 Di Fu1,2†‡
Di Fu1,2†‡ Dan-Dan Wu3‡
Dan-Dan Wu3‡ Hong-Li Guo1
Hong-Li Guo1 Ya-Hui Hu1
Ya-Hui Hu1 Ying Xia1Xing Ji1Wei-Rong Fang2Yun-Man Li2Jing Xu1
Ying Xia1Xing Ji1Wei-Rong Fang2Yun-Man Li2Jing Xu1 Feng Chen1*
Feng Chen1* Qian-Qi Liu3*
Qian-Qi Liu3*- 1Department of Pharmacy, Pharmaceutical Sciences Research Center, Children's Hospital of Nanjing Medical University, Nanjing, China
- 2School of Basic Medical Sciences and Clinical Pharmacy, China Pharmaceutical University, Nanjing, China
- 3Department of Children Health Care, Children's Hospital of Nanjing Medical University, Nanjing, China
Atomoxetine, a selective norepinephrine (NE) reuptake inhibitor, was approved for attention deficit/hyperactivity disorder (ADHD) treatment in children, adolescents and adults. We searched the database PubMed/MEDLINE (2000 to October 1, 2021). Only publications in English were considered. Atomoxetine inhibits the presynaptic norepinephrine transporter (NET), preventing the reuptake of NE throughout the brain along with inhibiting the reuptake of dopamine in specific brain regions such as the prefrontal cortex (PFC). The novel mechanism of atomoxetine also includes several new brain imaging studies and animal model studies. It is mainly metabolized by the highly polymorphic drug metabolizing enzyme cytochrome P450 2D6 (CYP2D6). Atomoxetine is effective and generally well tolerated. ADHD is often accompanied by multiple comorbidities. A series of studies have been published suggesting that atomoxetine is effective in the treatment of ADHD symptoms for children with various types of comorbidity. In some cases, it is possible that atomoxetine may have a positive influence on the symptoms of comorbidities. Atomoxetine can be administered either as a single daily dose or split into two evenly divided doses, and has a negligible risk of abuse or misuse. The latest guideline updated that clinical dose selection of atomoxetine was recommended based on both CYP2D6 genotype and the peak concentration. To have a more comprehensive understanding of atomoxetine, this review sets the focus on the mechanism, clinical efficacy and dosage regimen in detail, and also touches on those studies regarding adverse reactions of atomoxetine.
Introduction
ADHD is a neuropsychiatric disorder commonly diagnosed in children and adolescents. It affects their learning, emotion, cognition, and social behavior to varying degrees (1, 2). The pooled worldwide ADHD prevalence among children varies from 2 to 18% (3). The prevalence in Chinese children and adolescents can reach 5.6–8.4% (4), and there is a significant sex disparity in the prevalence (14% in boys and 6.3% in girls) (5). The core symptoms of ADHD include impaired levels of inattention, hyperactivity, or impulsivity, or a combination (6). ADHD is associated with neurochemical signaling dysregulations in several brain regions, particularly in the PFC, involving attention and executive functions (7, 8). Through dopamine and NE signaling mechanisms, brainstem neuronal projections connect to the PFC to regulate behavior (7, 9). There is growing evidence that the input of catecholamine in the PFC of patients with ADHD is reduced (8). Magnetic resonance imaging (MRI) studies have demonstrated that children with ADHD have slightly smaller, on average, entire brain and decreases in certain cortical and subcortical regions (10). Functional MRI (fMRI) is an emerging neuroimaging technique widely used to measure brain activity in vivo (11, 12). Compared with the control group, children with ADHD have decreased activation in the inferior frontal cortex (IFC), dorsolateral prefrontal cortex (DLPFC), insula, striatum, thalamic and parietal regions, as well as cerebellum, and increased activation in regions of the default mode network (DMN) in fMRI studies of attention functions (13–15). Additionally, comorbid psychiatric disorders are common among child patients with ADHD (16).
The commonly used treatment methods for ADHD include pharmacological treatment (17, 18), behavioral therapy (19, 20), combined medication and behavior therapy (21, 22). Pharmacological treatments for ADHD include stimulants (e.g., methylphenidate and amphetamines) generally recommended as the first-line treatment (23) and non-stimulants (e.g., alpha 2 agonists and atomoxetine) (24) considered to be the second-line treatment (3, 18). In contrast to European and North American guidelines, the 2014 Japanese clinical guidelines and the 2015 Chinese guideline recommend both non-stimulants and stimulants as the first-line pharmacological treatment for children and adolescents with ADHD. Atomoxetine is the first non-stimulant medication which was approved by the US Food and Drug Administration (FDA) to treat ADHD in late 2002 (25), and typically is prescribed to children who cannot tolerate or do not respond to stimulants (26). It generally takes 2–4 weeks for full impact on symptoms to be observed (27). Atomoxetine is generally considered to be safe and effective, and its use is associated with relatively few adverse reactions (1, 28). It is mainly metabolized by the highly polymorphic drug metabolizing enzyme CYP2D6, which has significant genetic polymorphism (29). The metabolic ability of CYP2D6 enzymes to atomoxetine is significantly different among different individuals, affecting the therapeutic efficacy and dosage regimen of clinical treatment of ADHD (29, 30).
This review focuses on the mechanism, clinical efficacy, dosage regimen, and adverse reactions of atomoxetine. Regarding the mechanism of atomoxetine, the known studies about norepinephrine reuptake inhibitor (NRI) and several new brain imaging studies were reported. The clinical efficacy was described through three aspects: short-term efficacy, long-term efficacy, and comorbidities. The reasons for the better efficacy in older children than in younger children were also discussed. In the description of dosage, not only the standard dosing regimen, but also CYP2D6 genotype and the peak concentration recommended in the latest guideline are included to guide the clinical atomoxetine dosage selection. In addition, the influence of administration time (in the morning or at night), administration frequency and administration rate on clinical efficacy was also discussed. Common adverse reactions include the latest research findings on somnolence and nighttime awakening.
Methods
We searched the database PubMed/MEDLINE (January 1, 2000 to October 1, 2021). Searches included keywords (Medical Subject Heading) and free-text terms for ADHD, atomoxetine, children, mechanism, brain, clinical efficacy, short-term efficacy, long-term efficacy, dosage, comorbidities, oppositional defiant disorder (ODD), anxiety, autism spectrum disorder (ASD), tics disorders (TD), Tourette's Syndrome (TS), learning disorders, adverse reactions, sleep, older, and safety. Only articles in English were reviewed to determine suitability for inclusion.
Mechanism of Action
While the precise mechanism of action (MOA) through which atomoxetine produces its therapeutic effects is unclear, the putative hypotheses have been elucidated (28, 31). Atomoxetine is thought to be related to its selective inhibition of presynaptic NE reuptake in the PFC (32). As a highly selective norepinephrine reuptake inhibitor (SNRI), atomoxetine highly binds to NE reuptake transporter on the presynaptic membrane of the nerve and inhibits NE reuptake (32). Its role is to increase the NE concentration in the synaptic cleft, which results in elevations of synaptic levels of noradrenaline in the central nervous system (1, 33, 34). However, it has little or no affinity for either the serotonin or dopamine transporters or other neurotransmitter receptors (35). Additionally, atomoxetine is also known to modulate cortical synaptic dopamine uptake via the nonspecific action of the abundant NET in the PFC, selectively increasing dopamine levels in the PFC in a regionally specific manner (27, 36), but not in motor or reward-related areas of the striatum (34), thereby improving the symptoms of ADHD and concentration of attention (Figure 1).
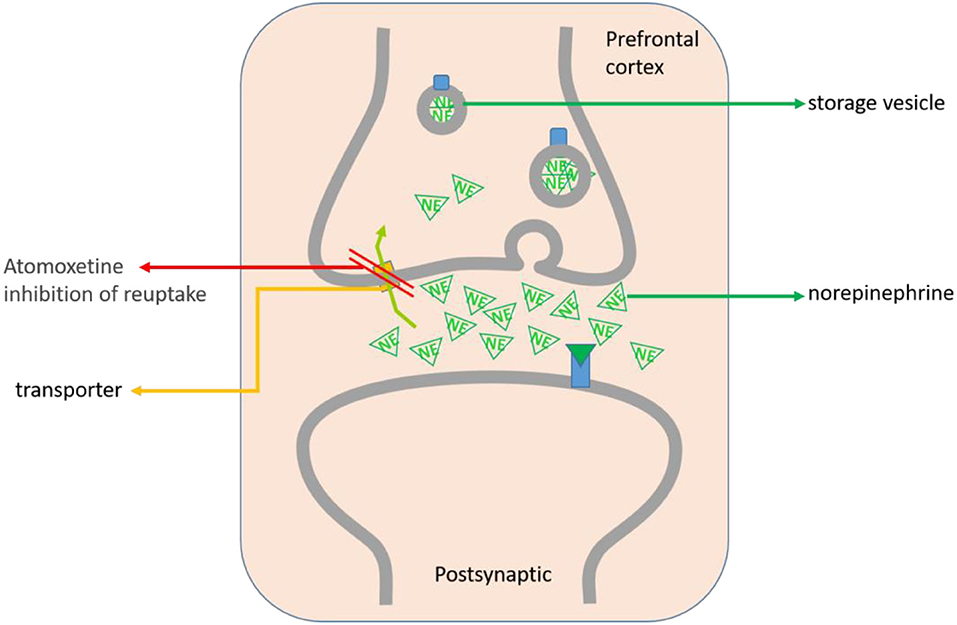
Figure 1. The MOA of atomoxetine on ADHD treatment is mainly located in the PFC. Atomoxetine can highly bind to the NE reuptake transporter on the presynaptic membrane of the PFC, selectively inhibit NE reuptake and increase the NE in the synaptic cleft of neurons. Atomoxetine can also modulatethe dopamine uptake in the synaptic cortex through NET, and increase the dopamine level in the PFC, but not in the nucleus accumbens and striatum.
As suggested by Barr et al. (37), the pathogenesis of ADHD is related to the dopamine decrease and the NE reversal effect. This finding is consistent with the pharmacological effects, which theoretically explains the effectiveness in the treatment of ADHD. Atomoxetine exerts a reversal effect by gradually increasing extracellular levels of NE. One rat study (32) found that atomoxetine showed a high affinity for the NET, a low affinity for the serotonin transporter, and a relatively low affinity for dopamine transporter. The high affinity for the NET prevented the reuptake of norepinephrine, leading to an increase in neurotransmitters at the neuronal synapses in the PFC of the rat brain.
Fortunately the progress of human brain imaging studies in recent years has provided us with new insights into the ADHD management with atomoxetine (10, 13, 38–40). The right inferior PFC is a key area of dysfunction in ADHD during inhibitory performance (41). Atomoxetine has beneficial effects on inhibitory control by regulating right inferior frontal function (38). These findings of the study provided important neurofunctional evidence for the MOAs (38). Moreover, a study provided the first fractional amplitude of low-frequency fluctuations (fALFF) evidence of distinct therapeutic mechanisms of atomoxetine and methylphenidate in the treatment of children with ADHD (39). Increased fALFF in the left lingual gyrus and inferior occipital gyrus was correlated with inattention improvement with the treatment of atomoxetine. In contrast, improvement in hyperactivity/impulsivity was associated with decreased fALFF in bilateral precentral and postcentral gyri in bilateral precentral and postcentral gyri (39). The fALFF effect of atomoxetine treatment associated with clinical improvement emphasized the importance of using resting-state functional MRI (RS-fMRI) techniques to exploring the medication effects on intrinsic brain activity in children with ADHD. Children ages 7–12 years with ADHD who respond clinically to atomoxetine had improvements of clinical symptoms, correlated with a decrease in motor cortex short interval cortical inhibition (40). A randomized, double-blind, placebo-controlled, crossover study (13) shows that atomoxetine upregulates inferior frontal activation and improves DMN deactivation during cognitive functions, improves attention functions and upregulates abnormal fronto-cortical activation during executive function tasks in ADHD patients, and appears to have drug-specific effects of up-regulating DLPFC. Most importantly, this study shows for the first time that during the period of sustained attention, a single dose of atomoxetine has a comparable effect to methylphenidate in normalizing fronto-striato-thalamo-parietal brain abnormalities in ADHD (10, 13). Actually, the first study that incorporated RS-fMRI into the randomized controlled trial (RCT) of atomoxetine in medication-naive adults with ADHD suggested an important mechanism of atomoxetine therapy (42). The results showed that atomoxetine treatment caused a strengthened anti-correlated relationship between DMN and the task-positive networks (cognitive control and dorsal attention networks) (42). Also, this study for the first time found that the strengthened anti-correlations were linked to the improved ADHD symptoms after the atomoxetine therapy (42). Although this clinical trial was conducted in adults, in this way, a new possibility opens up in this area of research. So it will be very intriguing to perform a similar study in children.
A 2014 study using positron emission tomography (PET) imaging to assess clinically relevant doses of atomoxetine in rhesus monkeys found that atomoxetine occupied not only NET, but also the serotonin transporters (43). A murine prenatal nicotine exposure model of ADHD was made to investigate the effects of atomoxetine on behavior and synaptic plasticity in the hippocampus and long-term potentiation (LTP) in hippocampal slices at the CA3–CA1 synapses (44). The results indicated that atomoxetine in this model reconstructed LTP in CA3–CA1 synapses. Postsynaptic changes in synaptic plasticity may be part of the mechanisms of atomoxetine-induced improvement in ADHD symptoms (44). These findings suggest that there may be one or more unknown pathways through which atomoxetine works. The neuropharmacology of these aspects awaits further study.
Clinical Efficacy
Clinically meaningful improvements in the core symptoms of ADHD (inattention, impulsivity, and hyperactivity) as well as quality of life and emotional lability (34) are often observed after atomoxetine therapy. The focus of this section is on data from fully published, randomized, controlled trials investigating the therapeutic effectiveness of atomoxetine in children with ADHD (Table 1). Clinical efficacy data for ADHD pediatric patients were pooled from short-term (6–16 weeks) studies (45–48, 52, 53) and long-term (>6 months) studies (49–51).
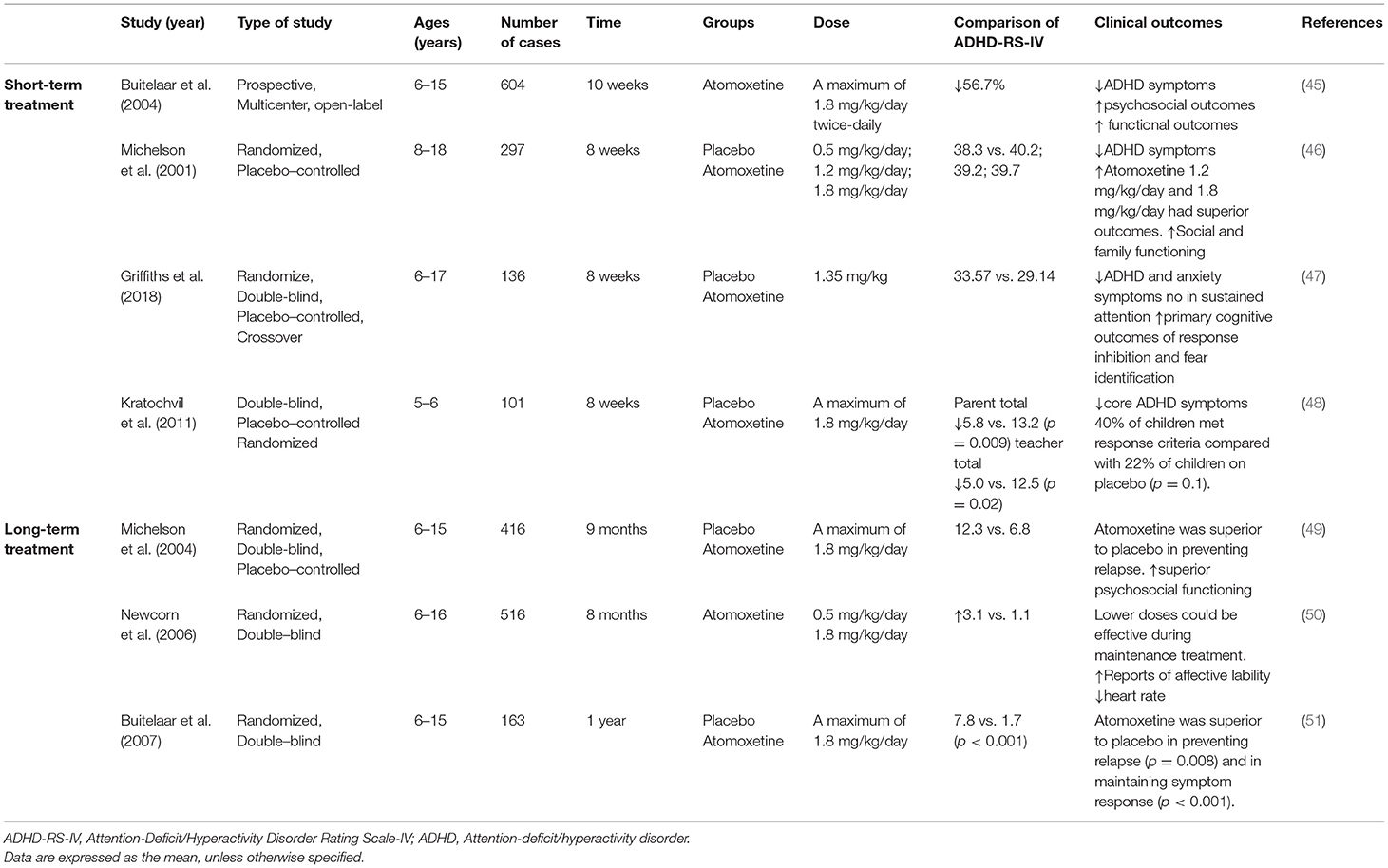
Table 1. Summary of efficacy trials in atomoxetine treatment studies.
Short-Term Treatment
Clinically meaningful improvements in ADHD symptoms are often observed after a few weeks of atomoxetine treatment (27, 45–47, 54). For instance, in a 10-week open-label study of 604 pediatric patients with ADHD (45), ADHD-Rating Scale (ADHD-RS) total scores decreased by 56.7%, such that 69% of patients were rated as having no or minimal symptoms. Significant improvement was also observed in psychosocial and functional outcomes. A randomized, placebo-controlled, dose-response trial of 8-week duration investigated the efficacy of 3 doses of atomoxetine compared with placebo in children and adolescents with ADHD (46). Of the 381 patients screened, 297 children and adolescents were randomized to placebo or atomoxetine. The atomoxetine groups had superior outcomes in ADHD symptoms compared with placebo group. Social and family functions were also significantly improved in the atomoxetine groups. Schwartz and colleagues (54) comprehensively evaluated the efficacy and safety of atomoxetine in pediatric ADHD patients. This largest and most comprehensive meta-analysis including 3,928 pediatric patients found atomoxetine to be superior to placebo for ADHD on a number of relevant outcomes. The results showed that the short-term atomoxetine treatment can significantly improve the core symptoms. As objectively measured by performance-based tests, response inhibition and sustained attention deficit are among the most common cognitive deficits associated with ADHD (55, 56). In a double-blind, randomized, placebo-controlled crossover trial (47), atomoxetine treatment resulted in moderate improvement in response inhibition but no significant improvement in sustained attention. It improved identification of fearful faces, particularly in younger children. The effect size of improvement in ADHD symptoms was lower than that found in a meta-analysis of previous studies (−0.35 relative to −0.64) (54). The growing studies confirm that short-term atomoxetine treatment significantly reduces core symptoms of ADHD.
Between children and adolescents, there seems to be no difference in the efficacy of atomoxetine, but it is indeed more effective among older children than younger children (57, 58). An earlier meta-analysis of six clinical trials of 6–9 weeks duration compared atomoxetine efficacy vs. placebo among young children [(6–7 years; n = 184 atomoxetine, and n = 96 placebo) vs. older children (8–12 years; n = 544 atomoxetine, and n = 316 placebo)] (52). It found that, while atomoxetine was superior to placebo for mean (SD) change in both age categories in ADHD-RS scores and response rates (p < 0.05), older children had significantly (p < 0.05) greater improvements in ADHD-RS scores than younger children, regardless of whether they were receiving atomoxetine or placebo (52). Moreover, atomoxetine was also evaluated in young children (5–7 years old) (26). A total of 93 subjects were dosed in an 8-week, double-blind, placebo-controlled randomized clinical trial (48). Subjects who received atomoxetine had significantly greater improvement in ADHD-RS-IV scores than patients who received placebo. This is the first RCT of atomoxetine in children as young as 5 years (48). Common medications used for ADHD also include stimulants, such as methylphenidate and osmotic release oral system methylphenidate (OROS MPH). Methylphenidate is traditionally recognized as the first-line treatment for ADHD (59). Efficacy of both methylphenidate and atomoxetine has been established in placebo-controlled trials (60). While atomoxetine has been shown to be superior to placebo, definitive evidence suggesting comparable efficacy to psychostimulants does not exist at this time (61). Several comparative efficacy studies conducted in American and European populations suggested that, compared with atomoxetine, OROS MPH resulted in greater reduction in ADHD symptoms (53, 62, 63). Kemner et al. found that methylphenidate (n = 378) and atomoxetine (n = 139) produced similar symptom rating scale score reductions at weeks 1 and 2 in the treatment-naive subgroup (n = 517) in a multicenter, randomized, prospective, open-label study in 1323 American children 6 to 12 years of age with ADHD (62). Subsequently, Newcorn et al. also conducted a large placebo-controlled, double-blind, randomized study for 6 weeks in America. It also found that the response rates for OROS MPH and atomoxetine were not significantly different, but that they were markedly superior to the rate for placebo in the treatment-naive subgroup at the end-point (53). In a 24-week, open-label, head-to-head clinical trial, children and adolescents randomly assigned to OROS MPH (n = 80) and atomoxetine (n = 80). Although as early as 2 weeks after randomization, primary efficacy measure improved in both treatment groups, the ADHD-RS-IV Inattention score of the OROS MPH group was significantly lower than that of the atomoxetine group (Cohen's d, 0.46; p = 0.004) at week 2. However, from week 4 through week 24, there was no significant difference in response to these two medications (64). Consequently, long-term studies are needed to evaluate changes in the relative efficacy of OROS MPH and atomoxetine (64). Additionally, a study suggested that the short-term efficacy of OROS MPH and atomoxetine was similar in China (65). Both of them were effective in reducing ADHD symptoms of Chinese children and adolescents. The results showed that percentages achieving remission, robust improvement, and improvement were comparable for OROS MPH and atomoxetine treatment (35.3 vs. 37.1%, 45.4 vs. 44.8%, 65.5 vs. 66.4%).
There appears to be some heterogeneity in response rates in geographic regions (27), although atomoxetine is an effective treatment in all locations (Asia, Europe, North America, and Russia) (66), and responses of ethnic groups (i.e., Caucasians, African Americans, and Latinos) in the America seem to be similar (67, 68).
Long-Term Treatment
Similar to the findings in short-term studies, atomoxetine remained efficacious in the long-term treatment of ADHD in children (35). Atomoxetine has been demonstrated to be effective through to the end of 8- to 24-month treatment periods (69). Thereafter, response to treatment was maintained over the ensuing period, out to 24 months after the initiation of treatment (70). However, few placebo-controlled, long-term studies of efficacy have been reported.
With respect to long-term treatment, two meta-analytic reviews of 13 trials each, one in 219 adolescents (aged 12–18 years) (70) and one in 97 young children (aged 6–7 years) (71) with ADHD who were treated with atomoxetine for at least 2 years, showed that atomoxetine retained significant (p < 0.001) improvement at endpoint vs. baseline in ADHD-RS scores with continuous drug intake. Data from 6- and 7-year-old children (n = 192) suggest that the effectiveness of atomoxetine treatment is maintained over 12–24 months (71). In this 13-study meta-analysis, the corresponding decrease in ADHD Rating Scale-IV Parent Version, Investigator Administered (ADHD – RS – IV Parent: Inv) total scores showed that there was a marked improvement in ADHD symptoms after 3 months of atomoxetine treatment, which was maintained for a minimum of 24 months in the 97 pediatric subjects who continued the atomoxetine treatment for at least 2 years (71).
In addition, atomoxetine was superior to placebo in maintaining response in a 9-month relapse prevention study (49). The results supported the value of maintenance treatment with atomoxetine in pediatric patients with ADHD who responded to initial treatment (49). Newcorn et al. (50) demonstrated that low-dose atomoxetine was an effective choice for retaining the treatment response during maintenance treatment in an 8-month, randomized, double-blind trial.
In two clinical studies with initial treatment periods of 10–52 weeks, atomoxetine has also been proved to be effective at preventing relapse of ADHD symptoms (49, 51). Buitelaar et al. (51) reported that atomoxetine was superior to placebo at preventing relapse and maintaining efficacy in children and adolescents (n = 163) treated with atomoxetine for 1 year, who were then randomized either to atomoxetine or placebo for a further 6 months. Many patients might stay in good condition for several months without atomoxetine therapy, after 1 year of atomoxetine therapy. As a matter of fact, in the 1 - year study, for the patients who were assigned to discontinue atomoxetine therapy, they were generally less severe than at study entry when symptoms returned (51).
In Patients With Comorbid Conditions
Comorbid psychiatric disorders are common among patients with ADHD, including ODD, anxiety and depression disorders, ASD, TD, learning disorders (LD), disruptive behavior disorders (DBDs), and TS (16, 35, 72, 73). More than half of children and adolescents with ADHD have a comorbid condition, and more than a quarter had two or more comorbidities (16, 35). In particular, ODD/conduct disorder (CD) is among the most common comorbidities with ADHD, affected approximately 50 % of children with ADHD (46, 74–76). Up to now, a series of published studies suggested that atomoxetine is effective in the treatment of ADHD symptoms for children with various types of comorbidity (27, 74, 77–83). In some cases, it is possible that atomoxetine may have a positive influence on the symptoms of comorbidities (27, 73, 82). Detailed information about these studies is summarized in Table 2.
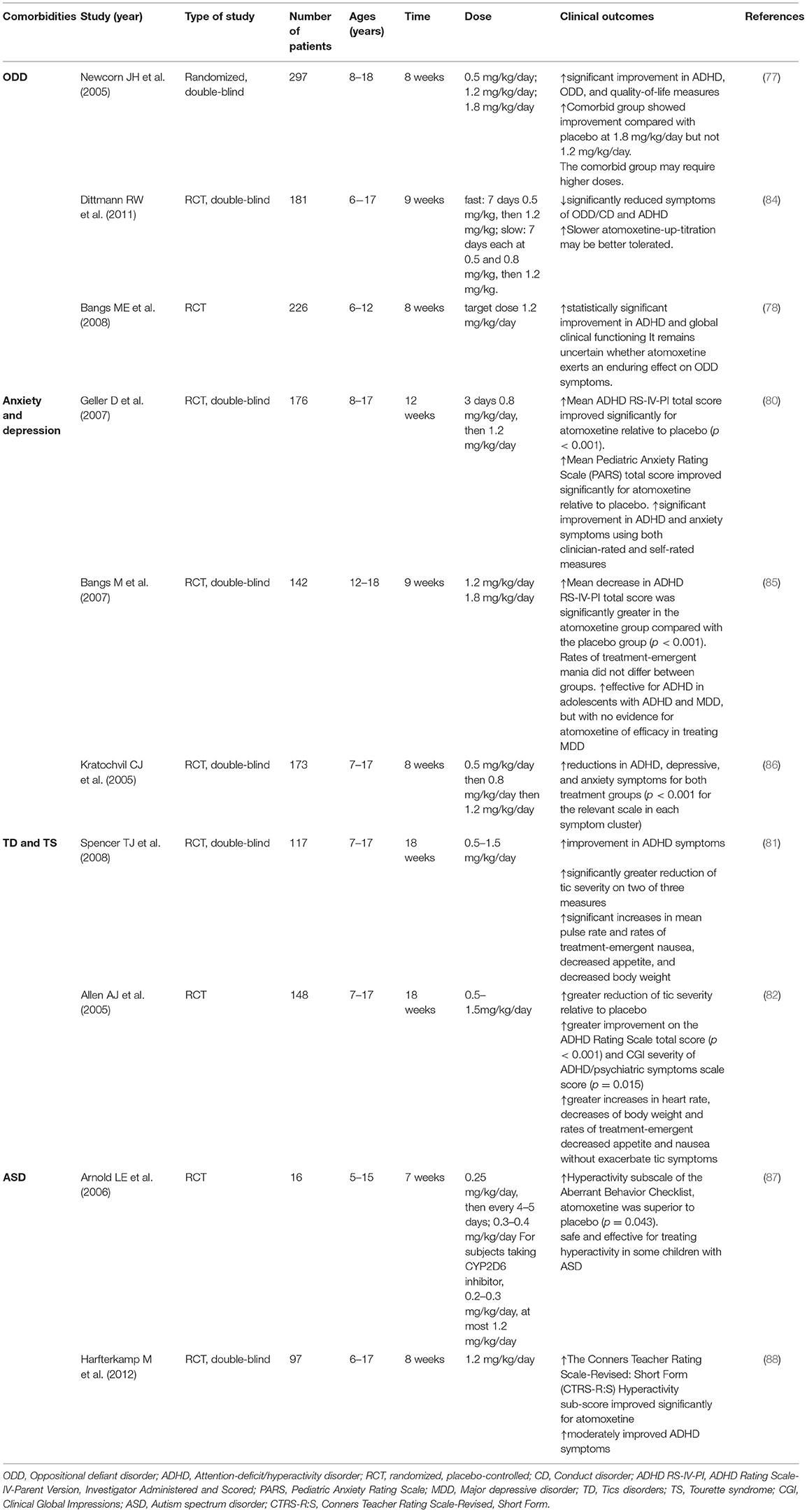
Table 2. Efficacy of atomoxetine treatment in comorbidities of ADHD.
Oppositional Defiant Disorder (ODD)
ODD is the most common and the most noticeable psychiatric disorder that co-exists with ADHD (73, 89, 90). Many well-designed studies indicated that ADHD symptoms were improved with atomoxetine treatment in ADHD patients with comorbid ODD (74, 77–79), several of which have also shown atomoxetine to be effective in improving ODD symptoms (73). However, it is currently uncertain whether or not the efficacy of atomoxetine as a treatment for ADHD is affected by comorbid ODD (27).
In a 9-week, randomized, placebo-controlled study in ADHD patients with comorbid ODD or CD, atomoxetine was significantly superior to placebo in reducing symptoms of ODD/CD and ADHD (p < 0.001) (84). Moreover, in a meta-analysis of 25 double-blind randomized controlled trials, atomoxetine was associated with somewhat less improvements in ODD symptoms (54). Newcorn et al. (77) reported on atomoxetine therapy in children and adolescents with ADHD and comorbid ODD. The results showed that atomoxetine treatment improved ADHD and ODD symptoms in youths, although the comorbid group may require higher doses (77). Currently, when ODD comorbidity is present, additional research may be warranted to evaluate whether higher doses are required. However, other studies indicate that although ADHD symptoms improved, there are no statistically significant improvements after atomoxetine therapy (78, 91).
Anxiety and Depression
Studies have reported that the prevalence of ADHD comorbid anxiety disorder is 5.6–37.9% (92, 93). Atomoxetine appears to be an effective treatment for ADHD in children with comorbid anxiety or depression (27, 80).
In 176 pediatric patients with ADHD and comorbid anxiety disorders, 12 weeks of atomoxetine appeared to be more efficacious as a treatment for ADHD symptoms vs. placebo (mean change from baseline −10.5 vs. −1.4; p < 0.001), and was accompanied by improvements in anxiety (80). Results supported consideration of atomoxetine for the treatment of ADHD in patients who have ADHD with comorbid anxiety disorder. In 142 adolescents with ADHD and comorbid major depressive disorder (MDD), improvements in ADHD symptoms were greater after 9 weeks of atomoxetine treatment vs. placebo, without improvement in MDD (85). The trial did not show any difference in improving depressive symptoms (Children's Depression Rating Scale-Revised [CDRS-R] scores −14.8 vs. −12.8 for atomoxetine vs. placebo; p = 0.34) (85). In some ways, atomoxetine has demonstrated a positive effect on anxiety symptoms (73). In a randomized, double-blind, placebo-controlled study (80), its efficacy was perceived by both the physicians and the pediatric patients with ADHD and anxiety disorders, and in a double-blind study comparing atomoxetine alone with atomoxetine in combination with fluoxetine, reductions in ADHD, depressive, and anxiety symptoms were marked for both treatment groups (p < 0.001 for the relevant scale in each symptom cluster) (86).
Tics Disorders (TD) and Tourette's Syndrome (TS)
Comorbidity of ADHD and TD or TS is common, with ADHD occurring in as many as 50% of all cases of TS in children (82). Atomoxetine appears to be effective in treating ADHD without aggravating in patients with both conditions (73).
Allen et al. (82) designed a clinical trial to determine whether atomoxetine was effective for ADHD symptoms in children with tics and ADHD. Patients were randomly assigned to double-blind treatment with placebo (n = 72) or atomoxetine (n = 76) for up to 18 weeks. The results indicated that atomoxetine was associated with a beneficial effect on tic severity, as atomoxetine treatment resulted in a significantly greater improvement than placebo (−0.7 vs. −0.1; p = 0.002) in the Clinical Global Impressions Tic/Neurologic Severity (CGI-Tic/Neuro-S) Scale scores, and both atomoxetine and placebo groups achieved significant improvements from baseline in tic severity assessed by the Yale Global Tic Severity Scale total score (YGTSS, primary measure of tic severity; −5.5 vs. −3.0) and the Tic Symptom Self-Report total score (TSSR; −4.7 vs. −2.9). Another study also has shown atomoxetine is efficacious for treatment of ADHD and well tolerated in ADHD children with comorbid TS (81).
Learning Disorders (LD)
The most common LD is reading disorder (RD), or dyslexia (94). Estimates of rates in those with ADHD and comorbid dyslexia range from 15 to 45%, much greater than by chance (95). A randomized, placebo-controlled trial evaluated the efficacy of atomoxetine in children with dyslexia only or ADHD and comorbid dyslexia (95).
The results showed reading scores were improved with atomoxetine therapy in children with ADHD and comorbid dyslexia. But in general, the improvements of ADHD symptoms in children with ADHD and comorbid dyslexia were not associated with improvement of reading scores (95–97). As a result, it is vital to treat ADHD and learning disorders together rather than in isolation (94). The association between atomoxetine and dyslexia-related improvements (including word recognition, comprehension, and reading ability) deserves more attention and research (72).
Autism Spectrum Disorder (ASD)
About 20–60% of children with ADHD have autism-like social difficulties higher than typically developing children (98). Initiation of medication in ADHD with ASD is much earlier than in ADHD children (83).
In some of studies to date, atomoxetine has been shown to be safe and effective for treating ADHD symptoms in some children with ASD (88, 99), but the response rate has been nominally less than that reported for developing children with ADHD alone (87). A small (n = 16), double-blind study in children with ASD and ADHD randomly assigned to order in a crossover of clinically titrated atomoxetine and placebo revealed that, compared with placebo, atomoxetine was associated with significant improvement in Aberrant Behavior Checklist—Hyperactivity (ABC-H) scores (primary endpoint) and ABC—Lethargy/Social Withdrawal scores (the ABC is a widely used rating scale for evaluating patients with developmental disabilities). On the primary outcomes, atomoxetine was superior to placebo on the hyperactivity subscale of the ABC (p = 0.043). ABC-H scores of the atomoxetine group decreased from 24.69 at baseline to 19.31 at week 6, and these of placebo group dropped from 22.50 at baseline to 22.37 at week 6 (p = 0.04), while ABC-Lethargy/Social Withdrawal scores were reduced from 8.69 to 6.50 in the atomoxetine group, but increased from 6.62 to 7.43 in the placebo group (p = 0.01) (87). Additionally, results of a systematic review and meta-analysis demonstrate the beneficial effect of atomoxetine therapy on ADHD symptoms in children with comorbid ASD (83). Although evidence suggests potential efficacy of atomoxetine, the existing evidences are not conclusive and more trials are needed (99, 100).
Dosage
Standard Dosage of Atomoxetine
Currently, atomoxetine is only used in pediatric patients over 6 years old with ADHD (101). The efficacy and safety of atomoxetine in ADHD patients ≤ 6 years old have not been established, and its application in preschool children with ADHD is still limited. Dosage of atomoxetine in children was initially studied in an open-label and prospective trial of 30 subjects with ADHD aged 7–14 years (102). Mean final total daily dose was 1.9 mg/kg/day (range: 0.4–3.2 mg/kg/day). Atomoxetine significantly decreased core ADHD symptoms as measured by the investigator-scored ADHD Rating Scale-IV (38.6% decrease vs. baseline, p < 0.001) (102).
In the European Summary of Product Characteristics (SPC) and US Full Prescribing Information for atomoxetine, body weight-based dosing is recommended for children and adolescents up to 70 kg. The starting dose recommended in the published prescribing information is approximately 0.5 mg/kg/day which can then be increased to a target maintenance dose of approximately 1.2 mg/kg/day (for a minimum of 7 days in Europe, and a minimum of 3 days in the America). The maximum total daily dose approved by the FDA for children and adolescents who weigh ≤ 70 kg is 1.4 mg/kg/day; for children and adolescents who weigh > 70 kg, it is 100 mg/day (according to the product labeling). However, the European SPC states that the safety of atomoxetine dose > 1.8 mg/kg/day “have not been systematically evaluated”. For children and adolescents over 70 kg, the recommended dose is to increase from a daily initiation dose of 40–80 mg, and the maximum total daily dose should not exceed 100 mg in the USA and Europe. It is manufactured in capsules containing 10, 18, 25, 40, 60, 80, or 100 mg of atomoxetine hydrochloride as well as in an oral solution (4 mg/ml) (103).
To date, only one study assessed the utility and tolerability of higher than standard dosage to treat ADHD (104). Two randomized, double-blind trials were conducted in patients ages 6–16 years who did not respond to atomoxetine comparing continued treatment with same-dose atomoxetine treatment using greater than standard dosage (study 1: up to 3.0 mg/kg/day; study 2: up to 2.4 mg/kg/day). The results showed no improved overall response in children or adolescents who did not respond to lower doses of atomoxetine (1.2 to 1.8 mg/kg/day) (104). Higher doses do not seem to achieve better efficacy outcomes. Currently, there is no data to support increased effectiveness at higher doses.
In addition, the initial and target doses of atomoxetine should be reduced to 50% of the normal dose in patients with moderate hepatic impairment and to 25% of the normal dose in those with severe hepatic impairment (105).
The Clinical Pharmacogenetic Implementation Consortium (CPIC) updated the guidelines in February 2019 for clinical dose selection of atomoxetine based on CYP2D6 genotype and the peak concentration (30). According to the individual's ability to metabolize drugs, individuals with different CYP2D6 phenotypes can be divided into four categories: extensive metabolizer (EM), poor metabolizer (PM), intermediate metabolizer (IM) and ultrarapid metabolizer (UM) (106). UMs rapidly metabolize atomoxetine, so that the plasma concentration of drugs decreases too fast to achieve the ideal clinical efficacy, while PMs may lead to the accumulation in the body because of slow metabolism, increasing the risk of adverse reactions (30, 107). The recommendation is to initiate dosing at 0.5 mg/kg/ day and increase to 1.2 mg/kg/ day after 3 days in EMs and UMs, while also utilizing plasma concentrations to reach peak concentrations approaching 400 ng/mL after 2 weeks if there is no clinical response or adverse reactions. In PMs and IMs, an initial dose of 0.5 mg/kg/ day is recommended, followed by a 2-week wait, with peak plasma concentrations guiding dose adjustments in the absence of clinical response and adverse reactions (30).
Administration Time and Titration Rate
With regard to once- or twice-daily dosing, and morning vs. afternoon/evening dosing, similar advice is issued in the European SPC and US Full Prescribing Information document for atomoxetine. Atomoxetine should be administered as a single dose in the morning, or twice daily as evenly divided doses in the morning and late afternoon/early evening (according to the product labeling). In this section, we reviewed findings from trials comparing once- or twice-daily dosing and the effect of titration rate on therapeutic efficacy of atomoxetine therapy and provided a summary of the dosing studies.
Atomoxetine appeared to be as effective when the daily dose was administered once in the morning as when the dose was divided and administered in the morning and evening in a double-blind study (79). Both once-daily morning and evening dosage regimens have been evaluated (74, 79, 108). A 3-arm and randomized trial of morning and evening atomoxetine dosing compared to placebo in 288 children aged 6–12 years showed that ADHD-RS-IV total scores improved significantly during the 6-week trial (p < 0.001) for morning dosing while ADHD-RS-IV total scores with evening dosing was not significantly different from placebo. Morning- and evening-dosed atomoxetine were significantly better than placebo in the mean changes for evening behavior using the Conners' Global Index-Parent Version (CGI-P) ratings (p < 0.001 and p < 0.05, respectively). Evening dosing showed greater tolerability than morning dosing (79).
In a post hoc analysis of 22 pediatric and 3 adult atomoxetine trials in subjects with ADHD, the effects of a daily dosage regimen and titration rate were evaluated (109). Pediatric patients who received once-a-daily dosing had a significantly earlier onset of all treatment-emergent adverse events (TEAEs), and the fast titration method has a shorter time to onset for common TEAEs than the slow titration method (109). Slower up-titration (0.5 mg/kg/day for 7 days, followed by 0.8 mg/kg/day for 7 days, and then 1.2 mg/kg/day) may be more beneficial than faster up-titration (0.5 mg/kg/day for 7 days, then 1.2 mg/kg/day) (26, 109). For children with ADHD who have seriously decreased appetite after atomoxetine treatment, the initial dose can be changed from once daily to twice daily, fast to slow. Additionally, Dittmann et al. (84) demonstrated that slower atomoxetine-up-titration may be better tolerated than faster up-titration, although improvements did not differ significantly between both titration groups in this 9-week study of 181 children or adolescents with ADHD and comorbid ODD.
Moreover, a non-randomized, open-labeled, prospective interventional study was conducted to clarify the relationship between the plasma concentration and clinical efficacy of atomoxetine (110). Participants aged 6–17 were first administered 0.5–0.8 mg/kg of atomoxetine and the dose was increased every 2 weeks to a maximum of 1.8 mg/kg, with the exceptional cases in which adverse reactions emerged. The responder-related dose (excluding outliers) of 1.55 ± 0.28 mg/kg identified in this study may be helpful to clinicians. When titrating atomoxetine in general clinical practice, this response-related dose may be one of the targets. The minimal adverse reactions in this study mean that even in clinical situations where atomoxetine plasma levels cannot be measured, atomoxetine can be relatively safely increased to the above target dose (110).
Adverse Reactions
Atomoxetine was generally well tolerated in children and adolescents with ADHD (1, 26, 33, 35, 54, 101, 111–116). This section focuses primarily on data from trials including common and rare adverse reactions.
Common Adverse Reactions
The most common adverse reactions of atomoxetine in children with ADHD include gastrointestinal symptoms, sleep disturbances (somnolence), cardiovascular adverse reactions and other general disorders (irritability, dizziness, fatigue, headache) (103, 117). These four aspects will be described in detail below.
Gastrointestinal adverse reactions are one of the commonest adverse reactions in children with atomoxetine therapy (101), including appetite decrease, abdominal pain, vomiting and dyspepsia (117). With regard to an efficacy and safety extrapolation analysis (58), decreased appetite was the most common TEAE in atomoxetine-treated children at ages 6 to 7 (n = 565). In addition, the analysis concluded that in 5-year-old patients with ADHD, atomoxetine may improve ADHD symptoms, with some mood-related adverse reactions occurring at a higher rate (58). In short-term clinical trials, atomoxetine was reported to be more likely to have gastrointestinal adverse events than placebo (101). A meta-analysis of 6- to 8-week RCTs showed a decrease in appetite in 18.1% of 507 atomoxetine-treated patients aged 6–11 years compared to 5.3% of 339 placebo-treated patients (p < 0.001) (57). However, the incidence of gastrointestinal adverse reactions appeared to be highest within the first 1–3 months of treatment, and thereafter tended to subside over time in children (111).
Several short-term trials reported decreased weight in children after 6–8 weeks of atomoxetine therapy (118–122). In a 6-week RCT of 72 children with ADHD (ages 6 to 16), 9.7% (7/72) of the observation group had a loss of body mass compared with 6.1% (2/33) of the placebo group (121). A meta-analysis showed that children with ADHD (6 to 11 years old) had an average weight loss of 0.58 kg after atomoxetine treatment for 6 to 8 weeks (n = 507) (57). However, Spencer et al. (123) followed up the relationship between atomoxetine treatment and body mass for 5 years, and found that the body mass of children with ADHD showed the largest decline after 15-month atomoxetine treatment, partially recovered after 24 months, and recovered to the standard body mass after 36 months. The effect on the growth rate may be temporary. With the prolongation of treatment time, the growth level and speed may be gradually corrected (71, 124). Reductions in growth appear to be reversible in the long term (101). It may be that weight loss are secondary to decreased appetite, which may itself be related to other adverse reactions such as nausea, vomiting, and/or upper abdominal pain. The decreases in growth after atomoxetine treatment may be associated with gastrointestinal adverse reactions, but the long-term treatment has little effect on the physical growth of children with ADHD (58, 101).
Atomoxetine may cause somnolence more often than insomnia (113). Somnolence is the most common sleep-related adverse reaction associated with atomoxetine compared to stimulants (114). Previous studies showed that atomoxetine therapy significantly reduced sleep structure and sleep-wake cycle problems probably on account of lack of dopaminergic effects and appeared to be superior to stimulants (115, 125). In a meta-analysis of double-blind RCTs of atomoxetine treatment in children with ADHD, the results demonstrated that compared with placebo treatment, children with atomoxetine treatment had no significant increase in the incidence of sleep-onset insomnia and rarely resulted in treatment interruption (54). Additionally, atomoxetine was related to shorter sleep-onset latencies, lower frequency of insomnia, higher frequency of somnolence and smaller effects on subjective measures of sleep compared to methylphenidate (116). Although both atomoxetine and methylphenidate decreased nighttime awakenings, atomoxetine treatment was correlated with more frequent night awakenings (57, 116, 126). Compared with placebo, children with atomoxetine therapy exhibited significantly higher rates of somnolence and headache, although there was no significant difference in rates of headache between children and adolescents (57). Irritability, dizziness, fatigue, and headache are common in ADHD children with atomoxetine therapy (103). It is not only parts of clinical presentation, but also adverse reactions of some standard medications. In short-term RCTs of ADHD medications, there was an increased risk of headache for atomoxetine treatment compared to placebo (103, 127). The comprehensive results showed a significant association between atomoxetine treatment and headache in children with ADHD (127).
A meta-analysis of 16 studies reported age-group differences in the tolerability profile of atomoxetine (71). Younger children (6–7 years old) were more likely to experience more impairing sedative effects or abdominal pain or upset with atomoxetine treatment compared with placebo. Older children (aged 8–12 years) reported feeling sleepy or tired, which were more often described as irritable. In both age groups, those taking atomoxetine were more likely to complain of a diminished appetite and increased blood pressure than those taking placebo (71).
Elevated blood pressure and heart rate have been reported in patients with atomoxetine therapy (101). However, the effects of most patients on the cardiovascular system have no clinical significance (101, 128, 129). Hammerness et al. (130) found a statistically significant increase in heart rate in 6- and 7-year-old children with ADHD who received atomoxetine compared with placebo (p < 0.001). A study in Italy observed that the average heart rate in children with ADHD increased by 2.93 beats /min after 6 months of atomoxetine treatment compared with the baseline value, with a statistically significant difference (p < 0.001), while there was no statistically significant difference between the heart rate at 12th and 24th month compared with the baseline value (p > 0.05). The results indicated that the effect of atomoxetine on heart rate tended to decrease with the prolongation of time (131). The US label and the European SPC describe reports of moderately elevated heart rate and blood pressure in children and adolescents with atomoxetine treatment, which may be more pronounced in 8–12 % of pediatric patients. However, in long-term analyses (≥ 2 years) of pediatric patients with atomoxetine therapy, mean changes in blood pressure were usually within age norms and were generally not clinically significant. Few patients discontinued due to cardiovascular adverse reactions (101, 129). Interestingly, in a recent in vitro study using patch-clamp technique to perform electrophysiological experiments at the heterogeneously expressed human heart muscle sodium channels (hNav1.5) in human embryonic kidney cells, atomoxetine blocked sodium channels in a state- and use-dependent manner (132). It means that atomoxetine potentially has antiarrhythmic properties and reveals stronger anti-arrhythmic than pro-arrhythmic properties (132).
Rare Adverse Reactions
Based on previous research reports, liver injuries, suicidality, aggression/hostility, psychosis, seizures and prolonged QT interval are uncommon or rare (101). Rarely, atomoxetine may be associated with severe liver injury (101). According to Bangs and colleagues, during the 4-year post-marketing period, when atomoxetine exposure had reached approximately 4.3 million patients, three spontaneously reported cases of reversible hepatitis have been identified with relation to atomoxetine therapy (133). Another study, using the Italian ADHD National Registry, found that two of 68 pediatric patients experienced severe hepatic events after receiving unspecified doses of atomoxetine for 7 months and 10 months. In both cases, liver enzyme levels returned to normal after discontinuing atomoxetine therapy (118). In the long-term study of Eli Lilly's clinical trials database, Donnelly et al. (111) reported that ≤ 2% of 704 children and adolescents who received atomoxetine showed potentially clinically significant hepatic changes. These findings were based on laboratory tests for hepatic enzymes, including alanine aminotransferase (ALT), aspartate aminotransferase (AST) and alkaline phosphatase, and total bilirubin (111). Crucially, no patients had both a clinically significant increase in bilirubin (> 1.5 x ULN) combined with a significant increase in ALT (3 x ULN), which is a marker for potentially significant hepatic damage (111).
When children were treated with atomoxetine, small changes, or no changes/no clinically significant changes occurred in electrocardiograms (ECGs), including mean corrected QT (QTc) interval. Furthermore, atomoxetine is generally not associated with QT interval prolongation (134). There is a small but potential risk of QT interval prolongation (101).
The US prescribing information carries a black box warning on an elevated risk of suicidal ideation in children and adolescents with atomoxetine therapy (135) and it appears to be more common among atomoxetine than placebo recipients. A long-term (3–4 years) study found that among 714 children, 508 of them took atomoxetine for more than 4 years, and the incidence of suicidal ideation and behaviors was 0.8% (4/508) (111). Despite the black box warning on atomoxetine related suicidal ideation, no evidence existed for an increased rate of suicide related events associated with the use of atomoxetine in the register based longitudinal study (136). Although it cannot be ruled out that atomoxetine may increase the risk of suicide, there are other factors, such as depression and antisocial behaviors, which often comorbid ADHD, that may also lead to suicide in children (137).
With regard to aggression and hostility, these behaviors are reported more frequently but not statistically significantly different with atomoxetine compared with placebo (54, 111, 138), but the data suggest that there may be no association between atomoxetine therapy and increased risk of aggression/hostility, and more data are required to draw a firm conclusion. Moreover, psychosis including bipolar affective disorder (BPD) appear to be uncommon in atomoxetine-treated children with ADHD.
Conclusion
Atomoxetine, the first non-stimulant drug to treat ADHD, is a selective NRI (28, 32, 35). It highly selectively binds to the presynaptic membrane NE reuptake transporter and inhibits NE reuptake, but has low affinity with other neurotransmitters (28, 31–34). Therefore, it can increase the level of NE in the synaptic cleft and dopamine level in the PFC, enhance children's memory and attention, and significantly improve ADHD symptoms (34); However, dopamine level in nucleus accumbens will not be increased, so it will not cause abuse or addiction, and there is no potential risk of abuse and addiction (32); At the same time, atomoxetine does not increase dopamine level in the striatum, so it will not induce tic symptoms or increase dyspraxia (27, 32, 139). There are few adverse reactions and high safety, which has been widely used at present (26, 35, 54, 111, 117).
In addition, the metabolic half-life of atomoxetine in the central nervous system is long, and the inhibitory effect of once a daily on NET can be lasted up to 24 h, so as to control the symptoms of ADHD patients in a sustained and stable way (31). Therefore, atomoxetine has a better effect on the long-term treatment of ADHD and patients with psychiatric symptoms (35, 69). In addition to improving the core symptoms of ADHD, atomoxetine can also improve multiple functions of children with long-term treatment, including learning function, peer relationship, family relationship, cognitive function, executive function, social function and so on (8, 140–143). Some studies have shown that common comorbidities (such as ODD, anxiety disorder, TD and ASD) in ADHD patients are unaffected or improved after atomoxetine therapy (16, 27, 35, 72, 73). In children with ADHD combined with transient tic disorder, atomoxetine therapy will not affect the secretion of dopamine and 5-hydroxytryptamine receptors in the body, effectively avoiding the aggravation of tic disorder and having high bioavailability (144). Atomoxetine may also be the first-line treatment for patients with comorbid tics. Actually, atomoxetine is recommended as the first-line treatment for ADHD patients with comorbid tic disorder and comorbid anxiety disorder in the latest Chinese guideline revised in 2015 by the Chinese Medical Association.
In the process of treatment, clinicians should pay special attention to controlling the dose of atomoxetine. Generally, oral administration of atomoxetine to children can achieve better results. However, due to the relatively active or deficient CYP2D6 enzyme in some children, the absorption of atomoxetine will be affected to a certain extent (29, 30). Therefore, the rate of improvement of clinical symptoms and therapeutic effects of children after atomoxetine therapy vary from patient to patient. For further treatment, timely monitoring and individualized medication are required.
The previous mention of atomoxetine being more effective in older children than in younger children raises some thoughts. Preschool children are not fully developed. The proportion of organs to body weight, water content, plasma protein concentration, acid-base balance and other physiological conditions are changing, thereby changing the distribution and penetration of atomoxetine. Atomoxetine is excreted mainly in urine and a small amount in feces (145). The glomerular filtration rate is higher during childhood, thereby influencing the excretion. CYP2D6 genotype may be irrelevant. Atomoxetine is primarily metabolized by CYP2D6 (29, 30), but this enzyme is thought to develop very rapidly early and reach adult capacity at several months of age (58). Therefore, it is expected that there will be no difference in CYP2D6 activity and function in patients aged 4–5 years compared with the older children (58). In addition, the younger children are more likely to suffer acute epigastric pain and vomiting than older children, which may cause loss and fail to fully absorb atomoxetine. Older children reported feeling sleepy or tired (52, 71). In a study of patients aged 6–18 years in South Korea, the 10–15 age group had lower adherence than the 16–18 age groups (146). The high school students are under substantial academic pressures and great expectations from their parents, especially regarding university entry (146). This finding may explain why high school students exhibited better adherence compared with elementary and middle school students. Children with comorbidities were more likely to have higher adherence (147–149). The comorbid conditions of children led to the parents' diligence in controlling symptoms (147). However, younger children may not have accurate diagnosis of comorbidities. More studies to support this suggestion are needed in the future. Atomoxetine currently has three dosage forms: tablet, capsule, and oral liquid (145, 150). The younger children have difficulty swallowing tablets and capsules, and oral liquid has a poor taste, so it is difficult to swallow completely, which will have a certain effect on the efficacy. Last but not least, younger children are too young and immature to understand care from parents or physicians during atomoxetine therapy. They may avoid taking atomoxetine or not take it as prescribed.
In this review, the safety of atomoxetine was described from two aspects: common adverse reactions and rare adverse reactions. The most common adverse reactions including gastrointestinal adverse reactions and cardiovascular related adverse reactions may be related to the inhibition of NE by atomoxetine (111, 124, 151). And the most common adverse reactions usually appear in the first few months of medication. With the extension of treatment time, its adverse reactions gradually decrease and can be gradually tolerated. The occurrence of prolonged QT interval may be associated with CYP2D6, but this enzyme may not be related to liver function-related adverse reactions (151, 152). The adverse reactions of atomoxetine were generally mild or moderate, and severe adverse events were quite rare.
For ADHD children with atomoxetine therapy, adverse reactions should be evaluated and rational drug use should be guided. At the same time, parents of children with ADHD should be informed of the medication, understanding the common adverse reactions and countermeasures, so as to improve the medication compliance of children with ADHD. In summary, the application of atomoxetine in the clinical treatment of children with ADHD can significantly improve their learning ability and clinical symptoms.
Author Contributions
FC and Q-QL: conceptualization. DF and D-DW: writing—original draft preparation. DF, D-DW, H-LG, and FC: writing—review and editing. Y-HH, YX, XJ, and W-RF: performed the reference collection and summary. Y-ML and JX: critical review. FC and H-LG: funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Specially Appointed Medical Expert Project of the Jiangsu Commission of Health (2019) and Special Fund for Clinical Research of the Wu Jieping Medical Foundation (320.6750.2020-04-07). This study was also supported by the Scientific Research Support Foundation for Top Young Scholars at the Children's Hospital of Nanjing Medical University (2020).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
NE, Norepinephrine; ADHD, Attention deficit/hyperactivity disorder; NET, Norepinephrine transporter; PFC, Prefrontal cortex; CYP2D6, Cytochrome P450 2D6; MRI, Magnetic resonance imaging; fMRI, Functional magnetic resonance imaging; IFC, Inferior frontal cortex; DLPFC, Dorsolateral prefrontal cortex; DMN, Default mode network; FDA, Food and Drug Administration; NRI, Norepinephrine reuptake inhibitor; ODD, Oppositional defiant disorder; ASD, Autism spectrum disorder; TD, Tics disorders; TS, Tourette syndrome; MOA, Mechanism of action; SNRI, Selective norepinephrine reuptake inhibitor; FALFF, Fractional amplitude of low-frequency fluctuations; RS-fMRI, Resting-state functional magnetic resonance imaging; PET, Positron emission tomography; LTP, Long-term potentiation; RCT, Randomized controlled trial; ADHD-RS, ADHD-Rating Scale; OROS MPH, Osmotic release oral system methylphenidate; ADHD – RS – IV Parent: Inv, ADHD Rating Scale-IV Parent Version, Investigator Administered; LD, Learning disorders; DBDs, Disruptive behavior disorders; CD, Conduct disorder; MDD, Major depressive disorder; CDRS-R, Children's Depression Rating Scale-Revised; CGI-Tic, Clinical Global Impressions Tic; Neuro-S, Neurologic Severity; YGTSS, Yale Global Tic Severity Scale total score; TSSR, Tic Symptom Self-Report total score; RD, Reading disorder; ABC-H, Aberrant Behavior Checklist – Hyperactivity; SPC, Summary of Product Characteristics; CPIC, Clinical Pharmacogenetic Implementation Consortium; EM, Extensive metabolizer; PM, Poor metabolizers; IM, Intermediate metabolizer; UM, Ultrarapid metabolizer; CGI-P, Conners' Global Index-Parent Version; TEAEs, Treatment-emergent adverse events; hNav1.5, Heart muscle sodium channels; ALT, Alanine aminotransferase; AST, Aspartate aminotransferase; ECGs, Electrocardiograms; QTc, Corrected QT; BPD, Bipolar affective disorder; ADHD-RS-IV, Attention-Deficit/Hyperactivity Disorder Rating Scale-IV; PARS, Pediatric Anxiety Rating Scale; CGI, Clinical Global Impressions; CTRS-R:S, Conners Teacher Rating Scale-Revised: Short Form.
References
1. Simpson D, Plosker G. Atomoxetine: a review of its use in adults with attention deficit hyperactivity disorder. Drugs. (2004) 64:205–22. doi: 10.2165/00003495-200464020-00005
2. Elsayed NA, Yamamoto KM, Froehlich TE. Genetic influence on efficacy of pharmacotherapy for pediatric attention-deficit/hyperactivity disorder: overview and current status of research. CNS Drugs. (2020) 34:389–414. doi: 10.1007/s40263-020-00702-y
3. Wolraich M, Hagan J, Allan C, Chan E, Davison D, Earls M, et al. Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics. (2019) 144. doi: 10.1542/peds.2019-2528
4. Danielson M, Bitsko R, Ghandour R, Holbrook J, Kogan M, Blumberg S. Prevalence of parent-reported adhd diagnosis and associated treatment among u.s. children and adolescents, 2016. J Clin Child Adolesc Psychol. (2018) 47:199–212. doi: 10.1080/15374416.2017.1417860
5. Xu G, Strathearn L, Liu B, Yang B, Bao W. Twenty-year trends in diagnosed attention-deficit/hyperactivity disorder among US children and adolescents, 1997-2016. JAMA Netw Open. (2018) 1:e181471. doi: 10.1001/jamanetworkopen.2018.1471
6. Feldman HM, Reiff MI. Clinical practice. Attention deficit-hyperactivity disorder in children and adolescents. N Engl J Med. (2014) 370:838–46. doi: 10.1056/NEJMcp1307215
7. Del Campo N, Chamberlain S, Sahakian B, Robbins T. The roles of dopamine and noradrenaline in the pathophysiology and treatment of attention-deficit/hyperactivity disorder. Biol Psychiatry. (2011) 69:e145–57. doi: 10.1016/j.biopsych.2011.02.036
8. Wu C, Shang C, Lin H, Gau S. Differential treatment effects of methylphenidate and atomoxetine on executive functions in children with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. (2021) 31:187–96. doi: 10.1089/cap.2020.0146
9. Arnsten A, Rubia K. Neurobiological circuits regulating attention, cognitive control, motivation, and emotion: disruptions in neurodevelopmental psychiatric disorders. J Am Acad Child Adolesc Psychiatry. (2012) 51:356–67. doi: 10.1016/j.jaac.2012.01.008
10. Pereira-Sanchez V, Franco A, Vieira D, de Castro-Manglano P, Soutullo C, Milham M, et al. Systematic review: medication effects on brain intrinsic functional connectivity in patients with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. (2021) 60:222–35. doi: 10.1016/j.jaac.2020.10.013
11. Yadav S, Bhat A, Hashem S, Nisar S, Kamal M, Syed N, et al. Genetic variations influence brain changes in patients with attention-deficit hyperactivity disorder. Transl Psychiatry. (2021) 11:349. doi: 10.1038/s41398-021-01473-w
12. Lee J, Durand R, Gradinaru V, Zhang F, Goshen I, Kim D, et al. Global and local fMRI signals driven by neurons defined optogenetically by type and wiring. Nature. (2010) 465:788–92. doi: 10.1038/nature09108
13. Kowalczyk O, Cubillo A, Smith A, Barrett N, Giampietro V, Brammer M, et al. Methylphenidate and atomoxetine normalise fronto-parietal underactivation during sustained attention in ADHD adolescents. Eur Neuropsychopharmacol. (2019) 29:1102–16. doi: 10.1016/j.euroneuro.2019.07.139
14. Hart H, Radua J, Nakao T, Mataix-Cols D, Rubia K. Meta-analysis of functional magnetic resonance imaging studies of inhibition and attention in attention-deficit/hyperactivity disorder: exploring task-specific, stimulant medication, and age effects. JAMA psychiatry. (2013) 70:185–98. doi: 10.1001/jamapsychiatry.2013.277
15. Christakou A, Murphy C, Chantiluke K, Cubillo A, Smith A, Giampietro V, et al. Disorder-specific functional abnormalities during sustained attention in youth with Attention Deficit Hyperactivity Disorder (ADHD) and with autism. Mol Psychiatry. (2013) 18:236–44. doi: 10.1038/mp.2011.185
16. Tsujii N, Usami M, Naya N, Tsuji T, Mishima H, Horie J, et al. Efficacy and safety of medication for attention-deficit hyperactivity disorder in children and adolescents with common comorbidities: a systematic review. Neurology and therapy. (2021). doi: 10.1007/s40120-021-00249-0
17. Levy F. Applications of pharmacogenetics in children with attention-deficit/hyperactivity disorder. Pharmgenomics Pers Med. (2014) 7:349–56. doi: 10.2147/PGPM.S52844
18. Bolea-Alamañac B, Nutt D, Adamou M, Asherson P, Bazire S, Coghill D, et al. Evidence-based guidelines for the pharmacological management of attention deficit hyperactivity disorder: update on recommendations from the British Association for Psychopharmacology. J Psychopharmacol (Oxford, England). (2014) 28:179–203. doi: 10.1177/0269881113519509
19. Sciberras E, Efron D, Patel P, Mulraney M, Lee K, Mihalopoulos C, et al. Does the treatment of anxiety in children with Attention-Deficit/Hyperactivity Disorder (ADHD) using cognitive behavioral therapy improve child and family outcomes? Protocol for a randomized controlled trial. BMC psychiatry. (2019) 19:359. doi: 10.1186/s12888-019-2276-3
20. Gould K, Porter M, Lyneham H, Hudson J. Cognitive-behavioral therapy for children with anxiety and comorbid attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. (2018) 57:481–90.e2. doi: 10.1016/j.jaac.2018.03.021
21. Pan M, Huang F, Zhao M, Wang Y, Wang Y, Qian Q, et al. comparison of efficacy between cognitive behavioral therapy (CBT) and CBT combined with medication in adults with attention-deficit/hyperactivity disorder (ADHD). Psychiatry Res. (2019) 279:23–33. doi: 10.1016/j.psychres.2019.06.040
22. Walls M, Allen C, Cabral H, Kazis L, Bair-Merritt M. Receipt of medication and behavioral therapy among a national sample of school-age children diagnosed with attention-deficit/hyperactivity disorder. Acad Pediatr. (2018) 18:256–65. doi: 10.1016/j.acap.2017.10.003
23. Cortese S. Pharmacologic treatment of attention deficit-hyperactivity disorder. N Engl J Med. (2020) 383:1050–6. doi: 10.1056/NEJMra1917069
24. Cortese S, Adamo N, Del Giovane C, Mohr-Jensen C, Hayes AJ, Carucci S, et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis. The Lancet Psychiatry. (2018) 5:727–38. doi: 10.1016/S2215-0366(18)30269-4
25. MacKenzie KR, Zhao M, Barzi M, Wang J, Bissig KD, Maletic-Savatic M, et al. Metabolic profiling of norepinephrine reuptake inhibitor atomoxetine. Eur J Pharm Sci. (2020) 153:105488. doi: 10.1016/j.ejps.2020.105488
26. Childress AC, A. critical appraisal of atomoxetine in the management of ADHD. Ther Clin Risk Manag. (2016) 12:27–39. doi: 10.2147/TCRM.S59270
27. Savill NC, Buitelaar JK, Anand E, Day KA, Treuer T, Upadhyaya HP, et al. The efficacy of atomoxetine for the treatment of children and adolescents with attention-deficit/hyperactivity disorder: a comprehensive review of over a decade of clinical research. CNS Drugs. (2015) 29:131–51. doi: 10.1007/s40263-014-0224-9
28. Camporeale A, Porsdal V, De Bruyckere K, Tanaka Y, Upadhyaya H, Deix C, et al. Safety and tolerability of atomoxetine in treatment of attention deficit hyperactivity disorder in adult patients: an integrated analysis of 15 clinical trials. J Psychopharmacol. (2015) 29:3–14. doi: 10.1177/0269881114560183
29. Brown J, Abdel-Rahman S, van Haandel L, Gaedigk A, Lin Y, Leeder J. Single dose, CYP2D6 genotype-stratified pharmacokinetic study of atomoxetine in children with ADHD. Clin Pharmacol Ther. (2016) 99:642–50. doi: 10.1002/cpt.319
30. Brown JT, Bishop JR, Sangkuhl K, Nurmi EL, Mueller DJ, Dinh JC, et al. Clinical pharmacogenetics implementation consortium guideline for cytochrome P450 (CYP)2D6 genotype and atomoxetine therapy. Clin Pharmacol Ther. (2019) 106:94–102. doi: 10.1002/cpt.1409
31. Clemow D, Bushe C. Atomoxetine in patients with ADHD: A clinical and pharmacological review of the onset, trajectory, duration of response and implications for patients. J Psychopharmacol (Oxford, England). (2015) 29:1221–30. doi: 10.1177/0269881115602489
32. Bymaster F, Katner J, Nelson D, Hemrick-Luecke S, Threlkeld P, Heiligenstein J, et al. Atomoxetine increases extracellular levels of norepinephrine and dopamine in prefrontal cortex of rat: a potential mechanism for efficacy in attention deficit/hyperactivity disorder. Neuropsychopharmacology: official publication of the American College of Neuropsychopharmacology. (2002) 27:699–711. doi: 10.1016/S0893-133X(02)00346-9
33. Kratochvil C, Vaughan B, Daughton J, Mayfield-Jorgensen M, Burke W. Atomoxetine in the treatment of attention deficit hyperactivity disorder. Expert Rev Neurother. (2004) 4:601–11. doi: 10.1586/14737175.4.4.601
34. Callahan PM, Plagenhoef MR, Blake DT, Terry AV. Jr. Atomoxetine improves memory and other components of executive function in young-adult rats and aged rhesus monkeys. Neuropharmacology. (2019) 155:65–75. doi: 10.1016/j.neuropharm.2019.05.016
35. Garnock-Jones K, Keating G. Atomoxetine: a review of its use in attention-deficit hyperactivity disorder in children and adolescents. Paediatr Drugs. (2009) 11:203–26. doi: 10.2165/00148581-200911030-00005
36. Arnsten A. Catecholamine influences on dorsolateral prefrontal cortical networks. Biol Psychiatry. (2011) 69:e89–99. doi: 10.1016/j.biopsych.2011.01.027
37. Barr CL, Kroft J, Feng Y, Wigg K, Roberts W, Malone M, et al. The norepinephrine transporter gene and attention-deficit hyperactivity disorder. Am J Med Genet. (2002) 114:255–9. doi: 10.1002/ajmg.10193
38. Chamberlain S, Hampshire A, Müller U, Rubia K, Del Campo N, Craig K, et al. Atomoxetine modulates right inferior frontal activation during inhibitory control: a pharmacological functional magnetic resonance imaging study. Biol Psychiatry. (2009) 65:550–5. doi: 10.1016/j.biopsych.2008.10.014
39. Shang C, Yan C, Lin H, Tseng W, Castellanos F, Gau S. Differential effects of methylphenidate and atomoxetine on intrinsic brain activity in children with attention deficit hyperactivity disorder. Psychol Med. (2016) 46:3173–85. doi: 10.1017/S0033291716001938
40. Chen T, Wu S, Welge J, Dixon S, Shahana N, Huddleston D, et al. Reduced short interval cortical inhibition correlates with atomoxetine response in children with attention-deficit hyperactivity disorder (ADHD). J Child Neurol. (2014) 29:1672–9. doi: 10.1177/0883073813513333
41. Rubia K, Smith A, Brammer M, Toone B, Taylor E. Abnormal brain activation during inhibition and error detection in medication-naive adolescents with ADHD. Am J Psychiatry. (2005) 162:1067–75. doi: 10.1176/appi.ajp.162.6.1067
42. Lin H, Gau S. Atomoxetine treatment strengthens an anti-correlated relationship between functional brain networks in medication-naïve adults with attention-deficit hyperactivity disorder: a randomized double-blind placebo-controlled clinical trial. Int J Neuropsychopharmacol. (2015) 19:pyv094. doi: 10.1093/ijnp/pyv094
43. Ding Y, Naganawa M, Gallezot J, Nabulsi N, Lin S, Ropchan J, et al. Clinical doses of atomoxetine significantly occupy both norepinephrine and serotonin transports: Implications on treatment of depression and ADHD. Neuroimage. (2014) 86:164–71. doi: 10.1016/j.neuroimage.2013.08.001
44. Piña R, Rozas C, Contreras D, Hardy P, Ugarte G, Zeise M, et al. Atomoxetine Reestablishes Long Term Potentiation in a Mouse Model of Attention Deficit/Hyperactivity Disorder. Neuroscience. (2020) 439:268–74. doi: 10.1016/j.neuroscience.2019.10.040
45. Buitelaar J, Danckaerts M, Gillberg C, Zuddas A, Becker K, Bouvard M, et al. A prospective, multicenter, open-label assessment of atomoxetine in non-North American children and adolescents with ADHD. Eur Child Adolesc Psychiatry. (2004) 13:249–57. doi: 10.1007/s00787-004-0401-3
46. Michelson D, Faries D, Wernicke J, Kelsey D, Kendrick K, Sallee F, et al. Atomoxetine in the treatment of children and adolescents with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled, dose-response study. Pediatrics. (2001) 108:E83. doi: 10.1542/peds.108.5.e83
47. Griffiths K, Leikauf J, Tsang T, Clarke S, Hermens D, Efron D, et al. Response inhibition and emotional cognition improved by atomoxetine in children and adolescents with ADHD: The ACTION randomized controlled trial. J Psychiatr Res. (2018) 102:57–64. doi: 10.1016/j.jpsychires.2018.03.009
48. Kratochvil C, Vaughan B, Stoner J, Daughton J, Lubberstedt B, Murray D, et al. A double-blind, placebo-controlled study of atomoxetine in young children with ADHD. Pediatrics. (2011) 127:e862–8. doi: 10.1542/peds.2010-0825
49. Michelson D, Buitelaar J, Danckaerts M, Gillberg C, Spencer T, Zuddas A, et al. Relapse prevention in pediatric patients with ADHD treated with atomoxetine: a randomized, double-blind, placebo-controlled study. J Am Acad Child Adolesc Psychiatry. (2004) 43:896–904. doi: 10.1097/01.chi.0000125089.35109.81
50. Newcorn J, Michelson D, Kratochvil C, Allen A, Ruff D, Moore R. Low-dose atomoxetine for maintenance treatment of attention-deficit/hyperactivity disorder. Pediatrics. (2006) 118:e1701–6. doi: 10.1542/peds.2005-2999
51. Buitelaar J, Michelson D, Danckaerts M, Gillberg C, Spencer T, Zuddas A, et al. A randomized, double-blind study of continuation treatment for attention-deficit/hyperactivity disorder after 1 year. Biol Psychiatry. (2007) 61:694–9. doi: 10.1016/j.biopsych.2006.03.066
52. Kratochvil C, Milton D, Vaughan B, Greenhill L. Acute atomoxetine treatment of younger and older children with ADHD: a meta-analysis of tolerability and efficacy. Child Adolesc Psychiatry Ment Health. (2008) 2:25. doi: 10.1186/1753-2000-2-25
53. Newcorn J, Kratochvil C, Allen A, Casat C, Ruff D, Moore R, et al. Atomoxetine and osmotically released methylphenidate for the treatment of attention deficit hyperactivity disorder: acute comparison and differential response. Am J Psychiatry. (2008) 165:721–30. doi: 10.1176/appi.ajp.2007.05091676
54. Schwartz S, Correll C. Efficacy and safety of atomoxetine in children and adolescents with attention-deficit/hyperactivity disorder: results from a comprehensive meta-analysis and metaregression. J Am Acad Child Adolesc Psychiatry. (2014) 53:174–87. doi: 10.1016/j.jaac.2013.11.005
55. Gau S, Shang C. Improvement of executive functions in boys with attention deficit hyperactivity disorder: an open-label follow-up study with once-daily atomoxetine. Int J Neuropsychopharmacol. (2010) 13:243–56. doi: 10.1017/S1461145709990836
56. Williams L, Tsang T, Clarke S, Kohn M. An 'integrative neuroscience' perspective on ADHD: linking cognition, emotion, brain and genetic measures with implications for clinical support. Expert Rev Neurother. (2010) 10:1607–21. doi: 10.1586/ern.10.140
57. Wilens T, Kratochvil C, Newcorn J, Gao H. Do children and adolescents with ADHD respond differently to atomoxetine? J Am Acad Child Adolesc Psychiatry. (2006) 45:149–57. doi: 10.1097/01.chi.0000190352.90946.0b
58. Upadhyaya H, Kratochvil C, Ghuman J, Camporeale A, Lipsius S, D'Souza D, et al. Efficacy and safety extrapolation analyses for atomoxetine in young children with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. (2015) 25:799–809. doi: 10.1089/cap.2014.0001
59. Conners C. Forty years of methylphenidate treatment in Attention-Deficit/ Hyperactivity Disorder. J Atten Disord. (2002) S17–30. doi: 10.1177/070674370200601S04
60. Hanwella R, Senanayake M, de Silva V. Comparative efficacy and acceptability of methylphenidate and atomoxetine in treatment of attention deficit hyperactivity disorder in children and adolescents: a meta-analysis. BMC Psychiatry. (2011) 11:176. doi: 10.1186/1471-244X-11-176
61. Gibson A, Bettinger T, Patel N, Crismon M. Atomoxetine vs. stimulants for treatment of attention deficit/hyperactivity disorder. Ann Pharmacother. (2006) 40:1134–42. doi: 10.1345/aph.1G582
62. Kemner J, Starr H, Ciccone P, Hooper-Wood C, Crockett R. Outcomes of OROS methylphenidate compared with atomoxetine in children with ADHD: a multicenter, randomized prospective study. Adv Ther. (2005) 22:498–512. doi: 10.1007/BF02849870
63. Yildiz O, Sismanlar S, Memik N, Karakaya I, Agaoglu B. Atomoxetine and methylphenidate treatment in children with ADHD: the efficacy, tolerability and effects on executive functions. Child Psychiatry Hum Dev. (2011) 42:257–69. doi: 10.1007/s10578-010-0212-3
64. Shang C, Pan Y, Lin H, Huang L, Gau S. An open-label, randomized trial of methylphenidate and atomoxetine treatment in children with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. (2015) 25:566–73. doi: 10.1089/cap.2015.0035
65. Su Y, Yang L, Stein M, Cao Q, Wang Y. Osmotic release oral system methylphenidate vs. atomoxetine for the treatment of attention-deficit/hyperactivity disorder in chinese youth: 8-week comparative efficacy and 1-year follow-up. J Child Adolesc Psychopharmacol. (2016) 26:362–71. doi: 10.1089/cap.2015.0031
66. Tanaka Y, Rohde L, Jin L, Feldman P, Upadhyaya H, A. meta-analysis of the consistency of atomoxetine treatment effects in pediatric patients with attention-deficit/hyperactivity disorder from 15 clinical trials across four geographic regions. J Child Adolesc Psychopharmacol. (2013) 23:262–70. doi: 10.1089/cap.2012.0049
67. Durell T, Pumariega A, Rothe E, Tamayo J, Baron D, Williams D. Effects of open-label atomoxetine on African-American and Caucasian pediatric outpatients with attention-deficit/hyperactivity disorder. Ann Clin Psychiatry. (2009) 21:26–37.
68. Tamayo J, Pumariega A, Rothe E, Kelsey D, Allen A, Vélez-Borrás J, et al. Latino vs. Caucasian response to atomoxetine in attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. (2008) 18:44–53. doi: 10.1089/cap.2006.0132
69. Huang Y, Tsai M. Long-term outcomes with medications for attention-deficit hyperactivity disorder: current status of knowledge. CNS Drugs. (2011) 25:539–54. doi: 10.2165/11589380-000000000-00000
70. Wilens T, Newcorn J, Kratochvil C, Gao H, Thomason C, Rogers A, et al. Long-term atomoxetine treatment in adolescents with attention-deficit/hyperactivity disorder. J Pediatr. (2006) 149:112–9. doi: 10.1016/j.jpeds.2006.01.052
71. Kratochvil C, Wilens T, Greenhill L, Gao H, Baker K, Feldman P, et al. Effects of long-term atomoxetine treatment for young children with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. (2006) 45:919–27. doi: 10.1097/01.chi.0000222788.34229.68
72. Hutchison S, Ghuman J, Ghuman H, Karpov I, Schuster J. Efficacy of atomoxetine in the treatment of attention-deficit hyperactivity disorder in patients with common comorbidities in children, adolescents and adults: a review. Ther Adv Psychopharmacol. (2016) 6:317–34. doi: 10.1177/2045125316647686
73. Dell'Agnello G, Zuddas A, Masi G, Curatolo P, Besana D, Rossi A. Use of atomoxetine in patients with attention-deficit hyperactivity disorder and co-morbid conditions. CNS Drugs. (2009) 23:739–53. doi: 10.2165/11314350-000000000-00000
74. Kelsey D, Sumner C, Casat C, Coury D, Quintana H, Saylor K, et al. Once-daily atomoxetine treatment for children with attention-deficit/hyperactivity disorder, including an assessment of evening and morning behavior: a double-blind, placebo-controlled trial. Pediatrics. (2004) 114:e1–8. doi: 10.1542/peds.114.1.e1
75. Weiss M, Tannock R, Kratochvil C, Dunn D, Velez-Borras J, Thomason C, et al. A randomized, placebo-controlled study of once-daily atomoxetine in the school setting in children with ADHD. J Am Acad Child Adolesc Psychiatry. (2005) 44:647–55. doi: 10.1097/01.chi.0000163280.47221.c9
76. Spencer T, Heiligenstein J, Biederman J, Faries D, Kratochvil C, Conners C, et al. Results from 2 proof-of-concept, placebo-controlled studies of atomoxetine in children with attention-deficit/hyperactivity disorder. J Clin Psychiatry. (2002) 63:1140–7. doi: 10.4088/JCP.v63n1209
77. Newcorn J, Spencer T, Biederman J, Milton D, Michelson D. Atomoxetine treatment in children and adolescents with attention-deficit/hyperactivity disorder and comorbid oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry. (2005) 44:240–8. doi: 10.1097/00004583-200503000-00008
78. Bangs M, Hazell P, Danckaerts M, Hoare P, Coghill D, Wehmeier P, et al. Atomoxetine for the treatment of attention-deficit/hyperactivity disorder and oppositional defiant disorder. Pediatrics. (2008) 121:e314–20. doi: 10.1542/peds.2006-1880
79. Michelson D, Allen A, Busner J, Casat C, Dunn D, Kratochvil C, et al. Once-daily atomoxetine treatment for children and adolescents with attention deficit hyperactivity disorder: a randomized, placebo-controlled study. Am J Psychiatry. (2002) 159:1896–901. doi: 10.1176/appi.ajp.159.11.1896
80. Geller D, Donnelly C, Lopez F, Rubin R, Newcorn J, Sutton V, et al. Atomoxetine treatment for pediatric patients with attention-deficit/hyperactivity disorder with comorbid anxiety disorder. J Am Acad Child Adolesc Psychiatry. (2007) 46:1119–27. doi: 10.1097/chi.0b013e3180ca8385
81. Spencer T, Sallee F, Gilbert D, Dunn D, McCracken J, Coffey B, et al. Atomoxetine treatment of ADHD in children with comorbid Tourette syndrome. J Atten Disord. (2008) 11:470–81. doi: 10.1177/1087054707306109
82. Allen A, Kurlan R, Gilbert D, Coffey B, Linder S, Lewis D, et al. Atomoxetine treatment in children and adolescents with ADHD and comorbid tic disorders. Neurology. (2005) 65:1941–9. doi: 10.1212/01.wnl.0000188869.58300.a7
83. Patra S, Nebhinani N, Viswanathan A, Kirubakaran R. Atomoxetine for attention deficit hyperactivity disorder in children and adolescents with autism: A systematic review and meta-analysis. Autism Res. (2019) 12:542–52. doi: 10.1002/aur.2059
84. Dittmann R, Schacht A, Helsberg K, Schneider-Fresenius C, Lehmann M, Lehmkuhl G, et al. Atomoxetine vs. placebo in children and adolescents with attention-deficit/hyperactivity disorder and comorbid oppositional defiant disorder: a double-blind, randomized, multicenter trial in Germany. J Child Adolesc Psychopharmacol. (2011) 21:97–110. doi: 10.1089/cap.2009.0111
85. Bangs M, Emslie G, Spencer T, Ramsey J, Carlson C, Bartky E, et al. Efficacy and safety of atomoxetine in adolescents with attention-deficit/hyperactivity disorder and major depression. J Child Adolesc Psychopharmacol. (2007) 17:407–20. doi: 10.1089/cap.2007.0066
86. Kratochvil C, Newcorn J, Arnold L, Duesenberg D, Emslie G, Quintana H, et al. Atomoxetine alone or combined with fluoxetine for treating ADHD with comorbid depressive or anxiety symptoms. J Am Acad Child Adolesc Psychiatry. (2005) 44:915–24. doi: 10.1097/01.chi.0000169012.81536.38
87. Arnold L, Aman M, Cook A, Witwer A, Hall K, Thompson S, et al. Atomoxetine for hyperactivity in autism spectrum disorders: placebo-controlled crossover pilot trial. J Am Acad Child Adolesc Psychiatry. (2006) 45:1196–205. doi: 10.1097/01.chi.0000231976.28719.2a
88. Harfterkamp M, van de Loo-Neus G, Minderaa R, van der Gaag R, Escobar R, Schacht A, et al. A randomized double-blind study of atomoxetine vs. placebo for attention-deficit/hyperactivity disorder symptoms in children with autism spectrum disorder. J Am Acad Child Adolesc Psychiatry. (2012) 51:733–41. doi: 10.1016/j.jaac.2012.04.011
89. Jensen P, Hinshaw S, Kraemer H, Lenora N, Newcorn J, Abikoff H, et al. ADHD comorbidity findings from the MTA study: comparing comorbid subgroups. J Am Acad Child Adolesc Psychiatry. (2001) 40:147–58. doi: 10.1097/00004583-200102000-00009
90. Wolraich M, Wibbelsman C, Brown T, Evans S, Gotlieb E, Knight J, et al. Attention-deficit/hyperactivity disorder among adolescents: a review of the diagnosis, treatment, and clinical implications. Pediatrics. (2005) 115:1734–46. doi: 10.1542/peds.2004-1959
91. Kaplan S, Heiligenstein J, West S, Busner J, Harder D, Dittmann R, et al. Efficacy and safety of atomoxetine in childhood attention-deficit/hyperactivity disorder with comorbid oppositional defiant disorder. J Atten Disord. (2004) 8:45–52. doi: 10.1177/108705470400800202
92. Inci S, Ipci M, Akyol Ardiç U, Ercan E. Psychiatric comorbidity and demographic characteristics of 1,000 children and adolescents with ADHD in Turkey. J Atten Disord. (2019) 23:1356–67. doi: 10.1177/1087054716666954
93. Mohammadi M, Zarafshan H, Khaleghi A, Ahmadi N, Hooshyari Z, Mostafavi S, et al. Prevalence of ADHD and its comorbidities in a population-based sample. J Atten Disord. (2021) 25:1058–67. doi: 10.1177/1087054719886372
94. Sexton C, Gelhorn H, Bell J, Classi P. The co-occurrence of reading disorder and ADHD: epidemiology, treatment, psychosocial impact, and economic burden. J Learn Disabil. (2012) 45:538–64. doi: 10.1177/0022219411407772
95. Shaywitz S, Shaywitz B, Wietecha L, Wigal S, McBurnett K, Williams D, et al. Effect of atomoxetine treatment on reading and phonological skills in children with dyslexia or attention-deficit/hyperactivity disorder and comorbid dyslexia in a randomized, placebo-controlled trial. J Child Adolesc Psychopharmacol. (2017) 27:19–28. doi: 10.1089/cap.2015.0189
96. Clemow D, Bushe C, Mancini M, Ossipov M, Upadhyaya H, A. review of the efficacy of atomoxetine in the treatment of attention-deficit hyperactivity disorder in children and adult patients with common comorbidities. Neuropsychiatr Dis Treat. (2017) 13:357–71. doi: 10.2147/NDT.S115707
97. Shaywitz B, Williams D, Fox B, Wietecha L. Reading outcomes of children and adolescents with attention-deficit/hyperactivity disorder and dyslexia following atomoxetine treatment. J Child Adolesc Psychopharmacol. (2014) 24:419–25. doi: 10.1089/cap.2013.0148
98. Grzadzinski R, Dick C, Lord C, Bishop S. Parent-reported and clinician-observed autism spectrum disorder (ASD) symptoms in children with attention deficit/hyperactivity disorder (ADHD): implications for practice under DSM-5. Mol Autism. (2016) 7:7. doi: 10.1186/s13229-016-0072-1
99. Rodrigues R, Lai M, Beswick A, Gorman D, Anagnostou E, Szatmari P, et al. Practitioner Review: Pharmacological treatment of attention-deficit/hyperactivity disorder symptoms in children and youth with autism spectrum disorder: a systematic review and meta-analysis. J Child Psychol Psychiatry. (2021) 62:680–700. doi: 10.1111/jcpp.13305
100. Ghanizadeh A. Atomoxetine for treating ADHD symptoms in autism: a systematic review. J Atten Disord. (2013) 17:635–40. doi: 10.1177/1087054712443154
101. Reed V, Buitelaar J, Anand E, Day K, Treuer T, Upadhyaya H, et al. The Safety of Atomoxetine for the Treatment of Children and Adolescents with Attention-Deficit/Hyperactivity Disorder: A Comprehensive Review of Over a Decade of Research. CNS Drugs. (2016) 30:603–28. doi: 10.1007/s40263-016-0349-0
102. Spencer T, Biederman J, Heiligenstein J, Wilens T, Faries D, Prince J, et al. An open-label, dose-ranging study of atomoxetine in children with attention deficit hyperactivity disorder. J Child Adolesc Psychopharmacol. (2001) 11:251–65. doi: 10.1089/10445460152595577
103. Mechler K, Banaschewski T, Hohmann S, Häge A. Evidence-based pharmacological treatment options for ADHD in children and adolescents. Pharmacol Therapeut. (2021) 107940. doi: 10.1016/j.pharmthera.2021.107940
104. Kratochvil C, Michelson D, Newcorn J, Weiss M, Busner J, Moore R, et al. High-dose atomoxetine treatment of ADHD in youths with limited response to standard doses. J Am Acad Child Adolesc Psychiatry. (2007) 46:1128–37. doi: 10.1097/chi.0b013e318074eeb3
105. Chalon S, Desager J, Desante K, Frye R, Witcher J, Long A, et al. Effect of hepatic impairment on the pharmacokinetics of atomoxetine and its metabolites. Clin Pharmacol Ther. (2003) 73:178–91. doi: 10.1067/mcp.2003.25
106. Gaedigk A, Simon S, Pearce R, Bradford L, Kennedy M, Leeder J. The CYP2D6 activity score: translating genotype information into a qualitative measure of phenotype. Clin Pharmacol Ther. (2008) 83:234–42. doi: 10.1038/sj.clpt.6100406
107. Xia Y, Guo H, Hu Y, Long J, Chen J, Chen F, et al. Determination of atomoxetine levels in human plasma using LC-MS/MS and clinical application to Chinese children with ADHD based on CPIC guidelines. Anal Methods. (2021) 13:2434–41. doi: 10.1039/d1ay00521a
108. Block S, Kelsey D, Coury D, Lewis D, Quintana H, Sutton V, et al. Once-daily atomoxetine for treating pediatric attention-deficit/hyperactivity disorder: comparison of morning and evening dosing. Clin Pediatr. (2009) 48:723–33. doi: 10.1177/0009922809335321
109. Wietecha L, Ruff D, Allen A, Greenhill L, Newcorn J. Atomoxetine tolerability in pediatric and adult patients receiving different dosing strategies. J Clin Psychiatry. (2013) 74:1217–23. doi: 10.4088/JCP.12m07991
110. Sugimoto A, Suzuki Y, Orime N, Hayashi T, Yoshinaga K, Egawa J, et al. The lowest effective plasma concentration of atomoxetine in pediatric patients with attention deficit/hyperactivity disorder: A non-randomized prospective interventional study. Medicine. (2021) 100:e26552. doi: 10.1097/MD.0000000000026552
111. Donnelly C, Bangs M, Trzepacz P, Jin L, Zhang S, Witte MM, et al. Safety and tolerability of atomoxetine over 3 to 4 years in children and adolescents with ADHD. J Am Acad Child Adolesc Psychiatry. (2009) 48:176–85. doi: 10.1097/CHI.0b013e318193060e
112. Wigal S. Efficacy and safety limitations of attention-deficit hyperactivity disorder pharmacotherapy in children and adults. CNS Drugs. (2009) 21–31. doi: 10.2165/00023210-200923000-00004
113. Cortese S, Holtmann M, Banaschewski T, Buitelaar J, Coghill D, Danckaerts M, et al. Practitioner review: current best practice in the management of adverse events during treatment with ADHD medications in children and adolescents. J Child Psychol Psychiatry. (2013) 54:227–46. doi: 10.1111/jcpp.12036
114. Hvolby A. Associations of sleep disturbance with ADHD: implications for treatment. Atten Defic Hyperact Disord. (2015) 7:1–18. doi: 10.1007/s12402-014-0151-0
115. Padilha S, Virtuoso S, Tonin F, Borba H, Pontarolo R. Efficacy and safety of drugs for attention deficit hyperactivity disorder in children and adolescents: a network meta-analysis. Eur Child Adolesc Psychiatry. (2018) 27:1335–45. doi: 10.1007/s00787-018-1125-0
116. Sangal R, Owens J, Allen A, Sutton V, Schuh K, Kelsey D. Effects of atomoxetine and methylphenidate on sleep in children with ADHD. Sleep. (2006) 29:1573–85. doi: 10.1093/sleep/29.12.1573
117. Cheng J, Chen R, Ko J, Ng E. Efficacy and safety of atomoxetine for attention-deficit/hyperactivity disorder in children and adolescents-meta-analysis and meta-regression analysis. Psychopharmacology. (2007) 194:197–209. doi: 10.1007/s00213-007-0840-x
118. Ruggiero S, Rafaniello C, Bravaccio C, Grimaldi G, Granato R, Pascotto A, et al. Safety of attention-deficit/hyperactivity disorder medications in children: an intensive pharmacosurveillance monitoring study. J Child Adolesc Psychopharmacol. (2012) 22:415–22. doi: 10.1089/cap.2012.0003
119. Cardo E, Porsdal V, Quail D, Fuentes J, Steer C, Montoya A, et al. Fast vs. slow switching from stimulants to atomoxetine in children and adolescents with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. (2013) 23:252–61. doi: 10.1089/cap.2012.0027
120. Dittmann R, Cardo E, Nagy P, Anderson C, Bloomfield R, Caballero B, et al. Efficacy and safety of lisdexamfetamine dimesylate and atomoxetine in the treatment of attention-deficit/hyperactivity disorder: a head-to-head, randomized, double-blind, phase IIIb study. CNS Drugs. (2013) 27:1081–92. doi: 10.1007/s40263-013-0104-8
121. Martenyi F, Zavadenko N, Jarkova N, Yarosh A, Soldatenkova V, Bardenstein L, et al. Atomoxetine in children and adolescents with attention-deficit/hyperactivity disorder: a 6-week, randomized, placebo-controlled, double-blind trial in Russia. Eur Child Adolesc Psychiatry. (2010) 19:57–66. doi: 10.1007/s00787-009-0042-7
122. Pott W, Albayrak O, Hinney A, Hebebrand J, Pauli-Pott U. Successful treatment with atomoxetine of an adolescent boy with attention deficit/hyperactivity disorder, extreme obesity, and reduced melanocortin 4 receptor function. Obes Facts. (2013) 6:109–15. doi: 10.1159/000348792
123. Spencer T, Kratochvil C, Sangal R, Saylor K, Bailey C, Dunn D, et al. Effects of atomoxetine on growth in children with attention-deficit/hyperactivity disorder following up to five years of treatment. J Child Adolesc Psychopharmacol. (2007) 17:689–700. doi: 10.1089/cap.2006.0100
124. Spencer T, Newcorn J, Kratochvil C, Ruff D, Michelson D, Biederman J. Effects of atomoxetine on growth after 2-year treatment among pediatric patients with attention-deficit/hyperactivity disorder. Pediatrics. (2005) 116:e74–80. doi: 10.1542/peds.2004-0624
125. Yektaş Ç, Tufan A, Sarigedik E. Sleep habits of children diagnosed with attention/ deficit/ hyperactivity disorder and effects of treatment on sleep related parameters. Asian J Psychiatr. (2020) 52:102045. doi: 10.1016/j.ajp.2020.102045
126. Stein M, Weiss M, Hlavaty L, ADHD. treatments, sleep, and sleep problems: complex associations. Neurotherapeutics. (2012) 9:509–17. doi: 10.1007/s13311-012-0130-0
127. Pan P, Jonsson U, Sahpazoglu Çakmak S, Häge A, Hohmann S, Nobel Norrman H, et al. Headache in ADHD as comorbidity and a side effect of medications: a systematic review and meta-analysis. Psychological Med. (2021) 1–12. doi: 10.1017/S0033291721004141
128. Houghton R, de Vries F, Loss G. Psychostimulants/atomoxetine and serious cardiovascular events in children with ADHD or autism spectrum disorder. CNS Drugs. (2020) 34:93–101. doi: 10.1007/s40263-019-00686-4
129. Hennissen L, Bakker M, Banaschewski T, Carucci S, Coghill D, Danckaerts M, et al. Cardiovascular effects of stimulant and non-stimulant medication for children and adolescents with ADHD: a systematic review and meta-analysis of trials of methylphenidate, amphetamines and atomoxetine. CNS Drugs. (2017) 31:199–215. doi: 10.1007/s40263-017-0410-7
130. Hammerness P, Karampahtsis C, Babalola R, Alexander M. Attention-deficit/hyperactivity disorder treatment: what are the long-term cardiovascular risks? Expert Opin Drug Saf. (2015) 14:543–51. doi: 10.1517/14740338.2015.1011620
131. Arcieri R, Germinario E, Bonati M, Masi G, Zuddas A, Vella S, et al. Cardiovascular measures in children and adolescents with attention-deficit/hyperactivity disorder who are new users of methylphenidate and atomoxetine. J Child Adolesc Psychopharmacol. (2012) 22:423–31. doi: 10.1089/cap.2012.0014
132. Föhr K, Nastos A, Fauler M, Zimmer T, Jungwirth B, Messerer D. Block of voltage-gated sodium channels by atomoxetine in a state- and use-dependent manner. Front Pharmacol. (2021) 12:622489. doi: 10.3389/fphar.2021.622489
133. Bangs M, Jin L, Zhang S, Desaiah D, Allen A, Read H, et al. Hepatic events associated with atomoxetine treatment for attention-deficit hyperactivity disorder. Drug safety. (2008) 31:345–54. doi: 10.2165/00002018-200831040-00008
134. Langley K, Fowler T, Ford T, Thapar A, van den Bree M, Harold G, et al. Adolescent clinical outcomes for young people with attention-deficit hyperactivity disorder. Br J Psychiatry. (2010) 196:235–40. doi: 10.1192/bjp.bp.109.066274
135. Pozzi M, Carnovale C, Mazhar F, Peeters G, Gentili M, Nobile M, et al. Adverse drug reactions related to mood and emotion in pediatric patients treated for attention deficit/hyperactivity disorder: a comparative analysis of the us food and drug administration adverse event reporting system database. J Clin Psychopharmacol. (2019) 39:386–92. doi: 10.1097/JCP.0000000000001058
136. Chen Q, Sjölander A, Runeson B, D'Onofrio B, Lichtenstein P, Larsson H. Drug treatment for attention-deficit/hyperactivity disorder and suicidal behaviour: register based study. BMJ (Clinical research ed). (2014) 348:g3769. doi: 10.1136/bmj.g3769
137. McCarthy S, Cranswick N, Potts L, Taylor E, Wong I. Mortality associated with attention-deficit hyperactivity disorder (ADHD) drug treatment: a retrospective cohort study of children, adolescents and young adults using the general practice research database. Drug safety. (2009) 32:1089–96. doi: 10.2165/11317630-000000000-00000
138. Polzer J, Bangs M, Zhang S, Dellva M, Tauscher-Wisniewski S, Acharya N, et al. Meta-analysis of aggression or hostility events in randomized, controlled clinical trials of atomoxetine for ADHD. Biol Psychiatry. (2007) 61:713–9. doi: 10.1016/j.biopsych.2006.05.044
139. Swanson C, Perry K, Koch-Krueger S, Katner J, Svensson K, Bymaster F. Effect of the attention deficit/hyperactivity disorder drug atomoxetine on extracellular concentrations of norepinephrine and dopamine in several brain regions of the rat. Neuropharmacology. (2006) 50:755–60. doi: 10.1016/j.neuropharm.2005.11.022
140. Shang C, Shih H, Pan Y, Lin H, Gau S. Comparative Efficacy of Methylphenidate and Atomoxetine on Social Adjustment in Youths with Attention-Deficit/Hyperactivity Disorder. J Child Adolesc Psychopharmacol. (2020) 30:148–58. doi: 10.1089/cap.2019.0139
141. Shih H, Shang C, Gau S. Comparative Efficacy of Methylphenidate and Atomoxetine on Emotional and Behavioral Problems in Youths with Attention-Deficit/Hyperactivity Disorder. J Child Adolesc Psychopharmacol. (2019) 29:9–19. doi: 10.1089/cap.2018.0076
142. Ince Tasdelen B, Karakaya E, Oztop D. Effects of atomoxetine and osmotic release oral system-methylphenidate on executive functions in patients with combined type attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. (2015) 25:494–500. doi: 10.1089/cap.2014.0155
143. Rubio Morell B, Hernández Expósito S. Differential long-term medication impact on executive function and delay aversion in ADHD. Applied neuropsychology Child. (2019) 8:140–57. doi: 10.1080/21622965.2017.1407653
144. Koda K, Ago Y, Cong Y, Kita Y, Takuma K, Matsuda T. Effects of acute and chronic administration of atomoxetine and methylphenidate on extracellular levels of noradrenaline, dopamine and serotonin in the prefrontal cortex and striatum of mice. J Neurochem. (2010) 114:259–70. doi: 10.1111/j.1471-4159.2010.06750.x
145. Yu G, Li G, Markowitz J. Atomoxetine: a review of its pharmacokinetics and pharmacogenomics relative to drug disposition. J Child Adolesc Psychopharmacol. (2016) 26:314–26. doi: 10.1089/cap.2015.0137
146. Bhang S, Kwack Y, Joung Y, Lee S, Kim B, Sohn S, et al. Factors that Affect the adherence to ADHD medications during a treatment continuation period in children and adolescents: a nationwide retrospective cohort study using Korean Health Insurance Data from 2007 to 2011. Psychiatry Investig. (2017) 14:158–65. doi: 10.4306/pi.2017.14.2.158
147. Barner J, Khoza S, Oladapo A. ADHD medication use, adherence, persistence and cost among Texas Medicaid children. Curr Med Res Opin. (2011) 13–22. doi: 10.1185/03007995.2011.603303
148. Thiruchelvam D, Charach A, Schachar R. Moderators and mediators of long-term adherence to stimulant treatment in children with ADHD. J Am Acad Child Adolesc Psychiatry. (2001) 40:922–8. doi: 10.1097/00004583-200108000-00014
149. Atzori P, Usala T, Carucci S, Danjou F, Zuddas A. Predictive factors for persistent use and compliance of immediate-release methylphenidate: a 36-month naturalistic study. J Child Adolesc Psychopharmacol. (2009) 19:673–81. doi: 10.1089/cap.2008.0146
150. Nakano M, Witcher J, Satoi Y, Goto T. Pharmacokinetic profile and palatability of atomoxetine oral solution in healthy japanese male adults. Clin Drug Investig. (2016) 36:903–11. doi: 10.1007/s40261-016-0430-y
151. Yamaguchi H, Nagumo K, Nakashima T, Kinugawa Y, Kumaki S. Life-threatening QT prolongation in a boy with attention-deficit/hyperactivity disorder on atomoxetine. Eur J Pediatr. (2014) 173:1631–4. doi: 10.1007/s00431-013-2206-1
Keywords: atomoxetine, ADHD, children, mechanism of action, clinical efficacy, dosage, adverse reactions
Citation: Fu D, Wu D-D, Guo H-L, Hu Y-H, Xia Y, Ji X, Fang W-R, Li Y-M, Xu J, Chen F and Liu Q-Q (2022) The Mechanism, Clinical Efficacy, Safety, and Dosage Regimen of Atomoxetine for ADHD Therapy in Children: A Narrative Review. Front. Psychiatry 12:780921. doi: 10.3389/fpsyt.2021.780921
Received: 24 September 2021; Accepted: 28 December 2021;
Published: 09 February 2022.
Edited by:
Daniel Shuen Sheng Fung, Institute of Mental Health, SingaporeReviewed by:
Utkarsh Karki, Kanti Children's Hospital, NepalHsiang-Yuan Lin, University of Toronto, Canada
Copyright © 2022 Fu, Wu, Guo, Hu, Xia, Ji, Fang, Li, Xu, Chen and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Feng Chen, Y3kuY2hlbjUwOEBnbWFpbC5jb20=; Qian-Qi Liu, MTg5NTE3Njk2MTdAMTYzLmNvbQ==
†Visiting graduate student from China Pharmaceutical University
‡These authors have contributed equally to this work