWF4aW5lLmdvc3NlbGxAdXdpbW9uYS5lZHUuam0=