 Roberta Dochnal1*
Roberta Dochnal1* Ágnes Vetró1
Ágnes Vetró1 Enikö Kiss1Ildikó Baji1
Enikö Kiss1Ildikó Baji1 Eszter Lefkovics1
Eszter Lefkovics1 Lauren M. Bylsma2
Lauren M. Bylsma2 Ilya Yaroslavsky3Jonathan Rottenberg4Maria Kovacs2
Ilya Yaroslavsky3Jonathan Rottenberg4Maria Kovacs2 Krisztina Kapornai1
Krisztina Kapornai1- 1Department of Child and Adolescent Psychiatry, Pediatrics and Child Health Center, University of Szeged, Szeged, Hungary
- 2Department of Psychiatry, School of Medicine, University of Pittsburgh, Pittsburgh, PA, United States
- 3Department of Psychology, Cleveland State University, Cleveland, OH, United States
- 4Department of Psychology, University of South Florida, Tampa, FL, United States
Background: Both depression and anxiety (two of the most common internalizing psychopathologies among youths) are associated with difficulties in emotion regulation (ER). Little is known about whether anxiety as a comorbid condition has an effect on the habitual use of different ER strategies in youngsters with depression histories. We aimed 1) to compare ER in adolescents with histories of childhood onset major depressive disorder (MDD) with and without comorbid anxiety and 2) to examine whether certain ER response clusters (Cognitive, Social, and Behavioral/Physical) characterize comorbid children and adolescents.
Methods: We analyzed data on 217 youth (11–18 years old) with depression history: 85 subjects with lifetime anxiety comorbidity (comorbid group) and 132 without lifetime anxiety (non-comorbid group). Psychiatric diagnosis was established by a comprehensive Diagnostic and Statistical Manual of Mental Disorders (DSM) IV-based diagnostic procedure. ER strategies were examined via the self-rated “Feelings and Me” Child version questionnaire (FAM-C).
Results: The comorbid group used maladaptive ER strategies significantly more frequently than the non-comorbid youngsters. The Behavioral/Physical and Social ER skills, especially those reflecting social withdrawal and self-harm, were responsible for the higher maladaptive scores.
Limitations: Because our study is a cross-sectional analysis, we have no information about the development or the onset of maladaptive ER strategies. Therefore, we were unable to examine whether maladaptive ER was a risk factor or a consequence of the internalizing psychopathology and comorbidity.
Conclusions: Comorbid anxiety worsens the impaired use of ER strategies in depression-prone youths. Further longitudinal research is needed to explore the causal role of dysfunctional ER in the development of internalizing psychopathology.
Introduction
The ability to regulate emotions and attenuate negative emotions is considered fundamental to healthy child development and functioning (1, 2). The concept and development of emotion regulation (ER) have been extensively discussed by several authors (1–6). According to Cole et al. (4), ER consists of several cognitive, behavioral, and social self-regulatory responses that can change the activated emotion by modulating its valence, intensity, or time course. Appropriate adaptive ER strategies (e.g., distraction, cognitive reappraisal, and seeking interpersonal support) attenuate dysphoria and facilitate functioning (7–9), while maladaptive responses (e.g., rumination and suppression) prolong and exacerbate dysphoria (8, 10). Furthermore, it is established in the literature that poor ER is implicated in most forms of childhood psychopathology; a variety of ER deficits are present in samples of children with internalizing disorders (11).
Depressed youngsters use a greater number of maladaptive mood repair strategies and fewer adaptive ones than do healthy controls (12, 13). The study by Kovacs et al. (8), based on clinical samples, indicates that maladaptive skills are correlated with a worsening of depression symptoms and increase the probability of recurrent depressive episodes. ER difficulties can persist even after depression has remitted. Our research group previously showed that both remitted and currently depressed young adult probands reported a greater number of maladaptive ER responses to sadness than did controls (8). ER difficulties have also been reported in children and adolescents with histories of depression than in healthy controls (13). In addition, younger depressed children (kindergarten to eighth grade) have been found to use maladaptive responses to regulate emotions more frequently than non-depressed children (14).
ER also seems to be impaired in individuals with anxiety symptoms (11, 15). A growing body of literature suggests that anxiety, similar to depression, is associated with the decreased use of adaptive regulation responses and increased use of maladaptive responses, in both youth and adults (e.g., 16–19). For example, Suveg and Zeman (20) found that children with anxiety disorders were less successful in controlling negative emotions than were healthy controls. Anxious children have lower levels of emotional understanding and more difficulty in regulating worry, sadness, and anger (2). According to Carthy et al. (21), children with anxiety disorder have greater negative emotionality and more deficits in using reappraisal in negative emotional situations. Mennin and colleagues (22) found in adult population sample that patients (mean age 19.52 years) with generalized anxiety disorder (GAD) had low self-soothing ability following a negative emotional experience.
Depression and anxiety disorders are the most common comorbid mental disorders. Based on comprehensive epidemiological data, the estimated rate of comorbid anxiety disorders in children and adolescents with depression ranges from 30% to 75% (23, 24). Comorbidity estimates in clinical samples can be as high as 86% (25–27).
Research on the impact of comorbidity of depression and anxiety disorder suggests that patients with comorbidity have greater impairment and symptom severity, more chronic course of illness, and decreased response to treatment relative to patients with these conditions in isolation (28–31). Furthermore, youths with both anxiety and depressive disorders had high risk for suicide attempt (32).
Previous ER research on anxiety and depression comorbid patients focused mainly on maladaptive cognitive skills and the role of ruminative thinking (33, 34). Results showed that patients with comorbidity use maladaptive ER strategies, such as rumination, suppression, and avoidance, more often than do adaptive ones (11, 12, 15, 35). Garnefski and Kraaij (37) investigated an adolescent community sample. Adolescents with symptoms of depression and anxiety used rumination, catastrophizing, other-blame, and self-blame, whereas adolescents with only depression used self-blame and rumination. Adaptive ER strategies (positive reappraisal and refocusing on planning) were inversely related to both depressive and anxiety symptoms, while positive refocusing was inversely related only to depressive symptoms. Garnefsky et al. (38) previously showed that the above maladaptive coping strategies were strongly related to symptoms of depression and anxiety in both adolescents and adults. A study conducted by d’Avanzato and Joormann, (39) in adult population with social anxiety and depression found that a higher level of rumination and a lower level of reappraisal were specific for patients with major depressive disorder (MDD).
The relationship between self-blame and depressive and anxiety symptoms was stronger in adolescents than in adults. Positive reappraisal, an adaptive coping strategy, was less often used by adolescents, indicating that they were less likely than adults to try to add positive meaning to a negative life event (38).
In summary, anxiety and depressive disorders are both associated with abnormalities in the processing and regulation of emotions. Understanding the link between these dysfunctional strategies and the psychopathology of children and adolescents with depression and anxiety may facilitate the development of more efficient prevention and treatment approaches.
The goal of this study was to compare the ER strategies of youngsters with histories of MDD with and without comorbid anxiety disorders. Specifically, we aimed 1) to compare the adaptive and maladaptive ER repertoires of youngsters with histories of MDD with and without comorbid anxiety and 2) to examine whether certain ER response clusters (Cognitive, Social, and Behavioral/Physical) characterize comorbid children and adolescents.
Materials and Methods
This study was approved by the institutional review boards of the University of Pittsburgh, USA, and the University of Szeged, Hungary. Parents provided written informed consent, and youths provided either assent or consent (depending on their ages) before any data were gathered. All procedures, schedules, rating scales, and instruments used in this study were first developed in English, translated to Hungarian, and then retranslated to English by bi-lingual child psychiatrists and clinical psychologists. Original and back-translated versions were compared, and discrepancies were resolved.
Sample
The subjects in our study were selected from a genetic and other risk factor study of childhood onset depression (Program Project Hungarian study) described elsewhere (40). The original study entry criteria were as follows: Diagnostic and Statistical Manual of Mental Disorders (DSM) IV MDD, 7 to 14 years old at initial assessment, no evidence of mental retardation or major systemic medical disorder, availability of at least one biological parent, and having at least one sibling aged 7–18 years.
Children in the cohort were clinical patients at 23 child psychiatry inpatient and outpatient facilities in Hungary at the time of study entry. For the present paper, we analyzed data on 217 children who were invited to participate in the Biobehavioral Inflexibility and Risk for Juvenile-onset Depression study. Their age ranged from 11 to 18 years at the time of assessment.
Measurement
Diagnostic Procedures
The Interview Schedule for Children and Adolescents—Diagnostic Version (ISCA-D) was used for establishing psychiatric diagnoses. ISCA-D is an extension and modification of the Interview Schedule for Children and Adolescents (ISCA) (41). It is a semi-structured interview assessing lifetime psychiatric disorders and current psychiatric status along with the onset and offset dates of each disorder in youths on the basis of DSM-IV (42). Psychiatric diagnoses were evaluated over the subject’s lifetime. The intake interviews were assessed during the original Program Project study and covered the time frame from birth to the time of the interview. The 217 youths who participated in the present study were re-evaluated by the follow-up version of ISCA-D (FU-ISCA-D) to assess their current diagnoses and also their psychiatric histories since the previous interview. Therefore, diagnostic evaluation covers the time from birth to current assessment. All diagnoses, number of episodes, and age at first depressive disorder were also evaluated from birth till the timepoint of the actual assessment. Diagnostic evaluations were carried out by trained child psychiatrists and psychologists who completed 3 months of didactic and practical training in the ISCA-D semi-structured interview technique and rendered best-estimate psychiatric consensus diagnosis. As reported elsewhere, interviewers have achieved satisfactory inter-rater reliability (40, 43, 44).
Self-Rating Scales
Self-rating scales for the present study were administered at the time of Biobehavioral Inflexibility and Risk for Juvenile-onset Depression study, after the FU-ISCA-D interview, on the same day. Interviewers were available to help younger children as needed.
ER strategies were examined via the self-rated “Feelings and Me” Child (FAM-C) version questionnaire, which evaluates the use of responses to depressed, dysphoric mood (13, 44, 45). It is presumed that there is a trait-like characteristic style of the use of the ER response repertoires. Therefore, there is no timeframe for this questionnaire.
The FAM-C is suitable for ages 7–17 and lists a total of 54 depression-relevant mood repair strategies focusing on coping with sadness: 32 strategies that are “adaptive” (i.e., serve to downregulate/regulate sadness, e.g., listen to music) and 22 strategies that are “maladaptive” (i.e., serve to exacerbate sadness, e.g., hit myself). Besides the Total Adaptive and Maladaptive scores, the items reflect three regulatory domains—Behavioral/Physical (24 items), Social-Interpersonal (12 items), and Cognitive (18 items)—with adaptive and maladaptive strategies in each. Each response is scored 0, 1, or 2, corresponding to the choice of “not true,” “sometimes true,” or “often true.” We have previously reported good psychometric properties of this measure across clinical and non-clinical populations (13, 44).
In order to control for depressive symptoms, the Child Depression Inventory (CDI-R) was administered. CDI-R is a 27-item, self-rated, symptom-oriented scale suitable for youths aged 7 to 17, sensitive to changes in depressive symptoms over time, and is a useful index of the severity of the depressive episode. It measures depressive symptoms in the last 2 weeks (46).
Statistical Analysis
We used SPSS Statistics 22.0 package for all the performed statistical analyses.
The percentage of missing data was very low: 0.4% in the whole dataset. By default, SPSS treated missing values as “missing,” and these items were not included in the statistical analyses.
To examine possible differences between groups on baseline characteristics, we used independent t-test for continuous and chi-square test for categorical variables. The general linear model (GLM)-univariate analysis was used to explore the differences in the ER responses between the groups. False discovery rate (Benjamini–Hochberg procedure) was used to control for multiple comparisons.
The dependent variables were Total Adaptive, Total Maladaptive, Adaptive Cognitive, Maladaptive Cognitive, Adaptive Social, Maladaptive Social, Adaptive Behavioral/Physical, and Maladaptive Behavioral/Physical scores as measured by the FAM-C.
The independent variable was group membership. The two groups were youth with any lifetime depression disorder and any lifetime anxiety disorder (comorbid group) and youth with any lifetime depression disorder and no lifetime anxiety disorder (non-comorbid group).
Covariates included CDI-R scores, number of MDD episodes, age, sex, and age of onset of first mood disorder (MDD or dysthymia). Based on the literature, depression severity and ER deficits are directly related (e.g., 8). Severity of depression can be reflected by CDI-R scores, number of MDD episodes, and age of onset of first mood disorder. We included these items as covariates, because these parameters were significantly different between the two groups and thus might have an influence on our hypothesis, namely, the relation between anxiety comorbidity and ER in depressed youths.
Results
Sample Description
Our sample included 217 children (ages: 11–18 years; mean age: 17.01; SD: 1.39; gender distribution: 139 male and 78 female) who had had at least one lifetime MDD episode: 54.8% had one, 30% had two, and 15.2% had three or more MDD episodes. Of the whole sample, 13.4% were currently in depressive episode. The exact pattern of past and current MDD and anxiety episodes in our sample is shown in Figure 1. Patients with bipolar disorder (n = 6) were excluded from the statistical analysis.
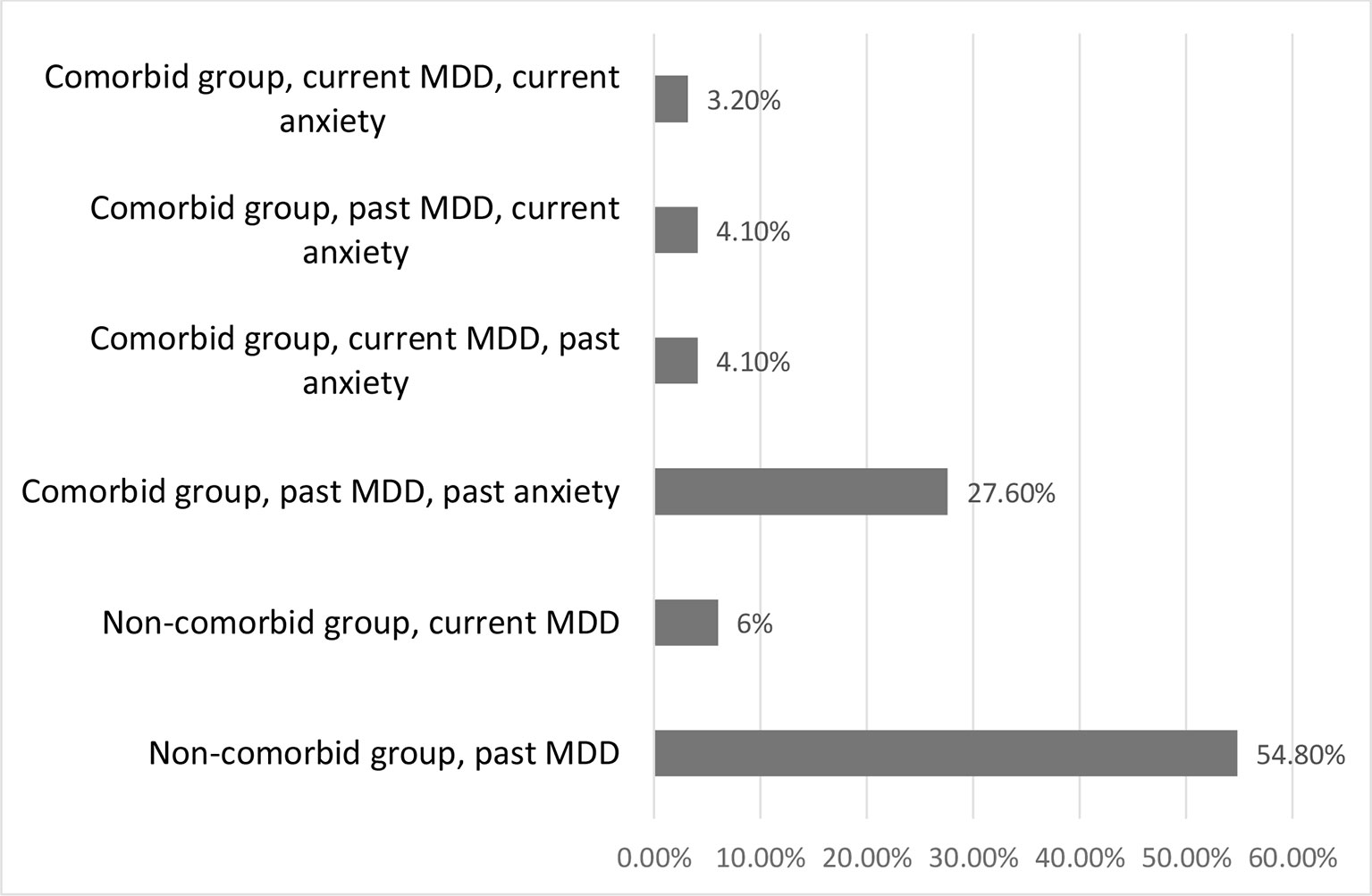
Figure 1 Comorbid vs. non-comorbid groups, compared based on current vs. past diagnoses of major depressive disorder (MDD) and anxiety disorder. MDD, major depressive disorder.
The characteristics of the comorbid and non-comorbid groups are shown in Table 1. The most frequent anxiety disorders in the comorbid group were phobia (33 subjects, 38.82%), GAD (28 subjects, 32.94%), and separation anxiety disorder (25 subjects, 29.41%). Other comorbidities were anxiety not otherwise specified (NOS) (14 subjects, 16.47%), obsessive compulsive disorder (7 subjects, 8.23%), panic disorder (4 subjects, 4.7%), and post-traumatic stress disorder (4 subjects, 4.7%). Of the 85 comorbid patients, 50 subjects had one comorbid anxiety disorder, and 35 subjects had two or more comorbid anxiety disorders.
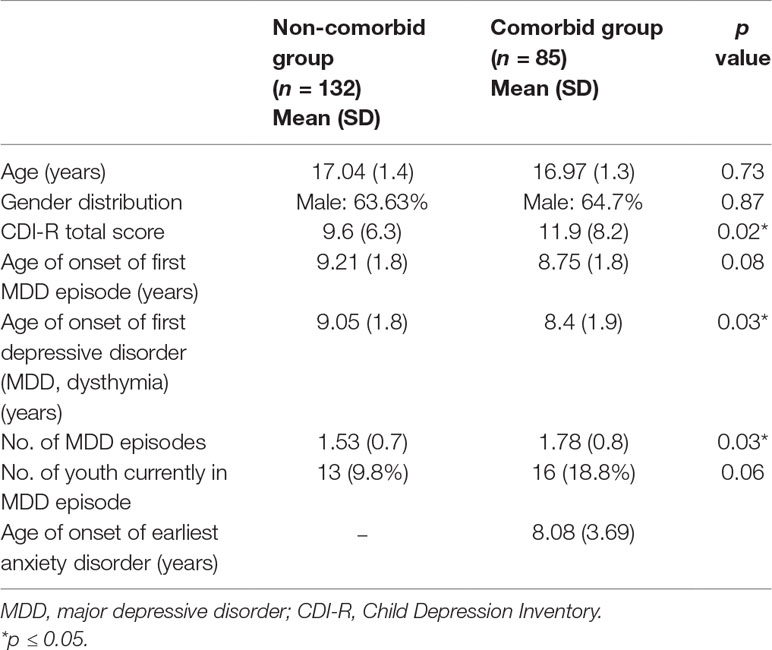
Table 1 Sample description non-comorbid vs. comorbid group.
The two groups did not differ in gender and age distribution, age of onset of first MDD episode, or the number of youths currently in MDD episode. However, the CDI-R scores, age of onset of first mood disorder, and the number of MDD episodes showed statistically significant differences in the two groups. Therefore, we used these variables as covariates in our group analyses (Table 1).
Comparison of Total Adaptive and Maladaptive ER Scores in the Non-Comorbid vs. Comorbid Group
The Total Adaptive score of the FAM-C did not show statistically significant difference between the groups [F(1, 205) = 1.023, p = 0.313, partial η2 = 0.005], while the Total Maladaptive score was significantly higher in the comorbid compared with non-comorbid subjects [F(1, 205) = 5.269, p = 0.023, partial η2 = 0.025].
Comparison of Subscales of Adaptive and Maladaptive ER Strategies in the Non-Comorbid vs. Comorbid Group
We found that none of the Adaptive subscales were significantly different between the groups: Cognitive [F(1, 204) = 0.648, p = 0.422, partial η2 = 0.03], Social [F(1, 204) = 0.287, p = 0.593, partial η2 = 0.001], and Behavioral/Physical [F(1, 202) = 0.699, p = 0.404, partial η2 = 0.003]. However, Maladaptive Social [F(1, 204) = 5.59, p = 0.019, partial η2 = 0.027] and Maladaptive Behavioral/Physical [F(1, 204) = 5.865, p = 0.016, partial η2 = 0.028] subscales were significantly higher in comorbid children (Table 2).

Table 2 FAM-C scores in the non-comorbid group vs. comorbid group
When we looked at specific items of the above-mentioned maladaptive subscales, the item reflecting social withdrawal in the Social subscale and the item reflecting self-harm in the Behavioral/Physical subscale were more frequently used by comorbid youth (data not shown). The Maladaptive Cognitive subscale was not significantly different across groups. However, one of the cognitive items similar to rumination was significantly more frequently endorsed by the patients in the comorbid group (think of being sad) [F(1, 205) = 4.794, p = 0.03, partial η2 = 0.023].
Discussion
The aim of our study was to examine whether anxiety as a comorbid condition was associated with the use of different ER strategies in youngsters with histories of depression. Our study included a large clinical sample of Hungarian children and adolescents with depressive history, of whom about 39% had lifetime comorbid anxiety disorder as well.
Poor regulation of emotions appears to be a factor common to anxiety and depression, but the nature of ER in comorbid patients has not been fully characterized. In fact, there is scant information about how anxiety as a comorbid condition affects the habitual use of different ER strategies in depressed youngsters. Queen and Ehrenreich-May (47) found that adolescents with anxiety and depression had poorer emotional awareness, greater emotional suppression, greater reluctance to express negative emotions, and greater inhibition of sadness than are patients with anxiety disorder. Research by Burklund et al. (48) in adults revealed altered ER in patients with comorbid social phobia and depression. Aldao et al. (12) concluded, also in adults, that maladaptive ER strategies (e.g., rumination and avoidance) had strong associations with psychopathology including depression and anxiety.
The current study extended previous findings in several ways: We examined multiple adaptive and maladaptive ER strategies; we used a large clinical sample of youngsters with childhood onset depression; and our sample was carefully diagnosed by trained psychiatrists and psychologists. We found that anxiety comorbidity in youngsters with lifetime depression was associated with dysfunctional ER, as children with comorbidity used maladaptive ER responses more frequently than non-comorbid peers. Our results are in line with findings from previous studies that showed more frequent use of maladaptive ER strategies in youths with comorbid depression and anxiety symptoms (11, 15, 36, 37, 47). It has been reported that the treatment of depression is more difficult in the presence of anxiety: comorbidity lengthens the duration of treatment and decreases the response to interventions (49, 50). Our results may suggest one possible explanation: Specifically depressed youngsters with anxiety comorbidity use maladaptive ER responses to sadness even more frequently than their non comorbid peers, which is likely to worsen their dysphoria. Even though the comorbid group used maladaptive (total, behavioral, and social) responses more frequently, the effect sizes were low. This suggests that anxiety comorbidity is attributed only to a small proportion of variance in maladaptive ER strategies in youths with lifetime depression. One explanation could be that we examined the discriminating effect of anxiety comorbidity on ER domains within a depressed sample. Our results show a different style of maladaptive ER strategies in children and adolescents with lifetime anxiety and depression than in youngsters with only depression, namely, that cognitive maladaptive strategies are used to the same extent whereas social and behavioral maladaptive ER strategies are used more often in the comorbid group.
We found in our clinical sample that the presence or absence of anxiety comorbidity in patients with depression histories made no significant difference to these two groups’ use of adaptive ER responses. Our results are in line with those of Aldao et al. (12), whose meta-analysis found that adaptive ER strategies were less associated with psychopathology, including depression or anxiety, than were maladaptive ones. Therefore, patients with comorbidity may not derive benefits from expanding their repertoires of adaptive ER responses.
Our study can also serve to augment existing data on the possible role of dysfunctional ER in internalizing psychopathology. In our study of youths diagnosed with lifetime comorbid depression and anxiety, we examined not only their cognitive strategies but also their coping strategies in the social and behavioral domains. When comparing ER response clusters, we found that youths with comorbid anxiety and depression were more likely to use maladaptive social and behavioral/physical responses than were their depressed peers without anxiety. Social withdrawal (“hide from people”) within the Social domain can be considered as social avoidant strategy consistent with the nature of anxiety. As reported by Schafer et al. (11), avoidant behavior was associated with depressive and anxiety symptoms. While avoiding social situations to cope with sadness might reduce negative emotion in the short term, however, it also prevents children from using social support to attenuate sadness. Self-harm or autoaggression (e.g., “hit myself”) within the behavioral/physical domain can be interpreted as negative somatic sensitivity response. The utilization of these negative, emotion-driven somatic, sensory-focused responses may indicate a lack of more sophisticated regulatory strategies, which can be potentially harmful. It is also possible that anxiety, as one of the earliest forms of childhood psychopathology, might itself predispose individuals to more somatically based and sensory-oriented ER responses. This might be the subject of further research.
Finally, these findings suggest that patients with comorbid depression and anxiety may benefit from psychotherapeutic methods that aim to replace maladaptive ER responses with adaptive ones (51, 52, 53). One effective psychotherapy is dialectical behavioral therapy (DBT), which aims to improve ER by teaching several ER skills (e.g., emotion identification, increasing positive emotional events, taking opposite action, and distress tolerance techniques) (54). Promising results have been reported regarding the development (55, 56, 57) and effectiveness of transdiagnostic-behavioral therapy for children and adolescents with comorbid depression and anxiety (symptoms or disorder) (58). In the light of our results, the module of modifying maladaptive emotion-driven behaviors of transdiagnostic behavioral therapy could be especially beneficial for depressed children and adolescents with anxiety comorbidity (59).
Limitations
Limitations of this research should also be mentioned. Since our study was cross-sectional, it was not possible to examine the causal relationship among the internalizing disorders and ER. We did not have enough subjects in current MDD and anxiety episodes in order to stratify our groups according to present or past diagnoses.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
This study was carried out in accordance with the recommendations of Federalwide Assurance for the Protection of Human Subjects with written informed consent from all subjects. All subjects gave written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by the Institutional Review Board (IRB number: IRB00003344) and Medical Research Council (ETT TUKEB, nr: 444-0/2010-1018eku).
Author Contributions
MK, KK, ÁV, EK, and IB conceptualized and received funding for the study. MK, KK, ÁV, EK, IB, EL, LB, IY, and JR planned and executed the study protocol. RD, KK, ÁV, EK, and IB contributed to data analysis and writing of the manuscript. RD, MK, KK, ÁV, EK, and IB assisted with the analysis of the data and contributed to the final draft of the manuscript.
Funding
This study was supported by NIH Grant MH084938-01 and by Hungarian Scientific Research Fund Grant NN85285.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationship that could be construed as a potential conflict of interest.
Acknowledgments
We are extremely grateful to all the families who took part in the study, to our colleagues for their help in recruiting them, and to the whole research study team, including interviewers, computer and laboratory technicians, administrators, and nurses.
References
1. Gross JJ, Thompson RA. Emotion regulation: conceptual foundations. In: Gross JJ, editor. Handbook of emotion regulation. The Guilford Press (2007). p. 3–24.
2. Zeman J, Cassano M, Perry-Parrish C, Stegall S. Emotion regulation in children and adolescents. J Dev Behav Pediatr. (2006) 27(2):155–68. doi: 10.1097/00004703-200604000-00014
3. Campos JJ, Frankel CB, Camras L. On the nature of emotion regulation. Child Dev (2004) 75:377–94. doi: 10.1111/j.1467-8624.2004.00681.x
4. Cole PM, Martin SE, Dennis TA. Emotion regulation as a scientific construct: methodological challenges and directions for child development research. Child Dev (2004) 75:317–33. doi: 10.1111/j.1467-8624.2004.00673.x
5. Gross JJ, Munoz RF. Emotion regulation and mental health. Clin Psychol Sci Pract (1995) 2(2):151–64. doi: 10.1111/j.1468-2850.1995.tb00036.x
6. Yap M, Allen N, Sheeber L. Using emotion regulation framework to understand the role of temperament and family process in risk for adolescent depressive disorders. Clin Child Family Psychol (2007) 10(2):180–95. doi: 10.1007/s10567-006-0014-0
7. Joormann J, Siemer M, Gotlib IH. Mood regulation in depression: differential effect of distraction and recall of happy memories on sad mood. J Abnorm Child Physiol (2007) 116(3):484–90. doi: 10.1037/0021-843X.116.3.484
8. Kovacs M, Rottenberg J, George C. Maladaptive mood repair responses distinguish young adults with early-onset depressive disorders and predict future depression outcomes. Psychol Med (2009) 39:1841–54. doi: 10.1017/S0033291709005789
9. Yaroslavsky I, Bylsma LM, Rottemberg J, Kovacs M. Combination of resting RSA and RSA reactivity impact maladaptive mood repair and depression symptoms. Biol Psychol (2013) 94(2):272–81. doi: 10.1016/j.biopsycho.2013.06.008
10. Joormann J, Gotlib IH. Emotion regulation in depression: relation to cognitive inhibition. Cogn Emot (2010) 24(2):281–98. doi: 10.1080/02699930903407948
11. Schafer J, Naumann E, Holmes EA, Tuschen-Caffier B, Samson AC. Emotion regulation strategies in depressive and anxiety symptoms in youth: a meta-analytic review. J Youth Adolesc (2017) 46(2):261–76. doi: 10.1007/s10964-016-0585-0
12. Aldao A, Nolen-Hoexema S, Schweizer S. Emotion-regulation strategies across psychopathology: a meta-analytic review. Clin Psychol Rev (2010) 30:217–36. doi: 10.1016/j.cpr.2009.11.004
13. Bylsma LM, Yaroslavsky I, Kiss E, Kapornai K, Halas K, Dochnal R, et al. Familiality of mood repair responses among children and adolescents with and without histories of depression. Cogn Emot (2015) 10:1–10. doi: 10.1080/02699931.2015.1025707
14. Garber J, Braafland N, Weiss B. Affect regulation in depressed and nondepressed children and young adolescents. Emot Dev Pschopatol (1995) 7:93–115
15. Klemanski DH, Curtis J, McLaughlin KA, Nolen-Hoexema S. Emotion regulation and the transdiagnostic role of repetitive negative thinking in adolescents with social anxiety and depression. Cogn Ther Res (2017) 41(2):206–19. doi: 10.1007/s10608-016-9817-6
16. Carl JR, Soskin DP, Kerns C, Barlow DH. Positive emotion regulation in emotional disorders: a theoretical review. Clin Psychol Rev (2013) 33(3):343–60. doi: 10.1016/j.cpr.2013.01.003
17. Cisler JM, Olatunji BO. Emotion regulation and anxiety disorders. Curr Psychiatry Rep (2012) 14:182–7. doi: 10.1007/s11920-012-0262-2
18. Suveg C, Morelen D, Brewer GA, Thomassin K. The emotion dysregulation model of anxiety: a preliminary examination. J Anxiety Disord. (2010) 24:924–30. doi: 10.1016/j.janxdis.2010.06.018
19. Turk CL, Heimberg RG, Luterek JA, Mennin DS, Fresco DM. Emotion dysregulation in generalized anxiety disorder: a comparison with social anxiety disorder. Cogn Ther Res (2005) 29:89–106. doi: 10.1007/s10608-005-1651-1
20. Suveg C, Zeman J. Emotion regulation in children with anxiety disorders. J Clin Child Adolesc Psychol (2004) 33:750–9. doi: 10.1207/s15374424jccp3304_10
21. Carthy T, Hores N, Apter A. Patterns of emotional reactivity and regulation in children with anxiety disorders. J Psychopathol Behav Assess (2010) 32:23–36. doi: 10.1007/s10862-009-9167-8
22. Mennin DS, Heimberg RG, Turk CL, Fresco DM. Preliminary evidence for an emotion dysregulation model of generalized anxiety disorder. Behav Res Ther (2005) 43:1281–310. doi: 10.1016/j.brat.2004.08.008
23. Angold A, Costello JE. Depressive comorbidity in children and adolescents: empirical, theoretical, and methodological issues. Am J Psychiatry. (1993) 150:1779–91. doi: 10.1176/ajp.150.12.1779
24. Cummings MC, Caporino EN, Kendall CP. Comorbidity of anxiety and depression in children and adolescents: 20 years after. Psychol Bull (2014) 140(3):816–45. doi: 10.1037/a0034733
25. Birmaher B, Ryan DN, Williamson ED, Brent AD, Kaufman J, Dahl ER, et al. Childhood and adolescent depression: a review of the past 10 years. J Am Acad Child Adolesc Psychiatry. (1996) 35(11):1427–39. doi: 10.1097/00004583-199611000-00011
26. Essau AC. Comorbidity of depressive disorders among adolescents in community and clinical settings. Psychiatry Res (2008) 158:35–42. doi: 10.1016/j.psychres.2007.09.007
27. Geller B, Chestnut EC, Miller MD, Price DT, Yates E. Preliminary data on DSM-III associated features of major depressive disorder in children and adolescents. Am J Psychiatry. (1985) 142:643–4. doi: 10.1176/ajp.142.5.643
28. Fichter MM, Quadflieg NN, Fischer UC, Kohlboeck GG. Twenty-five-year course and outcome in anxiety and depression in the Upper Bavarian Longitudinal Community Study. Acta Psychiatr Scand (2010) 122:75–85. doi: 10.1111/j.1600-0447.2009.01512.x
29. Franco X, Saavedra LM, Silverman WK. External validation of comorbid patterns of anxiety disorders in children and adolescents. J Anxiety Disord (2007) 21:717–29. doi: 10.1016/j.janxdis.2006.10.002
30. Masi G, Favilla L, Mucci M, Millepiedi S. Depressive comorbidity in children and adolescents with generalized anxiety disorder. Child Psychiatry Hum Dev (2000) 30:205–15. doi: 10.1023/A:1021351722364
31. Strauss CC, Last CG, Hersen M, Kazdin AE. Association between anxiety and depression in children and adolescents with anxiety disorders. J Abnorm Child Psychol (1988) 16:57–68. doi: 10.1007/BF00910500
32. Pawlak C, Pascual-Sanchez T, Rae¨ P, Fischer W, Ladame F. Anxiety disorders, comorbidity, and suicide attempts in adolescence: a preliminary investigation. Eur Psychiatry (1999) 14:132–6. doi: 10.1016/S0924-9338(99)80730-5
33. Nolen-Hoexema S. Role of rumination in depressive disorders and mixed anxiety/depressive symptoms. J Abnorm Psychol (2000) 109(3):504–5011. doi: 10.1037//0021-843X.109.3.504
34. Starr LR, Davila J. Responding to anxiety with rumination and hopelessness: mechanism of anxiety-depression symptom co-occurrence? Cogn Ther Res (2012) 36(4):321–37. doi: 10.1007/s10608-011-9363-1
35. McEvoy PM, Watson H, Watkins ER, Nathan P. The relationship between worry, rumination, and comorbidity: evidence for repetitive negative thinking as a transdiagnostic construct. J Affect Disord (2013) 151(1):313–20. doi: 10.1016/j.jad.2013.06.014
36. McLaughlin KA, Nolen-Hoeksema S. Rumination as a transdiagnostic factor in depression and anxiety. Behav Res Ther (2011) 49(3):186–93. doi: 10.1016/j.brat.2010.12.006
37. Garnefski N, Kraaij V. Specificity of relations between adolescents’ cognitive emotion regulation strategies and symptoms of depression and anxiety, Cogn Emot (2018) 32(7):1401–08. doi: 10.1080/02699931.2016.1232698
38. Garnefsky N, Legerstee. J, Kraaij V, Kommer T, Teerds J. Cognitive coping strategies and symptoms of depression and anxiety: a comparison between adolescents and adults. J Adolesc (2002) 25:603–11. doi: 10.1006/jado.2002.0507
39. D’Avanzato C, Joormann J. Emotion regulation in depression and anxiety: examining diagnostic specificity and stability of strategy use. Cogn Ther Res (2013) 37:968–80. doi: 10.1007/s10608-013-9537-0
40. Baji I, Lopez-Duran NL, Kovacs M, George CJ, Mayer L, Kapornai K, et al. Age and sex analyses of somatic complaints and symptom presentation of childhood depression in a Hungarian clinical sample. J Clin Psychiatry (2009) 70(10):1467–72. doi: 10.4088/JCP.08m04918
41. Sherrill JT, Kovacs M. Interview schedule for children and adolescents (ISCA). J Am Acad Child Adolesc Psychiatry (2000) 39(1):67–75. doi: 10.1097/00004583-200001000-00018
42. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th-TR ed. Washington, DC: American Psychiatric Association (2000).
43. Kiss E, Gentzler AM, George C, Kapornai K, Tamás Z, Kovacs M, et al. Factors influencing mother–child reports of depressive symptoms and agreement among clinically referred depressed youngsters in Hungary. J Affect Disord (2007) 100(1):143–51. doi: 10.1016/j.jad.2006.10.008
44. Tamás Z, Kovacs M, Gentzler AL, Tepper P, Gádoros J, Kiss E, et al. The relations of temperament and emotion self-regulation with suicidal behaviors in a clinical sample of depressed children in Hungary. Springer US. J Abnorm Child Psychol (2007) 35(4):640–52. doi: 10.1007/s10802-007-9119-2
45. Kovacs M. The Feelings and Me emotion regulatory strategy utilization questionnaires. Unpublished manuscript, University of Pittsburgh School of Medicine (2000)
46. Kovacs M. Children’s depression inventory. Technical manual update. Multi Health System: Toronto (2003).
47. Queen AH, Ehrenreich-May J. Anxiety-disordered adolescents with and without a comorbid depressive disorder: variations in clinical presentation and emotion regulation. J Emot Behav Disord (2014) 22(3):160–70. doi: 10.1177/1063426613478175
48. Burklund LJ, Craske MG, Taylor SE, Lieberman MD. Altered emotion regulation capacity in social phobia as a function of comorbidity. Soc Cogn Affect Neurosci (2015) 10(2):199–208. doi: 10.1093/scan/nsu058
49. Brent DA, Kolko DJ, Birmaher B, Baughróer M, Bridge J, Rith C, et al. Predictors of treatment efficacy in a clinical trial of three psychological treatments for adolescent depression. J Am Acad Child Adolesc Psychiatry. (1998) 37(9):906–14. doi: 10.1097/00004583-199809000-00010
50. Brown C, Schulberg HC, Madonia MJ, Shear MK, Houck PR. Treatment outcomes for primary care patients with major depression and lifetime anxiety disorders. Am J Psychiatry (1996) 153(10):1293–300. doi: 10.1176/ajp.153.10.1293
51. Adrian M, McCauley E, Berk M, Asarnow RJ, Korslund K, Avina C, et al. Predictors and moderators of recurring self-harm in adolescents participating in a comparative treatment trial of psychological interventions. J Child Pyschol Psychiatry (2019). 60(10):1123–32. doi.org/10.1111/jcpp.13099
52. Hawton K, Witt GK, Salisbury TLT, Arensman E, Gunnell D, Townsend E, et al. Interventions for self-harm in children and adolescents. Cochrane Database Syst Rev (2015) 12:1–105. doi.org/10.1002/14651858.CD012013
53. Mehlum L, Ramleth RK, Tormoen JA, Haga E, Diep ML, Stanley HB, et al. Long term effectiveness of dialectical behavior therapy versus enhanced usual care for adolescents with self-harming and suicidal behavior. J Child Pyschol Psychiatry (2019). 60(10):1112–1122. doi: 10.1111/jcpp.13077
54. Linehan M. Cognitive-behavioral treatment of borderline personality disorder. The Guilford Press (1993).
55. Ehrenreich-May J, Chu BC. Transdiagnostic treatments for children and adolescents: principles and practice. New York, NY, US: Guilford Press (2014).
56. Essau C, Olaya B, Sasagawa S, Pithia J, Bray D, Ollendick T. Integrating video-feedback and cognitive preparation, social skills training and behavioural activation in a cognitive behavioural therapy in the treatment of childhood anxiety. J Affect Disord (2014) 167:261–7. doi: 10.1016/j.jad.2014.05.056
57. Norton PJ, Paulus DJ. Toward a unified treatment for emotional disorders: update on the science and practice. Behav Ther (2016) 47(6):854–68. doi: 10.1016/j.beth.2015.07.002
58. García-Escalera J, Chorot P, Valiente RM, Reales JM, Sandín B. Efficacy of transdiagnostic cognitive-behavioral therapy for anxiety and depression in adults, children and adolescents: a meta-analysis. Revista de Psicopatología y Psicología Clínica (2016) 21:147–75. doi: 10.5944/rppc.vol.21.num.3.2016.17811
Keywords: pediatric depression, anxiety depression comorbidity, emotion regulation, internalizing psychopathology, adolescent
Citation: Dochnal R, Vetró Á, Kiss E, Baji I, Lefkovics E, Bylsma LM, Yaroslavsky I, Rottenberg J, Kovacs M and Kapornai K (2019) Emotion Regulation Among Adolescents With Pediatric Depression As a Function of Anxiety Comorbidity. Front. Psychiatry 10:722. doi: 10.3389/fpsyt.2019.00722
Received: 21 February 2019; Accepted: 09 September 2019;
Published: 07 October 2019.
Edited by:
Roberto Canitano, Siena University Hospital, ItalyReviewed by:
Prabha Siddarth, UCLA David Geffen School of Medicine, United StatesAnn Vander Stoep, University of Washington, United States
Copyright © 2019 Dochnal, Vetró, Kiss, Baji, Lefkovics, Bylsma, Yaroslavsky, Rottenberg, Kovacs and Kapornai. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roberta Dochnal, cmRvY2huYWxAZ21haWwuY29t