 Peiying Huang1
Peiying Huang1 Zhishang Li2Li Chen2Jing Zeng2Shuai Zhao2Yong Tang3Bixuan Huang4
Zhishang Li2Li Chen2Jing Zeng2Shuai Zhao2Yong Tang3Bixuan Huang4 Hansu Guan3Yan Chen2Yuchao Feng5
Hansu Guan3Yan Chen2Yuchao Feng5 Sisi Lei1Qihua Wu1Haobo Zhang1Xiaoyan Huang2Linsheng Zeng6Yuxiang Liu6Zhongyi Zeng6Bojun Chen1,2,5*
Sisi Lei1Qihua Wu1Haobo Zhang1Xiaoyan Huang2Linsheng Zeng6Yuxiang Liu6Zhongyi Zeng6Bojun Chen1,2,5*- 1The Second Clinical Medical School of Guangzhou University of Chinese Medicine, Guangzhou, China
- 2Emergency Department of Guangdong Provincial Hospital of Traditional Chinese Medicine, Guangzhou, China
- 3The Third Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, China
- 4Department of Nursing, Hubei University of Arts and Science, Xiangyang, China
- 5Guangdong Provincial Key Laboratory of Research on Emergency in Traditional Chinese Medicine, Clinical Research Team of Prevention and Treatment of Cardiac Emergencies with Traditional Chinese Medicine, Guangzhou, China
- 6Shenzhen Traditional Chinese Medicine Hospital, Shenzhen, China
Background: Stable angina is a common condition with high morbidity and mortality rates. It has been reported that combining oral Chinese patent medicines (OCPMs) and Western medicine (WM) could potentially achieve a better effect than WM alone. However, the optimal OCPMs for stable angina remain controversial and merit further empirical research.
Methods: PubMed, Embase, Web of Science, Cochrane Library, Ovid-Medline, Clinical Trials.gov, China National Knowledge Infrastructure, Wanfang Database, Weipu Journal Database, and Chinese Biomedical Literature Database were all searched from inception to 13 March 2022. We employed Version 2 of the Cochrane risk-of-bias tool (ROB2) to assess the overall quality of the selected studies. We also used R 4.1.2 and STATA 14.0 software applications to perform network meta-analysis, followed by sensitivity and subgroup analysis.
Results: A total of 179 randomized controlled trials with 16,789 patients were included. The selected trials were all assessed as some concerns. OCPMs combined with WM had a better treatment effect than WM alone. In terms of the effective clinical rate, a significant increase was detected for Qishen Yiqi dripping pill (QSYQ)+WM as compared with Shensong Yangxin capsule (SSYX)+WM, Shexiang Baoxin pill (SXBX)+WM, Tongxinluo capsule (TXL)+WM, Xuefu Zhuyu capsule (XFZY)+WM, Qiliqiangxin capsule (QLQX)+WM, Naoxintong capsule (NXT)+WM, Fufang Danshen dripping pill (FFDS)+WM, and Danlou tablet (DL)+WM. QSYQ + WM had the highest-ranking probability (98.12%). Regarding the effective rate in ECG, QSYQ + WM was superior to SXBX + WM, TXL + WM, DL + WM, FFDS + WM, and NXT + WM. QSYQ + WM ranked first (94.21%). In terms of weekly frequency of angina, QLQX + WM obtained a better effect than FFDS + WM, Kuanxiong aerosol (KXQW)+WM, NXT + WM, QLQX + WM, SSYX + WM, SXBX + WM, and TXL + WM. QLQX + WM ranked first (100.00%). Regarding the duration of an angina attack, KXQW + WM was superior to SSYX + WM; KXQW + WM ranked first (95.71%). Adverting to weekly nitroglycerin usage, TXL + WM had the highest-ranking probability (82.12%). Referring to cardiovascular event rate, DL + WM had the highest effect (73.94%). Additionally, SSYX + WM had the lowest rate of adverse drug reactions (1.14%).
Conclusion: OCPMs combined with WM had a higher efficacy. QSYQ + WM, QLQX + WM, KXQW + WM, TXL + WM, DL + WM, SSYX + WM, and SXBX + WM merit further investigation. SXBX + WM is presumably the optimal treatment prescription for both clinically effective and cardiovascular event rates. Further high-quality empirical research is needed to confirm the current results.
Systematic Review Registration: URL = https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=316534, CRD 42022316534
1 Introduction
Coronary artery disease, the leading cause of death worldwide, has affected 423 million people on a global scale, causing an estimated 31% of deaths (17.8 million) per year (Roth et al., 2017; Mensah et al., 2019). As a common manifestation of coronary heart disease, stable angina is conventionally defined as episodic discomfort in the anterior chest area (chest pain or tightness), lasting less than 10 min, typically being provoked by physical exertion or mental stimulation, and being relieved by rest or with nitroglycerin (Ohman, 2016). This disease suggests a certain degree of stenosis in a patient’s coronary arteries, resulting in a relative lack of blood supply to the heart when cardiac oxygen demand increases (Fihn et al., 2012; Montalescot et al., 2013; Joshi and De Lemos, 2021). Research suggests that stable angina might double the risk of major cardiovascular events (Jones et al., 2006; Bhatt et al., 2010).
The treatment of patients with stable angina currently primarily focuses on education for patients (e.g., smoking cessation and moderate exercise) and oral administration of Western medicine (WM) to control symptoms of discomfort, reduce the probability of adverse cardiovascular events, and improve the overall quality of life (Joshi and De Lemos, 2021). Percutaneous coronary intervention is not routinely applied to stable angina, primarily due to the growing evidence showing that it is not associated with any reduction in myocardial infarction and mortality rates for most patients (Boden et al., 2007; Joshi and De Lemos, 2021).
Apart from the treatment methods mentioned previously, Chinese clinicians choose oral Chinese patent medicines (OCPMs) for stable angina based on WM implementation. Some studies showed that OCPMs relieved symptoms and improved prognoses in some target populations, such as the reduction in the duration of angina attack and a decrease in the probability of acute coronary syndrome (Mao et al., 2013; Mao et al., 2021). However, there is a great variety of OCPMs for the treatment of stable angina, and it remains controversial which OCPM has the optimal effect on stable angina.
As an extension of conventional pairwise meta-analysis, network meta-analysis enables the comparison between two or more interventions by integrating a direct comparison between various interventions, as well as an indirect comparison and further implementation ranking among the interventions (Caldwell et al., 2005; Li et al., 2011; Mills et al., 2012). In light of this, we used a network meta-analysis to compare the OCPMs recommended in a Chinese guideline for the treatment of stable angina (Mao et al., 2021) to determine the difference between them and provide some suggestions for clinical medication. The profile of the current study is summarized in Figure 1.
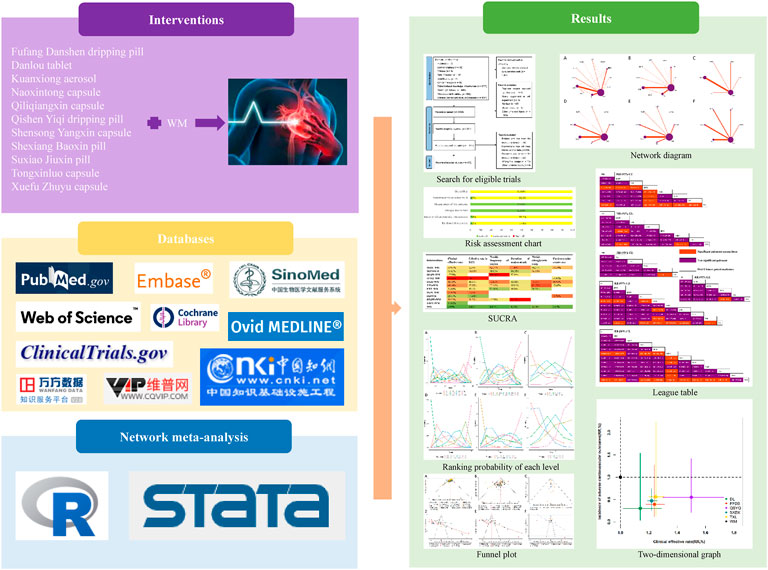
FIGURE 1. Graphical abstract of the network meta-analysis. WM, Western medicine.
2 Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Extension Statement to perform this network meta-analysis, with a PRISMA checklist detailed in Supplementary Material S1.
2.1 Search strategy
In this study, we searched nine academic databases for published research, including five English databases: PubMed, Embase, Web of Science, Cochrane Library, and Ovid-Medline; as well as four Chinese databases: China National Knowledge Infrastructure, Wanfang Database, Weipu Journal Database, and Chinese Biomedical Literature Database. Additionally, we also retrieved unpublished studies through Clinical Trials.gov. The database retrieval time was set from inception to 13 March 2022. The search strategies employed are detailed in Supplementary Material S2.
2.2 Inclusion and exclusion criteria
1) Patients with a definitive diagnosis of stable angina according to predefined guidelines were considered in this study (relying on angina symptoms and auxiliary examinations). It is worth noting that patients with other heart diseases such as arrhythmia or heart failure or with serious underlying diseases, for example, chronic obstructive pulmonary disease, advanced tumor, or shock, were beyond the scope of our study.
2) Patients in the experimental group were treated with one type of OCPM and WM without other traditional Chinese medicine treatments, such as the implementation of traditional Chinese medicine injections, oral traditional Chinese medicine decoction, acupuncture, or massage. Notably, the OCPMs must be within the 12 OCPMs recommended by the Chinese guideline (Mao et al., 2021).
3) Patients in comparison were a control group treated with WM alone or another experimental group treated with another type of OCPM and WM. WM treatment mainly included secondary coronary heart disease prevention, namely, ABCDE protocol for coronary heart disease (Dancy et al., 2018).
4) Outcomes of the selected studies included one or more of the following:
Primary outcomes:
1) Clinical effective rate (percentage of patients whose conditions improved after treatment).
2) Cardiovascular events rate (acute coronary syndrome, heart failure, and cardiac death).
Secondary outcomes:
1) Effective rate in electrocardiograph (ECG) (Percentage of patients with improved myocardial ischemia according to ECG after treatment, e.g., ST segment improved from depression, or T wave changes from inversion to normal).
2) Weekly frequency of angina.
3) Duration of an angina attack.
4) Weekly nitroglycerin usage.
5) Adverse drug reactions (ADRs).
5) We searched for only randomized controlled trials (RCTs) for inclusion in this network meta-analysis. Randomized crossover trials were excluded if the first phase’s results were unavailable.
2.3 Data collection
After software and manual removal of any duplicate studies, two investigators screened the remaining studies according to the pre-designed inclusion and exclusion criteria. They then extracted the following data from the final selected studies independently:
1) Trials information: trial title, study site, publication year, and author(s).
2) Population: sample size within each intervention group, sex ratio, age, and between-group comparison of patients’ baseline characteristics primarily for gender, age, underlying disease, and length of illness.
3) Intervention: treatment modalities and treatment courses for each trial.
4) Outcomes: details of the seven aforementioned outcomes.
5) Study design: randomized approach, allocation concealment, and blinding.
6) Additional information: pharmaceutical company sponsorship.
2.4 Quality assessment
Two investigators independently assessed the risk of bias of the selected RCTs according to Version 2 of the Cochrane risk-of-bias tool for randomized trials (RoB 2) in five entries: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported results (Sterne et al., 2019). All entries were rated as “low risk”, “high risk”, or “some concerns”, in which a trial was rated as “low risk” overall only if all the entries were assessed as “low risk”. Any disagreements were resolved by discussion first or, if necessary, by arbitration by a third investigator to reach a final consensus.
2.5 Data analysis
Direct and indirect comparisons of all interventions were integrated via a random-effects network meta-analysis within a Bayesian framework based on 200,000 iterations and 10,000 annealings (Salanti, 2012). A contribution plot was generated to present the contribution of every direct comparison and indirect comparison to the mixed effect. Continuous variables were integrated as Mean Differences (MD) with a 95% confidence interval (CI), while categorical variables were as Risk Ratio (RR) with 95% CI. A league table was generated to summarize the comparison among interventions included in each corresponding outcome. According to the pooled effect size, each intervention obtained a probability of each level and, through a “sucra” code, summarized these probabilities to obtain a total ranking probability of surface under the cumulative ranking curve (SUCRA) (Dias et al., 2013). Furthermore, two different outcomes were integrated by 2D coordinates to assess their comparison among different interventions after integration.
A design-by-treatment approach was performed to detect the global inconsistency, while a node-splitting method was applied to assess the local inconsistency of the model (Higgins et al., 2012; van Valkenhoef et al., 2016). In addition, global I2-statistic and predictive interval plots were employed to assess the extent of heterogeneity. A higher value of I2 suggests a greater degree of heterogeneity (Higgins and Thompson, 2002).
Sensitivity analysis of network meta-analysis was implemented by excluding studies published before 2010 to validate the robustness of the results. A subgroup network meta-analysis incorporated age group, sample size, and treatment course. Additionally, a comparison-adjusted funnel plot detected potential publication bias in the outcome with greater than or equal to 10 selected studies.
For data analysis, we applied R 4.1.2 (network meta-analysis, global heterogeneity, subgroup analysis, sensitivity analysis, probability rankings graph, and two-dimensional graph) and STATA 14.0 (network plot, inconsistency, predictive interval plot, contribution plot, and funnel plot).
3 Results
3.1 Literature retrieval and study characteristics
A total of 4,153 records were retrieved in this study. After removing 2,082 duplicates, the remaining 2,071 records were screened according to the pre-established criteria, from which 1,720 studies were deleted by abstract reading and 172 by full-text reading. Finally, 179 published RCTs with 16,789 patients (9,620 reported male patients; 57.30%) were included in the current analysis, involving 177 two-arm trials and two three-arm trials (see Supplementary Material S3 for citations of the selected studies). A flow chart of the literature screening process is presented in Supplementary Material S4. Overall, 11 OCPMs were included in our study, involving Fufang Danshen dripping pill (FFDS, 30 RCTs), Danlou tablet (DL, 5 RCTs), Kuanxiong aerosol (KXQW, 1 RCT), Naoxintong capsule (NXT, 10 RCTs), Qiliqiangxin capsule (QLQX, 3 RCTs), Qishen Yiqi dripping pill (QSYQ, 4 RCTs), Shensong Yangxin capsule (SSYX, 15 RCTs), Shexiang Baoxin pill (SXBX, 67 RCTs), Suxiao Jiuxin pill (SXJX, 6 RCTs), Tongxinluo capsule (TXL, 47 RCTs), and Xuefu Zhuyu capsule (XFZY, 2 RCTs) (see Supplementary Material S5 for details of the included OCPMs). Among the 179 selected RCTs, 159 RCTs, 89 RCTs, 11 RCTs, 38 RCTs, 29 RCTs, 12 RCTs, and 90 RCTs contributed to the effective clinical rate, effective rate in ECG, weekly frequency of angina, duration of an angina attack, weekly nitroglycerin usage, cardiovascular events rate, and ADRs, respectively. Baseline data were balanced between groups in all the included studies, with the course of treatment ranging from two to 144 weeks. Characteristics of the included studies are summarized in Supplementary Material S6. Meanwhile, a network graph visualized the relationship between different interventions in each outcome, in which the node sizes indicate the total sample sizes for treatment. Conversely, the width of the connecting line between each node represents the number of the included studies. The network graph is depicted in Figure 2.
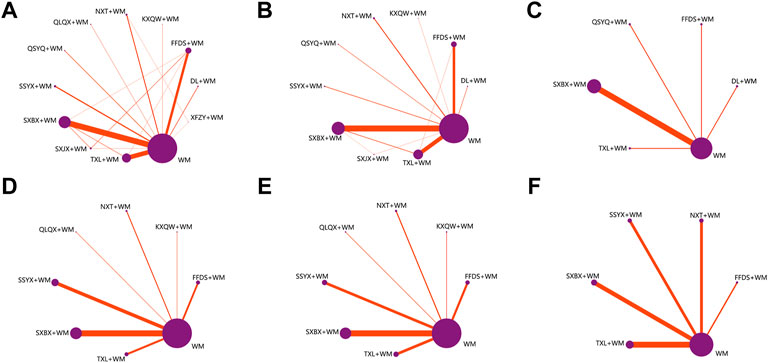
FIGURE 2. Network graph for different outcomes (A) Clinical effective rate; (B) Effective rate in ECG; (C) Cardiovascular events rate; (D) Weekly frequency of angina; (E) Duration of an angina attack; (F) Weekly nitroglycerin usage; WM, Western medicine; FFDS, Fufang Danshen dripping pill; DL, Danlou tablet; KXQW, Kuanxiong aerosol; NXT, Naoxintong capsule; QLQX, Qiliqiangxin capsule; QSYQ, Qishen Yiqi dripping pill; SSYX, Shensong Yangxin capsule; SXBX, Shexiang Baoxin pill; SXJX, Suxiao Jiuxin pill; TXL, Tongxinluo capsule; XFZY, Xuefu Zhuyu capsule.
3.2 Risk-of-bias assessment
Of the selected RCTs, 53 trials reported specific randomization methods, including 48 trials using simple random number tables, three trials performing central randomization, one RCT implementing block randomization, and one RCT using stratified randomization. Four studies reported allocation concealment, which was rated “low risk” in the “randomization process” (2.2%). Seven studies reported blinding, including two trials of single-blind methods and five trials of double-blind methods. In contrast, only five of them might use appropriate analytical methods for the results and be thus considered as “low risk” in “deviation from intended interventions” (2.8%). Although some trials had a minority of patients lost to follow-ups, all the included trials reported the number of participants in outcome assessment, causing a minor effect on outcomes assessment. Therefore, all the included trials were rated as “low risk” in “missing outcomes data” (100%). In addition, the selected studies were all rated as “low risk” in the “measurement of the outcome” primarily due to the objectivity of outcome measurement to investigators (100%). Three studies conducted experiments according to their pre-designed protocols and were considered “low risk” in the “selection of the reported result” (1.7%). Overall, the trials included in this network meta-analysis were rated as “some concerns”. Supplementary Material S7 summarizes the quality of the assessment of the trials.
3.3 Network meta-analysis
The contribution plots of this network meta-analysis suggested that SXBX + WM vs. WM had the greatest contribution for effective clinical rate, effective rate in ECG, weekly frequency of angina, duration of an angina attack, and cardiovascular events rate, with 32.52%, 37.08%, 39.47%, 37.93%, and 63.64%, respectively. Additionally, TXL + WM vs. WM contributed the most to weekly nitroglycerin usage (33.33%). The contribution plots are provided in Supplementary Material S8.
3.4 Primary outcomes
3.4.1 Effective clinical rate
Twelve treatment nodes were compared in effective clinical rate, including DL + WM, FFDS + WM, KXQW + WM, NXT + WM, QLQX + WM, QSYQ + WM, SSYX + WM, SXBX + WM, SXJX + WM, TXL + WM, XFZY + WM, and WM. We found that all the included OCPMs plus WM, apart from KXQW + WM and XFZY + WM, had a higher clinical effectiveness rate than WM alone. Additionally, QSYQ + WM improved its clinical effectiveness rate compared with SSYX + WM, SXBX + WM, TXL + WM, XFZY + WM, QLQX + WM, NXT + WM, FFDS + WM, and DL + WM. The comparison between each intervention is depicted in Figure 3E. Based on the ranking probability of each level and SUCRA, QSYQ + WM had the highest effective rate (98.12%), followed by SXJX + WM (71.04%) and TXL + WM (68.40%), whereas WM alone obtained the worst effect (3.09%). The ranking probability is presented in Figure 4A and Table 1.
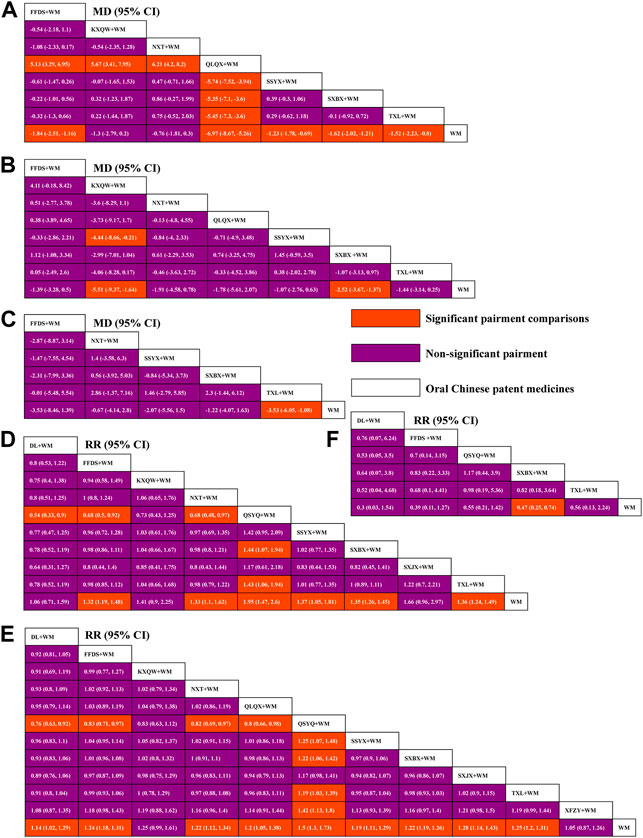
FIGURE 3. League tables for comparison between each intervention. (A) Weekly frequency of angina; (B) Duration of an angina attack; (C) Weekly nitroglycerin usage; (D) Effective rate in ECG; (E) Clinical effective rate; (F) Cardiovascular events rate; WM, Western medicine; FFDS, Fufang Danshen dripping pill; DL, Danlou tablet; KXQW, Kuanxiong aerosol; NXT, Naoxintong capsule; QLQX, Qiliqiangxin capsule; QSYQ, Qishen Yiqi dripping pill; SSYX, Shensong Yangxin capsule; SXBX, Shexiang Baoxin pill; SXJX, Suxiao Jiuxin pill; TXL, Tongxinluo capsule; XFZY, Xuefu Zhuyu capsule.
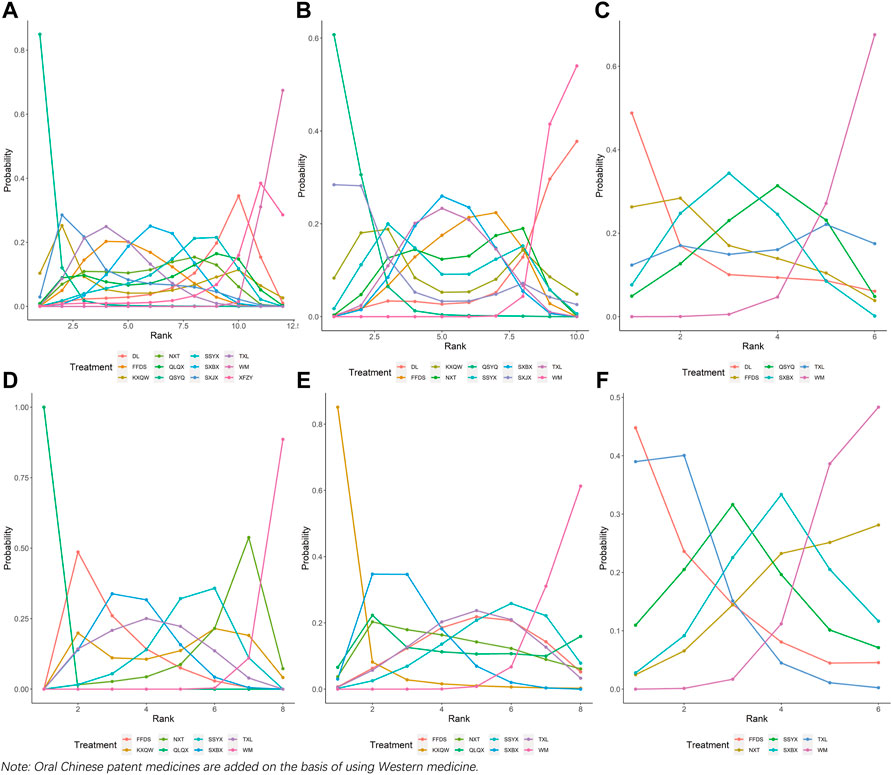
FIGURE 4. Ranking probability at each level for the included interventions. (A) Weekly frequency of angina; (B) Duration of an angina attack; (C) Weekly nitroglycerin usage; (D) Effective rate in ECG; (E) Clinical effective rate; (F) Cardiovascular events rate; WM, Western medicine; FFDS, Fufang Danshen dripping pill; DL, Danlou tablet; KXQW, Kuanxiong aerosol; NXT, Naoxintong capsule; QLQX, Qiliqiangxin capsule; QSYQ, Qishen Yiqi dripping pill; SSYX, Shensong Yangxin capsule; SXBX, Shexiang Baoxin pill; SXJX, Suxiao Jiuxin pill; TXL, Tongxinluo capsule; XFZY, Xuefu Zhuyu capsule.
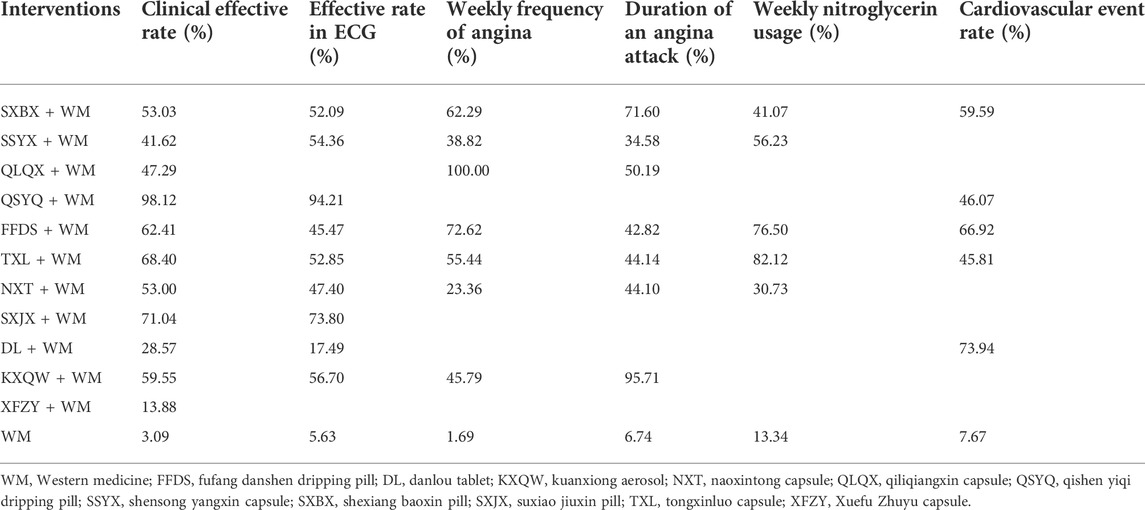
TABLE 1. Ranking probabilities of surface under the cumulative ranking area curves (SUCRA) for the outcomes.
3.4.2 Cardiovascular event rate
Six interventions were involved in evaluating cardiovascular events rate, including DL + WM, FFDS + WM, QSYQ + WM, SXBX + WM, TXL + WM, and WM alone. The decrease in cardiovascular events rate was statistically significant for SXBX + WM as compared with WM alone, while no significant association was found within other interventions. The comparison between each intervention is revealed in Figure 3F. Based on the ranking probability of each level and SUCRA, DL + WM had the highest effect (73.94%), followed by FFDS + WM (66.92%) and SXBX + WM (59.59%), whereas WM alone obtained the worst effect (7.67%). The ranking probability is demonstrated in Figure 4C and Table 1.
3.5 Secondary outcome
3.5.1 Effective rate in ECG
Ten treatment options were compared in this network geometry, including DL + WM, FFDS + WM, KXQW + WM, NXT + WM, QSYQ + WM, SSYX + WM, SXBX + WM, SXJX + WM, TXL + WM, and WM. Apart from DL + WM, KXQW + WM, and SXJX + WM, an improvement effect of effective rate in ECG was detected for all of the included OCPMs plus WM as compared with WM alone. QSYQ + WM obtained a better effect than SXBX + WM, TXL + WM, DL + WM, FFDS + WM, and NXT + WM. The comparison between each intervention is depicted in Figure 3D. Based on the ranking probability of each level and SUCRA, QSYQ + WM had the highest effective rate (94.21%), followed by SXJX + WM (73.80%) and KXQW + WM (56.70%), whereas WM alone obtained the worst effect (5.63%). The ranking probability is presented in Figure 4B; Table 1.
3.6 Weekly frequency of angina
Eight interventions were involved in the evaluation of the weekly frequency of angina, including FFDS + WM, KXQW + WM, NXT + WM, QLQX + WM, SSYX + WM, SXBX + WM, TXL + WM, and WM. Apart from KXQW + WM and NXT + WM, the remaining OCPMs plus WM earned a better effect of decreasing weekly angina frequency than WM alone. In addition, QLQX + WM statistically reduced the weekly frequency of angina as compared with other included OCPMs plus WM. The comparison between each intervention is revealed in Figure 3A. According to the ranking probability of each level and SUCRA, QLQX + WM had the highest effective rate in reducing the weekly frequency of angina (100.00%), followed by FFDS + WM (72.62%) and SXBX + WM (62.29%). In contrast, WM alone obtained the worst effect (1.69%). The ranking probability is presented in Figure 4D; Table 1.
3.7 Duration of an angina attack
There were eight separate treatment nodes in the network geometry for the duration of the angina attack, including FFDS + WM, KXQW + WM, NXT + WM, QLQX + WM, SSYX + WM, SXBX + WM, TXL + WM, and WM. KXQW + WM and SXBX + WM revealed a higher effect in shortening angina attack duration than WM; meanwhile, KXQW + WM was superior to SSYX + WM. The between-intervention differences were demonstrated in Figure 3B. According to the ranking probability of each level and SUCRA, KXQW + WM ranked first (95.71%), followed by SXBX + WM (71.60%) and QLQX + WM (50.19%), whereas WM alone obtained the worst effect (6.74%). The ranking probability is demonstrated in Figure 4E; Table 1.
3.8 Weekly nitroglycerin usage
Eight interventions (FFDS + WM, NXT + WM, SSYX + WM, SXBX + WM, TXL + WM, and WM) were involved in the evaluation of weekly nitroglycerin usage. TXL + WM was superior for WM alone in reducing weekly nitroglycerin usage. No significant association was found among other interventions. The comparison between each intervention is displayed in Figure 3C. According to the ranking probability of each level and SUCRA, TXL + WM had the highest SUCRA value (82.12%), followed by FFDS + WM (76.50%) and SSYX + WM (56.23%), whereas WM alone obtained the worst effect (13.34%). The ranking probability is demonstrated in Figure 4F; Table 1.
3.9 Adverse drug reactions
In the current study, network meta-analysis was impossible for ADRs as most studies reported negative results (0% in incidence). Of 4,514 patients observed, 250 occurred with ADRs (5.54%), involving 96 with mild abdominal discomfort, 91 with dizziness/headache, 11 with numbness of tongue and lips, 24 with rash, and 28 with mild chest discomfort, whereas had no serious ADRs. Among 1,951 SXBX + WM-treated patients, the incidences of mild abdominal discomfort, dizziness/headache, numbness of tongue and lips, rash, and mild chest discomfort, were 2.67%, 2.41%, 0.56%, 0.56%, and 0.67%, respectively, with the total adverse reaction rate of 6.87%. In 81 patients treated with SXJX + WM, the incidences of mild abdominal discomfort, dizziness/headache, rash, and mild chest discomfort, were 2.47%, 17.28%, 7.41%, and 8.64%, separately, with a total adverse reaction rate of 35.80%. The incidence of ADRs in FFDS + WM groups (616 patients) was 7.79%, in which 2.11% of mild abdominal discomfort, 3.25% of dizziness/headache, 1.14% of rash, and 1.30% of mild chest discomfort. DL + WM groups (54 patients) had an incidence of ADRs of 1.85%, in which only one patient occurred with mild abdominal discomfort. 188 patients treated with NXT + WM had an ADRs incidence of 1.60%, including 1.06% mild abdominal discomfort and 0.53% dizziness/headache. There was a 4.12% incidence of ADRs in 97 patients treated with QLQX + WM, including 3.09% mild abdominal discomfort and 1.03% dizziness/headache. Four of 350 patients treated with SSYX + WM reported mild abdominal discomfort, contributing to 1.14% of the incidence of ADRs. Among 832 TXL + WM-treated patients, the incidences of mild abdominal discomfort and dizziness/headache were 2.28% and 0.96%, individually, with a total adverse reaction rate of 3.25%. Additionally, no ADRs occurred in 55 patients treated with KXQW + WM and 190 patients treated with QSYQ + WM. The ADRs are detailed in Supplementary Material S9.
3.10 Integrated outcome
OCPMs + WM shared in effective clinical rate, and cardiovascular events rate were integrated into a two-dimensional graph with WM as the comparison. As depicted in Figure 5, the RR of each intervention was demonstrated as a center point while 95% CI was presented as the length of the horizontal and vertical lines. In the current analysis, only SXBX + WM had no vertical and horizontal lines intersecting the futility line, indicating that it may be the best intervention for the combined outcome.
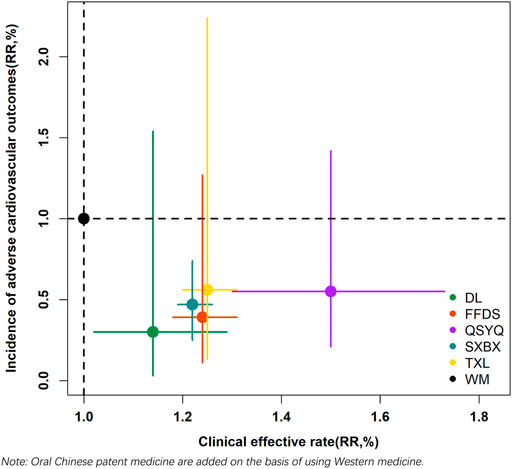
FIGURE 5. Two-dimensional graph. WM, Western medicine; FFDS, Fufang Danshen dripping pill; DL, Danlou tablet; QSYQ, Qishen Yiqi dripping pill; SXBX, Shexiang Baoxin pill; TXL, Tongxinluo capsule.
3.11 Inconsistency, heterogeneity, and publication bias
Inconsistency can only be detected within outcomes, with treatment nodes forming one or more loops; we detected an inconsistency in effective clinical rate and effective rate in ECG. The results of global inconsistency did not indicate any significant difference for each of the two outcomes (p = 0.077 and p = 0.081 for effective clinical rate and effective rate in ECG, respectively). The detection of the node-splitting model suggested that only three comparisons for effective clinical rate and two for effective rate in ECG presented significant differences between direct and indirect comparisons. The results of inconsistency detection are shown in Supplementary Material S10. Global I2-statistic were revealed as 0%, 0.4%, 98.15%, 99.67%, 99.51%, and 0% for effective clinical rate, effective rate in ECG, weekly frequency of angina, duration of an angina attack, weekly nitroglycerin usage, and cardiovascular events rate, individually. The results of predictive interval plots suggested that 10.61%, 17.78%, 14.29, 10.71%, 6.67%, and 6.67% of the comparisons of effective clinical rate, effective rate in ECG, weekly frequency of angina, duration of an angina attack, weekly nitroglycerin usage, and cardiovascular events rate, separately, were significantly affected by the estimated heterogeneity. The predictive interval plots are detailed in Supplementary Material S11. As depicted in Supplementary Material S12, all the fitted straight lines’ slopes are close to the centerline, and the points on both sides of the centerline are relatively symmetric, indicating that there was no obvious publication bias for all the outcomes.
3.12 Sensitivity analyses and subgroup analyses
Sensitivity analyses, the network meta-analyses being performed among studies published in 2010 and beyond/studies that do not include OCPMs with selected RCTs less than 3, i.e., KXQW + WM and XFZY + WM, confirmed the more-effective benefit of OCPMs plus WM in all the outcomes as compared with WM and further verified the best intervention for effective clinical rate, effective rate in ECG, weekly frequency of angina, and cardiovascular events rate as QSYQ + WM, QSYQ + WM, QLQX + WM, and DL + WM, respectively (see Supplementary Material S13 for sensitivity analyses). Subgroup analyses suggested that the benefits of effective clinical rate, effective rate in ECG, duration of an angina attack, and cardiovascular events rate of OCPMs + WM vs. WM, individually, were more evident in patients with a trial duration of fewer than three months, sample size less than 100, trial duration greater than or equal to three months, trial duration greater than or equal to three months/sample size greater than or equal to 100. The results of the subgroup analyses are provided in Supplementary Material S14.
4 Discussion
The current network meta-analysis is the first study investigating OCPMs on stable angina pectoris. Although there have been several published network meta-analyses reporting the efficacy of Chinese patent medicine on stable angina pectoris, they all included traditional Chinese medicine injections or unlisted oral decoctions as the interventions and enrolled unstable angina patients as the target population, with a limited number of included studies (Ding, 2017; Ji et al., 2019; Wang Z. X. et al., 2021; Sun et al., 2021). Our study revealed that the addition of OCPMs based on WM could achieve a better clinical effect than WM alone for stable angina pectoris, which was consistent with the results of published pairwise meta-analyses (Lu et al., 2017; Pan et al., 2019; Xi et al., 2019; Zheng et al., 2021; Zhuan et al., 2021). Additionally, by comparing different interventions, this study also suggested that QSYQ + WM, QLQX + WM, KXQW + WM, TXL + WM, DL + WM, SSYX + WM, and SXBX + WM deserve more attention in treating stable angina.
Stable angina pectoris belongs to the category of “chest impediment with stabbing pain” based on the theoretical principles of traditional Chinese medicine (Wang and Chen, 2018). The theory expounds that this disease is caused by blood stasis, status as a result of qi deficiency or qi stagnation, thereby leading to the occlusion of the heart vessel (Wu, 2017). Based on the pathogenesis, therefore, traditional Chinese medicines that possess efficacy for invigorating qi, activating blood, regulating qi, and dredging collaterals, are used to treat stable angina pectoris (Wu, 2017). The selected OCPMs in this study all belong to this class of drugs.
Among the included OCPMs, QSYQ is a dripping pill made by Astragalus mongholicus Bunge [Fabaceae], Salvia miltiorrhiza Bunge [Lamiaceae], Panax notoginseng (Burkill) F.H.Chen [Araliaceae], and Dalbergia odorifera T.C.Chen [Fabaceae] by water-extraction and an alcohol-precipitation method, primarily containing salvianolic acid, protocatechuic aldehyde, and flavonoids (Fu et al., 2012). Some published research demonstrated that QSYQ could ameliorate ventricular remodeling, suppress arachidonic acid lipoxygenase pathway as well as elevation of nitric oxide, improve dyslipidemia mediated via fatty acid oxidation, and regulate the PI3K/Akt-mTOR pathway, all of which possessed positive effects on the heart and blood vessels in patients with stable angina (Wang et al., 2017; Lv et al., 2020). QLQX is prepared from 11 different botanical drugs, including Astragalus mongholicus Bunge [Fabaceae], Panax ginseng C.A.Mey [Araliaceae], and Aconitum carmichaeli Debeaux [Ranunculaceae], containing mainly flavonoids, saponins, and triterpenoids (Lu et al., 2021). Based on a published study, the drug could potentially modulate metabolic proteins regionally to guide the border myocardium against hypoxia injuries and oxidize fatty acids to maximize energy utilization, thus protecting surviving cardiomyocytes (Cheng et al., 2020). KXQW are composed of Borneolum Syntheticum, volatile oils of Asarum heterotropoides F. Schmidt [Aristolochiaceae], Santalum album L [Santalaceae], Alpinia officinarum Hance [Zingiberaceae], and Piper longum L [Piperaceae], mainly containing 1, 8-cineole, borneol, methyleugenol, and satanol (Sun, 1985). The mechanism of action of KXQW includes dilating the coronary artery by activating the CaMK II/ERK signaling pathway and suppressing the influx and release of calcium, which might improve myocardial injury among stable angina patients (Lu et al., 2022). TXL is prepared from 12 different traditional Chinese medicines (e.g., Panax ginseng C.A.Mey [Araliaceae] and Santalum album L. [Santalaceae]), comprising active ingredients such as resveratrol, arbutin, and palmitic acid (Mi, 2018; Sun, 2018). A basic experiment elaborated on the effects of TXL on suppressing atherosclerosis development and stabilizing plaque by regulating inflammation, lipid metabolism, cell physical function, hormone secretion, protein binding, and immune response process (Ma et al., 2019). DL comprises ten different types of botanical drugs such as Trichosanthes rosthornii Harms [Cucurbitaceae] and Allium macrostemon Bunge [Amaryllidaceae] with components primarily as artemisinolide (17.49%), β-Elemene (11.07%), and (-) Spartol (8.95%) (Zhang et al., 2016). Studies of mechanism indicated that DL could inhibit NF-κB signaling, trigger PPARα/ABCA1 signaling pathway, and activate PI3K/Akt/mTOR-mediated autophagy of vascular adventitial fibroblasts, thus preventing atherosclerosis (Hao et al., 2019; Wang L. et al., 2021). SXBX is composed of seven traditional Chinese medicines such as Panax ginseng C.A.Mey [Araliaceae], Cinnamomum verum J. Presl [Lauraceae], and Liquidambar orientalis Mill [Altingiaceae]. A systematic review summarized the mechanism of SXBX for vessels and the heart, including promotion of angiogenesis, amelioration of inflammation, improvement of endothelium dysfunction, mitigation of dyslipidemia, proliferation/migration repression of vascular smooth muscle cells, and restraint of cardiac remodeling (Lu et al., 2018). SSYX contains 12 types of traditional Chinese medicines, including Panax ginseng C.A.Mey [Araliaceae], Ophiopogon japonicus (Thunb.) Ker Gawl [Asparagaceae], and Cornus officinalis Siebold and Zucc. [Cornaceae], etc. (Bai et al., 2018). Published studies confirmed that SSYX could reduce the incidence and severity of myocardial ischemic arrhythmias and decrease the area of myocardial necrosis caused by coronary insufficiency, which may be related to extending the action potential and alleviating Ca2+ overload (Zhao et al., 2016).
In addition to the curative effect of OCPMs on stable angina, the ADRs caused by the drug should also be of great concern, although our study demonstrated that the selected OCPMs did not cause severe ADRs. To generate fewer ADRs when using OCPMs, a study suggests avoiding taking the selected OCPMs on an empty stomach (Dai and Yu, 2002). Additionally, prescribing drugs according to patients’ traditional Chinese syndromes may be another suggestion (Ye et al., 2021).
4.1 Limitations
First, all trials included were assessed as some concerns according to RoB2. Therefore, the results should be interpreted cautiously. Second, some interventions included a limited number of studies, such as one RCT for KXQW + WM, three RCTs for QLQX + WM, and four RCTs for QSYQ + WM, and two RCTs for XFZY + WM. Therefore, these results should be interpreted with caution. Finally, the studies selected in the current network meta-analysis were conducted in China, so the results may not be generalizable to other countries.
5 Conclusion
In treating stable angina, adding OCPMs besides WM may acquire a better curative effect. QSYQ + WM, QLQX + WM, KXQW + WM, TXL + WM, DL + WM, SSYX + WM, and SXBX + WM are worth taking into account in treating patients with stable angina, while SXBX + WM merits more attention. Further careful assessment of this conclusion is needed in future clinical studies which must be of higher quality.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
Author contributions
PH and BC conceived the study. YF and SL performed the literature search, screening, and extraction. QW and HZ implemented quality assessment. PH, ZL, LC, JZ, YT, YC, BH, XH, and LZ performed the network meta-analysis. PH wrote the manuscript. BC, ZZ, YL, HG, and SZ coordinated the revision of the manuscript. All authors approved the final version of this manuscript.
Funding
This study was funded by the National Natural Science Foundation of China (Grant Nos. 81273961 and 81303117), the Municipal School (college) Joint Funding Project of Guangzhou Municipal Science and Technology Foundation (Grant No. 202201020352), Science and Technology Foundation of Shenzhen City (Grant No. JSGG20220226085800001), Science and Technology Foundation of Shenzhen City (Grant No. JCYJ20190812164009243), and Guangdong Medical Research Foundation (Grant No. B2020135).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.918689/full#supplementary-material
References
Bai, Y. D., Qiao, Z., Xue, J. W., Liu, F. L., and Liu, W. Y. (2018). Simultaneous determination of different constituents in Shensong Yangxin capsules and method validation. Chin. J. Pharm. Anal. 38 (08), 1358–1368. doi:10.16155/j.0254-1793.2018.08.10
Bhatt, D. L., Eagle, K. A., Ohman, E. M., Hirsch, A. T., Goto, S., Mahoney, E. M., et al. (2010). Comparative determinants of 4-year cardiovascular event rates in stable outpatients at risk of or with atherothrombosis. J. Am. Med. Assoc. 304 (12), 1350–1357. doi:10.1001/jama.2010.1322
Boden, W. E., O'Rourke, R. A., Teo, K. K., Hartigan, P. M., Maron, D. J., Kostuk, W. J., et al. (2007). Optimal medical therapy with or without PCI for stable coronary disease. N. Engl. J. Med. 356 (15), 1503–1516. doi:10.1056/NEJMoa070829
Caldwell, D. M., Ades, A. E., and Higgins, J. P. (2005). Simultaneous comparison of multiple treatments: combining direct and indirect evidence. Bmj 331 (7521), 897–900. doi:10.1136/bmj.331.7521.897
Cheng, W., Wang, L., Yang, T., Wu, A., Wang, B., Li, T., et al. (2020). Qiliqiangxin capsules optimize cardiac metabolism flexibility in rats with heart failure after myocardial infarction. Front. Physiol. 11, 805. doi:10.3389/fphys.2020.00805
Dai, L., and Yu, X. H. (2002). Rational use of proprietary Chinese medicines. Strait Pharm. J. 14 (04), 86–87. doi:10.3969/j.issn.1006-3765.2002.04.052
Dancy, L., O'Gallagher, K., Milton, P., and Sado, D. (2018). New NICE guidelines for the management of stable angina. Br. J. Gen. Pract. 68 (669), 202–203. doi:10.3399/bjgp18X695693
Dias, S., Sutton, A. J., Ades, A. E., and Welton, N. J. (2013). Evidence synthesis for decision making 2: a generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med. Decis. Mak. 33 (5), 607–617. doi:10.1177/0272989x12458724
Ding, L. L. (2017). Network Meta-analysis and summary evaluation of Chinese patent medicine adjuvant treatment of angina pectoris. Kunming: Kunming Medical University. Master.
Fihn, S. D., Gardin, J. M., Abrams, J., Berra, K., Blankenship, J. C., Dallas, A. P., et al. (2012). 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American college of cardiology foundation/American heart association task force on practice guidelines, and the American college of physicians, American association for thoracic surgery, preventive cardiovascular nurses association, society for cardiovascular angiography and interventions, and society of thoracic surgeons. J. Am. Coll. Cardiol. 60 (24), e44–e164. doi:10.1016/j.jacc.2012.07.013
Fu, J. Z., Song, Y. S., Jiang, M., Peng, J. M., Wang, J., Huang, H., et al. (2012). Simultaneous determination of the contents of astragaloside, danshensu, protocatechualdehyde, ginsenosides Rg1 and Rb1 in qishenyiqi dropping pills by LC-MS. Chin. Pharm. J. 47 (01), 61–64.
Hao, D., Danbin, W., Maojuan, G., Chun, S., Bin, L., Lin, Y., et al. (2019). Ethanol extracts of Danlou tablet attenuate atherosclerosis via inhibiting inflammation and promoting lipid effluent. Pharmacol. Res. 146, 104306. doi:10.1016/j.phrs.2019.104306
Higgins, J. P., and Thompson, S. G. (2002). Quantifying heterogeneity in a meta-analysis. Stat. Med. 21 (11), 1539–1558. doi:10.1002/sim.1186
Higgins, J. P., Jackson, D., Barrett, J. K., Lu, G., Ades, A. E., White, I. R., et al. (2012). Consistency and inconsistency in network meta-analysis: Concepts and models for multi-arm studies. Res. Synth. Methods 3 (2), 98–110. doi:10.1002/jrsm.1044
Ji, Z. C., Yang, F. W., Zhang, L. S., Jin, X. Y., Wang, H. C., Pang, W. T., et al. (2019). Network Meta-analysis of Yiqi Huoxue Chinese patent medicine for coronary heart disease with angina pectoris. China J. Chin. Materia Med. 44 (09), 1927–1937. doi:10.19540/j.cnki.cjcmm.20190114.001
Jones, M., Rait, G., Falconer, J., and Feder, G. (2006). Systematic review: prognosis of angina in primary care. Fam. Pract. 23 (5), 520–528. doi:10.1093/fampra/cml038
Joshi, P. H., and De Lemos, J. A. (2021). Diagnosis and management of stable angina: A review. J. Am. Med. Assoc. 325 (17), 1765–1778. doi:10.1001/jama.2021.1527
Li, T., Puhan, M. A., Vedula, S. S., Singh, S., and Dickersin, K. (2011). Network meta-analysis-highly attractive but more methodological research is needed. BMC Med. 9, 79. doi:10.1186/1741-7015-9-79
Lu, J. J., Lei, X., and Shang, H. C. (2017). Systematic review of Danlou Tablets in the treatment of stable angina pectoris with mutual resistance of phlegm and blood stasis. Chin. J. Integr. Med. Cardio/Cerebrovasc. Dis. 15 (10), 1198–1202. doi:10.3969/j.issn.1672-1349.2017.10.014
Lu, L., Sun, X., Chen, C., Qin, Y., and Guo, X. (2018). Shexiang Baoxin pill, derived from the traditional Chinese medicine, provides protective roles against cardiovascular diseases. Front. Pharmacol. 9, 1161. doi:10.3389/fphar.2018.01161
Lu, S. L., Feng, Y., Gao, J., Jin, X. G., Wang, Y. X., and Chen, K. J. (2021). Recent advances in clinical application of Panax notoginseng saponins in cardiovascular diseases. Chin. General Pract. 24 (5), 539–545. doi:10.12114/j.issn.1007-9572.2020.00.623
Lu, Y., Yang, M. L., Shen, A. L., Lin, S., Peng, M. Z., Wang, T. Y., et al. (2022). Pharmacodynamic mechanism of Kuanxiong aerosol for vasodilation and improvement of myocardial ischemia. Chin. J. Integr. Med. 28 (4), 319–329. doi:10.1007/s11655-021-2882-z
Lv, S., Yuan, P., Dong, J., Lu, C., Li, M., Qu, F., et al. (2020). QiShenYiQi pill improves the reparative myocardial fibrosis by regulating autophagy. J. Cell. Mol. Med. 24 (19), 11283–11293. doi:10.1111/jcmm.15695
Ma, J., Qiao, L., Meng, L., Ma, L., Zhao, Y., Liu, X., et al. (2019). Tongxinluo may stabilize atherosclerotic plaque via multiple mechanisms scanning by genechip. Biomed. Pharmacother. 113, 108767. doi:10.1016/j.biopha.2019.108767
Mao, C., Chung, V. C., Yuan, J. Q., Yu, Y. Y., Yang, Z. Y., Wu, X. Y., et al. (2013). Evaluation of the add-on effect of Chinese patent medicine for patients with stable or unstable angina: a systematic review and meta-analysis. Evid. Based. Complement. Altern. Med. 2013, 673193. doi:10.1155/2013/673193
Mao, J. Y., Wu, Y. J., and Shi, D. Z. (2021). Guidelines for clinical application of Chinese patent medicines in the treatment of coronary heart disease (2020). Chin. J. Integr. Med. Cardio/Cerebrovasc. Dis. 19 (09), 1409–1435. doi:10.12102/j.issn.1672-1349.2021.09.001
Mensah, G. A., Roth, G. A., and Fuster, V. (2019). The global burden of cardiovascular diseases and risk factors: 2020 and beyond. Washington, DC: American College of Cardiology Foundation.
Mi, H. Y. (2018). Analysis of the medical records of Professor Wu Yiling in the treatment of coronary heart disease and angina pectoris based on data mining and network pharmacology research of Tongxinluo Capsules. Hubei: Hebei Medical University. doctor.
Mills, E. J., Ioannidis, J. P., Thorlund, K., Schünemann, H. J., Puhan, M. A., Guyatt, G. H., et al. (2012). How to use an article reporting a multiple treatment comparison meta-analysis. J. Am. Med. Assoc. 308 (12), 1246–1253. doi:10.1001/2012.jama.11228
Montalescot, G., Sechtem, U., Achenbach, S., Andreotti, F., Arden, C., Budaj, A., et al. (2013). 2013 ESC guidelines on the management of stable coronary artery disease: the task force on the management of stable coronary artery disease of the European society of cardiology. Eur. Heart J. 34 (38), 2949–3003. doi:10.1093/eurheartj/eht296
Ohman, E. M. (2016). Chronic stable angina. N. Engl. J. Med. 374 (12), 293. doi:10.1056/NEJMc1605394
Pan, F. Q., Xi, Y. T., Huang, T. F., Cao, Y. H., and Wu, W. (2019). Meta-analysis of Shexiang Baoxin Pill in the treatment of stable angina pectoris. Shizhen Tradit. Chin. Med. 30 (12), 3041–3045. CNKI:SUN:SZGY.0.2019-12-078.
Roth, G. A., Johnson, C., Abajobir, A., Abd-Allah, F., Abera, S. F., Abyu, G., et al. (2017). Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J. Am. Coll. Cardiol. 70 (1), 1–25. doi:10.1016/j.jacc.2017.04.052
Salanti, G. (2012). Indirect and mixed-treatment comparison, network, or multiple-treatments meta-analysis: many names, many benefits, many concerns for the next generation evidence synthesis tool. Res. Synth. Methods 3 (2), 80–97. doi:10.1002/jrsm.1037
Sterne, J. A. C., Savović, J., Page, M. J., Elbers, R. G., Blencowe, N. S., Boutron, I., et al. (2019). RoB 2: a revised tool for assessing risk of bias in randomised trials. Bmj 366, l4898. doi:10.1136/bmj.l4898
Sun, Y. Z., Wang, Z. Y., Tang, Z. R., Huang, L. X., and Zhao, H. B. (2021). Network meta-analysis of Chinese patent medicines of regulating qi and activating blood circulation for angina pectoris. World Chin. Med. 16 (21), 3204–3212+3218. doi:10.3969/j.issn.1673-7202.2021.21.017
Sun, E. T. (1985). Gas chromatographic determination of Chinese patent medicine Kuanxiong aerosol. Chromatography 2 (06), 342–345+354.
Sun, M. S. (2018). The therapeutic effect and mechanism of Tongxinluo through PI3K/Akt pathway on cerebral ischemia reperfusion injury in rats. Jilin: Jilin University. doctor.
van Valkenhoef, G., Dias, S., Ades, A. E., and Welton, N. J. (2016). Automated generation of node-splitting models for assessment of inconsistency in network meta-analysis. Res. Synth. Methods 7 (1), 80–93. doi:10.1002/jrsm.1167
Wang, J., and Chen, G. (2018). Expert consensus on TCM diagnosis and treatment of stable angina pectoris with coronary heart disease. J. Traditional Chin. Med. 59 (05), 447–450. doi:10.13288/j.11-2166/r.2018.05.020
Wang, Y., Lin, W., Li, C., Singhal, S., Jain, G., Zhu, L., et al. (2017). Multipronged therapeutic effects of Chinese herbal medicine qishenyiqi in the treatment of acute myocardial infarction. Front. Pharmacol. 8, 98. doi:10.3389/fphar.2017.00098
Wang, L., Wu, T., Si, C., Wang, H., Yue, K., Shang, S., et al. (2021a). Danlou tablet activates autophagy of vascular adventitial fibroblasts through PI3K/Akt/mTOR to protect cells from damage caused by atherosclerosis. Front. Pharmacol. 12, 730525. doi:10.3389/fphar.2021.730525
Wang, Z. X., Ban, J. F., Li, R. L., Wang, T. F., and Ke, R. (2021b). Network-meta analysis of 9 kinds of patent Chinese medicine for nourishing qi and activating blood in the treatment of angina pectoris of coronary heart disease. J. Hainan Med. Univ. 27 (11), 845–854. doi:10.13210/j.cnki.jhmu.20200924.001
Wu, M. H. (2017). Internal medicine of traditional Chinese medicine. Beijing: China Traditional Chinese Medicine Press.
Xi, Y. T., Yuan, L. Y., Zeng, Y. Y., Yan, M. L., Liang, X. R., Feng, A. T., et al. (2019). Shensong Yangxin Capsules in the adjuvant treatment of stable angina pectoris:a Meta-analysis and trial sequential analysis. China J. Chin. Materia Med. 44 (17), 3816–3824. doi:10.19540/j.cnki.cjcmm.20190624.503
Ye, L., Xie, H., Yu, H. M., and Yuan, H. (2021). Analysis of the current situation of traditional Chinese medicine and rational drug use countermeasures. J. Tradit. Chin. Med. Manag. 29 (24), 86–88. doi:10.16690/j.cnki.1007-9203.2021.24.049
Zhang, N., Li, L., Gao, S., Zhu, Y., Wang, J. M., Zhang, P., et al. (2016). HS-SPEM-GC-MS analysis of the volatile components of Dan-lou tablets. J. Tianjin Univ. Tradit. Chin. Med. 35 (04), 258–261. doi:10.11656/j.issn.1673-9043.2016.04.10
Zhao, Y., Gao, F., Zhang, Y., Wang, H., Zhu, J., Chang, L., et al. (2016). Shensong Yangxin capsules prevent ischemic arrhythmias by prolonging action potentials and alleviating Ca2+ overload. Mol. Med. Rep. 13 (6), 5185–5192. doi:10.3892/mmr.2016.5203
Zheng, Y. Y., Wang, X. L., and Wang, X. Y. (2021). Meta-analysis and pharmacoeconomic evaluation of compound danshen dropping pills and isosorbide nitrate tablets in the treatment of stable Angina pectoris. China Pharm. 30 (12), 87–91. doi:10.3969/j.issn.1006-4931.2021.12.023
Zhuan, S. P., Zhu, Y. F., and Wei, J. R. (2021). A meta-analysis of the efficacy of compound Danshen dripping pills (CSDP) combined with nitrates in the treatment of stable angina pectoris of coronary heart disease. Int. Med. Health Guid. News 27 (04), 501–508. doi:10.3760/cma.j.issn.1007-1245.2021.04.007
Keywords: stable angina, oral chinese patent medicines, Western medicine, effect, network meta-analysis
Citation: Huang P, Li Z, Chen L, Zeng J, Zhao S, Tang Y, Huang B, Guan H, Chen Y, Feng Y, Lei S, Wu Q, Zhang H, Huang X, Zeng L, Liu Y, Zeng Z and Chen B (2022) The comparative effects of oral Chinese patent medicines combined with western medicine in stable angina: A systematic review and network meta-analysis of 179 trials. Front. Pharmacol. 13:918689. doi: 10.3389/fphar.2022.918689
Received: 12 April 2022; Accepted: 15 July 2022;
Published: 17 August 2022.
Edited by:
Ren-You Gan, Institute of Urban Agriculture (CAAS), ChinaReviewed by:
Qiaobo Ye, Chengdu University of Traditional Chinese Medicine, ChinaXin Li, Shanghai University of Traditional Chinese Medicine, China
Copyright © 2022 Huang, Li, Chen, Zeng, Zhao, Tang, Huang, Guan, Chen, Feng, Lei, Wu, Zhang, Huang, Zeng, Liu, Zeng and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bojun Chen, NzE5NTIzNDc2QHFxLmNvbQ==