 Luiz Carlos da Costa-Junior1,2
Luiz Carlos da Costa-Junior1,2 Daniely Regina Freitas-Alves3Amanda Melo Leite Leão4,5Hayra de Andrade Vieira Monteiro6Rita de Cássia Barbosa da Silva Tavares2
Daniely Regina Freitas-Alves3Amanda Melo Leite Leão4,5Hayra de Andrade Vieira Monteiro6Rita de Cássia Barbosa da Silva Tavares2 Maria Claudia Rodrigues Moreira2,7Marília Berlofa Visacri8
Maria Claudia Rodrigues Moreira2,7Marília Berlofa Visacri8 Teresa de Souza Fernandez5*
Teresa de Souza Fernandez5* Paulo Caleb Júnior de Lima Santos1,9*
Paulo Caleb Júnior de Lima Santos1,9*- 1Postgraduate Program in Medical Sciences, Faculdade de Medicina da Universidade de São Paulo (FMUSP), São Paulo, Brazil
- 2Bone Marrow Transplant Center, Instituto Nacional de Câncer (INCA), Rio de Janeiro, Brazil
- 3Escola Nacional de Saúde Pública Sérgio Arouca, Fundação Oswaldo Cruz (ENSP-FIOCRUZ), Rio de Janeiro, Brazil
- 4Escola de Ciências da Saúde, Universidade do Grande Rio (Unigranrio), Duque de Caxias, Brazil
- 5Cytogenetic Laboratory, Cell and Gene Therapy Program, Instituto Nacional de Câncer (INCA), Rio de Janeiro, Brazil
- 6Clinical Research Division, Instituto Nacional de Câncer (INCA), Rio de Janeiro, Brazil
- 7Bone Marrow Transplant Program, Hospital Universitário Clementino Fraga Filho (HUCFF), Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, Brazil
- 8Departament of Pharmacy, Faculdade de Ciências Farmacêuticas, Universidade de São Paulo (FCF-USP), São Paulo, Brazil
- 9Department of Pharmacology, Escola Paulista de Medicina, Universidade Federal de São Paulo (EPM-Unifesp), São Paulo, Brazil
This systematic review assessed the impact of CYP3A5, CYP3A4, and ABCB1 polymorphisms on the pharmacokinetics and clinical outcomes of calcineurin inhibitors in hematopoietic cell transplantation (HCT) recipients. Following PRISMA 2020 guidelines, the protocol was registered in PROSPERO (CRD42024517094). A comprehensive search in PubMed, BVS, Scopus, Web of Science, Embase, and Cochrane databases (2013–2024) identified observational studies focusing on tacrolimus or cyclosporine and the specified polymorphisms. Studies on non-human subjects, solid organ transplants, pharmacokinetic models, and drug interactions were excluded. Narrative synthesis was employed due to heterogeneity, and study quality was evaluated using the Newcastle–Ottawa Scale (NOS) and STREGA guidelines. Of 301 records, 11 studies met inclusion criteria, predominantly retrospective and involving adult populations, with sample sizes ranging from 20 to 420 HCT recipients from the USA, Japan, and France. Outcomes included drug levels, median concentration/dose (C/D) ratio, therapeutic index, and clinical endpoints such as graft-versus-host disease (GVHD) and acute kidney injury (AKI). CYP3A5*3 (rs776746) significantly influenced tacrolimus levels, C/D ratio, and clinical outcomes, highlighting its potential as a pharmacogenetic biomarker. CYP3A4 and ABCB1 polymorphisms demonstrated limited effects on tacrolimus pharmacokinetics and no significant clinical impact. Methodological quality was high, with 55% of studies achieving the maximum NOS score, although gaps in error rates and population modeling were noted. Limitations include variability in outcomes precluding meta-analysis, a small number of studies, particularly on cyclosporine, and insufficient data on CYP3A4 and ABCB1. Further research is necessary to validate findings.
Systematic Review Registration: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024517094, PROSPERO, CRD42024599998.
1 Introduction
Graft-versus-host disease (GVHD) after allogeneic hematopoietic cell transplantation (HCT) is associated with morbidity and mortality (Lee and Flowers, 2008; Malard et al., 2023). The most commonly used regimens for prevention of acute GVHD (aGVHD) consist of a combination of a calcineurin inhibitor (CNI), either cyclosporine (CSP) or tacrolimus (TAC), and an antimetabolite methotrexate (Funke et al., 2023; Penack et al., 2020; Storb et al., 1986; Storb et al., 1989). However, the use of these drugs presents major challenges in clinical practice due to their wide interindividual variability in pharmacokinetics, which may lead to frequent dose adjustments, substitution with other immunosuppressants, or even discontinuation. Therefore, successful treatment involves continuous monitoring of plasma levels within a target range (Brunet et al., 2019; Penack et al., 2024) to avoid subtherapeutic concentrations, which may increase the risk of GVHD (Arcuri et al., 2022; Yee et al., 1988), or supratherapeutic doses, which may increase the risk of toxicities (da Silva et al., 2014; Ram et al., 2012).
Regarding the pharmacokinetics of CNIs, both CSP and TAC undergo hepatic biotransformation primarily mediated by CYP3A4 (Cytochrome P450 Family 3 Subfamily A Member 4) and CYP3A5 (Cytochrome P450 Family 3 Subfamily A Member 5) enzymes, with a greater contribution from CYP3A5 to their oxidation and subsequent elimination. In addition, these drugs are also substrates of the P-glycoprotein (Pgp) efflux pump present in various compartments of the body and expressed by the ABCB1 (ATP-Binding Cassette Subfamily B Member 1) gene (Barbarino et al., 2013; Forsythe and Paterson, 2014; Hesselink, 2003; Iwasaki, 2007). Therefore, these proteins play a central role in the pharmacokinetics of these two immunosuppressants, potentially interfering with their absorption, distribution, biotransformation, and elimination. Genetic polymorphisms in the CYP3A5 (Khan et al., 2020; Zhang et al., 2017), CYP3A4 (Abdel-Kahaar et al., 2019; Kong et al., 2023; Wang et al., 2018), and ABCB1 (Hu et al., 2018; Lee et al., 2015; Oetting et al., 2018; Rotarescu et al., 2024) genes it could affect the expression of these biotransformation and transport proteins, which could contribute to this interindividual variability in CNI plasma levels and consequently, could contribute to different clinical outcomes.
Recent guideline from the Clinical Pharmacogenetics Implementation Consortium (CPIC) provide a comprehensive set of recommendations for pharmacogenetic-guided TAC starting dose prescribing (Birdwell et al., 2015). However, these recommendations are mainly based on experience in solid organ transplant patients, and there is a lack of evidence to support the application of CPIC recommendations to the allogeneic HCT recipient population. Additionally, there is a significant gap in studies on the pharmacogenetics of CSP, and unlike TAC, there are no established guidelines to inform its dosing in clinical practice. Within this context, the objective of this systematic review is to evaluate the impact of polymorphisms in the CYP3A5, CYP3A4, and ABCB1 genes on pharmacokinetics and/or clinical outcomes of the CNIs particularly in the population in HCT recipients.
2 Methods
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (PRISMA) 2020 checklist and reporting guideline (Page et al., 2021). The protocol of the systematic review was registered on PROSPERO, which is available at CRD42024517094.
2.1 Eligibility criteria
Inclusion criteria were: (1) articles published in English; (2) primary research articles; (3) observational studies on the pharmacogenetics of CNIs (tacrolimus and/or cyclosporine); and (4) studies that evaluated pharmacokinetic-related polymorphisms in the CYP3A5, CYP3A4, or ABCB1 genes, based on germline DNA from hematopoietic cell transplant recipients. Exclusion criteria were (1) non-human (animal models or in vitro); (2) approach in any type of solid organ transplant; (3) pharmacogenetics focused on a pharmacokinetic model; (4) genetic polymorphisms with a focus on drug interactions; and (5) articles published in non-Roman characters.
2.2 Search strategy
A comprehensive literature search was performed to identify relevant studies in the PubMed, BVS, Scopus, Web of Science, Embase and Cochrane databases published from 1 January 2013, to 9 February 2024. The detailed search strategy for all databases can be found in Supplementary Table S1. References found in included studies were screened for potential studies that had not yet been identified. Duplicate studies were excluded from the analysis.
2.3 Study selection
The population, exposure, comparator, outcomes, and study design (PECOS) model was used to select potential studies: P (population), HCT recipient; E (exposure) and C (comparator), patients with different genotypes (wild or altered) of polymorphisms in genes related to calcineurin inhibitors (i.e., genes influencing the pharmacokinetics of TAC and/or CSP: CYP3A5, CYP3A4 and ABCB1); O (outcomes), alteration in pharmacokinetic parameters and clinical outcomes such as acute GVHD, acute kidney injury (AKI), neurotoxicity, thrombotic microangiopathy (TMA), and transplant-related mortality, among other complications; and S (study design), observational (cohort, case-control, or cross-sectional). Conference abstracts, reviews, books or book chapters, case reports, letters, or trial registry records were excluded.
Two blinded reviewers (LCCJ and DRFA) independently screened the titles and abstracts of citations to identify potentially relevant studies. Full-text articles were retrieved, and the same two reviewers (LCCJ and DRFA) independently reviewed the articles according to the inclusion criteria. The third (HAVM) and fourth (AMLL) reviewer, after discussion, resolved any disagreements or questions. This process was performed using Rayyan (Ouzzani et al., 2016), a web application developed to assist researchers in conducting systematic reviews.
2.4 Data extraction
The information extracted for each included study encompassed the author, year of publication, country of origin, number of patients per study, study design, recruitment period, age range, genotyping method, polymorphisms evaluated in each study, including genotype and/or phenotype, outcomes evaluated, main results found, and funding sources/sponsors. Effect size estimates were analyzed based on metrics such as median drug levels, median concentration/dose (C/D) ratio, cumulative incidence of GVHD, AKI and TMA, in addition to the prevalence of the therapeutic index (supra or subtherapeutic), considered the main outcomes evaluated. Statistical significance was set at ≥ 95%, according to the description of each study. The extraction was conducted by two independent reviewers (LCCJ and DRFA) using standardized spreadsheets in Microsoft Excel and disagreements were resolved through discussion with the third (HAVM) and fourth (AMLL) reviewer.
2.5 Quality assessment
The assessment of the methodological quality of the studies (risk of bias) was performed using the Newcastle-Ottawa Scale (NOS) (Wells et al., 2024), applied by two independent reviewers (LCCJ and DRFA). Disagreements between the reviewers were resolved through discussion with a third (HAVM) and fourth (AMLL) reviewer. Three primary domains were assessed for each study: selection, comparability, and exposure. The maximum NOS scores for these domains were 4, 2, and 3 stars, respectively, resulting in a maximum possible total score of 9 stars per study. Studies were categorized as high quality (7–9 stars), moderate quality (4–6 stars), or low quality (0–3 stars).
To assess the quality of reporting of genetic association studies, we used the Strengthening the Reporting of Genetic Association (STREGA) guidelines (Little et al., 2009). These guidelines address five main categories: genotyping methods and errors, population stratification, haplotype variation, Hardy-Weinberg equilibrium, and replication. The first category encompasses five items: genotyping platform, error and call rates, batch genotyping, genotyping centers/laboratories, and the number of individuals with successful genotyping. A total of nine items were evaluated. To compare the quality of reporting of the studies, a total score was calculated by assigning one point to each item, with a higher score indicating better quality of reporting of the genetic study (range 0–9). This instrument was applied by two independent reviewers (LCCJ and DRFA), and disagreements were resolved through discussion with a third (HAVM) and fourth (AMLL) reviewer.
2.6 Data synthesis
The characteristics of the studies, their main results, and methodological quality were summarized descriptively through a narrative synthesis, supported by structured tables, as the data were too heterogeneous to be pooled.
3 Results
3.1 Search results
The electronic search of the databases resulted in the identification of 301 potentially relevant records. After removing duplicates and initial screening based on titles and abstracts, 21 articles were selected for full-text evaluation. Among the remaining 21 articles, 11 met all the inclusion criteria and did not provide reasons for exclusion. The justification for exclusion as well as the list of excluded articles are available in Supplementary Table S2. The review of the references of the included studies did not reveal any new relevant studies, consolidating the final selection of 11 articles for inclusion in this systematic review (Hamadeh et al., 2019; Ho et al., 2024; Khaled et al., 2016; Laverdière et al., 2015; Pasternak et al., 2022; Seligson et al., 2024; Suetsugu et al., 2019; Thoma et al., 2022; Yamashita et al., 2016; Yoshikawa et al., 2021; Zhu et al., 2020). The study selection process is illustrated in Figure 1.
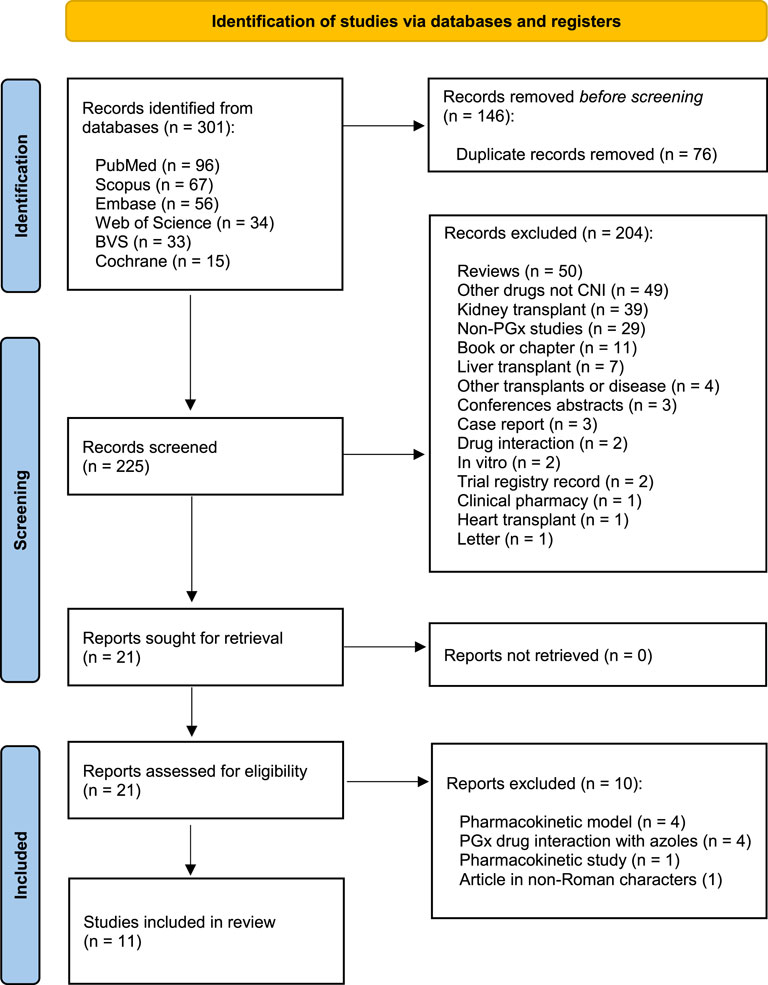
Figure 1. Study selection flowchart through literature search.
3.2 Study characteristics
The studies included in this systematic review present a diversity of settings, methodological designs, and demographic characteristics of participants, as described in Table 1. The review includes studies conducted in the USA (7), Japan (3), and France (1) with sample sizes ranging from 20 to 420 participants. Study designs include retrospective (n = 7) and prospective (n = 4) approaches. Most studies focused on adult populations, although some included adults and pediatric participants. The CNIs analyzed were predominantly TAC, with only 2 studies investigating CSP. The detailed clinical characteristics of the recipients, donors, and transplants from each of the studies included in this systematic review are available in Supplementary Table S3.
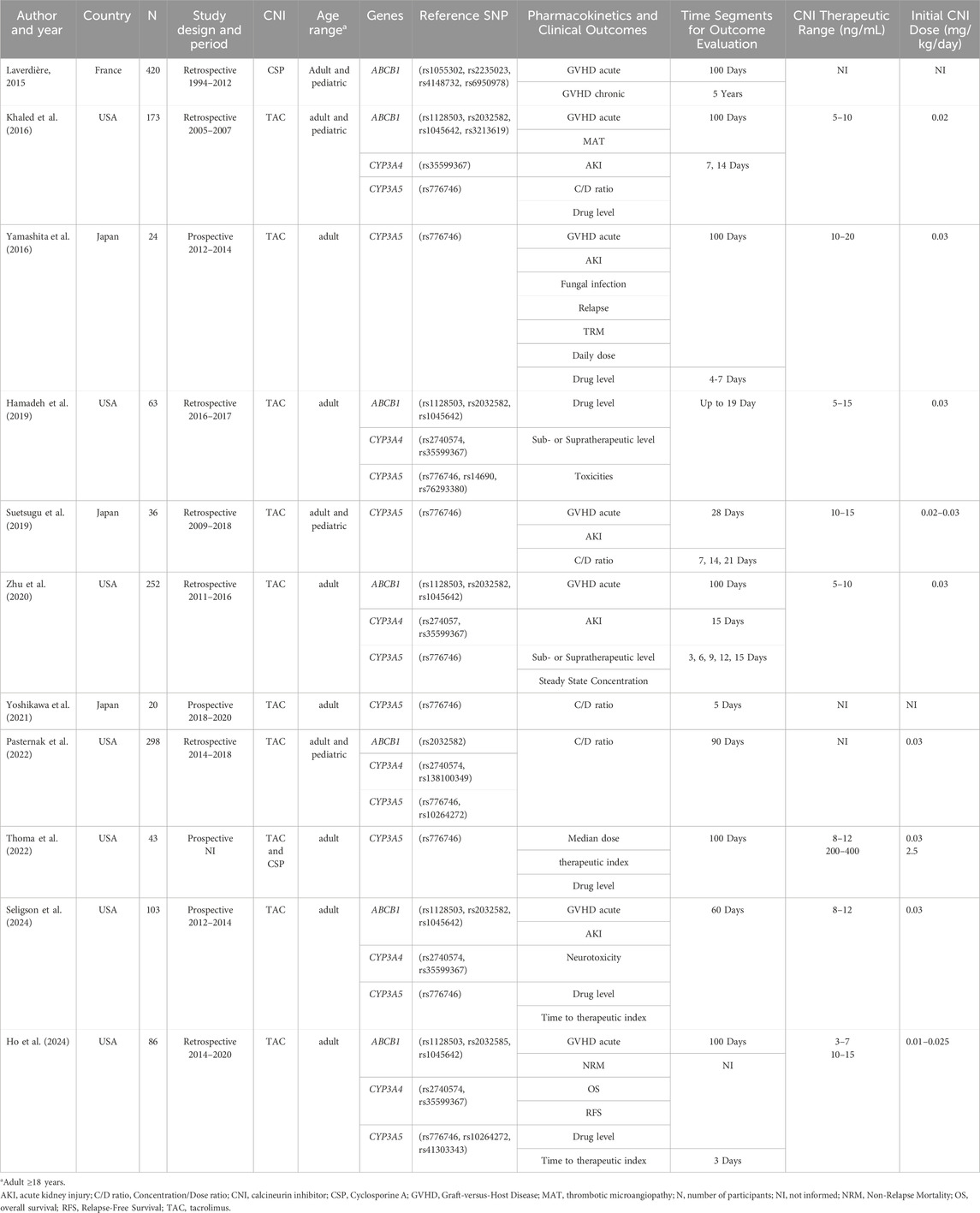
Table 1. General characteristics of the studies included in systematic review.
A variety of polymorphisms were examined across the studies, with the ABCB1 gene presenting the largest number of variants (9), followed by CYP3A5 (5 variants) and CYP3A4 (4 variants). Within the ABCB1 gene, the most widely analyzed polymorphisms were rs1045642, rs1128503 and rs2032582, which were addressed in five studies each. Regarding CYP3A4, the most frequently studied polymorphisms were rs2740574 and rs35599367, with 4 and 5 studies, respectively. For the CYP3A5 gene, the rs776746 polymorphism stands out as the most investigated (10 analyzed studies). Based on the findings of this systematic review, we highlight the role of polymorphisms in the CYP3A5 gene. The details of all genes and polymorphisms addressed in each of the studies are available in Supplementary Table S4.
Different outcomes were analyzed across the included studies. Clinical outcomes included graft-versus-host disease (GVHD), acute kidney injury (AKI), neurotoxicity, thrombotic microangiopathy (TMA), non-relapse mortality (NRM), overall survival (OS), and relapse-free survival (RFS). Pharmacokinetic outcomes encompassed drug levels, C/D ratio, steady-state concentrations, median dose, and the assessment of subtherapeutic or supratherapeutic ranges (therapeutic index). Additionally, some studies evaluated the time required to reach therapeutic levels.
3.3 Methodological quality of systematic reviews
The results of the quality assessment of the studies using the NOS are presented in Table 2. The total score in the studies ranged from six to nine stars. Most of the studies, 55% (6/11), achieved the maximum score (Hamadeh et al., 2019; Ho et al., 2024; Khaled et al., 2016; Laverdière et al., 2015; Pasternak et al., 2022; Zhu et al., 2020), indicating high methodological quality. Meanwhile 18% (2/11) scored eight, demonstrating minor deficiencies in comparability (Seligson et al., 2024) or selection (Suetsugu et al., 2019). Another 18% (2/11) scored 7, both (Yamashita et al., 2016; Yoshikawa et al., 2021) with limitations in representativeness and comparability. Finally, a study with six points (Thoma et al., 2022) presented weaknesses in selection and comparability, representing 9% (1/11) of the total. Overall, the three questions related to the outcome and selection domains were met consistently in all studies, which reinforces the predominance of high-quality studies and increases the reliability of the conclusions presented.
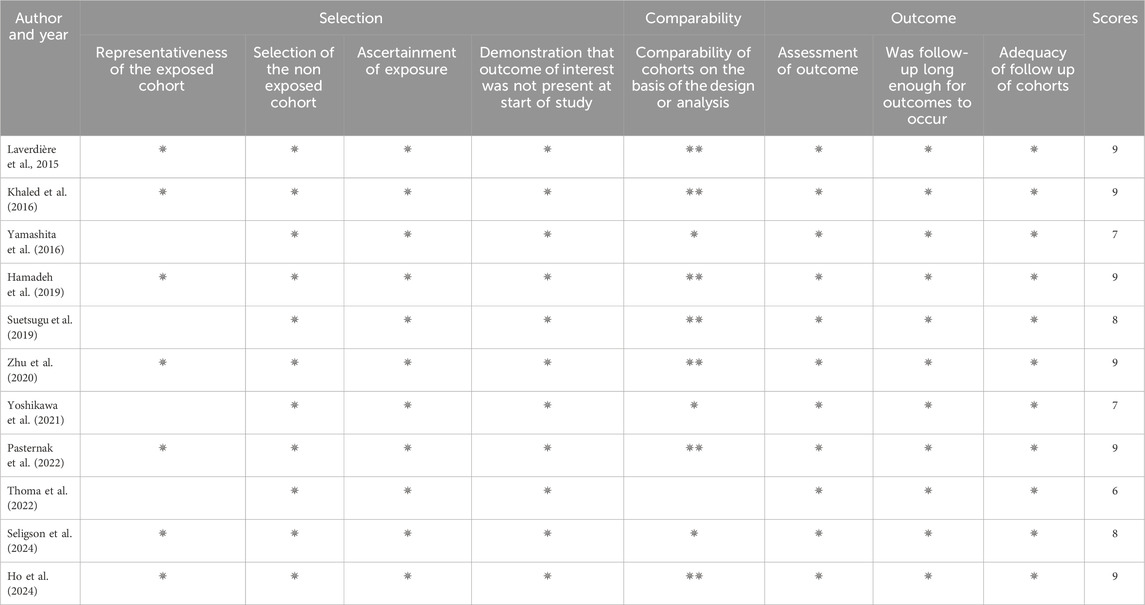
Table 2. Results of quality assessment using the Newcastle-Ottawa Scale (NOS) for studies.
Based on the STREGA guidelines, the quality of reporting in genetic studies included in this review is presented in Table 3. The scores of the 11 studies ranged from four to seven, with nine being the maximum possible points. The study conducted by Zhu et al. (2020) attained the highest score (seven), whereas Suetsugu et al. (2019) recorded the lowest score (four).
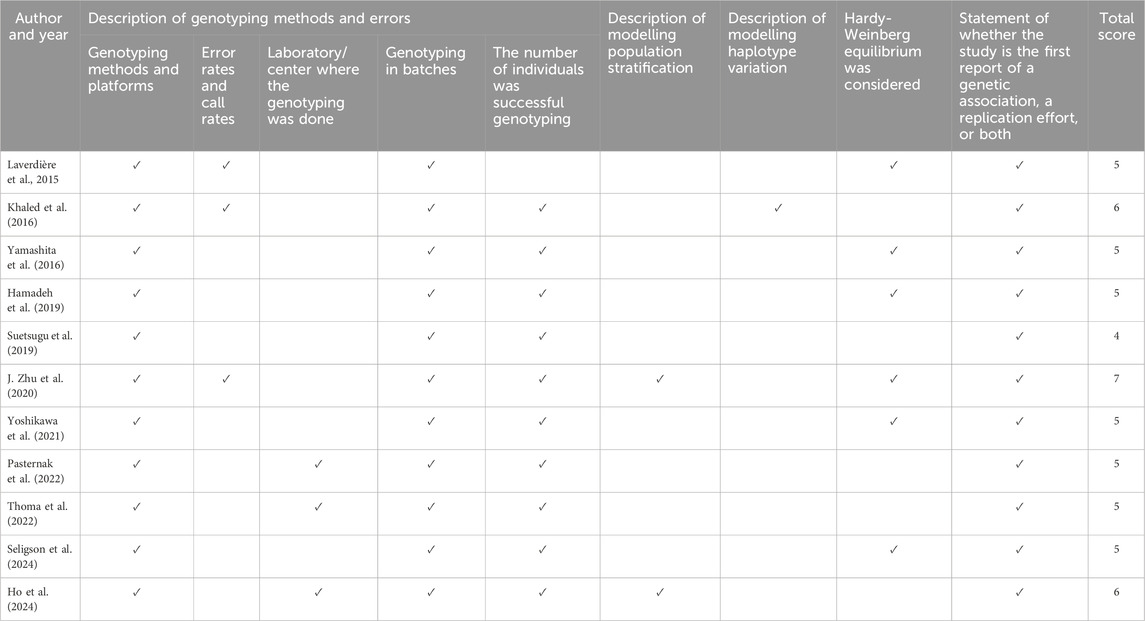
Table 3. The quality of reporting using the STrengthening the Reporting of Genetic Association (STREGA) guideline.
The other 9 studies were divided as follows: 18% (2/11) received a score of six (Ho et al., 2024; Khaled et al., 2016) and 64% (7/11) received a score of five (Hamadeh et al., 2019; Laverdière et al., 2015; Pasternak et al., 2022; Seligson et al., 2024; Thoma et al., 2022; Yamashita et al., 2016; Yoshikawa et al., 2021). The characteristics least reported in the articles were error and call rates, genotyping site, description of population model and haplotype stratification. In contrast, the platform used for genotyping, genotyping in batches, and number of individuals of successful genotyping and replication were reported in all studies. Finally, Hardy-Weinberg equilibrium was considered in six studies (Hamadeh et al., 2019; Laverdière et al., 2015; Seligson et al., 2024; Yamashita et al., 2016; Yoshikawa et al., 2021; Zhu et al., 2020).
3.4 Polymorphisms in the CYP3A5 gene
Except for Laverdière et al., 2015, all articles included in this review evaluated the influence of polymorphisms in CYP3A5 gene in relation to clinical and/or pharmacokinetic outcomes. The most studied polymorphism was rs776746, cited in ten studies (Hamadeh et al., 2019; Ho et al., 2024; Khaled et al., 2016; Pasternak et al., 2022; Seligson et al., 2024; Suetsugu et al., 2019; Thoma et al., 2022; Yamashita et al., 2016; Yoshikawa et al., 2021; J. Zhu et al., 2020), followed by rs10264272, in two (Hamadeh et al., 2019; Pasternak et al., 2022). A detailed description of all polymorphisms studied in each of the articles is available in Supplementary Table S4.
The results of some studies point to a significant impact of the CYP3A5*3 variant (rs776746) on the pharmacokinetics of TAC. Higher median TAC levels for the homozygous variant group of patients were observed by (Khaled et al., 2016; Seligson et al., 2024; Suetsugu et al., 2019). In addition, higher C/D ratios in the variant group were reported by (Khaled et al., 2016; Pasternak et al., 2022; Yoshikawa et al., 2021). Finally, a higher prevalence of supratherapeutic plasma levels in variant homozygotes was identified by (Khaled et al., 2016; Suetsugu et al., 2019). The details of the main results in each of the studies are presented in Table 4.

Table 4. Effect of CYP3A5, CYP3A4 and ABCB1 polymorphisms on pharmacokinetics and clinical outcomes.
Regarding clinical outcomes, two studies suggest the influence of polymorphisms on the incidence of acute GVHD. Khaled et al. (2016) reported a higher incidence of acute GVHD (grades II-IV) in the wild-type group (*1/*1) compared to homozygous variant (*3/*3) patients. Similarly, Yamashita et al. (2016) observed a higher incidence of severe acute GVHD (grades III-IV) in patients in the wild-type group (*1/*1) compared to the homozygous variant (*3/*3) group. On the other hand, four studies (Ho et al., 2024; Seligson et al., 2024; Thoma et al., 2022; J. Zhu et al., 2020) did not identify statistically significant association between the incidence of acute GVHD and polymorphisms.
Regarding the incidence of AKI, homozygous variant genotypes (*3/*3) were associated with a higher frequency, as demonstrated by Yamashita et al. (2016), Seligson et al. (2024). In contrast, four studies (Ho et al., 2024; Khaled et al., 2016; Suetsugu et al., 2019; Zhu et al., 2020) did not identify a statistically significant association between the incidence of AKI and polymorphisms.
3.5 Polymorphisms in the CYP3A4 gene
Four distinct polymorphisms were evaluated in 45% (5/11) of the studies in this review (Hamadeh et al., 2019; Ho et al., 2024; Khaled et al., 2016; Pasternak et al., 2022; Zhu et al., 2020). With citation in five different studies (Hamadeh et al., 2019; Ho et al., 2024; Khaled et al., 2016; Seligson et al., 2024; Zhu et al., 2020) rs35599367 was the most studied, followed by rs2740574 with four (Hamadeh et al., 2019; Ho et al., 2024; Pasternak et al., 2022; Seligson et al., 2024).
Differences in median plasma levels of TAC were observed in two studies. Hamadeh et al. (2019) demonstrated higher concentrations for the CYP3A4 IM/NM phenotype and Zhu et al. (2020) demonstrated higher concentrations for CYP3A4*1/*1B. In contrast, (Khaled et al., 2016; Ho et al., 2024) did not find differences between the groups according to the phenotype. Regarding the optimal therapeutic index of TAC, Hamadeh et al. (2019) demonstrated a higher prevalence of supratherapeutic plasma concentrations of TAC in patients with CYP3A4 IM and NM phenotype. On the other hand, Zhu et al. (2020) demonstrated a lower risk of subtherapeutic contractions for the group of patients with CYP3A4 *1/*1 phenotype.
Regarding the C/D ratio, Zhu et al. (2020) observed that the highest TAC ratio was in the CYP3A4 *1/*1 group, followed by the CYP3A4*1/*1B and CYP3A4*1B/*1B groups. Pasternak et al. (2022), in turn, demonstrated a higher ratio for the CYP3A4 NM phenotype in relation to CYP3A4 RM. In this case, no differences were observed between the CYP3A4 NM and CYP3A4 PM groups. Finally, in the study by Khaled et al. (2016), no significant differences were demonstrated in the C/D ratio.
The influence of polymorphisms in CYP3A4 on clinical outcomes was evaluated in four studies: AKI in four studies (Hamadeh et al., 2019; Ho et al., 2024; Khaled et al., 2016; Zhu et al., 2020), GVHD in three studies (Ho et al., 2024; Khaled et al., 2016; Suetsugu et al., 2019), TMA in one study (Khaled et al., 2016) and OS, RFS and NRM in one study (Ho et al., 2024). In all the studies reviewed, no statistically significant difference was identified between the groups of different genotypes/phenotypes regarding the occurrence of any of the outcomes mentioned above.
3.6 Polymorphisms in the ABCB1 gene
Nine different polymorphisms for the ABCB1 gene were evaluated in 63% (7/11) of the studies (Hamadeh et al., 2019; Ho et al., 2024; Khaled et al., 2016; Laverdière et al., 2015; Pasternak et al., 2022; Seligson et al., 2024; Zhu et al., 2020). The three most studied polymorphisms, each with five citations, were rs1045642 and rs1128503, both reported in studies (Hamadeh et al., 2019; Ho et al., 2024; Khaled et al., 2016; Seligson et al., 2024; Suetsugu et al., 2019; Zhu et al., 2020), and rs2032582, reported in studies (Hamadeh et al., 2019; Khaled et al., 2016; Pasternak et al., 2022; Seligson et al., 2024; Zhu et al., 2020). The other six polymorphisms had only one citation.
Among the studies included in this review, only Laverdière et al., 2015 used the CNI CSP for GVHD prophylaxis. They identified that wild-type genotypes for the rs4148732 and rs6950978 polymorphisms of the ABCB1 gene are associated with a lower competitive risk of death before the development of acute GVHD. However, none of the polymorphisms evaluated increased the incidence of grade II-IV or III-IV acute GVHD. Other studies (Ho et al., 2024; Khaled et al., 2016) that evaluated the risk of GVHD corroborate the lack of influence of polymorphisms in ABCB1 on the incidence of the disease.
Regarding TAC plasma levels, Khaled et al. (2016) pointed out that the genotype (heterozygous) of rs1128503 is associated with higher levels, while Hamadeh et al. (2019) demonstrated that the heterozygous or homozygous variant genotypes in rs2032582 also result in higher plasma concentrations. Zhu et al. (2020), on the other hand, demonstrated an association of the wild-type (CC) genotype in the rs1128503 and rs2032582 polymorphisms with a higher probability of subtherapeutic plasma concentrations of TAC. Despite this finding, other studies indicate the absence of significant associations between ABCB1 gene polymorphisms and plasma levels (Ho et al., 2024; Khaled et al., 2016; Seligson et al., 2024), C/D ratio (Khaled et al., 2016; Pasternak et al., 2022).
Finally, regarding the clinical outcomes evaluated in the studies, AKI (Khaled et al., 2016; Seligson et al., 2024; Zhu et al., 2020), TMA (Khaled et al., 2016) or OS, RFS and NRM (Ho et al., 2024) were not influenced by ABCB1 polymorphisms. Only the study by Hamadeh et al. (2019) highlighted that carriers of homozygous variant genotypes for rs2032582 have a higher risk of toxicity associated with the use of TAC.
4 Discussion
This is the first systematic review to investigate the influence of genetic polymorphisms on the pharmacokinetics and/or outcomes of CNIs (TAC and CSA), especially in HCT recipients. Eleven studies were included, mostly retrospective and conducted in the USA, with the majority focusing on TAC, and only two addressing CSA. We highlight the significant impact of the CYP3A5 rs776746 polymorphism on the pharmacokinetics of TAC, such as TAC levels, C/D ratio or therapeutic index, and on clinical outcomes, such as AKI and GVHD. In contrast, polymorphisms in CYP3A4 and ABCB1 showed less consistent results, evidencing a variability in the impact of these genes on pharmacokinetic and clinical parameters.
Previous research on the pharmacogenetics of CNIs has predominantly concentrated on solid organ transplantation populations (Hesselink, 2003; Kreutz et al., 2004; Sun et al., 2017; Zhu et al., 2011). However, the pharmacokinetic dynamics of these drugs in HCT differ substantially from those in solid organ transplant settings, leading to distinct clinical consequences. For example, the effects of GVHD (Przepiorka et al., 1999) and graft-versus-leukemia (GVL) (Arcuri et al., 2022; Kolb, 2008; Sweeney and Vyas, 2019) highlight the complex interplay between plasma drug levels and therapeutic outcomes in HCT recipients.
Regarding the characteristics of the population and transplantation, our study showed a predominance of TAC use compared to CSP. Only two studies (Laverdière et al., 2015; Thoma et al., 2022) reported the use of CSP for GVHD prophylaxis. Currently, there are no specific recommendations in the guidelines (Funke et al., 2023; Penack et al., 2020; Penack et al., 2024) of societies regarding the choice between CNIs. This finding highlights the importance of future studies investigating the use of CSP for GVHD prophylaxis, aiming to evaluate its impact and expand the available evidence.
The studies included in this review that investigated polymorphisms in the CYP3A5 gene unanimously demonstrated the influence of these polymorphisms on pharmacokinetics and/or clinical outcome mainly related to TAC. The pharmacokinetic alterations were drug level (Khaled et al., 2016; Seligson et al., 2024; Thoma et al., 2022; Yamashita et al., 2016; J. Zhu et al., 2020), C/D ratio (Khaled et al., 2016; Pasternak et al., 2022; Suetsugu et al., 2019; Yoshikawa et al., 2021), and therapeutic index (Hamadeh et al., 2019; Ho et al., 2024; Thoma et al., 2022; Zhu et al., 2020). The main polymorphism associated with the alterations was CYP3A5*3 (rs776746). However, three studies considered another phenotypic classification in addition to CYP3A5*3: (Pasternak et al., 2022) used CYP3A5*3 and CYP3A5*6, and (Hamadeh et al., 2019; Ho et al., 2024) used CYP3A5*3, CYP3A5*6 and CYP3A53*7 to classify HCT recipient.
The variant alleles of CYP3A5 (*3, *6, or *7) may result in a truncated messenger RNA with loss of expression of the functional protein in homozygotes or heterozygotes or encode a nonfunctional protein (Kuehl et al., 2001). Consequently, with a nonfunctional protein, more drugs would accumulate in the body, increasing drug levels, C/D ratio, and increased toxicities. The studies by Yamashita et al. (2016), Seligson et al. (2024) demonstrated an increase in AKI in non-expressing recipient HCT when compared to expressers. On the other hand, patients classified as expressers, with an efficient performance in drug biotransformation, may contribute to lower plasma levels. The studies by Khaled et al. (2016), Yamashita et al. (2016) demonstrated a higher incidence of acute GVHD in the CYP3A5*1 expresser group when compared to the CYP3A5*3 non-expresser group.
Regarding CYP3A4 gene polymorphisms, among the five studies analyzed, three demonstrated the influence of these polymorphisms on the pharmacokinetics of TAC. The associations were in relation to drug level, therapeutic index (Hamadeh et al., 2019; Zhu et al., 2020) and C/D ratio (Pasternak et al., 2022; Zhu et al., 2020). Of these three studies, (Pasternak et al., 2022; Hamadeh et al., 2019) used the phenotypic classification of the groups CYP3A4*1B and CYP3A4*22, while Zhu et al. (2020) evaluated the genotypes of each polymorphism separately. None of the studies that evaluated polymorphisms in CYP3A4 found associations with any clinical outcome. A possible explanation for this finding is the fact that CYP3A4 plays a supporting role in the biotransformation of TAC (Barbarino et al., 2013). Therefore, a reduction in the expression of this enzyme would not be able to cause the same impact as non-expressers of CYP3A5.
Regarding polymorphisms of the ABCB1 gene, of the seven studies that investigated these variants, four identified associations with the pharmacokinetics and/or clinical outcomes of TAC. The alterations c.1236C>T (rs1128503) and c.2677G>A (rs1128503) were the two most cited with associations with drug level (Hamadeh et al., 2019; Khaled et al., 2016), therapeutic index (Hamadeh et al., 2019; Zhu et al., 2020) and/or toxicity (Hamadeh et al., 2019). High levels of TAC were associated with alterations in heterozygosity or homozygosity of both polymorphisms. The polymorphism c.2677G>A (rs1128503) is a non-synonymous SNP, which causes the substitution of the amino acid alanine for serine or threonine at position 893 of P-glycoprotein, reducing the expression of the transport protein (Gréen et al., 2006; Kim, 2001). The c.1236C>T (rs1128503) is a silent polymorphism, and despite not having an amino acid change, changes in mRNA stability, in the amount of translated protein and in the function of the transporter are observed (Kimchi-Sarfaty et al., 2007). The reduction in expression and/or protein with low function could justify the accumulation of the drug in the body and consequently in plasma levels, which would increase the risk of adverse events, which was demonstrated by Hamadeh et al. (2019).
This systematic review has some limitations that should be considered when interpreting the results. The wide variability of outcomes reported in the studies made it impossible to perform a meta-analysis, reducing the ability to integrate the findings quantitatively. In addition, the relatively low number of articles available on the subject, especially those addressing the use of CSP, limits the generalization of the results. The lack of evaluation of polymorphisms in the ABCB1 and CYP3A4 genes in some of the studies limits the interpretations related to these genetic markers. Another limitation refers to the small number of patients in some of the included studies, which reduces the statistical power of the analyses and may compromise the robustness of the findings. The restriction to articles published in Roman characters may have resulted in the exclusion of relevant studies written in non-Roman characters, potentially limiting the comprehensiveness of the review. Finally, the long interval between the search strategy and the conduction of the analyses may have excluded relevant studies published later, impacting the timeliness and comprehensiveness of the data reviewed.
5 Conclusion
Based on the results of this systematic review, we highlight the role of polymorphisms in the CYP3A5 gene, especially CYP3A5*3 (rs776746), as a potential predictive biomarker for pharmacokinetic alterations of TAC in HCT recipients. The studies indicated the influence of this polymorphism on plasma levels, C/D ratio, therapeutic index and, in some cases, clinical outcomes. In contrast, polymorphisms investigated in the CYP3A4 and ABCB1 genes demonstrated a modest impact on the pharmacokinetics of TAC, being evaluated in a limited number of studies, like what occurs with CSP. These limitations suggest the need for new well-designed clinical studies, with adequate sample size, methodology and results described in detail, focused on the investigation of pharmacogenetics.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Author contributions
LC-J: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. DF-A: Conceptualization, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review and editing. AL: Methodology, Writing – original draft, Writing – review and editing. HM: Conceptualization, Formal Analysis, Methodology, Writing – original draft, Writing – review and editing. RT: Writing – original draft, Writing – review and editing. MM: Writing – original draft, Writing – review and editing. MV: Formal Analysis, Investigation, Methodology, Resources, Writing – original draft, Writing – review and editing. TF: Conceptualization, Funding acquisition, Project administration, Resources, Writing – original draft, Writing – review and editing. PS: Conceptualization, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPQ); 001 – Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES); Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP). Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro—FAPERJ, T.S.F. (FAPERJ/E-26/201.218/2022).
Acknowledgments
The authors of this review would like to thank Erinalva da Conceição Batista, librarian at the Faculdade de Medicina da USP, for her support in developing the search strategy, searching the databases and providing training in the use of the Rayyan program.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. During the preparation of this work the author(s) used ChatGPT to improve the readability and language of the manuscript in the English language. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the published article.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2025.1569353/full#supplementary-material
References
Abdel-Kahaar, E., Winter, S., Tremmel, R., Schaeffeler, E., Olbricht, C. J., Wieland, E., et al. (2019). The impact of CYP3A4*22 on tacrolimus pharmacokinetics and outcome in clinical practice at a single kidney transplant center. Front. Genet. 10, 871. doi:10.3389/fgene.2019.00871
Arcuri, L. J., Lerner, D., and Tavares, R. de C. B. da S. (2022). Lower levels of cyclosporine between days 0 and +21 May reduce later relapses without increasing graft-versus-host disease in children and adolescents with acute lymphoblastic leukemia who undergo myeloablative TBI -based allogeneic hematopoietic cell transplantation. Eur. J. Haematol. 109 (2), 182–185. doi:10.1111/ejh.13787
Barbarino, J. M., Staatz, C. E., Venkataramanan, R., Klein, T. E., and Altman, R. B. (2013). PharmGKB summary: cyclosporine and tacrolimus pathways. Pharmacogenetics Genomics 23 (10), 563–585. doi:10.1097/FPC.0b013e328364db84
Birdwell, K., Decker, B., Barbarino, J., Peterson, J., Stein, C., Sadee, W., et al. (2015). Clinical pharmacogenetics implementation consortium (CPIC) guidelines for CYP3A5 genotype and tacrolimus dosing. Clin. Pharmacol. and Ther. 98 (1), 19–24. doi:10.1002/cpt.113
Brunet, M., van Gelder, T., Åsberg, A., Haufroid, V., Hesselink, D. A., Langman, L., et al. (2019). Therapeutic drug monitoring of tacrolimus-personalized therapy: second consensus report. Ther. Drug Monit. 41 (3), 261–307. doi:10.1097/FTD.0000000000000640
da Silva, J. B., de Melo Lima, M. H., and Secoli, S. R. (2014). Influence of cyclosporine on the occurrence of nephrotoxicity after allogeneic hematopoietic stem cell transplantation: a systematic review. Rev. Bras. Hematol. Hemoter. 36 (5), 363–368. doi:10.1016/j.bjhh.2014.03.010
Forsythe, P., and Paterson, S. (2014). Ciclosporin 10 years on: indications and efficacy. Veterinary Rec. 174 (S2), 13–21. doi:10.1136/vr.102484
Funke, V., Rodrigues-Moreira, M. C., Vaz de Macedo, A., Melo, A., Schmidt Filho, J., Fatobene, G. B. S., et al. (2023). VI consensus of the Brazilian society of bone marrow transplantation (SBTMO) - Consensus on graft-versus-host disease (GVHD). J. BONE MARROW Transplant. Cell. Ther. 4 (1), 188. doi:10.46765/2675-374X.2023v4n1p188
Gréen, H., Söderkvist, P., Rosenberg, P., Horvath, G., and Peterson, C. (2006). mdr-1 single nucleotide polymorphisms in ovarian cancer tissue: G2677T/A correlates with response to paclitaxel chemotherapy. Clin. Cancer Res. 12 (3), 854–859. doi:10.1158/1078-0432.CCR-05-0950
Hamadeh, I. S., Zhang, Q., Steuerwald, N., Hamilton, A., Druhan, L. J., McSwain, M., et al. (2019). Effect of CYP3A4, CYP3A5, and ABCB1 polymorphisms on intravenous tacrolimus exposure and adverse events in adult allogeneic stem cell transplant patients. Biol. Blood Marrow Transplant. 25 (4), 656–663. doi:10.1016/j.bbmt.2018.12.766
Hesselink, D., van Schaik, R. H. N., van der Heiden, I. P., van der Werf, M., Gregoor, P. J. H. S., Lindemans, J., et al. (2003). Genetic polymorphisms of the CYP3A4, CYP3A5, and MDR-1 genes and pharmacokinetics of the calcineurin inhibitors cyclosporine and tacrolimus. Clin. Pharmacol. and Ther. 74 (3), 245–254. doi:10.1016/S0009-9236(03)00168-1
Ho, T. T., Perkins, J. B., Gonzalez, R., Hicks, J. K., Martinez, R. A., Duranceau, K., et al. (2024). Association between CYP3A4, CYP3A5 and ABCB1 genotype and tacrolimus treatment outcomes among allogeneic HSCT patients. Pharmacogenomics 25 (1), 29–40. doi:10.2217/pgs-2023-0204
Hu, R., Barratt, D. T., Coller, J. K., Sallustio, B. C., and Somogyi, A. A. (2018). CYP3A5*3 and ABCB1 61A>G significantly influence dose-adjusted trough blood tacrolimus concentrations in the first three months post-kidney transplantation. Basic and Clin. Pharmacol. and Toxicol. 123 (3), 320–326. doi:10.1111/bcpt.13016
Iwasaki, K. (2007). Metabolism of tacrolimus (FK506) and recent topics in clinical pharmacokinetics. Drug Metabolism Pharmacokinet. 22 (5), 328–335. doi:10.2133/dmpk.22.328
Khaled, S. K., Palmer, J. M., Herzog, J., Stiller, T., Tsai, N.-C., Senitzer, D., et al. (2016). Influence of absorption, distribution, metabolism, and excretion genomic variants on tacrolimus/sirolimus blood levels and graft-versus-host disease after allogeneic hematopoietic cell transplantation. Biol. Blood Marrow Transplant. 22 (2), 268–276. doi:10.1016/j.bbmt.2015.08.027
Khan, A. R., Raza, A., Firasat, S., and Abid, A. (2020). CYP3A5 gene polymorphisms and their impact on dosage and trough concentration of tacrolimus among kidney transplant patients: a systematic review and meta-analysis. Pharmacogenomics J. 20 (4), 553–562. doi:10.1038/s41397-019-0144-7
Kim, R., Leake, B. F., Choo, E. F., Dresser, G. K., Kubba, S. V., Schwarz, U. I., et al. (2001). Identification of functionally variant MDR1 alleles among European Americans and African Americans. Clin. Pharmacol. and Ther. 70 (2), 189–199. doi:10.1067/mcp.2001.117412
Kimchi-Sarfaty, C., Oh, J. M., Kim, I.-W., Sauna, Z. E., Calcagno, A. M., Ambudkar, S. V., et al. (2007). A “silent” polymorphism in the MDR 1 gene changes substrate specificity. Science 315 (5811), 525–528. doi:10.1126/science.1135308
Kolb, H.-J. (2008). Graft-versus-leukemia effects of transplantation and donor lymphocytes. Blood 112 (12), 4371–4383. doi:10.1182/blood-2008-03-077974
Kong, Q., Gao, N., Wang, Y., Hu, G., Qian, J., and Chen, B. (2023). Functional evaluation of cyclosporine metabolism by CYP3A4 variants and potential drug interactions. Front. Pharmacol. 13, 1044817. doi:10.3389/fphar.2022.1044817
Kreutz, R., Zürcher, H., Kain, S., Martus, P., Offermann, G., and Beige, J. (2004). The effect of variable CYP3A5 expression on cyclosporine dosing, blood pressure and long-term graft survival in renal transplant patients. Pharmacogenetics 14 (10), 665–671. doi:10.1097/00008571-200410000-00004
Kuehl, P., Zhang, J., Lin, Y., Lamba, J., Assem, M., Schuetz, J., et al. (2001). Sequence diversity in CYP3A promoters and characterization of the genetic basis of polymorphic CYP3A5 expression. Nat. Genet. 27 (4), 383–391. doi:10.1038/86882
Laverdière, I., Guillemette, C., Tamouza, R., Loiseau, P., de Latour, R. P., Robin, M., et al. (2015). Cyclosporine and methotrexate-related pharmacogenomic predictors of acute graft-versus-host disease. Haematologica 100 (2), 275–283. doi:10.3324/haematol.2014.109884
Lee, J., Wang, R., Yang, Y., Lu, X., Zhang, X., Wang, L., et al. (2015). The effect of ABCB 1 C 3435 T polymorphism on cyclosporine dose requirements in kidney transplant recipients: a meta-analysis. Basic and Clin. Pharmacol. and Toxicol. 117 (2), 117–125. doi:10.1111/bcpt.12371
Lee, S. J., and Flowers, M. E. D. (2008). Recognizing and managing chronic graft-versus-host disease. Hematology 2008 (1), 134–141. doi:10.1182/asheducation-2008.1.134
Little, J., Higgins, J. P. T., Ioannidis, J. P. A., Moher, D., Gagnon, F., von Elm, E., et al. (2009). STrengthening the REporting of genetic association studies (STREGA)—An extension of the STROBE statement. Genet. Epidemiol. 33 (7), 581–598. doi:10.1002/gepi.20410
Malard, F., Holler, E., Sandmaier, B. M., Huang, H., and Mohty, M. (2023). Acute graft-versus-host disease. Nat. Rev. Dis. Prim. 9 (1), 27. doi:10.1038/s41572-023-00438-1
Oetting, W. S., Wu, B., Schladt, D. P., Guan, W., Remmel, R. P., Dorr, C., et al. (2018). Attempted validation of 44 reported SNPs associated with tacrolimus troughs in a cohort of kidney allograft recipients. Pharmacogenomics 19 (3), 175–184. doi:10.2217/pgs-2017-0187
Ouzzani, M., Hammady, H., Fedorowicz, Z., and Elmagarmid, A. (2016). Rayyan—A web and Mobile app for systematic reviews. Syst. Rev. 5 (1), 210. doi:10.1186/s13643-016-0384-4
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ n71, n71. doi:10.1136/bmj.n71
Pasternak, A. L., Marcath, L. A., Li, Y., Nguyen, V., Gersch, C. L., Rae, J. M., et al. (2022). Impact of pharmacogenetics on intravenous tacrolimus exposure and conversions to oral therapy. Transplant. Cell. Ther. 28 (1), 19.e1–19.e7. doi:10.1016/j.jtct.2021.09.011
Penack, O., Marchetti, M., Aljurf, M., Arat, M., Bonifazi, F., Duarte, R. F., et al. (2024). Prophylaxis and management of graft-versus-host disease after stem-cell transplantation for haematological malignancies: updated consensus recommendations of the european society for blood and marrow transplantation. Lancet Haematol. 11 (2), e147–e159. doi:10.1016/S2352-3026(23)00342-3
Penack, O., Marchetti, M., Ruutu, T., Aljurf, M., Bacigalupo, A., Bonifazi, F., et al. (2020). Prophylaxis and management of graft versus host disease after stem-cell transplantation for haematological malignancies: updated consensus recommendations of the european society for blood and marrow transplantation. Lancet Haematol. 7 (2), e157–e167. doi:10.1016/S2352-3026(19)30256-X
Przepiorka, D., Petropoulos, D., Mullen, C., Danielson, M., Mattewada, V., and Chan, K.-W. (1999). Tacrolimus for prevention of graft-versus-host disease after mismatched unrelated donor cord blood transplantation. Bone Marrow Transplant. 23 (12), 1291–1295. doi:10.1038/sj.bmt.1701807
Ram, R., Storer, B., Mielcarek, M., Sandmaier, B. M., Maloney, D. G., Martin, P. J., et al. (2012). Association between calcineurin inhibitor blood concentrations and outcomes after allogeneic hematopoietic cell transplantation. Biol. Blood Marrow Transplant. 18 (3), 414–422. doi:10.1016/j.bbmt.2011.08.016
Rotarescu, C. A., Maruntelu, I., Rotarescu, I., Constantinescu, A.-E., and Constantinescu, I. (2024). Analysis of ABCB1 gene polymorphisms and their impact on tacrolimus blood levels in kidney transplant recipients. Int. J. Mol. Sci. 25 (20), 10999. doi:10.3390/ijms252010999
Seligson, N. D., Zhang, X., Zemanek, M. C., Johnson, J. A., VanGundy, Z., Wang, D., et al. (2024). CYP3A5 influences oral tacrolimus pharmacokinetics and timing of acute kidney injury following allogeneic hematopoietic stem cell transplantation. Front. Pharmacol. 14, 1334440. doi:10.3389/fphar.2023.1334440
Storb, R., Deeg, H., Pepe, M., Appelbaum, F., Anasetti, C., Beatty, P., et al. (1989). Methotrexate and cyclosporine versus cyclosporine alone for prophylaxis of graft-versus-host disease in patients given HLA-Identical marrow grafts for leukemia: long-term follow-up of a controlled trial. Blood 73 (6), 1729–1734. doi:10.1182/blood.V73.6.1729.1729
Storb, R., Deeg, H. J., Whitehead, J., Appelbaum, F., Beatty, P., Bensinger, W., et al. (1986). Methotrexate and cyclosporine compared with cyclosporine alone for prophylaxis of acute graft versus host disease after marrow transplantation for leukemia. N. Engl. J. Med. 314 (12), 729–735. doi:10.1056/NEJM198603203141201
Suetsugu, K., Mori, Y., Yamamoto, N., Shigematsu, T., Miyamoto, T., Egashira, N., et al. (2019). Impact of CYP3A5, POR, and CYP2C19 polymorphisms on trough concentration to dose ratio of tacrolimus in allogeneic hematopoietic stem cell transplantation. Int. J. Mol. Sci. 20 (10), 2413. doi:10.3390/ijms20102413
Sun, B., Guo, Y., Gao, J., Shi, W., Fan, G., Li, X., et al. (2017). Influence of CYP3A and ABCB1 polymorphisms on cyclosporine concentrations in renal transplant recipients. Pharmacogenomics 18 (16), 1503–1513. doi:10.2217/pgs-2017-0127
Sweeney, C., and Vyas, P. (2019). The graft-versus-leukemia effect in AML. Front. Oncol. 9, 1217. doi:10.3389/fonc.2019.01217
Thoma, M., Langer, K., McLean, P., and Dingli, D. (2022). The impact of pharmacogenomic CYP3A5 variants on calcineurin inhibitor metabolism and SLCO1B1 variants on methotrexate in adult allogeneic BMT patients. Transplant. Rep. 7 (4), 100115. doi:10.1016/j.tpr.2022.100115
Wang, C., Lu, K.-P., Chang, Z., Guo, M.-L., and Qiao, H.-L. (2018). Association of CYP3A4*1B genotype with cyclosporin A pharmacokinetics in renal transplant recipients: A meta-analysis. Gene 664, 44–49. doi:10.1016/j.gene.2018.04.043
Wells, G. A., Shea, B., O’Connell, D., Peterson, J., Welch, V., and Losos, M. (2024). The Newcastle-Ottawa scale (NOS) for assessing the quality if nonrandomized studies in meta-analyses. Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm. (Accessed 24, November, 2024)
Yamashita, T., Fujishima, N., Miura, M., Niioka, T., Abumiya, M., Shinohara, Y., et al. (2016). Effects of CYP3A5 polymorphism on the pharmacokinetics of a once-daily modified-release tacrolimus formulation and acute kidney injury in hematopoietic stem cell transplantation. Cancer Chemother. Pharmacol. 78 (1), 111–118. doi:10.1007/s00280-016-3060-4
Yee, G. C., Self, S. G., McGuire, T. R., Carlin, J., Sanders, J. E., and Deeg, H. J. (1988). Serum cyclosporine concentration and risk of acute graft-versus-host disease after allogeneic marrow transplantation. N. Engl. J. Med. 319 (2), 65–70. doi:10.1056/NEJM198807143190201
Yoshikawa, N., Takeshima, H., Sekine, M., Akizuki, K., Hidaka, T., Shimoda, K., et al. (2021). Relationship between CYP3A5 polymorphism and tacrolimus blood concentration changes in allogeneic hematopoietic stem cell transplant recipients during continuous infusion. Pharmaceuticals 14 (4), 353. doi:10.3390/ph14040353
Zhang, H. J., Li, D. Y., Zhu, H. J., Fang, Y., and Liu, T. S. (2017). Tacrolimus population pharmacokinetics according to CYP3A5 genotype and clinical factors in Chinese adult kidney transplant recipients. J. Clin. Pharm. Ther. 42 (4), 425–432. doi:10.1111/jcpt.12523
Zhu, H. J., Yuan, S. H., Fang, Y., Sun, X. Z., Kong, H., and Ge, W. H. (2011). The effect of CYP3A5 polymorphism on dose-adjusted cyclosporine concentration in renal transplant recipients: a meta-analysis. Pharmacogenomics J. 11 (3), 237–246. doi:10.1038/tpj.2010.26
Keywords: CYP3A5, CYP3A4, ABCB1, calcineurin inhibitors, hematopoietic cell transplantation
Citation: Costa-Junior LCd, Freitas-Alves DR, Leão AML, Monteiro HdAV, Tavares RdCBdS, Moreira MCR, Visacri MB, Fernandez TdS and Santos PCJdL (2025) Polymorphisms in CYP3A5, CYP3A4, and ABCB1 genes: implications for calcineurin inhibitors therapy in hematopoietic cell transplantation recipients—a systematic review. Front. Pharmacol. 16:1569353. doi: 10.3389/fphar.2025.1569353
Received: 31 January 2025; Accepted: 20 June 2025;
Published: 16 July 2025.
Edited by:
Claudia Pisanu, University of Cagliari, ItalyReviewed by:
Umamaheswaran Gurusamy, Abigail Wexner Research Institute, United StatesHaihong Bai, Capital Medical University, China
Stefania Braidotti, Institute for Maternal and Child Health Burlo Garofolo (IRCCS), Italy
Copyright © 2025 Costa-Junior, Freitas-Alves, Leão, Monteiro, Tavares, Moreira, Visacri, Fernandez and Santos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paulo Caleb Júnior de Lima Santos, cGF1bG8uY2FsZWJAdW5pZmVzcC5icg==; Teresa de Souza Fernandez, dGVyZXNhZmVybmFuZGV6QGluY2EuZ292LmJy